1Akande OW, et al. BMJ Global Health 2021;6:e007076. doi:10.1136/bmjgh-2021-007076
Epidemiological comparison of the first and second waves of the COVID- 19 pandemic in Nigeria, February 2020–April 2021
Oluwatosin Wuraola Akande ,1,2 Kelly Osezele Elimian ,1,2,3 Ehimario Igumbor ,2,4,5 Lauryn Dunkwu,6 Chijioke Kaduru,2,7 Olubunmi Omowunmi Olopha,1,2 Dabri Olohije Ohanu,2,4 Lilian Nwozor,1,2 Emmanuel Agogo,2,8 Olusola Aruna,9 Muhammad Shakir Balogun,10 Olaolu Aderinola,11 Anthony Ahumibe,12 Chinedu Arinze,13 Sikiru Olanrewaju Badaru,1 William Nwachukwu,13 Augustine Olajide Dada,10 Cyril Erameh,14 Khadeejah Hamza,15 Tarik Benjamin Mohammed,4 Nnaemeka Ndodo,12 Celestina Obiekea,12 Chinenye Ofoegbunam,13 Oladipo Ogunbode,1 Cornelius Ohonsi,1,2 Ekaete Alice Tobin ,14 Rimamdeyati Yashe,13 Afolabi Adekaiyaoja,6 Michael C. Asuzu,2,16 Rosemary Ajuma Audu,2,17 Muhammad Bashir Bello,2,18 Shaibu Oricha Bello,2,19 Yusuf Yahaya Deeni,2,20,21 Yahya Disu,1 Gbenga Joseph,11 Chidiebere Ezeokafor,2,22 Zaiyad Garba Habib,2,23 Christian Ibeh,2,24 Ifeanyi Franklin Ike,25 Emem Iwara,2,26 Rejoice Kudirat Luka- Lawal,11 Geoffrey Namara,27 Tochi Okwor,1,2 Lois Olajide,13 Oluwafunke Olufemi Ilesanmi,2,27 Solomon Omonigho,28 Ferdinand Oyiri,13 Koubagnine Takpa,2,29 Nkem Usha Ugbogulu,13 Priscilla Ibekwe,4 John Oladejo,11 Elsie Ilori,13 Chinwe Lucia Ochu ,1,2 Chikwe Ihekweazu2,4
Original research
To cite: Akande OW, Elimian KO, Igumbor E, et al. Epidemiological comparison of the first and second waves of the COVID- 19 pandemic in Nigeria, February 2020–April 2021. BMJ Global Health 2021;6:e007076. doi:10.1136/bmjgh-2021-007076
Handling editor Senjuti Saha
► Additional supplemental material is published online only. To view, please visit the journal online (http:// dx. doi. org/ 10. 1136/ bmjgh- 2021- 007076).
Received 3 August 2021Accepted 24 October 2021
For numbered affiliations see end of article.
Correspondence toDr Oluwatosin Wuraola Akande; akande. wuraola@ gmail. com
© Author(s) (or their employer(s)) 2021. Re- use permitted under CC BY- NC. No commercial re- use. See rights and permissions. Published by BMJ.
ABSTRACTBackground With reports of surges in COVID- 19 case numbers across over 50 countries, country- level epidemiological analysis is required to inform context- appropriate response strategies for containment and mitigation of the outbreak. We aimed to compare the epidemiological features of the first and second waves of COVID- 19 in Nigeria.Methods We conducted a retrospective analysis of the Surveillance Outbreak Response Management and Analysis System data of the first and second epidemiological waves, which were between 27 February and 24 October 2020, and 25 October 2020 to 3 April 2021, respectively. Descriptive statistical measures including frequencies and percentages, test positivity rate (TPR), cumulative incidence (CI) and case fatality rates (CFRs) were compared. A p value of <0.05 was considered statistically significant. All statistical analyses were carried out in STATA V.13.Results There were 802 143 tests recorded during the study period (362 550 and 439 593 in the first and second waves, respectively). Of these, 66 121 (18.2%) and 91 644 (20.8%) tested positive in the first and second waves, respectively. There was a 21.3% increase in the number of tests conducted in the second wave with TPR increasing by 14.3%. CI during the first and second waves were 30.3/100 000 and 42.0/100 000 respectively. During the
second wave, confirmed COVID- 19 cases increased among females and people 30 years old or younger and decreased among urban residents and individuals with travel history within 14 days of sample collection (p value <0.001). Most confirmed cases were asymptomatic at diagnosis during both waves: 74.9% in the first wave; 79.7% in the second wave. CFR decreased during the second wave (0.7%) compared with the first wave (1.8%).
Key questions
What is already known? ► Globally, there have been reports of the resurgence of COVID- 19 cases in waves. In Africa, some coun-tries have reported second and even third waves of COVID- 19 cases. A country- level descriptive ep-idemiology of COVID- 19 cases between February 2020 and June 2020 in Nigeria has been published. A continent- level analysis of the first and second waves in Africa reported a larger and more severe second wave. The study underscored the need for country- level analyses to inform the implementation of country- specific interventions to mitigate the out-break. To our knowledge, there is no country- level analysis comparing the epidemiological features of the first and second waves in Nigeria.
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from
on F
ebruary 5, 2022 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2021-007076 on 18 Novem
ber 2021. Dow
nloaded from
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from
on F
ebruary 5, 2022 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2021-007076 on 18 Novem
ber 2021. Dow
nloaded from
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from
on F
ebruary 5, 2022 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2021-007076 on 18 Novem
ber 2021. Dow
nloaded from
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from
on F
ebruary 5, 2022 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2021-007076 on 18 Novem
ber 2021. Dow
nloaded from
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from
on F
ebruary 5, 2022 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2021-007076 on 18 Novem
ber 2021. Dow
nloaded from
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from
on F
ebruary 5, 2022 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2021-007076 on 18 Novem
ber 2021. Dow
nloaded from
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from
on F
ebruary 5, 2022 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2021-007076 on 18 Novem
ber 2021. Dow
nloaded from
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from
on F
ebruary 5, 2022 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2021-007076 on 18 Novem
ber 2021. Dow
nloaded from
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from
on F
ebruary 5, 2022 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2021-007076 on 18 Novem
ber 2021. Dow
nloaded from
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from
on F
ebruary 5, 2022 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2021-007076 on 18 Novem
ber 2021. Dow
nloaded from
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from
on F
ebruary 5, 2022 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2021-007076 on 18 Novem
ber 2021. Dow
nloaded from
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from
on F
ebruary 5, 2022 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2021-007076 on 18 Novem
ber 2021. Dow
nloaded from

2 Akande OW, et al. BMJ Global Health 2021;6:e007076. doi:10.1136/bmjgh-2021-007076
BMJ Global Health
Conclusion Nigeria experienced a larger but less severe second wave of COVID- 19. Continued implementation of public health and social measures is needed to mitigate the resurgence of another wave.
INTRODUCTIONThe emergence of the COVID- 19, caused by the SARS- CoV- 2 was first identified in Wuhan, China, in December 2019. It has arguably been one of the biggest threats to global health security in the 21st century. Following the ‘alarming levels of spread and severity, and by the alarming levels of inaction’, the outbreak was declared a pandemic by the director- general of the WHO on 11 March 2020.1
The index case of the disease in Nigeria was recorded on the 27 February 2020.2 Within 5 months (by the 7 July 2020), all 36 states and the Federal Capital Terri-tory (FCT) had reported at least a case of the disease, with a total number of 29 789 cases and 669 deaths.3 The Federal Government of Nigeria, through the Presidential Task Force on COVID- 19 (now the Presidential Steering Committee on COVID- 19) and the Nigeria Centre for Disease Control (NCDC), the national public health institute, are leading and coordinating response activities to the pandemic.4 5
Implementation of outbreak preparedness interven-tions commenced in Nigeria, before the index case.6 Following the report of the index case, containment and subsequently, strategies to mitigate against the impact of the outbreak on health, community and economic systems were deployed at different phases during the pandemic.6 More recently, the country began the roll- out of COVID- 19 vaccines on 16 March 2021, and by 9 April
2021, all states including the FCT had commenced vacci-nation.7 The roll out of vaccines prioritised healthcare workers (HCWs), support staff, first responders, front-line workers and strategic leaders.8 Global vaccine ineq-uity has seen Nigeria secure just about 4 million doses of COVID- 19 vaccines through the COVAX facility, with only approximately 2% of the population vaccinated by 30 June 2021.9 10
Despite the increase in COVID- 19 testing capacity across the country since the beginning of the pandemic, the testing rate remains relatively low compared with other African countries. As of 22 June 2021, the number of tests in Nigeria, the most populous country on the African continent, was 11 per 1000 population.11 In comparison, other African countries such as South Africa, Ghana, Kenya and Uganda had tests per 1000 population of 212, 39, 31 and 27, respectively.11 Concerns over the low testing rates underpinned implementation of the population- based serosurveys conducted across some states in the country to estimate the true burden of infection.12 Repeated sero- surveillance surveys that are representative of the country are desirable but can be expensive and logistically challenging, largely leading to ongoing reliance on routine surveillance data.
Real- time epidemiological information for routine surveillance of COVID- 19 cases across all states in Nigeria, including the FCT, is captured on the Surveillance Outbreak Response Management and Analysis System (SORMAS). As of 15 July 2021, 2 362 757 samples had been tested, 1 68 916 cases had been confirmed (7.15% test positivity rate) and 2138 deaths had been reported among the confirmed (1.27% case fatality rate (CFR)).13
Although there is no formal epidemiological defini-tion of a wave of infection, it has been characterised as ‘a rising number of sick individuals, a defined peak and then a decline’14–16; this will be the working definition of a wave of infection for this paper. It is not unexpected for waves of infections to occur during pandemics of viral origin. Several countries have reported second waves of the COVID- 19 pandemic, and some countries including South Korea, Spain, Uganda and Zambia have described a third wave.17–21
On the continental level, African countries had expe-rienced two waves of the pandemic between the 14 February 2020 (when the first case on the continent was reported) and 31 December 2020, with a significantly higher number of cases in the second wave.22 A descrip-tive analysis of COVID- 19 epidemiological data of African countries found the peak of the first wave to be in July 2020, with a mean daily number of new cases of 18 273.22 By December 2020, almost three- quarters of countries in the region were experiencing or had experienced a second wave of infection, with a mean daily number of new cases of 23 790.
Nigeria experienced a gradual increase in the number of confirmed COVID- 19 cases from epidemiological week 9 of 2020 (23–29 February – when the index case was reported), peaked at epidemiological week 26 of
Key questions
What are the new findings? ► Nigeria reported a larger but less severe second wave of COVID- 19, with a notable increase in testing capacity in the second wave. Though there was an increase in test positivity rate and cumula-tive incidence, there was a decrease in the case fatality rate during the second wave, compared with the first wave. During the sec-ond wave, there was an increase in cases among the younger and female demographics. Mortality was highest among the elderly in both waves, with a significant increase in the mean age at death during the second wave.
What do the new findings imply? ► This retrospective analysis provides a better understanding of the epidemiological features of the first and second waves of COVID- 19 in Nigeria. The difference in the sociodemographic and clinical fea-tures of cases in both waves are informing the implementation of targeted country- level initiatives for containment and mitigation of the impact of the pandemic on health, community and socioeco-nomic systems. In the face of a possible third wave, the findings form the basis of our proposals for the sustenance of COVID- 19 public health and social measures and a prompt scale- up of vaccination.
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from

