-
8/17/2019 Fisio Digestion
1/121
-
8/17/2019 Fisio Digestion
2/121
Food
NutrientNutrient
Non NutrientNon Nutrient
AssimilatedAssimilated
EliminatedEliminated
DigestiveDigestive
systemsystem
Primary Functions of Digestive SystemPrimary Functions of
Digestive SystemActivity necessary:Activity necessary:
MotilityMotility SecretioSecretio
nnDigestioDigestio
nnAbsorptioAbsorptio
nn
-
8/17/2019 Fisio Digestion
3/121
Movement of food through tract ,includesingestion, mastication
(cheing food andmi!ing ith saliva", deglutition(salloing" and
#eristalsis (rh$thmiccontractions along %& tract that
#ro#elfood" muscular contraction.muscular contraction.
Primary Functions of Digestive SystemPrimary Functions of
Digestive SystemActivity necessary:Activity necessary:
MotilityMotility
SecretioSecretio
nn'ndocrine (secretion of hormones thatregulate digestive
#rocess"'!ocrine (secretion of ater, enz$mes,acid, bicarbonate,
into %& tract enz$me enz$me
other digestive juices.other digestive juices.
-
8/17/2019 Fisio Digestion
4/121
H$drol$sis reactions that brea) ingested #ol$mers(large
molecules" into their smaller subunits(monomers" brea)don of
substances.brea)don of substances.
! #roteins into amino acids! fats into gl$cerol and free
fatt$ acids
! com#le! sugars into monosaccharides
DigestioDigestionn
"ransfer of monomer subunits across #allof small intestine
into blood or lymph transport modi$ed nutrients%transport
modi$ed nutrients%
AbsorptioAbsorptio
nn
-
8/17/2019 Fisio Digestion
5/121
&egulation&egulation''
"here are t#o (nerve nets) *ple+uses,in -. tract that
contain neurons andinterneurons
! sub mucosal *Meissner,! Myenteric *Auerbach,
Ple+uses / brain of the gut
! stimulated by stretch *bolus of food,0chemicals0 and stomach
content *localstimuli,
Activity of ple+uses can be modi$ed
Neural:Neural:
-
8/17/2019 Fisio Digestion
6/121
Neural regulation via autonomic nervousNeural regulation via
autonomic nervoussystemsystem! -. tract receives both-. tract
receives both
s$m#athetics$m#athetic andand #aras$m#athetic #aras$m#athetic innervationsinnervations
Parasympathetic via vagus nerve andParasympathetic via vagus
nerve andspinal nerves in sacral region *to lo#erspinal nerves in
sacral region *to lo#erportion of large intestine,portion of large
intestine,→ stimulates motility and secretion'
favorsstimulates motility and secretion' favors
digestiondigestion SympatheticSympathetic
→ reduces motility and secretory activity andreduces
motility and secretory activity andstimulates sphincter
contractionstimulates sphincter contraction
-
8/17/2019 Fisio Digestion
7/121
Paracrine regulationParacrine regulation! production of
hormone1li2e molecules thatproduction of hormone1li2e molecules
that
are produced in one cell and travelare produced in one cell and
travel
through interstitial 3uid *not bloodstream,through interstitial
3uid *not bloodstream,
to a4ect activity of nearby cellsto a4ect activity of nearby
cells
5ormone regulation5ormone regulation! production of hormones
that are releasedproduction of hormones that are released
into the bloodstream and carried to targetinto the bloodstream
and carried to target
tissues #ithin digestive system #heretissues #ithin digestive
system #herethey a4ect digestive activitythey a4ect digestive
activity
5ormonal5ormonal%%
-
8/17/2019 Fisio Digestion
8/121
-
8/17/2019 Fisio Digestion
9/121
Mout Mout
h*h*
-
8/17/2019 Fisio Digestion
10/121
Teeth! grind and tear food into smaller pieces
! increases surface area upon which digestiveenzymes work
parotid gland parotid duct
sublingual gland submandibular gland
Mouth*Mouth*
Salivary glands
*parotid0 subma+illary0sublingual,secrete saliva
lubricates and softens
food' aids in s#allo#ingcontains amylase /en6yme that
beginsbrea2do#n of
carbohydrates
-
8/17/2019 Fisio Digestion
11/121
-
8/17/2019 Fisio Digestion
12/121
CONTROL OF SALIVARY SECRETION
cerebral cortex
salivary centre
in medulla
autonomic nerves
salivary glands
↑ salivary secretion
pressure receptors
and chemoreceptorsin the mouth
other inputs
7onditionedre3e+
simplere3e+
-
8/17/2019 Fisio Digestion
13/121
8ropharyn+8ropharyn+
"o convey food "o convey foodinto theinto the
esophagus%esophagus%
.mportant role.mportant role
in s#allo#ing%in s#allo#ing%
-
8/17/2019 Fisio Digestion
14/121
Esophagus%Esophagus%
5ollo# muscular tube5ollo# muscular tube
connecting pharyn+ andconnecting pharyn+ andstomach%stomach%
9ounded by sphincters%9ounded by sphincters%
ined #; strati$edined #; strati$ed
s
-
8/17/2019 Fisio Digestion
15/121
-
8/17/2019 Fisio Digestion
16/121
-
8/17/2019 Fisio Digestion
17/121
-
8/17/2019 Fisio Digestion
18/121
+tomach all+tomach all
-
8/17/2019 Fisio Digestion
19/121
StomachStomach::! "emporary "emporary stores
ingested food%stores ingested food% sphincterssphincters
prevent bac2#ard 3o# of materials intoprevent bac2#ard 3o# of
materials into
esophagus and regulate release of stomachesophagus and regulate
release of stomachcontents into small intestinecontents into small
intestine
! 7hurn0 mi+es food #ith gastric =uice%7hurn0 mi+es food #ith
gastric =uice%! Mechanical and chemical brea2do#n of
ingestedMechanical and chemical brea2do#n of ingested
materialmaterial
! Produces0 mucus0 57l and pepsinogen%Produces0 mucus0 57l and
pepsinogen%! 57l converts pepsinogen into pepsin%57l converts
pepsinogen into pepsin%! Sterili6ation of stomach contents by
acidSterili6ation of stomach contents by acid! Pepsin digests
proteins into peptide fragments%Pepsin digests proteins into
peptide fragments%! Absorbs some #ater0 al2ohol0 glucose%Absorbs
some #ater0 al2ohol0 glucose%! 9inds vit% 99inds vit%
9>?>? allo#s abs% in ileumallo#s abs% in ileum
+ecretionDigestion+ecretionDigestion
-
8/17/2019 Fisio Digestion
20/121
-
8/17/2019 Fisio Digestion
21/121
-ontrol of Acid +ecretion
Secretion isdependent uponactivity of 50 C1A"Pasepump%
-astrin0 histamineand acetylcholineincrease numbers ofen6yme in
plasma
membrane%Somatostatin inhibitsacid secretion%
Pepsinogen
Gastrin
H+K + ATP-ase
-
8/17/2019 Fisio Digestion
22/121
Control of Acid Secretion
May be considered
as three separate
phases.1. Cephalic phase.
