ARTIGO ORIGINAL: Biehl-Printes, C. et al (2019) Comparison on muscle strength, aerobic capacity and respiratory function in women with fibromyalgia, 8 (1): 141 – 159
JOURNAL OF AGING AND INNOVATION, ABRIL, 2019, 8 (1) ISSN: 2182-696X http://journalofagingandinnovation.org/ 141
Comparison on muscle strength, aerobic capacity and respiratory function in women with fibromyalgia
Comparação na força muscular, capacidade aeróbia e função respiratória em mulheres com fibromialgia
Comparación en la fuerza muscular, capacidad aeróbica y
función respiratoria en mujeres con fibromialgia Biehl-Printes Clarissa1, Tomas-Carus Pablo2, Pessoa Fernando3, Branco Jaime C.4, Parraca José A.5, Lancho Carolina 6
Poblador María S.7, Lancho José L.8
1Ph.D, Laboratorio de Ciencias Morfofuncionales del Deporte, Departamento de Ciencias Morfológicas, Facultad de Medicina Universidad de Córdoba, España, Instituto de Geriatria e Gerontologia, Pontifícia Universidade Católica do Rio Grande do Sul, Brasil 2Ph.D, Departamento de Desporto e Saúde, Escola de Ciência e Tecnologia, Universidade de Évora, Portuga, Comprehensive Health Research Center (CHRC), University of Évora, Portugal. Research Centre in Sports Sciences, Health Sciences and Human Development (CIDESD), Portugal 3Ph.D Centro Universitário do Serviço Nacional de Aprendizagem Industrial,SENAI CIMATEC, Brasil 4MD, Ph.D, CEDOC, Faculdade Ciências Médicas, Universidade Nova de Lisboa, Serviço de Reumatologia, CHLO, EPE-Hospital Egas Moniz, Lisboa, Portugal. 5Departamento de Desporto e Saúde, Escola de Ciência e Tecnologia, Universidade de Évora, Portuga; Comprehensive Health Research Center (CHRC), University of Évora, Portugal.
6 MD Clínica ASPACE.Donostia-San Sebastian. España. 7MD, Ph.D , Laboratorio de Ciencias Morfofuncionales del Deporte, Departamento de Ciencias Morfológicas, Facultad de Medicina Universidad de Córdoba, España
8 MD, Ph.D Laboratorio de Ciencias Morfofuncionales del Deporte, Departamento de Ciencias Morfológicas, Facultad de Medicina Universidad de Córdoba, España
Corresponding Author: [email protected]
Abstract
Objective: To compare two workout programs: the mode aerobic-breath to the mode combining aerobic-strength-breath, in order
to know the effects in the strength, aerobic fitness and respiratory function of women with fibromyalgia (FM) after a period of 24
weeks.
Methods: A prospective longitudinal study using two groups of women with fibromyalgia has been conducted. Nine participants
were monitored with regular exercise in the mode aerobic-breath group (AbG) and eight in the mode combining aerobic-strength-
breath group (CG). Both groups were complemented with respiratory exercise through diaphragmatic breathing (DB). The
measures used in the study were: measurements at rest, maximum and submaximal oxygen consumption (VO2); maximum and
submaximal aerobic power (W); concentric isokinetic strength at 60º/s of the extensor and flexor muscles of the leg (N.m);
pulmonary function measurements by spirometry (ventilatory test) and maximum respiratory pressures (MRP).
Results: Significant improvements in aerobic condition, strength and respiratory function were obtained by both groups. Initially
the participants AbG vs. CG presented decreased aerobic condition (20-24 ml/kg/min). The range of functional normality of the
strength for the classification of the Freedson percentile was reduced (≤ 10). Even discarding respiratory diseases, the respiratory
muscle strength was lower than the values predicted for healthy people. Over the 24 weeks, there were no differences between
AbG vs. CG in aerobic and respiratory exercises. The differences were mostly observed in the results of strength.
Biehl-Printes, C. et al (2019) Comparison on muscle strength, aerobic capacity and respiratory function in women with fibromyalgia, 8 (1): 141 – 159
Artigo Original

ARTIGO ORIGINAL: Biehl-Printes, C. et al (2019) Comparison on muscle strength, aerobic capacity and respiratory function in women with fibromyalgia, 8 (1): 141 – 159
JOURNAL OF AGING AND INNOVATION, ABRIL, 2019, 8 (1) ISSN: 2182-696X http://journalofagingandinnovation.org/ 142
Conclusion: Our results suggest that intervention programs may be supplemented with respiratory exercises. However, new
studies with longer-term programs are required to compare the absolute impact of different workouts. It is also mandatory to know
if the isolated practice of respiratory exercises has any applicability for patients with FM.
Key words: aerobic training, combined training, breathing exercise, fibromyalgia.
Resumo
Comparar dois treinos, um no modo aeróbio-respiratório e outro no modo combinado: aeróbio-força-respiratório, para conhecer
os efeitos na força muscular, capacidade aeróbia e função respiratória de mulheres com fibromialgia depois de um período de
24 semanas.
Métodos: Se realizou um estudo longitudinal prospectivo utilizando dois grupos de mulheres com fibromialgia. Nove participantes
foram monitoradas com o exercício regular aeróbio-respiratório (AbG) e oito no modo combinado: aeróbio-força-respiratório (CG).
Ambos foram complementados com exercicio respiratório a través de respiração diafragmática (RD). As medidas utilizadas foram:
medidas em repouso; consumo máximo e submáximo de oxigénio (VO2); potência aeróbia (W) máxima y submáxima; força
isocinética concéntrica a 60º/s dos músculos extensores y flexores da perna (N.m); medidas de função pulmonar por espirometria
(prova ventilatória) e pressões máximas respiratórias (PMR).
Resultados: Melhoras significativas na condição aeróbia, na força e na função respiratória foram obtidas por ambos os grupos.
Inicialmente os participantes AbG e CG apresentaram diminuída condição aeróbia (20-24 ml/kg/min). A escala de normalidade
funcional da força para a classificação do percentil de Freedson foi diminuído (≤ 10). Mesmo descartando patologias respiratórias,
a força muscular respiratória foi inferior a aos valores previstos para as pessoaos saudáveis. Ao longo de 24 semanas não se
observou diferenças entre os tipos de treino AbG vs CG no exercício aeróbio e respiratório. As diferenças foram mostradas em
grande parte dos resultados da força.
Conclusão: Nossos resultados sugerem que os programas de intervenção sejam complementados com exercícios respiratórios.
No entanto, novos estudos com programas a mais longo prazo são necessários para comparar o impacto absoluto dos diferentes
treinos. Igualmente, é necessário saber se a prática isolada de exercícios respiratórios tem alguma relevância em pacientes com
FM.
Palavras chaves: Treino aeróbio, treino combinado, exercício respiratório, fibromialgia.
1. Introduction
Fibromyalgia (FM) is a rheumatologic disorder characterized by widespread muscle
pain and tenderness of at least 11 of 18 specific tender points (Wolfe et al., 1990) usually
accompanied by a wide spectrum of symptoms such as: morning stiffness, fatigue, non-
restorative sleep, mood alterations and poor health-related quality of life (HRQoL) (Silverman,
Harnett, Zlateva & Mardekian, 2010; Segura-Jiménez, 2015). In addition, the population with
this disorder presents deterioration of articular amplitude, muscular resistance and strength
likewise below average cardiovascular fitness levels (Busch, Schachter, Overend, Peloso &

