
Dr CHARALAMPOS KAVVOURAS MD, Msc
ACHD Consultant Liverpool Heart and Chest Hospital, UK

Disclosures
No conflict of interest regarding this talk
Stress Test
Exercise stress testing preserve the integrity of the electromechanically response and provides valuable information regarding functional status
Provides links among
Symptoms
Cardiovascular workload
Wall motion abnormalities
Hemodynamic responses

Types of Exercise
Treadmill stress Echocardiography
Higher maximum heart rate (2-3 times the baseline)
Increase in BP
Increase in LV contractility
Functional aerobic capacity well defined
Bicycle Stress
Higher Blood pressure in supine position
Shorter duration of exercise /and lower HR due earlier leg fatigue
Allows better images and Doppler assessment

Pharmacological Stress
Dobutamine is a useful agent for evaluation of contractility and flow reserve (contraindicated in HCM)
Dodutamine HR X2-3 and Contractility >X4, mild BP increase ,causes less recruitment of venous blood volume
(LV volumes and wall stress less than exercise )
Vasodilator stress agents (dipyridamole, adenosine, regadenoson) are useful for wall motion abnormalities and coronary flow reserve
Contractile reserve LVEF >5% or GLS>2%
Flow reserve forward stroke volume > 20%
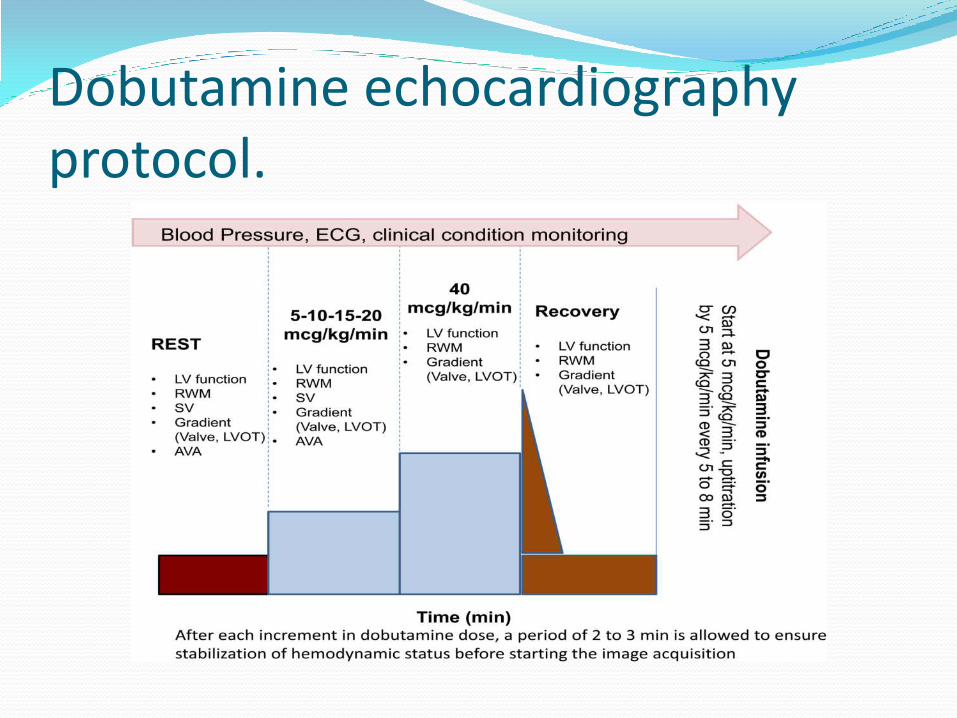
Dobutamine echocardiography protocol.

