1
Fouryearsofpublishedcoroners’Section28reportsonactiontopreventfuturedeathsinEnglandandWalesDrMinhAlexanderNHSwhistleblowerandformerconsultantpsychiatrist24August2017Contact:@alexander_minhandviaminhalexander.comContents PAGESummary Page1Introduction–coroners’warningreportsandpastfailuresoflearning
Page3
Databaseof4yearsofcoroners’Section28warningreports,publishedupto31July2017
Page10
Generalresults Page12NumbersofSection28reports Page17Austerityanddecency Page19Coroners’firesafetywarningsbeforeGrenfell Page21NHSsafety Page26Proportionofcoroners’warningsabouttheNHS Page23Coroners’warningsaboutambulanceservicesandrelatedmatters Page32Conclusion Page48Appendix–PresscriticismofCQCfailuretoactuponcoroners’warningsandCQCresponseSeptember2015
Page49
SUMMARYIntherecentyearsofausterity,thegovernmenthasrunanexplicitlyanti-redtapeprogramme,purportedlybusinessfriendlybutopenlyhostileto‘HealthandSafety’regulations.12
1In2012DavidCameronPMreportedlystatedthathewould“killoffthehealthandsafetycultureforgood”http://www.independent.co.uk/news/uk/politics/david-cameron-i-will-kill-off-safety-culture-6285238.html2CabinetOffice‘Cuttingredtapeprogramme’https://cutting-red-tape.cabinetoffice.gov.uk/
2
Thispapersharesadatabasecollatedfromfouryearsofcoroners’Section28warningreportsaboutpublicsafetythathavebeenpublishedbythechiefcoroner,andabroadinitialreportaboutthedata.AlthoughitispositivethatSection28reportshavebeenpublishedinrecentyears,Icollatedthisdatabecausethechiefcoroners’websiteisnotsearchableanddoesnotgivethepublicaccesssufficient,meaningfulaccesstoSection28reports.Patternsarefurtherobscuredbyinconsistentindexingofcases.Somenotableinstancesofmiscategorisationofimportantcaseswerefound(forexamplesuicides,policerelateddeaths,deathsincustody,deathsofarmedforcespersonnel).Questionsalsoariseaboutthecompletenessofthedatareleased.Itisverylikelythatanumberofreportshavenotbeenpublished.Ofthedatathatexists:
• Atleast57.2%(987of1725)ofpublishedSection28reportsrelatedtopoorNHScareandhazards.
• SeventySection28reportsrelatedtodeathsinthecustodyoftheState
• 350Section28reportsrelatedtoselfinflicteddeaths,whetherthrough
misadventureorbysuicide.
• 60Section28reportswereaboutdeathswheretherehadbeenneglect,includingeightdeathsinStatecustody.
• Themajorityofthe‘neglectcases’wereaccountedforbytheNHS.
Therewerenopublishedresponsesatallto62%(1070of1725)ofSection28reportsbyorganisationsandpersonswhohadbeensentthemforactiontopreventfuturedeaths.Moreover,noexplanationisprovidedforthisbythechiefcoroner’soffice.ThepaucityofpublishedresponsesisunexpectedbecausepastgovernmentrecordsshowedthevastmajorityoforganisationspreviouslyrespondedtoRule43reports,whichwerethepredecessortoSection28reports.ClarificationisneededonwhetherresponserateshavedeterioratedandorwhethertheChiefCoronerischoosingnottopublishresponses.Thelackofpublishedresponsestocoroners’warningsraisesquestionsaboutwhethertheauditcycleisbeingclosedandthereforetheeffectivenessofpublicprotection.TheGrenfellfirebeingthemostpainfulillustrationpossibleoftheconsequencesofsuchfailure.Relevanttofiresafety,thereweretwentypublishedSection28reportsinthelastfouryearsrelatingtofiresafety,includingrecommendationsforinstalmentoffiresprinklersandalarmsinsocialhousing,andtheneedtoinvestigatetheuseofflammableinsulatingmaterialinHotpointfridgefreezerswhichcanactasanaccelerant.
3
InrelationtoNHScases,notwithstandingthelimitationsofthecoroners’data,anumberofrecurringthemesareevident,raisingquestionsaboutorganisationallearning.Coronershighlightedalackofresourcesinanumberofimportantcases,someacute.Ofgreatconcerntopublicsafety,itisalsoclearthatcoronershavebeenseriouslyconcernedforseveralyearsaboutdeterioratingambulanceresponsesandtheroleofrelatedcallhandlinganddiversionservices.Ambulancedelayshavecostlivesandputthepublicatrisk.TheeffectivenessoftheDepartmentofHealth’sresponsetocoroners’concernsisinquestion.ThecredibilityofCQC’sratingsonambulancetrustsisalsochallengedbytheconcernsthatcoronershavebeenrepeatedlyflagging.CQC’srecentratingofanambulancetrustas‘Outstanding’isespeciallyquestionablewhenallareclearlyoperatinginseverelychallengingconditions.TheseconcernsareunderlinedbythefactthatCoroner’sSection28reportsrepresentonlythetipofasafetyiceberg.Currently,thereisnoevidenceofasystematicgovernmentapproachtolearningfromtheSection28reports.Thereisnopublishedevidenceofcentralanalysis.IhavewrittentoasktheChiefCoronerabout:
• HowmanyoftheSection28reportsissuedsofarhavebeenpublished• MissingresponsesfromrecipientsofSection28reports• Anygovernmentanalysisthatistakingplace• WhathappensifcoronersaredissatisfiedbySection28responses• Possibleimprovementstothewebsiteforgreatertransparency.
TheDepartmentofHealth,NHSregulatorsandotheroversightbodieswillbeaskedabouttheirhandlingofSection28reports.Ishouldbeverygratefulandinterestedtohearfromanyonewhoisawareofcoroners’Section28reportsthathavebeenissuedbuthavenotbeenpublished.INTRODUCTIONCoronershaveadutytoinvestigatecertaindeathsandtodeterminehowthesehappened.ThsesareuptodateHouseofCommonsbriefingsonwhatcoronersandtheChiefCoronerdo:
http://researchbriefings.parliament.uk/ResearchBriefing/Summary/SN03981http://researchbriefings.parliament.uk/ResearchBriefing/Summary/SN05721

4
Itisanimperfectsystemandheavilydependentonreporting.Coronersmaymisssalientissues.Powerfulorganisationswithunlimitedfundsforlegalservicesaremoreabletomanipulatethesystem,andbereavedfamiliesmaybedisadvantagedbyinequalityofarms.34Anumberofreformshavebeenintroduced.Debateandevaluationcontinuesonhoweffectivetheseare.56Thereisconsiderableregionalvariationinreportingtocoroners,andvariationbetweenindividualcoroners’departments.7
3Howtheinquestsystemfailsbereavedpeoplehttp://www.inquest.org.uk/pdf/how_the_inquest_system_fails_bereaved_people.pdf4DeathcertificationandinvestigationinEnglandWalesandNorthernIreland.Thereportofafundamentalreview2003.http://webarchive.nationalarchives.gov.uk/20131205105739/http://www.archive2.official-documents.co.uk/document/cm58/5831/5831.pdf5Reformofthecoroners’systemanddeathcertification,ConstitutionalAffairsCommittee,1August2006https://publications.parliament.uk/pa/cm200506/cmselect/cmconst/902/902i.pdf6ImplementingthecoronerreformsinPart1oftheCoronersandJusticeAct2009Responsetoconsultationonrules,regulations,coronerareasandstatutoryguidance.MoJ4July2013https://consult.justice.gov.uk/digital-communications/coroner-reforms/results/implementing-the-coroner-reforms-response.pdf7CoronersStatisticsAnnual2016EnglandandWales“Whenlookingatthenumberofdeathsreportedtocoronersin2016asaproportionofregistereddeaths21,whichallowforsomedifferencesinpopulationcharacteristics,thereisstillawidevariationacrosscoronerarease.g.28%inEastLancashirecomparedto96%inStoke-on-TrentandNorthStaffordshire.”“Theproportionofpost-mortemscarriedoutvariesfrom21%inNorthLincolnshireandGrimsbyto62%inIsleofWight.”“Theproportionofinquestscarriedoutvariesfrom8%inStoke-on-TrentandNorthStaffordshireto40%inNorthTyneside.”https://www.gov.uk/government/statistics/coroners-statistics-2016

5
Ofrelevance,anationalnetworkofmedicalexaminerstoimprovescrutinyofdeathsandtodetectpoorcaremorepromptlyhasbeenproposedbyvariouspublicinquiries,andstronglysupportedbytheRoyalCollegeofPathologists.89However,thishasbeenrepeatedlydelayed.Controversially,thegovernmentannouncedafurtherdelayearlierthisyear,withanewimplementationdeadlinesetfor2019.10Nevertheless,forallthelimitations,coroners’findingsprovideanimportantwindowintoriskstopublicsafety.Ofspecialinterestarethewarningreportsthatcoronersissueonanexceptionalbasiswhentheyconsiderthatactionneedstobetakentopreventfuturedeaths.Coronerspreviouslyhaddiscretionarypowerstoissuea‘Rule43’reportundertheCoronersRules1984onmattersarisingfromdeathstheyhadreviewedwhichcouldcausearecurrenceofsimilarfatalities.11
8Anoverviewofthedeathcertificationreforms.DepartmentofHealthMay2016https://www.gov.uk/government/publications/changes-to-the-death-certification-process/an-overview-of-the-death-certification-reforms9MedicalExaminers.RoyalCollegeofPathologists.May2016https://www.rcpath.org/discover-pathology/public-affairs/medical-examiners.html10StatementbyRoyalCollegeofPathologists30March2017inresponsetofurthergovernmentdelayhttps://www.rcpath.org/discover-pathology/news/medical-examiner-delay.html11“43.Acoronerwhobelievesthatactionshouldbetakentopreventtherecurrenceoffatalitiessimilartothatinrespectofwhichtheinquestisbeingheldmayannounceattheinquestthatheisreportingthematterinwritingtothepersonorauthoritywhomayhavepowertotakesuchactionandhemayreportthematteraccordingly.(a)aseniorcoronerhasbeenconductinganinvestigationunderthisPartintoaperson’sdeath,(b)anythingrevealedbytheinvestigationgivesrisetoaconcernthatcircumstancescreatingariskofotherdeathswilloccur,orwillcontinuetoexist,inthefuture,and(c)inthecoroner’sopinion,actionshouldbetakentopreventtheoccurrenceorcontinuationofsuchcircumstances,ortoeliminateorreducetheriskofdeathcreatedbysuchcircumstances,thecoronermustreportthemattertoapersonwhothecoronerbelievesmayhavepowertotakesuchaction.(2)Apersontowhomaseniorcoronermakesareportunderthisparagraphmustgivetheseniorcoronerawrittenresponsetoit.
6
ThispowerwasusedvariablyandwasreplacedwithastatutorydutyunderPart7ofSchedule5oftheCoronersandJusticeAct2009.Thisconferredawiderdutytoraiseallmattersdiscoveredduringinvestigationthatcouldpreventafuturerisktolife,whetherornottheyhadcontributedtothedeathinquestion.Suchreportsareknownasreportsonactiontopreventfuturedeaths,or“PFDs”.12OnreceiptofaSection28report,recipientsmustprovidethecoronerwithawrittenresponse,(atimelimitof56daysisgiven),andthecoronermustsendacopyoftheSection28reportandanyresponsestotheChiefCoroner,whomaypublishthem.
(3)Acopyofareportunderthisparagraph,andoftheresponsetoit,mustbesenttotheChiefCoroner.”http://www.legislation.gov.uk/uksi/1984/552/contents/made12CoronersandJusticeAct2009“Actiontopreventotherdeaths7(1)Where—(a)aseniorcoronerhasbeenconductinganinvestigationunderthisPartintoaperson’sdeath,(b)anythingrevealedbytheinvestigationgivesrisetoaconcernthatcircumstancescreatingariskofotherdeathswilloccur,orwillcontinuetoexist,inthefuture,and(c)inthecoroner’sopinion,actionshouldbetakentopreventtheoccurrenceorcontinuationofsuchcircumstances,ortoeliminateorreducetheriskofdeathcreatedbysuchcircumstances,thecoronermustreportthemattertoapersonwhothecoronerbelievesmayhavepowertotakesuchaction.(2)Apersontowhomaseniorcoronermakesareportunderthisparagraphmustgivetheseniorcoronerawrittenresponsetoit.(3)Acopyofareportunderthisparagraph,andoftheresponsetoit,mustbesenttotheChiefCoroner.”http://www.legislation.gov.uk/ukpga/2009/25/pdfs/ukpga_20090025_en.pdf
7
RecipientsofSection28reportsareofteninformedthattheymaymakerepresentationstocoronersaboutwhethertheirresponsesarepublished:
AsfarasIcansee,thereisnoprovisionsetoutintheChiefCoroner’sguidance13forcircumstanceswheretherecipientsofSection28reportsfailtorespondtocoroners.Thisseemsasignificantsystemweakness.Itseemsanoddprocessofjusticewherematterscansimplefizzleout,beyondthepubliceye.IcanseenoexplanationfromtheChiefCoroneronhowdecisionsaremadewithregardstowhetherSection28reportsandresponsesarepublishedornotpublished.Again,thisseemsanomissioninthefaceoftheprinciplethatjusticemustbeseentobedone.Section28reportsareissuedonlyinasmallnumberofinquestcases.DuetodatamissingfromtheChiefCoroner’sannualreportsonthenumberofSection28reportsthathavebeenissuedsincetheywereintroduced,itisnotpossibletosaydefinitivelywhatproportionofinquestshavegeneratedSection28reportssincethelatterwereintroducedin2013.
13TheChiefCoroner’sguidetotheCoronersandJusticeAct2009https://www.judiciary.gov.uk/publications/the-chief-coroners-guide-to-the-coroners-and-justice-act-2009/
8
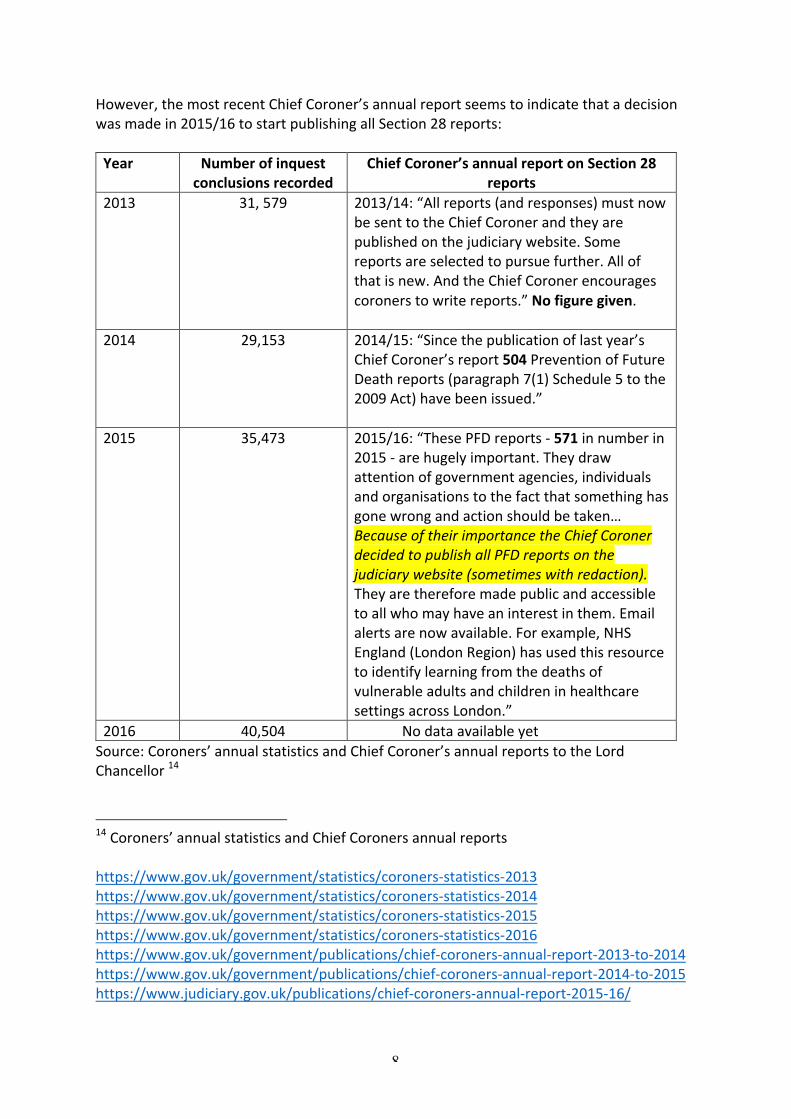
However,themostrecentChiefCoroner’sannualreportseemstoindicatethatadecisionwasmadein2015/16tostartpublishingallSection28reports:Year Numberofinquest
conclusionsrecordedChiefCoroner’sannualreportonSection28
reports2013 31,579 2013/14:“Allreports(andresponses)mustnow
besenttotheChiefCoronerandtheyarepublishedonthejudiciarywebsite.Somereportsareselectedtopursuefurther.Allofthatisnew.AndtheChiefCoronerencouragescoronerstowritereports.”Nofiguregiven.
2014 29,153 2014/15:“Sincethepublicationoflastyear’s
ChiefCoroner’sreport504PreventionofFutureDeathreports(paragraph7(1)Schedule5tothe2009Act)havebeenissued.”
2015 35,473 2015/16:“ThesePFDreports-571innumberin
2015-arehugelyimportant.Theydrawattentionofgovernmentagencies,individualsandorganisationstothefactthatsomethinghasgonewrongandactionshouldbetaken…BecauseoftheirimportancetheChiefCoronerdecidedtopublishallPFDreportsonthejudiciarywebsite(sometimeswithredaction).Theyarethereforemadepublicandaccessibletoallwhomayhaveaninterestinthem.Emailalertsarenowavailable.Forexample,NHSEngland(LondonRegion)hasusedthisresourcetoidentifylearningfromthedeathsofvulnerableadultsandchildreninhealthcaresettingsacrossLondon.”
2016 40,504 NodataavailableyetSource:Coroners’annualstatisticsandChiefCoroner’sannualreportstotheLordChancellor14
14Coroners’annualstatisticsandChiefCoronersannualreportshttps://www.gov.uk/government/statistics/coroners-statistics-2013https://www.gov.uk/government/statistics/coroners-statistics-2014https://www.gov.uk/government/statistics/coroners-statistics-2015https://www.gov.uk/government/statistics/coroners-statistics-2016https://www.gov.uk/government/publications/chief-coroners-annual-report-2013-to-2014https://www.gov.uk/government/publications/chief-coroners-annual-report-2014-to-2015https://www.judiciary.gov.uk/publications/chief-coroners-annual-report-2015-16/

