Embed Size (px)
DESCRIPTION
tendon healing
Citation preview

Tendon Structure Tendon Structure and Healingand Healing

Tendon
• A unit of musculoskeletal tissue that transmits force from muscle to bone1
• The functional link between the dynamic andthe static part of the musculoskeletal system transferringmuscle contraction to the skeletal system and thus leading to motion
• Composed predominately of collagen fibers and rod- or spindle-shaped fibroblast-like cells (tenocytes)
• Collagen constitutes the basic structural unit of tendon
1. James R, Kesturu G, Balian G, Chhabra B. Tendon: Biology, Biomechanics, Repair, GrowthFactors, and Evolving Treatment Options J Hand Surg 2008;33A:102–112

Composition of Tendons
(Kjaer, 2004)

Structure of Tendon
• High amount of collagen (70% of dry weight) and parallel fibre orientation account for high tensile strength the greatest in our body
• Type I collagen is the predominate type of collagen (95 %), the other 5% from type III and V and glycosaminoglycan.
• The collagen forms fibrils, organized into bundles with nerves and blood vessels covered by epitenon and paratenon
• Small amount of synovial fluid aids in motion smoothness

Structure of Tendon
TENDON CELLS (TENOCYTES)•Specialized fibroblast cells within the tendon•The primary role of tenocytes :– Control tendon metabolism (production and degradation
of the Extracellular Matrix) – Respond to the mechanical stimuli applied to the tendon
mechanotransductionEXTRACELLULAR MATRIX (ECM)•Largely composed of a network of collagen fibers.•Primary function is to maintain the tendon’s structure and facilitate the biomechanical response to mechanical loading

Structure of Tendon
COLLAGEN•Synthesized by tenocytes•The collagen network is dominated by type I fibers (60%)•Combine to form ordered units of microfibrils (5 collagen molecules), subfibrils, and fibrils•Proteoglycans and glycoproteins binding the fibrils together to form fasciclesELASTIN•Composes approximately 2% of the dry weight of tendon•Elastin fibers and several glycoproteins are also integral parts of tendon ECM and provide functional stability to the collagen fibers

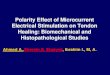
Macrostructure

Schematic representation of the microarchitecture of a tendon

Structure of Tendon
GROUND SUBSTANCE•Composed mainly of inorganic substances and other proteins.•The inorganic substances:Proteoglycans (PGs)Sulfated polysaccharide chains (glycosaminoglycans)Hyaluronic acid (HA) chain Glycoproteins and several other small molecules

Structure of Tendon
• Endotenon • Thin reticular network of connective tissue investing each
tendon fiber• Contains the vascular, lymphatic, and neural transmission
routes to maintain tendon fibroblasts
• Epitenon• Loose connective-tissue sheath containing the vascular,
lymphatic, and nerve supply to the tendon• Binds the fascicles together

Tendon Types
• Paratenon-covered (e.g. patellar, achilles)– Loose areolar connective tissue (paratenon)– Majority of tendons (move in a straight line)– Rich vascular supply
• Sheathed (e.g. hand flexor tendons)– Tendons that bend sharply– Sheath acts as a pulley and directs tendon path– Sliding is assisted by synovial fluid (parietal synovial
membrane and from the visceral synovial membrane or epitenon)
– Less vascularized and have avascular areas that receive nutrition by diffusion



Blood supply
• Paratenon-covered tendons– Perimysium– Paratenon / mesotenon– Periosteal insertion
• Tendons in sheaths:– Synovial diffusion in avascular regions– Osseous insertions– Proximal mesotenon via vinculae

Vascularity• Tendon with sheath • Tendon without sheath
Vessels enter from many points on the periphery and anastomose with a longitudinal system of capillaries.
Vascular supply through the vinculum longus

VINCULAE

Nerve Supply
• No nerve fibres within tendon body• Epitenon and peritenon contain nerve endings
(sensory)• Golgi tendon organs at musculo-tendinous
junction (proprioceptive)

Biomechanics
• Tendon possesses one of the highest tensile strengths of any soft tissue in the body.
• High mechanical strength, good flexibility, and an optimal level of elasticity
• The tensile properties characterized by:– The mechanical properties (stress-strain relationship) of
the collagen– The structural properties (load-elongation relationship) of
the bone-tendon-muscle structure
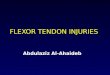
• At rest, collagen fibers and fibrils display a crimped configuration

Stress-strain Curve of Normal Tendon

Biomechanics
• Very high loads are placed on human Achilles tendon during running is 9 kN, corresponding to 12.5 times body weight
• Tendons are at the highest risk for rupture if tension is applied quickly and obliquely

Factors Affecting the Mechanical Properties of Tendons
• Age• Anatomic location• Exercise and immobilization• Heat treatment• Pregnancy• Comorbidities (diabetes mellitus, connective tissue
disorders, renal disease) • Pharmacologic agents (steroids, nonsteroidal anti-
inflammatory drugs or NSAIDs)

Factors Affecting the Mechanical Properties of Tendons
• Age– Tenocytes decrease in number and flattened and reduced
capability for the mechanotransduction for collagen production and maturation
• Anatomic location– Tensile strength of the digital flexor tendons twice as large
as the digital extensor tendons collagen concentration
• Exercise and immobilization– Immobilization stress deprivation decrease in collagen
synthesis and an increase in matrix metalloproteinases (MMPs) reduces the mechanical properties of the tissue

Factors Affecting the Mechanical Properties of Tendons
• Heat treatment– Significant tendon shrinkage after laser treatment
tensile testing shortened 10% of their resting length showed a decrease in load to failure to approximately one third
• Pregnancy– Increased laxity of the tendons and ligaments in the pubic
area during later stages of pregnancy and the postpartum period hormone relaxin