END POINTS Diagnostic end points
Max dose /workload
Target Heart rate
Obvious ECG changes
Obvious Echo changes
Severe Chest pain
Causes of test cessation
Intolerable symptoms
Muscular exhaustion
Hypertension >220mmHg systolic
Hypotension >40mmHg baseline
Arrhythmias/Frequent ectopics
(SVT /AF/NSVT/VT )
Positive test >1 criteria
Angina ,dyspnea, pre-syncope Ischemia >2mm ST depression or elevation Arrhythmia VT/AFib New regional wall motion abnormalities

Anatomical lesion Interventions Residual lesions
ASD
Surgical or percutaneous closure with a device
Residual shunt across the atrial septum
RV dilatation
RV dysfunction
Pulmonary hypertension
VSD
Surgical closure
Residual VSD
Aortic valve regurgitation
Tricuspid valve regurgitation
LV dilatation
LV dysfunction
Pulmonary hypertension
PDA
PDA closure either surgical or or with a device
percutaneous
LV dysfunction
Pulmonary hypertension
AVSD
ASD/VSD Closure
AV valve repair
Residual shunts across ASD/VSD
LV dysfunction
Pulmonary hypertension
AV valve regurgitation
LVOT Obstruction
TOF
Initial palliation and then
VSD closure
RV outflow tract muscle bundles resection
Patch enlargement of the RV outflow tract
Pulmonary valve replacement
Residual shunt across the VSD
Right Ventricle outflow tract or conduit
obstruction / stenosis
Pulmonary regurgitation /stenosis
Tricuspid regurgitation
Pulmonary hypertension
Aortic regurgitation
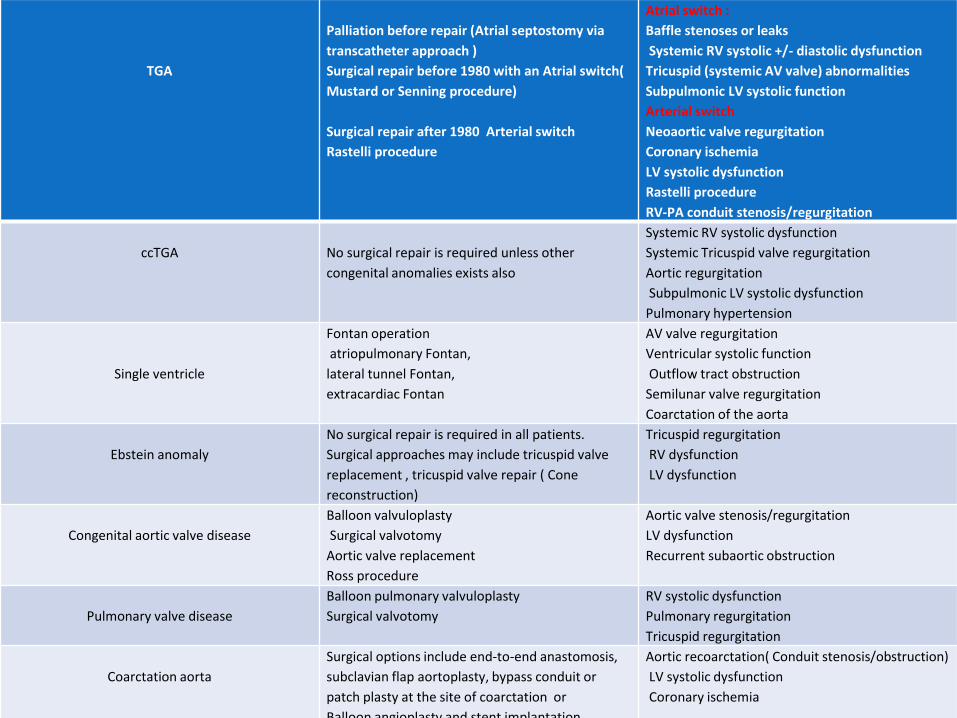
TGA
Palliation before repair (Atrial septostomy via
transcatheter approach )
Surgical repair before 1980 with an Atrial switch(
Mustard or Senning procedure)
Surgical repair after 1980 Arterial switch
Rastelli procedure
Atrial switch :
Baffle stenoses or leaks
Systemic RV systolic +/- diastolic dysfunction
Tricuspid (systemic AV valve) abnormalities
Subpulmonic LV systolic function
Arterial switch
Neoaortic valve regurgitation
Coronary ischemia
LV systolic dysfunction
Rastelli procedure
RV-PA conduit stenosis/regurgitation
ccTGA
No surgical repair is required unless other
congenital anomalies exists also
Systemic RV systolic dysfunction
Systemic Tricuspid valve regurgitation
Aortic regurgitation
Subpulmonic LV systolic dysfunction
Pulmonary hypertension
Single ventricle
Fontan operation
atriopulmonary Fontan,
lateral tunnel Fontan,
extracardiac Fontan
AV valve regurgitation
Ventricular systolic function
Outflow tract obstruction
Semilunar valve regurgitation
Coarctation of the aorta
Ebstein anomaly
No surgical repair is required in all patients.
Surgical approaches may include tricuspid valve
replacement , tricuspid valve repair ( Cone
reconstruction)
Tricuspid regurgitation
RV dysfunction
LV dysfunction
Congenital aortic valve disease
Balloon valvuloplasty
Surgical valvotomy
Aortic valve replacement
Ross procedure
Aortic valve stenosis/regurgitation
LV dysfunction
Recurrent subaortic obstruction
Pulmonary valve disease
Balloon pulmonary valvuloplasty
Surgical valvotomy
RV systolic dysfunction
Pulmonary regurgitation
Tricuspid regurgitation
Coarctation aorta
Surgical options include end-to-end anastomosis,
subclavian flap aortoplasty, bypass conduit or
patch plasty at the site of coarctation or
Balloon angioplasty and stent implantation
Aortic recoarctation( Conduit stenosis/obstruction)
LV systolic dysfunction
Coronary ischemia

