Epidemiology
Childhood Anxiety Disorders[With Emphasis on Anxiety Disorders- Issues,
Diagnosis, Management]
Selective MutismPost-traumatic Disorder
Obsessive Compulsive Disorders
Phobias - Specific
/Generalized
Generalized anxiety & Panic
disorder
ClassificationSlides before 1st Section Divider
Summary References
ChairpersonProf. Dr. Ramanujam MD, DPM
Dr. SJX Sugadev MD, Asst. Professor
19th June 2013Presented by
Dr. Anusa AM2nd Year MD PG
Madurai Medical College
Prepared by Prof. Rooban T,
Oral & Maxillofacial Pathologist

Anxiety Disorders
A set of syndromes
Signs and Symptoms – Part of many
disorders
No organic cause
Previously a part of “Neurotic”
With understanding of disorders – many
have been demonstrated to have organic
cause
Definition – “Neurotic”
All local and general nervous disorders which do not depend on known local pathological lesions of the nervous system.
Does not imply - diseases have an entirely unknown pathology, but cannot be morphologically classified.
Neurotic Disorders - Definition
Collection of psychiatric disorders without psychotic symptoms and lacking the intense psychopathology
Neurosis is an umbrella term for nonpsychotic personality disorders
Definition
Disorder that has no known or suspected basis in