Akande OW, et al. BMJ Global Health 2021;6:e007076. doi:10.1136/bmjgh-2021-007076 3
BMJ Global Health
2020 (21–27 June) and then experienced a gradual decrease until epidemiological week 43 of 2020 (18–24 October). As from epidemiological week 44 of 2020 (25–31 October), there was another steady increase in the number of confirmed cases, peaking at epidemiolog-ical week 3 of 2021 (17–23 January). A gradual decline of cases has since been seen up until epidemiological week 15 of 2021 (11–17 April). Based on these findings, we assume that Nigeria experienced its first wave of COVID- 19 infection between February 2020 and October 2020, and the second wave, which is still ongoing started in November 2020.
Epidemiological and clinical analyses of nationwide cases within the first wave (February–June 2020) using the SORMAS database have been published.2 The study found the cumulative incidence (CI) and CFR of the disease to be 5.6 per 100 000 population and 2.8%, respec-tively. The majority of confirmed cases were among males (65.8%) and those between 31 and 40 years old (25.5%). Two- thirds of cases were asymptomatic at diagnosis, and mortality was highest among males (79.0%) and those between 61 and 70 years old (26.6%).
There is a need for country- level analysis to further understand the epidemiology of this novel virus to aid informed decision making in controlling the epidemic. In addition to giving an update on the descriptive epide-miology of COVID- 19 cases between February 2020 and June 2020,2 this study aimed to compare the epidemio-logical features of the first and second waves of COVID- 19 in Nigeria between 27 February 2020 and 3 April 2021.
METHODSStudy design, period and settingsWe conducted a retrospective analysis of Nigeria’s surveil-lance and laboratory data between 27 February 2020 and 3 April 2021. Nigeria is made up of 36 states and the FCT, which are divided into six geopolitical zones: North- East (Adamawa, Bauchi, Borno, Gombe, Taraba and Yobe), North- West (Jigawa, Kaduna, Kano, Katsina, Kebbi, Sokoto and Zamfar), North- Central (Benue, FCT, Kogi, Kwara, Nasarawa, Niger and Plateau), South- South (Akwa Ibom, Bayelsa, Cross River, Delta, Edo and Rivers) South- West (Ekiti, Lagos, Ogun, Ondo, Osun and Oyo) and South- East (Abia, Anambra, Ebonyi and Enugu Imo). During the study period, all states and the FCT actively monitored for cases, and all reported confirmed COVID- 19 cases.
Data sourceThe sole source of data for this study was from the SORMAS, an open- source real- time electronic health surveillance database for diseases of public health impor-tance that was domesticated by the NCDC in 2017.23 It is the principal digital surveillance tool used for the implementation of the Integrated Disease Surveillance and Response strategy in Nigeria. In January 2020, a COVID- 19 module was added to the SORMAS platform.
The SORMAS platform is configured on mobile devices (tablets and smartphones) and laptops for reporting surveillance and laboratory data by trained personnel. The SORMAS database is owned by NCDC and cases across the states are reported on the platform. Data are processed and stored in a central server at its headquar-ters in Abuja, Nigeria, from where it is analysed for deci-sion making and action.
Study population and data collectionThe study population was made up of persons tested for SARS- CoV- 2 infection and captured on SORMAS during the study period. Eligibility for testing was based on the NCDC case definition for a COVID- 19 suspected case.24 However, samples were also collected from contacts of confirmed cases, and those who got tested for COVID- 19 as a mandatory requirement for international travel.
Every person who got tested had a Case Investigation Form, which contained sociodemographic information, epidemiological history and clinical characteristics. Sample collection, packaging and transportation to a molecular laboratory were conducted in accordance with the NCDC guidelines.25 At least one nasal (or naso-pharyngeal) swab and one oropharyngeal swab using synthetic fibre swabs with plastic shafts were collected. Collected specimens were triple packaged and trans-ported aseptically via viral transport media, under suit-able temperature conditions (2°C–4°C) to a designated NCDC- approved laboratory.26 Real- time PCR was used for the laboratory diagnosis of COVID- 19. All confirmed COVID- 19 cases were managed according to the NCDC’s national clinical management guidelines.27 All data and sample collection and processes were performed by trained health workers.
Data management and definition of study variablesDeidentified data were retrieved from SORMAS. The first epidemiological week (hereinafter: week) was defined as the week ending on the first Saturday of January 2020; subsequent weeks however began on Sunday and ended on Saturday.28 The current study covered weeks 9–53 of 2020 and weeks 1–13 of 2021. An epidemiological wave (hereinafter: wave) was defined as the time from the start of a peak (first week with increasing numbers of cases) to the end of a peak (week with a nadir of cases before the next rise). A wave was classified as a binary variable: first wave (week 9–43 of 2020) and second wave (week 44 of 2020 to week 13 of 2021). The definitions of other covariates are available in a previous paper.2 Owing to the significant proportion of missing data, the missing indicator approach, which is simple, more efficient and ensures all participants can be included in the analysis to maintain statistical significance, was used in handling missing data.29 30
Definition of variablesThe unit of analysis in this study is a confirmed case.
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from

4 Akande OW, et al. BMJ Global Health 2021;6:e007076. doi:10.1136/bmjgh-2021-007076
BMJ Global Health
Outcome variablesThe primary outcomes for this study were test positivity rate (TPR), CI and CFR. TPR was defined as the propor-tion of all tests conducted that was positive for COVID- 19, expressed as a percentage (number of confirmed COVID- 19 cases during the study period/total COVID- 19 tests conducted during the study period × 100%). CI was defined as the ratio of COVID- 19 cases in a defined area to the estimated population of that area. Using a national average growth rate of 3.2%, CI for each reporting state was calculated using the projected Nigerian population of 2021 from the 2006 national population census and was multiplied by 100 000 to ease interpretation. CFR was defined as the proportion of persons diagnosed with COVID- 19 who died during the study period, expressed as a percentage. TPR, CI and CFR were calculated for Nigeria and for each state separately.
Exposure variablesAge was categorised using a 10- year interval scale. The residential setting of each person was categorised into rural or urban, based on their local government area of residence. Persons with at least one symptom were reclas-sified as symptomatic, while those with no symptom at the time of testing were classified as asymptomatic.
Statistical analysesCategorical variables were described using frequen-cies and percentages. Mean and SD were calculated for normally distributed data, while median and IQRs were calculated for non- normally distributed data. Pearson’s χ2 test was used to evaluate the association between sociode-mographic and clinical characteristics with the first and second waves. A similar approach was used for the assess-ment of the association between sociodemographic/clin-ical characteristics and COVID- 19 deaths in the first and second waves. A p value of <0.05 was considered statisti-cally significant. All statistical analyses were carried out in STATA V.13 (Stata Corp). The report of this study was structured in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology statement of the Equator Network (V.4).31
Patient and public involvement statementPatients were not involved in this study.
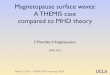
RESULTSDuring the first wave (27 February 2020–24 October 2020) and the second wave (25 October 2020–3 April 2021), 362 550 and 439 593 records, respectively, were entered into the SORMAS database, resulting in a total of 802 143 records. This is also equivalent to the total number of tests conducted during the study period with the second wave having a 21.3% increase in the number of tests. The national epi- curve showing the COVID- 19 cases during the first and second waves for the period under review is as shown in figure 1.
The COVID- 19 indicators at the national and subna-tional levels for the first and second waves are as captured in table 1. TPR increased from 18.2% in the first wave to 20.8% in the second wave, representing a 14.3% increase. Subnational disaggregation showed that states with the highest TPR during the first wave were Imo (48.0%), Abia (43.5%) and Osun (41.9%), while those with the lowest TPR were Kogi (2.9%), Katsina (4.7%) and Ekiti (5.2%). During the second wave, Oyo (44.9%), Plateau (40.7%) and Kano (40.5%) had the highest TPR, while Kogi (0%), Jigawa (6.0%) and Zamfara (6.2%) had the lowest TPR. The percentage increase in the absolute number of cases between the second and first waves in each state is as shown in figure 2. The top three states with the highest percentage increase were Taraba (83%), Anambra (82%) and Akwa- Ibom (76%). States that recorded a decrease in TPR during the second wave include Abia, Bayelsa, Borno, Delta, Ebonyi, Edo, Enugu, Jigawa, Ondo and Oyo States.
During the first wave, the CI was 30.3 per 100 000 as a national average, ranging from 0.1 per 100 000 in Kogi State to 167.6 per 100 000 in Lagos State. Corresponding figures for the second wave were 42.0 per 100 000 for the national average, ranging between 0 per 100 000 in Kogi State and 215.2 per 100 000 in Lagos State. There was a decrease in the CFR during the second wave (0.7%), compared with the first wave (1.8%) at the national level. During the first wave, the top three states with highest CFRs were Yobe (11.0%), Sokoto (11.0%) and Kebbi (8.6%). During the second wave, the top three states with the highest CFRs were Delta (2.8%), Edo (2.7%) and Katsina (2.7%). Notably, despite Lagos State having the highest CI in the country during the first and second waves, CFR was 0.9% and 0.4%, respectively.
The description of sociodemographic/clinical charac-teristics of the confirmed COVID- 19 cases and the waves in Nigeria are as shown in table 2. The mean (SD) age of those who tested positive was higher in the second wave – 33.57 (15.28) years, compared with the first wave – 37.67 (16.30) years (p value <0.001). There was a 10.09% increase in the proportion of people under the age of 30 years who got infected during the second wave, compared with the first wave. There was a statistically significant (p value <0.001) increase in the proportion of
Figure 1 Distribution of confirmed cases showing outcomes by epidemiological week.
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from

Akande OW, et al. BMJ Global Health 2021;6:e007076. doi:10.1136/bmjgh-2021-007076 5
BMJ Global Health
Tab
le 1
C
OV
ID- 1
9 in
dic
ator
s at
the
nat
iona
l and
sub
natio
nal l
evel
s fo
r th
e fir
st a
nd s
econ
d w
aves
Sta
te/r
egio
n
Po
pul
atio
n*Fi
rst
wav
eS
eco
nd w
ave
Tota
l te
sts
Per
cen
t p
osi
tive
ra
teC
ases
CI/
100
000
po
pul
atio
n
Dea
ths
fro
m
CO
VID
- 19
CFR
(%
)To
tal
test
s
Per
c en
t p
osi
tive
ra
teC
ases
CI/
100
000
po
pul
atio
n
Dea
ths
fro
m
CO
VID
- 19
CFR
(%)
Nat
iona
l21
7 97
1 54
836
2 55
018
.266
121
30.3
1221
1.80
439
593
20.8
91 6
4442
.061
10.
7
Sou
th- E
ast
A
bia
4 11
5 15
221
5843
.593
922
.89
0.9
5349
8.5
455
11.1
92.
0
A
nam
bra
6 15
5 89
216
0017
.928
64.
620
7.0
4504
35.0
1577
25.6
10.
1
E
bon
yi3
199
362
4316
27.8
1200
37.5
383.
257
3312
.068
921
.54
0.6
E
nugu
4 92
6 95
554
4024
.413
2726
.923
1.7
4787
20.1
964
19.6
40.
4
Im
o6
115
745
1280
48.0
614
10.0
142.
332
1631
.410
1116
.425
2.5
Sou
th- S
outh
A
kwa-
Ibom
6 26
0 32
226
1611
.429
74.
78
2.7
3766
32.8
1237
19.8
40.
3
B
ayel
sa2
541
682
2498
17.3
431
17.0
225.
170
256.
042
116
.66
1.4
C
ross
- Riv
er4
310
798
1358
10.6
144
3.3
117.
638
936.
725
96.
04
1.5
D
elta
6 36
9 84
910
610
17.1
1810
28.4
492.
712
576
6.3
798
12.5
222.
8
E
do
4 67
3 22
916
481
16.2
2674
57.2
121
4.5
20 6
919.
920
4843
.856
2.7
R
iver
s8
280
753
21 4
3013
.428
7234
.773
2.5
27 0
3815
.140
8749
.434
0.8
Sou
th- W
est
E
kiti
3 65
5 66
363
925.
233
39.
16
1.8
8579
6.3
540
14.8
50.
9
La
gos
14 0
09 1
2064
910
36.2
23 4
8416
7.6
221
0.9
112
921
26.7
30 1
4821
5.2
110.
0Ϯ
Ogu
n5
873
430
11 2
6618
.420
7535
.331
1.5
17 0
4314
.324
3441
.416
0.7
O
ndo
5 20
4 85
858
1928
.616
6632
.037
2.2
7370
20.5
1512
29.0
261.
7
O
sun
5 32
0 96
722
1341
.992
817
.419
2.0
4077
36.2
1475
27.7
60.
4
O
yo8
929
410
12 0
3528
.834
7238
.945
1.3
7032
44.9
3155
35.3
852.
7
Nor
th- C
entr
al
B
enue
6 38
1 98
534
4514
.851
08.
011
2.2
6459
12.3
796
12.5
121.
5
FC
T4
880
010
41 3
3115
.463
7713
0.7
951.
550
483
26.4
13 3
3127
3.2
730.
5
K
ogi
4 95
9 00
617
52.
95
0.1
00
2380
00
0-*
-*
K
war
a3
586
485
4723
22.6
1068
29.8
272.
512
459
16.4
2049
57.1
291.
4
N
asar
awa
2 81
8 37
137
7212
.948
817
.314
2.9
8200
21.5
1767
62.7
251.
4
N
iger
6 30
8 29
544
446.
327
94.
411
3.9
7170
9.1
656
10.4
60.
9
P
late
au4
615
698
20 7
5417
.836
9180
.034
0.9
13 1
7940
.753
6811
6.3
140.
3
Con
tinue
d
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from

6 Akande OW, et al. BMJ Global Health 2021;6:e007076. doi:10.1136/bmjgh-2021-007076
BMJ Global Health
Sta
te/r
egio
n
Po
pul
atio
n*Fi
rst
wav
eS
eco
nd w
ave
Tota
l te
sts
Per
cen
t p
osi
tive
ra
teC
ases
CI/
100
000
po
pul
atio
n
Dea
ths
fro
m
CO
VID
- 19
CFR
(%
)To
tal
test
s
Per
c en
t p
osi
tive
ra
teC
ases
CI/
100
000
po
pul
atio
n
Dea
ths
fro
m
CO
VID
- 19
CFR
(%)
Nor
th- E
ast
A
dam
awa
4 72
7 31
221
4312
.727
25.
819
7.0
4510
17.6
796
16.8
131.
6
B
auch
i7
468
016
7927
9.7
767
10.3
152.
087
528.
876
710
.34
0.5
B
orno
6 62
9 19
011
445
6.9
784
11.8
374.
765
708.
454
98.
30
0
G
omb
e3
658
473
12 9
287.
293
125
.429
3.1
7143
14.4
1030
28.2
151.
5
Ta
rab
a3
402
844
2035
6.5
132
3.9
53.
831
4724
.175
922
.38
1.1
Yo
be
3 75
7 94
791
09.
082
2.2
911
.029
837.
823
36.
21
0.4
Nor
th- W
est
Ji
gaw
a6
488
878
2403
13.5
325
5.0
113.
433
066.
019
73.
05
2.5
K
adun
a9
176
219
21 3
9013
.127
9630
.546
1.6
24 0
2125
.561
2266
.713
0.2
K
ano
14 7
83 5
1825
238
7.0
1757
11.9
543.
153
1340
.521
5214
.656
2.6
K
atsi
na8
761
794
20 8
224.
796
911
.126
2.7
9228
12.0
1110
12.7
80.
7
K
ebb
i4
965
722
746
12.5
931.
98
8.6
3229
11.1
357
7.2
72.
0
S
okot
o5
592
043
2602
6.3
164
2.9
1811
.029
7321
.664
111
.51
0.2
Z
amfa
ra5
066
556
895
8.8
791.
65
6.3
2488
6.2
154
3.0
31.
9
*Per
the
pro
ject
ed (b
ased
on
a na
tiona
l ave
rage
gro
wth
rat
e of
3.2
%) N
iger
ian
pop
ulat
ion
of 2
020
from
the
200
6 p
opul
atio
n ce
nsus
.C
FR, c
ase
fata
lity
rate
; CI,
cum
ulat
ive
inci
den
ce.
Tab
le 1
C
ontin
ued
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from

