Immunotherapy in Hemato-Oncology
Markus G. ManzDirector Department of Hematology and Oncology, University Hospital Zurich
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
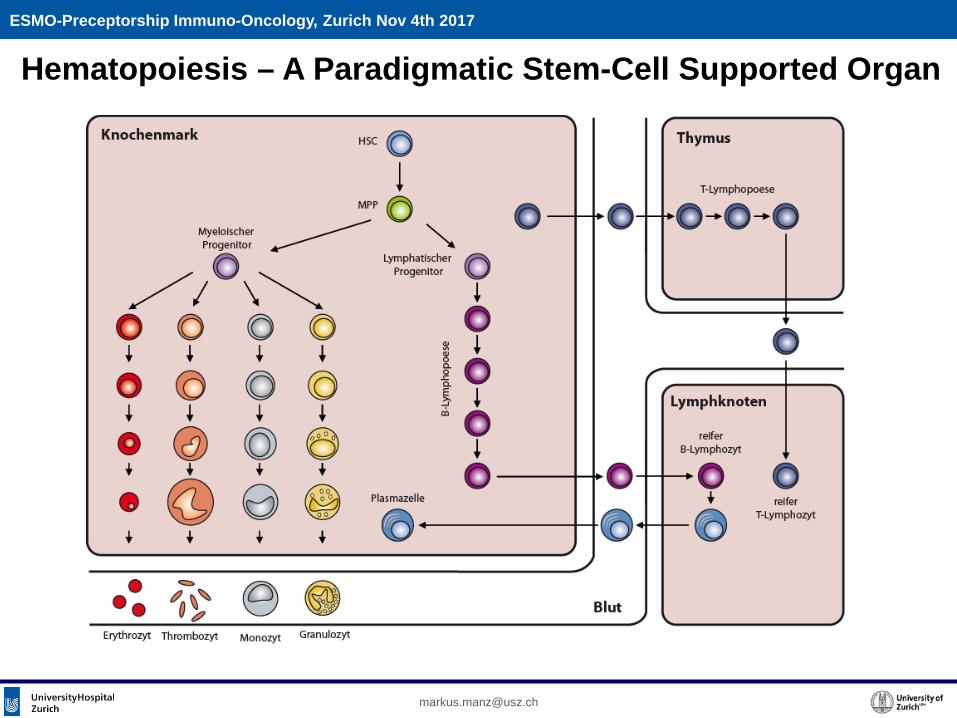
Hematopoiesis – A Paradigmatic Stem-Cell Supported Organ
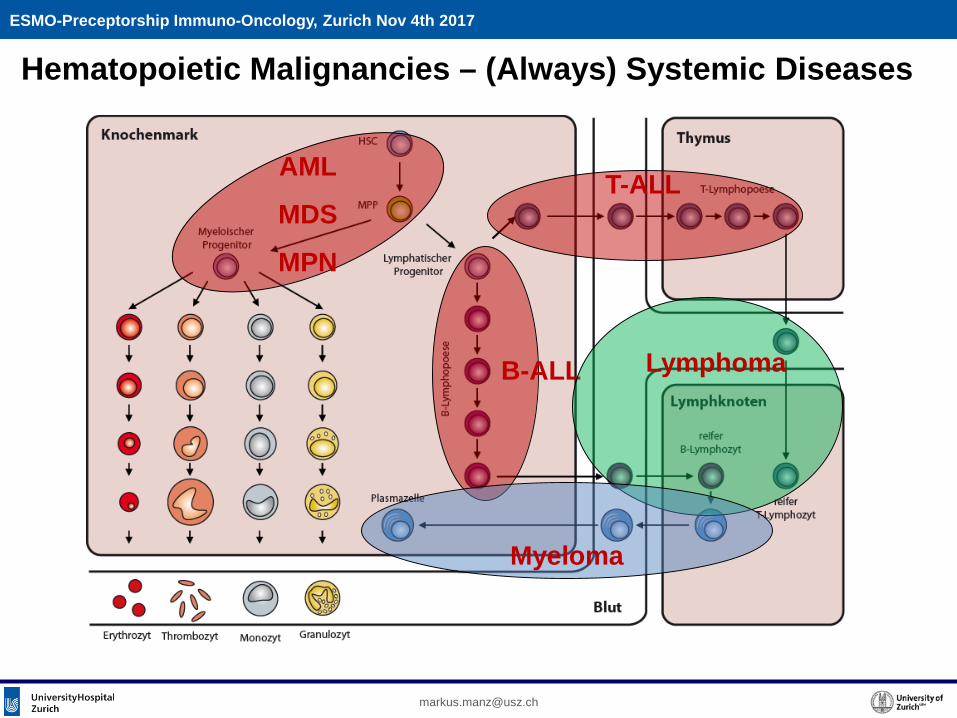
Hematopoietic Malignancies – (Always) Systemic Diseases
AML
MDS
MPN
B-ALL
T-ALL
Lymphoma
Myeloma
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
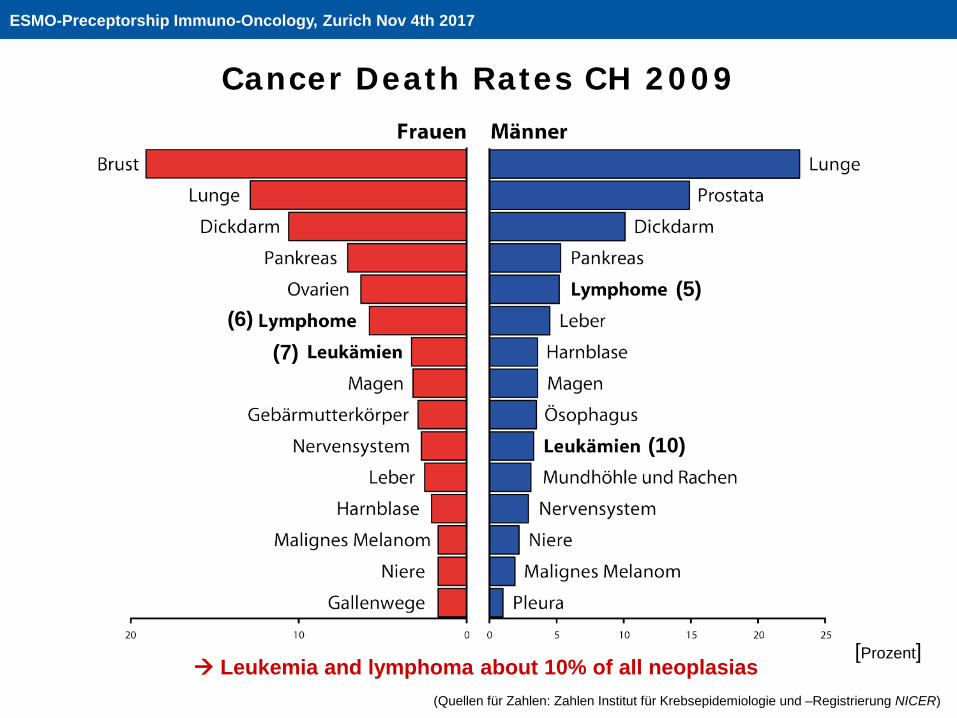
Cancer Death Rates CH 2009
(Quellen für Zahlen: Zahlen Institut für Krebsepidemiologie und –Registrierung NICER)
[Prozent]
(7)(6)
(10)
(5)
Leukemia and lymphoma about 10% of all neoplasias
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
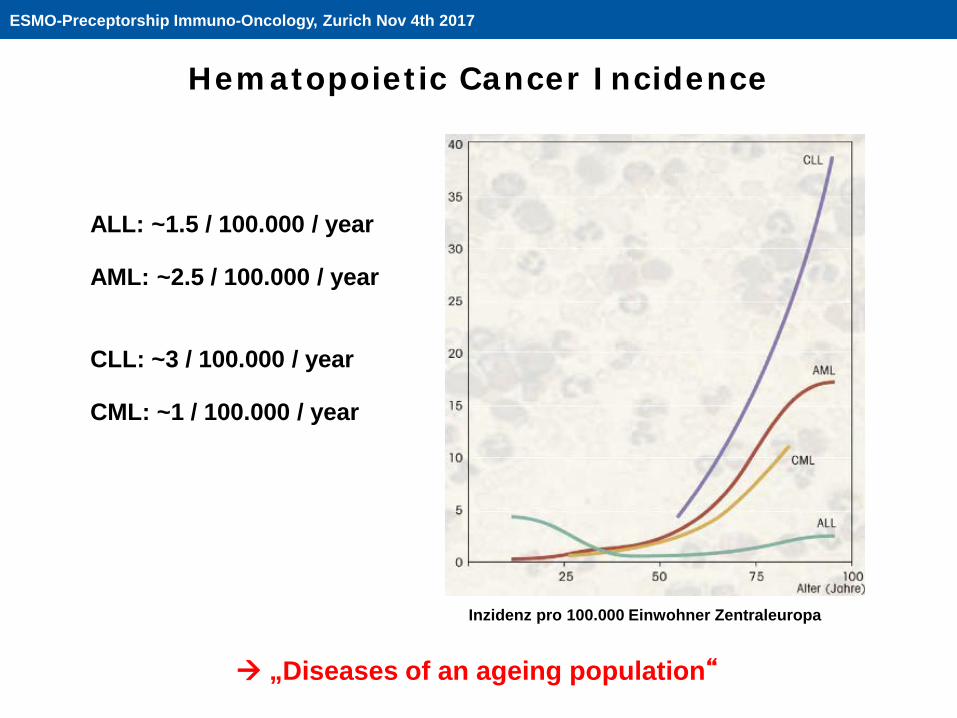
Inzidenz pro 100.000 Einwohner Zentraleuropa
ALL: ~1.5 / 100.000 / year
AML: ~2.5 / 100.000 / year
CLL: ~3 / 100.000 / year
CML: ~1 / 100.000 / year
„Diseases of an ageing population“
Hematopoietic Cancer Incidence
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
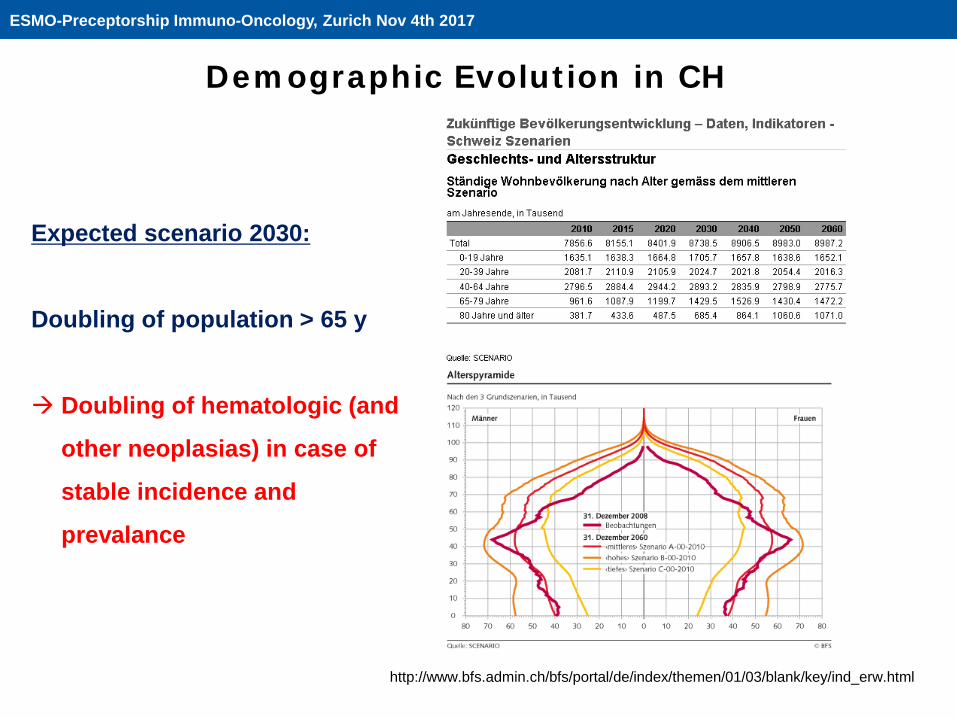
Expected scenario 2030:
Doubling of population > 65 y
Doubling of hematologic (and
other neoplasias) in case of
stable incidence and
prevalance
http://www.bfs.admin.ch/bfs/portal/de/index/themen/01/03/blank/key/ind_erw.html
Demographic Evolution in CH
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
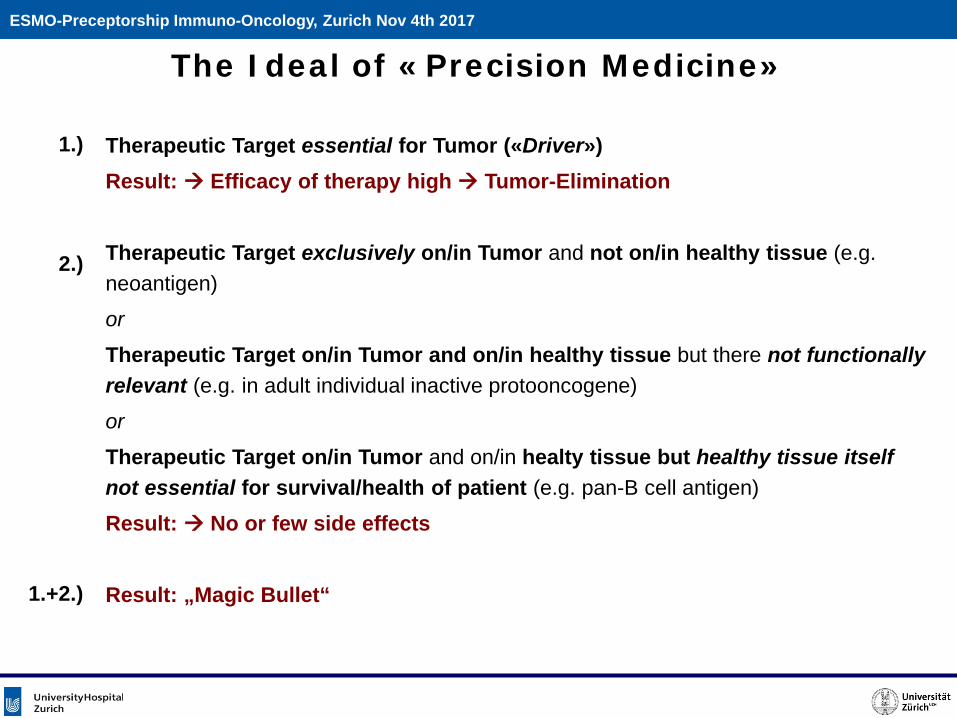
Therapeutic Target essential for Tumor («Driver»)Result: Efficacy of therapy high Tumor-Elimination
Therapeutic Target exclusively on/in Tumor and not on/in healthy tissue (e.g. neoantigen)
or
Therapeutic Target on/in Tumor and on/in healthy tissue but there not functionallyrelevant (e.g. in adult individual inactive protooncogene)
or
Therapeutic Target on/in Tumor and on/in healty tissue but healthy tissue itselfnot essential for survival/health of patient (e.g. pan-B cell antigen)
Result: No or few side effects
Result: „Magic Bullet“
1.)