organic pathology, and may lead to the distortions in
behavior and social adaptation – Cawley 1983
Is a disorder of internal balance and relationships with
the environment. These disturbances leading to
neurosis arise from internal conflicts and neurotic
tendencies – Lapiński, 1983
Neurotic symptoms occur when the organism is in
danger, and when it may not be able to cope with the
external or internal situation – Kępiński, 2005

Is the term “Valid”
Term “Neurosis”- Obsolete Discontinued by American
Psychiatric Association from 1992 Appears sparingly in ICD-10
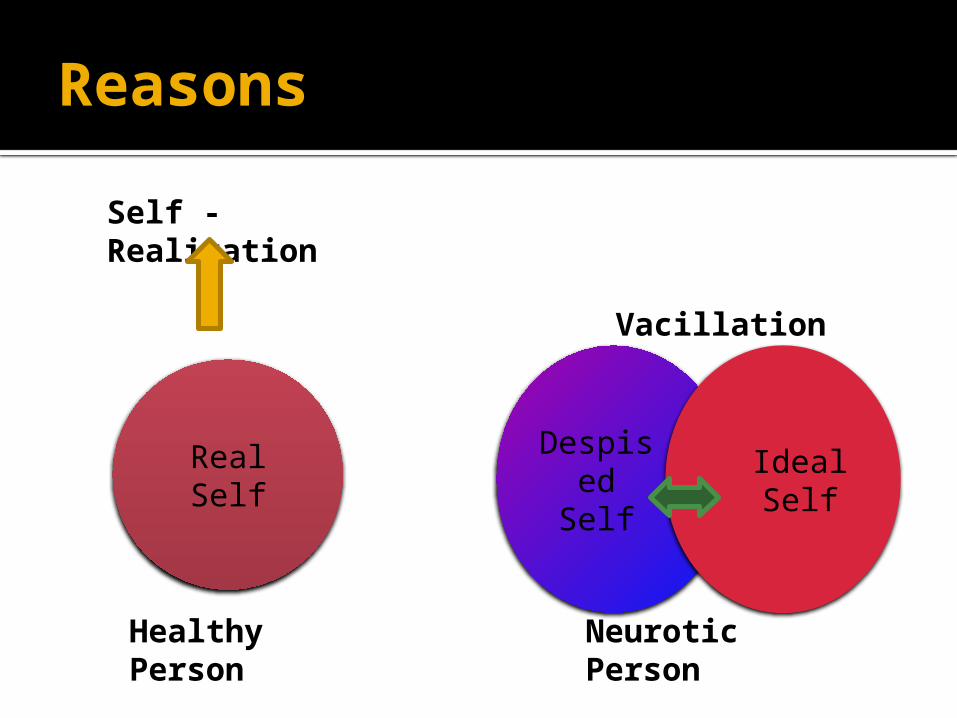
Reasons
Real Self Despised Self
Ideal Self
Healthy Person
Self - Realization
Neurotic Person
Vacillation
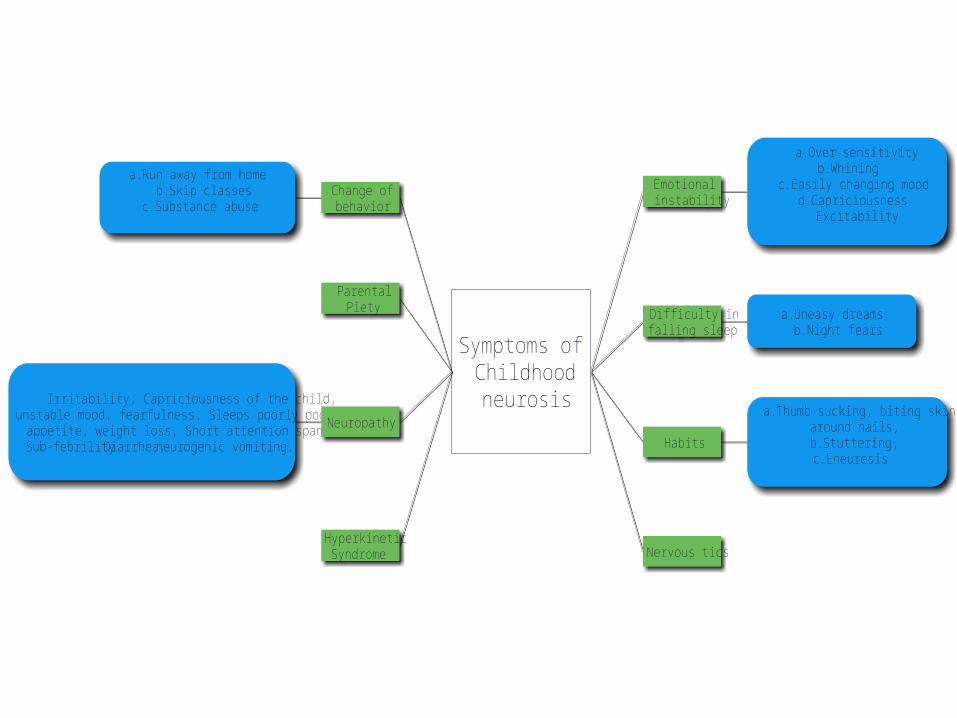
Nervous tics
a. Thumb sucking, biting skinaround nails,b. Stuttering,c. Eneuresis
Habits
a. Over-sensitivityb. Whining
c. Easily changing moodd. Capriciousness
Excitability
Emotionalinstability
a. Run away from homeb. Skip classes
c. Substance abuse
a. Uneasy dreamsb. Night fears
Difficulty infalling sleep
Symptoms ofChildhoodneurosis
HyperkineticSyndrome
Irritability, Capriciousness of the child,unstable mood, fearfulness. Sleeps poorly poor
appetite, weight loss, Short attention span,Sub-febrility Diarrhea, neurogenic vomiting.