Akande OW, et al. BMJ Global Health 2021;6:e007076. doi:10.1136/bmjgh-2021-007076 7
BMJ Global Health
females who tested positive in the second wave (41.90%) compared with first wave (35.64%). There was a signifi-cant decrease in the proportion of infected persons who were HCWs from 7.51% during the first wave to 2.89% during the second wave (p value <0.001). Compared with the second wave, there was a decrease in the proportion of those cases who had a history of travel within 14 days of sample collection: from 3.77% to 0.98% (p value <0.001). There was also a decrease in the proportion of confirmed cases who were admitted to treatment centres during the second wave (1.36%) compared with the first wave: 10.38% (p value <0.001).
At sample collection, there was an increase in the proportion of individuals who were asymptomatic during the second wave (79.70%), compared with the first wave (74.96%, p value <0.001). The most frequently reported symptoms among those who got infected during the first wave were cough (50.79%), fever (46.66%) and sore throat (22.90%), while during the second wave, cough (43.23%), fever (40.29%) and runny nose (38.23%) were the most reported (online supplemental file 1).
The sociodemographic and clinical characteristics of patients with COVID- 19 associated deaths during the first and second waves are shown in table 3. The mean age at death from COVID- 19 infection was higher in the second wave: 60.72±17.42 years, compared with the first wave: 56.93±16.27 years (p value <0.001). There was an 8.74% increase in the proportion of females who died during the second wave, compared with the first wave (p value <0.001). During the second wave, the proportion of those who died in urban areas increased from 45.54% to 51.39% (p value 0.036). At sample collection, there was a decrease in those who were asymptomatic during the second wave (39.48%), compared with the first wave (44.84%, p value 0.028)). Cough, fever and difficulty in breathing remained the most common symptoms among those who died during both waves.
During both waves, most of the confirmed cases were asymptomatic (first wave: 74.93%, second wave: 79.7%). The most frequently reported symptoms among confirmed cases that died during the first wave were cough (50.79%), fever (46.66%) and sore throat (22.90%), while during the second wave, cough (43.23%), fever (40.29%) and runny nose (38.23%) were the most reported (online supplemental file 2).
As shown in table 4, the median time from symptom onset to time of sample collection was 2 days (0–5) and 1 day (0–3) in the first and second waves, respectively. Similarly, the time from symptom onset to presentation at a health facility decreased from 1 day (0–5) in the first wave to 0 day (0–3) s wave. Median duration in isolation remained the same in both waves (14 days). There was a decrease in the median time of hospital admission, from 15 days (10-–21) in the first wave, to <1 day in the second wave.
DISCUSSIONTo our knowledge, this is the first study comparing the epidemiological characteristics of the first and the second waves of COVID- 19 across all states (including the FCT) in Nigeria. Our study found a 21.3% increase in the number of tests conducted and a 14.3% increase in TPR during the second wave. This finding suggests that there was increased transmission of the virus. These may be attributed to an increase in sample collection and testing capacity, increased surveillance activities and reopening of the economy and social gatherings during the second wave.6 32 The testing capacity in Nigeria was gradually built over several months of the first wave, and extensive testing infrastructure was already in place at the begin-ning of the second wave.32 The findings may also poten-tially point to the role of virus variants, which have been reported to have higher transmissibility and highlight the need for strengthened genomic surveillance.33
Similarly, there was an increase in CI in the second wave, and this may also be related to the general improve-ment in testing capacity in the country. Notably, there was a wide range in CI across the states during both waves. For instance, Kogi State recorded as low as 0.1 per 100 000 and 0 per 100 000 during the first and second waves, respectively, and Lagos State reported 167.6 per 100 000 and 215.2 per 100 000 during the first and second waves, respectively. However, during the first and second waves, Kogi State tested the least number of samples in the country. This may suggest an underestimation of the CI rate and, by extension, the CFR of COVID- 19 in the state. Across geopolitical zones, a lower CI was reported in the Northern zone (especially in the North- eastern zone) of the country compared with the Southern zone. These disparities may not be unrelated to the stark differ-ence in testing rates due to varying diagnostic capacities, as well as cultural, sociopolitical and security landscapes across the states and zones.
Figure 2 Percentage increase in cases between the first and second waves.
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from

8 Akande OW, et al. BMJ Global Health 2021;6:e007076. doi:10.1136/bmjgh-2021-007076
BMJ Global Health
Table 2 Sociodemographic characteristics and clinical features of confirmed COVID- 19 cases during the two waves in Nigeria
Variable Wave 1 (n=66 237) Wave 2 (n=91 664) P value
Sociodemographic characteristics
Mean (SD) age, years (n=62 915) (n=88 435)0.2178*33.57 (15.28) 37.67 (16.30)
Age group, years <0.001†
0–4 886 (1.34) 1424 (1.55)
5–13 2395 (3.62) 3560 (3.88)
14–20 3987 (6.02) 6638 (7.24)
21–30 13 597 (20.53) 20 184 (22.02)
31–40 17 691 (26.71) 21 689 (23.67)
41–50 12 232 (18.47) 16 121 (17.59)
51–60 7596 (11.47) 10 870 (11.86)
61–70 3064 (4.63) 5091 (5.56)
71–80 1116 (1.68) 2132 (2.33)
>80 351 (0.53) 726 (0.79)
Missing 3322 (5.02) 3229 (3.50)
Sex <0.001†
Female 23 609 (35.64) 38 403 (41.90)
Male 41 434 (62.55) 52 754 (57.56)
Missing 1194 (1.80) 487 (0.53)
Residential setting <0.001†
Rural 3825 (5.77) 5192 (5.67)
Urban 25 807 (38.96) 26 510 (28.93)
Missing 36 605 (55.26) 59 942 (65.41)
Education completed <0.001†
None 949 (1.43) 911 (0.99)
Nursery 180 (0.27) 123 (0.13)
Primary 1201 (1.81) 1285 (1.40)
Secondary 5673 (8.56) 4814 (5.25)
Tertiary 15 881 (23.98) 18 449 (20.13)
Alternative (eg, Almajiranci) 3102 (4.68) 1948 (2.13)
Missing 39 251 (59.26) 64 114 (69.96)
Current occupation <0.001†
Pupil/student 4419 (6.67) 4829 (5.27)
Housewife/child 1096 (1.65) 1373 (1.50)
Trader/business 2727 (4.12) 2342 (2.56)
Farmer/miner 718 (1.08) 1007 (1.10)
Healthcare worker 4973 (7.51) 2648 (2.89)
Animal- related work 70 (0.11) 57 (0.06)
Transporter 142 (0.21) 48 (0.05)
Religious leader 127 (0.19) 99 (0.11)
Traditional leader 22 (0.03) 36 (0.04)
Other 24 294 (36.68) 48 150 (52.54)
Missing 27 649 (41.74) 31 055 (33.89)
Quarantine location <0.001†
Continued
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from

Akande OW, et al. BMJ Global Health 2021;6:e007076. doi:10.1136/bmjgh-2021-007076 9
BMJ Global Health
Fewer positive cases (a decrease by about 74%) reported a local or international travel history within 14 days of sample collection in the second wave; this may imply that this wave was largely driven by community transmission as opposed to the importation of cases. Considering that the incubation period could be as long as 14 days, the epi- curve (figure 1) supports an argument that this community transmission could have partly been driven by the yuletide, with the curve peaking in week 3 2021 for the second wave.34
During the second wave, there was a slight demo-graphic shift towards a younger population. This is similar to findings by Saito et al35 in Japan. This shift may be attributed to certain activities that majorly involved this demographic during the second wave. In March 2020, the Nigerian government ordered the closure of schools, as part of its measures to curtail the pandemic, about 3 weeks after the incidence case of the disease was reported in the country.36 By the beginning of the second wave, most schools had reopened following the Federal Government’s approval of the phased reopening of schools, subject to compliance with non pharmacuet-ical intervention (NPIs) and the conduct of regular risk assessment activities.37 38 However, there were reports of COVID- 19 outbreaks in some schools following this reopening.39 40 Following the reopening of schools, National Youth Service Corps orientation camps were also reopened.41 All Corp members underwent manda-tory COVID- 19 tests.42 At about the same period, the #ENDSARS protest against police brutality, which lasted for over 3 weeks in almost all states in Nigeria, occurred.43 Though anecdotal, the mass gathering of protesters who were majorly young people could have
been a super spreader event for the transmission of the virus. Risk communications about the virus in Nigeria focused on emphasising the need for the general public to take responsibility to limit the transmission of the virus; it also amplified the higher risks for older popu-lations and those with comorbidities.44 This has the potential to impact on risk and threat perception among young people, all that shape behaviour as the outbreak persists.44
Nigeria reported a decrease of about 61.5% in HCW infections during the second wave. This is incongruent with findings from Australia where an increase in HCW infections was recorded in the second wave.45 Though gaps still exist in facility- based surveillance activities for COVID- 19 infection among HCWs, the findings from our study may be associated with the implementation and scale- up of innovative infection prevention and control measures and the increase in the distribution of personal protective equipment across health facilities in the country.46 47
The proportion of symptomatic individuals was lower in the second wave compared with the first wave. This is similar to findings from Spain, where there was a decrease in the proportion of symptomatic cases in the second wave.18 CFR was about three times less during the second wave, with a drop from 1.8% to 0.7%. These findings may be attributed to the higher proportion of younger people who got infected during the second wave. While young people contributed more to the number of COVID- 19 cases during the second wave, there were fewer deaths among this demographic compared with older adults. Consequently, this could have led to the decrease in CFR seen during the second wave.
Variable Wave 1 (n=66 237) Wave 2 (n=91 664) P value
None 5464 (8.25) 8230 (8.98)
Formal institution 1912 (2.89) 205 (0.22)
Home 6116 (9.23) 3757 (4.10)
Missing 52 745 (79.63) 79 452 (86.70)
Travel history
No 38 425 (58.01) 30 008 (32.74)
Yes 2495 (3.77) 901 (0.98)
Missing 25 317 (38.22) 60 735 (66.27)
Hospitalisation <0.001†
No 31 197 (47.10) 49 589 (54.11)
Yes 6885 (10.39) 1250 (1.36)
Missing 28 155 (42.51) 40 805 (44.53)
Symptomatic status <0.001†
Asymptomatic 49 652 (74.96) 73 038 (79.70)
Symptomatic 16 585 (25.04) 18 606 (20.30)
*P value for t- test.†P value for χ2 test.
Table 2 Continued
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from

10 Akande OW, et al. BMJ Global Health 2021;6:e007076. doi:10.1136/bmjgh-2021-007076
BMJ Global Health
Table 3 Sociodemographic characteristics and clinical features of COVID- 19 related deaths during the two waves in Nigeria
Variable Wave 1 (n=1221) Wave 2 (n=611) P value
Sociodemographic characteristics
Mean (SD) age, years 56.93 (16.27) 60.72 (17.42) <0.0001*
(n=1149) (n=580)
Age group, years <0.001†
0–4 2 (0.16) 5 (0.82)
5–13 9 (0.74) 4 (0.65)
14–20 17 (1.39) 11 (1.80)
21–30 56 (4.59) 13 (2.13)
31–40 106 (8.68) 42 (6.87)
41–50 167 (13.68) 59 (9.66)
51–60 276 (22.60) 127 (20.79)
61–70 298 (24.41) 142 (23.24)
71–80 161 (13.19) 123 (20.13)
>80 57 (4.67) 52 (0.51)
Missing 72 (5.90) 33 (5.40)
Sex <0.001†
Female 301 (24.65) 204 (33.39)
Male 911 (74.61) 407 (66.61)
Missing 9 (0.74) 0 (0.00)
Residential setting 0.036†
Rural 78 (6.39) 28 (4.58)
Urban 556 (45.54) 314 (51.39)
Missing 587 (48.08) 269 (44.03)
Education completed <0.001†
None 20 (1.64) 7 (1.15)
Nursery – –
Primary 22 (1.80) 2 (0.33)
Secondary 142 (11.63) 44 (7.20)
Tertiary 299 (24.49) 194 (31.75)
Alternative (eg, Almajiranci) 41 (3.36) 8 (1.31)
Missing 697 (57.08) 356 (58.27)
Current occupation 0.002†
Pupil/student 12 (0.98) 1 (0.16)
Housewife/child 23 (1.88) 6 (0.98)
Trader/business 103 (8.44) 30 (4.91)
Farmer/miner 52 (4.26) 18 (2.95)
Healthcare worker 50 (4.10) 15 (2.45)
Animal- related work 3 (0.49) 1 (0.16)
Transporter 6 (0.49) 0 (0.00)
Religious leader 7 (0.57) 1 (0.16)
Traditional leader 3 (0.25) 1 (0.16)
Other 451 (36.94) 237 (38.79)
Missing 511 (41.85) 301 (49.26)
Admission to treatment centre <0.001†
No 504 (41.28) 194 (31.75)
Continued
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from

