
Page 2 J Am Osteopath Coll Radiol 2013; Vol. 2, Issue 1
Indica ons Breast MR, Walters et al.
Introduc on
Breast cancer is the second most common cancer in women, following skin cancer. It accounts for 1 in 3 cancers diagnosed in women and is one of the leading causes of mortality in the United States. The average rela ve life me risk of breast cancer in women is about 1 in 8 (12%).1
MRI of the breast has become an important imaging modality in the detec on, evalua on, staging, and management of breast cancer. MRI has proven value in numerous clinical se ngs, including screening for breast cancer in select high‐risk pa ents with the wider use of gene c tes ng; evalua on for mul centricity or bilaterality of a known cancer; determining the efficacy of neoadjuvant chemotherapy; differen a on of scar ssue versus recurrent tumor in pa ents who have undergone breast‐conserva on surgery; and evalua on of pa ents with metasta c axillary adenopathy with an unknown primary. MRI may also be very useful in problem solving for pa ents with dense breast ssue, a difficult physical exam, equivocal mammogram and ultrasound findings, or discordant pathology results. This review offers guidelines and indica ons for breast MRI as represented in the literature.
Technique
Although there is no standardized technique for breast MRI, the American College of Radiology (ACR) has established minimum standards for breast MRI accredita on. The standards include a T2‐weighted sequence, and most importantly, a mul ‐phase T1 weighted sequence. In accordance with the ACR standards, both breasts must be examined simultaneously. Acquisi on during pre and post‐contrast T1 weighted sequences must have a slice thickness ≤ 3.0 mm. There should be no gap, and the maximum in plane pixel dimension for phase and frequency should be ≤ 1.0 mm.2 T1 weighted GRE imaging should be performed quickly with dynamic
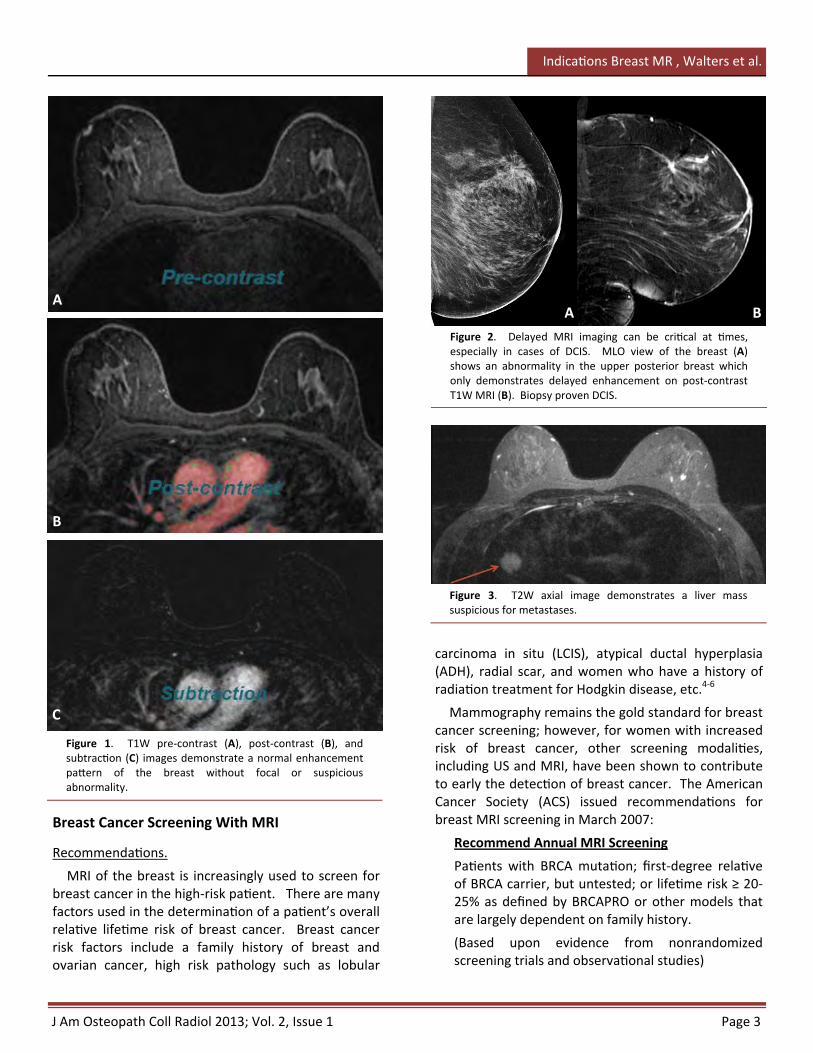
enhancement and delayed imaging performed. Computer aided detec on may be beneficial in interpreta on of the exam. Subtrac on images may prove useful as well. Diffusion weighted imaging (DWI) along with ADC evalua on has been shown to be useful for the differen a on of benign vs. malignant tumors.3 Figure 1 shows normal pre and post‐contrast T1 weighted images, along with a normal subtrac on image.
Evalua on of images and lesions should be based on several factors, most importantly enhancement characteris cs and morphology. Delayed imaging may be beneficial, especially with low grade DCIS (Figure 2). In our prac ce, we also include T1 and T2 weighted open field of view (FOV) sequences to evaluate the chest wall and other surrounding so ssues. We have discovered lung and liver metastases (Figure 3), as well as associated adenopathy (Figure 4), with open FOV sequences.
Repor ng
The most commonly accepted repor ng system for breast imaging is Bi‐Rads classifica on.
Bi‐Rads for MRI is iden cal to the Bi‐Rads classifica on in mammography.
For full lesion features and descrip ons for MRI, the ACR website has a MRI Lexicon Classifica on Form which may be used as a guideline.