ARTIGO ORIGINAL: Biehl-Printes, C. et al (2019) Comparison on muscle strength, aerobic capacity and respiratory function in women with fibromyalgia, 8 (1): 141 – 159
JOURNAL OF AGING AND INNOVATION, ABRIL, 2019, 8 (1) ISSN: 2182-696X http://journalofagingandinnovation.org/ 143
Barber, 2008). The deterioration of respiratory function is also described as a common feature
in these patients (Forti, Zamunér, Andrade & Silva, 2016).
The necessity of the recovery of the physical components of strength, aerobic fitness
and flexibility is supported by literature and associated to relieving symptoms like pain and
fatigue (de Bruijn et al., 2011). The decrease in respiratory muscle function, as it has been
described, is an important component which also needs to be explored in therapeutic physical
recovery (Sahin, Ulubas, Calikoglu & Erdogan, 2004). The respiratory alterations may
exacerbate the symptoms of fibromyalgia and chronic fatigue syndrome, including the
aggravation of these diseases (Uveges et al., 1990).
Proliferating studies on FM have contributed to disclose different clinical trials through
exercise and have showed interest in dose-response, impact on functionality, symptoms and
adherence (García-Hermoso, Saavedra & Escalante, 2015). On the other hand, along the last
years, the comparison between models of intervention exercise has been little approached.
One single review study with FM compared several clinical trials using different types
of exercise, but the investigation did not describe the direct comparison of aerobic exercise
(AE) vs. combined exercise (Aerobic and Strength); and did not include breathing exercises
as a supplement or isolated intervention (Valim, 2006). The combination of a 20-week
progressive program including strength and aerobic exercises was described as a secure
application, well tolerated and effective manner to improve the functional status of women with
FM (Rooks, Silverman & Kantrowitz, 2002). A more recent study, which adopted a program of
24-weeks, did a direct comparison between aerobic and combined exercises (aerobic, strength
and flexibility) taking into account the time-program. The authors reported that women with FM
gained additional health benefits when engaged in a combined exercise program (Sañudo et
al., 2010). The breathing exercises were recommended as complements in multi-modal, mind-
body yoga or water-based programs, all aiming at the improvement of symptoms such as pain,
anxiety and relaxation (Ayan, 2009; Carson, 2010; Ide, Laurindo, Rodrigues‐Júnior & Tanaka,
2008). The effectiveness of the response to respiratory muscle training was not directly
assessed.
The latest reviews are interested in the most accurate exercise prescription and in its
impact on functional status, symptom reduction and permanence in the workout programs
(Busch, Schachter, Overend, Peloso & Barber, 2008; Bidonde, Jean Busch, Bath &
Milosavljevic, 2014). The comparison between different types of programs that explore and
add new interventions seems a gap yet to be explored in these patients. The objective of this
study was to compare different types of exercise programs used in FM and to know their effects
phisiological on muscle recovery, aerobic fitness and respiratory function over a 24-week
period.

ARTIGO ORIGINAL: Biehl-Printes, C. et al (2019) Comparison on muscle strength, aerobic capacity and respiratory function in women with fibromyalgia, 8 (1): 141 – 159
JOURNAL OF AGING AND INNOVATION, ABRIL, 2019, 8 (1) ISSN: 2182-696X http://journalofagingandinnovation.org/ 144
Material and method
Participants
All members of a local FM association in Portugal were invited to participate in the
study. Thirty-nine potentially eligible subjects searched for more information, twenty persons
signed a written consent to participate in the study. Inclusion criteria were: i) women who were
diagnosed with FM according to the American College of Rheumatology criteria (Wolfe et al.,
1990; Wolfe et al., 2010), ii) sedentary for more than six months, and iii) aged between 35 and
55 years old. Exclusion criteria were: i) other diseases that could prevent physical loading, and
ii) who has attended other physical therapy in the last 6 months. These 20 female were
distributed either to an aerobic-breath group (AbG; n=10) or combined group – aerobic-
strength-breath (CG; n=10). From the 20 participants, one of AbG and two of CG were
excluded leaving voluntarily or failure to attend 80% of the exercise sessions. Finally, 9
participants from the AbG and 8 participants from the CG fully completed the study protocol
and their results were included in the analysis. The study was approved by the Committee on
Biomedical Ethics of the University of Córdoba and followed the updates of the Declaration of
Helsinki.
Procedure
Each participant performed the physical tests in two sessions. The order of application
was the same from the beginning to the end of the 24-week intervention. The first session was
divided in: lung function test (1) and cardiorespiratory exercise test (2) (CPET). After an interval
of 48 hours for recovery, the second session was performed by using a strength test (3).
Materials and measures
Lung function test was assessed by global body plethysmography Masterlab (Medizintechnik
mit System Erich Jaeger Gmbh®, Wuerzburg, Germany), with a specific software and
complying with the standards of the ERS and ATS. Conventional pulmonary function test was
used, based on the determination of the Spirometry (ventilatory proof) and Maximal
Respiratory Pressure (PMR). The spirometry was used as a diagnostic evaluation with the aim
to exclude additional diseases. The monitored parameters were: forced vital capacity (FVC),
maximum expiratory volume in the first second (FEV1), Tiffeneau index = FEV1/FVC, ratio and
maximal expiratory flow at 50% of FVC (MEF50). In the study of muscular efficiency, three
parameters were monitored: the maximal inspiratory pressure (MIP), maximal occlusion
pressure (P0.1 max) and maximal expiratory pressure (MEP). Basically, a high MIP (> - 80
cmH2O = 7.85Kpa) or a MEP high (> 90 cmH2O = 8.80Kpa) excludes inspiratory or expiratory
weakness as clinically important. The measurement of P0.1 max. is used because it is more