Akande OW, et al. BMJ Global Health 2021;6:e007076. doi:10.1136/bmjgh-2021-007076 11
BMJ Global Health
This study also found a decrease in the time from symptom onset to sample collection and a reduction in time from symptom onset to health facility visit. Increased risk perception with as high as 81% knowing that asymp-tomatic persons could transmit the infection, is a poten-tial driver of this increased demand for testing.18 The findings may also be related to improved health- seeking behaviour as a result of sustained risk communication activities, wider access to testing allowing prompt diag-nosis, isolation and treatment, enhancement in medical care and surveillance activities.32 48
Though there was an increase in morbidity and mortality among females in the second wave, males accounted for most of the cases reported during the first and second waves. This is congruent with results from other studies conducted in Nigeria.2 49 Galasso et al50 anal-ysed the gender differences in COVID- 19 attitudes and behaviour across eight high- income per capita countries with advanced health systems and found gender differ-ences in risk and threat perception of COVID- 19. Women were more likely to consider COVID- 19 a serious health problem and were more likely to adhere to public health and social measures (PHSMs) compared with males; however, the proportion of women who complied with PHSMs decreased during the second wave.50 There may be limited applicability in Nigeria, considering the distinct socioeconomic and sociocultural differences with the countries surveyed. The audience perception survey in Nigeria however, based on the extended parallel process model for risk communications during the second wave, did not find any substantial gender differences in the
perception of COVID- 19 and adherence to PHSMs.51 Women were almost as likely to have low threat percep-tion and low efficacy to comply with PHSMs (59%) as men (58%). The increase in morbidity and mortality during the second wave may be associated with the reopening of the economy and the general laxity in compliance with PHSMs, and other confounding factors like the presence of comorbidities and overall health status prior to infec-tion. During both waves, mortality was highest among the elderly (>60 years). Several studies have found mortality to be higher among the elderly compared with younger age groups.52 53 This may be due to the higher risk for severe disease and the increased likelihood for comor-bidities among this age group.54
Strengths and limitationsThis study presents findings from the epidemiological comparison of the first and second waves of the COVID- 19 pandemic in Nigeria based on reported cases on the SORMAS database. However, findings should be carefully interpreted considering certain limitations. A consider-able proportion of the data across the variables analysed was missing. A similar study that analysed data from the database during the first 4 months of the pandemic also reported substantial missing cases.2 Despite the imple-mentation of a data quality improvement project in April 2020 to drive data completeness of the SORMAS data-base to >90%, incomplete COVID- 19 data remain a chal-lenge, particularly at data collection points. Missing data across the variables ranged from 0.74% (sex – table 2) to 90.89% (quarantine location – table 1) and from 0.53%
Variable Wave 1 (n=1221) Wave 2 (n=611) P value
Yes 352 (28.83) 115 (18.82)
Missing 365 (29.89) 302 (49.43)
Symptomatic status 0.028†
Asymptomatic 482 (39.48) 274 (44.84)
Symptomatic 739 (60.52) 337 (55.16)
*P value for t- test.†P value for χ2 test.
Table 3 Continued
Table 4 Timeline of socioclinical variables among confirmed COVID- 19 cases
Time variable
First wave Second wave
Total cases with data (N)
Median number (IQR) of days
Total cases with data (N)
Median number (IQR) of days
Time from symptom onset to sample collection for diagnosis*
19 111 2 (0–5) 16 676 1 (0–3)
Time to health facility visit* 7275 1 (0–5) 2780 0 (0–3)
Duration in isolation 4570 14 (13–14) 539 14 (13–15)
Duration of hospital admission 4917 15 (10–21) 669 <1
Total laboratory turnaround time 61 363 0 (0–0) 87 984 <1
*Only symptomatic cases.
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from

12 Akande OW, et al. BMJ Global Health 2021;6:e007076. doi:10.1136/bmjgh-2021-007076
BMJ Global Health
(sex – table 2) to 86.70% (quarantine location – table 1) during the first and second waves, respectively. Across sociodemographic characteristics (age group, sex, resi-dential setting, education completed and current occu-pation), the average proportion of missing variables was 40.10% in the first wave and 46.60% in the second wave. Missing data may reduce the generalisability of the results to the target population and may lead to biased infer-ences. In addition, there could be a chance that some tests were carried out but not uploaded to SORMAS, thus excluding them from this analysis.
CONCLUSIONRegardless of the study limitations, this study provides country- level insight into the epidemiological character-istics of the first and second waves of COVID- 19. Nigeria reported a larger but less severe second wave of COVID- 19, with a notable increase in testing capacity in the second wave. Perhaps, the limited testing capacity during the first wave could have exaggerated the apparent increase in cases seen during the second wave. Further analysis at the subnational level could provide additional information on the drivers of COVID- 19 transmission across the various states and regions of the country. Genomic surveillance will also be helpful to provide further insights into the role of variant strains of the virus. With efforts to balance containment of COVID- 19 trans-mission and mitigation of its effects on health, commu-nity and economic systems, continued monitoring and analysis of epidemiological data is essential to implement evidence- based PHSMs. To aid the dissemination of accu-rate data to drive informed decision making, we propose the training and retraining of data collectors with close monitoring and periodic supportive supervision, in addi-tion to an improvement in the SORMAS data quality. We recommend the sustenance of COVID- 19 preventive measures and risk communication activities especially targeting the elderly who are at higher risk of mortality. We also recommend the rapid scale- up of vaccination to prevent the resurgence of another wave.
Author affiliations1Prevention Programmes & Knowledge Management, Nigeria Centre for Disease Control, Abuja, Federal Capital Territory, Nigeria2Nigeria COVID- 19 Research Coalition, Abuja, Federal Capital Territory, Nigeria3Department of Global Public Health, Karolinska Institute, Stockholm, Sweden4Office of the Director General, Nigeria Centre for Disease Control, Abuja, Federal Capital Territory, Nigeria5School of Public Health, University of the Western Cape, Bellville, South Africa6Tony Blair Institute for Global Change, Abuja, Federal Capital Territory, Nigeria7IQVIA, Abuja, Nigeria8Resolve to Save Lives, Abuja, Federal Capital Territory, Nigeria9International Health Regulations (IHR) Strengthening Project, Global Operations, UK Health Security Agency, London, UK10African Field Epidemiology Network, Abuja, Federal Capital Territory, Nigeria11Health Emergency Preparedness and Response, Nigeria Centre for Disease Control, Abuja, Federal Capital Territory, Nigeria12Public Health Laboratory Services, Nigeria Centre for Disease Control, Abuja, Federal Capital Territory, Nigeria
13Surveillance and Epidemiology, Nigeria Centre for Disease Control, Abuja, Federal Capital Territory, Nigeria14Irrua Specialist Teaching Hospital, Irrua, Edo State, Nigeria15Department of Community Medicine, Ahmadu Bello University, Zaria, Nigeria16Department of Community Medicine, University College Hospital, Ibadan, Oyo State, Nigeria17Department of Microbiology, Nigerian Institute of Medical Research, Yaba, Lagos State, Nigeria18Center for Advanced Medical Research and Training, Usmanu Danfodiyo University, Sokoto, Sokoto State, Nigeria19Department of Pharmacology & Therapeutics, College of Health Sciences, Usmanu Danfodiyo University, Sokoto, Sokoto State, Nigeria20Department of Microbiology & Biotechnology, Federal University Dutse, Dutse, Jigawa State, Nigeria21Centre for Environmental and Public Health Research and Development, Kano, Kano State, Nigeria22National Agency for the Control of AIDS, Abuja, Federal Capital Territory, Nigeria23University of Abuja Teaching Hospital, Gwagwalada, Abuja, Federal Capital Territory, Nigeria24Department of Community Medicine, Nnamdi Azikiwe University Teaching Hospital, Nnewi, Anambra State, Nigeria25eHealth Africa, Abuja, Federal Capital Territory, Nigeria26Maryland Global Initiatives Corporation, Abuja, Federal Capital Territory, Nigeria27World Health Organization, Abuja, Federal Capital Territory, Nigeria28Department of Microbiology, University of Benin, Benin, Edo State, Nigeria29Joint United Nations Programme on AIDS (UNAIDS), Abuja, Federal Capital Territory, Nigeria
Twitter Kelly Osezele Elimian @KElimian, Ehimario Igumbor @Ehimario, Olusola Aruna @solaruna, Tarik Benjamin Mohammed @Mohtareek, Afolabi Adekaiyaoja @aadekaiyaoja, Tochi Okwor @tokwor7, John Oladejo @johnoladejo and Chinwe Lucia Ochu @chinwe_ochu
Acknowledgements We appreciate all the Nigerian frontline health workers for their contribution to the collection of the data used for this study. We acknowledge the leadership and coordination provided by all state commissioners for health, epidemiologists and disease notification and surveillance officers. We are also grateful to colleagues, including members of the Epidemiological Working Group of the Nigeria COVID- 19 Research Coalition (NCRC) who provided technical and administrative support for this manuscript. In addition, we acknowledge the African Field Epidemiology Network (AFENET) for providing financial support towards the publication of this manuscript.
Contributors EI acts as the Guarantor of this study
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not- for- profit sectors.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient consent for publication Not applicable.
Ethics approval The study protocol was approved by the Nigerian National Health Research Ethics Committee (NHREC/01/01/2007- 22/06/2020).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer- reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from