MRI Breast Clinical Indica ons: A Comprehensive Review
Michelle C. Walters, D.O., FAOCR,1 and Lennard Nadalo M.D., FACR2
1Medical Director, Advanced Imaging, DeSoto, TX 2Department of Radiology, Methodist Health Systems, Dallas, TX
Category 0 – Incomplete: need for addi onal imaging
Category 1 – Nega ve
Category 2 – Benign findings
Category 3 – Probably benign findings
Category 4 – Suspicious abnormality
Category 5 – Highly sugges ve of malignancy
Category 6 – Known cancer
J Am Osteopath Coll Radiol 2013; Vol. 2, Issue 1 Page 3
Indica ons Breast MR , Walters et al.
Breast Cancer Screening With MRI
Recommenda ons.
MRI of the breast is increasingly used to screen for breast cancer in the high‐risk pa ent. There are many factors used in the determina on of a pa ent’s overall rela ve life me risk of breast cancer. Breast cancer risk factors include a family history of breast and ovarian cancer, high risk pathology such as lobular
Figure 1. T1W pre‐contrast (A), post‐contrast (B), and subtrac on (C) images demonstrate a normal enhancement pa ern of the breast without focal or suspicious abnormality.
carcinoma in situ (LCIS), atypical ductal hyperplasia (ADH), radial scar, and women who have a history of radia on treatment for Hodgkin disease, etc.4‐6
Mammography remains the gold standard for breast cancer screening; however, for women with increased risk of breast cancer, other screening modali es, including US and MRI, have been shown to contribute to early the detec on of breast cancer. The American Cancer Society (ACS) issued recommenda ons for breast MRI screening in March 2007:
Recommend Annual MRI Screening
Pa ents with BRCA muta on; first‐degree rela ve of BRCA carrier, but untested; or life me risk ≥ 20‐25% as defined by BRCAPRO or other models that are largely dependent on family history.
(Based upon evidence from nonrandomized screening trials and observa onal studies)
A
C
B
Figure 2. Delayed MRI imaging can be cri cal at mes, especially in cases of DCIS. MLO view of the breast (A) shows an abnormality in the upper posterior breast which only demonstrates delayed enhancement on post‐contrast T1W MRI (B). Biopsy proven DCIS.
Figure 3. T2W axial image demonstrates a liver mass suspicious for metastases.
A B

Page 4 J Am Osteopath Coll Radiol 2013; Vol. 2, Issue 1
Indica ons Breast MR, Walters et al.
Recommend Annual MRI Screening
Pa ents with radia on to the chest between the ages of 10 and 30 years or a personal history or first‐degree rela ve with Li‐Fraumeni, Cowden, and Bannayan‐Riley‐Ruvalcaba syndromes.
(Based upon expert consensus opinion/life me risk for breast cancer)
Insufficient Evidence to Recommend For or Against MRI Screening
Pa ents with a life me risk of 15‐20% as defined by BRCAPRO or other models that are largely dependent on family history; LCIS, ADH, or atypical lobular hyperplasia; heterogeneously or extremely dense breast on mammography; or a personal history of breast cancer, including DCIS. Screening decisions should be made on a case‐by‐case basis, as there may be par cular factors to support MRI. Payment should not be a barrier. More data on these groups is expected to be published soon.7
Recommend Against MRI Screening
Pa ents with <15% life me risk of breast cancer.
(Based upon expert consensus opinion)
BRCA1 and BRCA2 muta ons are responsible for 40‐50% of all familial cancers. The BRCA muta on increases the average life me risk of breast cancer to approximately 60‐80% and 40% for ovarian cancer (BRCA1).8 The ACS Guidelines recommend “intensified
surveillance” as an alterna ve to bilateral mastectomy. BRCA1 associated breast cancers tend to have benign morphological appearances (round shapes and minimal asymmetry) but an aggressive biological nature. Thus, screening should start at a younger age and occur more frequently in the case of BRCA muta ons. These women are younger at presenta on when average breast density is high. Earlier and more frequent screening in this popula on will result in a substan al cumula ve life me ionizing radia on dose.9,10 With the addi onal increased risk of breast cancer associated with mammographic screening (albeit minimal), poten ally dense breast
Figure 5. Dense breast ssue in a BRCA posi ve pa ent. Bilateral CC views (A) show dense breast ssue bilaterally, which limits the sensi vity of mammography. US (not shown) demonstrated several hypoechoic masses and patchy areas of shadowing. Axial T1W post‐contrast image with fat‐suppression (B) demonstrates benign bilateral fibrocys c changes, Bi‐Rads 2.
A B
Figure 4. T2W axial image reveals medias nal adenopathy.

J Am Osteopath Coll Radiol 2013; Vol. 2, Issue 1 Page 5
Indica ons Breast MR , Walters et al.
ssue in the younger pa ent, and the need for increased sensi vity in the evalua on of these pa ents, MRI has become accepted as an integral part of surveillance in the high risk popula on (Figure 5).
For women with an average risk of breast cancer, there is no data that supports breast MRI for screening at this me. Although MRI does have increased sensi vity in the detec on of breast cancer, the posi ve predic ve value (PPV) is much lower than in the high risk popula on; therefore, the cost of rou ne MRI screening is not jus fied. Long‐term studies and further surveillance may change this perspec ve in the future.
Third Party Reimbursement
Insurance companies tend to follow the above guidelines for reimbursement. For the lower risk pa ent with dense breast ssue, a difficult physical exam, or significant fibrocys c changes, there are less objec ve recommenda ons and MRI of the breast may not be covered by insurance. Most insurance companies u lize a calcula on of risk factors using one of several methods: BRCAPRO ‐ Claus model ‐ Gail model – Tyrer‐Cuzick . The major carriers have policy guidelines for breast MRI.