Neuropathy
ParentalPiety
Change ofbehavior
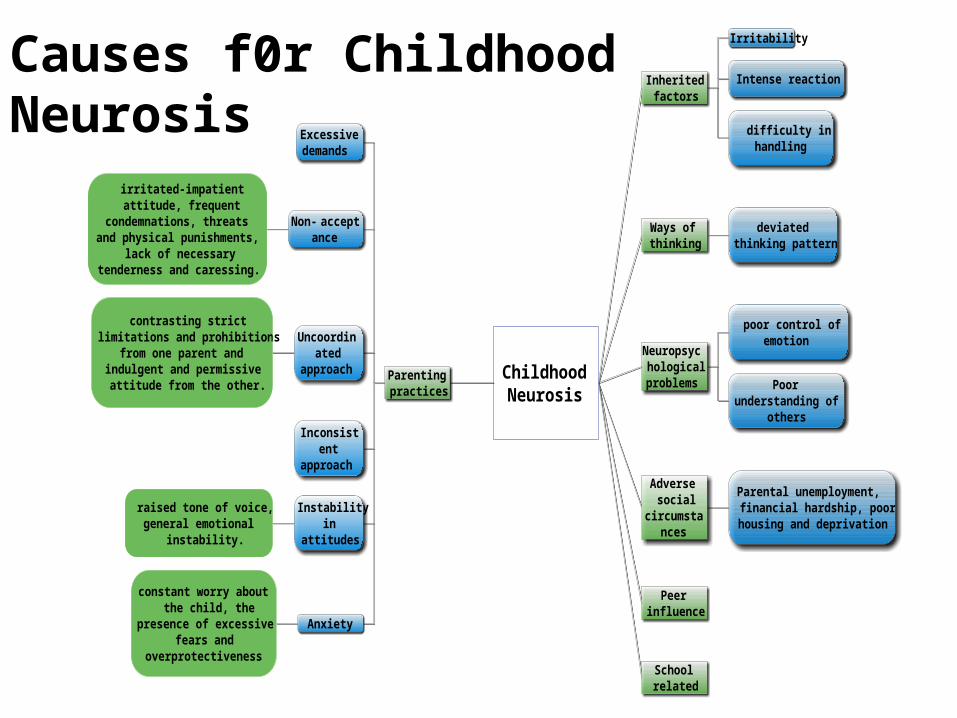
Causes f0r Childhood Neurosis
Ways ofthinking
Peerinfluence
Parental unemployment,financial hardship, poorhousing and deprivation
Adversesocial
circumstances
constant worry aboutthe child, the
presence of excessivefears and
overprotectiveness
Anxiety
raised tone of voice,general emotional
instability.
Instabilityin
attitudes
Inconsistent
approach
contrasting strictlimitations and prohibitions
from one parent andindulgent and permissiveattitude from the other.
Uncoordinated
approach
irritated-impatientattitude, frequent
condemnations, threatsand physical punishments,
lack of necessarytenderness and caressing.
Non-acceptance
Excessivedemands
Poorunderstanding of
others
poor control ofemotion
Neuropsychologicalproblems
difficulty inhandling
