
Fault TreeAnalysis

Fault Tree Analysis
• Used in both reliability engineering and system safety engineering
• Developed in 1961 for US ICBM program• Guide published in 1981• Used in almost every engineering discipline• Not a model of all system or component
failures

Applying Fault Tree Analysis
• Postulate top event (fault)• Branch down listing faults in the system
that must occur for the top event to occur• Consider sequential and parallel or
combinations of faults• Use Boolean algebra to quantify fault tree
with event probabilities• Determine probability of top event

Fault Tree Logic
• Use logic gates to show how top event occurs
• Higher gates are the outputs from lower gates in the tree
• Top event is output of all the input faults or events that occur

Terms
• Faults and failures
• System and subsystem faults
• Primary and secondary failure
• Command fault

Fault Tree Symbols
Intermediate Event Symbol
Gate Symbols
AND
OR
Exclusive OR
Priority AND
Inhibit
Transfer Symbols
Transfer IN Transfer OUT
Basic Event
Conditioning Event
Undeveloped Event
External Event
Primary Event Symbols
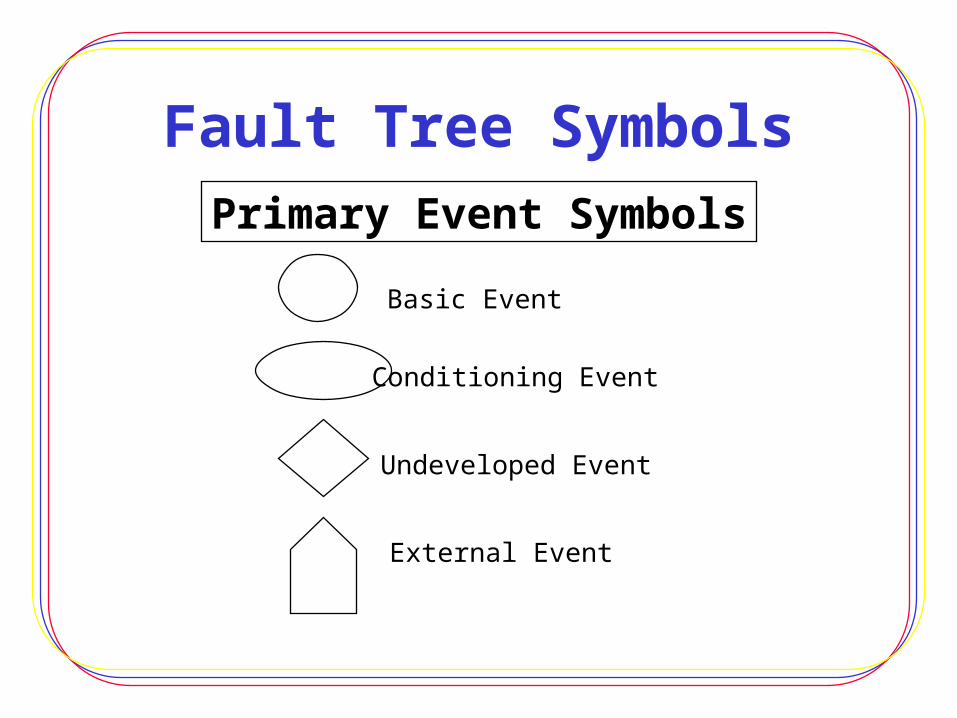
Fault Tree Symbols
Basic Event
Conditioning Event
Undeveloped Event
External Event
Primary Event Symbols

Fault Tree Symbols
Gate Symbols
AND
OR
Exclusive OR
Priority AND
Inhibit

Fault Tree Symbols
Intermediate Event Symbol
Transfer Symbols
Transfer IN Transfer OUT

Union
A=B + CA=B Union C
B OR C must occurfor event A to occur
No Current
Switch AOpen
Battery B0 Volts
A
B C

Intersection
D=E * FD= E Intersection FE AND F must occur
for D to occur
Over-heatedWire
5mA Currentin System
Power Appliedt >1ms
D
E F

Fault Tree Quantification
• Fault tree analysis - is not a quantitative analysis but can be quantified
• How to– Draw fault tree and derive Boolean equations– Generate probability estimates– Assign estimates to events– Combine probabilities to determine top event

Fault Tree Example
PressureSwitch
S
PressureTankSwitch S1
Motor
Timer Relay
Pump
RelayK1
RelayK2
Outlet Valve