9
Thereappeartohavebeenlimitedeffortstomakesystematicuseofthedatafromcoroner’swarningreports.TheChiefCoronerpreviouslypublishedperiodicsixmonthlysummariesonRule43reportswhichprovidedbriefsummariesofcoroners’concernsanddetailsofthebodiesinvolved.15AfterthesystemchangedfromRule43reportstoSection28reports,theChiefCoronerpublishedaninitialsummaryreportfortheperiod1April2013to30September2013,butnoothersseemtohavefollowed.
https://minhalexander.files.wordpress.com/2016/09/april-2013-to-september-2013-summaryreportofpfdreportsapr-sep2013-10th.pdf
Icouldfindnoothersignsofrecentanalysis,indepthorotherwise,ofwarningreports.
15MoJSummariesofReportsandResponsesunderRule43oftheCoronersRulesJuly2008toMarch2013https://minhalexander.files.wordpress.com/2016/09/july-2008-to-march-2009-summary-rule-43-v1.pdfhttps://minhalexander.files.wordpress.com/2016/09/april-2009-to-september-summary-rule-43-v2.pdfhttps://minhalexander.files.wordpress.com/2016/09/oct-2009-to-march-2010-third-summary-coroners-reports-rule43a.pdfhttps://minhalexander.files.wordpress.com/2016/09/april-2010-to-oct-2010-rule-43-coroners-report-4th.pdfhttps://minhalexander.files.wordpress.com/2016/09/oct-2010-to-march-2011-summary-rule-43-070312-5th.pdfhttps://minhalexander.files.wordpress.com/2016/09/april-2011-to-september-2010-summary-rule-43-6th.pdfhttps://minhalexander.files.wordpress.com/2016/09/oct-2011-to-march-2012-summary-rule-43-v7.pdfhttps://minhalexander.files.wordpress.com/2016/09/april-2012-to-sept-2012-summary-rule-43-report-v8.pdfhttps://minhalexander.files.wordpress.com/2016/09/oct-2012-march-2013-9th-rule-43-report.pdf
10
ThecharityINQUEST,inparticular,hasbeencriticaloftheresistancetolearningfromdeathsincustodyandmentalhealthdeaths,inwhichthesamegrievouserrorsareendlesslyrepeateddespiteveryspecificcoroners’warnings.16ThereisalsoaquestionofwhathappenswhencoronersaredissatisfiedwiththeresponsesthattheyreceivetotheirSection28reports.Itappearsthatthetrailendsuntilthenextsimilardeath,whenthecoronermakesreferencetothepasthistoryandprevioussimilardeaths.DATABASEOF4YEARSOFCORONERS’SECTION28WARNINGSPUBLISHEDUPTO31July2017SinceJuly2013allSection28reportshadtobesenttotheChiefCoronerforpossiblepublication.PublicationbeganinJanuary2014whenthethenChiefCoronerPeterThorntonreportedlyemphasisedtheimportanceoftransparency:“Iplacegreatemphasisonthevaluableworkofcoronersinsavinglivesbyhighlightingriskswhichneedtobeeliminated.Thatiswhypublishingthesereportsandputtingthemintothepublicdomainissoimportant.”17Ihavebeenfollowingthechiefcoroner’spublicationofSection28reportsforthelastyear.Ihavefoundthatreports,andresponsestothereports,areuploadedsomewhaterratically,sometimeswithvariabledelaysofmonths.Asnapshottakenatanypointintimeislikelytobeasignificantunderestimateofthereportsthatexist.IhaveloggeddetailsofallpublishedSection28reportsuptoof31July2017ontothisdownloadabledatabase:
https://minhalexander.files.wordpress.com/2017/08/all-section-28-reports-on-action-to-prevent-future-deaths-published-by-chief-coroner-up-to-31-july-2017-pub.xlsx
Thedatabaseprovideslinkstotheindividualpublishedreportsandanyassociatedresponsesbypersonstowhomthereportsweresent.Namesofdeceased,coroner’scasereferencenumbers,coroners’categoriesofdeathandcoroners’areasarealsoprovided.Thisdatacanbesearched.
16http://inquest.org.uk/pdf/INQUEST_deaths_in_mental_health_detention_Feb_2015.pdfhttp://www.inquest.org.uk/pdf/reports/Learning_from_Death_in_Custody_Inquests.pdf17https://www.crimeline.info/news/publication-of-reports-to-prevent-future-deaths
11
IhavefoundtheChiefCoroner’swebsiteuserun-friendlyforthefollowingreasons:
• Thewebsiteisnotsearchable,unlikecomparablewebsitesoperatedbytheCourtsandTribunalsJudiciary
• Pagesmustbescrolledlaboriouslyandslowly.Losingone’splacerequiresstartingagainfromsquareone,makingsearchesagargantuantask.
• Itprovidesaflawedandmisleadingsystemofindexingwhereusersaresignpostedtocategoriesofdeathwhichareinfactincomplete,becausesomecasesarenotcorrectedlabelledandrelevantcasesaredispersedthroughoutotherdifferentcategories.
Forexample,therewere94Section28reportsaboutdeathsdeterminedtobesuicides,butoverhalfofthese(54)werenotlabelledassuchontheChiefCoroner’swebsite.Theywouldhavebeenmissedbyanymemberofthepubliclookingfordeathsbysuicide,unlesstheysystematicallyscrolledthroughthewholedatabase.
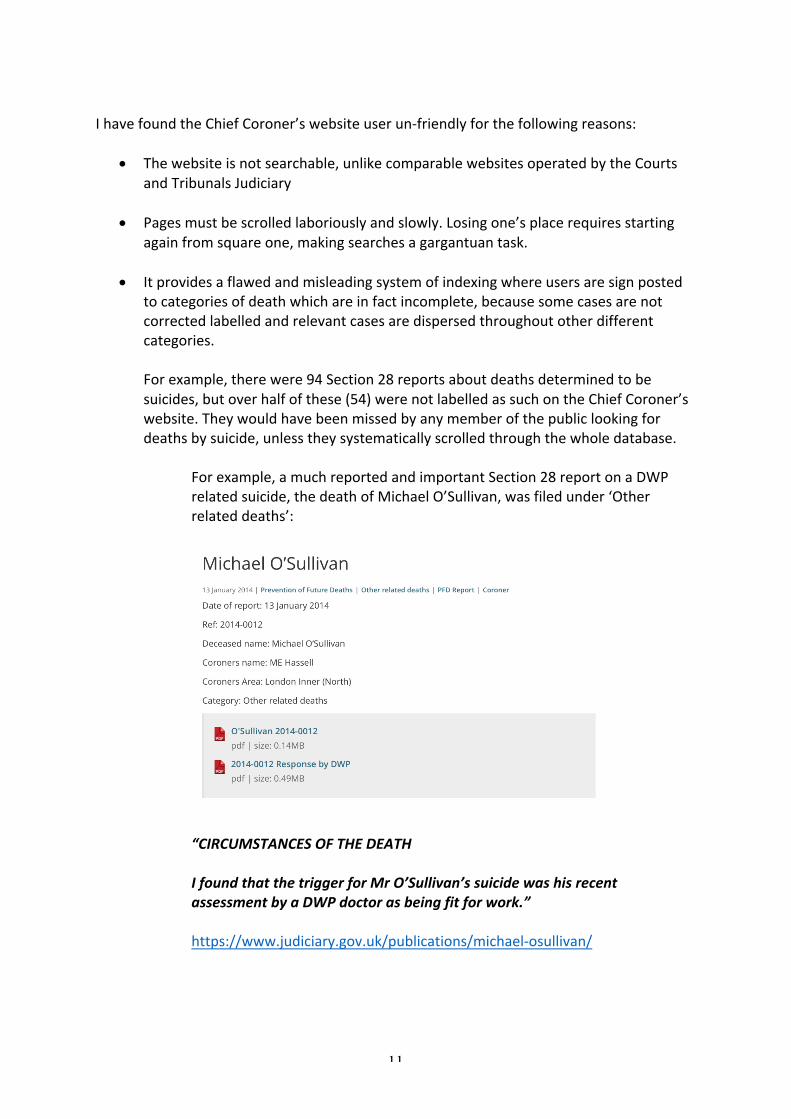
Forexample,amuchreportedandimportantSection28reportonaDWPrelatedsuicide,thedeathofMichaelO’Sullivan,wasfiledunder‘Otherrelateddeaths’:
“CIRCUMSTANCESOFTHEDEATHIfoundthatthetriggerforMrO’Sullivan’ssuicidewashisrecentassessmentbyaDWPdoctorasbeingfitforwork.”https://www.judiciary.gov.uk/publications/michael-osullivan/
12
Thiscaseandafewothermislabelledsuicidescouldbeaccountedforbythefactthatthecategoryof‘suicide’wasnotintroducedbythechiefcoroner’sofficeuntil2015.However,thisdoesnotaccountformanymislabelledSection28reportswhichwereissuedin2015andafter.Conversely,afewdeathswerelabelledassuicideswhentheSection28reportsgavenoindicationofspecificintentorevenexplicitlystatedthatnospecificintenthadbeenproven.ThisisthelistofpublishedSection28reportsonsuicides,showingwhichreportswerecorrectlylabelledandwhichwereobscured:https://minhalexander.files.wordpress.com/2016/09/section-28-reports-on-deaths-by-suicide-published-by-chief-coroner-up-to-31-july-2017.xlsx
Inadditiontosuicides,otherimportantexamplesofmislabelleddeathsincludeddeathsincustody,policerelateddeaths,servicepersonneldeathsandconstructionindustrydeaths.18
Initscurrentstate,theChiefCoroner’swebsiteisnotsufficientlyaccessibletothepublic.Thisisbecauseitdoesnotallowinterrogationwithoutextraordinaryusereffort,thereisobfuscationoftrendsandsystemicrisksbecauseofthewaydataispresented.Thereisariskthatbereavedfamiliesmaybedeniedanswers.Makingthewebsitesearchable,includingbyfreetextandbydifferentparameterssuchasdates,namesofdeceased,namesofcoroner,coronerareaandcategoryofdeathswouldincreaseaccessibilityandtransparency.GENERALRESULTSIfoundatotalof1725Section28reportsbycoronersinEnglandandWalespublishedupto31July2017,relatingtothedeathsof1799people.Theearliestofthereportshadbeenissuedon30July2013.TheSection28reportsrelatedtothedeathsofatleast1142malesand646females(dataongenderwasmissinginafewcases).
18Examplesofimportantcasesthatweremislabelledorincompletelycrossreferencedincluded:Duggan2014-0182filedunder‘Otherrelateddeaths’,Cunningham2014-0087filedunder‘Productrelateddeaths’,Overy2014-0535filedunder‘Otherrelateddeaths’,Dalrymple2014-0410filedunder‘Otherrelateddeaths’McGlasson2014-0001aconstructionindustrydeathfiledunder‘Alcohol,drugandmedicationrelateddeaths”
13
Thereatleast175childdeaths(definedasagebeloweighteen).Atleast350Section28reportsrelatedtoself-inflicteddeaths18b,withaspecificfindingofsuicideindicatedin94ofthereports.70ofthepublishedSection28reportsrelatedtodeathsinStatecustody,whichoccurredmostlyinprisonsbutalsoinpolicecustody,immigrationcentresandsecurepsychiatricunits.60ofthepublishedSection28reportsrelatedtocasesinwhichinquestshadmadefindingsofneglect,althoughinonecaseneglectwasnotedbutwasnotconsideredtohavecontributedtothedeath.Onecaseofneglect,thedeathofIvyAtkinacarehomeresident,wassogrossthataninquestmadeafindingofunlawfulkilling.Shereportedlylostalmosthalfherbodyweightin48daysandwasdiscoveredclosetodeathwithaninfectedpressuresore.Therewasanaccompanyingcriminalconvictionofmanslaughteragainstthecarehomeowner.Theregulator,CQC,wascriticisedforfailings.19Shamefully,eightofthepublished60casesofneglect(13.3%)relatedtoStatedetention.Fouroutofeightofthesecustodycasesprimarilyinvolvedprivateproviders.20
18bIhaveusedtheclassificationofselfinflicteddeath,asusedforcustodydeaths,whichencompassesbothdeathsinwhichintentofsuicideisclearbeyondreasonabledoubtandotherinstanceswherepeoplediedbytheirownhandsbutdefinitesuicidalintentwasnotfound,orwhererecklessnessandmisadventurewereconsideredtobemorelikely.19Nottinghamcarehomebossjailedformanslaughter,BBC6February2016http://www.bbc.co.uk/news/uk-england-nottinghamshire-3549986520Custodydeathswithneglectfindings-casereferencedetails:Thedetainedpatientsdiedinprison,animmigrationcentre,undertheMentalHealthActandDeprivationofLibertySafeguards.PeterBarnesCygnetHospitalRef.2013-0291,ShalaneBlackwoodHMPNottinghamRef.2016–0179,KingsleyBurrellBirminghamandSolihullMentalHealthNHSTrustRef.2015-0472,BrianDalrympleHarmondsworthImmigrationRemovalCentreGEOGroupUKLtd(formerlyG4S)Ref.2014-0410,DaleProverbsMHAPartnershipsinCareRef.2015-0010,ChristopherRoyalBaron’sParkNursingHomeRef.2014-0354,DeanSaundersHMPChelmsfordRef.2017-0056,RichardWalshHMPBelmarshRef.2016-0377