2. Gastric phase.
3. Intestinal phase.
-
8/17/2019 Fisio Digestion
23/121
1. CEPHALIC PHASE
Siht" s#ell or
thouht of foo!
Parasy#$athetic acti%ation
of astric #otility & astric 'uice secretion
agus nerve
-
8/17/2019 Fisio Digestion
24/121
/ood arrival causes
muscular re0e!es gastrin secretion b$ %
cells.
2. GASTRIC PHASE
Gastrin
GGFOODFOOD
%astrin stimulates secretion from both
chief
-
8/17/2019 Fisio Digestion
25/121
Arri%al of foo! in !uo!enu# triers release of
hor#ones that inhiit astric #otility &secretions*
3. INTESTINAL PHASE
Circulation
Secretin
Cholecysto!inin "CC#$
Intestinal $haseIntestinal $hase!
signals come from intestine and have inhibitory e4ect i%e%
slo#signals come from intestine and have inhibitory e4ect i%e%
slo#the rate of gastric secretionthe rate of gastric secretion
! stretch of duodenum0 and increase in osmolality stimulate
nervestretch of duodenum0 and increase in osmolality stimulate
nervere3e+ that inhibits gastric motility and secretionre3e+ that
inhibits gastric motility and secretion
! presence of fat in duodenum stimulates secretion of
inhibitorypresence of fat in duodenum stimulates secretion of
inhibitoryhormones *enterogastrones,hormones *enterogastrones,
-
8/17/2019 Fisio Digestion
26/121
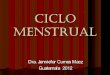
Hormones Released During the Intestinal Phase
When acidic chyme arrives, hormones are released by
the duodenum.
1. Secretin• stimulates pancreas to secrete bicarbonate
ions
that neutralise stomach acid• inhibits gastric
secretion and motility of stomach
2. Cholecystokinin (CCK)• stimulates production / release
of pancreatic enzymes
• stimulates bile release from gallbladder
• inhibits gastric secretion and motility of stomach
-
8/17/2019 Fisio Digestion
27/121
+mall+mall
&ntestine&ntestine
/unctions in digestion/unctions in digestion
! -H1 digestion resumes-H1 digestion resumesand is com#leted
hereand is com#leted here
! Protein digestionProtein digestioncontinues and
com#letescontinues and com#letesherehere
! /at digestion is initiated/at digestion is initiatedand
com#leted hereand com#leted here
Also functions to absorb Also functions to
absorbnutrients, 0uids, andnutrients, 0uids,
andelectrol$teselectrol$tes
Divisions (2 34 feet long totalDivisions (2 34 feet long
totallength"length" segments *>? ft long0 ?? ft incadaver,
duodenum 5 u##er #ortion (2 3duodenum 5 u##er #ortion (2 3
foot long" closest to stomachfoot long" closest to stomach
jejunum 5 middle section jejunum 5 middle section
-
8/17/2019 Fisio Digestion
28/121
PhysiologyPhysiology
"#o primary function "#o primary function!
DigestionDigestion! Absorption of nutrients and #aterAbsorption of
nutrients and #ater
DigestionDigestion! Mainly in duodenum ! small intestine
andMainly in duodenum ! small intestine and
pancreatic en6ymespancreatic en6ymes
! 9icarbonate from pancreas neutrali6es9icarbonate from pancreas
neutrali6es
acidsacids
! Mucous protects from acidsMucous protects from acids
! 9ile emulsi$es fats9ile emulsi$es fats
-
8/17/2019 Fisio Digestion
29/121
Hormones &m#ortant in +m.Hormones &m#ortant in +m.
&ntestine Digestive Activit$ &ntestine Digestive
Activit$ +ecretin+ecretin
-holec$cto)inin (--6"-holec$cto)inin (--6"
'ntero)inase'ntero)inase
Pancreatic enz$mesPancreatic enz$mes
! 7i#ase, Am$lase, Pe#tidases,7i#ase, Am$lase,
Pe#tidases,8r$#sinogen, 8r$#sin8r$#sinogen, 8r$#sin
-
8/17/2019 Fisio Digestion
30/121
PhysiologyPhysiology
! Digestive en6ymesDigestive en6ymes
Salivary amylaseSalivary amylase PepsinPepsin Pancreatic
en6ymes:Pancreatic en6ymes:
! "rypsin "rypsin
! 7hymotrypsin7hymotrypsin! 7arbo+ypeptidase7arbo+ypeptidase
! NucleasesNucleases
! Pancreatic lipasePancreatic lipase
! Pancreatic amylasePancreatic amylase
.ntestinal en6ymes:.ntestinal en6ymes:! PeptidasesPeptidases
! DisaccharidasesDisaccharidases
! ipaseipase
!NucleotidasesNucleotidases
-
8/17/2019 Fisio Digestion
31/121
PhysiologyPhysiology
! 5ormones5ormones
7holecysto2inin ! secretion stimulated by7holecysto2inin !
secretion stimulated byfat in duodenumfat in duodenum
! 7ontraction of gall bladder7ontraction of gall bladder!