2.)
1.+2.)
The Ideal of «Precision Medicine»ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
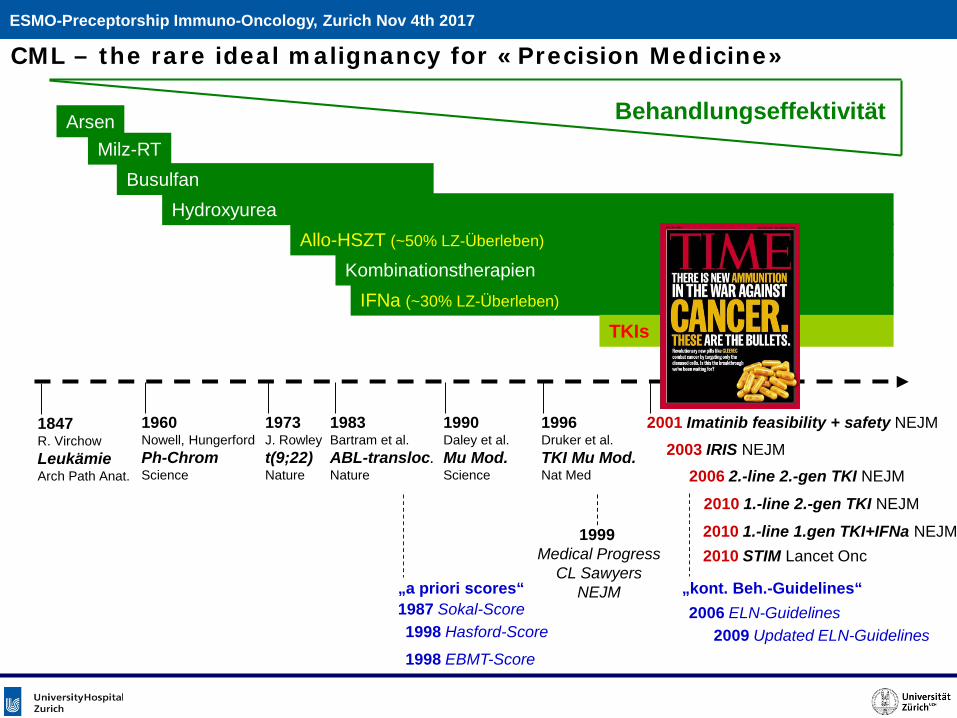
CML – the rare ideal malignancy for «Precision Medicine»
ArsenMilz-RT
BusulfanHydroxyurea
Allo-HSZT (~50% LZ-Überleben)
KombinationstherapienIFNa (~30% LZ-Überleben)
TKIs
Behandlungseffektivität
1847R. VirchowLeukämieArch Path Anat.
1960Nowell, HungerfordPh-ChromScience
1973J. Rowleyt(9;22)Nature
1983Bartram et al.ABL-transloc.Nature
1990Daley et al.Mu Mod.Science
1996Druker et al.TKI Mu Mod.Nat Med
2001 Imatinib feasibility + safety NEJM
2003 IRIS NEJM
2006 2.-line 2.-gen TKI NEJM
2010 1.-line 2.-gen TKI NEJM
2010 1.-line 1.gen TKI+IFNa NEJM2010 STIM Lancet Onc
1987 Sokal-Score1998 Hasford-Score
1998 EBMT-Score
2006 ELN-Guidelines2009 Updated ELN-Guidelines
„a priori scores“ „kont. Beh.-Guidelines“
1999 Medical Progress
CL SawyersNEJM
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
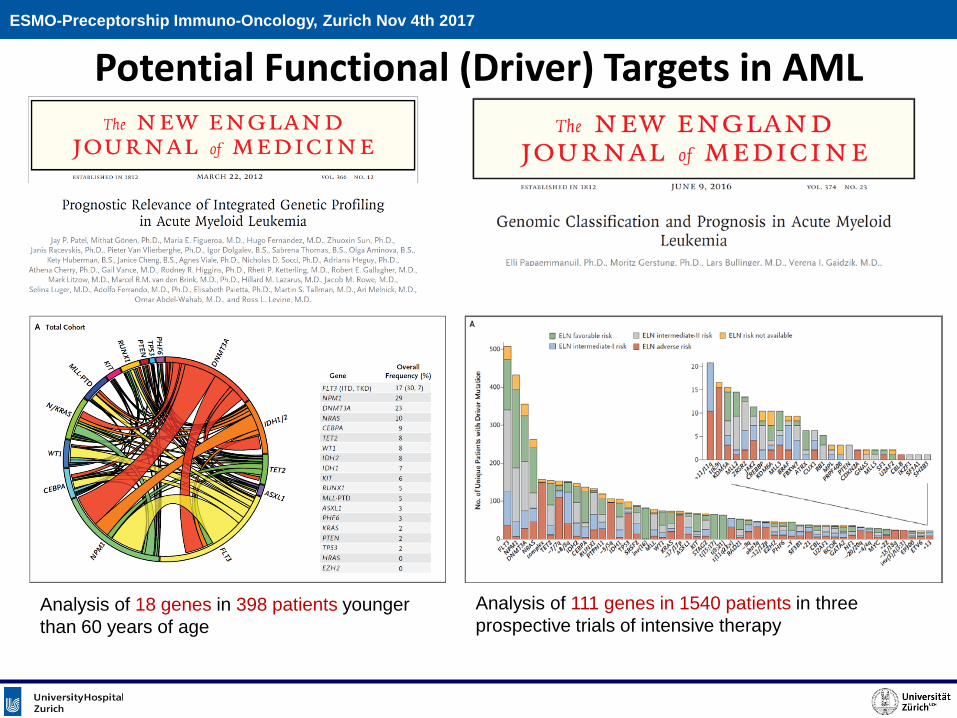
Potential Functional (Driver) Targets in AML
Analysis of 111 genes in 1540 patients in three prospective trials of intensive therapy
Analysis of 18 genes in 398 patients younger than 60 years of age
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
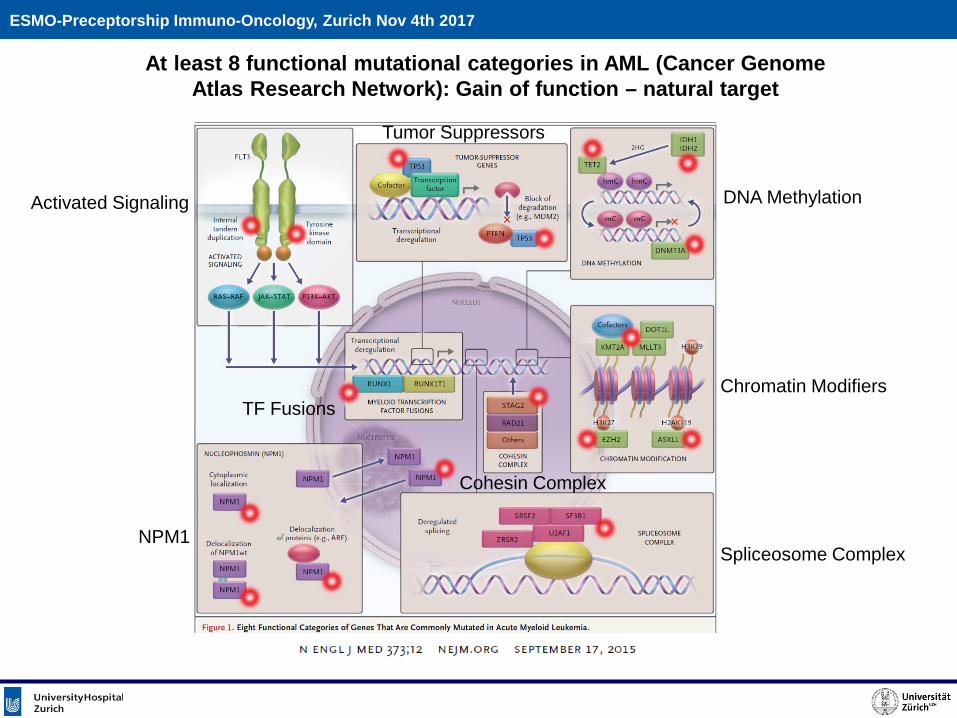
At least 8 functional mutational categories in AML (Cancer Genome Atlas Research Network): Gain of function – natural target
TF Fusions
Tumor Suppressors
DNA MethylationActivated Signaling
Chromatin Modifiers
Spliceosome ComplexNPM1
Cohesin Complex
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
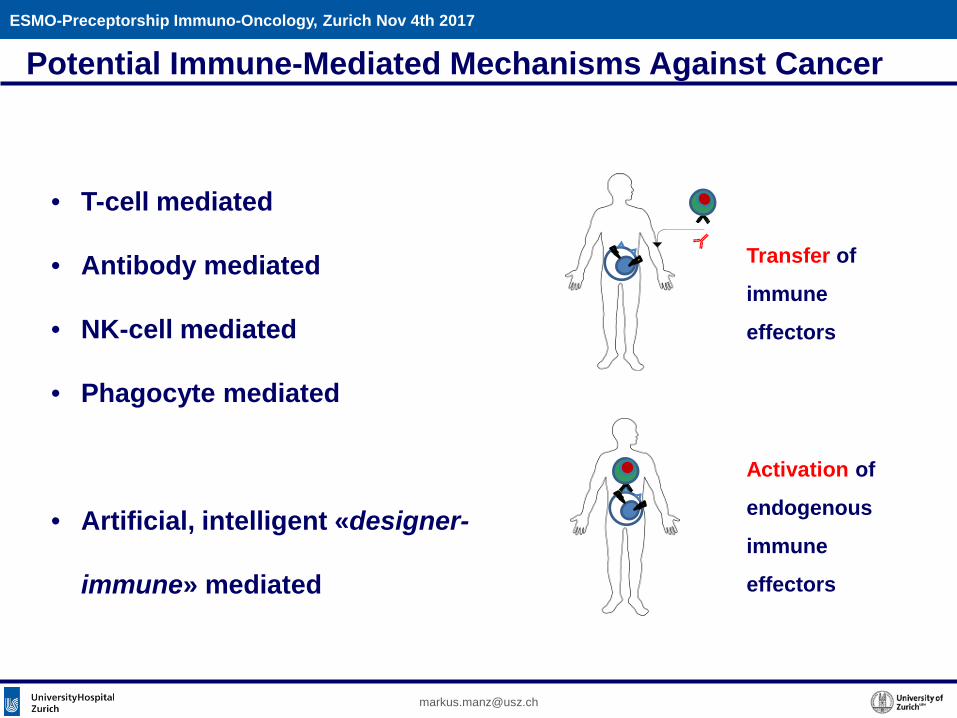
• T-cell mediated
• Antibody mediated
• NK-cell mediated
• Phagocyte mediated
• Artificial, intelligent «designer-
immune» mediated
Potential Immune-Mediated Mechanisms Against Cancer
Transfer of
immune
effectors
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
Activation of
endogenous
immune
effectors
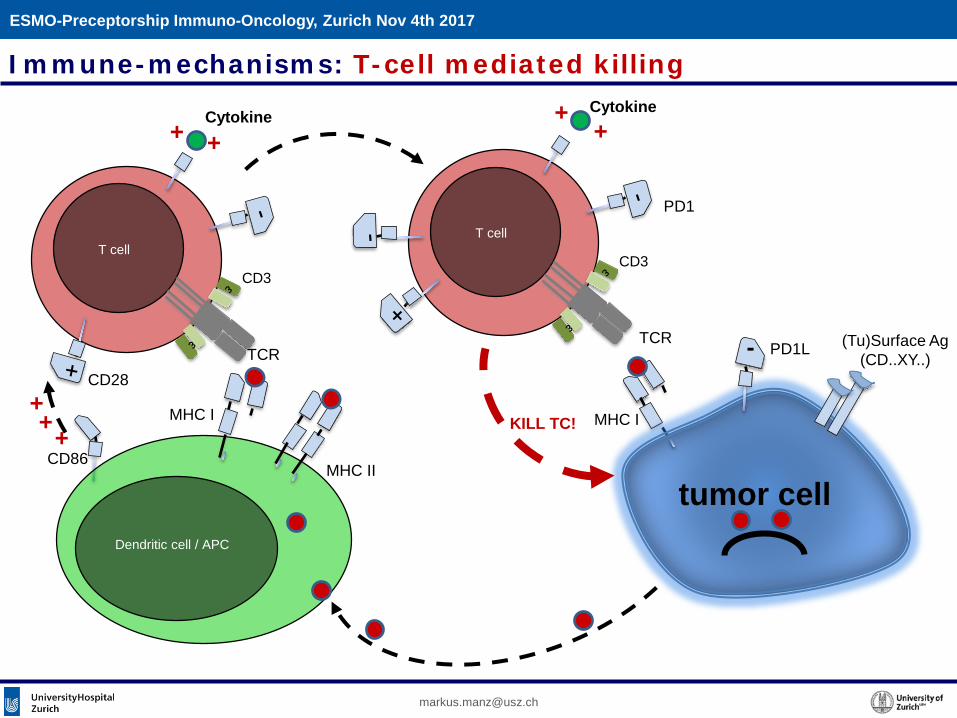
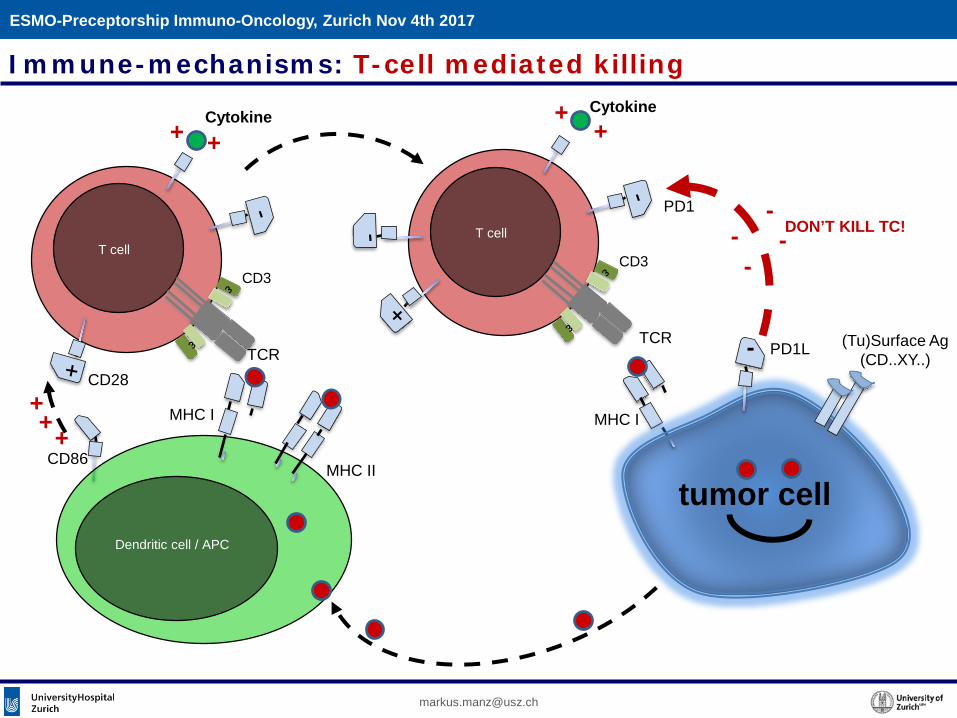
MHC I
tumor cell
T cell
TCR
CD3
(Tu)Surface Ag(CD..XY..)