ARTIGO ORIGINAL: Biehl-Printes, C. et al (2019) Comparison on muscle strength, aerobic capacity and respiratory function in women with fibromyalgia, 8 (1): 141 – 159
JOURNAL OF AGING AND INNOVATION, ABRIL, 2019, 8 (1) ISSN: 2182-696X http://journalofagingandinnovation.org/ 145
specific and is not affected by external interference. A minimum of 5 attempts was carried out
to demonstrate a consistent effort, being two of these maximum reproducible manoeuvres (i.e.
that were not different among themselves more than 5%) (ATS/ERS, 2002). The predicted
values for healthy persons were calculated according to sex, age and height (Wilson, Cooke,
Edwards & Spiro, 1984). This calculation was performed by global body plethysmography
Masterlab software (Medizintechnik mit System Erich Jaeger Gmbh®).
Cardiopulmonary test was evaluated by cardiopulmonary exercise test (CPET) in a cycle-
ergometer (oxy-ergometry) with direct determination of VO2 and blood gases.
It was used an electromagnetic bicycle ergometer JAEGER (0-600 Watt), an
electrocardiograph 12-channel, a sphygmomanometer, a microanalyser equipment blood
gases Radiometer ABL 5 and a set ergo-spirometric computerized Oxicon Pró - JAEGER
(RFA) for the registration of volumes and ventilatory debits by pneumatocagrofia open circuit
(Medizintechnik mit System Erich Jaeger Gmbh®, Wuerzburg, Germany). The parameters that
were used for this study were: the measurements at rest, the submaximal and maximum
oxygen consumption (VO2) and the submaximal and maximal of aerobic power (W). The
Wassermann incremental protocol was adopted in cycle ergometer (Wasserman, Van Kessel
& Burton, 1967). The level of aerobic fitness for women according to age – VO2max (ml/kg/min)
is based on the classification of the American Heart Association – AHA reference (American
College of Cardiology & American Heart Association, 2000). The predicted values for healthy
people were calculated by specific software.
Strenght Test was evaluated by isokinetic dynamometer (Biodex, System 3, NY, U.S.A.) to
measure isokinetic concentric strength of knee flexion/extension (N.m). The participant was
positioned according to the instructions established for this equipment by Biodex Medical
System. The test was preceded by 5 minutes of warming of the lower limbs on a bicycle
(Monark) at 60 rpm and load regulation at 2% of total body weight. Moreover, before testing
the participants, there was still a previous period of familiarization with the dynamometer. For
the test interpretation, we evaluated the absolute values of the peak torque (N.m): three
repetitions at 60º/s. The Freedson classification to the degree of muscular strenght to 60º/s
(low) was applied (Zeevi, 2002).
Exercise intervention
Aerobic-breath group (AbG). The exercise program consisted of 3 weekly sessions of 60
minutes for 24-weeks. Each session included 30 minutes of aerobic exercise divided in static
bicycle and treadmill. The intensity of aerobic exercise was individualized by power
measurements (W) and heart rate of the anaerobic threshold (HR-AT) obtained through CPET
with controlled speed between 50 and 60 RPM (revolutions per minute). After aerobic training,

ARTIGO ORIGINAL: Biehl-Printes, C. et al (2019) Comparison on muscle strength, aerobic capacity and respiratory function in women with fibromyalgia, 8 (1): 141 – 159
JOURNAL OF AGING AND INNOVATION, ABRIL, 2019, 8 (1) ISSN: 2182-696X http://journalofagingandinnovation.org/ 146
joint mobilization exercises, stretches of major and the most contracted muscle groups were
held. The workout ended with breathing exercises.
Combined group (CG). Combined exercise: aerobic-breath-strength training. The program
consisted of 3 weekly sessions of 60 minutes. Each session included 30 minutes of aerobic
exercise divided alike in static bicycle and treadmill. The intensity was also individualized
through the measures of power (W) and anaerobic threshold (HR-AT) obtained CPET and the
same 50 and 60 RPM. After and following aerobic exercises, it was combined strength
exercises (muscular resistance) for 15 minutes in two of the three-day programs. This research
complied with the recovery of 48 hours recommended. The strength exercises were carried
out on bodybuilding machines for the large muscle groups of the trunk, with upper and lower
limbs, based on guidelines suggested in the bibliography for fibromyalgia (Jones, Clark &
Bennett, 2002). The measurements of the lower limbs were selected to analyse and interpret
the results of this experiment. The CG patients also ended with breathing exercises.
Breathing exercises (carried out in both groups): At the end of each session, the exercise
programs were completed with 15 minutes of breathing exercises (Goldstein, 1997). This
consisted in five exercises (3 minutes for each) which were performed in the form of a circuit:
an exercise on awareness of breathing, an exercise on costal expansion, and three
diaphragmatic breathing exercise (Biehl-Printes & Costa, 2006).
Statistical analysis
Normality and homogeneity of variance of data were initially tested using the Shapiro-
Wilke and Levene tests, respectively. The statistical significance between groups was
evaluated using non-parametric Mann-Whitney test to compare independent samples, in
baseline (M0), in 24-week (M1). Wilcoxon test was implicated to compare paired data before
and after intervention (M0-M1) and also to compare the values of ventilatory parameters,
maximum respiratory pressures and VO2max with predicted values calculated for healthy
persons. The relationships between the selected variables were assessed by the Spearman
test. The effect size (ES) analysis for all outcomes that did not achieve statistical significance
was conducted using Cohen interpretation (< 0.5 small, 0.5 - 0.8 average, and > 0.8 large)
(Sullivan & Feinn, 2012). For all tests it was considered a significance level < 0.05. The
analyses were performed using SPSS v.22.0 (IBM, New York, USA).
Results
Baseline data did not show any significant differences in characteristics
Table 1. Characteristics of females with fibromyalgia at baseline.

ARTIGO ORIGINAL: Biehl-Printes, C. et al (2019) Comparison on muscle strength, aerobic capacity and respiratory function in women with fibromyalgia, 8 (1): 141 – 159
JOURNAL OF AGING AND INNOVATION, ABRIL, 2019, 8 (1) ISSN: 2182-696X http://journalofagingandinnovation.org/ 147
Table 1. Values expressed as mean ± standard deviation. P-values of Mann-Whitney test to
compare differences between groups in baseline. AbG: aerobic-breath group (n=9); CG:
combined group (n=8). Considered a significance level < 0.05
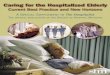
between groups (table 1). nor in ventilatory parameters compared to predicted values
calculated for healthy people used to exclude respiratory diseases (figure 1).
Figure 1: Ventilatory parameters used as a diagnostic to exclude respiratory diseases in
baseline. Values of forced vital capacity (FVC), maximum expiratory volume in the first second
(FEV1), FEV1/FVC ratio, and maximal expiratory flow at 50% of FVC (MEF50) in women with
fibromyalgia syndrome and predicted values for healthy persons calculated according to sex,
age and height in software (Medizintechnik mit System Erich Jaeger Gmbh®, Wuerzburg,
Germany). Values expressed as mean. AbG: aerobic-breath group (n=9); CG: combined group
AbG CG P
Age (years) 49.0 ± 6.3 46.1 ± 5.8 0.435
Weight (kg) 64.2 ± 7.5 60.5 ± 7.7 0.520
Height (m) 1.57 ± 0.05 1.55 ± 0.03 0.260
Body mass index (kg/m2) 26.1 ± 3.5 25.2 ± 3.3 0.873
Number of tender points (scale 1-18) 16.3 ± 2.1 17.0 ± 1.8 0.181
Duration of condition (years) 12.1 ± 10.6 10.8 ± 7.3 0.747
Diagnostic (years) 4.0 ± 1.1 5.1 ± 1.9 0.204
Number of specific drugs (antidepressives,
muscular relaxants, analgesics)
2.2 ± 1.8 2.8 ± 2.1 0.870

