
COPD in-patient management : guideline development, implementation
and follow-up in the acute hospital setting Don Campbell
Caroline Brand
Clinical Epidemiology & Health Service Evaluation Unit
Melbourne Health
Acknowledgements
Report
Dr Caroline Brand and Ms Fiona Landgren
Project Conception
Dr Donald Campbell
Dr Peter Greenberg
Dr Harry Teichtahl
Prof Anne Maree Kelly
Prof Peter Cameron
Project Development and Research Design
Dr Caroline BrandMs Fiona LandgrenMs Jill NosworthyDr Don CampbellData collection Ms Fiona LandgrenMs Ana HutchinsonMs Catherine JonesDr Caroline Brand Data analysis Dr Lachlan MacGregorDr Caroline Brand
Funding support:EBCPRP, SRDC, NHMRC

Clinical Practice Guidelines
“Systematically developed statements developed to assist practitioner and patient decisions about appropriate health care for specific circumstances” .
What is known about:
• Implementation?
• Long-term impact?

What did we do?
What did we find?
What difference did it make?
Was it sustainable?
What would we do differently?

What we set out to do
Goal
To improve the standard of care and health related quality of life for patients who have experienced an acute exacerbation of COPD requiring hospitalisation at Royal Melbourne (RMH) and Western Hospitals (WH).
Aim
Development and implementation of evidence-based clinical practice guidelines for the acute in-patient episode.

Project activities
1 Examine VIMD database
2 Prospective case-note audit (pre/post intervention)
3 CPG development– pathway
– decision nodes
– evidence-based (consensus driven)
4 Implementation Strategy– multi-faceted, evidence-based

Project activities 2
5 Outcome measures– Patient: Satisfaction
HRQoL
– Institution: LOSReadmission rate
6 Process measures– medication use, tests
– clinical indicators (ACHS for asthma, ?? For COPD)

Guideline Implementation and Evaluation
Time period:
pre-implementation phase: 3/6/99 to 9/9/99
post-implementation phase: 7/11/99 to 31/3/00
Patients admitted:
WH RMH
pre-implementation 141 68
post- implementation 138 62

Demographic characteristics
WH RMH• Parameter Pre Post Pre Post• Av Age (yrs) 68 69 70 72• Males (% of total) 60 52 71 51• Current Smokers (% of total) 35 32 31 30• Ex Smokers (% of total) 63 62 56 57• Language Barrier(% of total) 11 11 25 10*• Presentation to hospital 51 72 43 51
previous 12 months (% of total) • Average duration of illness 4.1 5.7** 8.6 5.8
for presenting episode (in days)• No of deaths (% total) 0 0 4 (6%) 3 (5%)

What happened?
• Short-term impact evaluation

LOS and Readmission rates
WH RMH
Pre Post Pre Post
(172) (173) (72) (70)
Ave LOS (days) 7.1 7.1 8.4 4.5 **
(6,1-50) (5,1-37) (7,0-28) (4, 1-13)
Unplanned re-admission
28 days post discharge 18 16 3 8
(% of total) (10%) (9%) (4%) (11%)

Hours in ED
WH RMH
Pre Post Pre Post
(65) (65) (68) (63)
Ave Time in ED (hrs) 9.4 8.8 8.7 12.4 *
median 8.2 7.8 7.3 9.8
(range) (1-23) (2-34.2) (0.8-26.4) (2.7-34.6)

Test use at initial assessment
Triage Category Pulse Ox (SpO2) ABG CXR FBE1 X X X X2 X X X X3 X X X4 X X X5 X X X
(X indicates test recommended)
CXRs and ABGs-• Reduced at RMH (unchanged at WH). • ABG reduction significant at RMH (2= 11.44, p < 0.001).
Sputum m&c tests reduced at WH.