Sensi vity and Specificity in MRI Breast
Screening
Sensi vity of mammography alone decreases in propor on to the increased density of the breast ssue. However, breast density does not affect the
sensi vity of MRI (Figure 6).11 There are numerous literature references for sensi vity and specificity of mammography, US, and MRI. The references vary but all clearly state that MRI is by far more sensi ve than mammography and US in the detec on of breast cancer for high‐risk pa ents, dense breast ssue,
A
C
B
Figure 6. Pa ent with personal and family history of breast cancer. Bilateral MLO views (A) demonstrate findings of prior lumpectomy on the le for invasive ductal carcinoma; right breast is very dense. US (not shown) demonstrated several hypoechoic masses bilaterally with patchy areas of shadowing. T1W pre (B), post‐contrast (C), and MIP (D) images reveal a cobblestone enhancement pa ern in the right breast at the 9‐10 o’clock posi on. Biopsy revealed high‐grade DCIS with central necrosis. D

Page 6 J Am Osteopath Coll Radiol 2013; Vol. 2, Issue 1
Indica ons Breast MR, Walters et al.
pa ents on hormone replacement therapy (HRT), and in the younger popula on.12,13 According to the Na onal Cancer Ins tute (NCI) Breast Cancer Surveillance Consor um (BCSC), the sensi vity of screening mammography in the detec on of breast cancer (star ng at age 40) ranges from as low as 64% to as high as 100% based upon age and me from prior mammogram. Specificity was as low as 78% to as high as 94%.14
MRI breast does not replace screening mammography or diagnos c mammography with US evalua on. Rather, MRI is used in conjunc on with these modali es (Figure 7). Although breast MRI is more sensi ve in the detec on of breast cancer when compared to mammography and US, it has been reported as less specific overall.15 It should be noted, however, that in a recent ACRIN trial, the specificity of MRI breast was as high as 88%.16 MRI’s imperfect sensi vity comes from its inability to detect low grade DCIS due to the lack of enhancement. Mammography, on the other hand, may detect low grade DCIS as amorphous calcifica ons or small foci of architectural distor on, which may not be detected or be very subtle on breast MRI. Overall, however, MRI has been shown to be superior to mammography in detec ng cases of unsuspected DCIS.17 Contrast‐enhanced MRI of the breast has shown rela vely high sensi vi es, ranging from 94‐99% for invasive cancer and 50‐80% for in situ cancers.18
MRI Breast in the Newly Diagnosed Breast
Cancer Pa ent
Clinical Indica ons and Applica ons of Breast MRI.
The Na onal Comprehensive Cancer Network (NCCN) discussion of breast MRI recommends the use of MRI for the following clinical indica ons and applica ons:
Staging evalua on to define extent of cancer orpresence of mul focal or mul centric cancer in the ipsilateral breast.
Screening for contralateral breast cancer at meof ini al diagnosis.
Evalua on before and a er neoadjuvanttherapy to define extent of disease, response to treatment, and poten al for breast conserving therapy.
Figure 7. Complimentary role of mammography and MRI. Bilateral MLO views (A) demonstrate suspicious calcifica ons in the posterior le breast (biopsy proven DCIS), as well as faint, sca ered calcifica ons in the upper, posterior right breast; the calcifica ons on the right could not be seen well or biopsied on stereotac c technique. Pre (B) and post (C) contrast MR images reveal very minimal nodular enhancement in the far posterior, lateral right breast. Due to the faint calcifica on in this area, the pa ent underwent biopsy with the pathologic diagnosis of low‐grade DCIS. Pa ent also had lumpectomy changes on the le for intermediate grade DCIS. She subsequently opted for bilateral mastectomies.
A
C
B

J Am Osteopath Coll Radiol 2013; Vol. 2, Issue 1 Page 7
Indica ons Breast MR , Walters et al.
staging of breast cancer is outlined in the 7th Edi on of the American Joint Commi ee on Cancer. Key staging components include tumor size; involvement of overlying skin or chest wall; involvement of local or regional lymph nodes, to include mobile or fixed, conglomerate, or extracapsular spread; and presence or absence of distant metastases.
MRI has been shown to increase the sensi vity in the evalua on of local‐regional disease involving the breast and axilla. When combined with mammography, US, and clinical exam, the sensi vity of MRI is as high as 99% in cases of newly diagnosed breast cancer (Figure 9).19 The reported low sensi vity of clinical exam (50%), mammography (60%), and US (83%) alone substan ate the use of MRI in the preopera ve staging of breast cancer pa ents. Breast MRI has been shown to detect both mul centric and bilateral breast cancers with increased sensi vity over clinical exams, mammography, and US (Figures 10 and 11).20,21 Ipsilateral mul centric disease detected with MRI has been reported in 10‐27% of pa ents. MRI detects occult contralateral breast cancer in about 3% of pa ents with invasive ductal carcinoma and in 6% of pa ents with invasive lobular carcinoma. Bilaterality has been reported in up to 10% in selected series.22,23
Overall tumor size is more accurately depicted on MRI compared to mammography when correlated with pathology specimens (Figure 9).24,25 Although it was thought that this may decrease the need for reexcision due to unclear margins, this has recently
Figure 8. Pa ent presented with signs and symptoms of Paget’s disease of the le nipple. CC and MLO views of the le breast (A) demonstrate skin thickening around the nipple region but no other findings. US (not shown) added no addi onal informa on. Post‐contrast color‐coded MR image (B) reveals the extent of the pa ent’s invasive disease.
A
B
Detect addi onal disease in women with mammographically dense breasts.
Iden fy primary cancer in women with axillary nodal adenocarcinoma or Paget’s disease of the nipple (Figure 8) with a breast primary not iden fied on mammography, ultrasound, or physical examina on.