Dendritic cell / APC
T cell
TCR
CD3++
+
Cytokine+ +
Cytokine++
-
PD1
PD1L
CD86
CD28
MHC II
MHC I KILL TC!
Immune-mechanisms: T-cell mediated killing
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
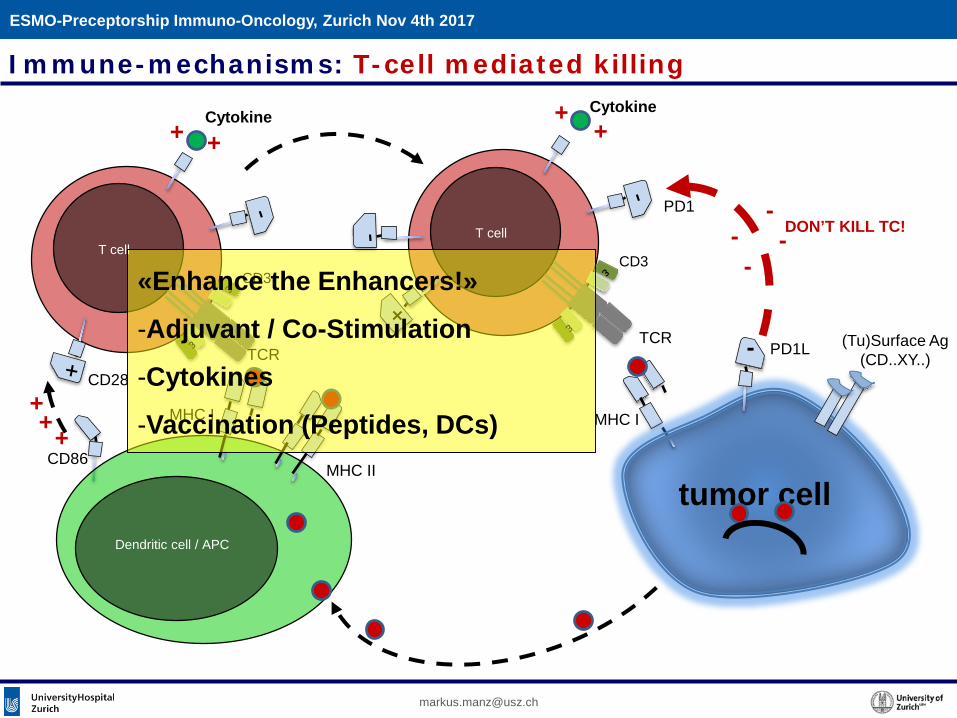
MHC I
tumor cell
T cell
TCR
CD3
(Tu)Surface Ag(CD..XY..)
Dendritic cell / APC
T cell
TCR
CD3++
+
Cytokine+ +
Cytokine++
-
--PD1
PD1L
--
CD86
CD28
MHC II
MHC I
DON’T KILL TC!
Immune-mechanisms: T-cell mediated killing
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
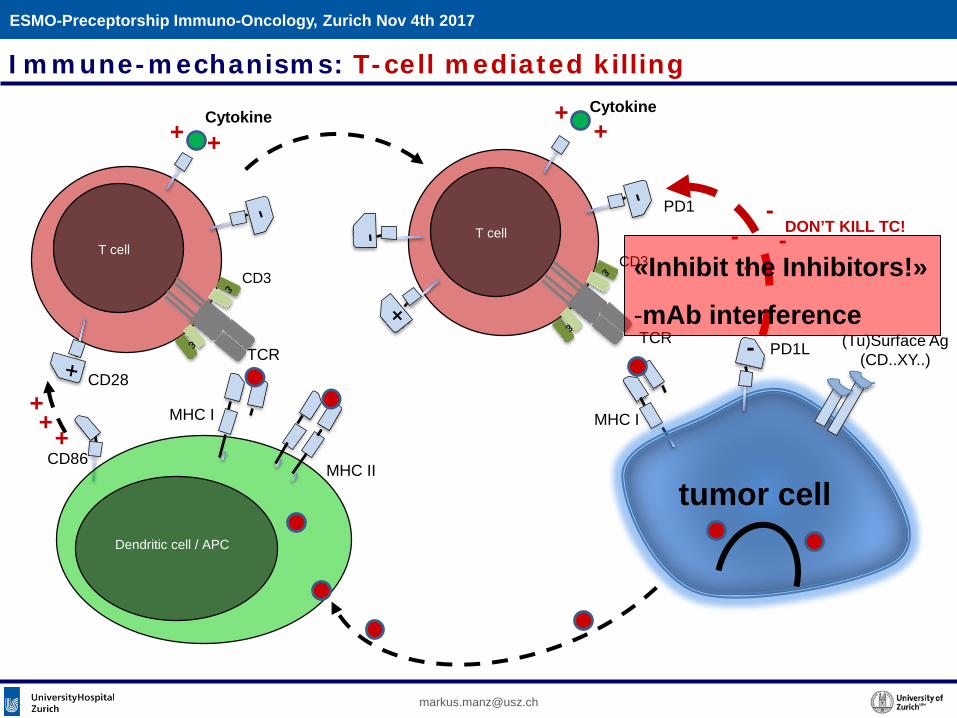
MHC I
tumor cell
T cell
TCR
CD3
(Tu)Surface Ag(CD..XY..)
Dendritic cell / APC
T cell
TCR
CD3++
+
Cytokine+ +
Cytokine++
-
--PD1
PD1L
--
CD86
CD28
MHC II
MHC I
DON’T KILL TC!
«Enhance the Enhancers!»
-Adjuvant / Co-Stimulation
-Cytokines
-Vaccination (Peptides, DCs)
Immune-mechanisms: T-cell mediated killing
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
MHC I
tumor cell
T cell
TCR
CD3
(Tu)Surface Ag(CD..XY..)
Dendritic cell / APC
T cell
TCR
CD3++
+
Cytokine+ +
Cytokine++
-
--PD1
PD1L
--
CD86
CD28
MHC II
MHC I
DON’T KILL TC!
«Inhibit the Inhibitors!»
-mAb interference
Immune-mechanisms: T-cell mediated killing
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
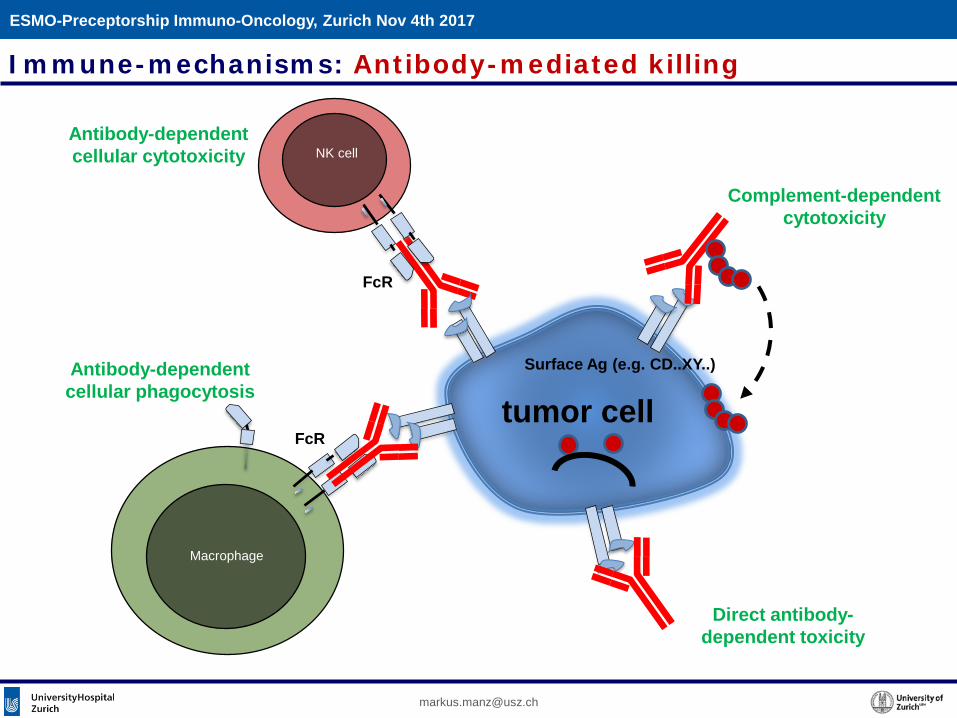
Immune-mechanisms: Antibody-mediated killing
tumor cell
NK cell
Surface Ag (e.g. CD..XY..)
Macrophage
FcR
FcR
Complement-dependentcytotoxicity
Antibody-dependentcellular cytotoxicity
Antibody-dependentcellular phagocytosis
Direct antibody-dependent toxicity
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
tumor cell
T cell
TCR
CD3
Surface Ag(CD..XY..)
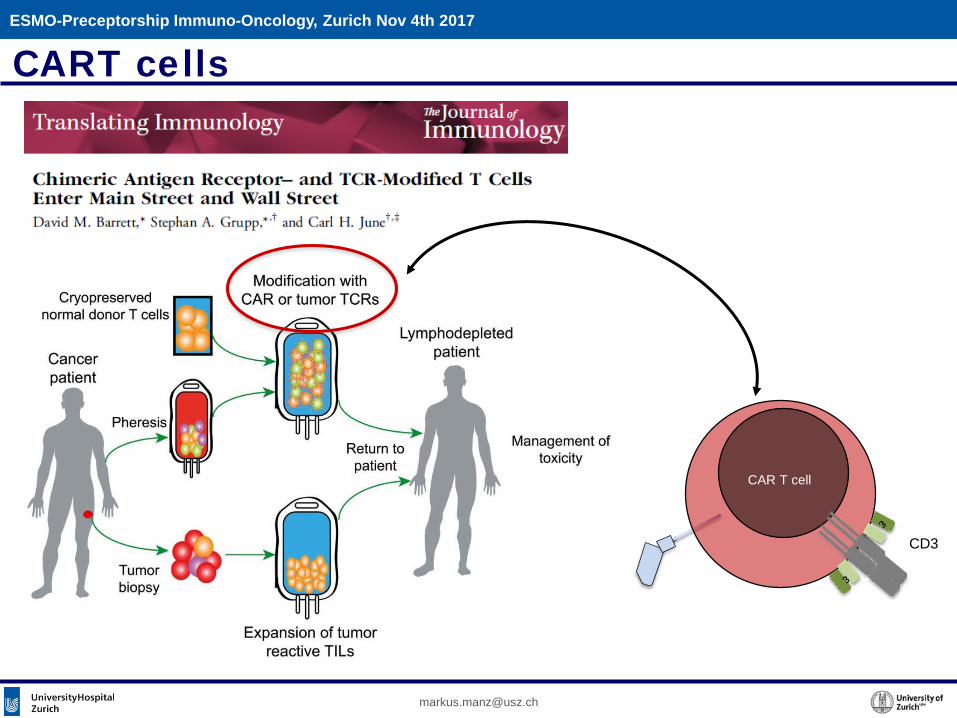
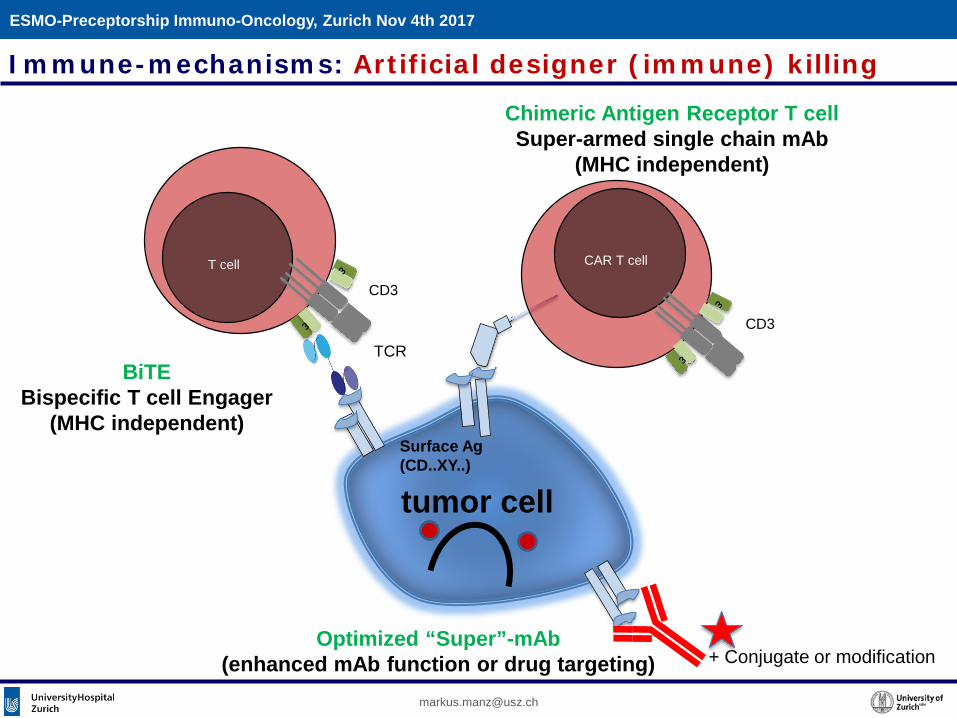
Immune-mechanisms: Artificial designer (immune) killing
CAR T cell
CD3
+ Conjugate or modification
Chimeric Antigen Receptor T cellSuper-armed single chain mAb
(MHC independent)
Optimized “Super”-mAb(enhanced mAb function or drug targeting)
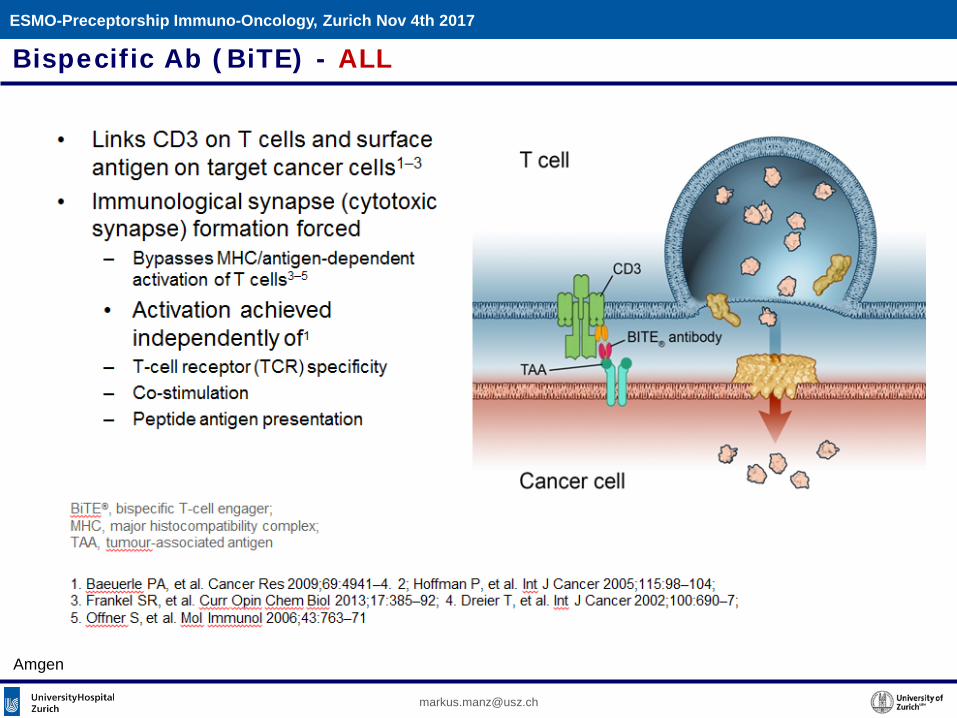
BiTEBispecific T cell Engager
(MHC independent)
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
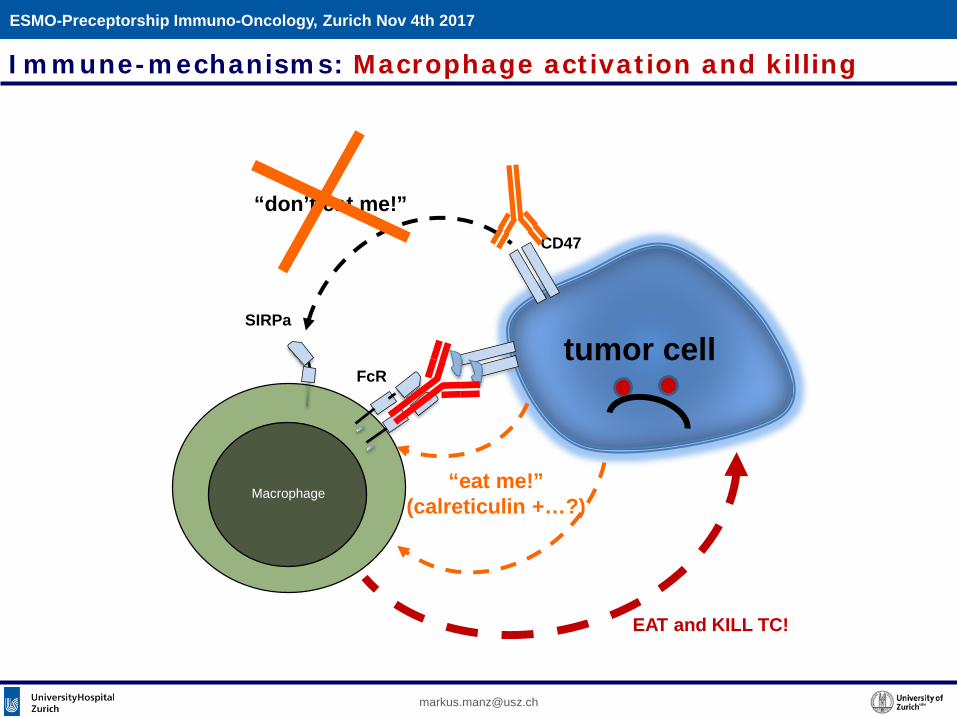
tumor cell
“don’t eat me!”
Macrophage
FcR
SIRPa
CD47
“eat me!”(calreticulin +…?)
Immune-mechanisms: Macrophage activation and killing
EAT and KILL TC!
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
Overview
Immunotherapy in Hemato-Oncology (examples)
• Allogeneic hematopoietic (stem) cell transplantation
• Checkpoint control (post-allo-HSCT, HD)
• Optimized monoclonal Abs (CLL, MM)
• Bispecific Abs (BiTE; ALL)
• CART cells (CD19 CART, ALL, MM; BCMA CART, MM)
• «eat me» control – CD47-SIRPa