Akande OW, et al. BMJ Global Health 2021;6:e007076. doi:10.1136/bmjgh-2021-007076 13
BMJ Global Health
Open access This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY- NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non- commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non- commercial. See: http:// creativecommons. org/ licenses/ by- nc/ 4. 0/.
ORCID iDsOluwatosin Wuraola Akande http:// orcid. org/ 0000- 0001- 6906- 895XKelly Osezele Elimian http:// orcid. org/ 0000- 0003- 2729- 1613Ehimario Igumbor http:// orcid. org/ 0000- 0002- 6313- 6031Ekaete Alice Tobin http:// orcid. org/ 0000- 0001- 5059- 807XChinwe Lucia Ochu http:// orcid. org/ 0000- 0002- 0630- 7332
REFERENCES 1 Cucinotta D, Vanelli M. WHO Declares COVID- 19 a pandemic. Acta
Biomed 2020;91:157–60. 2 Elimian KO, Ochu CL, Ilori E, et al. Descriptive epidemiology of
coronavirus disease 2019 in Nigeria, 27 February- 6 June 2020. Epidemiol Infect 2020;148:e208.
3 Nigeria Centre for Disease Control. COVID- 19 Situation Report 130 [Internet]. Nigeria Centre for Disease Control, 2020. Available: https:// ncdc. gov. ng/ diseases/ sitreps/? cat= 14& name= An% 20update% 20of% 20COVID- 19% 20outbreak% 20in% 20Nigeria [Accessed 13 Apr 2021].
4 Ochu CL, Akande OW, Ihekweazu V, et al. Responding to a pandemic through social and behavior change communication: Nigeria's experience. Health Secur 2021;19:223–8.
5 Abubakar I, Dalglish SL, Ihekweazu CA, et al. Lessons from co- production of evidence and policy in Nigeria's COVID- 19 response. BMJ Glob Health 2021;6:e004793.
6 Dan- Nwafor C, Ochu CL, Elimian K, et al. Nigeria's public health response to the COVID- 19 pandemic: January to may 2020. J Glob Health 2020;10:020399.
7 National Primary Health Care Development Agency. Percentage (%) of Total Target Reached with 1st Dose of COVID- 19 Vaccine [Internet], 2021. Available: https:// twitter. com/ NphcdaNG/ status/ 1382374114774675458/ photo/2 [Accessed 10 Apr 2021].
8 National Primary Health Care Development Agency. COVID- 19 Vaccination Plan [Internet]. @NphcdaNG, 2021. Available: https:// twitter. com/ NphcdaNG/ status/ 1381587371032993796 [Accessed 14 Apr 2021].
9 World Health Organization. COVID- 19 vaccines shipped by COVAX arrive in Nigeria [Internet]. WHO | Regional Office for Africa, 2021. Available: https://www. afro. who. int/ news/ covid- 19- vaccines- shipped- covax- arrive- nigeria [Accessed 05 Jul 2021].
10 Burki T. Global COVID- 19 vaccine inequity. Lancet Infect Dis 2021;21:922–3.
11 Our World in Data. Coronavirus (COVID- 19) Testing - Statistics and Research [Internet]. Our World in Data, 2021. Available: https:// ourworldindata. org/ coronavirus- testing [Accessed 14 Apr 2021].
12 Nigeria Centre for Disease Control. NCDC and NIMR launch COVID- 19 Household Seroprevalence Surveys in Selected States of Nigeria [Internet], 2020. Available: https:// ncdc. gov. ng/ news/ 267/ ncdc- and- nimr- launch- covid- 19- household- seroprevalence- surveys- in- selected- states- of- nigeria [Accessed 14 Apr 2021].
13 Nigeria Centre for Disease Control. COVID- 19 Nigeria [Internet], 2021. Available: https:// covid19. ncdc. gov. ng/ [Accessed 17 Sep 2020].
14 Wibawa T, Walsh M. Is there even such a thing as a “second wave”? [Internet], 2020. Available: https://www. abc. net. au/ news/ 2020- 06- 24/ coronavirus- covid- 19- countries- second- wave- explainer- south- korea/ 12385882 [Accessed 14 Apr 2021].
15 Gallagher J. Coronavirus: What is a second wave and is one coming? BBC News [Internet], 2020. Available: https://www. bbc. com/ news/ health- 53113785 [Accessed 14 Apr 2021].
16 Wagner A. What Makes a “Wave” of Disease? An Epidemiologist Explains [Internet], 2020. Available: https:// sph. umich. edu/ pursuit/ 2020posts/ what- makes- a- wave- of- disease. html [Accessed 14 Apr 2021].
17 James N, Menzies M, Radchenko P. COVID- 19 second wave mortality in Europe and the United States. Chaos 2021;31:031105.
18 Soriano V, Ganado- Pinilla P, Sanchez- Santos M, et al. Main differences between the first and second waves of COVID- 19 in Madrid, Spain. Int J Infect Dis 2021;105:374–6.
19 Seong H, Hyun HJ, Yun JG, et al. Comparison of the second and third waves of the COVID- 19 pandemic in South Korea: importance of early public health intervention. Int J Infect Dis 2021;104:742–5.
20 Taboada M, González M, Alvarez A, et al. First, second and third wave of COVID- 19. what have we changed in the ICU management of these patients? J Infect 2021;82:e14–15.
21 World Health Organisation Regional Office for Africa. Africa faces steepest COVID- 19 surge yet [Internet]. WHO | Regional Office for Africa, 2021. Available: https://www. afro. who. int/ news/ africa- faces- steepest- covid- 19- surge- yet [Accessed 05 Jul 2021].
22 Salyer SJ, Maeda J, Sembuche S, et al. The first and second waves of the COVID- 19 pandemic in Africa: a cross- sectional study. Lancet 2021;397:1265–75.
23 Nigeria Centre for Disease Control. Digitalising surveillance in Nigeria: Surveillance, Outbreak Response Management and Analysis System (SORMAS) [Internet], 2018. Available: https:// ncdc. gov. ng/ reports/ 136/ 2018- july- week- 30 [Accessed 28 Sep 2021].
24 Nigeria Centre for Disease Control. National Interim Guidelines for Clinical Management of Covid- 19: Version 1 [Internet]. Nigeria Centre for Disease Control, 2020. Available: https:// ncdc. gov. ng/ themes/ common/ docs/ protocols/ 177_ 1584210847. pdf [Accessed 07 May 2020].
25 Nigeria Centre for Disease Control. Specimen Collection, Packaging and Transportation for SARS- CoV- 2 testing [Internet], 2020. Available: https:// covid19. ncdc. gov. ng/ media/ files/ SOP_ Specimen_ collection_ and_ transportation_ for_ SARS- CoV- 2_ testing_ final_ Version. pdf [Accessed 07 Jun 2021].
26 Nigeria Centre for Disease Control. NCDC Approved COVID- 19 Laboratories [Internet], 2021. Available: https:// gloepid. org [Accessed 07 Jun 2021].
27 Nigeria Centre for Disease Control. National Interim Guidelines for Clinical Management of Covid- 19: Version 4 [Internet]. Nigeria Centre for Disease Control, 2020. Available: https:// covid19. ncdc. gov. ng/ media/ files/ COVIDCaseMgtVersion4. pdf [Accessed 07 Jun 2021].
28 Center for Disease Control and Prevention. MMWR Weeks [Internet], 2021. Available: https:// ndc. services. cdc. gov/ wp- content/ uploads/ MMWR_ Week_ overview. pdf [Accessed 05 Jul 2021].
29 Chibnik L. Biostatistics Workshop: Missing Data [Internet]. Sub- Saharan Africa CFAR Meeting, 2016. Available: https://www. brown. edu/ academics/ medical/ about- us/ research/ centers- institutes- and- programs/ aids/ sites/ center- aids/ files/ Biostat_ MissingData_ LoriChibnik. pdf [Accessed 10 Feb 2021].
30 Groenwold RHH, White IR, Donders ART, et al. Missing covariate data in clinical research: when and when not to use the missing- indicator method for analysis. CMAJ 2012;184:1265–9.
31 Equator Network. STROBE Statement—Checklist of items that should be included in reports of cross- sectional studies [Internet], 2015. Available: https://www. equator- network. org/ wp- content/ uploads/ 2015/ 10/ STROBE_ checklist_ v4_ cross- sectional. pdf [Accessed 02 Oct 2021].
32 Nigeria Centre for Disease Control. One Year After: Nigeria’s COVID- 19 Public Health Response, February 2020 – January 2021 [Internet]., 2021. Available: https:// covid19. ncdc. gov. ng/ media/ files/ COVIDResponseMarch1. pdf [Accessed 05 Jul 2021].
33 Centers for Disease Control and Prevention. SARS- CoV- 2 Variant Classifications and Definitions [Internet]. Centers for Disease Control and Prevention, 2020. Available: https://www. cdc. gov/ coronavirus/ 2019- ncov/ variants/ variant- info. html [Accessed 15 Jul 2021].
34 World Health Organisation. Transmission of SARS- CoV- 2: implications for infection prevention precautions [Internet], 2020. Available: https://www. who. int/ news- room/ commentaries/ detail/ transmission- of- sars- cov- 2- implications- for- infection- prevention- precautions [Accessed 15 Jul 2021].
35 Saito S, Asai Y, Matsunaga N, et al. First and second COVID- 19 waves in Japan: a comparison of disease severity and characteristics. J Infect 2021;82:84–123.
36 Adedigba A. Coronavirus: Nigerian govt orders closure of schools nationwide [Internet]., 2020. Available: https://www. premiumtimesng. com/ news/ top- news/ 382806- coronavirus- nigerian- govt- orders- closure- of- schools- nationwide. html [Accessed 02 Oct 2021].
37 Centre for the the Study of the Economies of Africa. Reopening Schools for Learning amid Covid- 19 [Internet], 2020. Available: http:// cseaafrica. org/ post- covid- 19- reopening- schools- for- learning/ [Accessed 02 Oct 2021].
38 Punch Newspapers. PTF okays phased reopening of schools, orders risk assessment [Internet]. Punch Newspapers, 2020. Available: https:// punchng. com/ ptf- okays- phased- reopening- of- schools- orders- risk- assessment/ [Accessed 02 Oct 2021].
39 Reuters. Nearly 200 at school in Nigeria’s Lagos test positive for COVID- 19 - health commissioner. Reuters [Internet], 2020. Available: https://www. reuters. com/ article/ health- coronavirus- nigeria- idINKBN27203Q [Accessed 02 Oct 2021].
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from

14 Akande OW, et al. BMJ Global Health 2021;6:e007076. doi:10.1136/bmjgh-2021-007076
BMJ Global Health
40 Premium Times. Lagos discovers more COVID- 19 cases in another school [Internet, 2020. Available: https://www. premiumtimesng. com/ regional/ ssouth- west/ 425027- lagos- discovers- more- covid- 19- cases- in- another- school. html [Accessed 02 Oct 2021].
41 Adebowale N. COVID- 19: Nigeria approves reopening of orientation camps [Internet], 2020. Available: https://www. premiumtimesng. com/ news/ top- news/ 412364- covid- 19- nigeria- approves- reopening- of- orientation- camps. html [Accessed 02 Oct 2021].
42 Nigeria Centre for Disease Control. Guidelines on 2020 National Youth Service Corps (NYSC) Orientation Camp Activities [Internet], 2020. Available: https:// covid19. ncdc. gov. ng/ media/ files/ Guidelines_ on_ 2020_ National_ Youth_ Service_ Corps_ NYSC_ Orientation_ Camp_ activities. pdf [Accessed 10 Feb 2021].
43 Ohia C, Salawu MM. COVID- 19 pandemic and civil unrests in Africa: implication of recent #EndSARS protests for increased community transmission in Nigeria. Pan Afr Med J 2020;37:47.
44 Nigeria Centre for Disease Control. Risk Communication and Community Engagement Strategy for COVID- 19 Prevention and Control in Nigeria [Internet], 2021. Available: https:// covid19. ncdc. gov. ng/ media/ files/ 04122020_ RCCE_ Strategy_ Review_ copy2. pdf [Accessed 14 Jul 2021].
45 Smith P. Covid- 19 in Australia: most infected health workers in Victoria's second wave acquired virus at work. BMJ 2020;370:m3350.
46 Ochu CL, Akande OW, Oyebanji O, et al. ‘Fighting a Global War Using a Local Strategy’: contextualism in COVID- 19 response in Africa. BMJ Innov 2021;7:347–55.
47 Ogboghodo EO, Osaigbovo II, Obarisiagbon OO, et al. Facility- Based surveillance activities for COVID- 19 infection and outcomes among healthcare workers in a Nigerian tertiary hospital. Am J Trop Med Hyg 2021;104:1034–40.
48 Partnership for Evidence- Based Response to COVID- 19. Finding the Balance: Public Health and Social Measures in Nigeria [Internet], 2021. Available: https:// preventepidemics. org/ wp- content/ uploads/ 2021/ 03/ nigeria_ en_ 20210323_ 1721. pdf [Accessed 05 Jul 2021].
49 Ibrahim OR, Suleiman BM, Abdullahi SB, et al. Epidemiology of COVID- 19 and predictors of outcome in Nigeria: a single- center study. Am J Trop Med Hyg 2020;103:2376–81.
50 Galasso V, Pons V, Profeta P, et al. Gender differences in COVID- 19 attitudes and behavior: panel evidence from eight countries. Proc Natl Acad Sci U S A 2020;117:27285–91.
51 Centre for Communication and Social Impact. COVID 19 Audience perception survey based on the extended parallel processing model second wave, 2020.
52 Yanez ND, Weiss NS, Romand J- A, et al. COVID- 19 mortality risk for older men and women. BMC Public Health 2020;20:1742.
53 Elimian KO, Ochu CL, Ebhodaghe B, et al. Patient characteristics associated with COVID- 19 positivity and fatality in Nigeria: retrospective cohort study. BMJ Open 2020;10:e044079.
54 Osibogun A, Balogun M, Abayomi A, et al. Outcomes of COVID- 19 patients with comorbidities in Southwest Nigeria. PLoS One 2021;16:e0248281.
on February 5, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-007076 on 18 N
ovember 2021. D
ownloaded from

Supplementary File 1: Distribution of Sociodemographic and Clinical Characteristics of the Study Population in Relation to COVID-19 Infection in Nigeria, 27
February—3 April, 2021
First wave Second wave First and second waves
Variable Negative
[n=296,429
(%)]
Positive
[n=66,121 (%)]
Negative
[n=347,949
(%)]
Positive
[n=91,644 (%)]
Negative
[n=644,378 (%)]
Positive
[n=157,765 (%)]
Total
[n=802,143 (%)]
Sociodemographic characteristics
Mean (SD) age, year
[n=784,239]
34.73 (15.56) 37.57 (15.28) 34.15 (14.06) 37.67 (16.30) 34.42 (14.77) 37.63 (15.88) 35.04 (15.04)
Age group, year
0-4
5-13
14-20
21-30
31-40
41-50
51-60
5,498 (1.85)
17,326 (5.84)
32,124 (10.84)
65,554 (22.11)
73,669 (24.85)
50,309 (16.97)
29,870 (10.08)
886 (1.34)
2,393 (3.62)
3,980 (6.02)
13,569 (20.52)
17,665 (26.72)
12,212 (18.47)
7,577 (11.46)
4,120 (1.18)
10,921 (3.14)
23,758 (6.83)
132,768 (38.16)
73,762 (21.20)
51,101 (14.69)
31,249 (8.98)
1,424 (1.55)
3,560 (3.88)
6,638 (7.24)
20,184 (22.02)
21,689 (23.67)
16,121 (17.59)
10,870 (11.86)
9,618 (1.49)
28,247 (4.38)
55,882 (8.67)
198,322 (30.78)
147,431 (22.88)
101,410 (15.74)
61,119 (9.48)
2,310 (1.46)
5,953 (3.77)
10,618 (6.73)
33,753 (21.39)
39,354 (24.94)
28,333 (17.96)
18,447 (11.69)
11,928 (1.49)
34,200 (4.26)
66,500 (8.29)
232,075 (28.93)
186,785 (23.29)
129,743 (16.17)
79,566 (9.92)
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health
doi: 10.1136/bmjgh-2021-007076:e007076. 6 2021;BMJ Global Health, et al. Akande OW