The u lity of MRI in follow‐up screening of women with prior breast cancer is undefined. It should generally be considered only in those whose life me risk of a second primary breast cancer is greater than 20% based on models largely dependent on family history, such as in those with a risk associated with inherited suscep bility to breast cancer.
There is no data demonstra ng that the use of MRI to affect choice of local therapy improves outcomes (local recurrence or survival). Although breast MRI is more sensi ve than mammography or US, false posi ve findings on MRI are common. Therefore, surgical decisions should not be based solely on MRI findings. Tissue sampling of areas of concern iden fied by breast MRI is recommended prior to treatment planning.
Staging.
Treatment op ons for breast cancer are based upon staging. Breast cancer staging is determined by the extent of disease in the breast and axilla, as well as metasta c disease determina on. The current TNM

Page 8 J Am Osteopath Coll Radiol 2013; Vol. 2, Issue 1
Indica ons Breast MR, Walters et al.
Figure 9. Pa ent presents with palpable mass on right. Bilateral MLO views of the breast (A) demonstrate a mass in this region with an US correlate (B). Biopsy revealed invasive ductal carcinoma. MRI breast (C and D) demonstrates more anterior and superior lateral extension than is perceived by mammogram or US.
Figure 10. Bilateral/contralateral breast cancer. MLO (A) and CC (B) views demonstrate a mass in the upper outer le breast, which was confirmed as suspicious on US (not shown). Post‐contrast (C), MIP (D), and color‐coded (E) images reveal the known breast cancer on the le , as well as an unsuspected enhancing mass in the right breast. Second look US was performed with subsequent biopsy; pathological diagnosis was invasive ductal carcinoma.
A
C B
D
A
B
C
D
E

J Am Osteopath Coll Radiol 2013; Vol. 2, Issue 1 Page 9
Indica ons Breast MR , Walters et al.
been shown not to be true. The COMICE trial performed in the UK demonstrated similar need for reexcision in pa ents who had pre‐opera ve MRIs versus those who did not. However, further study with long‐term evalua on and follow‐up is needed.26
In the clinical se ng of DCIS, MRI is useful to rule out underlying invasive carcinoma. This can be accomplished with MRI due to its high nega ve predic ve value (NPV) in the diagnosis of invasive breast cancer. MRI and mammography compliment each other in the diagnosis of DCIS. Although MRI has greater overall sensi vity, it does not detect all DCIS cases, especially those which are non‐enhancing and are only seen as calcifica ons on mammography. Mammography is similarly limited in the detec on of DCIS, especially in the absence of calcifica ons where lesions are only detected as abnormal enhancement on MRI. Research has shown that the overall sensi vity of MRI for high‐grade DCIS is higher than that of mammography.27
Controversy.
Breast surgeons have concerns regarding MRI causing a delay in treatment and/or increasing mastectomy rates. In most cases, the delay in treatment is minimal, since an MRI can be performed quickly a er biopsy with the diagnosis of cancer. As for the increase in mastectomy rates related to breast MRI and the opinion that radia on therapy eradicates or delays progression of residual disease, these are not proven. While there have been reports of unnecessary mastectomies based upon false‐posi ve MRI exams, this emphasizes the point that surgical management of breast cancer should be based upon confirmed histology, i.e. MRI‐guided biopsy.28
With breast conserva on therapy, the rate of recurrence is low but not zero. The statement that outcomes in women who undergo breast conserva on
Figure 11. Bilateral/contralateral breast cancer in a pa ent with a palpable mass on the right. MLO (A) and CC (B) views reveal an asymmetry in the mid‐lower, inner right breast, similar to prior studies. US was performed (not shown), and biopsy demonstrated invasive ductal carcinoma. Color‐coded (C) and MIP (D) post‐contrast images be er delineate the breast cancer on the right and iden fy an addi onal suspicious mass in the le breast. Second look US of le breast was performed with biopsy; pathological diagnosis was invasive ductal carcinoma.
A
B
C
D

Page 10 J Am Osteopath Coll Radiol 2013; Vol. 2, Issue 1
Indica ons Breast MR, Walters et al.
are equivalent to the outcomes in women who undergo mastectomy is debatable. The trials that have been performed to date have shown that women who undergo breast conserva on have a higher risk of local recurrence. Thus, disease free survival is not equivalent.29 It was previously thought that local recurrence did not affect overall survival. However, it is now well accepted that local relapse does affect overall survival. Therefore, preven ng local recurrence is considered as important as the early diagnosis of the primary breast cancer. The ability to prevent local recurrence requires more accurate staging and subsequent treatment; this is where MRI can play a cri cal role.30‐32
The threshold of radia on therapy to eradicate any residual disease has not been established. Each pa ent should be offered the best treatment for long‐term survival. In essence, a staging MRI examina on which demonstrates only one focal cancer site allows the pa ent, surgeon, and oncologist to explore the op on of conserva on therapy, since the likelihood of any residual disease will be low. It should also be clarified that mul centricity does not necessarily require mastectomy.
It must be stated clearly that there are no published
randomized, prospec ve trials that have assessed the impact of breast MRI on mastectomy rates, or the impact on the recurrence rates or mortality. The long‐term determina on of this controversy will only come from controlled studies with long‐term follow‐up. Un l that me, MRI should be used in the context of staging and improved pathologic confirma on of local regional disease. Treatment plans in tumor boards can be discussed and implemented with be er knowledge of the pa ent’s disease extent and the treatment needed.