Common Mistakes inFault Trees
• Inputs with small probabilities• Passive components• Does quantified tree make sense• Don’t fault tree everything• Careful with Boolean expressions• Independent Vs dependent failure modes• Ensure top event is high priority

FMECA, Human Factors,and Software Safety

Non-Safety Tools
• Failure Modes, Effects, and
Criticality Analysis
• Human Factors Analysis
• Software Safety Analysis

FMEA• Reliability engineering tool• Originated in 1960s• OSHA recognized• Limitation - failure does not have to
occur for a hazard to be present in system
• Used to investigate how a particular failure can come about

FMEA Process
• Define system & analysis scope• Construct block diagrams• Assess each block for effect on system• List ways that components can fail
• Assess failure effects for each failure mode
• Identify single point failures• Determine corrective actions• Document results on worksheet

System Breakdown
Subsystem 1 Subsystem 2 Subsystem 3
Assembly 1 a
Assembly 1 bAssembly 1 c
Subassembly 1c.1
Subassembly 1c.2
Subassembly 1c.3
Component 1c.3.1Component 1c.3.2
Component 1c.3.3Part 1c.3.3.a
Part 1c.3.3.bPart 1c.3.3.c
Total System

FMEA Worksheet
• Component #, name, function• Failure modes• Mission phase• Failure effects locally• Failure propagation to the next level• Single point failure• Risk failure class• Controls, recommendations

Failure Modes
• Premature operation• Failure to operate on time• Intermittent operation• Failure to cease operation on time• Loss of output or failure during operation• Degraded output or operational capability• Unique failure conditions

Failure Modes, Effects, & Criticality Analysis
• Virtually same as FMEA • Identifies criticality of components• Emphasizes probability of failure• Criticality components
– Failure effect probability– Failure mode ratio– Part failure rate– Operating time

Human Factors Safety Analysis
• Many different techniques• Human element must be considered in
engineering design• The merging of three fields:
– Human factors– Ergonomics– Human reliability

Performance & Human Error
• Why do people make mistakes?• Combination of causes - internal/external• Performance shaping factors (factors
that influence how people act)– External PSF– Internal PSF– Stressor PSF

Human Error• Out of tolerance action within human/machine
system• Mismatch of task and person• Significant contributor to many accidents• False assumptions
– Human error is inevitable– People are careless
• More complex systems must be less dependent on how well people operate them

Human Error Categories
• Omission - leaving out a task• Commission
–Selection error–Error of sequence–Time error–Qualitative error

HF Safety AnalysisThe Process
• Describe system goals and functions• List & analyze related human operations• Analyze human errors• Screen errors & select • Quantify errors & affect on system• Recommend changes to reduce impact of
human error

Software Safety• Newest member of system safety field• Software controls millions of systems• Treat software like any system component
– Determine the hazards– If software is involved in hazard - deal with it
• Common tools– Software Hazard Analysis– Software Fault Tree Analysis– Software Failure Modes & Effects

Software Facts• Software is not a hazard• Software doesn’t fail• Health monitoring of software only assures it
performs as intended• Every line of code cannot be reviewed• Fault tolerant is not the same as safe• Shutting down a computer may aggravate a an
already dangerous situation

Software Safety Analysis (SSA)Flow Process
• Software Requirements Development• Top-level System Hazards Analysis• Detailed Design Hazard Analysis• Code Hazard Analysis• Software Safety Testing• Software User Interface Analysis• Software Change Analysis

SSA
Required when software is used to:• Identify a hazard• Control a hazard• Verify a control is in place• Provide safety-critical information or
safety related system status• Recovery from a hazardous condition

Safety Tool Categories• Software safety requirements analysis
– Flowdown analysis– Criticality analysis
• Architectural design analysis• Detailed design analysis
– Soft tree analysis– Petri-Net
• Code analysis

Software Testing
• Software testing
• System safety testing
• Software changes
• IV &V organization

Other Techniques

MORT• Qualitative tool used in 1970s• Merges safety mgt & safety engineering • Analyses mgt policy in relation to RA and
hazard analysis process• Uses a predefined graphical tree• Analyze from top event down• Too large and doesn’t tailor well to
smaller problem

Energy Trace Barrier Analysis (ETBA)
• Qualitative tool for hazard analysis• Developed as part of MORT• Traces energy flow into, through, & out of
system• Four typical energy sources• Energy transfer points & barriers analyzed• Advantages