Intense reaction
Irritability
Inheritedfactors
Schoolrelated
ChildhoodNeurosis
Parentingpractices
deviatedthinking pattern
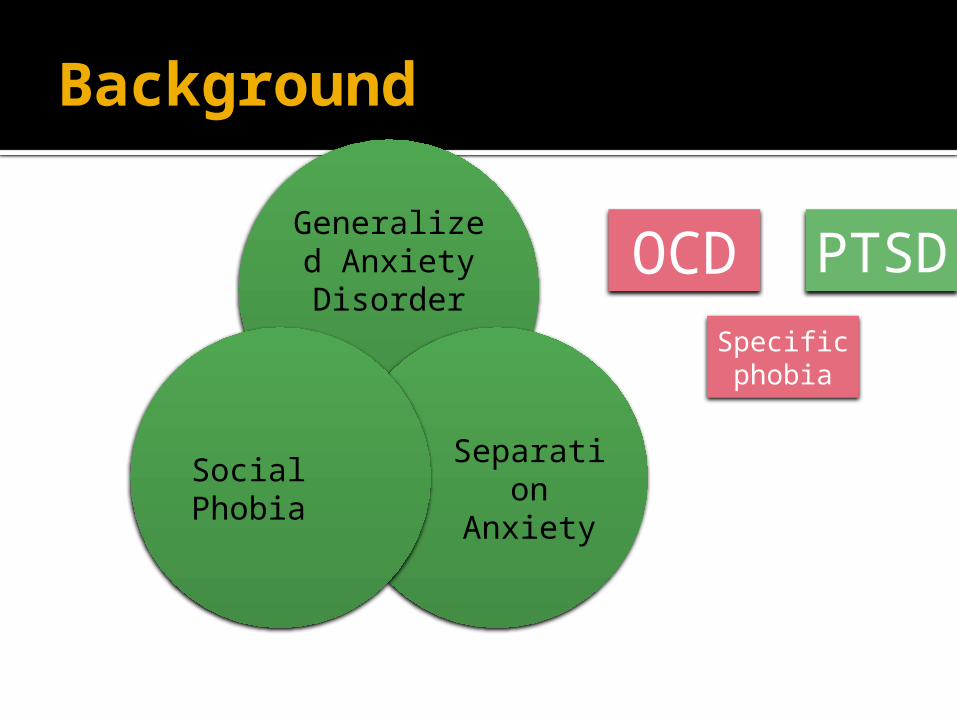
Background
Generalized AnxietyDisorder
Separation Anxiety
Social Phobia
OCD PTSD
Specific phobia
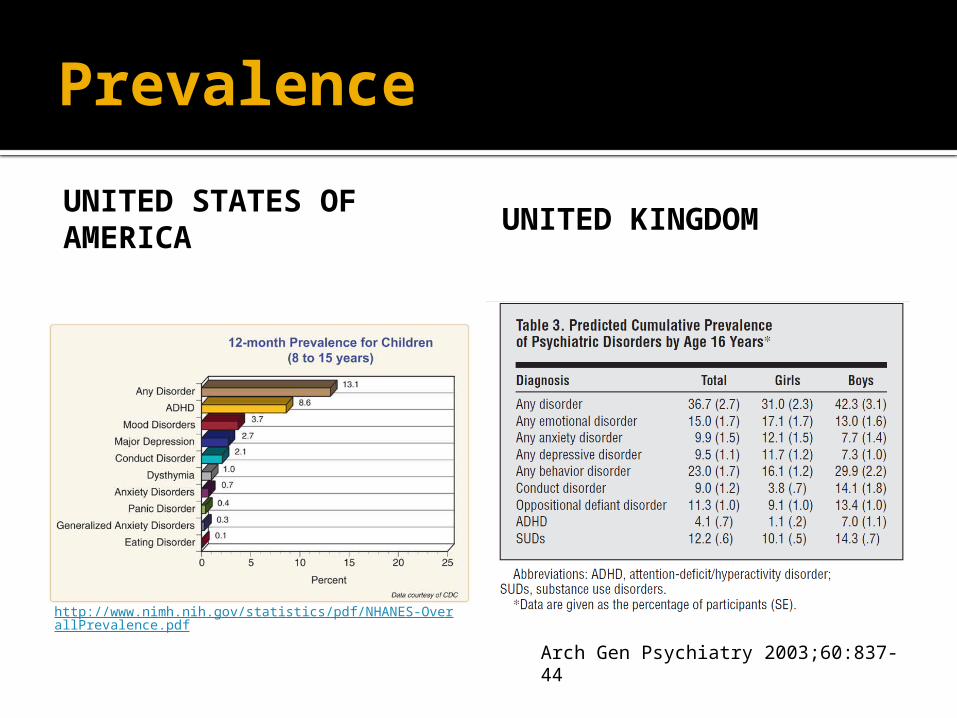
Prevalence
UNITED STATES OF AMERICA
UNITED KINGDOM
http://www.nimh.nih.gov/statistics/pdf/NHANES-OverallPrevalence.pdf
Arch Gen Psychiatry 2003;60:837-44
In India Prevalence of Childhood Neurosis
Nagaraja, 1966 - 9.7 % of out-patient ; 9.3% of inpatients
Manchanda et al. 1969 27.3% admitted for physical ailments
Raju et al, 1969. 3.71% were neurotics
Lal and Sethi, 1977 Neurotic disorders in 11.0%
Manchanda and Manchanda, 1978 1.1% among inpatients ; 8.2% in General OP
Indian J Psychiatry. 2010 January; 52(Suppl1): S210–S218.
