140
HKJOS Wong TC, Cheung FMF, Siu TH, et alHong Kong Journal of Orthopaedic Surgery2002;6(2):140-144.
PATHOLOGY FINDINGS
This patient presented with multiple skin and soft tis-sue swellings over a period of 9 years. According totheir locations, the swellings were separately diagnosedas xanthofibroma (tendinous-fascia at elbow), xan-thelasma (eye-lid), xanthoma (nose bridge), and giantcell tumour of tendon sheath (finger tendon). Reviewof all the biopsy material showed the same diseasemorphology as xanthogranulomatosis (Fig. 10). Therewere nodular sheets of lipid-laden foamy macrophagesadmixed with chronic inflammatory cells and Touton-type, multinucleated, giant cells. There were varyingdegrees of fibrosis in the background, and eosinophilswere notably absent. In the elbow mass, there weresheets of histiocytes with kidney-shaped nuclei. Theystained positively on immunostudies for Langerhanscell markers, including S100 protein and CD1a (Fig.11). This raised the possibility of Langerhans cell his-tiocytosis (LCH). As Langerhans cells were not seenin the other biopsy material, and given the fact that eosi-nophils (important accompanying cells in LCH) wereabsent, the possibility of LCH was excluded in this case.On the other hand, the multifocal occurrence did pin-point a systemic infiltrative disease rather than a coin-cidental occurrence of a localised disease at differentsites. Xanthomatous lesions over tendons and eyelidsnecessitated an investigation into familial or acquiredhypercholesterolaemia. This possibility was subse-quently excluded by blood tests, which revealed nor-mal cholesterol levels and lipid profiles. Without otherclues, the cause of this systemic xanthogranulomatosisremained enigmatic.
RADIOLOGY FINDINGS
The initial radiograph of the left middle finger showednonspecific soft tissue swelling around the proximal in-terphalangeal joint and middle phalanx. No bony ero-sion was noted. Computed tomography and MRI of thefacial region were performed that showed soft tissuemasses in the periorbital region and over the right na-sal bridge (Fig. 12). No retro-orbital mass was detected.
Separate MRI studies of the right knee and both ankleswere subsequently performed. Apart from the prepa-
Continuation of ORTHOPAEDIC. RADIOLOGY. PATHOLOGY
CONFERENCE from page 114
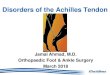
Figure 10 Xanthogranulomatous tissue containing lipid-ladenfoamy macrophages, chronic inflammatory cells, and Touton giantcells.
Figure 11 Sheets of CD1a-positive Langerhans cells in the elbowmass.
tellar mass detected on physical examination, therewere actually multiple soft tissue masses around theright knee. They were of similar signal intensity, beingisointense on T1-weighted images (Fig. 13) and het-erogeneously slightly hyperintense on T2-weightedimages (Fig. 14). Some intralesional cystic areas werepresent. They were infiltrative and encased the rightpatellar tendon, right biceps femoris (Fig. 15), and bothAchilles tendons (Fig. 16).
There were extensive irregular hypointense lesions in
Recommended