ETBA Procedure
• Examine system / identify energy sources
• Trace each energy source through system
• Identify vulnerable targets to energy
• Identify all barriers in energy path
• Determine if controls are adequate
Sneak Circuit Analysis• Standardized by Boeing in 1967• Formal analysis of all paths that a
process could take• Find sneak paths, timing, or procedures
that could yield an undesired effect• Review engineer drawings, translate, &
identify patterns• Disadvantages

Cause-Consequence Analysis• Uses symbolic logic trees• Determine accident or failure scenario
that challenges the system• Develop a bottom-up analysis• Failure probabilities calculated• Consequences identified from top event • Consequence may have variety of
outcomes

Dispersion Modeling• Quantitative tool for environmental and
system safety engineering• Used in chemical process plants, can
determine seriousness of chemical release• Internationally recognized model -
CAMEO• Features of the system• Advantages

Test Safety
• Not an analysis technique• Assures safe environment during testing• Must integrate system safety process into
test process• Three layers of test environment• Safety analysis needed at each level• Test readiness review

Comparing Techniques• Complex Vs simple• Apply to different phases of system life
cycle• Quantitative Vs qualitative• Expense• Time and personnel requirements• Some are more accepted in certain
industries

Selecting A Technique• All techniques are good analyses• Consider advantages and disadvantages• Select technique most suited to the
problem, industry, or desired outcome• Ask yourself a few questions
– What’s the purpose? – What is the desired result?– Does it fit your company and achieve goals?– What are your resources and time available?
Data Sources and Training

Data Reliability
• Start with company historical data
• Analyses only as good as the data that is
used
• Caution about misunderstanding data
• Quantifiable data is not always the best
• Always cite sources and assumptions

Data Limits
• Most failure data is generic
• Break large items into smaller parts
• Data may not consider environmental
changes
• Use expert judgement to convert generic
data into realistic values

Government Data Banks
• Government Printing Office– Books from DoD, NASA, EPA, & OSHA
• Government-Industry Data Exchange Program– Army, Navy, FAA, Dept of Labor, Dept of
Energy, National institute of Standards and Technology
• Databases of other countries

Industry Data Banks
• Corporations• Insurance companies• Electronics Industries Associations• Consumer Product Commission• System Safety Society• Material Safety Data Sheets

Creating Your Own Databank• Collect data on system
– Design– Assessments– Hazard identification– Compliance verification
• Make the data easily accessible and consolidated in one place
• Computers and new software make collection easier

Data Bank
• Hazardous materials• MSDS• System design info• Safety critical systems• Best design practices• Testing history• Failure history
• Safety analyses• Accident histories• Safety Standards• Identified hazards• Causes of hazards• Proven hazard controls• Hazard consequences• Hazard tracking system
Systems Info System Safety Data

Safety Training
• Twofold approach–Employee training–Emergency response
• Types of training– Initial training–Refresher training–New training for changes

Employee Training
• Training needs assessment• Purpose of training• Assess current operations• Review hazard analysis data• Develop and implement training• Record training

Emergency Preparedness andResponse Training
• Train all personnel affected by possible emergency
• Training subjects– Evacuation procedures– Shutdown of equipment– Firefighting and first aid– Crowd control and panic prevention
• Conduct exercises

Certification for Hazardous Operations
• Determine personnel that require training
• Certification program elements– Certification examination– Physical examination– Classroom and hands-on training– Test of safe working practices– Recertification schedule

Safety Awareness
• Highlight safety in organization
• Positive incentives
• Establish safety representatives in each area
• Conduct meetings to discuss safety program
• Safety reps should be trained in workplace
safety inspections and program monitoring
Accident Reporting, Investigation,
and Documentation

Reporting the Accident
• Accident reporting without retribution
• Posting of reportable accidents
• New-employee briefing
• Management involvement

Setting Up a Closed-LoopReporting System
• Pre-accident plan
• Report within 24 hours– Pass data up the chain
– Initiate board
– Capture perishable information
• Investigate all accidents

Forming a Board
• Company policy– Accident classification– Standing list of board candidates
• Selecting the Board members– Various backgrounds– Voting members and advisors
• Board responsibilities

Conducting the Investigation
• Preparing for investigation
• Gathering evidence and information
• Analyzing the data
• Discussion of analysis and conclusions
• Recommendations

Investigation Report• Abstract of report
• Summary of F &
R
• Procedure used
• Background
• Sequence of events
• Analysis
methodology
• Analysis results
• Conclusions
• Detailed F & R
• Minority reports
• Appendixes