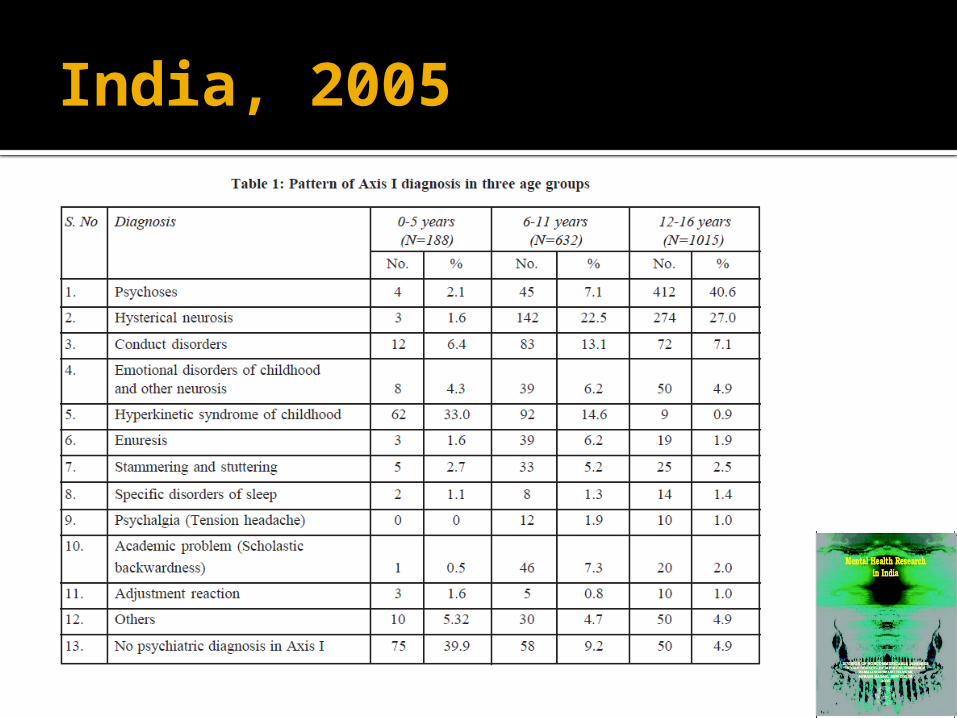
India, 2005
Disorders with neurotic features – ICD 10
F40 Phobic anxiety disorders F41 Other anxiety disorders F42 Obsessive-compulsive disorder F43 Reaction to severe stressF48 Other neurotic disordersF93 Childhood anxiety disorder
DSM- IV – TR 2000
Mood state characterized by strong negative
emotion and bodily symptoms of tension in
anticipation of future danger or misfortune
Most common in children
10-15% of kids - by teen years
Onset early in life
Under-recognized and under treated
Often quiet, “good” kids
Often lifelong chronic disorders
Anxiety Disorders
Why so common?
Protective role of anxiety
▪ Body’s warning system for danger
▪ Avoid separation from parents
▪ Be vigilant for predators/dangers
Mild anxiety enhances concentration,
performance
Anxiety disorders--too much of a good
thing
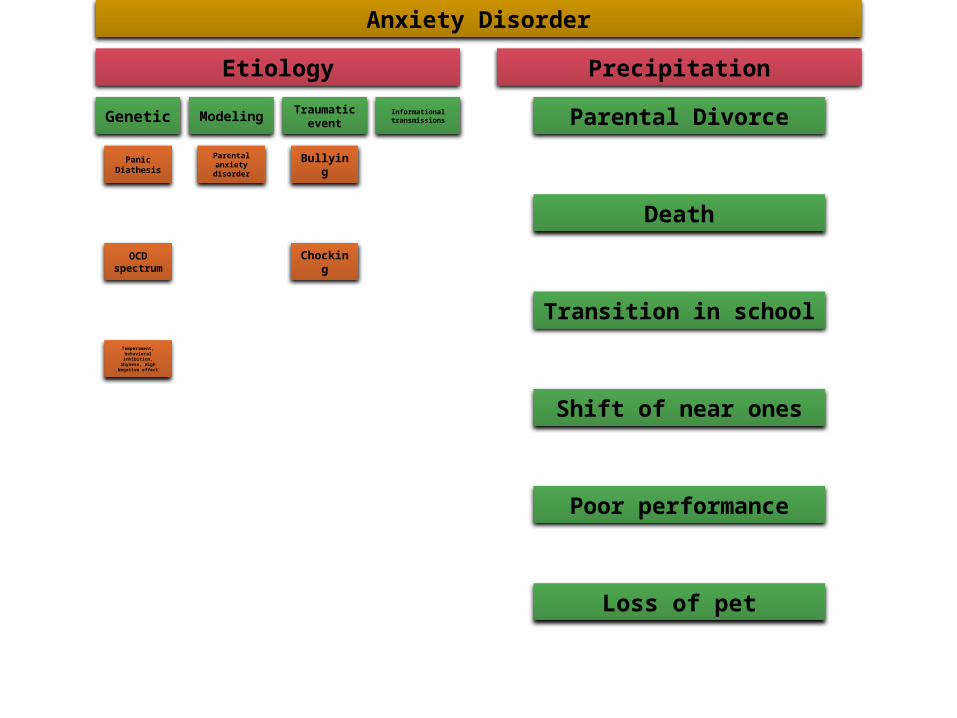
Anxiety Disorder
Etiology
Genetic
Panic Diathesis
OCD spectrum
Temperament, behavioral inhibition,
Shyness, High Negative effect
Modeling
Parental anxiety disorder
Traumatic event
Bullying
Chocking
Informational transmissions
Precipitation
Parental Divorce
Death
Transition in school
Shift of near ones
Poor performance
Loss of pet
Differential Diagnosis
Normal Anxiety-mild and manageable