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
Overview
Immunotherapy in Hemato-Oncology (examples)
• Allogeneic hematopoietic (stem) cell transplantation
• Checkpoint control (post-allo-HSCT, HD)
• Optimized monoclonal Abs (CLL, MM)
• Bispecific Abs (BiTE; ALL)
• CART cells (CD19 CART, ALL, MM; BCMA CART, MM)
• «eat me» control – CD47-SIRPa
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
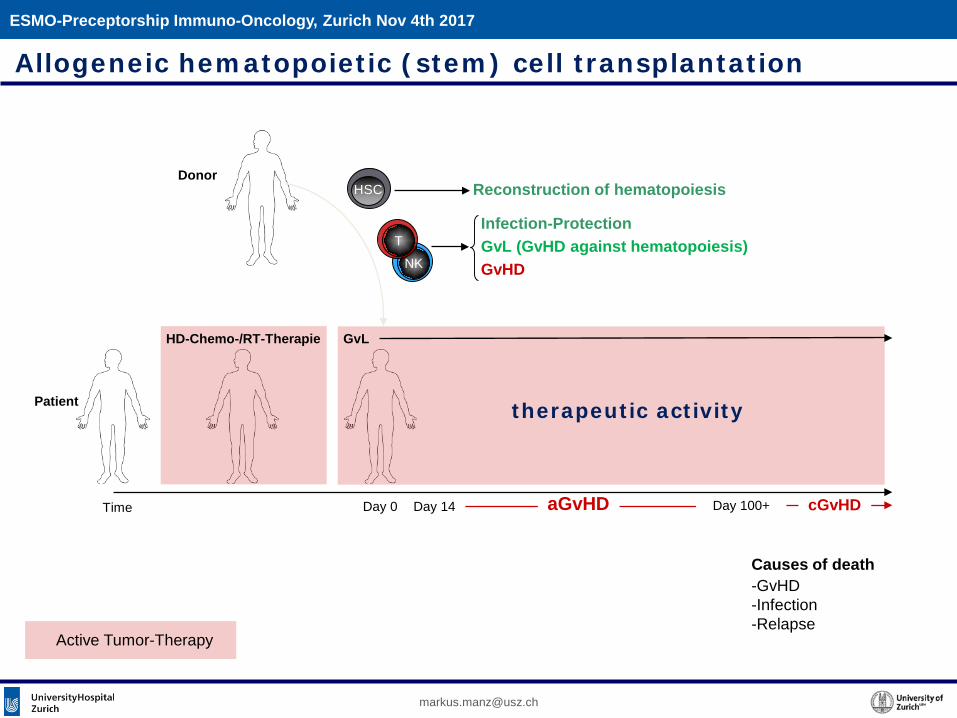
Allogeneic hematopoietic (stem) cell transplantation
NK
HD-Chemo-/RT-Therapie
Time
Patient
HSCDonor
T
Day 0
Reconstruction of hematopoiesis
Active Tumor-Therapy
Infection-ProtectionGvL (GvHD against hematopoiesis)GvHD
aGvHD cGvHD
Causes of death-GvHD-Infection-Relapse
Day 14
GvL
Day 100+
therapeutic activity
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
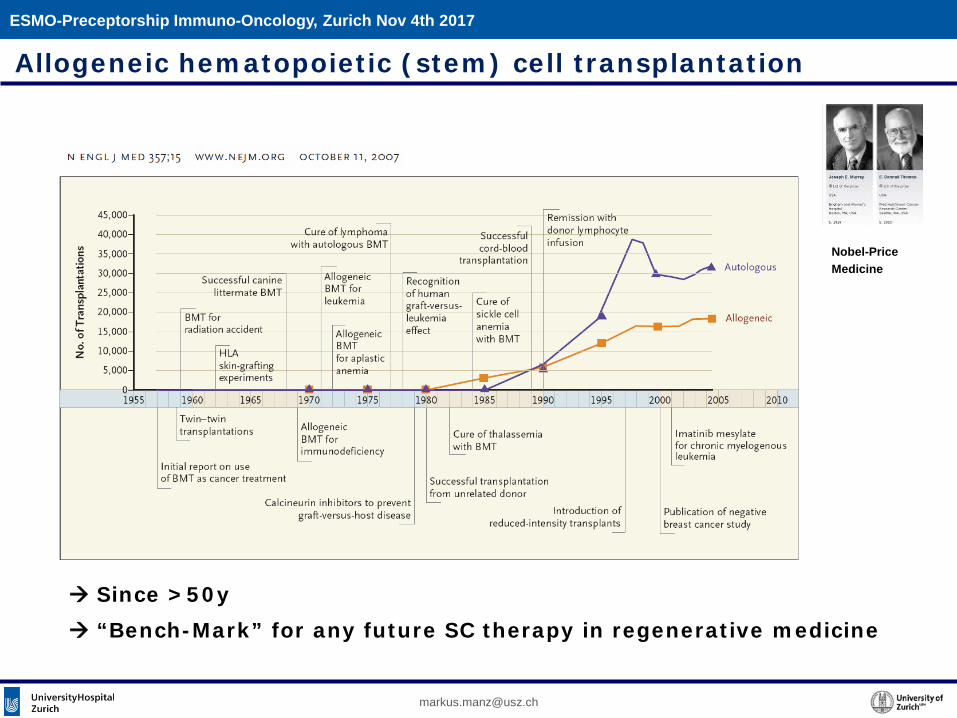
Allogeneic hematopoietic (stem) cell transplantation
Nobel-PriceMedicine
Since >50y “Bench-Mark” for any future SC therapy in regenerative medicine
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
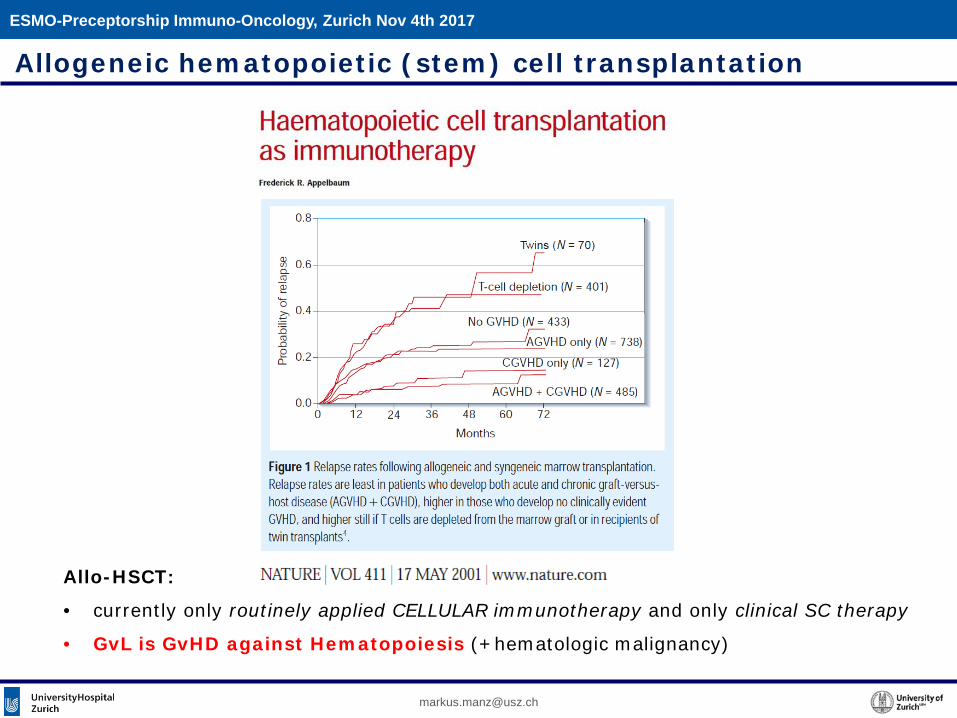
Allogeneic hematopoietic (stem) cell transplantation
Allo-HSCT:
• currently only routinely applied CELLULAR immunotherapy and only clinical SC therapy
• GvL is GvHD against Hematopoiesis (+hematologic malignancy)
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
Overview
Immunotherapy in Hemato-Oncology (examples)
• Allogeneic hematopoietic (stem) cell transplantation
• Checkpoint control (post-allo-HSCT, HD)
• Optimized monoclonal Abs (CLL, MM)
• Bispecific Abs (BiTE; ALL)
• CART cells (CD19 CART, ALL, MM; BCMA CART, MM)
• «eat me» control – CD47-SIRPa
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
Allogeneic hematopoietic (stem) cell transplantation
Ipilimumab – a CTLA4-blocking mAb
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
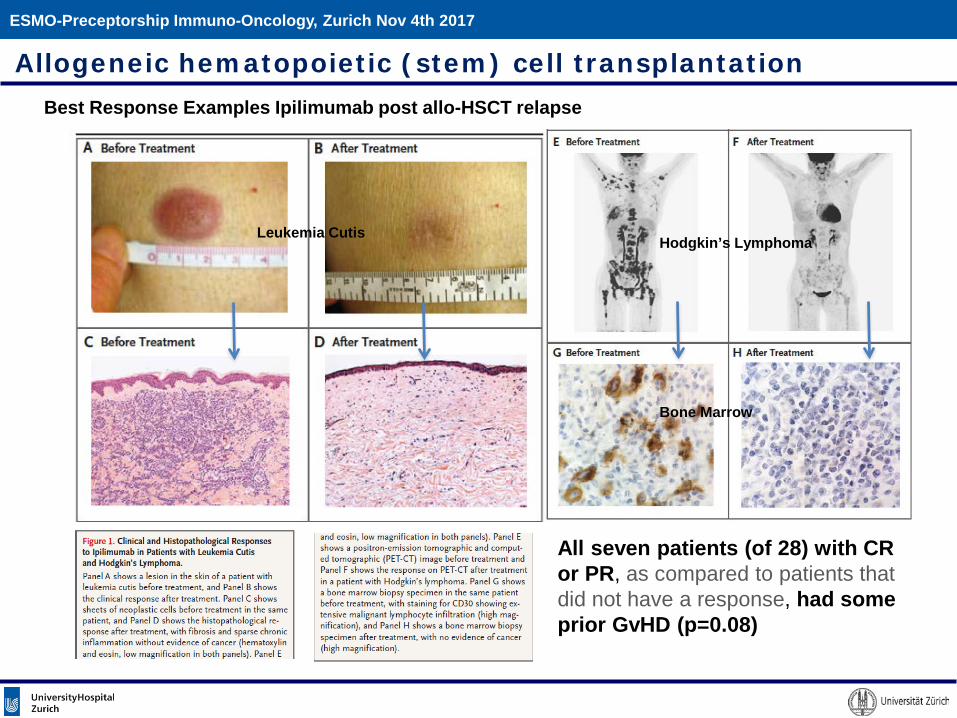
Best Response Examples Ipilimumab post allo-HSCT relapse
Hodgkin’s Lymphoma
Bone Marrow
Leukemia Cutis
Allogeneic hematopoietic (stem) cell transplantation
All seven patients (of 28) with CR or PR, as compared to patients thatdid not have a response, had someprior GvHD (p=0.08)
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
Checkpoint control - Hodgkin’s Lymphoma ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
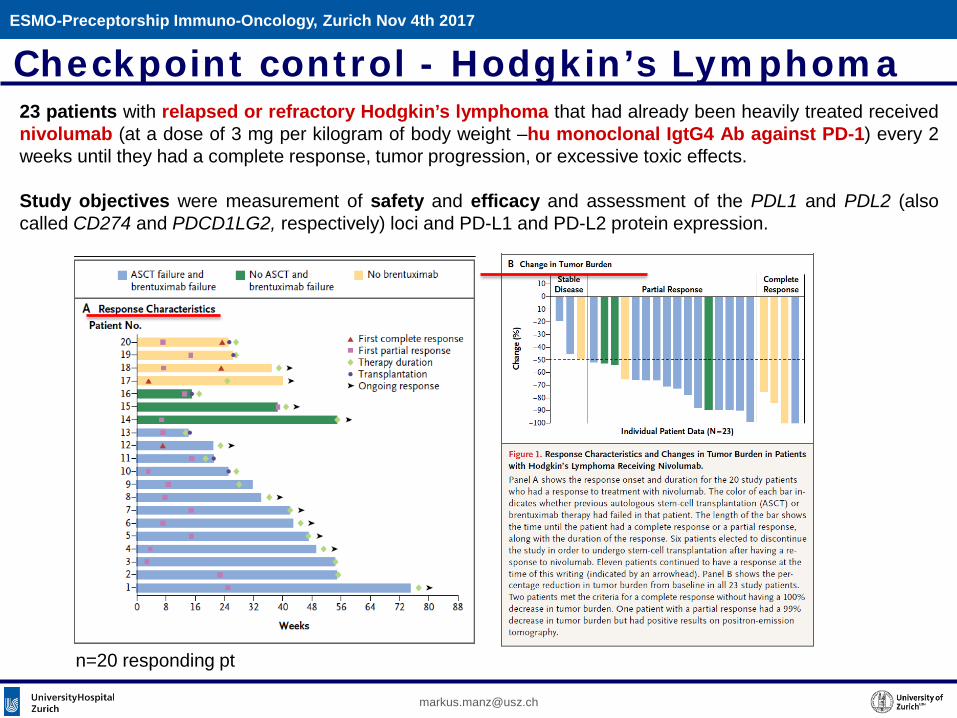
n=20 responding pt
23 patients with relapsed or refractory Hodgkin’s lymphoma that had already been heavily treated receivednivolumab (at a dose of 3 mg per kilogram of body weight –hu monoclonal IgtG4 Ab against PD-1) every 2weeks until they had a complete response, tumor progression, or excessive toxic effects.