Factors Affecting the Mechanical Properties of Tendons
• Comorbidities– Diabetes Melitus• Changes in connective tissue and the metabolic
fluctuations microvascularity and promote collagen accumulation in periarticular tissues
– Connective Tissue Disorders• Rheumatologic conditions (e.g., rheumatoid arthritis,
spondyloarthropathies) inflammatory infiltrate that promotes the destruction of collagenous tissue
– Renal Disease• Increase in the amount of elastin and collagen
destruction

Factors Affecting the Mechanical Properties of Tendons
• Pharmacologic agents– Steroids• Inhibition of collagen synthesis altered healing and a
decrease on the peak load of these tissues
– Fluoroquinolones• Cause an increase in the activity of matrix
metalloproteinases (MMPs)

TENDON INJURIES

Tendon Injuries
• Direct trauma– Laceration or contusion– Sharp tools– Special importance to the hand and upper
extremity
• Indirect trauma – Tensile overload– Multifactorial (anatomic location, vascularity, and
skeletal maturity, magnitude of the forces)

Incidence
• An acceleration-deceleration mechanism has been reported in up to 90% of sports-related Achilles tendon ruptures
• Degenerative tendinopathy is the most common finding in spontaneous tendon ruptures

Healing process
• Healing process in a paratenon-covered tendon
• Healing process in sheated tendon

Phases of tendon healing

Healing in Paratenon-Covered Tendon
• Immediate– Blood cell– Inflammatory products– Fibrin– Nuclear debris
• 1st week– Proliferating tissue from paratenon– Undifferentiated and disorganised fibroblasts– Capillary buds– Collagen synthesis
Granulation tissue

• 2nd weeks– Stumps fused by fibrous bridge– Fibroblast proliferation– Collagen production– Fibrils accumulate
perpendicular to long axis– Vascular proliferation in stumps– Fibrovascular tissue from
paratenon blends with epitenon to form ‘tendon callus’
Healing in Paratenon-Covered Tendon

• 3-4 weeks– Fibroblasts and collagen fibers • Rorientation & Organisation
• > 4 weeks– Tensile properties increase– Remodelling and further organisation– Minimal histological difference by 20 weeks– Months to regain full strength
Healing in Paratenon-Covered Tendon

Healing in Sheathed Tendon
• Healing of these tendons has been a controversial topic
• Early data suggest: Healing by granulation from tendon sheath - Fibroblasts derived from the tendon sheath and
surrounding tissues invade the healing site and initiate, regeneration
- Tendon cells played no active role• Recent data suggest– Tenocytes have intrinsic repair capabilities– Proliferation and cell migration at tendon ends from epitenon
and endotenon

Healing in Sheathed Tendon
• 3 weeks– Cells from the epitenon migrated into the wound site
via desmosome phagocytes or macrophages – Cell from endotenon increased protein synthesis
• 6 weeks– Number of phagocytes within the repair site had
increased• 9 weeks– Cellular activity at repair site continued– Extracellular matrix of collagen fibrils in various stages – Remodeling process phagocytosis and collagen
synthesis.

Healing in Sheathed Tendon
• Repaired tendons treated– Controlled passive motion
intrinsic response epitenon predominates
– Immobilized tendon ingrowth of connective tissue from the digital sheath and cellular proliferation of the endotenon

Tendon Repair
• Factor determines quality of tendon repair– Suture material– Type of suture repair– Knotting of sutures– Continuous passive motion– Weightbearing– Nature and location

Tendon Repairs
• Suturing technique– Passed perpendicular to the tendon before
passing it across the injury, parallel to the tendon stronger tendon-suture-tendon constructs
– Minimize gap formation between the tendon stumps

Tendon Repairs
• Predicting the success of tendon repair gliding function after injury
• Large scar or adhesion formation detrimental to the gliding function
• Early weightbearing / early active mobilization rupture and gap formation
• Carefully controlled early passive mobilization stimulates repair and improves strength in the first few months

Tendon Transfer
• Indications:– Peripheral nerve injury – Replacement of ruptured tendons in rheumatoid patients – Central nervous system disorders such as cerebral palsy
• Considerations for transfer – Absence of inflammation and edema– Mobility of the joints– Adequacy of the tissue bed– Adequacy of skin coverage– Potential for an effective line of action of the transferred
tendon

Tendon Transfer
• Postoperatively long and rigorous rehabilitation desired joint motion

Adhesions Formation
• Lack of mechanical stimulus proliferation of scar tissue and subsequent adhesions impede normal tendon function
• Mechanical loading associated with motion of the healing tendon decreases formation of postoperative adhesions and increases the strength

Adhesions Formation
• Many attempts have been made to reduce adhesion formation
• Materials– Mechanical barriers such as polyethylene or
silicone – Pharmacological agents such as indomethacin and
ibuprofen, hyaluronate, 5-fluorouracil
no significant differences in adhesion formation in a rat Achilles tendon model

Rehabilitation
• After the inflammatory phase, controlled stretching – Increase collagen synthesis by tenocytes and
improve fiber alignment
Higher tensile strength • Immobilization results in tendon atrophy

Summary
• There are many factors affecting the mechanical properties of tendons
• Tendon healing process consist of 4 phases– Regain most of original strength by 21-28 days
• Early mobilisation Increases ROM but can decrease tendon repair strength
– Controlled stretching can be done after the inflammatory phase
• Adhesion formation may impede normal tendon function• Many attempts have been made to reduce adhesion
formation no significant result

THANK YOU