ARTIGO ORIGINAL: Biehl-Printes, C. et al (2019) Comparison on muscle strength, aerobic capacity and respiratory function in women with fibromyalgia, 8 (1): 141 – 159
JOURNAL OF AGING AND INNOVATION, ABRIL, 2019, 8 (1) ISSN: 2182-696X http://journalofagingandinnovation.org/ 148
(n=8). P-value of Wilcoxon test; n.s. = not significant differences. It was considered a
significance level < 0.05.
In (table 2) significant differences were detected in MIP and P0.1 max in favour of
predicted values calculated for healthy persons. Additionally, no significant differences in
baseline data for muscular efficiency of the MRP between AbG and CG. After 24-weeks MIP
and P01 max were significant in both groups. There were not observed any significant
differences between groups for these variables. The effect size was small in most of the
variables (ES <0.5). For MEP no significant difference was observed. Moreover, the significant
correlations were shown between P0.1 max and MIP in baseline (r = 0.61; p = 0.030) and week
24 (r = 0.60; p = 0.030).
Table 2. Maximal respiratory pressures in women with fibromyalgia syndrome at baseline and after 24 weeks of intervention.
Baseline (M0)
Week 24 (M1)
Effect Size Cohen´s d
AbG CG AbG CG †P AbG
†P CG
¶P
M0
¶P
M1
(M0-M1) AbG
(M0-M1) CG
M0 M1
MIP (kPa) 5.2 ±
1.7
4.3 ±
0.9
6.3 ±
1.2
5.8 ±
1.5
.027 .027 .521 .748 N.A. N.A. 0.59 0.33
MIP (kPa) 11.0 ±
0.0
11.0 ±
0.0
11.0±
0.0
11.0±
0.0
.027 .027 N.A. N.A. N.A. N.A. N.A. N.A.
MEP (kPa) 5.8 ±
1.4
6.6 ±
2.5
5.9 ±
1.8
7.0 ±
3.2
.753
.345 .872 .471 0.06 0.12 0.35 0.38
MEP (kPa) 7.2 ±
0.6
7.7 ±
0.3
7.2 ±
0.6
7.7 ±
0.3
.115 .173 N.A. N.A. N.A. N.A. N.A. N.A.
P0.1max
(kPa)
1.1 ±
0.4
1.4 ±
0.72
1.6 ±
0.7
2.4
±
0.7
.043
.027 .423 .128 N.A. N.A. 1.13 0.89
P0.1 max
(kPa)
7.6 ±
0.0
7.7 ±
0.0
7.6 ±
0.0
7.7±
0.0
.027
.027 N.A. N.A. N.A. N.A. N.A. N.A.
Table 2. Values expressed as mean ± standard deviation. P-values of Wilcoxon test to
compare differences within group after 24 weeks of intervention and to compare the values
maximum respiratory pressures with predicted values calculated for healthy persons.
P-values of Mann-Whitney test to compare differences between groups in baseline (M0) and
week 24 (M1). M0-M1: effect size within group; M0: effect size between groups in baseline;
M1: effect size between groups in week 24; (ES>0.8): N.A: not applied. Parameters: MIP:

ARTIGO ORIGINAL: Biehl-Printes, C. et al (2019) Comparison on muscle strength, aerobic capacity and respiratory function in women with fibromyalgia, 8 (1): 141 – 159
JOURNAL OF AGING AND INNOVATION, ABRIL, 2019, 8 (1) ISSN: 2182-696X http://journalofagingandinnovation.org/ 149
maximum inspiratory pressure; MEP: maximum expiratory pressure; P0.1max: maximum
occlusion pressure and MIP; MEP; P01max predicted values to health persons calculated
according with software (Medizintechnik mit System Erich Jaeger Gmbh®, Wuerzburg,
Germany). AbG: aerobic-breath group (n=9); CG: combined group (n=8). Considered a
significance level < 0.05.
In (Table 3) at baseline, each group has physiological parameters within normal limits, as well
the basal rate shows no significant differences. After 24-weeks, differences (p <0.05) were
found in the oxygen consumption by both groups on the aerobic-anaerobic transition i.e.
anaerobic threshold (VO2AT) at maximum VO2max (ml/min), VO2max (ml/kg/min) and in the
% VO2max. The power (W) was significant in either group. There were no significant
differences between groups for these variables. The effect size was small in most of the
variables (ES <0.5).
Table 3. Oxygen consumption, and power in women with fibromyalgia syndrome at baseline and after 24 weeks of intervention.
Baseline (M0) Week 24 (M1)
AbG
CG AbG CG †P AbG †P CG
¶P M0 ¶P M1
(M0-
M1) AbG
M0-M1) CG
M0 M1
VO2 basal
(mL/min)
198.5±50.
4
219.0±72.2 239.5±80.2 264.5±83.0 .086 .057
.287 .260
0.55
0.52
0.31 0.27
VO2AT
(mL/min)
1051.5±
204.5
1017.6±116.
7
1210.3±172 1264.8±170.
6
.013 .013
.436 .131
N.A.
N.A.
-0.18
0.28
VO2Max
(mL/min)
1330.8±
225.6
1428.1±
101.5
1497.0±141
.3
1628.3±143.
9
.013 .013
.186 .039
N.A.
N.A.
0.50
N.A.
VO2Max
health persons predicted (mL/min)
1461.1±
186.4
1525.3±
111.2
1423.5±
182.7
1537.6±97.1 .053 .102
N.A. N.A.
N.A
N.A
.
N.A.
N.A.
VO2Max (mL/kg/mi
n)
20.6± 3.3 24.4± 5.0 24.3± 3.4 27.1± 4.4 .027 .027
.200 .298
N.A.
N.A.
0.80
0.64
%VO2
Max 91.1%±
12.3
94.1± 11.3 106.6± 12.1 106.5± 13.7 .013 .013
.344 .436
N.A.
N.A.
0.23 -0.01
W-AT 44.0±11.4 45.0±10.
5
60.0±4.5 63.0±5.
2
.033 .013
.374 .315
N.A.
N.A.
0.08
0.55