Study objectives were measurement of safety and efficacy and assessment of the PDL1 and PDL2 (alsocalled CD274 and PDCD1LG2, respectively) loci and PD-L1 and PD-L2 protein expression.
Checkpoint control - Hodgkin’s Lymphoma
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
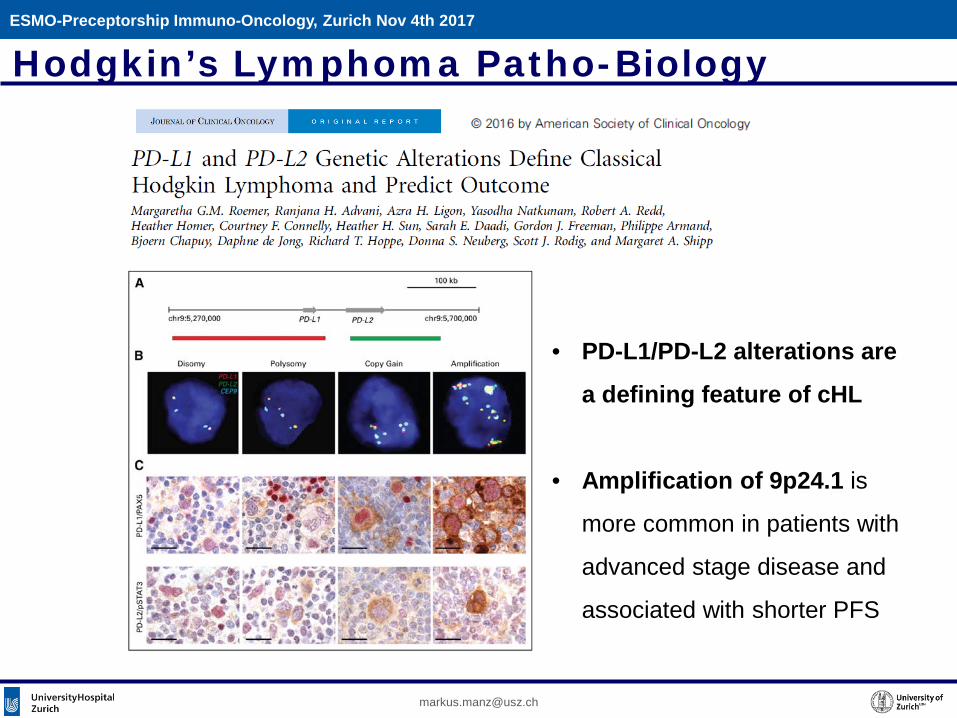
Hodgkin’s Lymphoma Patho-Biology
• PD-L1/PD-L2 alterations are
a defining feature of cHL
• Amplification of 9p24.1 is
more common in patients with
advanced stage disease and
associated with shorter PFS
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
Checkpoint inhibition in other Lymphoma(s)+MM?
Large B-cell lymphoma PD-L1 overexpression is not commonly seen on B NHL cells.ORR of 30-40% in heavily pretreated r/r DLBCL and also patients with r/r primary mediastinal large B-cell lymphoma
Mantle cell lymphoma: no larger pt group data available
Follicular lymphoma: Ten FL patients were included in a phase I study of nivolumab in a variety of r/r hematologic malignancies; the ORR was 40% and three responses were ongoing after a median follow-up of 91.4 weeks, which encouraged further clinical trials.
Chronic lymphocytic leukemia: Richter syndrome, showed an ORR of 21%
Other Lymphoma: T cell lymphoma and virus-related lymphomas (i.e. Epstein-Barr virus- or hepatitis C virus-related) might be susceptible, CNS Lymphoma, Testicular Lymphoma, Primary mediastinal B cell lymphoma
MM: Trials ongoing
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
Overview
Immunotherapy in Hemato-Oncology (examples)
• Allogeneic hematopoietic (stem) cell transplantation
• Checkpoint control (post-allo-HSCT, HD)
• Optimized monoclonal Abs (CLL, MM)
• Bispecific Abs (BiTE; ALL)
• CART cells (CD19 CART, ALL, MM; BCMA CART, MM)
• «eat me» control – CD47-SIRPa
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
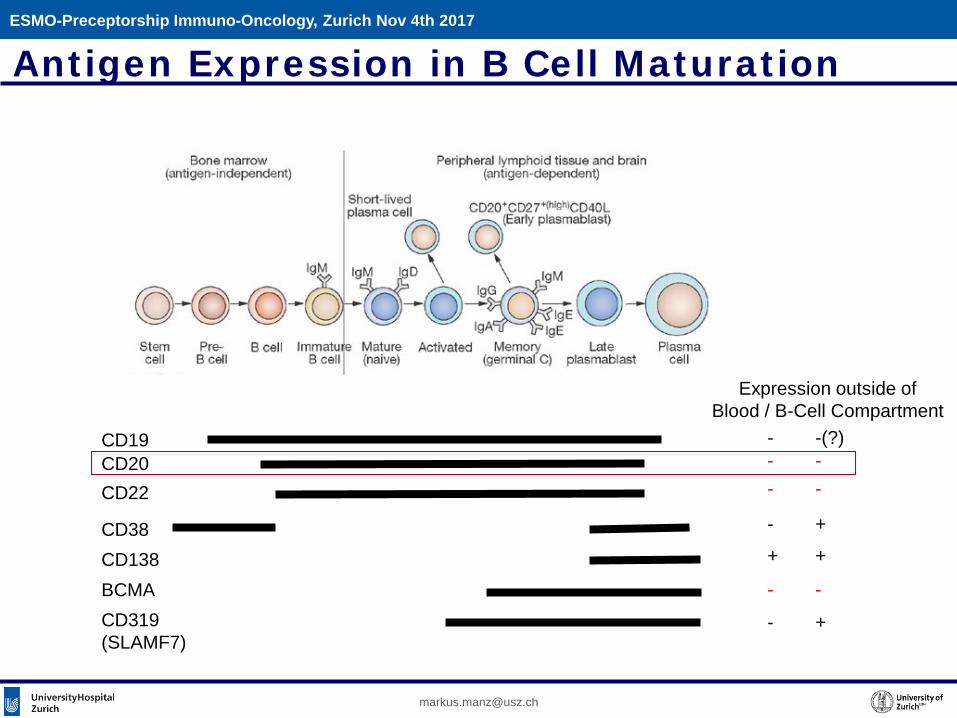
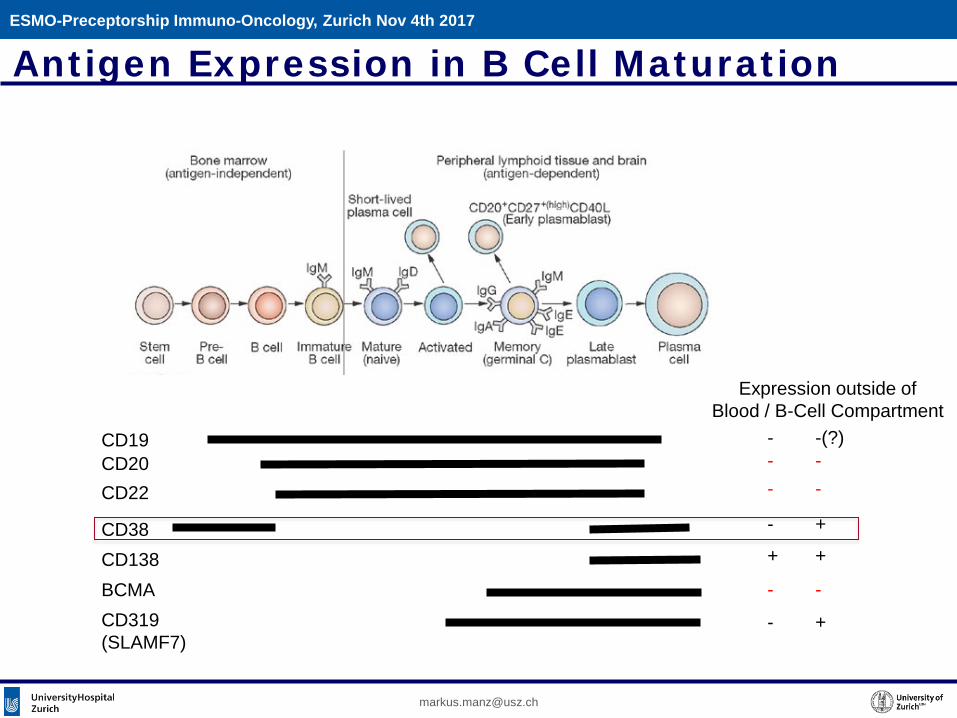
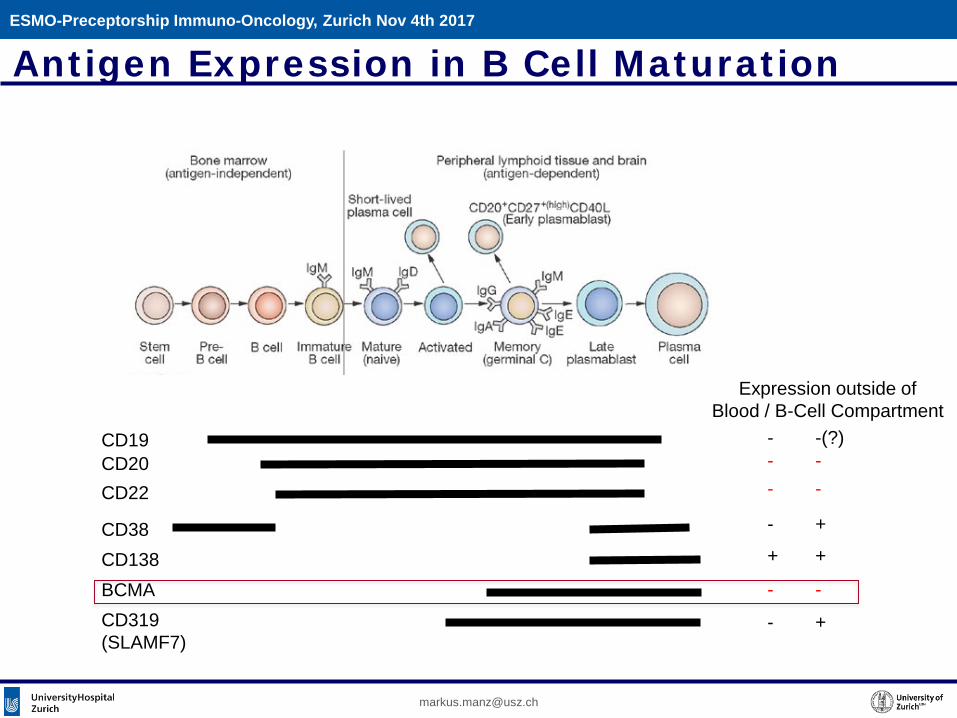