Excessive Anxiety-atypical and persistent
Psychiatric:
Depression (vs. demoralization 2° anxiety)
Adjustment Disorder
Bipolar Disorder
Substance Use
Psychotic disorder
Differential Diagnosis
Physical:
thyroid disease
hyper/hypoglycemia
Anemia
substance induced
▪ Caffeine—energy drinks
▪ sympathomimetics-ventolin, allergy medication
Specific Anxiety Disorders
Separation Anxiety Disorder
Generalized Anxiety Disorder
Panic Disorder +/- Agoraphobia
Social Phobia
Specific Phobia
Post Traumatic Stress Disorder
Obsessive Compulsive Disorder
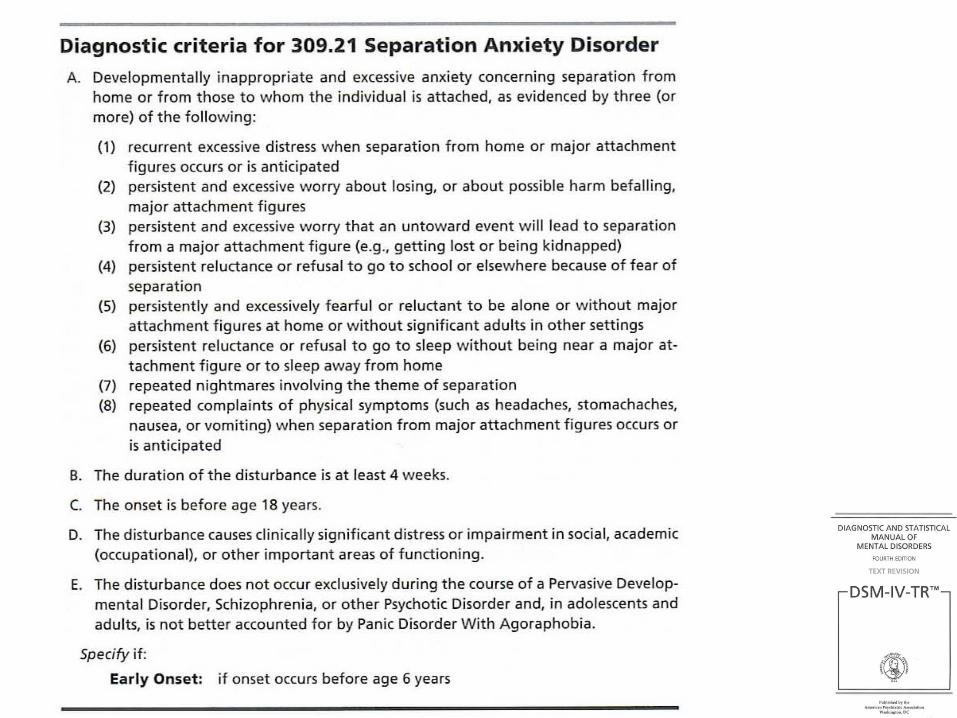
Separation Anxiety Disorder
Fears of separation from parent, school
refusal, difficulty sleeping alone, nightmares
Can’t be alone
Social, but friends must come to their house
Typical age of onset: school entry
SAD - Etiology
Unknown Genetic
Early temperamental
Family / Environm
ent
Treatment Principles
Consider age, severity, comorbidity,
impairment
Environmental management
Education about anxiety
Cognitive Behavioral Therapy
Medications
Mostly SSRI’s
Benzodiazepines in select situations
Environmental Management
Home: consistent routines and structure
Ensure adequate sleep
Healthy diet-small frequent meals often better
Exercise
Schedule time for homework and activities-avoid