ARTIGO ORIGINAL: Biehl-Printes, C. et al (2019) Comparison on muscle strength, aerobic capacity and respiratory function in women with fibromyalgia, 8 (1): 141 – 159
JOURNAL OF AGING AND INNOVATION, ABRIL, 2019, 8 (1) ISSN: 2182-696X http://journalofagingandinnovation.org/ 150
W-Max 59.5±9.6 60.3±5.2 80.0±8.2 83.3±10.
3
.03
3
.01
3
.315 .189
N.A.
N.A.
0.09 0.32
Table 3. Values expressed as mean ± standard deviation. †P-values of Wilcoxon test to compare differences within group after 24 weeks of intervention and to compare the values VO2 max (mL/min) with predicted values VO2 max (mL/min) calculated for healthy persons. ¶P-values of Mann-Whitney test to compare differences between groups in baseline (M0) and week 24 (M1). M0-M1: effect size within group; M0: effect size between groups in baseline; M1: effect size between groups in week 24; (ES>0.8); N.A.: not applied. Parameters: Oxygen consumption (VO2): Oxygen consumption basal (VO2 basal), Anaerobic Threshold (VO2AT), Maximal oxygen consumption in absolute values VO2 max (mL/min), Maximal oxygen consumption for health persons predicted (VO2 max health persons) calculated by specific software. Maximal oxygen consumption in relative values VO2 max (mL/(kg/min), Percentage maximal oxygen consumption VO2Max/VO2Max health persons predicted (%VO2 max); Power (W) in Anaerobic Threshold (W-AT), Watts in Maximal (W-Max); In the AbG: aerobic-breath group (n=9); CG: combined group (n=8). Considered a significance level < 0.05.
In (Table 4) it is seen that both groups show significant differences in the strength after
24- weeks. In the M1, in the majority of the results significant differences were found (p <0.05)
between the groups. The effect size was medium on right extensors and flexor 60°/s. The level
of classification of the normative values (N.m) of Freedson was initially low with evolution no
more than an percentile of 50 after 24 weeks.
Table 4. Isokinetic concentric strength of knee flexion/extension and normative values in women with fibromyalgia syndrome at baseline and after 24 weeks of intervention.
Baseline (M0)
Week 24 (M1)
Effect Size Cohen´s d
AbG CG AbG CG †P AbG
†P CG
¶P
M0
¶
P
M
1
(M0-M1)
AbG
(M0-M1)
CG
M0
M1
Right leg strength Extensors 60°/s Percentile Freedson (10-30-50-70- 90)
90.3
5±2
0.6
<10
102.23±1
7.23
10
102.71±25
.99
10
118.7±18.
33
30
.013
.013
.168
.168
N.A.
N.A.
0.56
0.64

ARTIGO ORIGINAL: Biehl-Printes, C. et al (2019) Comparison on muscle strength, aerobic capacity and respiratory function in women with fibromyalgia, 8 (1): 141 – 159
JOURNAL OF AGING AND INNOVATION, ABRIL, 2019, 8 (1) ISSN: 2182-696X http://journalofagingandinnovation.org/ 151
Right leg strength Flexors 60°/s Percentile Freedson (10-30-50-70- 90)
46.6
1±8.
22
<10
55.23±13
.32
<10
55.23±13.
32
<10
65.33±9.41
10
.013
.13 .078
.100
N.A.
N.A.
N.A.
0.78
Left leg strength Extensors 60°/s Percentile Freedson (10-30-50-70- 90)
90.5
3±2
2.20
<10
105.66±1
6.78
10
99.86±23.
22
10
122.87±21
.22
50
.013
.013
.100
.027
N.A.
N.A.
0.69
N.A.
Left leg strength Flexors 60°/s Percentile Freedson (10-30-50-70- 90)
43.9
8±1
0.92
<10
55.11±5.
88
<10
52.25±12.
56
<10
65.99±7.2
3
10
.013
.013
.051
.027
N.A.
N.A.
N.A.
N.A.
Table 4. Values expressed in N.m (mean ± standard deviation). †P-values of Wilcoxon test to compare differences within group after 24 weeks of intervention. ¶P-values of Mann-Whitney test to compare differences between groups in baseline (M0) and week 24 (M1). M0-M1: effect size within group; M0: effect size between groups in baseline; M1: effect size between groups in week 24; (ES>0.8); N.A.: not applied. Normative value Freedson. AbG: aerobic-breath group (n=9); CG: combined group (n=8). Considered a significance level < 0.05.
Discussion
In the last 25 years aerobic exercise and strength training has been strongly
recommended for the management of FM (Busch et al., 2011). The respiratory disorders,
identified as a common factor for these individuals, is attributed to a dysfunction of the
respiratory muscles much associated with the diaphragm (Lurie, Caidahl, Johansson &
Bake,1990; Sahin, Ulubas, Calikoglu & Erdogan, 2004). Despite this, the literature is still
scarce about the effects of respiratory intervention on these patients. In this sense, the present
study showed that patients with FM recover in 24 weeks the functional performance in
traditional physical components, aerobic fitness, strength and respiratory function, without
differences between the programs.
Symptoms such as tiredness, fatigue and non-restorative sleep directly influence the
functional response of people with FM, impairing the carrying out the activities of daily living
(ADLs) (Huijnen, Verbunt, Meeus & Smeets, 2015). Still associated with this low capacity of
strength and resistance aerobic, the limitations in respiratory muscle function interfere in the
best performance of cardiorespiratory function (Pamplona & Morais, 2007). Therefore, seems
more prudent a guideline of exercise focused on the simultaneous recovery of diminished
parameters through a combination of these elements than interventions in isolation.

ARTIGO ORIGINAL: Biehl-Printes, C. et al (2019) Comparison on muscle strength, aerobic capacity and respiratory function in women with fibromyalgia, 8 (1): 141 – 159
JOURNAL OF AGING AND INNOVATION, ABRIL, 2019, 8 (1) ISSN: 2182-696X http://journalofagingandinnovation.org/ 152
As reported in other studies with combined training (aerobic strength) in patients with
FM, this study also shows significant evidence through the combined program in mode
gradually and progressively (Rooks, Silverman & Kantrowitz, 2002). Studies on the strength
production of the lower limbs with isokinetic assessment in patients with FM also reported a
reduction of this capacity and indicated these patients have this function impaired (Tomas-
Carus et al., 2009). According with these authors, the present study shows that participants
with FM have the muscle strength in the lower limbs decreased relatively to baseline. This is
confirmed according to Freedson's percentile as the FM participants have this decreased
functional condition, in both extension and flexion of the knees 21. After the interventions, the
improvements are remarkable, the normative level is increasing up to 50 of the percentiles as
can be seen by the greater expressiveness of the results in CG. The muscle strengthening
through the resistance muscle training appears as the most effective method for the recovery
of muscle strength and has been described by many health organizations for the improvement
of health and muscular conditio (Pollock et al., 1998). The extensor and flexor muscles of the
knees play a determining role in the stability of the body and locomotion. The use in the slow
and fast walking, climbing stairs and raising from a chair has been well documented in studies
kinematics, electromyography and kinetic analysis (Collado-Mateo et al., 2016). It also has
been considered essential to enable the activities of daily living in patients with FM (Tomas-
Carus et al., 2009). The effect of strength exercises applied to the lower limbs of CG caused
an increase in muscle strength contributing to better performance on tasks such as locomotion,
crouch down and up and down stairs.
On the other hand, another aspect that has been described in patients with FM and
elderly is the consequence of the reduced muscle mass associated with the alterations in
energy metabolism and aerobic capacity which predisposes the weakness and atrophy that
leads the condition of increased risk of falls (Jones, Horak, Winters, Morea & Bennett, 2009;
Lord, Ward, Williams & Strudwick, 1995). In this sense, un low aerobic capacity were assessed
in the present study, which showed that both groups presented alterations, both at the
submaximal level and at the maximum level of the evaluated parameters. In the basal rate
there was an improvement in the availability of oxygen but expressionless in the statistical
level. Therefore, the measurement of the maximum oxygen uptake (VO2max), which
corresponds to the maximum aerobic capacity of each individual, is the estimated parameter
that best reflects the capacity of the cardiocirculatory and respiratory systems, and more
specifically, the performance of the system for collecting, transport and peripheral utilization
O2 (American College of Cardiology & American Heart Association, 2000). Indeed, these
results corroborate with other studies based on the American Heart Association (AHA)
classification, which described that most FM patients is below average levels of conditioning,