Neoadjuvant Chemotherapy Follow‐Up
Neoadjuvant chemotherapy has been increasingly used over the past several years for pa ents with locally advanced breast cancer (LABC). LABC typically refers to breast cancer lesions that are larger than 5 cm with or without spread to lymph nodes. The primary advantage of neoadjuvant chemotherapy is to reduce the size of the overall tumor burden. This allows for a higher percentage of pa ents to undergo breast conserva on therapy, while s ll offering significant reduc on in local recurrence rates and improved overall survival.33,34
Figure 12. Good response to neoadjuvant chemotherapy. Color‐coded post‐contrast MR images pre (A) and post (B) treatment reveal markedly decreased enhancement of the mass within the inner, posterior right breast.
Figure 13. Good response to neoadjuvant chemotherapy. Color‐coded post‐contrast MR images pre (A) and post (B) treatment reveal markedly decreased rim‐enhancement of the mass within the mid, anterior right breast, as well as the mul centric masses in the le breast.
B B
A A

J Am Osteopath Coll Radiol 2013; Vol. 2, Issue 1 Page 11
Indica ons Breast MR , Walters et al.
Diagnos c imaging is performed to monitor the tumor response to chemotherapy as early as possible and to iden fy any residual tumor. Informa on regarding tumor response during the early stages of neoadjuvant chemotherapy is useful for treatment op miza on. Tumor size may not necessarily decrease immediately in the early phase of treatment; therefore, evalua on of metabolic response becomes important. PET scanning and MRI have established roles in the early assessment of metabolic “func onal” response. MRI demonstrates a posi ve response to chemotherapy as a decrease in the enhancement characteris cs of the tumor (Figures 12 and 13). The enhancement curve changes and typically fla ens with a diminished wash‐out pa ern. Wash‐in changes occur as well; the wash‐in will be slower. A decrease in tumor size typically occurs later.35 MR Spectroscopy and diffusion‐weighted (DWI) MRI have been shown to help evaluate “responders” versus “non‐responders” as early as 24 hours a er the first cycle of chemotherapy. DWI detects cytotoxic effects of the chemotherapy by the change in the free inters al water diffusion rates. There are standard protocols for DWI and ADC mapping; the literature provides sugges ons for protocols and visual and numerical references. As protocols become standardized and controlled studies are performed, DWI and ADC may become standard in the evalua on for ini al response to chemotherapy.36
A er neoadjuvant chemotherapy, MRI is o en used to evaluate for any residual tumor. A recent ACRIN study (Protocol 6657) concluded that tumor response to chemotherapy as measured volumetrically by MRI was a much stronger and early predictor of pathologic response than clinical or tumor diameter. Several studies have demonstrated similar findings, indica ng that MRI is superior to conven onal mammography, US, and clinical exam.37,38 However, MRI correla on with tumor response is not 100%. It has been shown in some cases, par cularly with chemotherapeu c agents that demonstrate an vascular effects, that residual vital tumor may be iden fied in up to 30% of pa ents whose MRI showed no residual abnormal enhancement. The accuracy of MRI in post‐neoadjuvant chemotherapy evalua on also appears to vary with tumor subtype. It appears to be more accurate in ER‐/HER2+ and triple nega ve and less accurate in luminal tumors.39,40
Problem Solving
MRI can be used for problem solving in clinical scenarios such as discordant pathology results (Figures 14 and 15), markedly dense breast ssue with mul ple palpable lumps (Figure 16), or complex mammographic findings (Figure 17). MRI is also useful in cases with equivocal or inconclusive findings on mammograms or US. Pa ents who have undergone breast conserva on therapy may benefit from MRI if there is clinical concern of recurrent tumor versus developing scar ssue.
If there is a single abnormality on either US or mammogram, then US‐guided or stereotac c biopsy is more efficient. These two biopsy techniques are readily available, rela vely safe, easy to perform, and provide a histologic diagnosis.
In the pa ent with mul ple areas of asymmetry on a mammogram (without calcifica on) and no US abnormality; a mammographic abnormality seen only on one view; or for the pa ent with mul ple round, smooth masses that are equivocal on mammogram and US (i.e. breast cancer vs. mul ple sclero c fibroadenomas or mul ple complex cysts), MRI has a very high nega ve predic ve value (NPV). Some ins tu ons may put these pa ents in short‐term 6 month follow‐up, Bi‐Rads 3, diagnosis; however, rather than short‐term follow‐up or biopsy, MRI may also be considered. A 3‐year consecu ve study recently reported that breast MRI should be used in the diagnos c work‐up of non‐calcified Bi‐Rads 3 lesions. It was stated that malignancy is ruled out with a very high level of confidence in the majority of pa ents, thus avoiding invasive diagnos c procedures.41
Abnormal nipple discharge is most o en caused by benign e ologies, such as ductal ectasia or solitary or mul ple papillomas.42 Mammogram and US are performed ini ally to evaluate for the underlying cause and to rule out associated or causa ve breast cancer. Mammography and US are complimentary in evalua ng abnormal nipple discharge. However, in the majority of cases, both exams will o en be normal. Galactography may be performed and can be helpful; however, o en mes (up to 10% of cases) a galactogram cannot be performed due to technical reasons (i.e. intermi ent discharge, discharge from more than one orifice, etc). Also, the diagnos c informa on obtained with a galactogram is limited.

Page 12 J Am Osteopath Coll Radiol 2013; Vol. 2, Issue 1
Indica ons Breast MR, Walters et al.
Figure 14. Problem solving with discordant results. Bilateral CC views (compressed and magnified on the le ) (A) demonstrate suspicious calcifica ons within the outer, posterior le breast, as well as a mass in the posterior right breast. Right breast US (B) reveals a suspicious, lobulated, hypoechoic mass with posterior shadowing. Le breast biopsy demonstrated invasive ductal carcinoma. Right breast US‐guided biopsy demonstrated sclerosing adenosis, which was felt to be discordant with the imaging findings. Post‐contrast color‐coded MR image (C) reveals extensive tumor in the le breast and findings highly sugges ve of malignancy (abnormal rapid enhancement as well as irregular margins) on the right. MRI‐guided right breast biopsy revealed infiltra ng carcinoma with apocrine features.