Pancreatic secretion of en6yme rich materialPancreatic secretion of
en6yme rich material
Secretin ! secretion stimulated by lo# p5Secretin ! secretion
stimulated by lo# p5in duodenumin duodenum
! Secretion of bile from the liverSecretion of bile from the
liver! Pancreatic secretion of 578Pancreatic secretion of
57811 rich =uice rich =uice
-
8/17/2019 Fisio Digestion
32/121
PhysiologyPhysiology
AbsorptionAbsorption! Nutrients bro2en do#n into simple
sugars0Nutrients bro2en do#n into simple sugars0
fatty acids and amino acidsfatty acids and amino acids
! Principle sites of absorptionPrinciple sites of absorption
Duodenum: iron0 calcium0 vitamins0 fats0 sugars0Duodenum: iron0
calcium0 vitamins0 fats0 sugars0amino acids0 vitaminsamino acids0
vitamins
e=unum: fat0 sugar0 amino acid *largely complete
by e=unum: fat0 sugar0 amino acid *largely complete by
mid =e=unum,0 vitaminsmid =e=unum,0 vitamins .leum: vitamin
9.leum: vitamin 9>?>? and bile saltsand bile salts
! Most bile salts are absorbed and recirculated to theMost bile
salts are absorbed and recirculated to the
liver ! important in maintaining bile poolliver ! important in
maintaining bile pool
-
8/17/2019 Fisio Digestion
33/121
Pancreatic 'nz$mesPancreatic 'nz$mes
Am$lase 9 brea)s -H1 starch to maltose, Am$lase 9
brea)s -H1 starch to maltose,maltriose, and small branched
structuresmaltriose, and small branched structures
7i#ase 9 brea)s don trigl$cerides into7i#ase 9 brea)s don
trigl$cerides intofatt$ acids and gl$cerolfatt$ acids and
gl$cerol
Proteol$tic enz$mes brea) #e#tides donProteol$tic enz$mes brea)
#e#tides donto amino acids and di#e#tide fragmentsto amino acids
and di#e#tide fragments
8r$#sinogen8r$#sinogen! converted to tr$#sin b$ enz$me
(entero)inase"converted to tr$#sin b$ enz$me (entero)inase"
located along inner all of small intestinelocated along inner
all of small intestine
! tr$#sin converts other #ancreatic z$mogenstr$#sin converts
other #ancreatic z$mogens(inactive forms" to their active forms
ithin(inactive forms" to their active forms ithinthe small
intestinethe small intestine
-
8/17/2019 Fisio Digestion
34/121
Pancreatic 'nz$mesPancreatic 'nz$mes
(continued"(continued" Most #ancreatic enz$mes are #roducedMost
#ancreatic enz$mes are #roduced
as inactive molecules 5 z$mogensas inactive molecules 5
z$mogens
Are trans#orted to small intestine in Are trans#orted
to small intestine in z$mogen form z$mogen form
Protects the #ancreas from :selfProtects the #ancreas from
:selfdigestion; digestion;
-
8/17/2019 Fisio Digestion
35/121
-
8/17/2019 Fisio Digestion
36/121
7iver (continued"7iver (continued"
Digestive functionsDigestive functions! secretes bile 9
essential for digestion andsecretes bile 9 essential for digestion
and
absor#tion of fatsabsor#tion of fats
! Function 1 overall is to $lter and processFunction 1 overall
is to $lter and processnutrient1rich blood0 not =ust a digestive
functionnutrient1rich blood0 not =ust a digestive function
regulates carbohydrate metabolism through glycogenregulates
carbohydrate metabolism through glycogenstorage and releasestorage
and release
regulates many aspects of lipid metabolism0 eg%0regulates many
aspects of lipid metabolism0 eg%0
cholesterol synthesis and release of 2etonescholesterol
synthesis and release of 2etones deto+i$es blooddeto+i$es blood
urea and bile synthesisurea and bile synthesis
-
8/17/2019 Fisio Digestion
37/121
Non9digestive functionsNon9digestive functions! circulator$
functions> destro$s aged orcirculator$ functions> destro$s
aged or
abnormal blood cells and #roduces clottingabnormal blood cells
and #roduces clotting
factorsfactors
! converts #rotein metabolites to urea forconverts #rotein
metabolites to urea for
elimination b$ )idne$selimination b$ )idne$s
! immune function (6u#?er cells"immune function (6u#?er cells"!
functions as blood reservoir in regulation offunctions as blood
reservoir in regulation of
blood volumeblood volume
7iver (continued"7iver (continued"
-
8/17/2019 Fisio Digestion
38/121
%all
-
8/17/2019 Fisio Digestion
39/121
brea)s large fat globules into
smaller fat dro#lets, #rovides greater surfacesmaller fat
dro#lets, #rovides greater surfacearea on hich li#ase can
act area on hich li#ase can act
-
8/17/2019 Fisio Digestion
40/121
9ile Synthesis9ile Synthesis "his is the main digestive
function of the liver' "his is the main digestive function of
the liver'
Appro+imately > liter per day is producedAppro+imately >
liter per day is produced
bile salts are cholesterol derivatives and function tobile salts
are cholesterol derivatives and function toemulsify fatsemulsify
fats
bile salts are recycled0 not e+cretedbile salts are recycled0
not e+creted
main bile pigment is bilirubin0 derived from &97main bile
pigment is bilirubin0 derived from &97
hemeheme bile is synthesi6ed in the liver and stored in thebile
is synthesi6ed in the liver and stored in the
gallbladdergallbladder
release is stimulated by cholecysto2inin and vagusrelease is
stimulated by cholecysto2inin and vagus
nervenerve
-
8/17/2019 Fisio Digestion
41/121
Intestinal Contractions and Motility
• 2 major types ofcontractions occur inthe small
intestine: – Peristalsis:
• Slow movement.
• Pressure at thepyloric end ofsmall intestine isreater than
atthe distal end.
– Sementation:
• Major contractileactivity of thesmall intestine.
• Contraction ofcircular smoothmuscle.
– Mi! chyme.
.nsert $g% >%>G
-
8/17/2019 Fisio Digestion
42/121
-
8/17/2019 Fisio Digestion
43/121
Large
Intestine
-
8/17/2019 Fisio Digestion
44/121
Anatomy andAnatomy and
PhysiologyPhysiology
Functions *convertsFunctions *convertschyme to feces,chyme to
feces,
! Absorption of #ater andAbsorption of #ater andelectrolytes
*mainly onelectrolytes *mainly onright side,right side, Absorbs HH
ml #ater;dayAbsorbs HH ml #ater;day 7apacity >IHH1?HHH7apacity
>IHH1?HHH
ml;day *#hen e+ceededml;day *#hen e+ceededresults in
diarrhea,results in diarrhea,
! Sigmoid colon reservoirSigmoid colon reservoirfor dehydrated
fecalfor dehydrated fecalmassmass J?HH g feces;dayJ?HH g
feces;day
! Kater ! H1LHKater ! H1LH! Food residueFood residue!