ARTIGO ORIGINAL: Biehl-Printes, C. et al (2019) Comparison on muscle strength, aerobic capacity and respiratory function in women with fibromyalgia, 8 (1): 141 – 159
JOURNAL OF AGING AND INNOVATION, ABRIL, 2019, 8 (1) ISSN: 2182-696X http://journalofagingandinnovation.org/ 153
as well as the maximum oxygen consumption and the decreased anaerobic threshold are
attributed to the consequences of physical inactivity, pain or fatigue (Pollock et al., 1998; Valim
et al., 2002). Additionally, as also has been prized and recommended by the literature the use
of submaximal parameters for the assessment and exercise prescription (Valim, 2006; Valim
et al., 2002). As such, the criteria for classification of participants with FM in this study were
initially low, classified as steady (24 ml/kg/min) to the CG and weak (20 ml/kg/min) to AbG.
The CPET were suspended in all participants due to early muscle fatigue. The results obtained
in the CPET show that in the baseline the physiological tolerance of the FM participants is
normal to the effort. The average value of VO2max is within the normal range for either group,
i.e, above 84% of VO2max (Saltin & Rowel, 1980). Concluding that, the functional capacity of
the organism involved in O2 transport system and the use of peripheral muscles is normal or
that those small non-relevant changes that exist would be compensated by intervention. This
includes the normality respiratory system (ventilation, diffusion capacity, exchanges of
alveolar-capillary gases and pulmonary circulation) from the heart (HR and Systolic Volume)
of the circulation (blood vessels and hemoglobin concentration) and the ability of the skeletal
muscles to remove enough O2 during exercise.
In sedentary individuals changes in aerobic condition are expected when they are
subjected to an exercise program for a period of 6 months, 3 times / week, 30 min / day and
the intensity of 75% VO2max (Pollock, 1973). The established aerobic training for both groups
showed significant evidence for obtaining VO2max. This response was most evident in CG. In
accordance with the proposed of training aerobic for patients with FM, based on submaximal
measures, a greater effect of gains was obtained in the anaerobic threshold of VO2 (VO2AT)
than in the maximum level (VO2max) in both groups. Studies of sedentary individuals and
patients with FM have demonstrated that lactic anaerobic threshold can increase with training,
even without significant changes in VO2max (Saltin & Rowel, 1980; Denis, Fouquet, Poty,
Geyssant & Lacour, 1982). The significant increase in the VO2AT obtained in both groups adds
value to submaximal training and shows the positive effect of this. Once interested in the
impact of submaximal training on fitness of the lower limbs, it is also important to highlight the
changes in aerobic power (W) in both groups. Basically, in the analysis of oxygen consumption
the CG shows a tendency to be more effective than AbG in 24 weeks. The results obtained in
the study of aerobic condition were important because it enabled the accomplishment of most
activities of daily living (ADLs) in aerobiosis. This way and through regular training the pain
caused by physical effort may be excluded in moderate AVD.
The respiratory function associated with physical intervention in patients with FM has
been a shortcoming in physical activity programs of non-pharmacological treatment. Although
there nearly three decades of conclusions on respiratory muscle weakness in these patients,

ARTIGO ORIGINAL: Biehl-Printes, C. et al (2019) Comparison on muscle strength, aerobic capacity and respiratory function in women with fibromyalgia, 8 (1): 141 – 159
JOURNAL OF AGING AND INNOVATION, ABRIL, 2019, 8 (1) ISSN: 2182-696X http://journalofagingandinnovation.org/ 154
it was shown little besides characteristics of these parameters (Lurie, Caidahl, Johansson &
Bake, 1990; Sahin, Ulubas, Calikoglu, & Erdogan, 2004).
Considering the set of physical disorders in FM, this study considered relevant
integration of breathing exercises aiming to develop conditions to better explore the effect of
aerobic training. The re-education of breath of a person interferes directly in the work and
action of the respiratory muscle. The MRP have been used for assessing the respiratory
muscle strength in patients with FM, showing that these patients have lower MIP and MEP
values, which may indicate respiratory muscle dysfunction, including the diaphragm muscle
(Forti, Zamunér, Andrade & Silva, 2016; Printes, 2012).
However, the influence of a possible mechanism related to the central brainstem
should not be completely eliminated (Green, 2002). This study showed lower MIP and MEP
values in these patients. In this sense, the test of spirometry was initially conducted to rule out
any pathology superimposed. Thus, as shown in other studies, ours also showed that the
parameters analysed for ventilator exclude the possibility of respiratory pathology (Forti,
Zamunér, Andrade & Silva, 2016; Sahin, Ulubas, Calikoglu, & Erdogan, 2004).
The previous literature reported that factors such as motivation and cooperation of
patients may affect maximal respiratory pressures measurements (ATS/ERS, 2002; Vincken,
Ghezzo & Cosio, 1987). In this sense the use of plethysmografhy provides the measure of
occlusion maximum pressure of air in the airways using 0.1 second (P0.1 max), measure that
is not influenced by cooperation or motivation of the patient and has been explored in studies
of respiratory function as a complement of MIP and MEP (Vincken, Ghezzo & Cosio, 1987;
Burki, Mitchell, Chaudhary & Zechman, 1977). According to these bases, our study showed
significant correlation between MIP and P0.1 max in baseline (r=0.61) and after 24 weeks of
intervention (r=0.60), which could rule out any effect related to lack of motivation of patients in
the measurements. Furthermore, the influence of the factor learning effect was excluded for
having complied accurately with the conventional protocol of the European Respiratory Society
(ERS) (ATS/ERS, 2002).
In the present study, differences for MIP were observed between participants with FM
and predicted values calculated for healthy persons. The respiratory muscle training focused
on the DB uses exclusively the muscle diaphragm (abdominal wall), reducing the movement
of upper thoracic region, with a normal tidal volume and passive expiration (Goldstein, 1997;
Biehl-Printes & Costa, 2006). Thus, our results indicate that the respiratory muscle training DB
could also be useful for improving respiratory muscle strength and tolerance to exercise in
patients with FM, as already proved for patients with asthma and subjects with subacute stroke
(Burgess, Ekanayake, Lowe, Dunt, Thien & Dharmage, 2011; Sutbeyaz, Koseoglu, Inan &
Coskun, 2010). As suggested in the few studies of respiratory function in FM patients, the