Figure 15. Problem solving with discordant results. Ini al bilateral MLO analog images from 6 months earlier (A) are normal. Follow‐up MLO (B) and CC (C) digital images of the le breast demonstrate an area of spicula on (best seen on the MLO view) underlying the palpable marker. Le breast US (D) reveals an ill‐defined area of low level echoes. Biopsy was performed with US guidance and the pathology results were fibrosis and chronic inflamma on, which was felt to be discordant. Post‐contrast MR images demonstrates two irregular suspicious enhancing masses in the le breast (E), as well as a very large enhancing mass in the inferior le lateral axilla (F). Biopsy under MR guidance revealed infiltra ng ductal carcinoma with axillary metastasis.
A
C B
A C B
E
F
D

J Am Osteopath Coll Radiol 2013; Vol. 2, Issue 1 Page 13
Indica ons Breast MR , Walters et al.
Figure 16. Young woman with dense breast ssue and palpable mass on the right. MLO (A) and CC (B) views demonstrate a mass in the mid, posterior right breast. US (C) with biopsy revealed mucinous carcinoma. Post‐contrast MR image (D) is beneficial in determining size and extent of tumor, especially in the se ng of markedly dense breast ssue and difficult US and physical exams.
Figure 17. Problem solving with complex mammogram. Bilateral MLO views (A) reveal numerous silicone injec on granulomas, greatly reducing the sensi vity of mammography. Post‐contrast color‐coded MR image (B) demonstrates normal enhancement of underlying breast ssue. There may be normal rim enhancement of some of
the silicone granulomas.
A
A
C
B
D
B

Page 14 J Am Osteopath Coll Radiol 2013; Vol. 2, Issue 1
Indica ons Breast MR, Walters et al.
Sensi vity for detec on of a malignant lesion has been reported as very low (0‐55%).43 MRI can help detect intraductal lesions not seen on mammogram and/or US and allows for localiza on of the lesion (Figure 18); subsequent image‐guided biopsy may be performed.44
Axillary Adenopathy With Unknown Primary
Few women diagnosed with breast cancer ini ally present with metasta c axillary adenopathy. Historically, mastectomy was the treatment of choice in a pa ent with adenocarcinoma metastasis to the axillary lymph nodes in which the clinical exam, conven onal mammogram, and/or US were unable to detect an abnormality, as it was usually thought to originate from a primary breast cancer in the ipsilateral breast. MRI can detect the primary tumor in up to 70% of these pa ents (Figure 19).45,46 This effec vely changes their staging from T0 (unknown primary) to a defined TNM classifica on. The pa ent can then undergo more appropriate and focused surgical and oncologic therapy.
Due to the nega ve predic ve value of MRI in the detec on of invasive breast cancer, a nega ve MRI can be used to suggest that a mastectomy is not needed. Some oncologists advocate the use of radia on
therapy alone in women with a nega ve MRI.47
Ongoing Screening Debate
Recent controversial opinions concerning the value of breast cancer screening have challenged the very basis of why we offer mammography and by extension, breast MRI.48 It is cri cal that breast imagers base their prac ce on the firm convic on that mammography ‐ and by extension MRI of the breast ‐ saves lives. Nearly 20% of cancers which are detected with screening mammograms are found in women 40‐50 years old. Recent nega ve opinions have been the products of retrospec ve analysis by physicians who do not directly treat or diagnose breast cancer. The mantra that “early detec on save lives” is s ll as true as ever before. Breast MRI allows very early detec on of cancers in women who are at high risk. Breast MRI also allows for a less invasive means of follow‐up for those women at moderate risk. It is important to support prospec ve studies related to breast cancer detec on while we con nue to offer the safest means possible to detect and manage breast cancer in our pa ents.
Figure 18. Le ‐sided nipple discharge. MLO and CC views of the le breast (A) are normal, as was ini al US (not shown). Post‐contrast subtrac on MR image (B) shows abnormal ductal enhancement within the le breast at the 4 o’clock posi on. Second look US (C) demonstrates low level echoes, sugges ng an intraductal mass. Biopsy demonstrated a papillary lesion, which was surgically excised.
A B
C
D

J Am Osteopath Coll Radiol 2013; Vol. 2, Issue 1 Page 15
Indica ons Breast MR , Walters et al.
Summary
In summary, breast MRI has proven to be a valuable tool in the diagnosis, work‐up, and management of breast cancer. Common indica ons include screening for breast cancer in select high‐risk pa ents, problem solving in cases of dense breast ssue or equivocal or discordant findings on mammogram or US, evalua on for mul centricity or bilaterality of a known cancer, determining the efficacy of neoadjuvant chemotherapy, differen a on of scar ssue versus recurrent tumor, and evalua on of axillary adenopathy with an unknown primary. The clinical indica ons will likely con nue to expand as clinical trials demonstrate addi onal benefits of MRI in breast imaging. When used in conjunc on with mammogram and US, this useful tool will assist in decreasing morbidity and mortality associated with breast cancer.
Figure 19. Axillary adenopathy with unknown primary. Bilateral MLO views performed at an outside ins tu on (A) were read as benign and unchanged from an exam two years prior. Pa ent felt a mass in her right underarm one week a er the mammogram. A surgeon performed a biopsy in his office, and the pathology came back as cancer. Post‐contrast MR images demonstrate a mass far lateral posterior right breast at the 7 o’clock posi on with abnormal enhancement and abnormal morphology (B), as well as an enlarged right axillary lymph node (C) which was previously biopsied. MRI‐guided biopsy demonstrated invasive lobular carcinoma.