14
ThebulkoftheneglectcasesrelatedtotheNHS.Therewereanumberof‘repeatoffender’trusts.PennineAcuteNHSTrustreceivedfourSection28reportsindeathswheretherehadbeenafindingofaneglect.21Thisisthefulllistofthe60publishedcaseswhereneglecthadbeenfound:
https://minhalexander.files.wordpress.com/2016/09/section-28-reports-with-findings-of-neglect-published-up-to-31-july-20171.xlsx
ResponsesTherewerenopublishedresponsesatallto1070ofthe1725(62%)coroners’Section28reports.Therewerenopublishedresponsesfor43ofthe70(61%)section28reportsondeathsinStatecustody,whenonemightimaginethatthisisakeyareaforaccountabilityandtransparency.Therewerealsonopublishedresponsesto32ofthe60(53.3%)Section28reportsondeathswereafindingofneglecthadbeenmade.Whereresponseswerepublished,therewasnotalwaysafullsetofresponsesfromallthepartieswhohadbeensentSection28reportsasanamedrespondentforactiontopreventfuturedeath.Particularlyworryingwasalackofconsistentpublishedresponsesbygovernmentdepartmentsandoversightbodies.Forexample,therenoresponsesto60outof172Section28reportssenttotheDepartmentofHealthforactiontopreventfuturedeaths.Therewerenoresponsesto45outof100Section28sentpersonallytotheSecretaryofStateforHealthforactiontopreventfuturedeaths.Wethereforedonotknowwhataction,ifany,JeremyHuntproposedtotakeinresponsematterssuchas:
- ConcernsaboutcontinuingNeverEventsandpoorgovernanceatNorthCumbriaUniversityHospitalsNHSTrust,oneoftheso-called14‘Keogh’trusts
21PennineAcuteHospitalNHSTrustdeathswithfindingsofneglect:Ref.2017-0063,ColinMoulton10July2015Ref.2015-0267,DominicSmith30June2016Ref.2016-0240,MillyZemmel6April2016Ref.2016–0139,Ref2014-0421,KathleenCooper8March2017
15
https://www.judiciary.gov.uk/publications/amanda-coulthard/
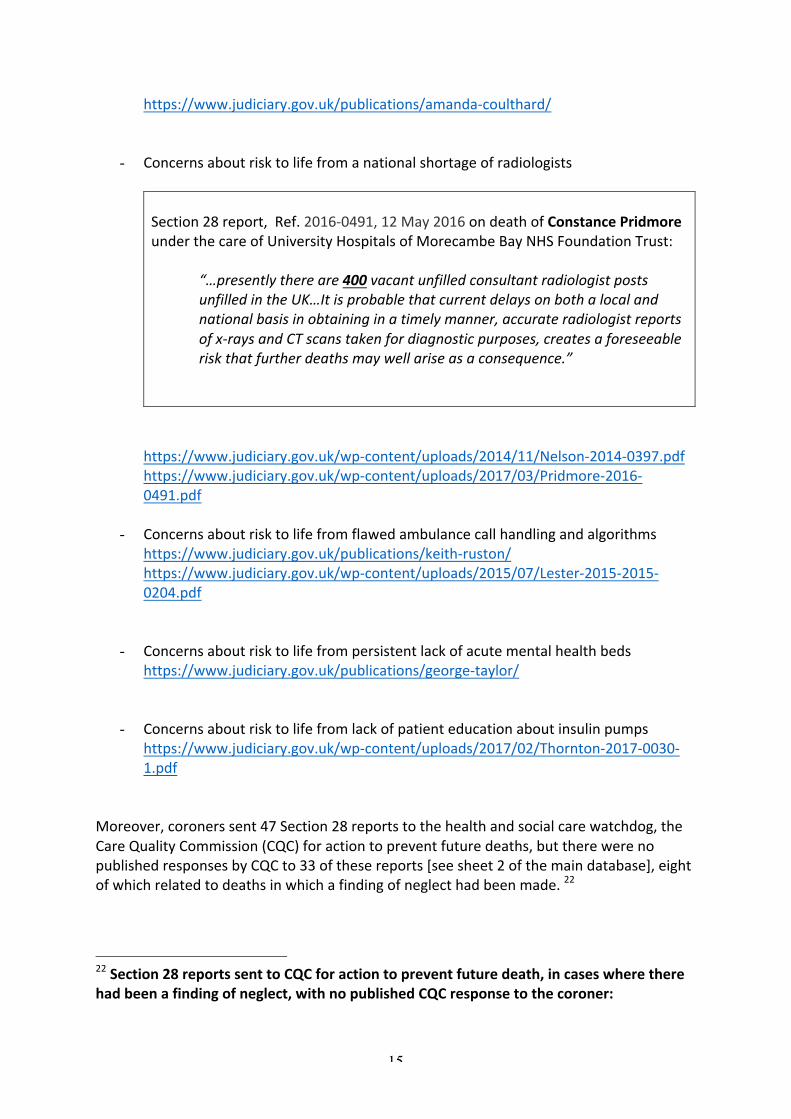
- ConcernsaboutrisktolifefromanationalshortageofradiologistsSection28report,Ref.2016-0491,12May2016ondeathofConstancePridmoreunderthecareofUniversityHospitalsofMorecambeBayNHSFoundationTrust:
“…presentlythereare400vacantunfilledconsultantradiologistpostsunfilledintheUK…Itisprobablethatcurrentdelaysonbothalocalandnationalbasisinobtaininginatimelymanner,accurateradiologistreportsofx-raysandCTscanstakenfordiagnosticpurposes,createsaforeseeableriskthatfurtherdeathsmaywellariseasaconsequence.”
https://www.judiciary.gov.uk/wp-content/uploads/2014/11/Nelson-2014-0397.pdfhttps://www.judiciary.gov.uk/wp-content/uploads/2017/03/Pridmore-2016-0491.pdf
- Concernsaboutrisktolifefromflawedambulancecallhandlingandalgorithmshttps://www.judiciary.gov.uk/publications/keith-ruston/https://www.judiciary.gov.uk/wp-content/uploads/2015/07/Lester-2015-2015-0204.pdf
- Concernsaboutrisktolifefrompersistentlackofacutementalhealthbeds
https://www.judiciary.gov.uk/publications/george-taylor/
- Concernsaboutrisktolifefromlackofpatienteducationaboutinsulinpumpshttps://www.judiciary.gov.uk/wp-content/uploads/2017/02/Thornton-2017-0030-1.pdf
Moreover,coronerssent47Section28reportstothehealthandsocialcarewatchdog,theCareQualityCommission(CQC)foractiontopreventfuturedeaths,buttherewerenopublishedresponsesbyCQCto33ofthesereports[seesheet2ofthemaindatabase],eightofwhichrelatedtodeathsinwhichafindingofneglecthadbeenmade.22
22Section28reportssenttoCQCforactiontopreventfuturedeath,incaseswheretherehadbeenafindingofneglect,withnopublishedCQCresponsetothecoroner:
16
TheCQCisinfactaspecialcasebecauseithasamemorandumofunderstandingwiththeCoroners’Society23whichensuresthatitreceivescopiesofallSection28reports,andisthustheoreticallyinapositiontotrackandactupontheintelligencethatcoronersprovide.TherearesignsthattheCQCfailstodosoandisnotopenaboutitsactivities.24ThelackofaudittrailonresponsestoSection28reportsandactiontakentopreventfuturedeathsisbothofconcernandsurprising,asthepastsummaryreportsontheoldRule43arrangements15recordedthatcoronersalmostalwaysreceivedresponsestotheirreports.Questionsariseaboutwhethertheresponseratehasdeteriorated,oralternatively,whytheresponsestoSection28reportsarenotbeingpublishedandwhetherthisisjustifiable.Thelackoftransparencyandpublicaccountabilityrunscountertotheacceptedprinciplethatjusticeshouldbeseentobedone.Togiveaspecificexample,therewasnopublishedCQCresponsetoaSection28reportonIvyAtkin’sabovedeathduetounlawfulkillingfromgrossneglect.
https://www.judiciary.gov.uk/publications/ivy-atkin/(TheCQC’sresponsetothecoronerwaspublishedsomeafter11August2017whenthefailuretopublishhadbeenpointedout).https://www.judiciary.gov.uk/publications/dorothy-clarkson/https://www.judiciary.gov.uk/publications/edwin-thompson/https://www.judiciary.gov.uk/publications/barbara-cooke/https://www.judiciary.gov.uk/publications/crittall-mr/https://www.judiciary.gov.uk/publications/beryl-farmer/https://www.judiciary.gov.uk/publications/crittall-mr/https://www.judiciary.gov.uk/publications/tommi-ray-vigrass/23MemorandumofunderstandingbetweenCQCandCoronersSocietyofEnglandandWaleshttps://minhalexander.files.wordpress.com/2016/09/mou_cqc_and_csocew_final.pdf24https://minhalexander.com/2016/11/11/coroners-warnings-terminal-inexactitude-and-cqc-opacity/https://minhalexander.com/2016/10/08/care-home-deaths-and-more-broken-cqc-promised/https://minhalexander.com/2016/09/25/letter-9-september-2016-to-david-behan-cqc-chief-executive-on-cqc-under-reporting-of-coroners-mental-health-deaths-warnings/
17
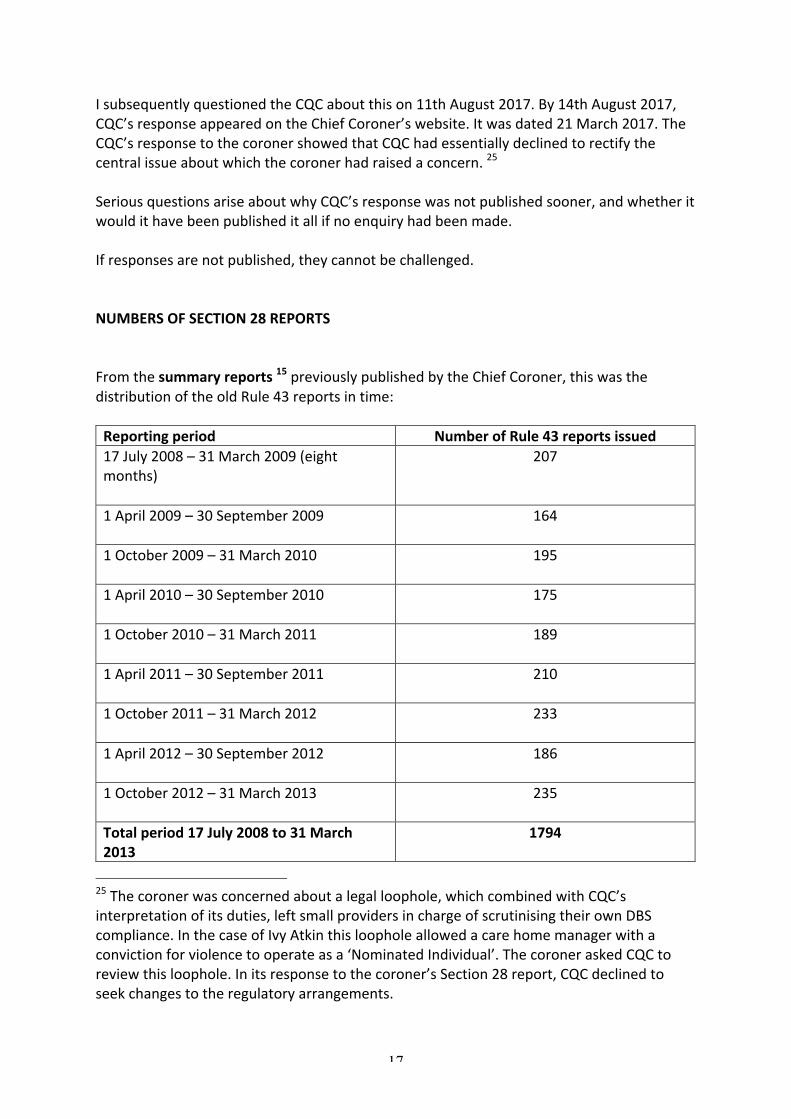
IsubsequentlyquestionedtheCQCaboutthison11thAugust2017.By14thAugust2017,CQC’sresponseappearedontheChiefCoroner’swebsite.Itwasdated21March2017.TheCQC’sresponsetothecoronershowedthatCQChadessentiallydeclinedtorectifythecentralissueaboutwhichthecoronerhadraisedaconcern.25SeriousquestionsariseaboutwhyCQC’sresponsewasnotpublishedsooner,andwhetheritwouldithavebeenpublisheditallifnoenquiryhadbeenmade.Ifresponsesarenotpublished,theycannotbechallenged.NUMBERSOFSECTION28REPORTSFromthesummaryreports15previouslypublishedbytheChiefCoroner,thiswasthedistributionoftheoldRule43reportsintime:Reportingperiod NumberofRule43reportsissued17July2008–31March2009(eightmonths)
207
1April2009–30September2009
164
1October2009–31March2010
195
1April2010–30September2010
175
1October2010–31March2011
189
1April2011–30September2011
210
1October2011–31March2012
233
1April2012–30September2012
186
1October2012–31March2013
235
Totalperiod17July2008to31March2013
1794
25Thecoronerwasconcernedaboutalegalloophole,whichcombinedwithCQC’sinterpretationofitsduties,leftsmallprovidersinchargeofscrutinisingtheirownDBScompliance.InthecaseofIvyAtkinthisloopholeallowedacarehomemanagerwithaconvictionforviolencetooperateasa‘NominatedIndividual’.ThecoroneraskedCQCtoreviewthisloophole.Initsresponsetothecoroner’sSection28report,CQCdeclinedtoseekchangestotheregulatoryarrangements.
18
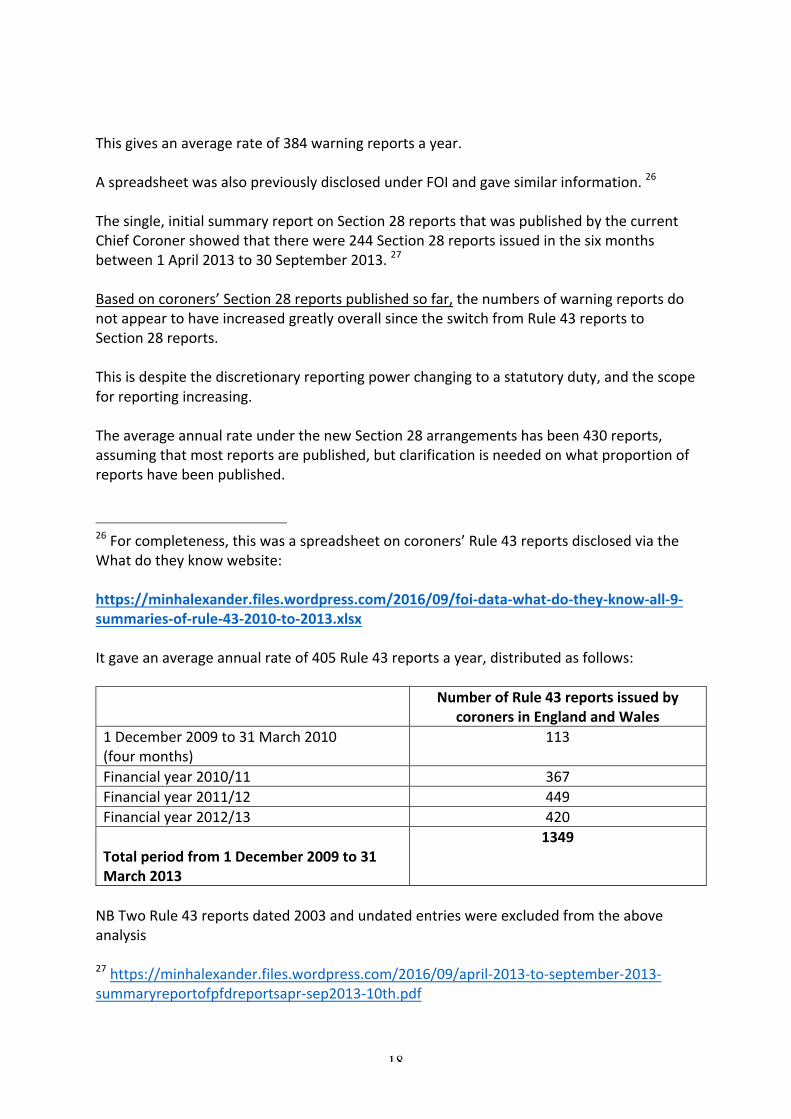
Thisgivesanaveragerateof384warningreportsayear.AspreadsheetwasalsopreviouslydisclosedunderFOIandgavesimilarinformation.26Thesingle,initialsummaryreportonSection28reportsthatwaspublishedbythecurrentChiefCoronershowedthattherewere244Section28reportsissuedinthesixmonthsbetween1April2013to30September2013.27Basedoncoroners’Section28reportspublishedsofar,thenumbersofwarningreportsdonotappeartohaveincreasedgreatlyoverallsincetheswitchfromRule43reportstoSection28reports.Thisisdespitethediscretionaryreportingpowerchangingtoastatutoryduty,andthescopeforreportingincreasing.TheaverageannualrateunderthenewSection28arrangementshasbeen430reports,assumingthatmostreportsarepublished,butclarificationisneededonwhatproportionofreportshavebeenpublished.
26Forcompleteness,thiswasaspreadsheetoncoroners’Rule43reportsdisclosedviatheWhatdotheyknowwebsite:https://minhalexander.files.wordpress.com/2016/09/foi-data-what-do-they-know-all-9-summaries-of-rule-43-2010-to-2013.xlsxItgaveanaverageannualrateof405Rule43reportsayear,distributedasfollows: NumberofRule43reportsissuedby
coronersinEnglandandWales1December2009to31March2010(fourmonths)
113
Financialyear2010/11 367Financialyear2011/12 449Financialyear2012/13 420Totalperiodfrom1December2009to31March2013
1349
NBTwoRule43reportsdated2003andundatedentrieswereexcludedfromtheaboveanalysis27https://minhalexander.files.wordpress.com/2016/09/april-2013-to-september-2013-summaryreportofpfdreportsapr-sep2013-10th.pdf
19
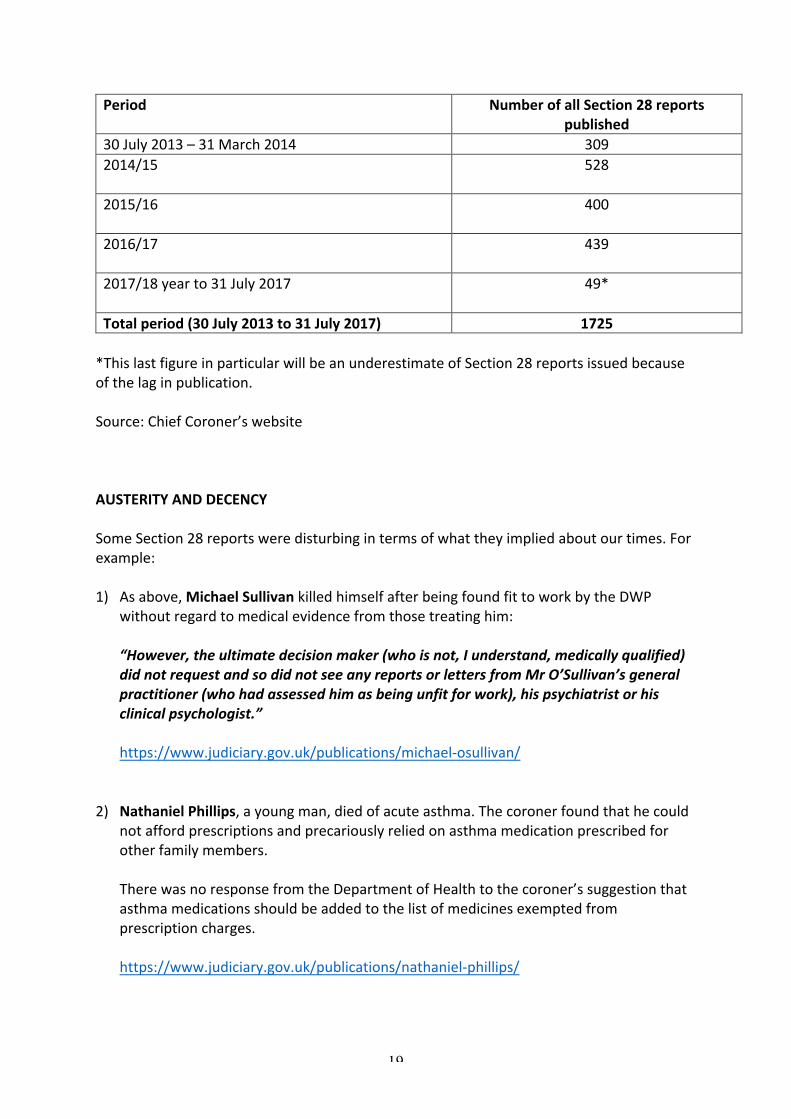
Period NumberofallSection28reportspublished
30July2013–31March2014 3092014/15
528
2015/16
400
2016/17
439
2017/18yearto31July2017
49*
Totalperiod(30July2013to31July2017) 1725*ThislastfigureinparticularwillbeanunderestimateofSection28reportsissuedbecauseofthelaginpublication.Source:ChiefCoroner’swebsiteAUSTERITYANDDECENCYSomeSection28reportsweredisturbingintermsofwhattheyimpliedaboutourtimes.Forexample:1) Asabove,MichaelSullivankilledhimselfafterbeingfoundfittoworkbytheDWP
withoutregardtomedicalevidencefromthosetreatinghim:
“However,theultimatedecisionmaker(whoisnot,Iunderstand,medicallyqualified)didnotrequestandsodidnotseeanyreportsorlettersfromMrO’Sullivan’sgeneralpractitioner(whohadassessedhimasbeingunfitforwork),hispsychiatristorhisclinicalpsychologist.”https://www.judiciary.gov.uk/publications/michael-osullivan/
2) NathanielPhillips,ayoungman,diedofacuteasthma.Thecoronerfoundthathecould
notaffordprescriptionsandprecariouslyreliedonasthmamedicationprescribedforotherfamilymembers.TherewasnoresponsefromtheDepartmentofHealthtothecoroner’ssuggestionthatasthmamedicationsshouldbeaddedtothelistofmedicinesexemptedfromprescriptioncharges.https://www.judiciary.gov.uk/publications/nathaniel-phillips/