9acteria9acteria! 7ells7ells! Unabsorbed mineralsUnabsorbed
minerals
-
8/17/2019 Fisio Digestion
45/121
Anatomy and PhysiologyAnatomy and Physiology! Secretes mucus *no
en6ymes,Secretes mucus *no en6ymes,
! 9acteria produce vitamin C and several 9)s9acteria produce
vitamin C and several 9)s
! Flatus *N5Flatus *N50 780 78??0 50 5??0 50 5??S0 75S0 75GG,,
7878?? produced #hen fatty acids and 57l areproduced #hen fatty
acids and 57l are
neutrali6ed by bicarbonateneutrali6ed by bicarbonate
9acterial fermentation of carbohydrates9acterial fermentation of
carbohydratesproduces 78produces 78??0 50 5??0 750 75GG
J>HHH ml e+pelled each dayJ>HHH ml e+pelled each day
E+cess occurs #ith aerophagia and diets high inE+cess occurs #ith
aerophagia and diets high in
indigestible carbohydratesindigestible carbohydrates
! &ectum and anus sites of some of most&ectum and anus
sites of some of most
common disorders 2no#n to humanscommon disorders 2no#n to humans
7onstipation7onstipation 5emorrhoids5emorrhoids Abscesses and
$stulasAbscesses and $stulas 7olon and rectal cancer7olon and
rectal cancer
-
8/17/2019 Fisio Digestion
46/121
9acteria live in the colon and9acteria live in the colon
andstimulate the production of vitamin Cstimulate the production of
vitamin C
and some of the 9 comple+ vitaminsand some of the 9 comple+
vitamins
Mucus is produced but no en6ymesMucus is produced but no
en6ymesare secreted in the large intestineare secreted in the large
intestine
-
8/17/2019 Fisio Digestion
47/121
D.-ES".E A7"..".ES 8FD.-ES".E A7"..".ES 8F
A&-E .N"ES".NEA&-E .N"ES".NE
STRUCTURE ACTIVITY RESULT
Mucosa Secretesmucus
"u#ricates colon $protects mucosa
%#sor#s water Maintains water#alance&
solidifiesfeces& a#sor#s
vitamins $ some ions
-
8/17/2019 Fisio Digestion
48/121
D.-ES".E A7"..".ES 8FD.-ES".E A7"..".ES 8F
A&-E .N"ES".NEA&-E .N"ES".NE
STRUCTURE ACTIVITY RESULT
"umen 'acterialactivity
'rea(s downundiestedcar#ohydrates)protein) $ amino acidsinto
products that can#e e!pelled in feces
or a#sor#ed $deto!ified #y liver
Synthesi*es certain 'vitamins $ vitamin +
-
8/17/2019 Fisio Digestion
49/121
-
8/17/2019 Fisio Digestion
50/121
D.-ES".E A7"..".ES 8FD.-ES".E A7"..".ES 8F
A&-E .N"ES".NEA&-E .N"ES".NE
STRUCTURE ACTIVITY RESULT
Muscularis Massperistalsis
-orces contents intosimoid colon
efecationrefle!
/liminates feces #ycontractions in simoidcolon $ rectum
-
8/17/2019 Fisio Digestion
51/121
Secretion &
H 2O
absorption
2000 ml – 150 ml = ?
-
8/17/2019 Fisio Digestion
52/121
Ion & Vitamin
absorption
-
8/17/2019 Fisio Digestion
53/121
Rectum
0he
efecation
1efle!
-
8/17/2019 Fisio Digestion
54/121
Defecation processDefecation process
&e3e+ rela+ation of internal sphincter&e3e+ rela+ation
of internal sphincter
alsalva maneouvre raisingalsalva maneouvre raising
intraabdominal pressureintraabdominal pressure &ela+ation of
puborectalis *anorectal&ela+ation of puborectalis
*anorectal
angle,angle,
oluntary rela+ation of e+ternaloluntary rela+ation of
e+ternalsphinctersphincter
Defecation reflex
-
8/17/2019 Fisio Digestion
55/121
Defecation reflex> 15 mm Hg
-
8/17/2019 Fisio Digestion
56/121
Disorders of the -. tractDisorders of the -. tract
Mouth and throatMouth and throat! gingivitis 1 infection of the
gum0 can leadgingivitis 1 infection of the gum0 can lead
to periodonititis involving the supportingto periodonititis
involving the supporting
bone of the teethbone of the teeth! incent)s disease 1 a 2ind of
gingivitisincent)s disease 1 a 2ind of gingivitis
caused by a spirochetecaused by a spirochete
! eu2opla2ia 1 characteri6ed by thic2enedeu2opla2ia 1
characteri6ed by thic2ened
#hite patches on the mucous membranes#hite patches on the mucous
membranesof the mouth 1 common in smo2ers andof the mouth 1 common
in smo2ers and
may be a precursor to cancermay be a precursor to cancer
Symptoms of esophageal disordersSymptoms of esophageal
disorders
-
8/17/2019 Fisio Digestion
57/121
Symptoms of esophageal disordersSymptoms of esophageal
disorders
DysphagiaDysphagia! Sub=ective a#areness of an impairment
ofSub=ective a#areness of an impairment of
s#allo#ings#allo#ing
! Ma=or symptom for diseases of the pharyn+ orMa=or symptom for
diseases of the pharyn+ oresophagusesophagus
! 8ccurs in some non1esophageal disorders resulting8ccurs in
some non1esophageal disorders resulting
from vascular or neurologic diseasefrom vascular or neurologic
disease! May be of obstructive or motor originMay be of obstructive
or motor origin 8bstructive causes8bstructive causes
! StrictureStricture
! "umors "umors
Motor causesMotor causes! .mpaired peristalsis.mpaired
peristalsis! Dysfunction of UES or ESDysfunction of UES or ES
! 7ommon motor disorders ! achalasia0 scleroderma0 di4use7ommon
motor disorders ! achalasia0 scleroderma0 di4useesophageal
spasmesophageal spasm
Symptoms of esophageal disorders ! cont%Symptoms of esophageal
disorders ! cont%
-
8/17/2019 Fisio Digestion
58/121
Symptoms of esophageal disorders cont%Symptoms of esophageal
disorders cont%
Pyrosis *heart burn,Pyrosis *heart burn,! 7aused by re3u+ of
gastric acid or bile secretions7aused by re3u+ of gastric acid or
bile secretions
! Persistent re3u+ caused by incompetent ESPersistent re3u+
caused by incompetent ES! results from e+cess stretching of the
lo#erresults from e+cess stretching of the lo#er
esophagus' not due to hyperacidity of theesophagus' not due to
hyperacidity of thestomachstomach
8dynophagia8dynophagia! Pain induced by s#allo#ingPain induced
by s#allo#ing
&egurgitation&egurgitation! 9ac2 3o# into mouth9ac2 3o#
into mouth
! E4ortless *as opposed to vomiting,E4ortless *as opposed to
vomiting,
! 7ommon in infants7ommon in infants! &e3ects both ES
incompetence and failure of UES&e3ects both ES incompetence and
failure of UES
to serve as regurgitation barrierto serve as regurgitation
barrier
Disorders of esophageal motilityDisorders of esophageal
motility
-
8/17/2019 Fisio Digestion
59/121
Disorders of esophageal motilityDisorders of esophageal
motility
AchalasiaAchalasia! De$nition / uncommon hypomotility
disorderDe$nition / uncommon hypomotility disorder
characteri6ed by #ea2 and uncoordinated peristalsischaracteri6ed
by #ea2 and uncoordinated peristalsisor aperistalsis #ithin the
body of the esophagus0or aperistalsis #ithin the body of the
esophagus0
elevated ES pressure and failure of ES to rela+elevated ES
pressure and failure of ES to rela+
completelycompletely
Foods and li
-
8/17/2019 Fisio Digestion
60/121
Disorders of esophageal motilityDisorders of esophageal
motility
Achalasia 1 cont%Achalasia 1 cont%!