61-70
71-80
>80
Missing
10,292 (3.47)
3,745 (1.26)
1,052 (0.35)
6,990 (2.36)
3,055 (4.62)
1,114 (1.68)
351 (0.53)
3,319 (5.02)
10,992 (3.16)
3,764 (1.08)
1,128 (0.32)
4,386 (1.26)
5,091 (5.56)
2,132 (2.33)
726 (0.79)
3,209 (3.50)
21,284 (3.30)
7,509 (1.17)
2,180 (0.34)
11,376 (1.77)
8,146 (5.16)
3,246 (2.06)
1,077 (0.68)
6,528 (4.14)
29,430 (3.67)
10,755 (1.34)
3,257 (0.41)
17,904 (2.23)
Sex
Female
Male
Missing
114,645 (38.68)
179,596 (60.59)
2,188 (0.74)
23,558 (35.63)
41,370 (62.57)
1,193 (1.80)
143,508 (41.24)
203,776 (58.56)
665 (0.19)
38,403 (41.90)
52,754 (57.56)
487 (0.53)
258,153 (40.06)
383,372 (59.49)
2,853 (0.44)
61,961 (39.27)
94,124 (59.66)
1,680 (1.06)
320,114 (39.91)
477,496 (59.53)
4,533 (0.57)
Residential setting
Rural
Urban
Missing
27,893 (9.41)
99,596 (33.60)
168,940 (56.99)
3,822 (5.78)
25,738 (38.93)
36,561 (55.29)
20,970 (6.03)
64,113 (18.43)
262,866 (75.55)
5,192 (5.67)
26,510 (28.93)
59,942 (65.41)
48,863 (7.58)
163,709 (25.41)
431,806 (67.01)
9,014 (5.71)
52,248 (33.12)
96,503 (61.17)
57,877 (7.22)
215,957 (26.92)
528,309 (65.86)
Formal education completed
None
Nursery
Primary
Secondary
6,287 (2.12)
1,164 (0.39)
7,500 (2.53)
28,249 (9.53)
949 (1.44)
180 (0.27)
1,200 (1.81)
5,670 (8.58)
3,615 (1.04)
493 (0.14)
6,041 (1.74)
18,987 (5.46)
911 (0.99)
123 (0.13)
1,285 (1.40)
4,814 (5.25)
9,902 (1.54)
1,657 (0.26)
13,541 (2.10)
47,236 (7.33)
1,860 (1.18)
303 (0.19)
2,485 (1.58)
10,484 (6.65)
11,762 (1.47)
1,960 (0.24)
16,026 (2.00)
57,720 (7.20)
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health
doi: 10.1136/bmjgh-2021-007076:e007076. 6 2021;BMJ Global Health, et al. Akande OW

Tertiary
Alternative (e.g.Almajiranci)
Missing
63,350 (21.37)
9,179 (3.10)
180,700 (60.96)
15,815 (23.92)
3,102 (4.69)
39,205 (59.29)
42,834 (12.31)
4,635 (1.33)
271,344 (77.98)
18,449 (20.13)
1,948 (2.13)
64,114 (69.96)
106,184 (16.48)
13,814 (2.14)
452,044 (70.15)
34,264 (21.72)
5,050 (3.20)
103,319 (65.49)
140,448 (17.51)
18,864 (2.35)
55,363 (69.23)
Current occupation
Pupil/student
Housewife/child
Trader/business
Farmer/miner
Healthcare worker
Animal-related work
Transporter
Religious leader
Traditional leader
Other
Missing
27,696 (9.34)
8,382 (2.83)
11,591 (3.91)
6,457 (2.18)
17,935 (6.05)
425 (0.14)
686 (0.23)
396 (0.13)
84 (0.03)
101,973 (34.40)
120,804 (40.75)
4,419 (6.68)
1,096 (1.66)
2,727 (4.12)
718 (1.09)
4,972 (7.52)
70 (0.11)
142 (0.21)
127 (0.19)
22 (0.03)
24,224 (36.64)
27,604)
19,922 (5.73)
6,105 (1.75)
9,274 (2.67)
6,372 (1.83)
6,024 (1.73)
398 (0.11)
359 (0.10)
364 (0.10)
46 (0.01)
214,979 (61.78)
84,106 (24.17)
4,829 (5.27)
1,373 (1.50)
2,342 (2.56)
1,007 (1.10)
2,648 (2.89)
57 (0.06)
48 (0.05)
99 (0.11)
36 (0.04)
48,150 (52.54)
31,055 (33.89)
47,618 (7.39)
14,487 (2.25)
20,865 (3.24)
12,829 (1.99)
23,959 (3.72)
823 (0.13)
1,045 (0.16)
760 (0.12)
130 (0.02)
316,952 (49.19)
204,910 (31.80)
9,248 (5.86)
2,469 (1.56)
5,069 (3.21)
1,725 (1.09)
7,620 (4.83)
127 (0.08)
190 (0.12)
226 (0.14)
58 (0.04)
72,374 (45.87)
58,659 (37.18)
56,866 (7.09)
16,956 (2.11)
25,934 (3.23)
14,554 (1.81)
31,579 (3.94)
950 (0.12)
1,235 (0.15)
986 (0.12)
188 (0.02)
389,326 (48.54)
263,569 (32.86)
Quarantine location
None
45,855 (15.47)
5,464 (8.26)
22,732 (6.53)
8,230 (8.98)
68,587 (10.64)
13,694 (8.68)
82,281 (10.26)
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health
doi: 10.1136/bmjgh-2021-007076:e007076. 6 2021;BMJ Global Health, et al. Akande OW

Formal institution
Home
Missing
1,363 (0.46)
21,954 (7.41)
227,257 (76.66)
1,912 (2.89)
6,116 (9.25)
52,629 (79.59)
220 (0.06)
7,539 (2.17)
317,458 (91.24)
205 (0.22)
3,757 (4.10)
79,452 (86.70)
1,583 (0.25)
29,493 (4.58)
544,715 (84.53)
2,117 (1.34)
9,873 (6.26)
132,081 (83.72)
3,700 (0.46)
39,366 (4.91)
676,796 (84.37)
Travel history (last 14 days)
No
Yes
Missing
180,757 (60.98)
12,934 (4.36)
102,738 (34.66)
38,421 (58.11)
2,495 (3.77)
25,205 (38.12)
93,624 (26.91)
9,552 (2.75)
244,773 (70.35)
30,008 (32.74)
901 (0.98)
60,735 (66.27)
274,381 (42.58)
22,486 (3.49)
347,511 (53.93)
68,429 (43.37)
3,396 (2.15)
85,940 (54.47)
342,810 (42.74)
25,882 (3.23)
433,451 (54.04)
Admission to treatment
centre
No
Yes
Missing
164,799 (55.59)
8,022 (2.71)
123,608 (41.70)
31,127 (47.08)
6,885 (10.41)
28,109 (42.51)
169,034 (48.58)
1,382 (0.40)
177,533 (51.02)
49,589 (54.11)
1,250 (1.36)
40,805 (44.53)
333,833 (51.81)
9,404 (46.73)
301,141 (46.73)
80,716 (51.16)
8,135 (5.16)
68,914 (43.68)
414,549 (51.68)
17,539 (2.19)
370,055 (46.13)
Mean (SD) temperature, oC
[n=132,268]
36.45 (0.80) 36.68 (0.95) 36.40 (0.82) 36.44 (1.23) 36.43 (0.81) 36.58 (1.08) 36.46 (0.86)
Temperature source
Axillary
Non-contact
17,051 (5.75)
53,210 (17.95)
4,014 (6.07)
8,092 (12.24)
7,176 (2.06)
33,283 (9.57)
2,568 (2.80)
6,657 (7.26)
24,227 (3.76)
86,493 (13.42)
6,582 (4.17)
14,749 (9.35)
30,809 (3.84)
101,242 (12.62)
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health
doi: 10.1136/bmjgh-2021-007076:e007076. 6 2021;BMJ Global Health, et al. Akande OW

Oral
Rectal
Unknown
132 (0.04)
15 (0.01)
226,021 (76.25)
26 (0.04)
4 (0.01)
53,985 (81.65)
142 (0.040
34 (0.01)
307,314 (88.32)
33 (0.04)
16 (0.02)
82,370 (89.88)
274 (0.04)
49 (0.01)
533,335 (82.77)
59 (0.04)
20 (0.01)
136,355 (86.43)
333 (0.04)
69 (0.01)
669,690 (83.49)
Symptomatic status
Asymptomatic
Symptomatic
243,665 (82.20)
52,764 (17.80)
49,542 (74.93)
16,579 (25.07)
294,411 (84.61)
53,538 (15.39)
73,038 (79.70)
18,606 (20.30)
538,076 (83.50)
106,302 (16.50)
122,580 (77.70)
35,185 (22.30)
660,656 (82.36)
141,487 (17.64)
Clinical characteristics
n=52,764 n= 16,579 n= 53,538 n=18,606 n=106,302 n=35,185 N=141,487
Abdominal pain
No
Yes
Missing
47,460 (89.950
693 (1.310
4,611 (8.74)
16,222 (97.85)
137 (0.83)
220 (1.33)
36,763 (68.67)
714 (1.33)
16,061 (30.00)
14,445 (77.64)
320 (1.72)
3,841 (20.64)
84,223 (79.23)
1,407 91.320
20,672 (19.450
30,667 (87.16)
457 (1.300
4,061 (11.54)
114,890 (81.20)
1,864 (1.32)
24,733 (17.48)
Chest pain
No
Yes
Missing
46,866 (88.82)
1,286 (2.44)
4,612 (8.74)
15,793 (95.26)
575 (3.470
211 (1.27)
44,193 (82.55)
2,815 (5.26)
6,530 (12.20)
16,874 (90.69)
856 (4.60)
876 (4.710
91,059 (85.66)
4,101 (3.86)
11,142 (10.48)
32,667 (92.84)
1,431 (4.07)
1,087 (3.09)
123,726 (87.45)
5,532 (3.91)
12,229 (8.64)
Chills/sweat
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health
doi: 10.1136/bmjgh-2021-007076:e007076. 6 2021;BMJ Global Health, et al. Akande OW

No
Yes
Missing
47,555 (90.13)
578 (1.10)
4,631 (8.78)
16,137 (97.33)
227 (1.37)
215 (1.30)
37,331 (69.73)
454 (0.85)
15,753 (29.42)
14,306 (76.89)
166 (0.89)
4,134 (22.220
84,886 (79.85)
1,032 (0.97)
20,384 (19.18)
30,443 (86.52)
393 (1.120
4,349 (12.36)
115,329 (81.510
1,425 (1.010
24,733 (17.480
Cough
No
Yes
Missing
34,215 (64.85)
18,203 (34.50)
346 (0.66)
8,086 (48.77)
8,420 (50.790
73 (0.44)
39,484 (73.75)
13,733 (25.65)
321 (0.60)
10,403 (55.91)
8,044 (43.23)
159 (0.85)
73,699 (69.33)
31,936 (30.04)
667 (0.63)
18,489 (52.55)
16,464 (46.79)
232 (0.66)
92,188 (65.16)
48,400 (34.21)
899 (0.64)
Diarrhoea
No
Yes
Missing
49,625 (94.05)
2,642 (5.01)
497 (0.94)
15,400 (92.89)
1,024 (6.18)
155 (0.93)
50,672 (94.65)
2,121 (3.96)
745 (1.39)
17,369 (93.35)
815 (4.38)
422 (2.27)
100,297 (94.35)
4,763 (4.48)
1,242 (1.17)
32,769 (93.13)
1,839 (5.23)
577 (1.64)
133,066 (94.05)
6,602 (4.67)
1,819 (1.29)
Difficulty in breathing
No
Yes
Missing
46,968 (89.02)
5,281 (10.01)
515 (0.98)
13,969 (84.26)
2,454 (14.80)
156 (0.94)
41,511 (77.54)
2,632 (4.92)
9,395 (17.55)
14,431 (77.56)
3,024 (16.25)
1,151 (6.19)
88,479 (83.23)
7,913 (7.44)
9,910 (9.32)
28,400 (80.72)
5,478 (15.57)
1,307 (3.71)
116,879 (82.61)
13,391 (9.46)
11,217 (7.93)
Fatigue
No
45,252 (85.76)
15,332 (92.48)
41,489 (77.49)
13,763 (73.97)
86,741 (81.60)
29,095 (82.69)
115,836 (81.87)
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health
doi: 10.1136/bmjgh-2021-007076:e007076. 6 2021;BMJ Global Health, et al. Akande OW

Yes
Missing
2,602 (4.93)
4,910 (9.31)
1,024 (6.18)
223 (1.35)
5,107 (9.54)
6,942 (12.97)
2,891 (15.54)
1,952 (10.49)
7,709 (7.25)
11,852 (11.15)
3,915 (11.13)
2,175 (6.18)
11,624 (8.22)
14,027 (9.91)
Fever
No
Yes
Missing
30,194 (57.22)
22,345 (42.35)
225 (0.43)
8,776 (52.93)
7,736 (46.66)
67 (0.40)
34,215 (63.91)
18,789 (35.09)
534 (1.00)
10,905 (58.61)
7,497 (40.29)
204 (1.10)
64,409 (60.59)
41,134 (38.70)
759 (0.71)
19,681 (55.94)
15,233 (43.29)
271 (0.77)
84,090 (59.43)
56,367 (39.840
1,030 (0.73)
Headache
No
Yes
Missing
41,274 (78.22)
7,107 (13.47)
4,383 (8.31)
13,946 (84.12)
2,473 (14.92)
160 (0.97)
34,452 (64.35)
12,675 (23.67)
6,411 (11.97)
12,992 (69.83)
4,838 (26.00)
776 (4.17)
75,726 (71.24)
19,782 (18.61)
10,794 (10.15)
26,938 (76.56)
7,311 (20.78)
936 (2.66)
102,664 (72.56)
27,093 (19.15)
11,730 (8.29)
Joint pain
No
Yes
Missing
47,391 (89.82)
433 (0.82)
4,940 (9.36)
16,168 (97.52)
182 (1.10)
229 (1.38)
37,663 (70.35)
626 (1.17)
15,249 (28.48)
16,504 (88.70)
455 (2.45)
1,647 (8.85)
85,054 (80.01)
1,059 (1.00)
20,189 (18.99)
32,672 (92.86)
637 (1.81)
1,876 (5.33)
117,726 (83.21)
1,696 (1.20)
22,065 (15.60)
Malaise
No
Yes
7,464 (14.15)
134 (0.25)
2,123 (12.81)
96 (0.58)
2,095 (3.91)
36 (0.07)
5,229 (28.10)
126 (0.68)
9,559 (8.99)
170 (0.16)
7,352 (20.90)
222 (0.63)
16,911 (11.95)
392 (0.28)
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health
doi: 10.1136/bmjgh-2021-007076:e007076. 6 2021;BMJ Global Health, et al. Akande OW