Page 16 J Am Osteopath Coll Radiol 2013; Vol. 2, Issue 1
Indica ons Breast MR, Walters et al.
References
1. American Cancer Society. Detailed Guide: Breast Cancer What Are the Key Sta s cs for Breast Cancer?. AmericanCancer Society Cancer Resource Informa on. h p://www.cancer.org
2. ACR Breast Magne c Resonance Imaging Accredita onProgram Requirements.
3. Tsushima Y, Takahashi‐Taketomi A, Endo K. Magne cresonance (MR) differen al diagnosis of breast tumors usingapparent diffusion coefficient (ADC) on 1.5T. Journal ofMagne c Resonance Imaging: JMRI 2009;30(2):249‐255.
4. Bedeil, Falcini F, Sanna PA, et al. Atypical ductal hyperplasiaof the breast: The controversial management of a borderlinelesion: experience of 47 cases diagnosed at vacuum‐assistedbiopsy. Breast 2006; 15(2): 196‐202.
5. Chuba PJ, Hamre MR, Yap J, et al. Bilateral risk for subsequentbreast cancer a er lobular carcinoma‐in‐situ: analysis ofsurveillance, epidemiology, and end results data. J Clin Oncol2005;23:5534‐5541.
6. Ford D, Easton DF, Bishop DT, et al. Risks of cancer in BRCA 1‐muta on carriers. Breast Cancer Linkage Consor um. Lancet1994;343:692‐695.
7. Saslow D, Boetes, C, Burke W, et al. American Cancer SocietyGuidelines for Breast Screening with MRI as an Adjunct toMammography. CA Cancer J Clin 2007;57:75‐89.
8. Hoskins KF, Stopfer JE, Calzone KA, et al. Assessment andcounseling for women with a family history of breast cancer: aguide for clinicians. JAMA 1995 ;273:577 ‐585.
9. Kriege M, Brekelmans CT, Boetes C, et al. Efficacy of MRI andmammography for breast‐cancer screening in women with afamilial or gene c predisposi on. N Engl J Med 2004;351:427‐437.
10. Kuhl CK, Schrading S, Leutner CK, et al. Mammography,breast ultrasound, and magne c resonance imaging forsurveillance of women at high gene c risk for breast cancer.J Clin Oncol 2005;23:8469‐8876.
11. Berg WA, Gu erriz L, Ness Aiver MS, et al. Diagnos c accuracyof mammography, clinical examina on, US, and MR imagingin preopera ve assessment of breast cancer. Radiology.2004;233:830‐849.
12. Vachon CM, van Gils CH, Sellers TA, et al. Mammographicdensity, breast cancer risk and risk predic on. Breast Cancer Res 2007;9:217.
13. Carney PA, Migliore DL, Yankaskas B, et al. Individual andcombined effects of age, breast density, and hormonereplacement therapy use on the accuracy of screeningmammography. Ann Intern Med 2003;138:168‐175.
14. Na onal Cancer Ins tute, Breast Cancer SurveillanceConsor um. Performance measures for 1,960,150 ScreeningMammography Examina ons from 2002 to 2006 by Age &Time (Months) Since Prior Mammography – based on BCBSdata as of 2009. www.cancer.org
15. Lord SJ, Lei W, Cra P, et al.: A systema c review of theeffec veness of magne c resonance imaging (MRI) as anaddi on to mammography and ultrasound in screening youngwomen at high risk of breast cancer. Eur J Cancer 2007; 43(13): 1905‐17.
16. Lehman CD, Gatsonis C, Kuhl CK, et al. MRI Evalua on of theContralateral Breast in Women with Recently DiagnosedBreast Cancer. N Engl J Med 2007;356:1295‐1303.
17. Hwang ES, Kinkel K, Esserman LI, et al. Magne c resonanceimaging in pa ents diagnosed with ductal‐carcinoma‐in‐situ:Value in the diagnosis of residual disease, occult invasion andmul centricity. Ann Surg Oncol. 2003;10:381‐388.
18. Sardanelli F, Giusseppe GM, Panizza P, et al. Sensi vity ofMRI Versus Mammography for Detec ng Foci of Mul focal,Mul centric Breast Cancer in Fa y and Dense Breasts Usingthe Whole‐Breast Pathologic Examina on as a Gold Standard.AJR 2004; 183:1149‐1157.
19. Houssami N, Cia o S, Macaskill P, et al. Accuracy and surgicalimpact of magne c resonance imaging in breast cancerstaging: systema c review and meta‐analysis in detec on ofmul focal and mul centric cancer. J Clin Oncol 2008;26:3248‐3258.
20. Berg WA, Gu errez L, Ness Aiver MS, et al. Diagnos caccuracy of mammography, clinical examina on, US, and MRimaging in preopera ve assessment of breast cancer.Radiology. 2004;233:830‐849.
21. Bedrosian I, Mick R, Orel SG, et al. Changes in the surgicalmanagement of pa ents with breast carcinoma based on preopera ve magne c resonance imaging. Cancer.2003;98:468‐473.
22. Lehman CD, Gatsonis C, Kuhl CK, et al. MRI evalua on of thecontralateral breast in women with recently diagnosed breastcancer. N Engl J Med. 2007;356:1295‐1303.
23. Samant RS, Olivo o IA, Jackson JS, et al. Diagnosis ofmetachronous contralateral breast cancer. Breast J2001;7:405‐410.
24. VanGoethem M, Schelfout K, Kersschot E, et al. Enhancingarea surrounding breast carcinoma on MR mammography:Comparison with pathological examina on. Eur Radiol.2004;14:1363‐1370.