Atrial septal defect
Chronic volume overload of the right ventricle
SE testing is feasible to evaluate the RV performance in both open and closed atrial septal defect
RV performance indirectly relates to SPAP at maximal exercise.
Increased SPAP at rest is associated with a worse outcome inpatients with closed atrial septal defects.

Ventricular septal defect
In patients with repaired VSD, chest pain may be related to the previous scar from the sternotomy or it can related to other musculoskeletal reasons. It can also be due to LV dysfunction.
SE is a valuable diagnostic tool to differentiate between the causes.
In cases of a residual small left-to-right shunt, chronic left ventricle volume overload may occur which can lead to chest pain.

Tetralogy of Fallot
Exercise echocardiography to study the RV and LV contractile reserve.
RV function can be studied measuring RVFAC, TAPSE and tissue Doppler velocities.
SE can also identify increased pressure gradients in patients with RV-PA conduits
RV dysfunction by stress echocardiography could be helpful at determining optimal timing for pulmonary valve replacement
Transposition of great arteries
Chronic systemic pressure load on the RV might lead to ventricular dysfunction, progressive TR, and HF
The evaluation of systolic performance is particularly difficult since no standardized methods have been established for systemic RV
SE may provide information about myocardial contractile reserve and the behaviour of the TR during stress

Univentricular hearts Assess Systemic LV
Assess Systemic RV
Doppler assessment of regurgitant or obstructive valvular and vascular lesions as exercise increases may be beneficial for surgical planning.

Treated coarctation of the aorta Subclinical hypertension.
Exercise-induced systemic arterial hypertension (defined as a peak systolic blood pressure >200 mmHg) was predictive of chronic hypertension in adults after coarctation repair.
Exercise testing can also be used to assess dynamic residual gradients after repaired CoA
ALCAPA
Incidence of 0.008%
Coronary steal phenomenon resulting in severe myocardial ischemia and dysfunction.
SE can be utilized to identify any systolic and diastolic dysfunction of the LV before and after surgery.

VALVULAR HEART DISEASES
Severe valve disease without symptoms
Non-severe valve disease with symptoms
Valve disease with low flow state.

VALVE DISEASES IN ACHD Repaired VSD TR/MR/AR
Repaired ASD TR
Repaired TOF PR /TR/AR
Repaired AVSD LAVVR /RAVVR
Ross Procedure AR/AS PR/PS
Ebstein anomaly TR
TGA(atrial switch) TR
TGA (arterial switch) AR/PR

VALVULAR HEART DISEASES.