20
3) MalcolmBurgearetiredgardenerwithnohistoryofdebtsethimselfonfireafterNewhamCouncilpursuedhimforadebtof£800.69thatarosefromoverpaymentofhousingbenefitandcounciltaxbenefit.https://www.judiciary.gov.uk/publications/malcolm-burge/
4) Inanumberofrailwaydeaths(LewisGhessen9June2015,MichaelBovell29June
2015,LaurisKodors13September2016)coronersnotedthatRSSBrulesallowtraindriverstostopifapersononthetracksmightdamageatrain,butnotviceversa.
https://www.judiciary.gov.uk/publications/lewis-ghessen/https://www.judiciary.gov.uk/publications/michael-bovell/https://www.judiciary.gov.uk/publications/lauris-kodors/
5) TheaccidentaldeathofGarrettElseywhoshelteredinacommercialwastebinovernight.Thecoroner’ssection28reportrevealedthatnotonlydoesoursocietyneedrulestopreventinjuriestopeoplewhosleepinbins,butthatthesearenotalwaysfollowed.https://www.judiciary.gov.uk/publications/elsey-2013-0316/HealthandSafetyExecutive25:https://minhalexander.files.wordpress.com/2016/09/hse-waste25-people-in-commercial-waste-containers.pdf
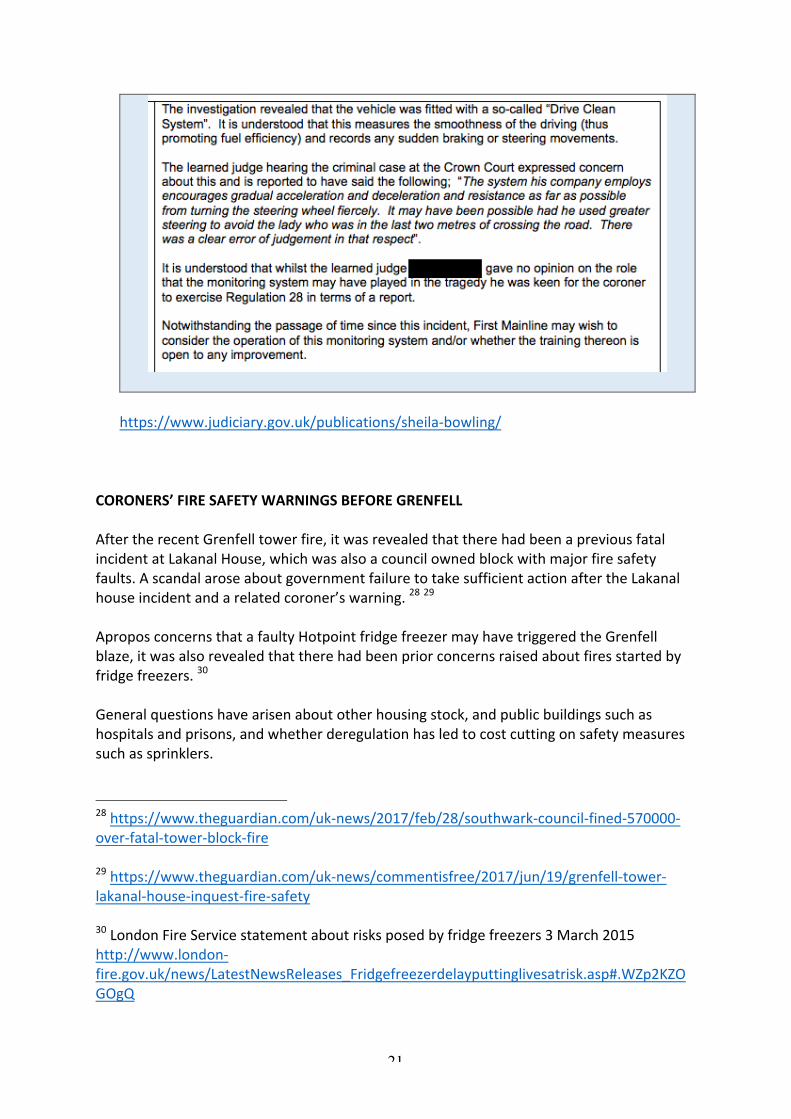
6) ThedeathofSheilaBowlingwhowasknockeddownbyabusrevealedthatthebuscompanyoperatedasystemofdrivingwhichinvolvedminimalacceleration,brakingandsharpturns.Thissavesonfuel.
21
https://www.judiciary.gov.uk/publications/sheila-bowling/
CORONERS’FIRESAFETYWARNINGSBEFOREGRENFELLAftertherecentGrenfelltowerfire,itwasrevealedthattherehadbeenapreviousfatalincidentatLakanalHouse,whichwasalsoacouncilownedblockwithmajorfiresafetyfaults.AscandalaroseaboutgovernmentfailuretotakesufficientactionaftertheLakanalhouseincidentandarelatedcoroner’swarning.2829AproposconcernsthatafaultyHotpointfridgefreezermayhavetriggeredtheGrenfellblaze,itwasalsorevealedthattherehadbeenpriorconcernsraisedaboutfiresstartedbyfridgefreezers.30Generalquestionshavearisenaboutotherhousingstock,andpublicbuildingssuchashospitalsandprisons,andwhetherderegulationhasledtocostcuttingonsafetymeasuressuchassprinklers.
28https://www.theguardian.com/uk-news/2017/feb/28/southwark-council-fined-570000-over-fatal-tower-block-fire29https://www.theguardian.com/uk-news/commentisfree/2017/jun/19/grenfell-tower-lakanal-house-inquest-fire-safety30LondonFireServicestatementaboutrisksposedbyfridgefreezers3March2015http://www.london-fire.gov.uk/news/LatestNewsReleases_Fridgefreezerdelayputtinglivesatrisk.asp#.WZp2KZOGOgQ

22
ApublicinquiryintoGrenfellisnowunderway.Thisisthecoroner’sRule43documentationontheLakanalHousefire,withkeyresponses:
https://minhalexander.files.wordpress.com/2016/09/lakanal-house-ec-letter-to-dclg-pursuant-to-rule43-28march2013.pdf
https://minhalexander.files.wordpress.com/2016/09/lakanal-house-ec-letter-to-london-borough-southwark-pursuant-to-rule43-28march2013.pdfhttps://minhalexander.files.wordpress.com/2016/09/lakanal-house-ec-letter-to-london-fire-brigade-pursuant-to-rule43-28march2013.pdfhttps://minhalexander.files.wordpress.com/2016/09/lakanal-house-ec-letter-from-rt-hon-eric-pickles-mp-20may2013.pdfhttps://minhalexander.files.wordpress.com/2016/09/lakanal-house-ec-london-borough-southwark-letter-response-to-rule-43-23may2013.pdfhttps://minhalexander.files.wordpress.com/2016/09/lakanal-house-ec-london-fire-brigade-response-to-coroners-rule43-report-23may2013.pdf
Inthelastfouryears,beforetheGrenfelldeaths,therehavebeentwentycoroners’Section28reportspublishedonfirerelateddeaths.TheseSection28reportshaveincludedmatterssuchastheneedtoensurethatsprinklersandsmokealarmsareinstalledinhousingstock,especiallyforvulnerablepeoplewithreducedmobilityoratgreaterriskofcausingfires,issuesaboutemergencyresponseandcutstofireservicesandtheriskoffirepresentedbyHotpointfridgefreezersbecauseofaflammableinsulantthatcanactasafireaccelerant.Someofthecasesareasfollows:1. DeathofEmmaWaringavulnerableadult.Thecoroneradvisedthatregulationsshould
beamendedtoincludeinstallationofsprinklersespeciallyinhousingforvulnerablepeople.TherewasnopublishedresponsebytheDepartmentforCommunitiesandLocalGovernment.

23
https://www.judiciary.gov.uk/publications/emma-waring/
2. UnlawfulkillingofStephenHuntafiremanrelatedtoanincidentofarson,inwhichthe
coronermadeadetailedfindingaboutFireServiceoperationswithnationalimplications,addressedtoTheresaMayasthethenHomeSecretary.TherewasnopublishedresponsebytheHomeOffice.http://www.manchestereveningnews.co.uk/news/greater-manchester-news/stephen-hunt-inquest-jury-finds-11350611http://www.manchestereveningnews.co.uk/news/greater-manchester-news/stephen-hunt-inquest-jury-finds-11350611
3. DeathofEllenKellyinaCamdenCouncilblockofflats,inwhichthecoronerfounda
numberoffiresafetybreaches.
https://www.judiciary.gov.uk/publications/ellen-kelly/
24
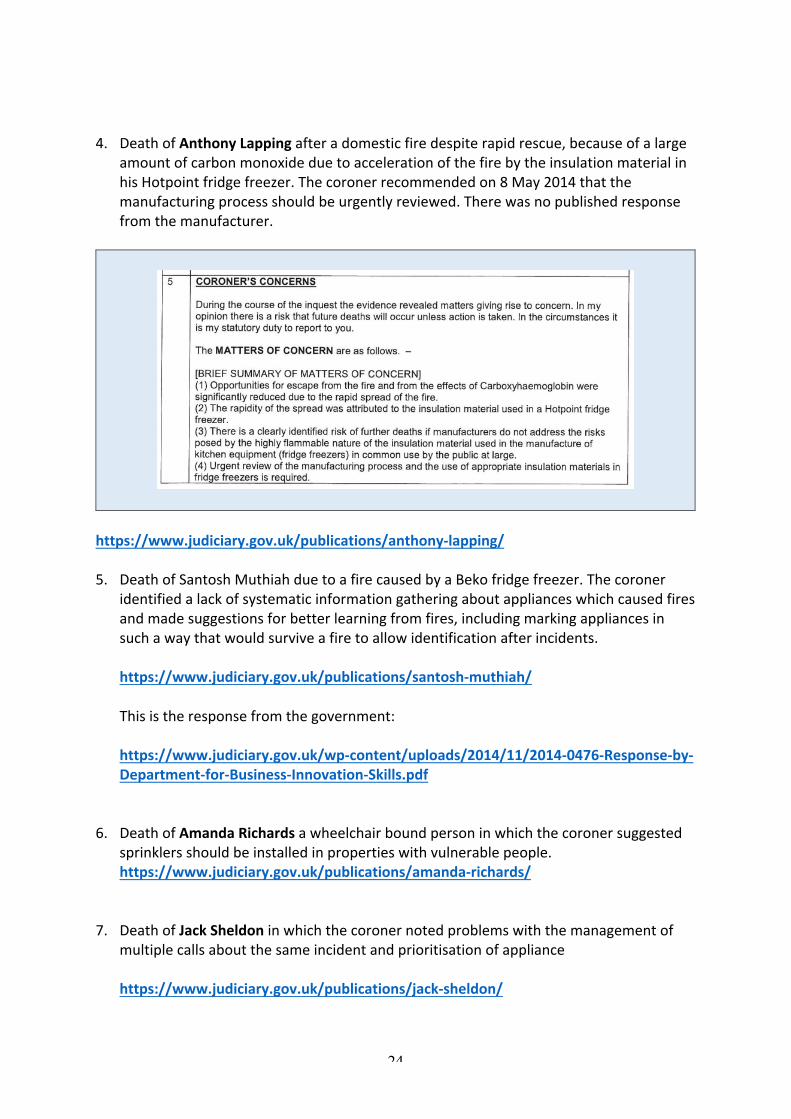
4. DeathofAnthonyLappingafteradomesticfiredespiterapidrescue,becauseofalargeamountofcarbonmonoxideduetoaccelerationofthefirebytheinsulationmaterialinhisHotpointfridgefreezer.Thecoronerrecommendedon8May2014thatthemanufacturingprocessshouldbeurgentlyreviewed.Therewasnopublishedresponsefromthemanufacturer.
https://www.judiciary.gov.uk/publications/anthony-lapping/
5. DeathofSantoshMuthiahduetoafirecausedbyaBekofridgefreezer.Thecoroner
identifiedalackofsystematicinformationgatheringaboutapplianceswhichcausedfiresandmadesuggestionsforbetterlearningfromfires,includingmarkingappliancesinsuchawaythatwouldsurviveafiretoallowidentificationafterincidents.https://www.judiciary.gov.uk/publications/santosh-muthiah/Thisistheresponsefromthegovernment:https://www.judiciary.gov.uk/wp-content/uploads/2014/11/2014-0476-Response-by-Department-for-Business-Innovation-Skills.pdf
6. DeathofAmandaRichardsawheelchairboundpersoninwhichthecoronersuggestedsprinklersshouldbeinstalledinpropertieswithvulnerablepeople.https://www.judiciary.gov.uk/publications/amanda-richards/
7. DeathofJackSheldoninwhichthecoronernotedproblemswiththemanagementofmultiplecallsaboutthesameincidentandprioritisationofappliancehttps://www.judiciary.gov.uk/publications/jack-sheldon/
25
8. DeathofKennethBaileyinwhichthecoronernotedreportsfromlocalresidentsthatduetoveryparttimeopeninghoursofalocalfirestation,thefireserviceresponsewasnotasfastasitusedtobe.https://www.judiciary.gov.uk/publications/kenneth-bailey/
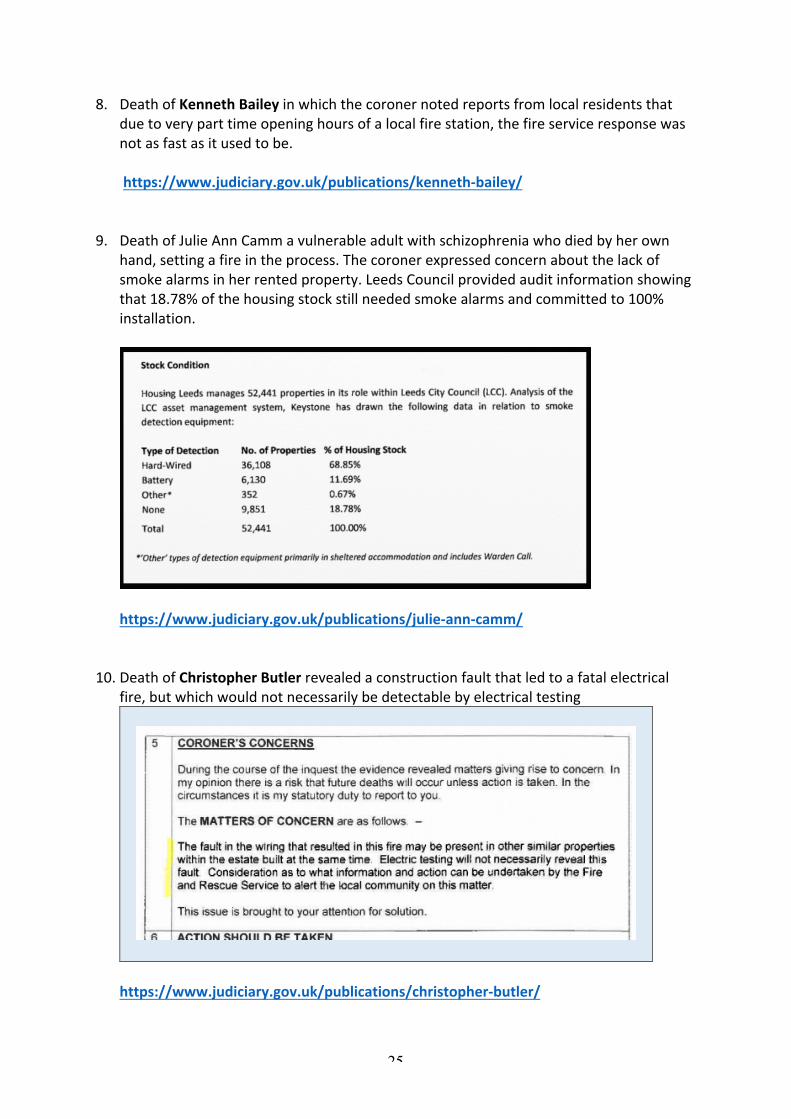
9. DeathofJulieAnnCammavulnerableadultwithschizophreniawhodiedbyherown
hand,settingafireintheprocess.Thecoronerexpressedconcernaboutthelackofsmokealarmsinherrentedproperty.LeedsCouncilprovidedauditinformationshowingthat18.78%ofthehousingstockstillneededsmokealarmsandcommittedto100%installation.
https://www.judiciary.gov.uk/publications/julie-ann-camm/
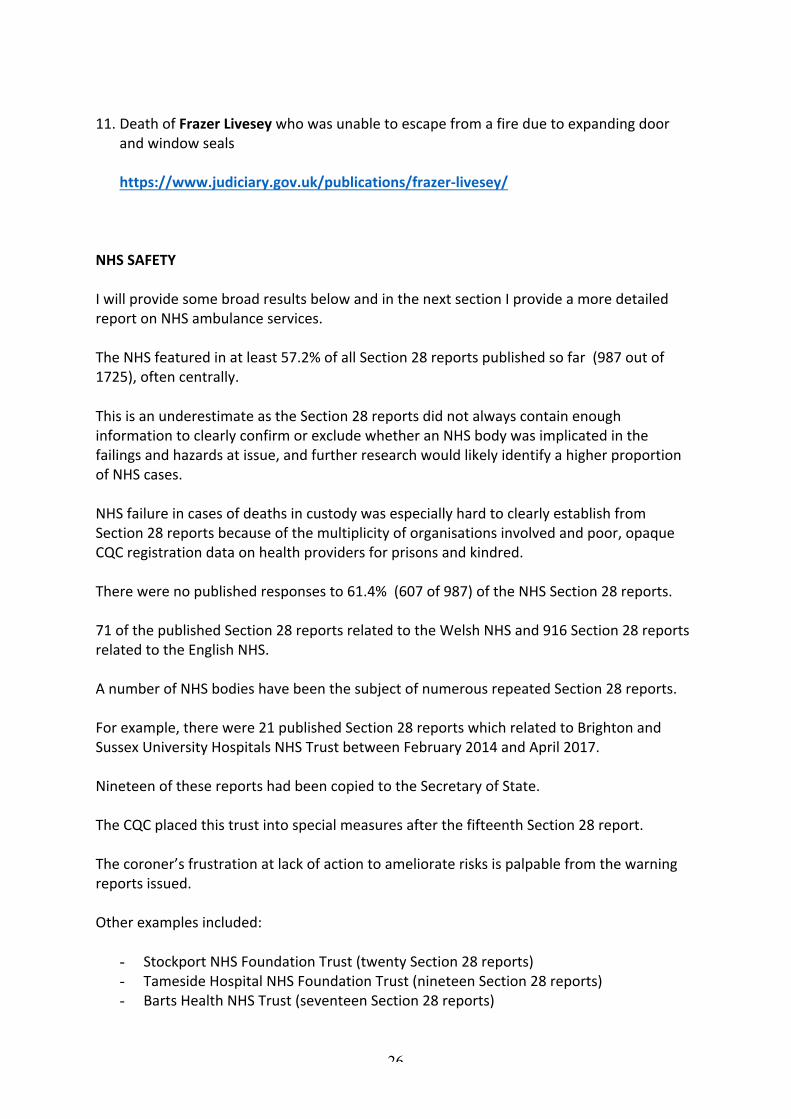
10. DeathofChristopherButlerrevealedaconstructionfaultthatledtoafatalelectrical
fire,butwhichwouldnotnecessarilybedetectablebyelectricaltesting
https://www.judiciary.gov.uk/publications/christopher-butler/
26
11. DeathofFrazerLiveseywhowasunabletoescapefromafireduetoexpandingdoor
andwindowsealshttps://www.judiciary.gov.uk/publications/frazer-livesey/
NHSSAFETYIwillprovidesomebroadresultsbelowandinthenextsectionIprovideamoredetailedreportonNHSambulanceservices.TheNHSfeaturedinatleast57.2%ofallSection28reportspublishedsofar(987outof1725),oftencentrally.ThisisanunderestimateastheSection28reportsdidnotalwayscontainenoughinformationtoclearlyconfirmorexcludewhetheranNHSbodywasimplicatedinthefailingsandhazardsatissue,andfurtherresearchwouldlikelyidentifyahigherproportionofNHScases.NHSfailureincasesofdeathsincustodywasespeciallyhardtoclearlyestablishfromSection28reportsbecauseofthemultiplicityoforganisationsinvolvedandpoor,opaqueCQCregistrationdataonhealthprovidersforprisonsandkindred.Therewerenopublishedresponsesto61.4%(607of987)oftheNHSSection28reports.71ofthepublishedSection28reportsrelatedtotheWelshNHSand916Section28reportsrelatedtotheEnglishNHS.AnumberofNHSbodieshavebeenthesubjectofnumerousrepeatedSection28reports.Forexample,therewere21publishedSection28reportswhichrelatedtoBrightonandSussexUniversityHospitalsNHSTrustbetweenFebruary2014andApril2017.NineteenofthesereportshadbeencopiedtotheSecretaryofState.TheCQCplacedthistrustintospecialmeasuresafterthefifteenthSection28report.Thecoroner’sfrustrationatlackofactiontoamelioraterisksispalpablefromthewarningreportsissued.Otherexamplesincluded:
- StockportNHSFoundationTrust(twentySection28reports)- TamesideHospitalNHSFoundationTrust(nineteenSection28reports)- BartsHealthNHSTrust(seventeenSection28reports)