"reatment "reatment
Palliative0 measures to relieve obstruction ofPalliative0
measures to relieve obstruction of
lo#er esophaguslo#er esophagus! No #ay to restore peristalsisNo
#ay to restore peristalsis
"#o forms of therapy "#o forms of therapy! Dilation
of ES #ith pneumatic bag or mercuryDilation of ES #ith pneumatic
bag or mercury
$lled bag *bougie,$lled bag *bougie,
! Surgery to open ES accompanied by pyloroplastySurgery to open
ES accompanied by pyloroplasty
i d f h l ili
-
8/17/2019 Fisio Digestion
61/121
Disorders of esophageal motility ! cont%Disorders of esophageal
motility ! cont%
Di4use esophageal spasmDi4use esophageal spasm! De$nition /
uncoordinated0 nonpropulsiveDe$nition / uncoordinated0
nonpropulsive
contractions in response to s#allo#ingcontractions in response
to s#allo#ing
! 7ause un2no#n ! more common in patients O IH7ause un2no#n !
more common in patients O IH Fairly commonFairly common
! Usually asymptomaticUsually asymptomatic Sometimes dysphagia
and odynophagia that areSometimes dysphagia and odynophagia that
are
aggravated by cold foods0 large boluses and nervousaggravated by
cold foods0 large boluses and nervoustensiontension
Sometimes chest pain that may be confused #ith anginaSometimes
chest pain that may be confused #ith angina
! "reatment "reatment Avoid cold foods and large
mealsAvoid cold foods and large meals Antacids0 sedatives0
nitroglycerineAntacids0 sedatives0 nitroglycerine Esophageal
dilation is symptoms persistent andEsophageal dilation is symptoms
persistent and
distressingdistressing
Disorders of esophageal motility ! cont%Disorders of esophageal
motility ! cont%
-
8/17/2019 Fisio Digestion
62/121
SclerodermaScleroderma!
Esophageal motor dysfunction occurs inEsophageal motor
dysfunction occurs inO ?; of patients #ith progressiveO ?; of
patients #ith progressive
systemic sclerosis *scleroderma,systemic sclerosis
*scleroderma,
! Atrophy of smooth muscle in lo#erAtrophy of smooth muscle in
lo#er
portion of esophagusportion of esophagus! .ncompetence of ES
often leads to re3u+.ncompetence of ES often leads to re3u+
esophagitis and subse
-
8/17/2019 Fisio Digestion
63/121
EsophagitisEsophagitis
De$nition / in3ammation of theDe$nition / in3ammation of the
esophageal mucosaesophageal mucosa May be acute or chronicMay be
acute or chronic
! .nnocuous type follo#s ingestion of hot.nnocuous type follo#s
ingestion of hot
li
-
8/17/2019 Fisio Digestion
64/121
-
8/17/2019 Fisio Digestion
65/121
0he lower esophaus here shows sharply demarcated ulcerations
that
have a #rownred #ase) contrasted with the normal pale white
esophaeal mucosa at the far left. Such 4punched out4 ulcers
are
suestive of heres simle# in$e%"ion&
EsophagitisEsophagitis
-
8/17/2019 Fisio Digestion
66/121
EsophagitisEsophagitis
7hronic re3u+ esophagitis and 5iatus7hronic re3u+ esophagitis
and 5iatus
5ernia5ernia! Most common formMost common form
! 7ause ! incompetence of ES and re3u+ of7ause ! incompetence of
ES and re3u+ of
gastric or intestinal =uice into esophagusgastric or intestinal
=uice into esophagus often associated #ith hiatus herniaoften
associated #ith hiatus hernia
! Mechanisms that prevent re3u+Mechanisms that prevent re3u+
"one of sphincter in ES "one of sphincter in ES
Angle of entry ! creates a 3ap valveAngle of entry ! creates a
3ap valve .ntra1abdominal pressure closes segment of.ntra1abdominal
pressure closes segment of
esophagus belo# diaphragmesophagus belo# diaphragm
Esophagitis ! cont%Esophagitis ! cont%
-
8/17/2019 Fisio Digestion
67/121
! 5iatus *hiatal, hernia5iatus *hiatal, hernia
5erniation of portion of stomach into chest5erniation of portion
of stomach into chest
? types? types! Direct or sliding *most common,Direct or sliding
*most common,
-astroesophageal =unctions slides into thoracic-astroesophageal
=unctions slides into thoracic
cavitycavity
ES opens causing re3u+ES opens causing re3u+ 8ften
asymptomatic8ften asymptomatic
! Paraesophageal or rollingParaesophageal or rolling
Part of fundus roles through hiatusPart of fundus roles through
hiatus
ES remains competent and no re3u+ES remains competent and no
re3u+
Ma=or complication is strangulationMa=or complication is
strangulation
.mportant clinical consideration is if there is.mportant
clinical consideration is if there isre3u+re3u+
Esophagitis ! cont%Esophagitis ! cont%
-
8/17/2019 Fisio Digestion
68/121
"reatment of sliding hernia "reatment of sliding
hernia
! -oal is to prevent re3u+ or neutrali6e-oal is to prevent re3u+
or neutrali6ere3u+re3u+
Fre
-
8/17/2019 Fisio Digestion
69/121
Disorders of the -. tractDisorders of the -. tract
StomachStomach! 5iatal hernia 1 a #ea2ness in the5iatal hernia 1
a #ea2ness in the
diaphragm at the point #here thediaphragm at the point #here
the
esophagus connects allo#ing theesophagus connects allo#ing