ARTIGO ORIGINAL: Biehl-Printes, C. et al (2019) Comparison on muscle strength, aerobic capacity and respiratory function in women with fibromyalgia, 8 (1): 141 – 159
JOURNAL OF AGING AND INNOVATION, ABRIL, 2019, 8 (1) ISSN: 2182-696X http://journalofagingandinnovation.org/ 155
present study corroborates and proposes that PMR values are attributed to probable muscle
weakness of the respiratory muscles due to lack of use (Forti, Zamunér, Andrade & Silva,
2016; Sahin, Ulubas, Calikoglu, & Erdogan, 2004; Lurie, Caidahl, Johansson & Bake, 1990).
The present study also included limitations which require further discussion. The limited
size of the sample may have contributed to lower statistical power to detect changes in some
variables. Nevertheless, the most variables measured that did not show positive effects
presented a small effect size (<0.5). The lack of difference after 24 weeks of different trial of
exercise, AbG vs. CG, is attributed to the introduction of the training mode: “gradual and
progressive”. We emphasize the importance of following the initial procedure indicated to
preserve the security, adaptation, comfort and furthermore ensure adhesion and permanency
of patients in programs (Rooks, D. S., Silverman, C. B., & Kantrowitz, F. G. (2002); Sañudo et
al., 2010; Bidonde, Jean Busch, Bath & Milosavljevic, 2014; Jones, Clark & Bennett, 2002).
In conclusion, breathing exercises applied to both groups have an impact to be
considered for rehabilitation due to the lack of studies applying the intervention of the DB as a
co-adjuvant of physical exercise in the treatment of fibromyalgia. However, new studies with
long-term programs are suggested to compare the absolute impact of different workouts, as
well as the isolated practice of breathing exercises can be considered.
References
1. American College of Cardiology, & American Heart Association. (2000). Clinical competence
statement on stress testing. J Am Coll Cardiol, 36, 1441-53.
2. Ayan, C., Alvarez, M. J., Alonso-Cortés, B., Barrientos, M. J., Valencia, M., & Martín, V.
(2009). Health education home-based program in females with fibromyalgia: a pilot study.
Journal of back and musculoskeletal rehabilitation, 22(2), 99-105.
3. Bidonde, J., Jean Busch, A., Bath, B., & Milosavljevic, S. (2014). Exercise for adults with
fibromyalgia: an umbrella systematic review with synthesis of best evidence. Current
rheumatology reviews, 10(1), 45-79.
4. Biehl-Printes C, Costa RG. (2006). Fibromialgia em movimento: prática diária de exercícios
(p. 21-26). Lisboa. (Eds) Myos – Associação Nacional Contra a Fibromialgia e Síndrome da
Fadiga Crónica.
5.Burgess, J., Ekanayake, B., Lowe, A., Dunt, D., Thien, F., & Dharmage, S. C. (2011).
Systematic review of the effectiveness of breathing retraining in asthma management. Expert
review of respiratory medicine, 5(6), 789-807.

ARTIGO ORIGINAL: Biehl-Printes, C. et al (2019) Comparison on muscle strength, aerobic capacity and respiratory function in women with fibromyalgia, 8 (1): 141 – 159
JOURNAL OF AGING AND INNOVATION, ABRIL, 2019, 8 (1) ISSN: 2182-696X http://journalofagingandinnovation.org/ 156
6.Burki, N. K., Mitchell, L. K., Chaudhary, B. A., & Zechman, F. W. (1977). Measurement of
mouth occlusion pressure as an index of respiratory centre output in man. Clinical Science,
53(2), 117-123.
7.Busch, A. J., Schachter, C. L., Overend, T. J., Peloso, P. M., & Barber, K. A. (2008). Exercise
for fibromyalgia: a systematic review. The Journal of rheumatology, 35(6), 1130-1144.
8.Busch, A. J., Webber, S. C., Brachaniec, M., Bidonde, J., Dal Bello-Haas, V., Danyliw, A. D.,
... & Schachter, C. L. (2011). Exercise therapy for fibromyalgia. Current pain and headache
reports, 15(5), 358.
9.Carson, J. W., Carson, K. M., Jones, K. D., Bennett, R. M., Wright, C. L., & Mist, S. D. (2010).
A pilot randomized controlled trial of the Yoga of Awareness program in the management of
fibromyalgia. PAIN®, 151(2), 530-539.
10.Collado-Mateo, D., Adsuar, J. C., Olivares, P. R., Dominguez-Muñoz, F. J., Maestre-
Cascales, C., & Gusi, N. (2016). Performance of women with fibromyalgia in walking up stairs
while carrying a load. PeerJ, 4, e1656.
11.de Bruijn, S. T., van Wijck, A. J., Geenen, R., Snijders, T. J., van der Meulen, W. J., Jacobs,
J. W., & Veldhuijzen, D. S. (2011). Relevance of physical fitness levels and exercise-related
beliefs for self-reported and experimental pain in fibromyalgia: an explorative study. JCR:
Journal of Clinical Rheumatology, 17(6), 295-301.
12.Denis, C., Fouquet, R., Poty, P., Geyssant, A., & Lacour, J. R. (1982). Effect of 40 weeks
of endurance training on the anaerobic threshold. International Journal of Sports Medicine,
3(04), 208-214.
13.European, R. S., & American Thoracic Society. (2002). ATS/ERS Statement on respiratory
muscle testing. American journal of respiratory and critical care medicine, 166(4), 518.
14.García-Hermoso, A., Saavedra, J. M., & Escalante, Y. (2015). Effects of exercise on
functional aerobic capacity in adults with fibromyalgia syndrome: a systematic review of
randomized controlled trials. Journal of back and musculoskeletal rehabilitation, 28(4), 609-
619.
15.Green, M. (2002). Road J, Sieck GC, Similowski T. Tests of respiratory muscle strength.
Am J Respir Crit Care Med, 166(4), 528-47.
16.Goldstein RS. (1997). Inspiratory Muscle Training. In: Morgan M, and Singh S. Pratical
Pulmonary Rehabilitation (p. 99-115). United Kingdom. Chapman and Hall.
17.Huijnen, I. P., Verbunt, J. A., Meeus, M., & Smeets, R. J. (2015). Energy expenditure during
functional daily life performances in patients with fibromyalgia. Pain Practice, 15(8), 748-756.
18.Ide, M. R., Laurindo, I. M. M., Rodrigues‐Júnior, A. L., & Tanaka, C. (2008). Effect of aquatic
respiratory exercise‐based program in patients with fibromyalgia. International Journal of
Rheumatic Diseases, 11(2), 131-140.