27
- PennineAcuteNHSTrust(sixteenSection28reports)- SussexPartnershipNHSFoundationTrust(thirteenSection28reports)- NorfolkandSuffolkNHSFoundationTrust(twelveSection28reports)
ThereferencedetailsoftherelevantSection28reportsarelistedhere:
https://minhalexander.files.wordpress.com/2016/09/examples-of-nhs-trusts-which-have-been-subject-to-repeated-coroners_-section-28-reports-for-action-to-prevent-future-deaths2.pdf
SomeofCQC’sflagship‘Oustanding’trustshavealsobeensubjecttorepeatedSection28reports,somerecent,forexampleSalfordRoyalNHSFoundationTrustandWestMidlandsAmbulanceService:Coroner’sSection28reportspublishedonSalfordRoyalNHSFoundationTrustupto31July2017:1 GordonArthur,Ref.2017-0009,issued2February20172 PaulAshton,Ref.2014-0170,issued14April20143 DanielMcCallumKeane,Ref.2014-0260,issued9June144 MartinDeane,Ref.2014-0416,issued22September2014CQCratedSalfordRoyalNHSFoundationTrust‘Outstandingon27March2015“Theconceptofprovidingsafe,harmfreecarewasconsideredasaprioritybyallmembersofstaff.”5 StanleyOliver,Ref.2015-0281,issued16July20156 WendyThorne,Ref.2016-0408,issued11November20167 NatalieThornton,Ref.2017-0030,issued6February20178 KatherineDerbyshire,Ref.201,7-0199,issued16June2017
Coroner’sSection28reportspublishedonWestMidlandsAmbulanceNHSFoundationTrustupto31July2017:1 MaryWaldron,Ref.2014-0127,issued10January2014
2 CarolineCrowther,Ref.2014-0418,issued24September20143 KingsleyBurrell,Ref.2015-0472,issued20March20154 FrederickWhite,Ref.2015-0212,issued3June20155 CaraghMelling,Ref.2016–0167,issued27April2016
Inthiscase,WMASacknowledgedthatitstriagesystemdidnotdetectagonalbreathing(asignofcriticalillness)
6 JaneReason,Ref.2016-0376,issued25October2016

28
Inthiscase,WMAS’defibrillationequipmentfailedandabackupbatterywasflat.
7 RexHall,Ref.2016-0422,issued29November2016Inthiscase,thecoronerfoundthatWMASparamedicswereunabletoreadanECGinordertotellifapatienthadsufferedaheartattack)
On25January2017,CQCratedWestMidlandsAmbulanceService‘Outstanding’“Staffwerecompetentintheirrolesandprovidedwithtimelyappraisalsandlearningopportunities.”ThenumbersofpublishedSection28reportsonWelshNHSHealthBoardswereasfollows:WelshNHSHealthBoard NumberofpublishedSection28reports
upto31July2017BetsiCadwaladrUniversityHealthBoard
24reports
CwmTafUniversityHealthBoard 13reportsAbertaweBroMorgannwgUniversityHealthBoard
10reports
CardiffandValeUniversityHealthBoard 9reports
HywelDdaUniversityHealthBoard 6reportsAneurinBevanUniversityHealthBoard 6reportsPowysTeachingHealthBoard 1reportThesearetherelevantcasereferencesforWelshhealthboards:
https://minhalexander.files.wordpress.com/2016/09/section-28-reports-relating-to-welsh-nhs-health-boards-published-by-the-chief-coroner-up-to-31-july-2017.pdf
Ishouldstressagainthatthesefiguresarebasedononlyonpublishedreports,andthatclarificationisneededontheactualnumberofreportsissued.Also,organisationsmaysometimeshavelowernumbernumbersofcoroners’warningsdespitesafetyconcerns.Forexample,SouthernHealthNHSFoundationTrustattractedonlyahandfulofcoroners’warningreportsintheperiodinwhichhundredsofdeathswerenotproperlyreviewed.31
31TheMazarsdeathsreviewofSouthernHealthNHSFoundationTrustreportedthattherewere375inquestsontrustpatientsduringtheperiodcoveredbythereview(April2011toMarch2015)–page174:
29
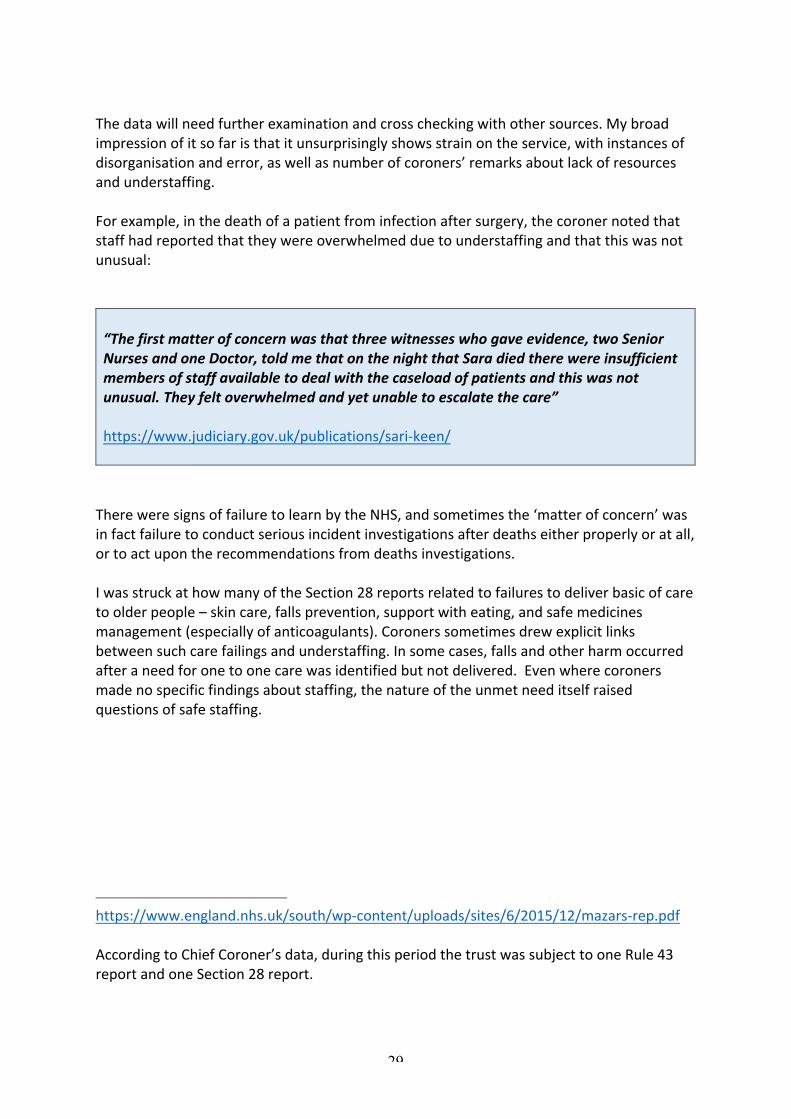
Thedatawillneedfurtherexaminationandcrosscheckingwithothersources.Mybroadimpressionofitsofaristhatitunsurprisinglyshowsstrainontheservice,withinstancesofdisorganisationanderror,aswellasnumberofcoroners’remarksaboutlackofresourcesandunderstaffing.Forexample,inthedeathofapatientfrominfectionaftersurgery,thecoronernotedthatstaffhadreportedthattheywereoverwhelmedduetounderstaffingandthatthiswasnotunusual:“Thefirstmatterofconcernwasthatthreewitnesseswhogaveevidence,twoSeniorNursesandoneDoctor,toldmethatonthenightthatSaradiedtherewereinsufficientmembersofstaffavailabletodealwiththecaseloadofpatientsandthiswasnotunusual.Theyfeltoverwhelmedandyetunabletoescalatethecare”https://www.judiciary.gov.uk/publications/sari-keen/ThereweresignsoffailuretolearnbytheNHS,andsometimesthe‘matterofconcern’wasinfactfailuretoconductseriousincidentinvestigationsafterdeathseitherproperlyoratall,ortoactupontherecommendationsfromdeathsinvestigations.IwasstruckathowmanyoftheSection28reportsrelatedtofailurestodeliverbasicofcaretoolderpeople–skincare,fallsprevention,supportwitheating,andsafemedicinesmanagement(especiallyofanticoagulants).Coronerssometimesdrewexplicitlinksbetweensuchcarefailingsandunderstaffing.Insomecases,fallsandotherharmoccurredafteraneedforonetoonecarewasidentifiedbutnotdelivered.Evenwherecoronersmadenospecificfindingsaboutstaffing,thenatureoftheunmetneeditselfraisedquestionsofsafestaffing.
https://www.england.nhs.uk/south/wp-content/uploads/sites/6/2015/12/mazars-rep.pdfAccordingtoChiefCoroner’sdata,duringthisperiodthetrustwassubjecttooneRule43reportandoneSection28report.
30
ToputahumanfaceontheNHSSection28reports,hereareafewstrikingcases:
ErrolManndiedofpulmonaryembolismafterfailuretoameliorateknownrisks.ITUstaffinglevelsreportedlycontributedtohisdeath.Awitnessreportedthattherewerepersistentmedicalstaffrotagaps,akeyissueinthebitterdisputebetweentheSecretaryofStateandthejuniordoctors.TherewasnopublishedresponsefromanypartysenttheSection28reportforactiontopreventfuturedeaths.https://www.judiciary.gov.uk/publications/errol-mann/
DrJohnDaviesdiedalonelydeathbyhisownhandinahotelroom,withafindingbythecoronerabouttheGMC’sbehaviourtowardsdoctorswhowerethesubjectofcomplaints.TherewasnopublishedresponsebytheGMCtotheSection28report.https://www.judiciary.gov.uk/publications/john-davies/AlvaJulliendiedofpneumoniadueto‘recumbency’imposeduponherbydelayeddischargefromhospitalfornogoodreasonanddespitethefactthatherfamilywouldhavebeenwillingtocareforher.Shewasmadenilbymouthwithoutsufficientevidencethatthisiswasappropriate,andplacedonthenotoriousLiverpoolcarepathway.TherewasnopublishedresponsebyStockportNHSFoundationTrusttotheSection28report.https://www.judiciary.gov.uk/publications/jullien-2013-0232/MohammedChaudhurysufferedmultipleinjuriesafteratrafficcollisionanddiedofsepticpressuresoresof‘unusualinextentandseverity’whichdevelopedatKingsCollegeHospitalNHSFoundationTrust.TherewasnopublishedresponsefromthetrustorfromMikeRichards,formerCQCChiefInspectortotheSection28report.https://www.judiciary.gov.uk/publications/mohammed-chaudhury/CarolGibsondiedofafatalreactiontoadrugwhichshehadbeenprescribedforafourthandfinaltimeinerrorbyherGPpractice,allafterithadbeenflaggedbyhospitalsservicesthatshehadsufferedanearlier,seriousadversereactiontothisdrug.TherewasnopublishedresponsebyherGPsurgeryorbyNHSEnglandtotheSection28report.https://www.judiciary.gov.uk/publications/carol-ann-gibson/
31
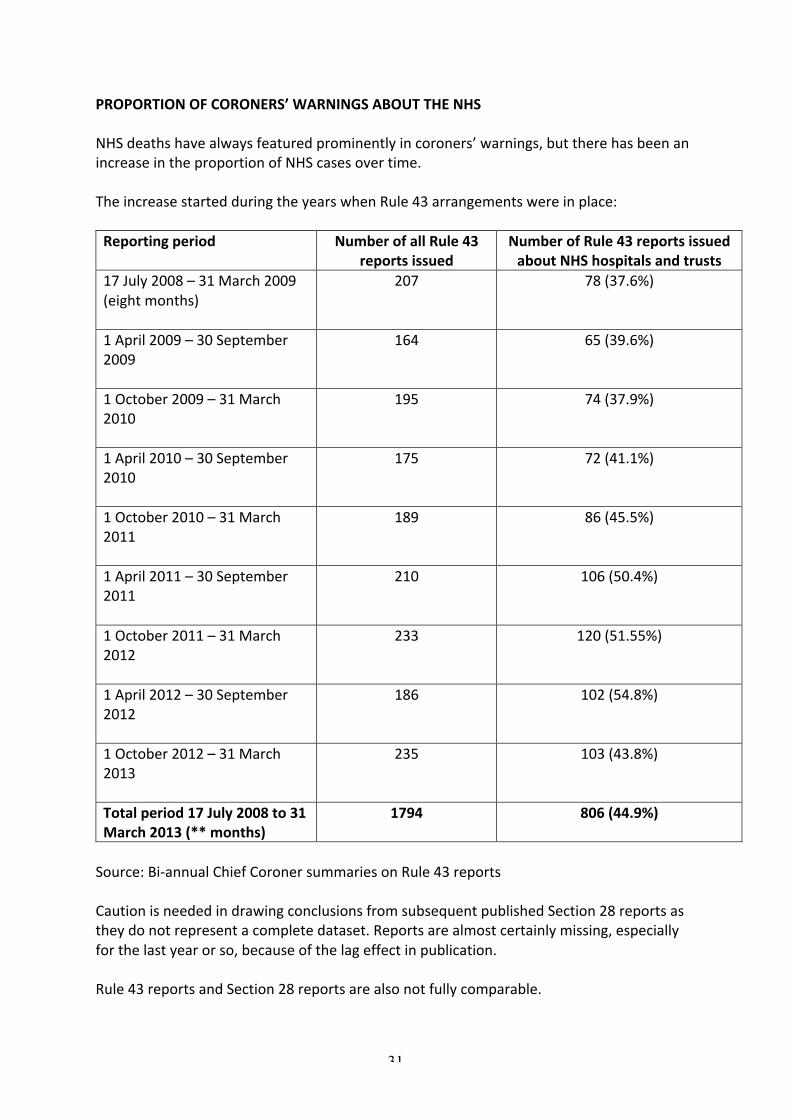
PROPORTIONOFCORONERS’WARNINGSABOUTTHENHSNHSdeathshavealwaysfeaturedprominentlyincoroners’warnings,buttherehasbeenanincreaseintheproportionofNHScasesovertime.TheincreasestartedduringtheyearswhenRule43arrangementswereinplace:Reportingperiod NumberofallRule43
reportsissuedNumberofRule43reportsissuedaboutNHShospitalsandtrusts
17July2008–31March2009(eightmonths)
207 78(37.6%)
1April2009–30September2009
164 65(39.6%)
1October2009–31March2010
195 74(37.9%)
1April2010–30September2010
175 72(41.1%)
1October2010–31March2011
189 86(45.5%)
1April2011–30September2011
210 106(50.4%)
1October2011–31March2012
233 120(51.55%)
1April2012–30September2012
186 102(54.8%)
1October2012–31March2013
235 103(43.8%)
Totalperiod17July2008to31March2013(**months)
1794 806(44.9%)
Source:Bi-annualChiefCoronersummariesonRule43reportsCautionisneededindrawingconclusionsfromsubsequentpublishedSection28reportsastheydonotrepresentacompletedataset.Reportsarealmostcertainlymissing,especiallyforthelastyearorso,becauseofthelageffectinpublication.Rule43reportsandSection28reportsarealsonotfullycomparable.