thestomach or other abdominal organsstomach or other abdominal
organs
protrude up#ardsprotrude up#ards
! nausea and vomiting 1 caused by annausea and vomiting 1 caused
by an
interruption of for#ard movement ofinterruption of for#ard
movement ofnutrition' reverse peristalsisnutrition' reverse
peristalsis
-
8/17/2019 Fisio Digestion
70/121
Disorders of the -. tractDisorders of the -. tract
Stomach0 continuedStomach0 continued! gastritis 1 in3ammation of
the stomachgastritis 1 in3ammation of the stomach
mucosa' causes include irritation by spicymucosa' causes include
irritation by spicy
food0 drugs0 alcohol0 or nicotinefood0 drugs0 alcohol0 or
nicotine
! stomach cancer 1 males are morestomach cancer 1 males are
more
susceptible than females' symptoms usuallysusceptible than
females' symptoms usually
long standing indigestionlong standing indigestion
! peptic ulcer 1 most common ages H1GI'peptic ulcer 1 most
common ages H1GI'causative factors include smo2ing0
drin2ing'causative factors include smo2ing0 drin2ing'
anti1in3ammatory drugs and bacterium0anti1in3ammatory drugs and
bacterium0
5elicobacter pylori5elicobacter pylori
-astritis ! in3ammation or hemorrhagic-astritis ! in3ammation or
hemorrhagicdi i f h
-
8/17/2019 Fisio Digestion
71/121
condition of the mucosacondition of the mucosa
Acute super$cial gastritisAcute super$cial gastritis
! Erodes surface of epithelium in di4use orErodes surface of
epithelium in di4use orlocali6ed patternslocali6ed patterns
! 7auses7auses Drugs ! NSA.DSDrugs ! NSA.DS
7hemicals ! alcohol0 bile acids0 pancreatic en6ymes07hemicals !
alcohol0 bile acids0 pancreatic en6ymes0ca4eine0 strong
spicesca4eine0 strong spices 5elicobacter pylori5elicobacter
pylori
! 7linical manifestations7linical manifestations ague abdominal
discomfortague abdominal discomfort
Epigastric tendernessEpigastric tenderness 9leeding9leeding
omitingomiting 5ematemesis5ematemesis
-
8/17/2019 Fisio Digestion
72/121
0his is a typical a%u"e !as"ri"is with a diffusely
hyperemic
astric mucosa. 0here are many causes for acute astritis:
alcoholism) drus) infections) etc.
-astritis ! in3ammation or hemorrhagic condition of the-astritis
! in3ammation or hemorrhagic condition of the
tmucosa cont
-
8/17/2019 Fisio Digestion
73/121
mucosa 1 cont%mucosa 1 cont%
! Usually resolves #hen o4ending agentUsually resolves #hen
o4ending agentremovedremoved
Antiemitic drugs to relieve nausea and vomitingAntiemitic drugs
to relieve nausea and vomiting
May need to correct 3uids and electolytesMay need to correct
3uids and electolytes
Acid bloc2ers and antacidsAcid bloc2ers and antacids Sulcrafate
to coat stomach liningSulcrafate to coat stomach lining
-astritis 1 cont%-astritis 1 cont%
-
8/17/2019 Fisio Digestion
74/121
7hronic atrophic gastritis7hronic atrophic gastritis!
Progressive atrophy of glandularProgressive atrophy of
glandular
epithelium #ith loss of parietal and chiefepithelium #ith loss
of parietal and chief
cellscells
Decreased 57l0 pepsin and intrisic factorDecreased 57l0 pepsin
and intrisic factorproductionproduction
! 7aused mainly by 5% pylori7aused mainly by 5% pylori
More often in elderlyMore often in elderly
Alcohol0 hot tea and smo2ing may predisposeAlcohol0 hot tea and
smo2ing may predispose
! May lead to gastric ulcers or carcinomaMay lead to gastric
ulcers or carcinoma
-
8/17/2019 Fisio Digestion
75/121
5astritis is often accompanied #y infection with 'eli%oba%"er
ylori&
0his small curved to spiral rodshaped #acterium is found in
the
surface epithelial mucus of most patients with active astritis.
0he rods
are seen here with a methylene #lue stain.
-
8/17/2019 Fisio Digestion
76/121
0his of astric mucosa reveals the presence of many short) curved
rodli(e oranisms
overlyin the mucosa. 0hese are 'eli%oba%"er ylori oranisms)
whose home is theastric mucus. 0he incidence of ,. pylori infection
increases with ae) with half of
%merican adults infected #y ae 67. ,. pylori oranisms
#rea( down mucosal
lycoproteins and damae epithelial cells) leadin to inflammationa
chronic astritis
that is asymptomatic in most cases. Peptic ulcer disease)
particularly duodenal
ulceration) is stronly associated with ,. pylori infection)
which may also play a role in
development of astric carcinoma. %nti#iotic treatment of ,.
pylori reduces these
complications
-
8/17/2019 Fisio Digestion
77/121
-astritis 1 cont%-astritis 1 cont%
! Symptoms generally varied andSymptoms generally varied and
vaguevague
Feeling of fullnessFeeling of fullness
Anore+iaAnore+ia ague epigastric distressague epigastric
distress
! "reatment varies depending on "reatment varies
depending on
causecause
AntibioticsAntibiotics
Avoid irritantsAvoid irritants
7orrect iron de$ciency if present7orrect iron de$ciency if
present
itamin 9itamin 9>?>? supplementsupplement
-
8/17/2019 Fisio Digestion
78/121
PA"8-ENES.S B "E&AP.PA"8-ENES.S B "E&AP.