25. Schnall M. MRI imaging of cancer extent: is there clinicalrelevance? Magn Reson Imaging Clin N Am 2006; 14:379‐381.
26. Turnbull L, Brown S, Harvey I, et al. Compara ve effec veness of MRI in breast cancer (COMICE) trial: arandomized controlled trial. Lancet 2010; 375:563‐571.
27. Kuhl CK, Schrading S, Bieling HB, et al. MRI for diagnosis ofpure ductal carcinoma in situ: a prospec ve observa onalstudy. Lancet 2007;370:485‐492.

J Am Osteopath Coll Radiol 2013; Vol. 2, Issue 1 Page 17
Indica ons Breast MR , Walters et al.
28. Bilimoria KY, Cambic A, Hansen NM, et al. Evalua ng theimpact of preopera ve breast magne c resonance imaging onthe surgical management of newly diagnosed breast cancers.Arch Surg 2007;142:441‐445; discussion 445‐447.
29. Jatoil, Proschan MA. Randomized trials of breast‐conservingtherapy versus mastectomy for primary breast cancer: apooled analysis of updated results. Am J Clin Oncol2005;28:289‐294.
30. Poggi MM, Danforth DN, Sciuto LC, et al. Eighteen‐yearresults in the treatment of early breast carcinoma withmastectomy versus breast conserva on therapy: the Na onalCancer Ins tute randomized trial. Cancer 2003;98:697‐702.
31. Doyle T, Schultz DJ, Peters C, et al. Long‐term results of localrecurrence a er breast conserva on treatment for invasivebreast cancer. Int J Radiat Oncol Biol Phys 2001;51:74‐80.
32. vanDongen JA, Voogd AC, Fen man IS, et al. Long‐termresults of a randomized trial comparing breast‐conservingtherapy with mastectomy: European Organiza on forResearch and Treatment of Cancer 10801 trial. J Natl Cancer Inst 2000;92:1143‐1150.
33. Bonadonna G, Valagussa P. Primary chemotherapy inoperable breast cancer. Semin Ocol 1996;23:464‐74.
34. Shin HJ, Kim HH, Ahn, JH, et al. Comparison ofmammography, sonography, MRI and clinical examina on inpa ents with locally advanced or inflammatory breast cancerwho underwent neoadjuvant chemotherapy. The Bri shJournal of Radiology 2011;84:612‐620.
35. El Khoury C, Servois V, Thibault F, et al. MR quan fica on ofthe washout changes in breast tumors under preopera vechemotherapy: feasibility and preliminary results. Am JRoentgenol 2005;184:149‐1504.
36. Woodhams R, Ramadan S, Stanwell P, et al. Diffusion‐weighted imaging of the breast: Principles and clinicalapplica ons. Radiographics 2011;31:1059‐1084.
37. Hylton N, Blume C, Gatsonis R, et al. MRI tumor volume forpredic ng response to neoadjuvant chemotherapy in locallyadvanced breast cancer: Findings from ACRIN 6657/CALGB150007. Abstracts presented at the 2009 ASCO AnnualMee ng. Cita on: J Clin Oncol 27:15s, 2009 (supple; abstr529).
38. Yeh E, Slanetz P, Kopans DB, et al. Prospec ve comparison ofmammography, sonography, and MRI in pa ents undergoingneoadjuvant chemotherapy for palpable breast cancer. Am JRoentgenol 2005;184:868‐877.
39. Denis F, Desbiez‐Bourcier AV, Chapiron C, et al. Contrastenhanced magne c resonance imaging underes matesresidual disease following neoadjuvant docetaxel basedchemotherapy for breast cancer. Eur J Surg Oncol2004;30:1069‐1076.
40. McGuire KP, Toro‐Burguete J, Dang H, et al. MRI staging a erneoadjuvant chemotherapy for breast caner: does tumorbiology affect accuracy? Ann Surg Oncol 2011;18;3149‐54.
41. Dorrius MD, Pijnappel RM, Sijens PE, et al. The nega vepredic ve value of breast Magne c Resonance Imaging in thenoncalcified BIRADS 3 lesions. Eur J Radiol 2012;81:209‐213.
42. Cabiolglu N, Hunt KK, Singletary SE, et al. Surgical decisionmaking and factors determining a diagnosis of breastcarcinoma in women presen ng with nipple discharge. J AmColl Surg 2003;196:354‐364.
43. Dinkel HP, Trusen A, Gassel AM, et al. Predic ve value ofgalactorgraphic pa erns for benign and malignant neoplasmsof the breast in pa ents with nipple discharge. Br J Radiol2000;73:706‐714.
44. Daniel BL, Gardner RW, Birdwell RL, et al. Magne cresonance imaging of intraductal papilloma of the breast.Magn Reson Imaging 2003;21:887‐892.
45. Olson JA Jr, Morris EA, Van Zee KJ, et al. Magne c resonanceimaging facilitates breast conserva on for occult breastcancer. Ann Surg Oncol 2000;7:411‐415.
46. De Bresser J, de Vos B, van der Ent F, Hulsewe’ K. Breast MRIin clinically and mammographically occult breast cancerpresen ng with an axillary metastasis: a systema c review.Eur J Surg Oncol 2010;36:114.
47. Masinghe SP, Faluyi OO, Kerr GR, et al. Breast radiotherapyfor occult breast cancer with axillary nodal metastases – doesit reduce the local recurrence rate and increase overallsurvival? Clin Oncol (R Coll Radiol) 2011;23:95.
48. Hendrick RE, Helvie MA. Mammography screening: a newes mate of number needed to screen to prevent one breastcancer death. Am J Roentgenol 2012; 198: 723‐728.
Recommended

















