Embed Size (px)
Citation preview

ECHO FOR ACHDHOW DOES IT DIFFER
Dr Haifa Abdul Latiff
Consultant Pediatric Cardiologist
Institut Jantung Negara Kuala Lumpur
Malaysia
7th TSC 2019

INTRODUCTION• Adults with CHD (ACHD) is a newly emerging, fast growing
population
• Improve survival rates of patients with complex CHD –early diagnosis, better treatment results and perioperative care
• 2 groups
– Long term complications from treatment received during childhood (e.g. Post TOF repair, Fontan)
– Presenting in adulthood with complications (defaulted treatment, undiagnosed) e.g. ASD with PHT

482
257
190
182
123
107
91
71
47
53
42
35
30
30
17
15
16
13
13
12
12
13
10
0 100 200 300 400 500 600
ASD
Post TOF Repair
PHT/Eisenmengers
VSD
Others
TOF
Post ASD Closure
Post VSD Closure
PDA
Pulmonary Stenosis
Ebstein's Anomaly
CRHD
ccTGA
Post Rastelli
Post Mustard/Senning
Post Fontan
Post PDA Closure
Post Ebstein Repair
AVSD
PAVSD
Aortic Stenosis
Normal Heart
Coarctation repair
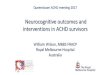
DIAGNOSIS ON REFERRAL
Adult Congenital Heart Disease
IJN NEW CASES - OUTPATIENT
3
OTHER DIAGNOSIS Frequency
CORTRIATRIUM 3
HOCM 5
KAWASAKI DISEASE 3
PAPVD 2
POST IAA REPAIR 2
POST PAPVD REPAIR 1
POST PAVM OCC. 2
POST ROSS / MR 1
TRICUSPID ATRESIA WITH PS 2
TRICUSPID STENOSIS 1
MITRAL VALVE PROLAPSE 5
POST TRUNCUS REPAIR 4
SINGLE VENTRICLE 4
POST COA REPAIR 4
POST GLENN SHUNT 3
POST A. SWITCH 9
PULMONARY ATRESIA 4
POST CAF OCCLUSION 1
VPC'S 1
POST PTBV - PS 2
POST MVR 3
UNIVENTRICULAR HEART 7
AORTIC REGURGITATION 2
PFO 8
PULMONARY EMBOLISM 1
POST ALCAPA 1
COMPLETE HEART BLOCK 2
TRICUSPID REGURGITATION 4
SINUS TACHYCARDIA 2
SVC 1
SVT 1
PULMONARY REGURGITATION 2
POST AVR 1
POST RSOV REPAIR 1
MITRAL REGURGITATION 4
PAIVS 2
CARDIOMYOPATHY 4
DORV-TGA 2
TGA 8
BICUSPID AORTIC VALVE 1
RIGHT ISOMERISM 1
ATRIAL ISOMERISM 1
TGA-IVS 1
DCRV 3
MITRAL STENOSIS 2
POST PPM 1
TRUNCUS ARTERIOSUS 1
INFUNDIBULAR STENOSIS 1
2008 – FEB 2018
ACHD CASES RANGE FROM SIMPLE TO COMPLEX LESIONSPOST SURGICAL REPAIR OR DEVELOPED COMPLICATIONS OF DISEASE Most common: ASD and post TOF repair
Courtesy Dr Geetha

5
8
26
20
45
60
172
429
427
0 50 100 150 200 250 300 350 400 450 500
Pulmonary Thrombosis/Embolism
PLE/PE
Others
Hemotypsis
Neurological
Infective Endocarditis
Heart Failure
PHT
Arrythmia
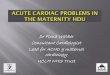
COMPLICATION
4
NONE = 3280
OUTPATIENT
Adult Congenital Heart Disease
Hypercyanotic spells 1
Thallasemia trial B 1
G6PD 1
Bilateral ankle edema 1
PPCM 1
Vocal cord dysfunction 3
Residual 2
Asthma 2
Right subclavian aneurysm 2
Mechanical 1
Mechanical valve dysfunction 1
LAA Clot 2
Gastritis 1
Others 1
PV preserved 1
Mediastinitis 1
Free flow PR 3
2008 – FEB 2018
Significant numbers (1/3) suffer from complications of CHD
Courtesy Dr Geetha

Roles of ECHO in ACHDACHD patients require a lifelong surveillance
Echocardiography is important first line in imaging assessment, easily available non invasive tool
• Determine the diagnosis (explain cause of symptoms) in newly referred patient
• Assess the status of previous intervention/surgery (?functioning)
• Look for potential complications of disease or previous surgery intervention -decide further diagnostic investigations (e.g. TOF PS/PA: free flow PR post TOF correction,
conduit stenosis, dilated aortic root and AR, RV dysfunction, ventricular failure)
• Progression of disease/complications (e.g. conduit stenosis, failure) that may require intervention or further investigation
• Response to treatment/intervention

ECHO in ACHD: how does it differ?• Nature of cardiac problem:
– Pediatric only structural and Adult only functional abnormality– ACHD: Structural and functional abnormalities
• Technical problem : challenging window, modified views– Chest deformity, scars– Artificial materials causing acoustic shadows – conduits, patch– Important structures not in usual position e.g. placed behind the sternum : RVOT in post
ASO, conduits/baffles – need modified echo view
• Type of Ventricular failure– Adults – mainly LVF. ECHO assessment, parameters and references are well established– ACHD – mainly RVF. Functional assessment involves a complex ventricular geometry - not
well established
• Normal reference value for echo parameters– Pediatric – Z score– ACHD? Outgrown pediatric age group but adult standard value base on normal heart