ARTIGO ORIGINAL: Biehl-Printes, C. et al (2019) Comparison on muscle strength, aerobic capacity and respiratory function in women with fibromyalgia, 8 (1): 141 – 159
JOURNAL OF AGING AND INNOVATION, ABRIL, 2019, 8 (1) ISSN: 2182-696X http://journalofagingandinnovation.org/ 157
19.Jones, K. D., Horak, F. B., Winters, K. S., Morea, J. M., & Bennett, R. M. (2009).
Fibromyalgia is associated with impaired balance and falls. Journal of clinical rheumatology:
practical reports on rheumatic & musculoskeletal diseases, 15(1),16.
20.Jones, K. D., Clark, S. R., & Bennett, R. M. (2002). Prescribing exercise for people with
fibromyalgia. AACN Advanced Critical Care, 13(2), 277-293.
21.Forti, M., Zamunér, A. R., Andrade, C. P., & Silva, E. (2016). Lung Function, Respiratory
Muscle Strength, and Thoracoabdominal Mobility in Women With Fibromyalgia Syndrome.
Respiratory care, 61(10), 1384-1390.
22.Lurie, M., Caidahl, K., Johansson, G., & Bake, B. (1990). Respiratory function in chronic
primary fibromyalgia. Scandinavian journal of rehabilitation medicine, 22(3), 151-155.
23.Lord, S. R., Ward, J. A., Williams, P., & Strudwick, M. (1995). The Effect of a 12‐Month
Exercise Trial on Balance, Strength, and Falls in Older Women: A Randomized Controlled
Trial. Journal of the American Geriatrics Society, 43(11), 1198-1206.
24.Pamplona, P., & Morais, L. (2007). Treino de exercício na doença pulmonar crónica.
Revista Portuguesa de Pneumologia, 13(1), 101-128.
25.Printes, C. B. (2012). La asociación de ejercicios de resistencia muscular localizada y su
influencia en la aptitud muscular en enfermos con fibromialgia.
26.Pollock, M. L., Gaesser, G. A., Butcher, J. D., Després, J. P., Dishman, R. K., Franklin, B.
A., & Garber, C. E. (1998). ACSM position stand: the recommended quantity and quality of
exercise for developing and maintaining cardiorespiratory and muscular fitness, and flexibility
in healthy adults. Med Sci Sports Exerc, 30(6), 975-991.
27.Pollock, M. L. (1973). The quantification of endurance training programs. Exercise and sport
sciences reviews, 1(1), 155-188.
28.Rooks, D. S., Silverman, C. B., & Kantrowitz, F. G. (2002). The effects of progressive
strength training and aerobic exercise on muscle strength and cardiovascular fitness in women
with fibromyalgia: a pilot study. Arthritis Care & Research, 47(1), 22-28.
29.Sahin, G., Ulubas, B., Calikoglu, M., & Erdogan, C. (2004). Handgrip strength, pulmonary
function tests, and pulmonary muscle strength in fibromyalgia syndrome: is there any
relationship? Southern medical journal, 97(1), 25-30.
30.Saltin, B., & Rowell, L. B. (1980). Functional adaptations to physical activity and inactivity.
In Federation proceedings (Vol. 39, No. 5, pp. 1506-1513).
31.Sañudo, B., Galiano, D., Carrasco, L., Blagojevic, M., de Hoyo, M., & Saxton, J. (2010).
Aerobic exercise versus combined exercise therapy in women with fibromyalgia syndrome: a
randomized controlled trial. Archives of Physical Medicine and Rehabilitation, 91(12), 1838-
1843.

ARTIGO ORIGINAL: Biehl-Printes, C. et al (2019) Comparison on muscle strength, aerobic capacity and respiratory function in women with fibromyalgia, 8 (1): 141 – 159
JOURNAL OF AGING AND INNOVATION, ABRIL, 2019, 8 (1) ISSN: 2182-696X http://journalofagingandinnovation.org/ 158
32.Segura-Jiménez, V., Álvarez-Gallardo, I. C., Carbonell-Baeza, A., Aparicio, V. A., Ortega,
F. B., Casimiro, A. J., & Delgado-Fernández, M. (2015, April). Fibromyalgia has a larger impact
on physical health than on psychological health, yet both are markedly affected: the al-Andalus
project. In Seminars in Arthritis and Rheumatism (Vol. 44, No. 5, pp. 563-570). Elsevier.
33.Silverman, S. L., Harnett, J., Zlateva, G., & Mardekian, J. (2010). Identifying Fibromyalgia‐
Associated Symptoms and Conditions from a Clinical Perspective: A Step Toward Evaluating
Healthcare Resource Utilization in Fibromyalgia. Pain Practice, 10(6), 520-529.
34.Sullivan, G. M., & Feinn, R. (2012). Using effect size—or why the P value is not enough.
Journal of graduate medical education, 4(3), 279-282.
35.Tomas-Carus, P., Gusi, N., Häkkinen, A., Häkkinen, K., Raimundo, A., & Ortega-Alonso, A.
(2009). Improvements of muscle strength predicted benefits in HRQOL and postural balance
in women with fibromyalgia: an 8-month randomized controlled trial. Rheumatology, 48(9),
1147-1151.
36.Uveges, J. M., Parker, J. C., Smarr, K. L., McGowan, J. F., Lyon, M. G., Irvin, W. S., ... &
Hewett, J. E. (1990). Psychological symptoms in primary fibromyalgia syndrome: relationship
to pain, life stress, and sleep disturbance. Arthritis & Rheumatology, 33(8), 1279-1283.
37.Valim, V., Oliveira, L. M., Suda, A. L., Silva, L. E., Faro, M., Neto, T. L. B., ... & Natour, J.
(2002). Peak oxygen uptake and ventilatory anaerobic threshold in fibromyalgia. The Journal
of rheumatology, 29(2), 353-357.
38.Valim V. (2006). Benefits of Exercise in the Fibromyalgia. Review Article. Rev Bras
Reumatol, 46(1):49-55.
39.Vincken, W., Ghezzo, H., & Cosio, M. G. (1987). Maximal static respiratory pressures in
adults: normal values and their relationship to determinants of respiratory function. Bulletin
europeen de physiopathologie respiratoire, 23(5), 435-439.
40.Sutbeyaz, S. T., Koseoglu, F., Inan, L., & Coskun, O. (2010). Respiratory muscle training
improves cardiopulmonary function and exercise tolerance in subjects with subacute stroke: a
randomized controlled trial. Clinical rehabilitation, 24(3), 240-250.
41.Wasserman, K., Van Kessel, A. L., & Burton, G. G. (1967). Interaction of physiological
mechanisms during exercise. Journal of Applied Physiology, 22(1), 71-85.
42.Wilson, S. H., Cooke, N. T., Edwards, R. H., & Spiro, S. G. (1984). Predicted normal values
for maximal respiratory pressures in caucasian adults and children. Thorax, 39(7), 535-538.
43.Wolfe, F., Smythe, H. A., Yunus, M. B., Bennett, R. M., Bombardier, C., Goldenberg, D. L.,
... & Fam, A. G. (1990). The American College of Rheumatology 1990 criteria for the
classification of fibromyalgia. Arthritis & Rheumatology, 33(2), 160-172.

ARTIGO ORIGINAL: Biehl-Printes, C. et al (2019) Comparison on muscle strength, aerobic capacity and respiratory function in women with fibromyalgia, 8 (1): 141 – 159
JOURNAL OF AGING AND INNOVATION, ABRIL, 2019, 8 (1) ISSN: 2182-696X http://journalofagingandinnovation.org/ 159
44.Wolfe F, Clauw DJ, Fitzcharles MA, Goldenberg DL, Katz RS, Mease P, et al. The American
College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of
symptom severity. Arthritis Care Res. 2010; 62:600-10.
45.Zeevi Dvir, (2002). Isokinetics Muscle testing, Interpretation and Clinical Applications (p.73-
143). United Kingdom. Churchill Livingstone.
Recommended