Accident Documentation
• Investigation Report– Retained with supporting documents
– Corrective action implemented
– Available for future safety analysis
• Retain the records
• Public release of information

Risk Assessment

What is Risk?• Severity of consequences of an accident
times the probability of occurrence• Risk perception may vary from actual risk• Risk: realization of unwanted, negative
consequences of an event (Rowe)• Risk: summation of three elements
– Event scenario– Probability of occurrence– Consequence

Risk Perception
Factors concerning perception of risk• Voluntary Vs nonvoluntary• Chronic Vs catastrophic• Dreaded Vs common• Fatal Vs nonfatal• Known Vs unknown risk• Immediate or delayed danger• Control over technology
Risk Assessment Methodology
1 Define objectives
2 Define system
3 Develop scenarios
4 Develop event
trees
5 Quantify
scenarios
6 Consequences
7 Risk evaluation
8 Risk management
Formal process of calculating risk and making a decision on how to react
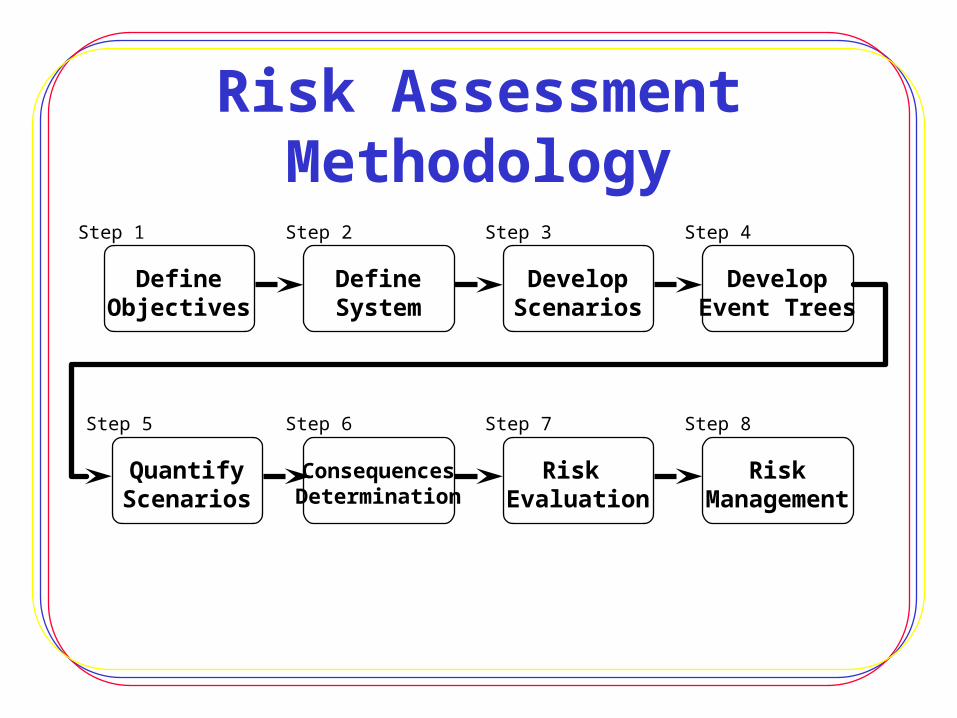
Risk Assessment Methodology
DefineObjectives
DefineSystem
DevelopEvent Trees
DevelopScenarios
QuantifyScenarios
ConsequencesDetermination
RiskManagement
Risk Evaluation
Step 1 Step 2 Step 3 Step 4
Step 5 Step 6 Step 7 Step 8

Identifying Risk in a System
• Risk identified through analysis techniques
• Use several techniques
• Construct fault tree
• Use analysis tools to focus on which
component is the trigger
Risk Communication• Communicating with public
– Acknowledge the community – Do not imply irrationality or ignorance
• Methods to promote communication– Community participation– Approach “group” appropriately– Consultation with community– Involve community in negotiations– Be open with information

Risk Evaluation

A Probabilistic Approach
• Quantifying risk through probability of
failure
• Hard to quantify probability of some events
• Understand the data, the sources, & the
limitations
• Follow rules of probability

Risk Analysis Model
• Developing accident scenarios & initiating event
• Event Trees• Consequences determination• Uncertainty• Risk evaluation - Risk profiles
Calculating Safety Costs
• Tracking data costs– System downtime (lost productivity)– Equipment damage and replacement– Accident clean-up– Personnel injuries and death
• Expected value• Cost-benefit analysis
Recommended

