Standard acquisition protocol for TTE ACHDISACHD International J of Cardiology 272(2018) 77-83

Echocardiography for ACHD
Requires systematic approach
I. Anatomy : situs, position and connections of cardiac segments
II. Structural functions (stenosis, regurgitation)
III. Ventricular functions

I. Anatomical Assessment
ATRIA SITUS
CARDIAC POSITION
ATRIO-VENTRICULAR CONNECTION
VENTRICULO-ARTERIAL CONNECTION
At least once for a new patient unless therapeutic intervention performed
REQUIRES SWEEP TECHNIQUESNon conventional window /modified viewsInverted image for subcostal and apical 4 chamber

SEGMENTAL APPROACH: Atrial and Abdominal situs

SEGMENTAL APPROACH: Cardiac Position
Base-apex axis (ventricular apex): levocardia, mesocardia, dextrocardia
Cardiac apex is independent of cardiac situs
Position in the mediastinum : levoposition, dextroposition, mesoposition, can be determined by lung
pathology e.g. collapsed/hypoplastic lung, diaphragmatic hernia etc.

SEGMENTAL APPROACH: VA connection

SEGMENTAL APPROACH: VA connection

II. Structural functions
• Systemic veins – Anomalous drainage (heterotaxy) or post atrial switch/Glenn/Fontan circuit
• Pulmonary veins drainage : total/ partial anomalous pulmonary venous drainage
• Shunts and complications (PHT) : ASD, VSD, PDA
• AV valves abn. and function (stenosis/regurgitation): Ebstein’sanomaly, Cleft mitral valve, parachute etc, Common AVVs
• LV and RV Outflow tract stenosis/ regurgitation – native or conduit
• Pulmonary artery branches – stenosis, hypoplastic, disconnected
• Aorta – Right arch, aberrant subclavian, hypoplastic, coarctation

Pulmonary hypertension: look for secondary cause
TR gradient 144mmHgPR gradient 64mmHg
Large perimembranous VSD with bidirectional shunt

TR gradient 144mmHgPR gradient 64mmHg
Large PDA with birectional shunt

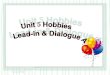
29 YEARS OLD HEART FAILUREECHO SEVERE ECCENTRIC MR. TR GRADIENT 68mmHg. Moderate PEPREOP ECHO NO CLEAR SUPRASTERNAL VIEWUNDERWENT MV REPAIR 10/6/2016
Post op persistent HPT4/7/2016
10/8/2019
ECHO SIGNS FOR COARCNON PULSATILE ABDOMINAL AORTA ON SC VIEW(SHORT AND LONG AXIS )SMALL ITHMUS - < NECK VESSEL

40 year old with cyanosis
VSD bidirectional shunt - Eisenmenger’s?

Tetralogy of Fallot

Post atrial switch complications
Severe TR due to RV failure or pathology of TV
Baffle leak

III. Ventricular functionsLV and RV systolic and diastolic functions
CHALLENGES:
• Complex ventricular geometry in ACHD:
– Right ventricle, Single ventricle, altered LV geometry (RV dysfunction, subpulmonary RV (CCTGA, post atrial switch)
– Standard method (M-Mode, Simpson) not reliable
• Normal reference values are based on adults with structurally normal heart
– Important to record serial measurements as patient own baseline and reference to monitor progress or changes in the echo parameters

Functional assessment for ACHD: challenges• RV systolic functions
– FAC (fractional area change) and TAPSE on 4CH view widely used, reproducible, easy to measure (represents longitudinal contractile function of RV) . TAPSE has prognostic value for Eisenmenger’s but angle dependent, may be influence by TR, abn. RV geometry, recent surgical procedures
– 3DE for function, volume – cannot be utilized in severely dilated heart
– TDI & speckle for regional and global deformation – but its clinical implication in CHD remains to be elucidated
• Diastolic dysfunction– lack of reliable parameters (E:E’ may not be accurate in all CHD as reduced E’ may result of
localized surgical scarring in the septum or free wall rather than impaired global LV diastolic function).
– Lack of standard echo criterial for diastolic function in systemic RV at present

TOF free flow PR
Non functioning monocusp valveResidual PS/conduit stenosisBranch PA stenosis

Assessment of RV systolic function
Eur Heart J (2016)37:1182-1195

Altered LV geometry
29Years, 10 years Post Ebstein’s repairReliability of standard Simpson?

Adult: asymptomatic previously, pinkC/O palpitations on exertion
Congenitally Corrected Transposition of Great Arteries (CTGA)

CCTGA – assessment of systolic function
Speckle tracking (?for systemic RV)
Simpson ? reliable

Systemic RVCCTGA develops severe TR
Post TVREyeballing – RV dysfunction
AV discordance wit severe TRSystemic RV dysfunction or valve abnormality?
Fractional Area Change to measure RV systolic function

SUMMARY• Echocardiogram for ACHD patients is very challenging for adult and
pediatric cardiologists/CVTs
• Requires comprehensive assessment of cardiac morphology, physiology, pathophysiology and function a in all ACHD patients
• Systematic segmental analysis approach with ventricular function assessment using basic and advance echo modalities (e.g. speckle tracking, 3DE) is recommended in all patients
• A specialized ACHD echo specialist/echocardiographer trained in both adults and pediatric echo is important to complement ACHD program
• Plenty room for research in this field

Thank you