-AS"&.".S DAN "UCAC-AS"&.".S DAN
"UCACPEP".C PEP".C
-
8/17/2019 Fisio Digestion
79/121
P+NDA,-L-AP+NDA,-L-A
NN enyebab gastritis dan tukak peptikenyebab gastritis
dan tukak peptikadalah
dalah
multifaktor
ultifaktor
atofisiologi dasar adalah gangguan
atofisiologi dasar adalah gangguan
keseimbangan antara faktor-faktoreseimbangan antara
faktor-faktor agresifgresif
dan faktor-faktor
an faktor-faktor
defensif
efensif
Sebagian penderita yang telah diobati
ebagian penderita yang telah diobati
dan sembuh ternyataan sembuh ternyata
kambuhambuh lagilagi
Kualitas penyembuhan luka
ualitas penyembuhan luka
diduga
diduga
berperan penting dalam terjadinya
erperan penting dalam terjadinya
kekambuhan penyakit iniekambuhan penyakit ini
Pathophysiology of Peptic Ulceration
-
8/17/2019 Fisio Digestion
80/121
I&I& (as"ri% a%id se%re"ion homeos"a"a"is and
!as"roduodenal(as"ri% a%id se%re"ion homeos"a"a"is and
!as"roduodenal
mo"ili"ymo"ili"yII&II& Ei"helial de$ense
me%hanismEi"helial de$ense me%hanism
III&III& ')')
IV&IV& *SAID*SAID
V&V& O"her ul%ero!eni%O"her ul%ero!eni%
Multi$le causes of P-DMulti$le causes of P-D
NSAIDs -astric acid Stress
Defense
.n3ammation,* Pylori
Pathophysiology of Peptic Ulceration
-
8/17/2019 Fisio Digestion
81/121
-
8/17/2019 Fisio Digestion
82/121
% 8 cm acute !as"ri% ul%er is shown here in
the
upper fundus. 0he ulcer is shallow and sharply
demarcated) with surroundin hyperemia. It is
pro#a#ly #enin. ,owever) all astric ulcers should
#e #iopsied to rule out a malinancy.
-
8/17/2019 Fisio Digestion
83/121
0he stronest association
with ,elico#acter pylori is
with duodenal e"i%
ul%era"ionover 96 of
duodenal ulcers. Seen
here is a penetratin acuteulceration in the duodenum
just #eyond the pylorus. %n
acute duodenal ulcer is
seen in two views on upper
endoscopy in the lowerpanels.
Peptic ulcer disease 1 cont%Peptic ulcer disease 1 cont%
-
8/17/2019 Fisio Digestion
84/121
7omplications7omplications!
5emorrhage5emorrhage
Most freI1?HMost freI1?H
Most common in ulcers of the posterior #all of duodenalMost
common in ulcers of the posterior #all of duodenalbulb due to
pro+imity of arteriesbulb due to pro+imity of arteries
Symptoms depend on severitySymptoms depend on severity
! AnemiaAnemia! 8ccult blood in stool8ccult blood in stool
! 9lac2 and tarry stool9lac2 and tarry stool
! 5ematemesis5ematemesis
! Shoc2Shoc2 Mortality up to >H 1 higher for patients over
IHMortality up to >H 1 higher for patients over IH
Peptic ulcer disease 1 cont%Peptic ulcer disease 1 cont%
-
8/17/2019 Fisio Digestion
85/121
! PerforationPerforation
Appro+imately I of all ulcers perforate 1Appro+imately I of all
ulcers perforate 1accounts for I of deaths from peptic
ulcersaccounts for I of deaths from peptic ulcers
Usually on anterior #all of duodenum orUsually on anterior #all
of duodenum orstomachstomach
"hought to be due to e+cess acid and often a "hought
to be due to e+cess acid and often aresult of NSA.DSresult of
NSA.DS
7haracteristic presentation7haracteristic presentation! Sudden
onset of e+cruciating pain in upperSudden onset of e+cruciating
pain in upper
abdomen ! chemical peritonitisabdomen ! chemical peritonitis
! Patient fears to move or breathPatient fears to move or
breath
! Abdomen becomes silent to auscultationAbdomen becomes silent
to auscultation
and board li2e rigidity to palpationand board li2e rigidity to
palpation
"reatment ! immediate surgery "reatment ! immediate
surgery
l b i
-
8/17/2019 Fisio Digestion
86/121
Malabsorption !Malabsorption ! intestinal mucosalintestinal
mucosalabsorption of single or multiple nutrients isabsorption of
single or multiple nutrients is
impaired resulting in inade
-
8/17/2019 Fisio Digestion
87/121
Disorders of the -. tractDisorders of the -. tract
Stomach0 continuedStomach0 continued! pyloric stenosis 1 more
common inpyloric stenosis 1 more common in
males than females0 causes persistentmales than females0 causes
persistentvomiting because of the stricture in thevomiting because
of the stricture in the
pyloric sphincter' re
-
8/17/2019 Fisio Digestion
88/121
Disorders of the -. tractDisorders of the -. tract
.ntestinal disorders.ntestinal disorders! diarrhea 1 abnormal
fre
-
8/17/2019 Fisio Digestion
89/121
.ntestinal obstruction.ntestinal obstruction
De$nition / an interference #ith theDe$nition / an interference
#ith thenormal 3o# of intestinal contentsnormal 3o# of intestinal
contents
through the intestinal tractthrough the intestinal tract
! May be acute or chronic0 partial or completeMay be acute or
chronic0 partial or complete
7hronic obstruction usually involves colon as a7hronic
obstruction usually involves colon as aresult of a tumorresult of a
tumor
Most obstructions involve S.Most obstructions involve S.
7omplete is serious and re
-
8/17/2019 Fisio Digestion
90/121
-
8/17/2019 Fisio Digestion
91/121
Disorders of the -. tractDisorders of the -. tract
.ntestinal Disorders0 continued.ntestinal Disorders0 continued!