Missing 45,166 (85.60) 14,360 (86.62) 51,407 (96.02) 13,251 (71.22) 96,573 (90.85) 27,611 (78.47) 124,184 (87.77)
Muscle pain
No
Yes
Missing
46,835 (88.76)
991 (1.88)
4,938 (9.36)
16,0.35 (96.72)
316 (1.91)
228 (1.38)
37,304 (69.68)
1,022 (1.91)
15,212 (28.41)
16,441 (88.36)
560 (3.01)
1,605 (8.63)
84,139 (79.15)
2,013 (1.89)
20,150 (18.89)
32,476 (92.30)
876 (2.49)
1,833 (5.21)
116,615 (82.42)
2,889 (2.04)
21,983 (15.54)
Nausea
No
Yes
Missing
49,062 (92.980
3,163 (5.99)
539 (1.020
15,185 (91.590
1,220 (7.360
174 (1.050
49,164 (91.830
3,811 (7.120
563 (1.050
17,015 (91.45)
1,278 (6.87)
313 (1.68)
98,226 (92.40)
6,974 (6.560
1,102 (1.040
32,200 (91.52)
2,498 (7.100
487 (1.38)
130,426 (92.18)
9,472 (6.69)
1,589 (1.12)
Rapid breathing
No
Yes
Missing
45,544 (86.32)
491 (0.93)
6,729 (12.75)
15,028 (90.64)
264 (1.59)
1,287 (7.76)
37,248 (69.570
196 (0.370
16,094 (30.060
13,889 (74.650
143 (0.770
4,574 (24.58)
82,792 (77.88)
687 (0.65)
22,823 (21.47)
28,917 (82.19)
407 (1.160
5,861 (16.660
111,709 978.95)
1,094 (0.770
28,684 (20.270
Runny nose
No
Yes
Missing
41,975 (79.55)
10,330 (19.580
459 (0.870
11,922 (71.91)
4,495 (27.11)
162 (0.980
38,622 (72.140
14,491 (27.07)
425 (0.79)
11,263 (60.530
7,113 (38.230
230 (1.240
80,597 (75.820
24,821 (23.350
884 (0.83)
23,185 (65.89)
11,608 (32.99)
392 (1.11)
103,782 (73.35)
36,429 (25.75)
1,276 (0.90)
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health
doi: 10.1136/bmjgh-2021-007076:e007076. 6 2021;BMJ Global Health, et al. Akande OW

Sore throat
No
Yes
Missing
41,451 (78.56)
10,862 (20.59)
451 (0.85)
12,660 (76.36)
3,796 (22.90)
123 (0.74)
44,270 (82.69)
8,788 (16.41)
480 (0.90)
15,800 (84.92)
2,542 (13.66)
264 (1.420
85,721 (80.64)
19,650 (18.49)
931 (0.88)
28,460 (80.89)
6,338 (18.01)
387 (1.10)
114,181 (80.70)
25,988 (18.37)
1,318 (0.93)
Vomiting
No
Yes
Missing
50,126 (95.00)
2,110 (4.00)
528 (1.00)
15,606 (94.13)
809 (4.88)
164 (0.99)
51,026 (95.31)
1,687 (3.15)
825 (1.540
15,877 (85.33)
680 (3.650
2,049 (11.01)
101,152 (95.16)
3,797 (3.570
1,353 (1.27)
31,483 (89.48)
1,489 (4.23)
2,213 (6.29)
132,635 (93.740
5,286 (3.74)
3,566 (2.52)
Loss of smell
No
Yes
Missing
46,597 (88.31)
1,233 (2.34)
4,934 (9.35)
13,661 (82.40)
1,839 (11.09)
1,079 (6.51)
50,979 (95.22)
2,041 (3.81)
518 (0.97)
15,123 (81.28)
3,180 (1.63)
303 (1.630
97,576 (91.79)
3,274 (3.08)
5,452 (5.13)
28,784 (81.81)
5,019 (14.26)
1,382 (3.93)
126,360 (89.31)
8,293 (5.86)
6,834 (4.83)
Loss of taste
No
Yes
Missing
46,455 (88.04)
1,372 (2.60)
4,937 (9.36)
13,907 (83.88)
1,593 (9.61)
1,079 (6.51)
50,904 (95.08)
2,118 (3.96)
516 (0.96)
16,729 (89.91)
1,576 (8.47)
301 (1.62)
97,359 (91.59)
3,490 (3.28)
5,453 (5.13)
30,636 (87.07)
3,169 (9.01)
1,380 (3.92)
127,995 (90.46)
6,659 (4.71)
6,833 (4.83)
ARDS
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health
doi: 10.1136/bmjgh-2021-007076:e007076. 6 2021;BMJ Global Health, et al. Akande OW

No
Yes
Missing
47,529 (90.08)
299 (0.57)
4,936 (9.35)
16,207 (97.76)
152 (0.92)
220 (1.33)
37,378 (69.82)
91 (0.17)
16,069 (30.01)
13,973 (75.10)
65 (0.35)
4,568 (24.55)
84,907 (79.87)
390 (0.37)
21,005 (19.76)
30,180 (85.78)
217 (0.62)
4,788 (13.61)
115,087 (81.34)
607 (0.43)
25,793 (18.23)
Pneumonia
No
Yes
Missing
47,653 (90.31)
99 (0.19)
5,012 (9.50)
16,279 (98.19)
46 (0.28)
254 (1.53)
37,216 (69.51)
25 (0.05)
16,297 (30.44)
13,903 (74.72)
30 (0.16)
4,673 (25.12)
84,869 (79.84)
124 (0.12)
21,309 (20.05)
30,182 (85.78)
76 (0.22)
4,927 (14.00)
115,051 (81.32)
200 (0.14)
26,236 (18.54)
*: 343,563 records; **: 88,435 records;
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health
doi: 10.1136/bmjgh-2021-007076:e007076. 6 2021;BMJ Global Health, et al. Akande OW

BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health
doi: 10.1136/bmjgh-2021-007076:e007076. 6 2021;BMJ Global Health, et al. Akande OW

Supplementary File 2: Distribution of sociodemographic and clinical characteristics of the study population in relation to deaths from COVID-
19 infection in Nigeria, 27 February—3 April, 2021
Variable
First wave Second wave First and second waves
Survivor
[n=61,092
(%)]
Dead
[n=1,221 (%)]
Survivor
[n=85,649
(%)]
Dead
[n=611 (%)]
Survivor
[n=146,741
(%)]
Dead
[n=1,832 (%)]
Total
[n=148,573
(%)]
Sociodemographic characteristics
Mean (SD) age, year
[n=784,239]
37.28 (15.05) 56.93 (16.27) 37.53 (16.22) 60.72 (17.42) 37.43 (15.75) 58.20 (16.75) 37.63 (15.88)
Age group, year
0-4
5-13
14-20
21-30
31-40
41-50
51-60
845 (1.38)
2,274 (3.72)
3,732 (6.11)
12,722 (20.82)
16,717 (27.36)
11,547 (18.90)
6,964 (11.40)
2 (0.16)
9 (0.74)
17 (1.39)
56 (4.59)
106 (8.68)
167 (13.68)
276 (22.60)
1,348 (1.57)
3,388 (3.96)
6,229 (7.27)
19,133 (22.34)
20,404 (23.82)
15,135 (17.67)
10,084 (11.77)
5 (0.82)
4 (0.65)
11 (1.80)
13 (2.13)
42 (6.87)
59 (9.66)
127 (20.79)
2,193 (1.49)
5,662 (3.86)
9,961 (6.79)
31,855 (21.71)
37,121 (25.30)
26,682 (18.18)
17,048 (11.62)
7 (0.38)
13 (0.71)
28 (1.53)
69 (3.77)
148 (8.08)
226 (12.34)
403 (22.00)
2,200 (1.48)
5,675 (3.82)
9,989 (6.72)
31,924 (21.49)
37,269 (25.08)
26,9.8 (18.11)
17,451 (11.75)
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health
doi: 10.1136/bmjgh-2021-007076:e007076. 6 2021;BMJ Global Health, et al. Akande OW

61-70
71-80
>80
Missing
2,632 (4.31)
923 (1.51)
285 (0.47)
2,451 (4.01)
298 (24.41)
161 (13.19)
57 (4.67)
72 (5.90)
4,723 (5.51)
1,928 (2.25)
649 (0.76)
2,628 (3.07)
142 (23.24)
123 (20.13)
52 (8.51)
33 (5.40)
7,355 (5.01)
2,851 (1.94)
934 (0.64)
5,079 (3.46)
440 (24.02)
284 (15.50)
109 (5.95)
105 (5.73)
7,795 (5.25)
3,135 (2.11)
1,043 (0.70)
5,184 (3.49)
Sex
Female
Male
Missing
22,077 (36.14)
38,277 (62.65)
738 (1.21)
301 (24.65)
911 (74.61)
9 (0.74)
36,066 (42.11)
49,150 (57.39)
433 (0.51)
204 (33.39)
407 (66.61)
0 (0.00)
58,143 (39.62)
87,427 (59.58)
1,171 (0.80)
505 (27.57)
1,318 (71.94)
9 (0.49)
58,648 (39.47)
88,745 (59.73)
1,180 (0.79)
Residential setting
Rural
Urban
Missing
3,697 (6.05)
24,695 (40.42)
32,700 (53.53)
78 (6.39)
556 (45.54)
587 (48.08)
5,086 (5.94)
25,934 (30.28)
54,629 (63.78)
28 (4.58)
314 (51.39)
269 (44.03)
8,783 (5.99)
50,629 (34.50)
87,329 (59.51)
106 (5.79)
870 (47.49)
856 (46.72)
8,889 (5.98)
51,499 (34.66)
88,185 (59.35)
Formal education completed
None
Nursery
Primary
Secondary
894 (1.46)
176 (0.29)
1,149 (1.88)
5,442 (8.91)
20 (1.64)
0 (0.00)
22 (1.80)
142 (11.63)
893 (1.04)
118 (0.14)
1,252 (1.46)
4,678 (5.46)
7 (1.15)
0 (0.00)
2 (0.33)
44 (7.20)
1,787 (1.22)
294 (0.20)
2,401 (1.64)
10,120 (6.90)
27 (1.47)
0 (0.00)
24 (1.31)
186 (10.15)
1,814 (1.22)
294 (0.20)
2,425 (1.63)
10,306 (6.94)
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health
doi: 10.1136/bmjgh-2021-007076:e007076. 6 2021;BMJ Global Health, et al. Akande OW

Tertiary
Alternative (e.g.Almajiranci)
Missing
15,229 (24.93)
3,001 (4.91)
35,201 (57.62)
299 (24.49)
41 (3.36)
697 (57.08)
17,743 (20.72)
1,790 (2.09)
59,175 (69.09)
194 (31.75)
8 (1.31)
356 (58.27)
32,972 (22.47)
4,791 (3.26)
94,376 (64.31)
493 (26.91)
49 (2.67)
1,053 (57.48)
33,465 (22.52)
4,840 (3.26)
95,429 (64.23)
Current occupation
Pupil/student
Housewife/child
Trader/business
Farmer/miner
Healthcare worker
Animal-related work
Transporter
Religious leader
Traditional leader
Other
Missing
4,325 (7.08)
1,052 (1.72)
2,586 (4.23)
660 (1.08)
4,823 (7.89)
66 (0.11)
133 (0.22)
119 (0.19)
19 (0.03)
23,301 (38.14)
24,008 (39.30)
12 (0.98)
23 (1.88)
103 (8.44)
52 (4.26)
50 (4.10)
3 (0.25)
6 (0.49)
7 (0.57)
3 (0.25)
451 (36.94)
511 (41.85)
4,725 (5.52)
1,350 (1.58)
2,271 (2.65)
977 (1.14)
2,585 (3.02)
54 (0.06)
48 (0.06)
94 (0.11)
35 (0.04)
47,052 (54.94)
26,458 (30.89)
1 (0.16)
6 (0.98)
30 (4.91)
18 (2.95)
15 (2.45)
1 (0.16)
0 (0.00)
1 (0.16)
1 (0.16)
237 (38.79)
301 (49.26)
9,050 (6.17)
2,402 (1.64)
4,857 (3.31)
1,637 (1.12)
7,408 (5.05)
120 (0.08)
181 (0.12)
213 (0.15)
54 (0.04)
70,353 (47.94)
50,466 (34.39)
13 (0.71)
29 (1.58)
133 (7.26)
70 (3.82)
65 (3.55)
4 (0.22)
6 (0.33)
8 (0.44)
4 (0.22)
688 (37.55)
812 (44.32)
9,063 (6.10)
2,431 (1.64)
4,990 (3.36)
1,707 (1.15)
7,473 (5.03)
124 (0.08)
187 (0.13)
221 (0.15)
58 (0.04)
71,041 (47.82)
51,278 (34.51)
Admission to treatment centre
No
29,696 (48.61)
504 (41.28)
48,435 (56.55)
194 (31.75)
78,131 (53.24)
698 (38.10)
78,829 (53.06)
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health
doi: 10.1136/bmjgh-2021-007076:e007076. 6 2021;BMJ Global Health, et al. Akande OW