Antigen Expression in B Cell Maturation
CD19CD20CD22
CD38CD138BCMACD319(SLAMF7)
Expression outside ofBlood / B-Cell Compartment
- -(?)- -- -
- +
+ +
- -
- +
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
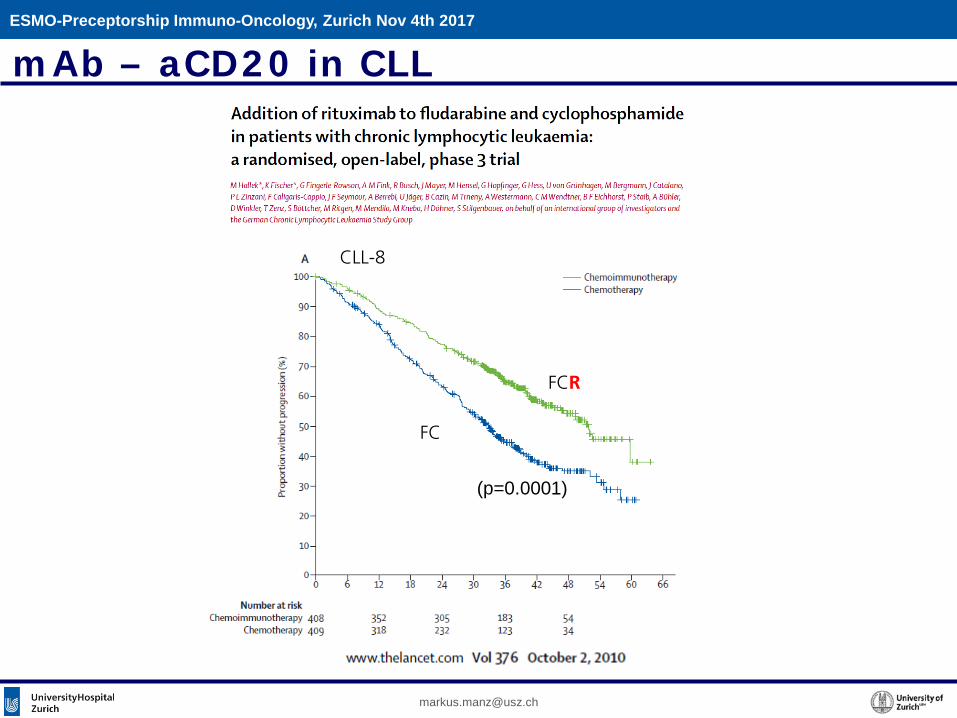
mAb – aCD20 in CLL
(p=0.0001)
FC
FCR
CLL-8
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
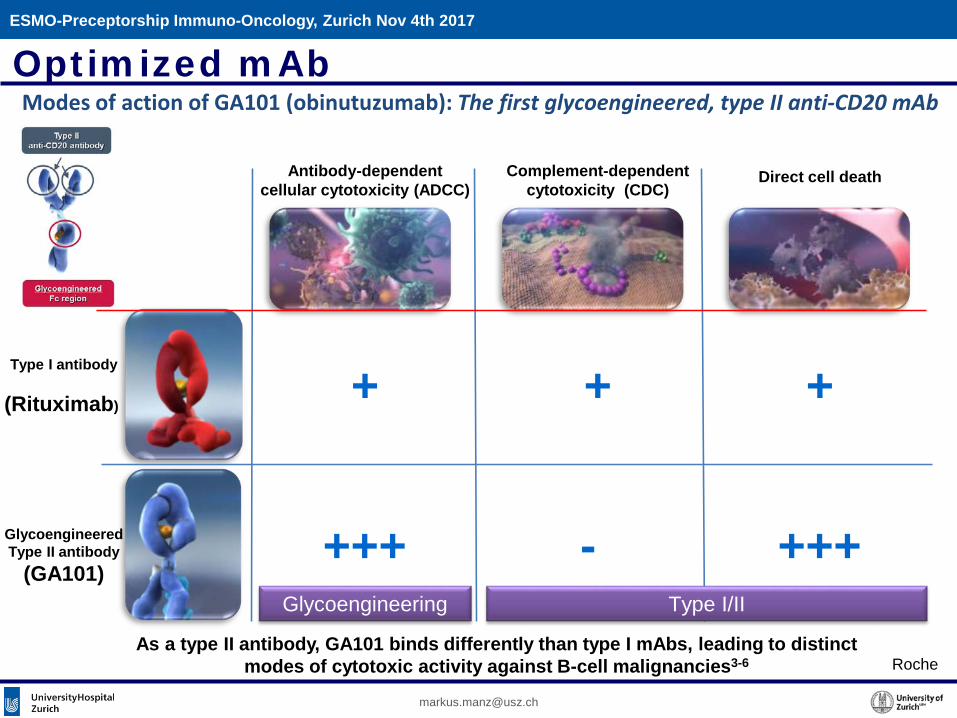
As a type II antibody, GA101 binds differently than type I mAbs, leading to distinct modes of cytotoxic activity against B-cell malignancies3-6
Glycoengineering Type I/II
Complement-dependentcytotoxicity (CDC)
Antibody-dependentcellular cytotoxicity (ADCC)
Direct cell death
++ +
+++-+++
Type I antibody
(Rituximab)
Glycoengineered Type II antibody
(GA101)
Modes of action of GA101 (obinutuzumab): The first glycoengineered, type II anti-CD20 mAbOptimized mAb
Roche
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
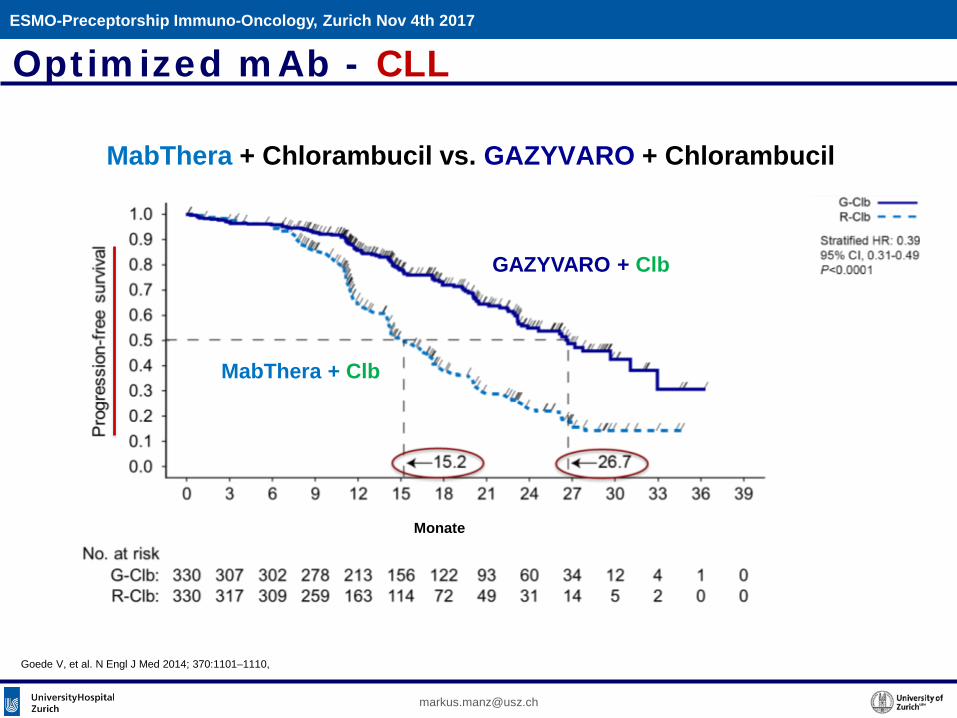
Goede V, et al. N Engl J Med 2014; 370:1101–1110,
Monate
MabThera + Clb
GAZYVARO + Clb
MabThera + Chlorambucil vs. GAZYVARO + Chlorambucil
Optimized mAb - CLL
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
Antigen Expression in B Cell Maturation
CD19CD20CD22
CD38CD138BCMACD319(SLAMF7)
- -(?)- -- -
- +
+ +
- -
- +
Expression outside ofBlood / B-Cell Compartment
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
Optimized mAb – Multiple Myeloma
“Daratumumab represents a landmark advance in the treatment of myeloma. It is likely to
be incorporated into the treatment of all stages of the disease over the next several years.”
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
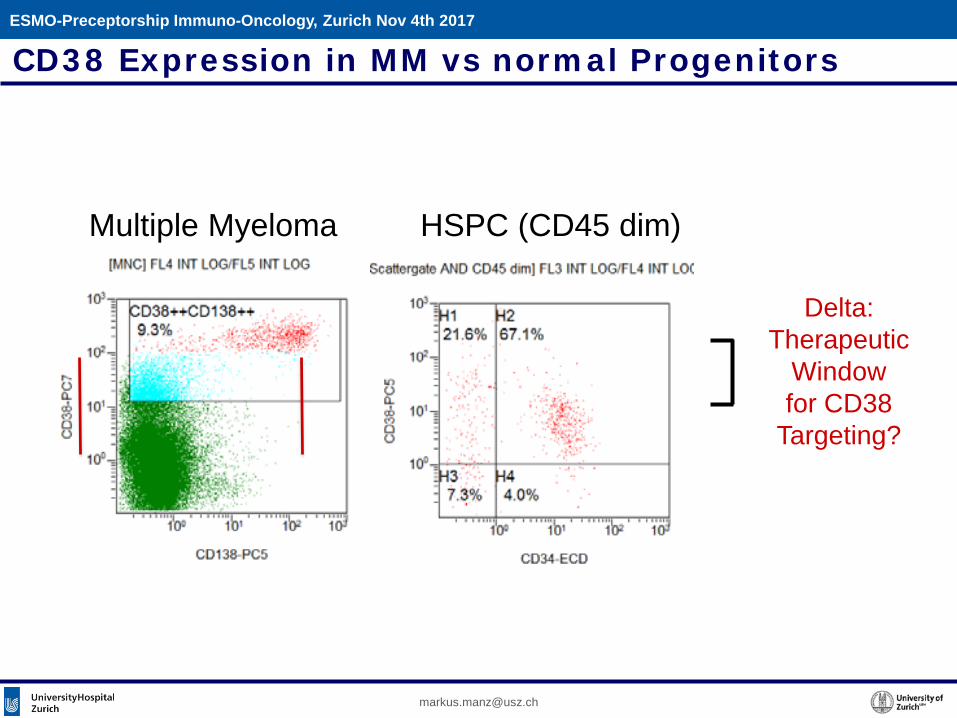
Multiple Myeloma HSPC (CD45 dim)
CD38 Expression in MM vs normal Progenitors
Delta:Therapeutic
Windowfor CD38
Targeting?
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
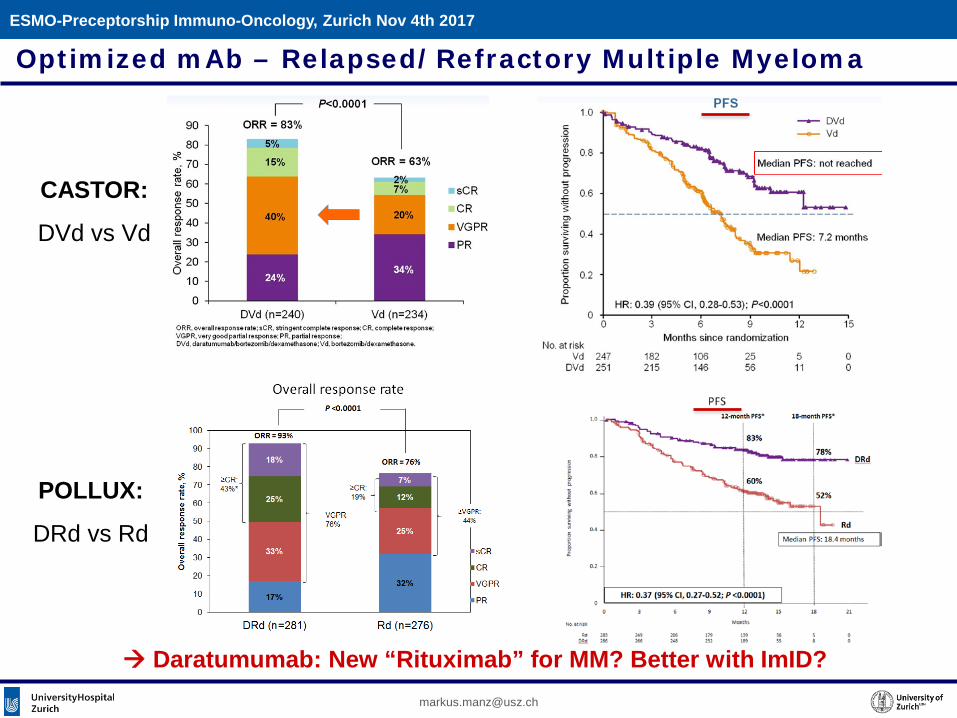
CASTOR:
DVd vs Vd
POLLUX:
DRd vs Rd
Daratumumab: New “Rituximab” for MM? Better with ImID?