Recommended ongoing therapy for COPD
WH RMH
Pre Post Pre Post
(65) (65) (68) (63)
IV line inserted 85% 74% 93% 54%
IV removed at 24 hours 24% 35% 25% 47%*
Oral Antibiotics (wards) 89% 80% 80% 53%**
IV Antibiotics (wards) 56% 35%* 60% 25%**
Oral C’steroids (wards) 91% 95% 85% 77%
IV C’steroids (wards) 64% 49% 20% 11%
Ipratropium nebs (wards) 94% 88% 88% 74%
MDI (+/- spacer) (wards) 88% 85% 57% 61%
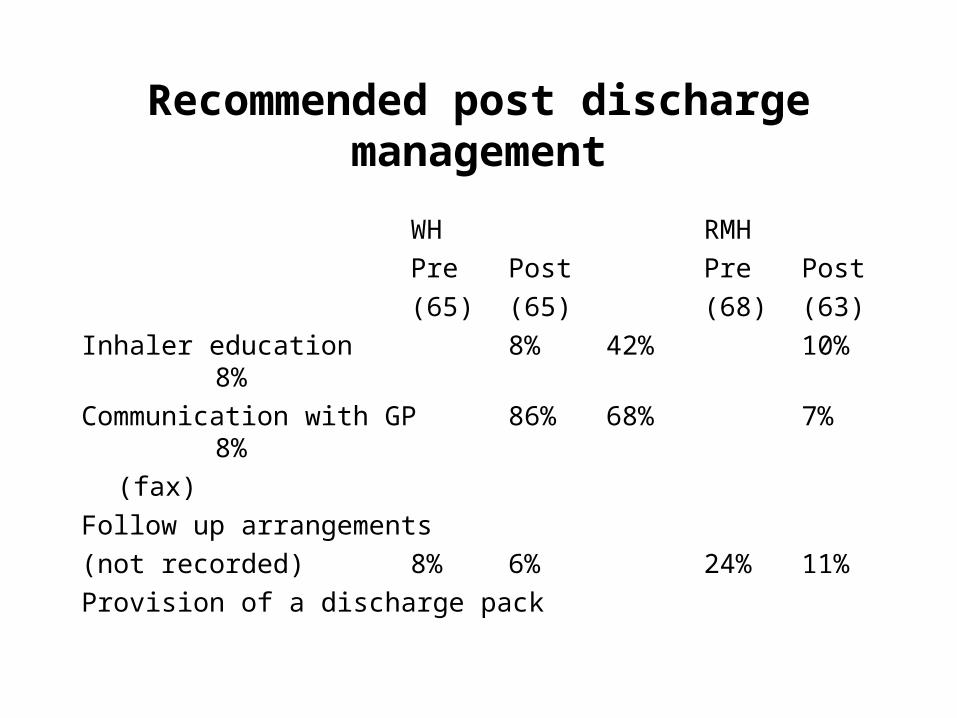
Recommended post discharge management
WH RMH
Pre Post Pre Post
(65) (65) (68) (63)
Inhaler education 8% 42% 10% 8%
Communication with GP 86% 68% 7% 8%
(fax)
Follow up arrangements
(not recorded) 8% 6% 24% 11%
Provision of a discharge pack

Results
Quality of lifeDisease specific QOL (SOLQ)-
• Coping reduced 28 days after discharge.
Generic QOL (SF12) post implementation-
• MCS improved at both hospitals (NS).
Satisfaction with care moderately high at both hospitals
(low score for hospital reputation post implementation at one hospital )

Long-term sustainability?
• Two years later

CPG-Two Year Evaluation
1 Medical Record Audit
(6 months post implementation)
2 Staff survey: awareness & use of CPG’s
3 Survey Intranet access and CPG quality
4 Focus Groups & Key Informant Interviews

Summary Audit
• Some medical units may be protocol driven
• Specific drug recommendations accepted
– ? related to CPG use
• Poor uptake:
– process of care and non drug recommendations
Uptake of CPG recommendations usually but not invariably relates to level of evidence

CPG - Staff Survey N=188
• Medical 43.7% Nursing 29.0% Students 21.3%
• Age 20-49 (75.4%)
• Medical (57.9%) Surgical (22%)
• Senior staff 73%
• Gender F80:M57 (>39yrs F20:M52)

Staff Survey Summary- CPG use
Barriers• Difficult to locate
• Poor Index
• Too prescriptive
• No allowance for variation
• Not evidence based
• Lack of time
• Too general
Facilitating Factors• Represent best practice
• Evidence-based
• Easy to access
• Expedite decision making
• Concise
• Support treatment decisions
• Refresh memory

Variable access to department home sites
Inconsistency: layout, terminology and content
Poor adherence to NHMRC guidelines for CPG construction
Intranet Survey Summary

Most health professionals favoured use of CPG/protocols
Some staff expressed concern about “cookbook” medicine
Emphasis on use as guidelines not proscriptive documents
Access and quality of guidelines is a major issue
Occupational preferences identified- :• nurses prefer protocols/pathways
• “nurses do not make decisions where there is ambiguity”
Departments are variably protocol driven: ED, ICU, Renal
Medicolegal issues not a major concern
High staff turnover limited corporate memory and training in use
Focus Groups and Key Informant Interviews
• Senior clinician support and advocacy essential• Consistency in terminology needs to be addressed• Existing access to guidelines needs to be reviewed• Infrastructure for access to decision support systems is required• Integration with ongoing education programs is essential• Establishment of KPI around audit and guidelines
implementation is necessary• Greater involvement of consumers in guideline development
required
Integration with formal hospital quality processes is lacking
Summary

Contextual analysis
Staff turnover
Relationship to quality program
Interdisciplinary teams?
(or professional isolation: multitude of teams)
Information Technology support?
Integrated care?
Executive Leadership??

Signposts for the future
“Finding the imperatives that will drive systems integration in public sector health care”
• Narrative to find simple rules
• Values and ethical frameworks
• Science of complexity
• Rewarding teamwork

Knowing what we now know, what would we do (differently) next time?
Leadership
Build into Quality framework
Communication
Simple rules for providing quality care– Patient-centred: involve from Day 1- meet needs
– Collaborative: build manager-clinician partnership
– Knowledge-based: CPG plus expertise
Reward and recognition– Team-play
– Communication
Recommended













![GARD Kazakhstan 2008[1] - WHO · urogenital system diseases respiratory diseases digestion diseases. Epidemiology of COPD in the Republic of Kazakhstan (for 100 000 population ) «Kazakhstan](https://img.pdfslide.us/doc/110x75/606e919650e0dc018747cbdb/gard-kazakhstan-20081-who-urogenital-system-diseases-respiratory-diseases-digestion.jpg)