Yes
Missing
6,436 (10.53)
24,960 (40.86)
352 (28.83)
365 (29.89)
1,109 (1.29)
36,42.15)
115 (18.82)
302 (49.43)
7,545 (5.14)
61,065 (41.61)
467 (25.49)
667 (36.41)
8,012 (5.39)
61,732 (41.55)
Mean (SD) temperature, oC
[n=21,567]
36.64 (0.93) 37.14 (1.13) 36.44 (1.23) 37.03 (1.32) 36.55 (1.08) 37.11 (1.18) 36.58 (1.08)
Symptomatic status
Asymptomatic
Symptomatic
45,852 (75.05)
15,240 (24.95)
482 (39.48)
739 (60.52)
68,279 (79.72)
17,370 (20.28)
274 (44.84)
337 (55.16)
114,131 (77.78)
32,610 (22.22)
756 (41.27)
1,076 (58.73)
114,887 (77.33)
33.686 (22.67)
Clinical characteristics‡
n=15,240 n=739 n=17,370 n=337 n=32,478 n=1,076 N=33,686
Abdominal pain
No
Yes
Missing
14,917 (97.88)
119 (0.78)
204 (1.34)
710 (96.08)
16 (2.17)
13 (1.76)
13,787 (79.37)
309 (1.78)
3,274 (18.85)
326 (96.74)
0 (0.00)
11 (3.26)
28,704 (88.02)
428 (1.31)
3,478 (10.67)
1,036 (96.28)
16 (1.49)
24 (2.23)
29,740 (88.29)
444 (1.32)
3,502 (10.40)
Chest pain
No
Yes
Missing
14,550 (95.47)
494 (1.29)
196 (1.29)
681 (92.15)
46 (6.22)
12 (1.62)
16,240 (93.49)
815 (4.69)
315 (1.81)
306 (90.80)
25 (7.42)
6 (1.780
30,790 (94.42)
1,309 (4.01)
511 (1.57)
987 (91.73)
71 96.60)
18 (1.67)
31,777 (94.33)
1,380 (4.10)
529 (1.57)
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health
doi: 10.1136/bmjgh-2021-007076:e007076. 6 2021;BMJ Global Health, et al. Akande OW

Chills/sweat
No
Yes
Missing
14,835 (97.34)
205 (1.35)
200 (1.31)
710 (96.08)
17 (2.30)
12 (1.62)
13,648 (78.57)
164 (0.94)
3,558 (20.48)
326 (96.74)
2 (0.59)
9 (2.67)
28,483 (87.34)
369 (1.13)
3,758 (11.52)
1,036 (96.28)
19 (1.77)
21 (1.95)
29,519 (87.63)
388 (1.15)
3,779 (11.22)
Cough
No
Yes
Missing
7,530 (49.41)
7,645 (50.16)
65 (0.43)
243 (32.88)
488 (66.04)
8 (1.08)
9,485 (54.61)
7,729 (44.50)
156 (0.90)
146 (43.32)
189 (56.08)
2 (0.59)
17,015 (52.18)
15,374 (47.15)
221 (0.680
389 (36.15)
677 (62.92)
10 (0.93)
17,404 (51.67)
16,051 (47.65)
231 (0.69)
Diarrhoea
No
Yes
Missing
14,162 (92.93)
935 (6.14)
143 (0.94)
667 (90.26)
60 (8.12)
12 (1.62)
16,179 (93.14)
788 (4.54)
403 (2.32)
313 (92.88)
16 (4.75)
8 (2.37)
30,341 (93.04)
1,723 (5.28)
546 (1.67)
980 (91.08)
76 (7.06)
20 (1.86)
31,321 (92.98)
1,799 (5.34)
566 (1.68)
Difficulty in breathing
No
Yes
Missing
13,030 (85.50)
2,063 (13.54)
147 (0.96)
370 (50.07)
360 (48.71)
9 (1.220
13,376 (77.01)
2,858 (16.45)
1,136 (6.54)
190 (56.38)
142 (42.14)
5 (1.48)
26,406 (80.98)
4,921 (15.09)
1,283 (3.93)
560 (52.04)
502 (46.65)
14 (1.30)
26,966 (80.05)
5,423 (16.10)
1,297 (3.85)
Fatigue
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health
doi: 10.1136/bmjgh-2021-007076:e007076. 6 2021;BMJ Global Health, et al. Akande OW

No
Yes
Missing
14,117 (92.63)
914 (6.00)
209 (1.37)
653 (88.36)
75 (10.15)
11 (1.490
13,151 (75.71)
2,837 (16.33)
1,382 (7.96)
298 (88.43)
33 (9.79)
6 (1.78)
27,268 (83.62)
3,751 (11.50)
1,591 (4.880
951 (88.38)
108 (10.04)
17 (1.58)
28,219 (83.77)
3,859 (11.46)
1,608 (4.770
Fever
No
Yes
Missing
8,128 (53.33)
7,054 (46.29)
58 (0.38)
294 (39.78)
436 (59.000
9 (1.22)
10,476 (60.31)
6,698 (38.56)
196 (1.13)
182 (54.01)
154 (45.70)
1 (0.30)
18,604 (57.05)
13,752 (42.17)
254 (0.78)
476 (44.24)
590 (54.83)
10 (0.93)
19,080 (56.64)
14,342 (42.58)
264 (0.78)
Headache
No
Yes
Missing
12,945 (84.94)
2,153 (14.13)
142 (0.93)
644 (87.14)
80 (10.83)
15 (2.03)
12,489 (71.90)
4,660 (26.83)
221 (1.27)
294 (87.24)
41 (12.17)
2 (0.59)
25,434 (77.99)
6,813 (20.89)
363 (1.11)
938 (87.17)
121 (11.25)
17 (1.58)
26,372 (78.29)
6,934 (20.58)
380 (1.13)
Joint pain
No
Yes
Missing
14,864 (97.53)
164 (1.080
212 (1.39)
714 (96.62)
11 (1.49)
14 (1.89)
15,844 (91.21)
446 (2.57)
1,080 (6.22)
326 (96.74)
2 (0.59)
9 (2.67)
30,708 (94.17)
610 (1.87)
1,292 (3.96)
1,040 (96.65)
13 (1.21)
23 (2.14)
31,748 (94.25)
623 (1.85)
1,315 (3.90)
Malaise
No
1,972 (12.94)
114 (15.43)
5,163 (29.72)
42 (12.46)
7,135 (21.88)
156 (14.50)
7,291 (21.64)
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health
doi: 10.1136/bmjgh-2021-007076:e007076. 6 2021;BMJ Global Health, et al. Akande OW

Yes
Missing
84 (0.55)
13,184 (86.51)
11 (1.49)
614 (83.09)
124 (0.71)
12,083 (69.56)
0 (0.00)
295 (87.54)
208 (0.64)
25,267 (77.48)
11 (1.02)
909 (84.48)
219 (0.65)
26,176 (77.71)
Muscle pain
No
Yes
Missing
14,742 (96.73)
287 (1.88)
211 (1.38)
704 (95.26)
21 (2.84)
14 (1.89)
15,799 (90.96)
532 (3.06)
1,039 (5.98)
315 (93.47)
14 (4.15)
8 (2.37)
30,541 (93.66)
819 (2.51)
1,250 (3.83)
1,019 (94.70)
35 (3.25)
22 (2.04)
31,560 (93.69)
854 (2.54)
1,272 (3.78)
Nausea
No
Yes
Missing
13,927 (91.38)
1,152 (7.56)
161 (1.06)
678 (91.75)
48 (6.50)
13 (1.76)
15,847 (91.23)
1,228 (7.07)
295 (1.70)
314 (93.18)
15 (4.45)
8 (2.37)
29,774 (91.30)
2,380 (7.30)
456 (1.40)
992 (92.19)
63 (5.86)
21 (1.95)
30,766 (91.33)
2,443 (7.25)
477 (1.42)
Rapid breathing
No
Yes
Missing
13,879 (91.07)
203 (1.33)
1,158 (7.60)
600 (81.19)
57 (7.71)
82 (11.10)
13,245 (76.25)
124 (0.71)
4,001 (23.03)
315 (93.47)
16 (4.75)
6 (1.78)
27,124 (83.18)
327 (1.00)
5,159 (15.82)
915 (85.04)
73 (6.78)
88 (8.18)
28,039 (83.24)
400 (1.19)
5,247 (15.58)
Runny nose
No
Yes
10,843 (71.15)
4,247 (27.87)
615 (83.22)
112 (15.16)
10,208 (58.77)
6,945 (39.98)
252 (74.78)
80 (23.74)
21,051 (64.55)
11,192 (34.32)
867 (80.58)
192 (17.84)
21,918 (65.07)
11,384 (33.79)
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health
doi: 10.1136/bmjgh-2021-007076:e007076. 6 2021;BMJ Global Health, et al. Akande OW

Missing 150 (0.98) 12 (1.62) 217 (1.25) 5 (1.48) 367 (1.13) 17 (1.580 384 (1.14)
Sore throat
No
Yes
Missing
11,517 (75.57)
3,608 (23.67)
115 (0.75)
611 (82.68)
120 (16.24)
8 (1.08)
14,697 (84.61)
2,424 (13.96)
249 (1.43)
281 (83.38)
50 (14.84)
6 (1.78)
26,214 (80.39)
6,032 (18.50)
364 (1.12)
892 (82.90)
170 (15.80)
14 (1.30)
27,106 (80.47)
6,202 (18.41)
378 (1.12)
Vomiting
No
Yes
Missing
14,366 (94.27)
721 (4.73)
153 (1.00)
659 (89.17)
69 (9.34)
11 (1.49)
14,682 (84.53)
656 (3.78)
2,032 (11.70)
314 (93.18)
16 (4.75)
7 (2.08)
29,048 (89.08)
1,377 (4.22)
2,185 (6.70)
973 (90.43)
85 (7.90)
18 (1.67)
30,021 (89.12)
1,462 (4.34)
2,203 (6.54)
Loss of smell
No
Yes
Missing
12,491 (81.96)
1,775 (11.65)
974 (6.39)
627 (84.84)
29 (3.92)
83 (11.23)
13,958 (80.36)
3,129 (18.01)
283 (1.63)
309 (91.69)
19 (5.64)
9 (2.67)
26,449 (81.11)
4,904 (15.04)
1,257 (3.85)
936 (86.99)
48 (4.46)
92 (8.55)
27,385 (81.29)
4,952 (14.70)
1,349 (4.00)
Loss of taste
No
Yes
Missing
12,736 (83.57)
1,528 (10.03)
976 (6.40)
620 (83.90)
38 (5.14)
81 (10.96)
15,553 (89.54)
1,536 (8.84)
281 (1.62)
310 (91.99)
18 (5.34)
9 (2.67)
28,289 (86.75)
3,064 (9.40)
1,257 (3.85)
930 (86.43)
56 (5.20)
90 (8.36)
29,219 (86.74)
3,120 (9.26)
1,347 (4.00)
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health
doi: 10.1136/bmjgh-2021-007076:e007076. 6 2021;BMJ Global Health, et al. Akande OW

ARDS
No
Yes
Missing
14,935 (98.00)
99 (0.65)
206 (1.35)
680 (92.02)
48 (6.50)
11 (1.49)
13,328 (76.73)
48 (0.28)
3,994 (22.99)
313 (92.88)
16 (4.75)
8 (2.37)
28,263 (86.67)
147 (0.45)
4,200 (12.88)
993 (92.29)
64 (5.95)
19 (1.77)
29,256 (86.85)
211 (0.63)
4,219 (12.52)
Pneumonia
No
Yes
Missing
14,973 (98.25)
28 (0.18)
239 (1.57)
710 (96.08)
17 (2.30)
12 (1.62)
13,264 (76.36)
11 (0.06)
4,095 (23.58)
308 (91.64)
19 (5.64)
10 (2.97)
28,237 (86.59)
39 (0.12)
4,334 (13.29)
1,018 (94.61)
36 (3.35)
22 (2.04)
29,255 (86.85)
75 (0.22)
4,356 (12.93)
‡: 35,185 symptomatic cases only
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health
doi: 10.1136/bmjgh-2021-007076:e007076. 6 2021;BMJ Global Health, et al. Akande OW

BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any relianceSupplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health
doi: 10.1136/bmjgh-2021-007076:e007076. 6 2021;BMJ Global Health, et al. Akande OW
Recommended