ESC /ACC guidelines consider aortic valve replacement (AVR) class I indication, level of evidence B, in patients with severe AR and symptoms revealed by exercise testing
The increase in MR severity (≥1 grade),dynamic PH (SPAP ≥ 60 mmHg),the absence of contractile reserve (<5% increase in EF or <2% increment in global longitudinal strain) and a limited RV contractile recruitment (quantified by tricuspid annular plane systolic excursion (TAPSE) <19 mm) are all parameters of poor prognosis.
In patients with asymptomatic severe AS, exercise SE may uncover the development of symptoms, necessitating consideration for AVR. Increase in mean gradient is considered an indication for early elective AVR (Class IIb recommendation, level of evidence C in ESC guidelines) in asymptomatic patients with severe AS.
Pulmonary hypertension and pulmonary arterial pressure assessment
There are no validated diagnostic criteria for PH during exercise.
The term exercise-induced pulmonary hypertension should generally be avoided.
Careful attention to study quality, including signal acquisition and measurement, is needed to prevent overestimation or underestimation of PAP.
TRV is higher in 5-10% of normal outliers, patients over 50 years of age, obese individuals, and elite athletes.
Except in the above-stated conditions, TRV >3.1 m/sec and estimated PAP >43 mmHg may be abnormal and prompt further evaluation.
PH during stress echocardiography may be seen in pathologic conditions such as high-flow states, HFpEF, and valvular heart disease.
PH seen during stress echocardiography is most commonly due to left heart disease.
PH during stress echocardiography may be seen in patients at risk of or with subclinical PAH.

Congenital heart disease Indications for SE
ASD/VSD
Chest pain
SPAP
RV Contractile reserve
Diastolic function
Tetralogy Fallot
RV systolic and diastolic function
Evaluation of RV to pulmonary artery conduit
PR Severity
Optimal time for PVR
Transposition of great arteries
Myocardial Dysfunction
Baffle Stenosis
Single ventricle
Systolic and diastolic ventricle dysfunction
Assessment of contractile reserve
AV valve regurgitation
Valvular diseases
Severe valvular disease without symptoms
Non severe valvular disease with symptoms
Change of valvular severity with exertion+/- SPAP increase
ALCAPA
Myocardial Ischemia
Coarctation aorta
Assessment of blood pressure response
Gradient across repaired CoA
Assessment of LV contractile reserve
Pulmonary hypertension
Exercise induced PH / SPAP on exertion

RBHT Data 2013/2017 215 patients with congenital heart diseases
Stress echocardiography was normal in 78% and abnormal in 22%.
A positive SE was reported in 48/215 patients (22%).
commonest findings
New onset RWMA (n= 19, 35%)
Worsening valvular haemodynamic (n= 16, 22 %)
Worsening symptoms (n=6, 15%)
Increased gradient across the previous repaired coarctation (n=4, 20%)
Exercise induced PHT (n=3, 6%).

Condition Number of patients
Valve
Stenosis
Regurgitation
64
42
22
Transposition of great arteries (arterial switch) 38
TGA –Atrial switch
Mustard
Senning
ccTGA
20
16
4
2
Single ventricle
4
Coarctation 8
Ventricular septal defect 11
ALCAPA 10
ASD 10
Repaired AVSD 5

In all 48 patients after SE
optimize medical therapy due to stress induced symptoms
To predict the development symptoms or LV dysfunction in asymptomatic patients
In patients with mild or moderate valvular disease SE useful in elucidating the cause of symptoms.
Risk stratification
Help to define optimal time of intervention

CONCLUSION Stress echo is an emerging technique in patients with CHD.
The indications for the use of SE in patients with congenital heart disease are continuously evolving.
SE can be used in a consecutive manner for the assessment of a certain patient for
diagnosis,
risk stratification,
follow-up,
evaluation of treatment.
Following a negative study, patients can be reassured of the low-likelihood of a major adverse cardiovascular event.

THANK YOU
Recommended

