Optimized mAb – Relapsed/Refractory Multiple MyelomaESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
Overview
Immunotherapy in Hemato-Oncology (examples)
• Allogeneic hematopoietic (stem) cell transplantation
• Checkpoint control (post-allo-HSCT, HD)
• Optimized monoclonal Abs (CLL, MM)
• Bispecific Abs (BiTE; ALL)
• CART cells (CD19 CART, ALL, MM; BCMA CART, MM)
• «eat me» control – CD47-SIRPa
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
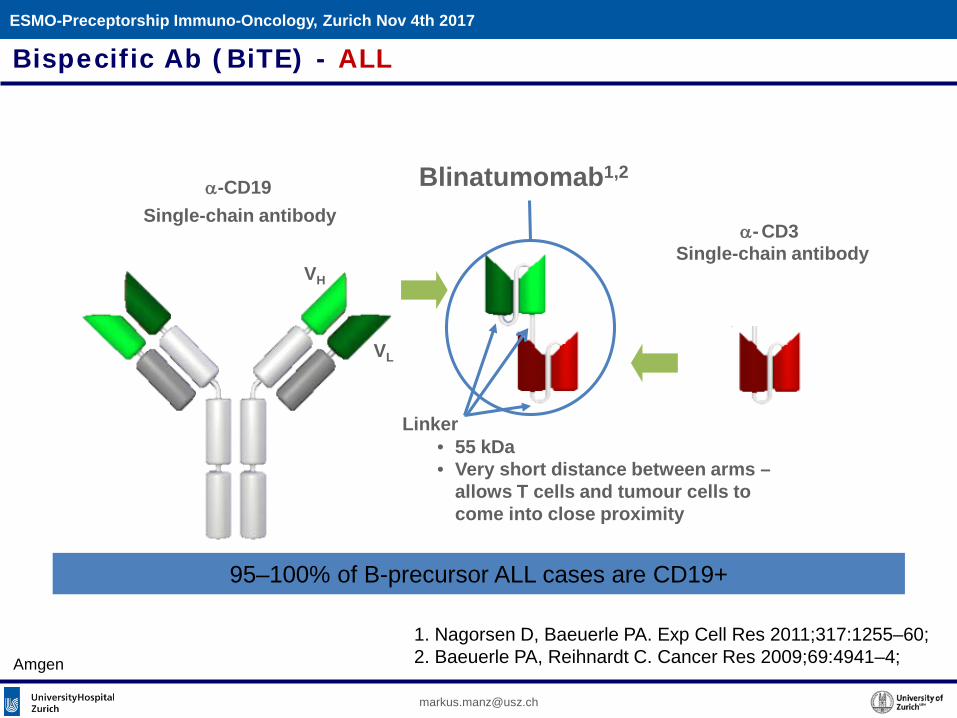
α-CD19 Blinatumomab1,2
Single-chain antibodyα-CD3
Single-chain antibody
Linker
VL
VH
• 55 kDa• Very short distance between arms –
allows T cells and tumour cells to come into close proximity
1. Nagorsen D, Baeuerle PA. Exp Cell Res 2011;317:1255–60;2. Baeuerle PA, Reihnardt C. Cancer Res 2009;69:4941–4;
Bispecific Ab (BiTE) - ALL
95–100% of B-precursor ALL cases are CD19+
Amgen
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
Amgen
Bispecific Ab (BiTE) - ALLESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
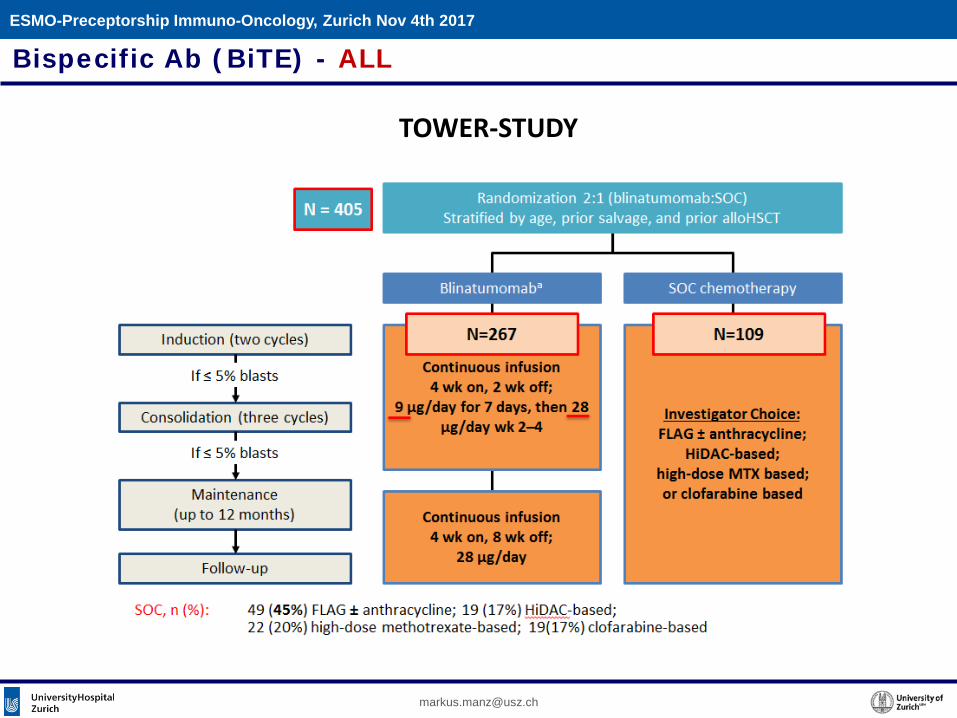
TOWER-STUDY
Bispecific Ab (BiTE) - ALLESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
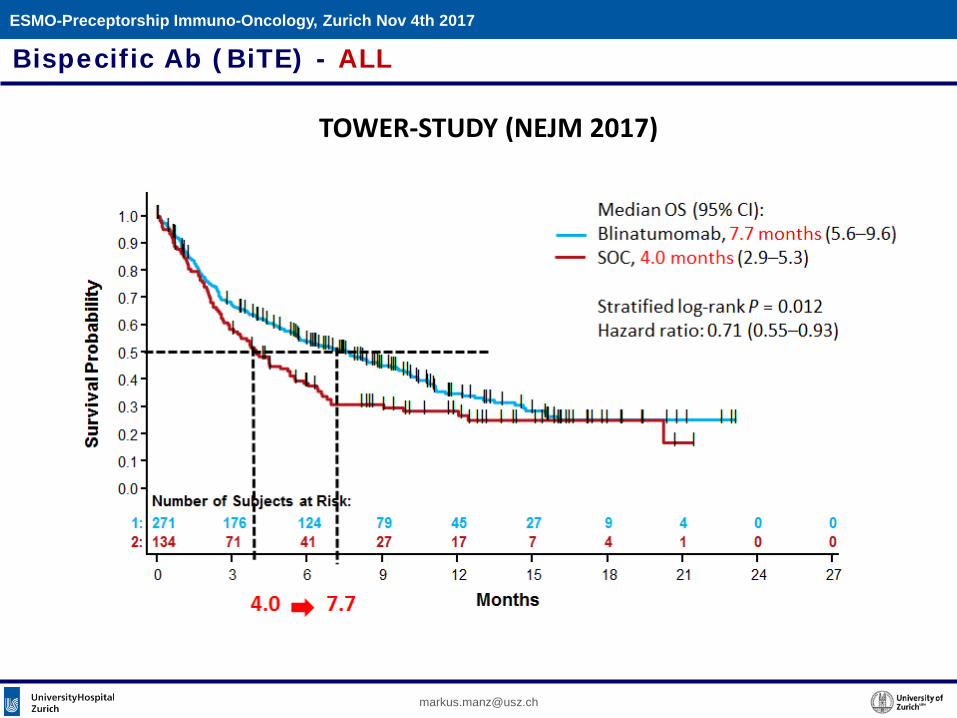
TOWER-STUDY (NEJM 2017)
Bispecific Ab (BiTE) - ALLESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
Overview
Immunotherapy in Hemato-Oncology (examples)
• Allogeneic hematopoietic (stem) cell transplantation
• Checkpoint control (post-allo-HSCT, HD)
• Optimized monoclonal Abs (CLL, MM)
• Bispecific Abs (BiTE; ALL)
• CART cells (CD19 CART, ALL, MM; BCMA CART, MM)
• «eat me» control – CD47-SIRPa
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
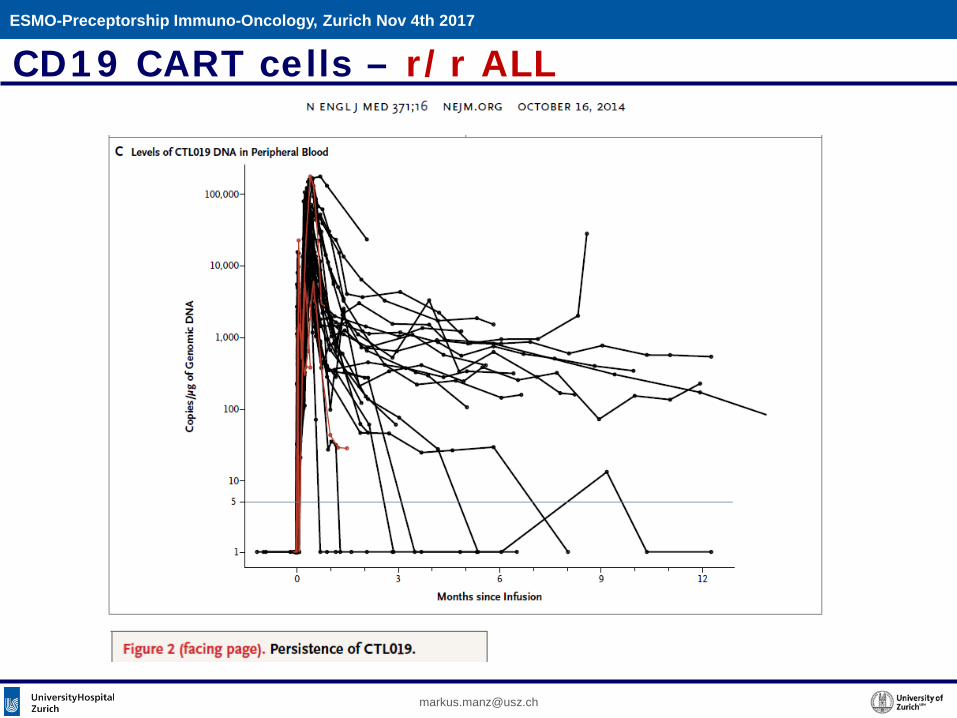
CD19 CART cells – r/r ALL
Emma WhiteheadNY Times DEC. 9, 2012
“Last spring Emma, then 6, was near death from leukemia. She had relapsed twice after chemotherapy»
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
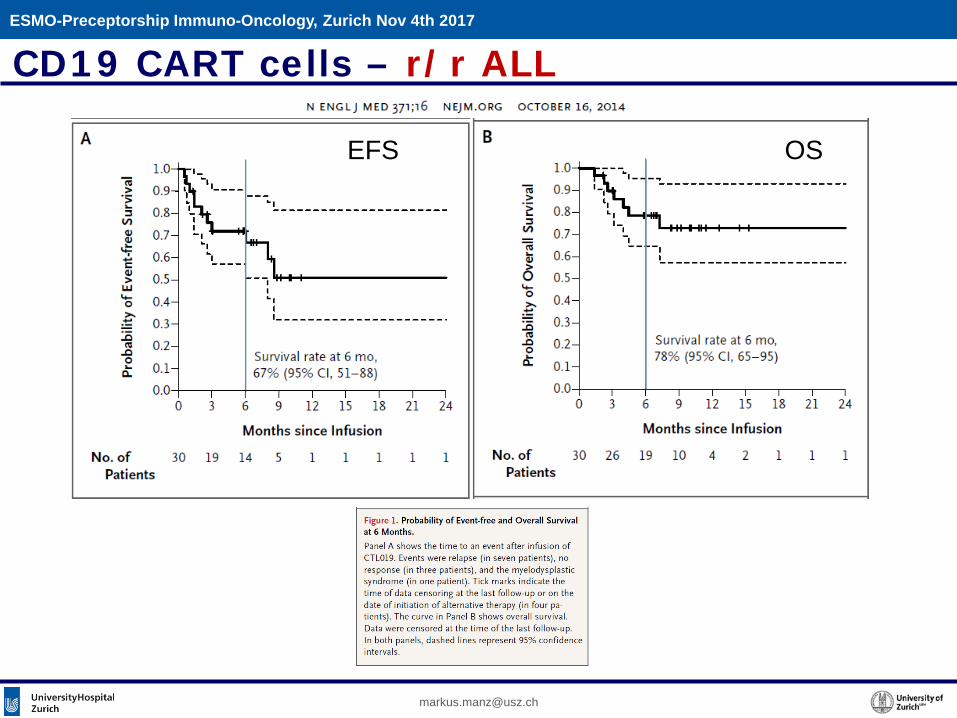
EFS OS
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
CD19 CART cells – r/r ALL
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
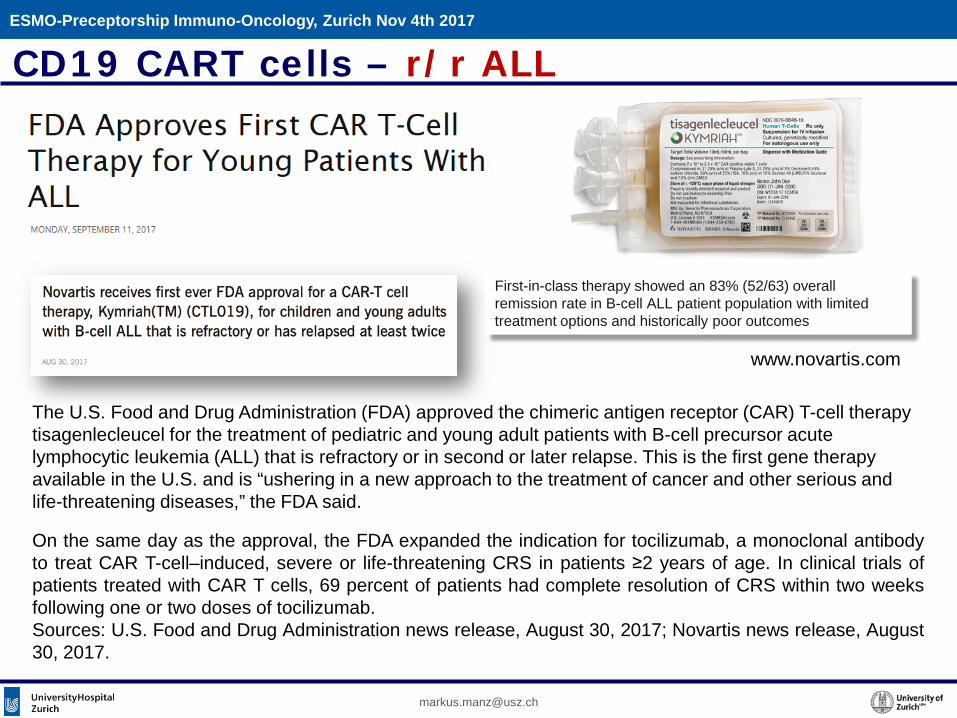
On the same day as the approval, the FDA expanded the indication for tocilizumab, a monoclonal antibodyto treat CAR T-cell–induced, severe or life-threatening CRS in patients ≥2 years of age. In clinical trials ofpatients treated with CAR T cells, 69 percent of patients had complete resolution of CRS within two weeksfollowing one or two doses of tocilizumab.Sources: U.S. Food and Drug Administration news release, August 30, 2017; Novartis news release, August30, 2017.
The U.S. Food and Drug Administration (FDA) approved the chimeric antigen receptor (CAR) T-cell therapy tisagenlecleucel for the treatment of pediatric and young adult patients with B-cell precursor acute lymphocytic leukemia (ALL) that is refractory or in second or later relapse. This is the first gene therapy available in the U.S. and is “ushering in a new approach to the treatment of cancer and other serious and life-threatening diseases,” the FDA said.