32
Butforcompleteness,thishasbeenthedistributionovertimeofpublishedcoroners’Section28reportsontheNHS(includingprimarycare).Period NumberofallSection28reports
publishedNumberofSection28reports
publishedaboutallNHSservicesincludingprimarycare
20July2013–31March2014
309 167(54%ofallreports)
2014/15
528 309(58.5%ofallreports)
2015/16
400 229(57.2%ofallreports)
2016/17
439 245(55.8%ofallreports)
2017/18yearto31July2017
49 37(75.5%ofallreports)
Totalperiod(20July2013to31July2017)
1725 987(57.2%ofallreports)
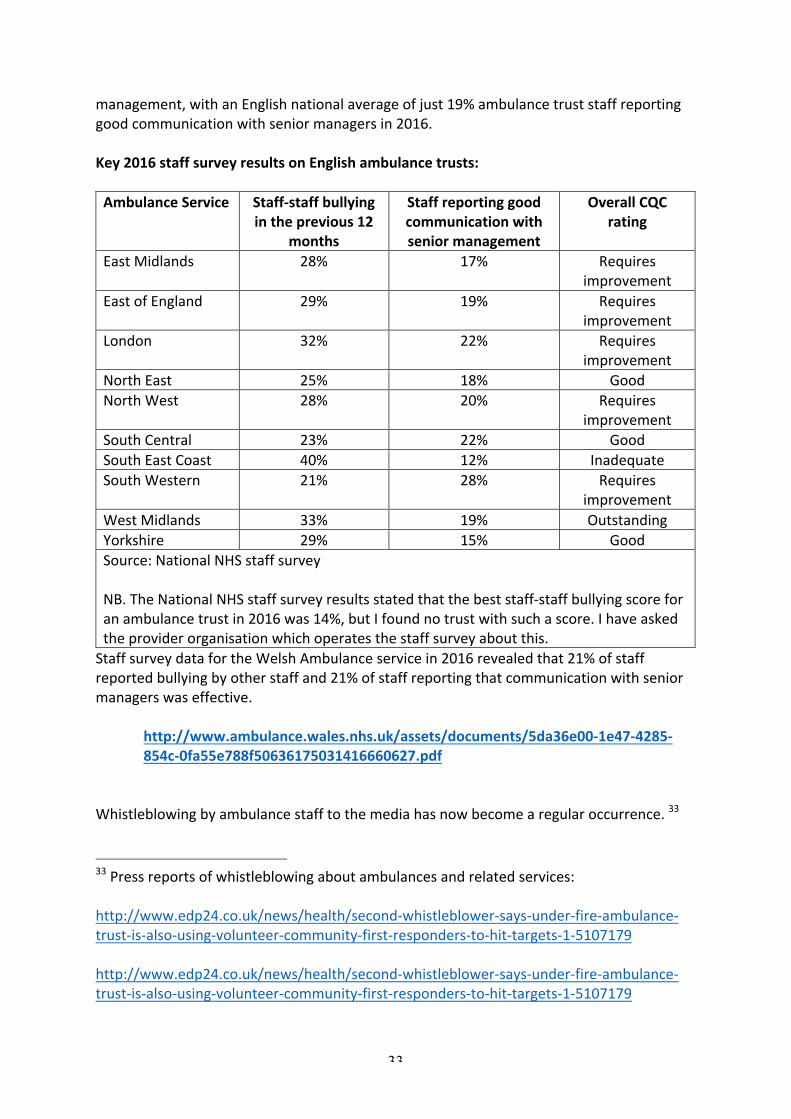
CORONERS’WARNINGSABOUTAMBULANCESERVICESANDRELATEDMATTERSTheeffectivenessofambulanceservicesmatterstoall.Ambulanceperformanceisamatterofpoliticalsensitivityasarethecontroversialschemesfordivertingpatientstolessacuteformsofcare,whichsomehavecriticisedasameansofsavingmoneyanddowngradingservices.32Thereare10EnglishNHSambulancetrustsandoneWelshambulancetrust.Theyoperateundergreatpressure.EnglishnationalNHSstaffsurveyreturnsforambulancetrustsshowthehighestlevelsofbullyingoutofalltypesofNHStrusts(averageof28%in2016).Ambulancetrustsalsoreturnverylowscoresoncommunicationbetweenstaffandsenior
32NHStorevamp111helplineaftersustainedcriticismofservice,DenisCampbellGuardian8March2017https://www.theguardian.com/society/2017/mar/08/nhs-to-revamp-111-helpline-after-sustained-criticism-of-serviceNationalreviewofschemestodivertpatientsfromA&Eamidsafetyfears,LauraDonnellyTelegraph23July2017http://www.telegraph.co.uk/news/2017/07/23/exclusive-national-review-schemes-divert-patients-ae-amid-safety/
33
management,withanEnglishnationalaverageofjust19%ambulancetruststaffreportinggoodcommunicationwithseniormanagersin2016.Key2016staffsurveyresultsonEnglishambulancetrusts:AmbulanceService Staff-staffbullying
intheprevious12months
Staffreportinggoodcommunicationwithseniormanagement
OverallCQCrating
EastMidlands 28% 17% Requiresimprovement
EastofEngland 29% 19% Requiresimprovement
London 32% 22% Requiresimprovement
NorthEast 25% 18% GoodNorthWest 28% 20% Requires
improvementSouthCentral 23% 22% GoodSouthEastCoast 40% 12% InadequateSouthWestern 21% 28% Requires
improvementWestMidlands 33% 19% OutstandingYorkshire 29% 15% GoodSource:NationalNHSstaffsurveyNB.TheNationalNHSstaffsurveyresultsstatedthatthebeststaff-staffbullyingscoreforanambulancetrustin2016was14%,butIfoundnotrustwithsuchascore.Ihaveaskedtheproviderorganisationwhichoperatesthestaffsurveyaboutthis.StaffsurveydatafortheWelshAmbulanceservicein2016revealedthat21%ofstaffreportedbullyingbyotherstaffand21%ofstaffreportingthatcommunicationwithseniormanagerswaseffective.
http://www.ambulance.wales.nhs.uk/assets/documents/5da36e00-1e47-4285-854c-0fa55e788f50636175031416660627.pdf
Whistleblowingbyambulancestafftothemediahasnowbecomearegularoccurrence.33
33Pressreportsofwhistleblowingaboutambulancesandrelatedservices:http://www.edp24.co.uk/news/health/second-whistleblower-says-under-fire-ambulance-trust-is-also-using-volunteer-community-first-responders-to-hit-targets-1-5107179http://www.edp24.co.uk/news/health/second-whistleblower-says-under-fire-ambulance-trust-is-also-using-volunteer-community-first-responders-to-hit-targets-1-5107179

34
Curiouslythough,therearenopublishedCQC‘intelligentmonitoring’reportsatallonambulancetrusts.ItwasthereforenotpossibletochecktheextenttowhichCQChasreceivedwhistleblowingalertsaboutambulanceservices.33
https://www.hsj.co.uk/east-of-england-ambulance-service-nhs-trust/exclusive-whistleblower-warns-trust-is-worst-its-ever-been-as-staff-shortage-revealed/7020389.article#.WZgIBxoBC3Q.twitterhttp://www.telegraph.co.uk/news/2017/02/13/bullying-desperate-999-call-handlers-led-suicide-attempts-scandal/http://www.bristolpost.co.uk/news/bristol-news/whistleblower-nhs-bristol-ambulance-paramedics-163044http://www.bbc.co.uk/news/uk-england-38694213http://www.yorkpress.co.uk/newS/11682028.Row_after_launch_of_ambulance_service_whistleblower_website/?commentSort=scorehttp://www.mirror.co.uk/news/uk-news/ambulance-service-crisis-warns-paramedic-6961702http://www.plymouthherald.co.uk/probe-launched-whistleblower-s-claims-health/story-29308468-detail/story.htmlhttp://www.bbc.co.uk/news/health-38535946https://www.hsj.co.uk/hsj-local/providers/south-western-ambulance-service-nhs-foundation-trust/exclusive-regulator-to-probe-whistleblower-ambulance-trust/7004930.articlehttp://archive.camdennewjournal.com/news/2011/oct/whistleblower-says-ae-ambulance-crews-go-out-without-paramedicshttps://planetradio.co.uk/mfr/local/news/watch-safety-watchdog-looking-north-ambulances/https://www.spectator.co.uk/2014/08/londons-999-emergency/33CQC‘intelligentmonitoring’reportsareoflimiteduseinprovidinginformationonwhistleblowingeventsastheyonlysaywhethertherehavebeenalertsreceivedduringagivenreportingperiod,withoutindicatinghowmanyreportshavebeenreceived.
35
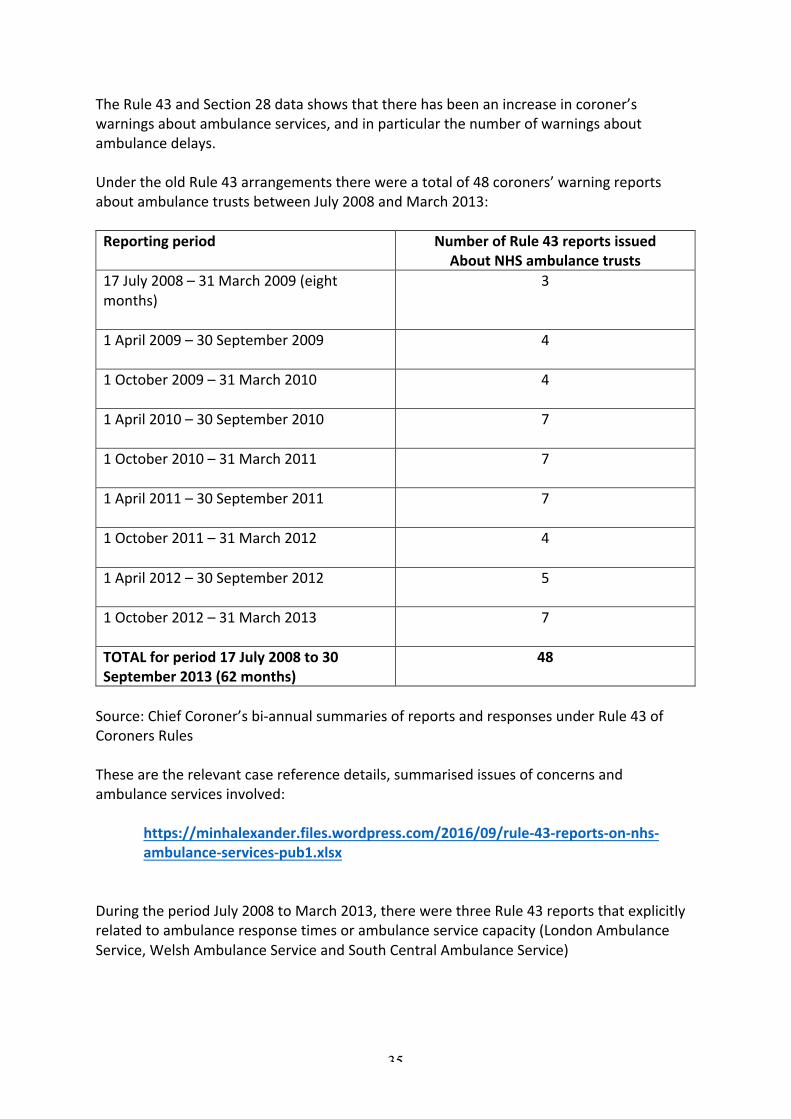
TheRule43andSection28datashowsthattherehasbeenanincreaseincoroner’swarningsaboutambulanceservices,andinparticularthenumberofwarningsaboutambulancedelays.UndertheoldRule43arrangementstherewereatotalof48coroners’warningreportsaboutambulancetrustsbetweenJuly2008andMarch2013:Reportingperiod NumberofRule43reportsissued
AboutNHSambulancetrusts17July2008–31March2009(eightmonths)
3
1April2009–30September2009
4
1October2009–31March2010
4
1April2010–30September2010
7
1October2010–31March2011
7
1April2011–30September2011
7
1October2011–31March2012
4
1April2012–30September2012
5
1October2012–31March2013
7
TOTALforperiod17July2008to30September2013(62months)
48
Source:ChiefCoroner’sbi-annualsummariesofreportsandresponsesunderRule43ofCoronersRulesThesearetherelevantcasereferencedetails,summarisedissuesofconcernsandambulanceservicesinvolved:
https://minhalexander.files.wordpress.com/2016/09/rule-43-reports-on-nhs-ambulance-services-pub1.xlsx
DuringtheperiodJuly2008toMarch2013,therewerethreeRule43reportsthatexplicitlyrelatedtoambulanceresponsetimesorambulanceservicecapacity(LondonAmbulanceService,WelshAmbulanceServiceandSouthCentralAmbulanceService)
36
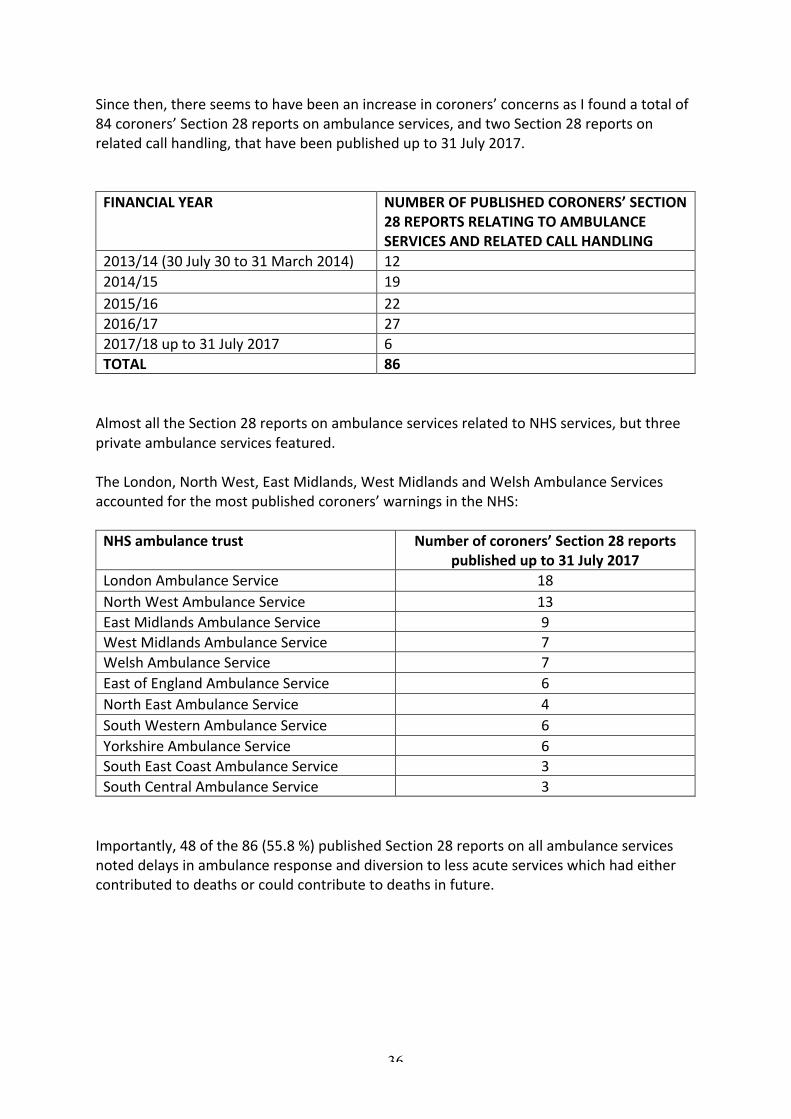
Sincethen,thereseemstohavebeenanincreaseincoroners’concernsasIfoundatotalof84coroners’Section28reportsonambulanceservices,andtwoSection28reportsonrelatedcallhandling,thathavebeenpublishedupto31July2017.FINANCIALYEAR NUMBEROFPUBLISHEDCORONERS’SECTION
28REPORTSRELATINGTOAMBULANCESERVICESANDRELATEDCALLHANDLING
2013/14(30July30to31March2014) 122014/15 192015/16 222016/17 272017/18upto31July2017 6TOTAL 86AlmostalltheSection28reportsonambulanceservicesrelatedtoNHSservices,butthreeprivateambulanceservicesfeatured.TheLondon,NorthWest,EastMidlands,WestMidlandsandWelshAmbulanceServicesaccountedforthemostpublishedcoroners’warningsintheNHS:NHSambulancetrust Numberofcoroners’Section28reports
publishedupto31July2017LondonAmbulanceService 18NorthWestAmbulanceService 13EastMidlandsAmbulanceService 9WestMidlandsAmbulanceService 7WelshAmbulanceService 7EastofEnglandAmbulanceService 6NorthEastAmbulanceService 4SouthWesternAmbulanceService 6YorkshireAmbulanceService 6SouthEastCoastAmbulanceService 3SouthCentralAmbulanceService 3Importantly,48ofthe86(55.8%)publishedSection28reportsonallambulanceservicesnoteddelaysinambulanceresponseanddiversiontolessacuteserviceswhichhadeithercontributedtodeathsorcouldcontributetodeathsinfuture.
37
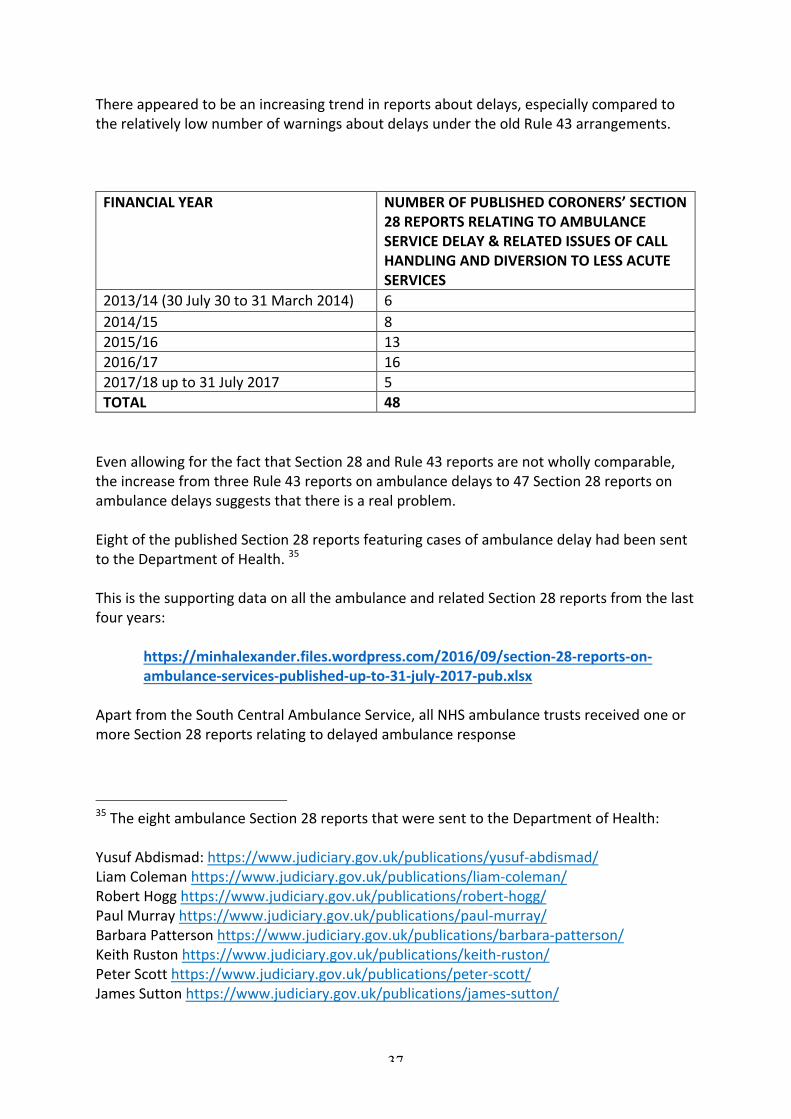
Thereappearedtobeanincreasingtrendinreportsaboutdelays,especiallycomparedtotherelativelylownumberofwarningsaboutdelaysundertheoldRule43arrangements.FINANCIALYEAR NUMBEROFPUBLISHEDCORONERS’SECTION
28REPORTSRELATINGTOAMBULANCESERVICEDELAY&RELATEDISSUESOFCALLHANDLINGANDDIVERSIONTOLESSACUTESERVICES
2013/14(30July30to31March2014) 62014/15 82015/16 132016/17 162017/18upto31July2017 5TOTAL 48EvenallowingforthefactthatSection28andRule43reportsarenotwhollycomparable,theincreasefromthreeRule43reportsonambulancedelaysto47Section28reportsonambulancedelayssuggeststhatthereisarealproblem.EightofthepublishedSection28reportsfeaturingcasesofambulancedelayhadbeensenttotheDepartmentofHealth.35ThisisthesupportingdataonalltheambulanceandrelatedSection28reportsfromthelastfouryears:
https://minhalexander.files.wordpress.com/2016/09/section-28-reports-on-ambulance-services-published-up-to-31-july-2017-pub.xlsx
ApartfromtheSouthCentralAmbulanceService,allNHSambulancetrustsreceivedoneormoreSection28reportsrelatingtodelayedambulanceresponse
35TheeightambulanceSection28reportsthatweresenttotheDepartmentofHealth:YusufAbdismad:https://www.judiciary.gov.uk/publications/yusuf-abdismad/LiamColemanhttps://www.judiciary.gov.uk/publications/liam-coleman/RobertHogghttps://www.judiciary.gov.uk/publications/robert-hogg/PaulMurrayhttps://www.judiciary.gov.uk/publications/paul-murray/BarbaraPattersonhttps://www.judiciary.gov.uk/publications/barbara-patterson/KeithRustonhttps://www.judiciary.gov.uk/publications/keith-ruston/PeterScotthttps://www.judiciary.gov.uk/publications/peter-scott/JamesSuttonhttps://www.judiciary.gov.uk/publications/james-sutton/