7olon cancer 1 one of the most common7olon cancer 1 one of the most
common
types in the US 1 usuallytypes in the US 1 usually
adenocarcinomas that arise from theadenocarcinomas that arise
from the
mucosal lining% 8ccurrence is e
-
8/17/2019 Fisio Digestion
92/121
Disorders of the -. tractDisorders of the -. tract
iver Disordersiver Disorders! 5epatitis 1 in3ammation of the
liver by drugs05epatitis 1 in3ammation of the liver by drugs0
alcohol or infectionalcohol or infection
A 1 transmitted in fecal matter' rarely fatal' infectionA 1
transmitted in fecal matter' rarely fatal' infectiona4ords
life1long immunity' accine availablea4ords life1long immunity'
accine available
9 1 transmitted by direct e+change of blood or body 3uids'9 1
transmitted by direct e+change of blood or body 3uids'accine
availableaccine available
7 1 primarily transmitted by direct e+change of blood'7 1
primarily transmitted by direct e+change of blood'
se+ual transmission can occur0 but limitedse+ual transmission
can occur0 but limited
D 1 transmitted by direct e+change of blood0 only inD 1
transmitted by direct e+change of blood0 only inconcert #ith 5ep9
infectionconcert #ith 5ep9 infection
E 1 transmitted by fecal contamination of #aterE 1 transmitted
by fecal contamination of #ater
i d f h
-
8/17/2019 Fisio Digestion
93/121
Disorders of the -. tractDisorders of the -. tract
iver Disorders0 continuediver Disorders0 continued! 7irrhosis 1
chronic disease in #hich active7irrhosis 1 chronic disease in #hich
active
liver cells are replaced by inactive connectiveliver cells are
replaced by inactive connective
tissue' most common cause is alcoholismtissue' most common cause
is alcoholismcompounded #ith malnutrition% .n latercompounded #ith
malnutrition% .n later
stages there is hampering of portal circulationstages there is
hampering of portal circulation
causing congestion in the peritoneal cavity 1causing congestion
in the peritoneal cavity 1
ascitesascites! 7ancer 1 the liver is a common site for7ancer 1
the liver is a common site for
metastasesmetastases
i d f h
-
8/17/2019 Fisio Digestion
94/121
Disorders of the -. tractDisorders of the -. tract
iver Disorders0 continuediver Disorders0 continued! aundice
1 yello# coloring of the s2in and aundice 1 yello# coloring of
the s2in and
eyes' cause is damage to the livereyes' cause is damage to the
liver
ma2ing it unable to con=ugate bilirubinma2ing it unable to
con=ugate bilirubin
or a bloc2age in the bile ducts #ith bileor a bloc2age in the
bile ducts #ith bile
pigment accumulation in the bloodpigment accumulation in the
blood
Di d f h -.
-
8/17/2019 Fisio Digestion
95/121
Disorders of the -. tractDisorders of the -. tract
-allbladder-allbladder! -all stones *cholelithiasis, 1 formed
from-all stones *cholelithiasis, 1 formed from
cholesterol and bloc2 the ducts' paincholesterol and bloc2 the
ducts' pain
occurs #hen the stones prevent the 3o#occurs #hen the stones
prevent the 3o#
of bile and hamper the digestive processof bile and hamper the
digestive process
! 7holecystitis 1 .n3ammation of the gall7holecystitis 1
.n3ammation of the gall
bladderbladder
-
8/17/2019 Fisio Digestion
96/121
i d f hDi d f th -. t t
-
8/17/2019 Fisio Digestion
97/121
Disorders of the -. tractDisorders of the -. tract
Digestive DisordersDigestive Disorders! Anore+ia 1 chronic loss
of appetite' causesAnore+ia 1 chronic loss of appetite' causes
can be physical *heavy e+ercise, or mentalcan be physical *heavy
e+ercise, or mental
*more li2ely to be emotional and;or social*more li2ely to be
emotional and;or social
rather than physiological disruption in therather than
physiological disruption in the
brain,% Anore+ia nervosa a4ects mostlybrain,% Anore+ia nervosa
a4ects mostly
young #omenyoung #omen
! 9ulimia *binge1purge syndrome, 1 prevention9ulimia
*binge1purge syndrome, 1 prevention
of the absorption of food because of induceof the absorption of
food because of induce
vomiting or large doses of la+ativesvomiting or large doses of
la+atives
-
8/17/2019 Fisio Digestion
98/121
"han2 Qou "han2 Qou
Pencernaan di rongga mulut
-
8/17/2019 Fisio Digestion
99/121
Pengaturan salivasi
-
8/17/2019 Fisio Digestion
100/121
Struktur oesophagus
-
8/17/2019 Fisio Digestion
101/121
Proses menelan
-
8/17/2019 Fisio Digestion
102/121
oses e e a
Struktur !ungsi
-
8/17/2019 Fisio Digestion
103/121
"ambung
Sekresi
-
8/17/2019 Fisio Digestion
104/121
#erakan
"ambung
#erakan "ambung
-
8/17/2019 Fisio Digestion
105/121
$untah
-
8/17/2019 Fisio Digestion
106/121
$untah
%&omitus'
Pancreas
-
8/17/2019 Fisio Digestion
107/121
Pengaturan
-
8/17/2019 Fisio Digestion
108/121
sekresi pancreas
!ungsi Hati
-
8/17/2019 Fisio Digestion
109/121
Hepar !esica
-
8/17/2019 Fisio Digestion
110/121
&ellea
-
8/17/2019 Fisio Digestion
111/121
Pengaturan
sekresi empedu
(sus Halus
-
8/17/2019 Fisio Digestion
112/121
-
8/17/2019 Fisio Digestion
113/121
-
8/17/2019 Fisio Digestion
114/121
-
8/17/2019 Fisio Digestion
115/121
-
8/17/2019 Fisio Digestion
116/121
-
8/17/2019 Fisio Digestion
117/121
-
8/17/2019 Fisio Digestion
118/121
-
8/17/2019 Fisio Digestion
119/121
-
8/17/2019 Fisio Digestion
120/121
-
8/17/2019 Fisio Digestion
121/121
Physiology of Physiology
of Digestion Digestion
Department of PhysiologyDepartment of Physiology
School of MedicineSchool of MedicineUniversity of Sumatera
UtaraUniversity of Sumatera Utara
Dr% QudiDr% Qudi5erlambang5erlambang