First-in-class therapy showed an 83% (52/63) overallremission rate in B-cell ALL patient population with limitedtreatment options and historically poor outcomes
www.novartis.com
CD19 CART cells – r/r ALL
CD19 CART cells – r/r NHL
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
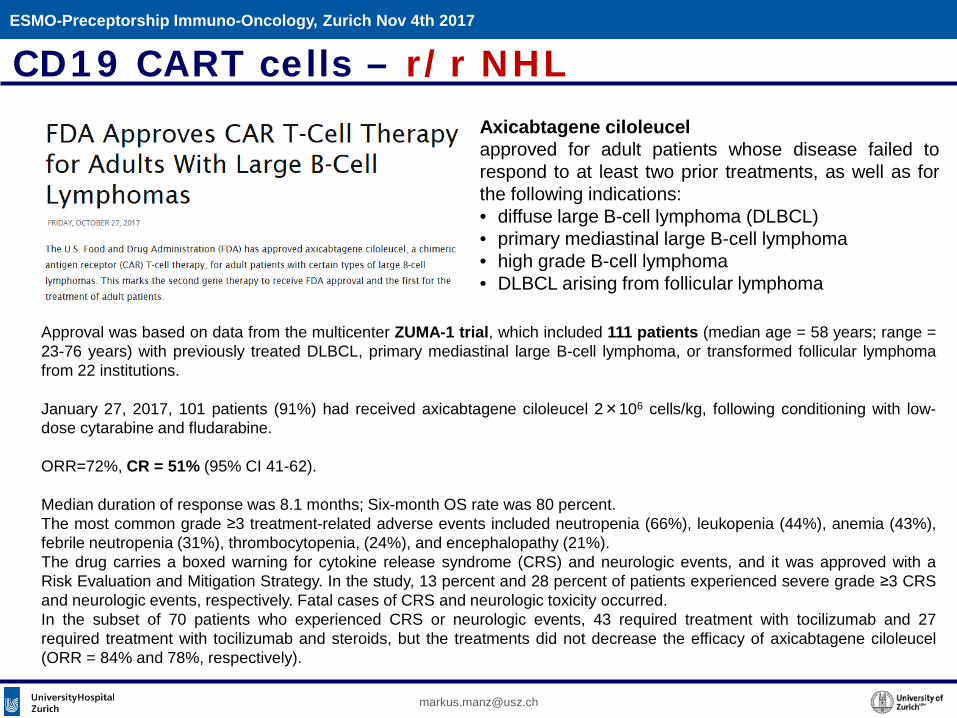
Approval was based on data from the multicenter ZUMA-1 trial, which included 111 patients (median age = 58 years; range =23-76 years) with previously treated DLBCL, primary mediastinal large B-cell lymphoma, or transformed follicular lymphomafrom 22 institutions.
January 27, 2017, 101 patients (91%) had received axicabtagene ciloleucel 2×106 cells/kg, following conditioning with low-dose cytarabine and fludarabine.
ORR=72%, CR = 51% (95% CI 41-62).
Median duration of response was 8.1 months; Six-month OS rate was 80 percent.The most common grade ≥3 treatment-related adverse events included neutropenia (66%), leukopenia (44%), anemia (43%),febrile neutropenia (31%), thrombocytopenia, (24%), and encephalopathy (21%).The drug carries a boxed warning for cytokine release syndrome (CRS) and neurologic events, and it was approved with aRisk Evaluation and Mitigation Strategy. In the study, 13 percent and 28 percent of patients experienced severe grade ≥3 CRSand neurologic events, respectively. Fatal cases of CRS and neurologic toxicity occurred.In the subset of 70 patients who experienced CRS or neurologic events, 43 required treatment with tocilizumab and 27required treatment with tocilizumab and steroids, but the treatments did not decrease the efficacy of axicabtagene ciloleucel(ORR = 84% and 78%, respectively).
Axicabtagene ciloleucelapproved for adult patients whose disease failed torespond to at least two prior treatments, as well as forthe following indications:• diffuse large B-cell lymphoma (DLBCL)• primary mediastinal large B-cell lymphoma• high grade B-cell lymphoma• DLBCL arising from follicular lymphoma
Antigen Expression in B Cell Maturation
CD19CD20CD22
CD38CD138BCMACD319(SLAMF7)
- -(?)- -- -
- +
+ +
- -
- +
Expression outside ofBlood / B-Cell Compartment
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
BCMA CART cells – Multiple MyelomaESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
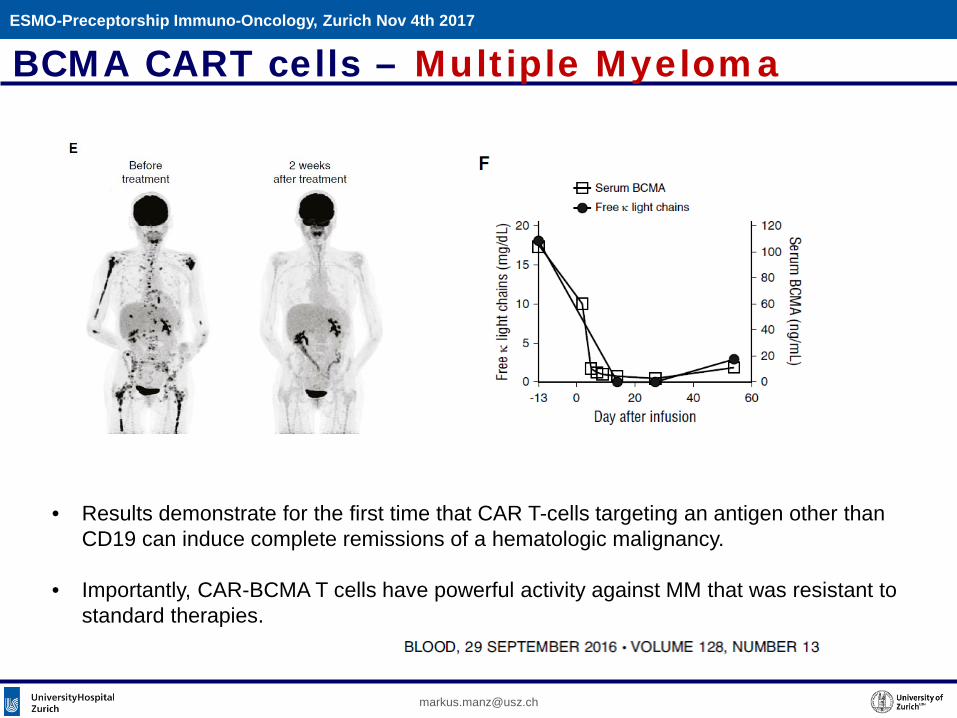
• Results demonstrate for the first time that CAR T-cells targeting an antigen other than CD19 can induce complete remissions of a hematologic malignancy.
• Importantly, CAR-BCMA T cells have powerful activity against MM that was resistant to standard therapies.
BCMA CART cells – Multiple MyelomaESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
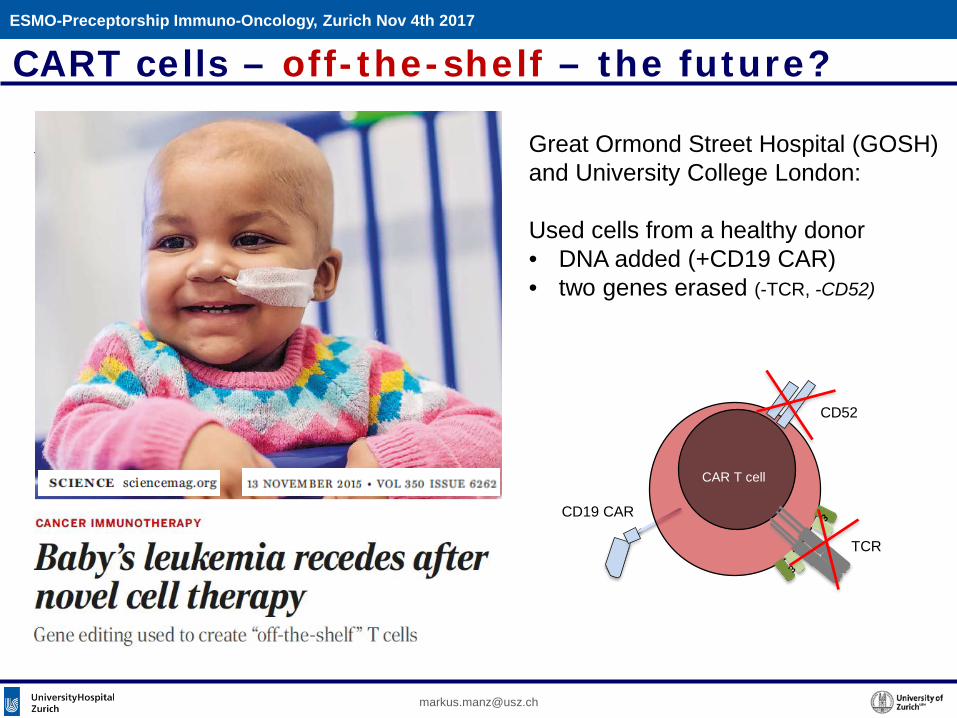
CART cells – off-the-shelf – the future?
Great Ormond Street Hospital (GOSH) and University College London:
Used cells from a healthy donor• DNA added (+CD19 CAR)• two genes erased (-TCR, -CD52)
CAR T cell
TCR
CD52
CD19 CAR
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
Overview
Immunotherapy in Hemato-Oncology (examples)
• Allogeneic hematopoietic (stem) cell transplantation
• Checkpoint control (post-allo-HSCT, HD)
• Optimized monoclonal Abs (CLL, MM)
• Bispecific Abs (BiTE; ALL)
• CART cells (CD19 CART, ALL, MM; BCMA CART, MM)
• «eat me» control – CD47-SIRPa
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
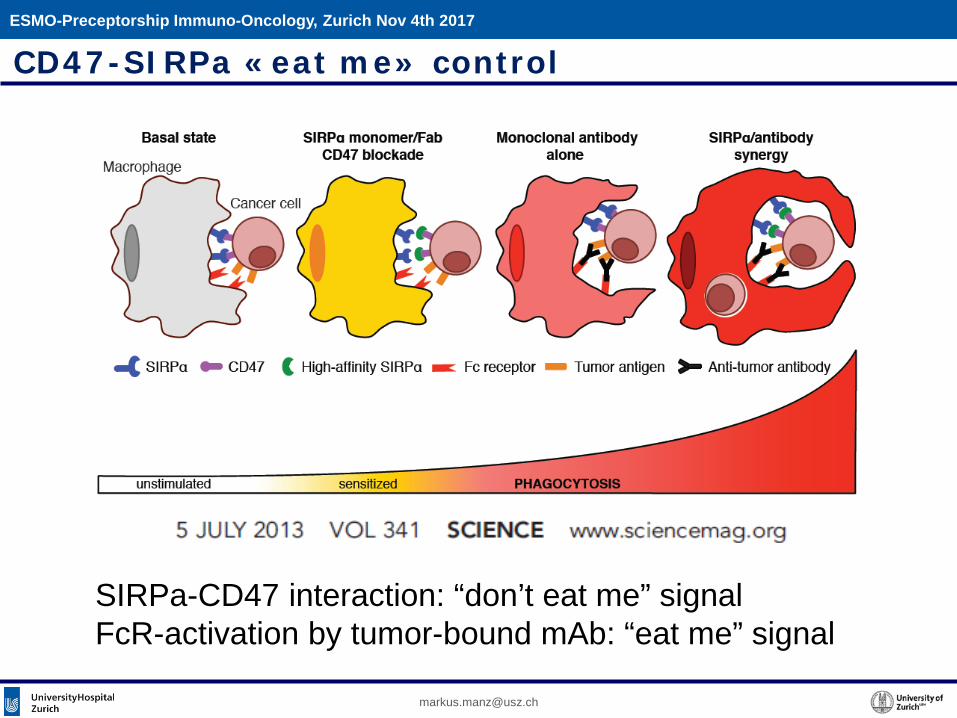
CD47-SIRPa «eat me» control
SIRPa-CD47 interaction: “don’t eat me” signalFcR-activation by tumor-bound mAb: “eat me” signal
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
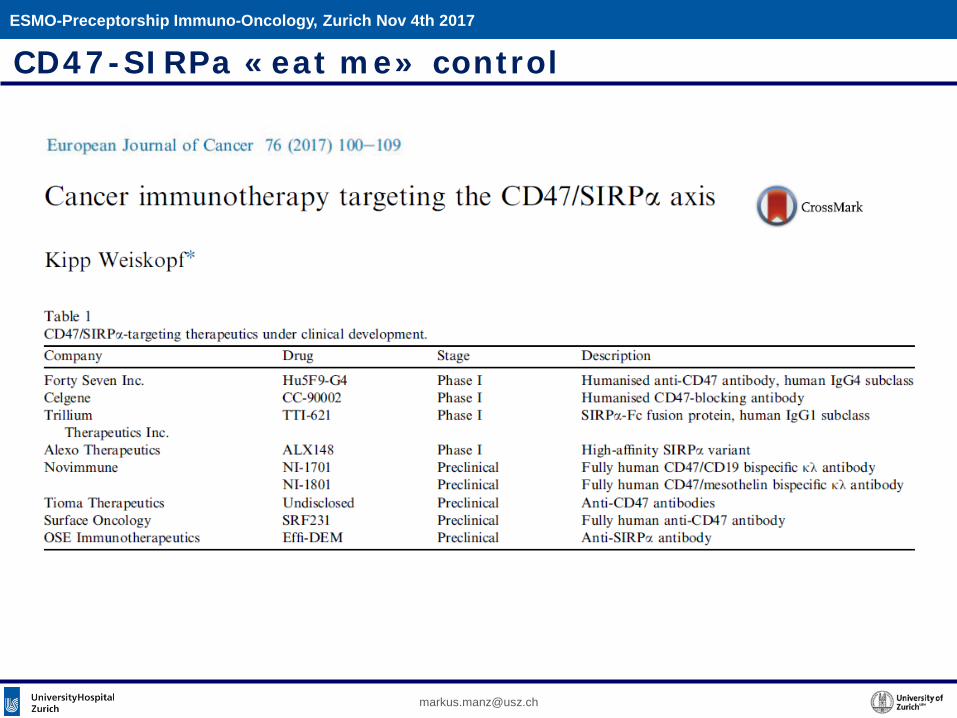
CD47-SIRPa «eat me» control
Overview
Immunotherapy in Hemato-Oncology (examples)
• Allogeneic hematopoietic (stem) cell transplantation
• Checkpoint control (post-allo-HSCT, HD)
• Optimized monoclonal Abs (CLL, MM)
• Bispecific Abs (BiTE; ALL)
• CART cells (CD19 CART, ALL, MM; BCMA CART, MM)
• «eat me» control – CD47-SIRPa
An ongoing (R)Evolution
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
Thank you for your attention
ESMO-Preceptorship Immuno-Oncology, Zurich Nov 4th 2017
Recommended