38
Moreover,someofthecoroners’remarksindicatedthattherehadbeenpreviousincidentsofdelayandrelatedsystemicissues.Coronerspointedoutthatambulancedelayswereduetocapacityandcloselyrelatedtootherseverepressuresinthesystem,whichcausedelaysinhospitalhandoverandambulancequeuingatA&Edepartments.CompoundingproblemsofservicecapacityandhandoverdelaysatA&E,therewerealsoissuesabouttheeffectivenessandsafetyofcallhandlinganddiversionservices.Insomedeaths,referralstoambulanceserviceshadbeenassignedlowerprioritythanwasappropriate.Aquestionarisesofwhetherthisispartlyaconsequenceofasystemthatissooverwhelmedthatitisunderstandablyandforeseeablybecomingde-sensitisedtorisk.Someexamplesfollow.
Afteradeathinwhichittookoneandhalfhoursforanambulancetoattend,thecoronerforExeterandGreaterDevonnotedon21June2017:
https://www.judiciary.gov.uk/publications/colin-james/TheBrighton&Hovecoronernotedon5April2017:
39
https://www.judiciary.gov.uk/publications/ronald-bennett/
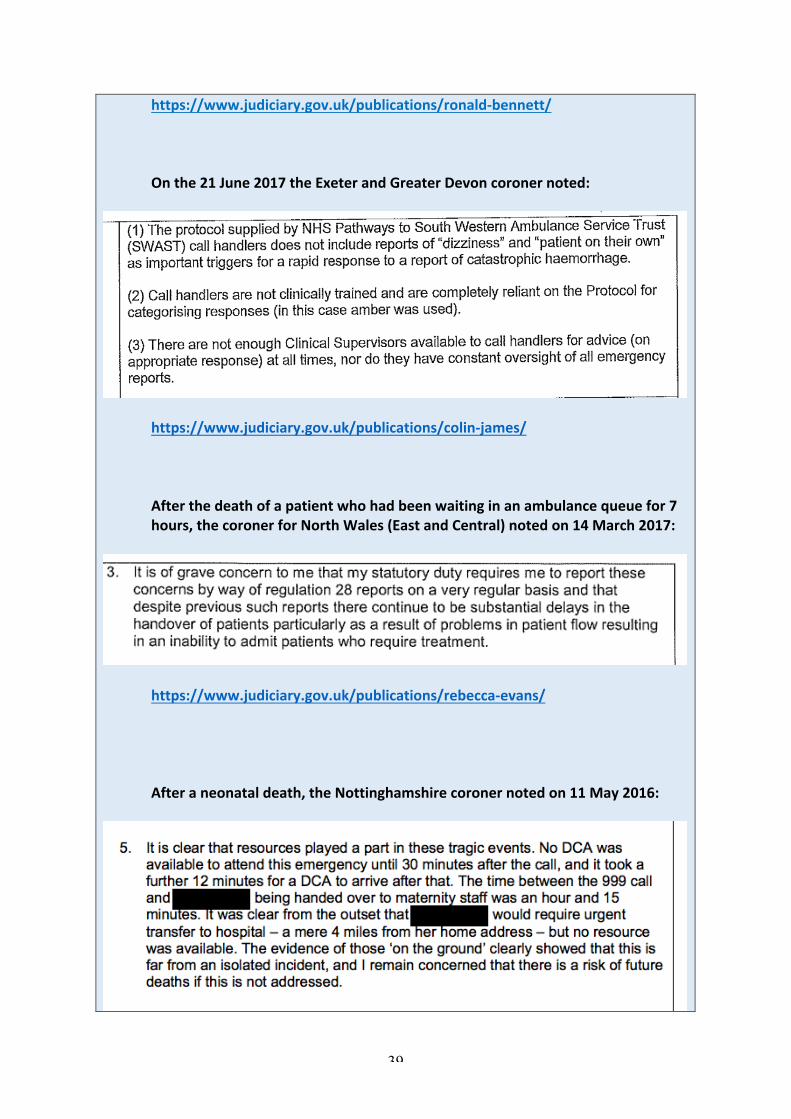
Onthe21June2017theExeterandGreaterDevoncoronernoted:
https://www.judiciary.gov.uk/publications/colin-james/Afterthedeathofapatientwhohadbeenwaitinginanambulancequeuefor7hours,thecoronerforNorthWales(EastandCentral)notedon14March2017:
https://www.judiciary.gov.uk/publications/rebecca-evans/Afteraneonataldeath,theNottinghamshirecoronernotedon11May2016:
40
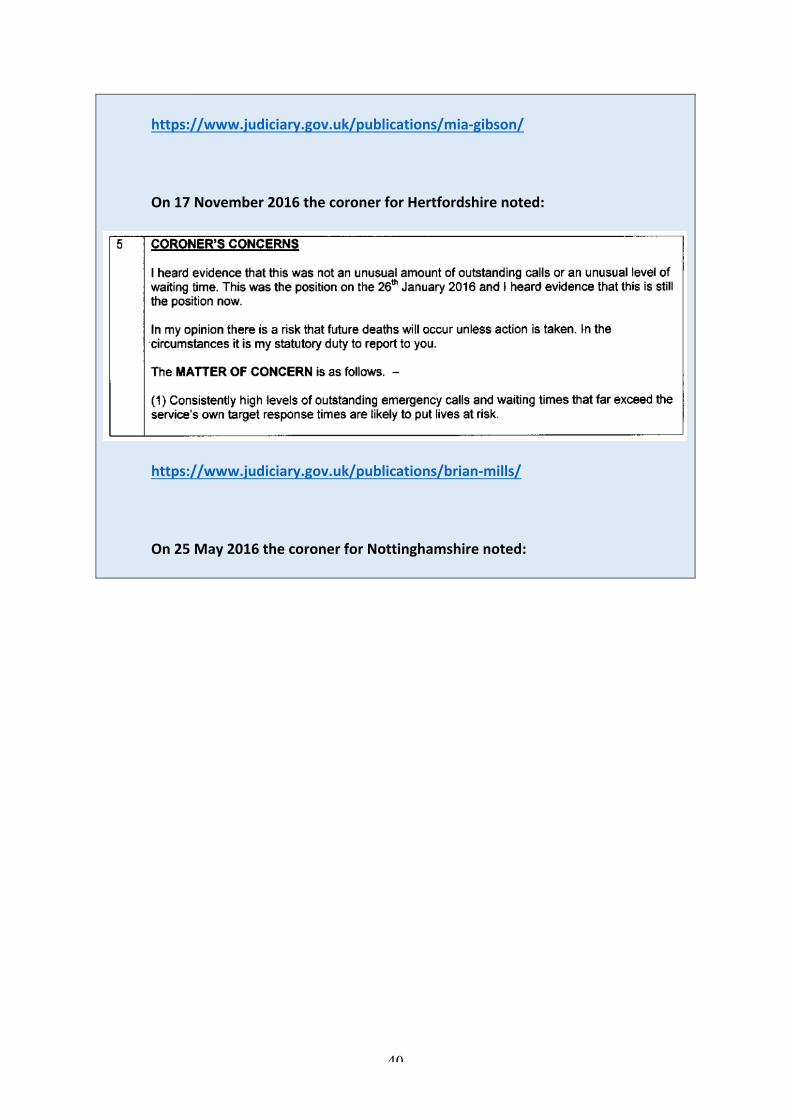
https://www.judiciary.gov.uk/publications/mia-gibson/
On17November2016thecoronerforHertfordshirenoted:
https://www.judiciary.gov.uk/publications/brian-mills/
On25May2016thecoronerforNottinghamshirenoted:
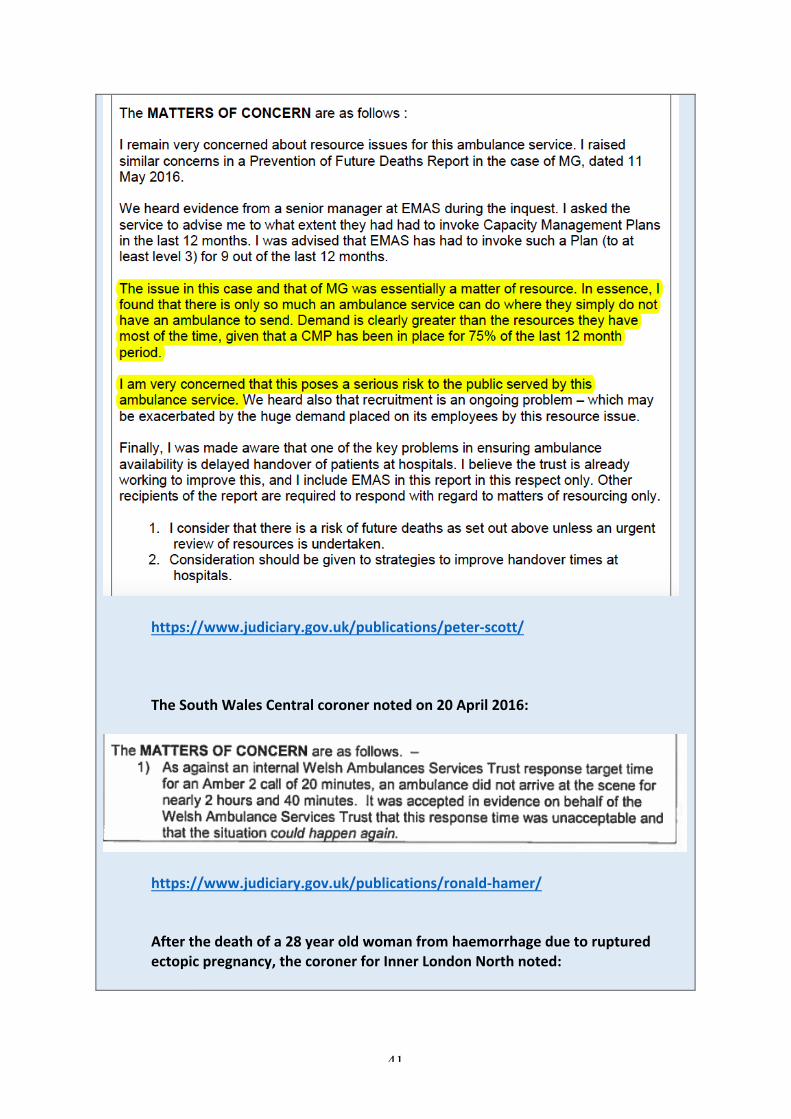
41
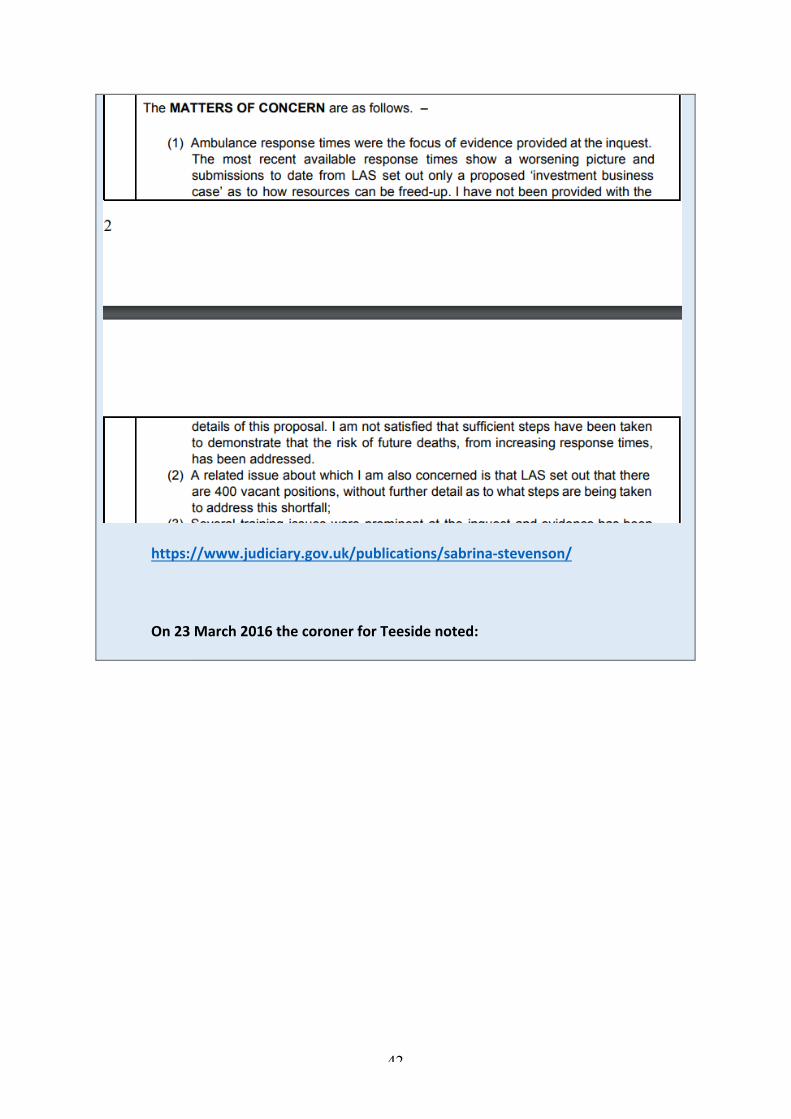
https://www.judiciary.gov.uk/publications/peter-scott/TheSouthWalesCentralcoronernotedon20April2016:
https://www.judiciary.gov.uk/publications/ronald-hamer/Afterthedeathofa28yearoldwomanfromhaemorrhageduetorupturedectopicpregnancy,thecoronerforInnerLondonNorthnoted:
42
https://www.judiciary.gov.uk/publications/sabrina-stevenson/On23March2016thecoronerforTeesidenoted:
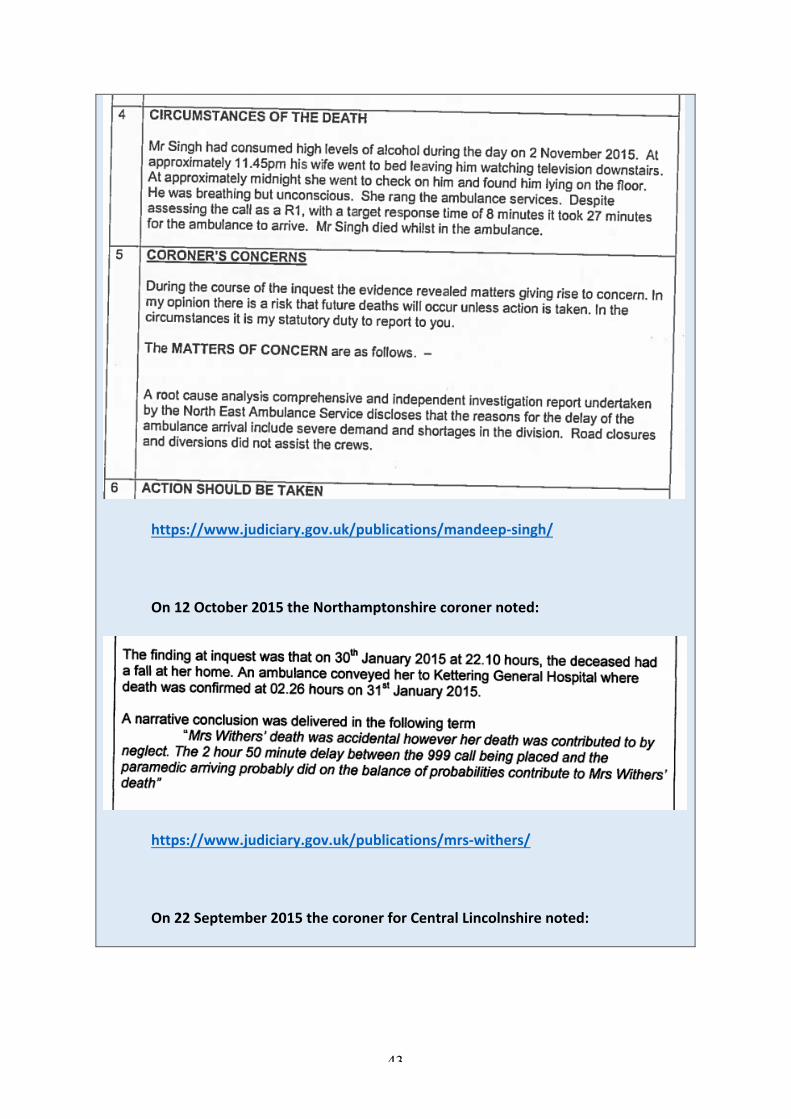
43
https://www.judiciary.gov.uk/publications/mandeep-singh/On12October2015theNorthamptonshirecoronernoted:
https://www.judiciary.gov.uk/publications/mrs-withers/On22September2015thecoronerforCentralLincolnshirenoted:

44
https://www.judiciary.gov.uk/publications/stuart-knight/On21May2015thecoronerforNorthNorthumberlandnoted:
https://www.judiciary.gov.uk/publications/barbara-patterson/
On13May2015theNorthLondoncoronernoted:
45
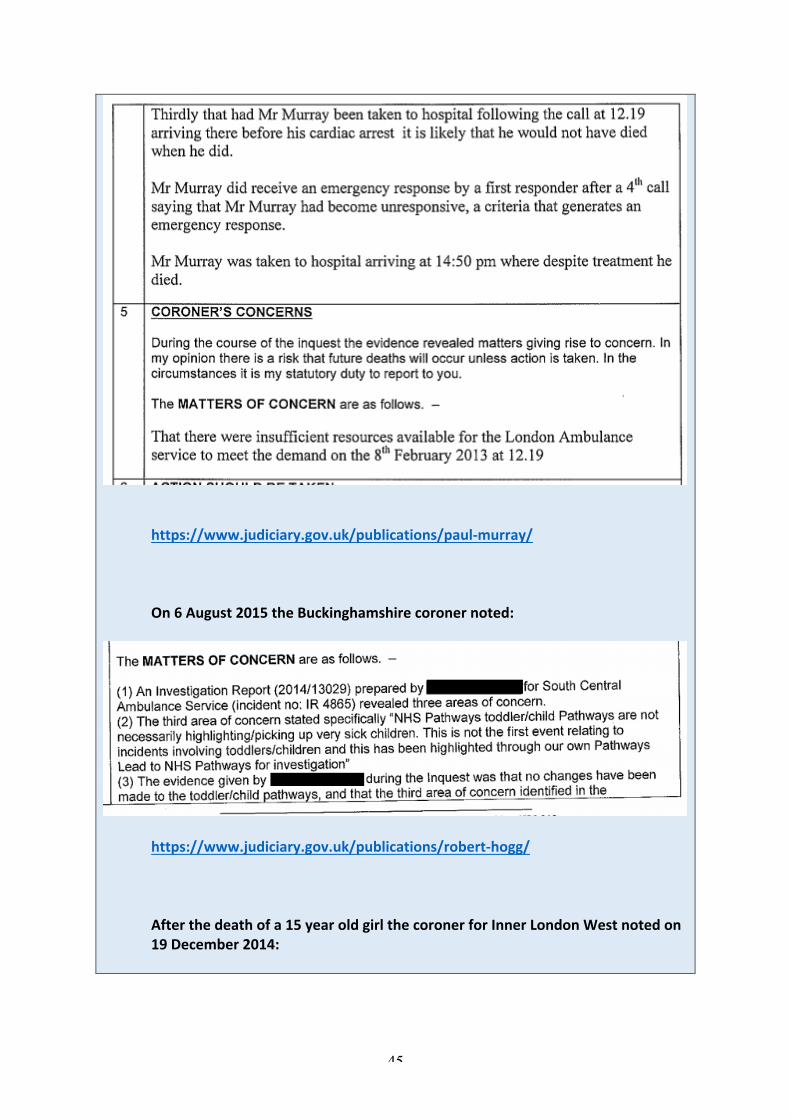
https://www.judiciary.gov.uk/publications/paul-murray/
On6August2015theBuckinghamshirecoronernoted:
https://www.judiciary.gov.uk/publications/robert-hogg/
Afterthedeathofa15yearoldgirlthecoronerforInnerLondonWestnotedon19December2014:
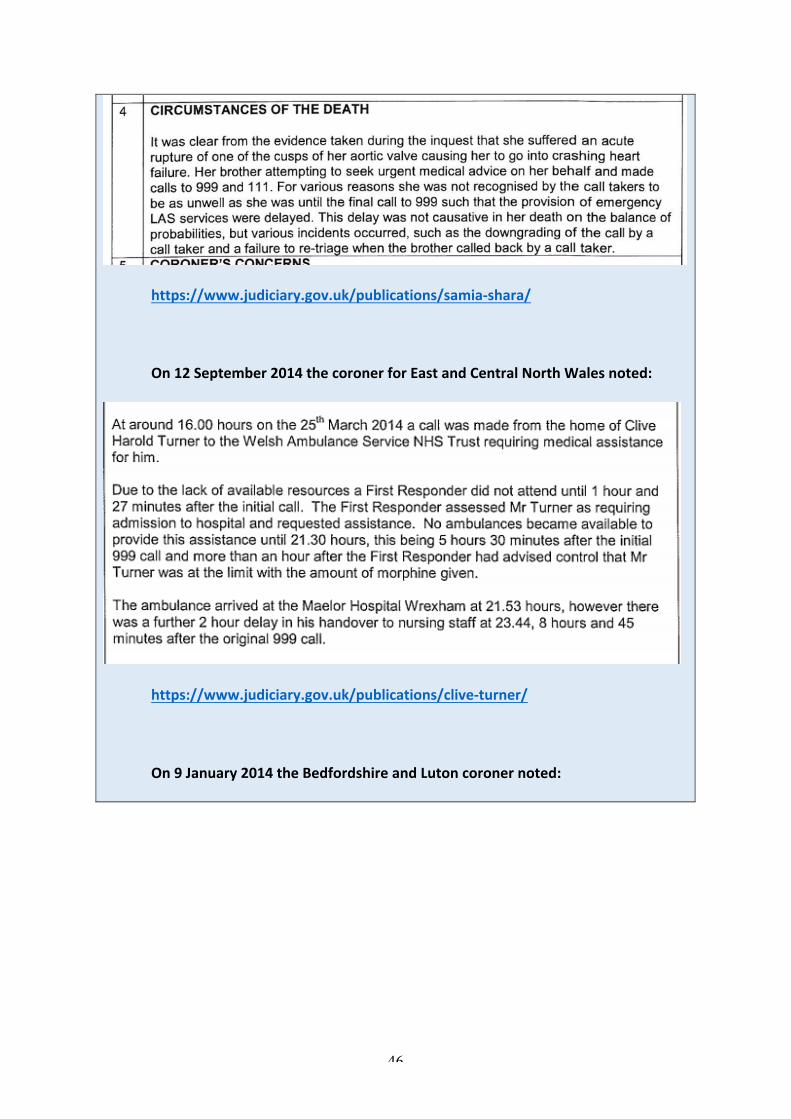
46
https://www.judiciary.gov.uk/publications/samia-shara/
On12September2014thecoronerforEastandCentralNorthWalesnoted:
https://www.judiciary.gov.uk/publications/clive-turner/On9January2014theBedfordshireandLutoncoronernoted:
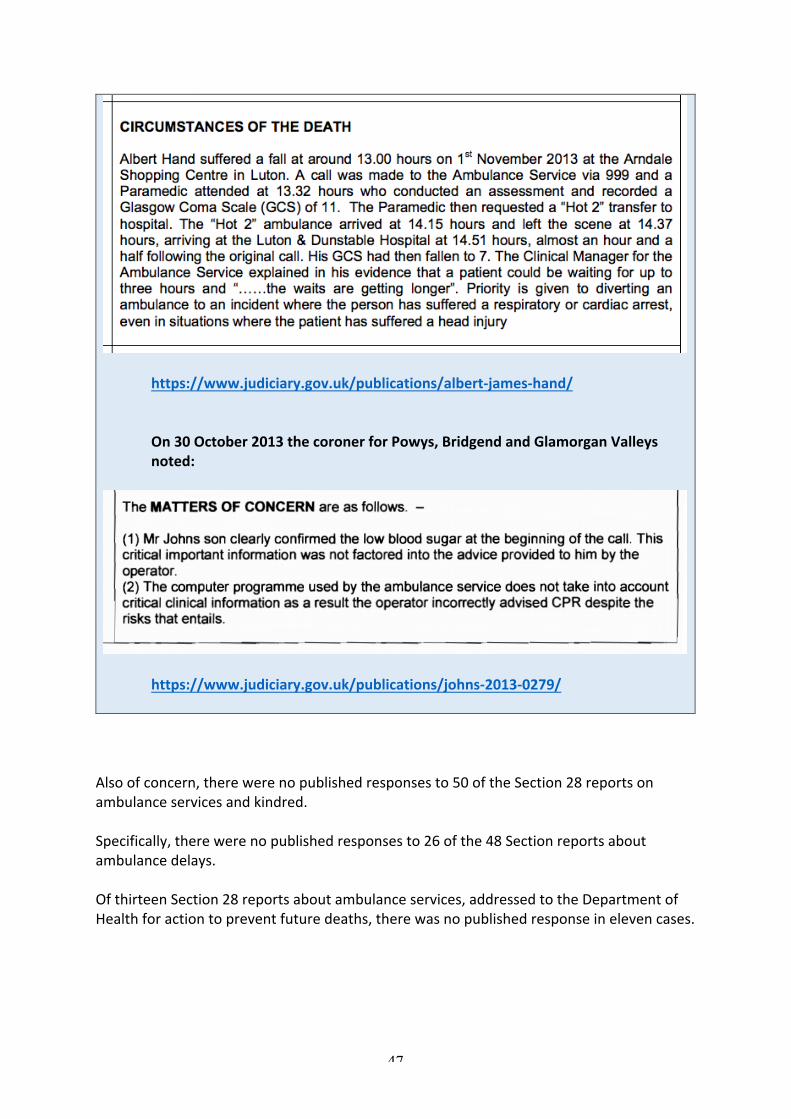
47
https://www.judiciary.gov.uk/publications/albert-james-hand/On30October2013thecoronerforPowys,BridgendandGlamorganValleysnoted:
https://www.judiciary.gov.uk/publications/johns-2013-0279/Alsoofconcern,therewerenopublishedresponsesto50oftheSection28reportsonambulanceservicesandkindred.Specifically,therewerenopublishedresponsesto26ofthe48Sectionreportsaboutambulancedelays.OfthirteenSection28reportsaboutambulanceservices,addressedtotheDepartmentofHealthforactiontopreventfuturedeaths,therewasnopublishedresponseinelevencases.
48
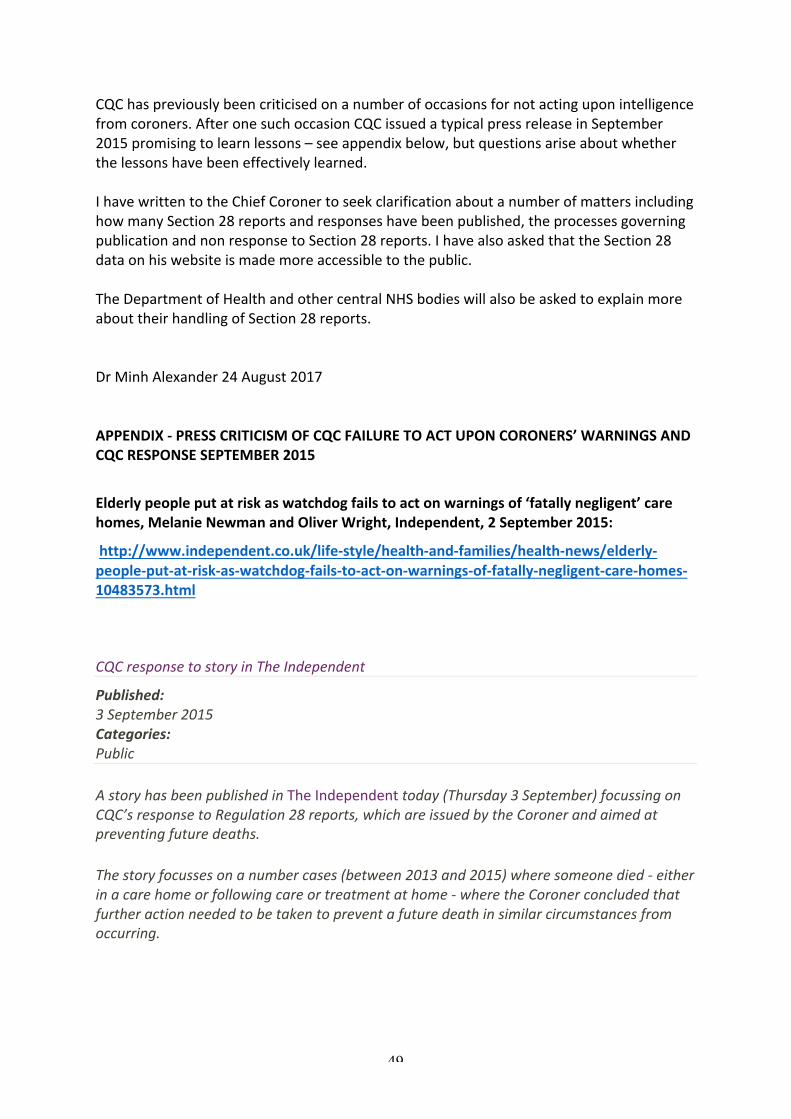
Ofthepublishedresponsesbythegovernmentandcentralbodiesaboutambulancedeaths,therewererepeatedpromisestoreviewandmentionsofworkinprogress,includinganNHSEnglandreviewledbyBruceKeoghNHSEnglandMedicalDirector.However,thecontinuingstreamofcoroner’swarningssuggeststhatseriousrisktothepublicisnotbeingamelioratedquicklyenough.CONCLUSIONThepublishedSection28reportdataforEnglandandWales,itscompletenessandpresentationraiseissuesofgovernmenttransparency,learningfromdeathsandwhetherthegovernmentisdoingenoughtoprotectthepublic.TheincompletedataonresponsestoCoroners’warningsandtheapparentlackofaclearprocessfordealingwithunsatisfactoryresponsesraisequestionsaboutthepurposeandeffectivenessoftheSection28reportingsystem.Theauditcycleneedstobemoreclearlyandproactivelyclosed,withproperaccountabilitytothepublic.Failuretotakeactioninresponsetoavoidabledeathsorunacceptableriskstothepublicshouldnotbeexposedbythenextsimilardeath,asseemstobeimpliedbysomeoftheSection28reports,butbyactivetrackingbytheState.Thehundredsofcoroners’warningsabouttheNHSandnotwithstandingthecaveatsaboutthedata,anapparentescalationinwarningsaboutNHSemergencyservicesemphasisetheneedtoforthegovernmenttodemonstratethatitistakingeffectiveaction.Thedataonrepeatedcoroners’warningsaboutambulancedeathsandseriousrisktopublicsafetycallsintoquestionthevalidityofCQC’sregulatoryperformanceandfindings.Inparticular,CQC’srecentratingofWestMidlandsAmbulanceServiceas‘Outstanding’36ishardtoreconcilewiththerealityontheground.
36http://www.cqc.org.uk/provider/RYA
49
CQChaspreviouslybeencriticisedonanumberofoccasionsfornotactinguponintelligencefromcoroners.AfteronesuchoccasionCQCissuedatypicalpressreleaseinSeptember2015promisingtolearnlessons–seeappendixbelow,butquestionsariseaboutwhetherthelessonshavebeeneffectivelylearned.IhavewrittentotheChiefCoronertoseekclarificationaboutanumberofmattersincludinghowmanySection28reportsandresponseshavebeenpublished,theprocessesgoverningpublicationandnonresponsetoSection28reports.IhavealsoaskedthattheSection28dataonhiswebsiteismademoreaccessibletothepublic.TheDepartmentofHealthandothercentralNHSbodieswillalsobeaskedtoexplainmoreabouttheirhandlingofSection28reports.DrMinhAlexander24August2017APPENDIX-PRESSCRITICISMOFCQCFAILURETOACTUPONCORONERS’WARNINGSANDCQCRESPONSESEPTEMBER2015
Elderlypeopleputatriskaswatchdogfailstoactonwarningsof‘fatallynegligent’carehomes,MelanieNewmanandOliverWright,Independent,2September2015:
http://www.independent.co.uk/life-style/health-and-families/health-news/elderly-people-put-at-risk-as-watchdog-fails-to-act-on-warnings-of-fatally-negligent-care-homes-10483573.html
CQCresponsetostoryinTheIndependent
Published:3September2015Categories:Public
AstoryhasbeenpublishedinTheIndependenttoday(Thursday3September)focussingonCQC’sresponsetoRegulation28reports,whichareissuedbytheCoronerandaimedatpreventingfuturedeaths.
Thestoryfocussesonanumbercases(between2013and2015)wheresomeonedied-eitherinacarehomeorfollowingcareortreatmentathome-wheretheCoronerconcludedthatfurtheractionneededtobetakentopreventafuturedeathinsimilarcircumstancesfromoccurring.

50
OurChiefExecutive,DavidBehan,gaveaninterviewtoTheIndependenttoexplainhowCQChasimprovedtheprocesseswehavetoinplacetoensurethatwerespondtoandlearnfromtheissueshighlightedbytheseRegulation28reports.
CQC’sChiefExecutive,DavidBehan,said:.
“WhensomeonedieswhilebeingcaredforinahealthorsocialcaresettingandtheCoronerconcludesthatactionisneededtopreventfuturedeathsfromoccurring,aRegulation28reportisissued.Inmostcases,theproviderwillbethenamedrespondent,meaningthattheyhaveresponsibilityforpreventingafuturedeathinsimilarcircumstances.
“Insomecases,however,CQCisthenamedrespondent,meaningthattheCoronerhasconcludedthattheregulatoralsohasaroletoplayinensuringthatpeopleareprotectedinthefuture.
“InthosecaseswhereCQCisidentifiedasthenamedrespondent,itisabsolutelyrightthatweshouldexpectCQCtousethisinformationtoinformourregulatoryactivities.ThisincludeshowwerespondtolevelsofriskaswellasensuringprovidersactontherecommendationsofCoroner’sReports.
“Lastyear,Iinitiatedareviewofourprocessesandprocedures,asIhadrecognisedthatwewerenotalwaysreceivingtheseReports.Insomecaseswherewedid,itwasalsoclearwewerenotalwaysdealingwiththeseeffectivelyenough.
“Wehavemadeanumberofchangestostrengthenandtightenourwaysofworking,including:
• EstablishingasinglepointofcontactforCoroners’reportstoensureanyconcernsraisedareeffectivelylogged,analysed,managedandreviewed.
• BetterandearlierengagementwithCoronersaroundthetimeofaperson’sdeath.• AproposedanddraftedMemorandumofUnderstandingwiththeCoroners’Society
tostrengthenourworkingrelationshipsandensurewereceiveallCoroners’reportsinhealthandsocialcareinquestsinordertohelpreduceriskmoreeffectivelyandpromptly.
“We’vemadeprogress,butI’mfarfrombeingcomplacent.Weknowthereismoreworktodo.Improvementisacontinualcommitmentandwearemakingsureweareproperlyembeddingournewprocess,furtherdevelopingourrelationshipwiththeCoroners’Societyandbeingreallyclearaboutwhatweexpectourstafftodowhentheyreceivethesetypesofreports.
“Butthisisn’tjustaboutprocesses–it’saboutpeople’slives.Forthatreason,weneedtokeepworkinghardtoensurethatwegetitrighteverytime.”
Lastupdated:

51
29May2017
https://www.cqc.org.uk/news/stories/cqc-response-story-independent
Recommended

