overload
School involvement: accommodations, study block
for teens,
Address parental anxiety disorders
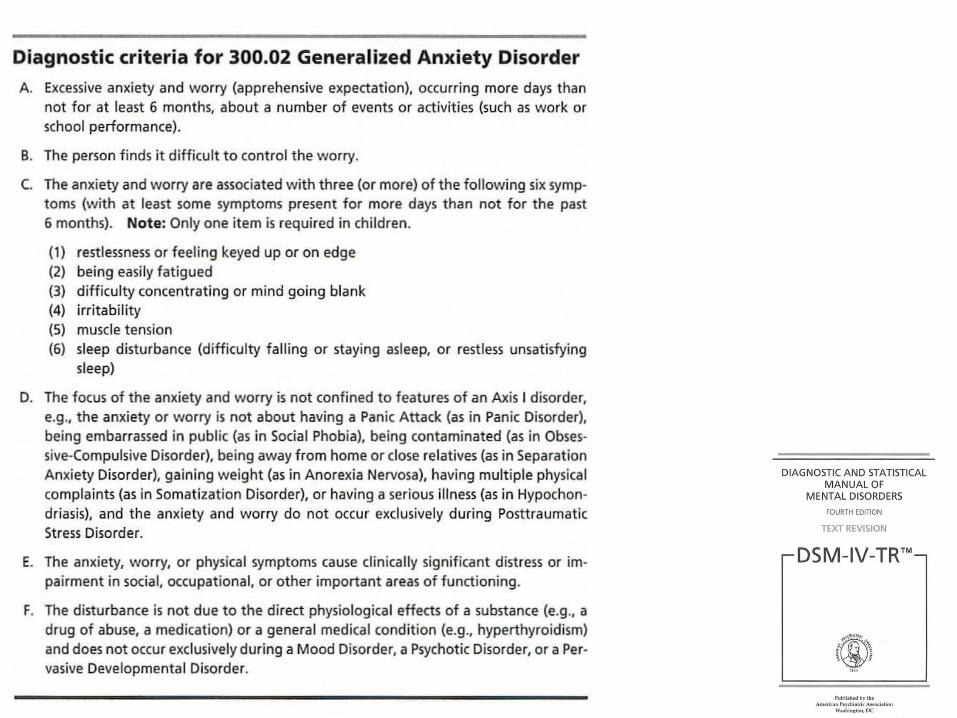
Generalized Anxiety Disorder
Excessive, uncontrollable worry for at least 6
months plus ≥ 1 other symptom:
sleep, fatigue, restlessness, irritability, muscle tension,
difficulty concentrating
Overlaps with anxious temperament:
perfectionistic “worry warts”
worry about school work, health issues, friends….
Commonly starts in intermediate years of
elementary
Medications
When to consider?
Severity: ++functional impairment
Acuity/Urgency
▪ ↓↓sleep, ↓↓eating
Failure to improve despite CBT
Patient preference
Medications
What to use? SSRI’s: mainstay of treatment▪ Fluoxetine , fluvoxamine ▪ Sertraline , Citalopram
Benzodiazepines:▪ Ativan, clonazepam
Other▪ Buspirone-very little evidence it is helpful▪ Low dose atypical neuroleptics-augmentation
of SSRI’s with OCD
Panic Disorder
Fear: present-oriented emotional reaction to current danger, characterized by strong escape tendencies and surge in sympathetic nervous system
Panic: Group of physical symptoms of fight/flight response that unexpectedly occur in the absence of obvious danger or threat
Panic Disorder
Panic attack: sudden,
overwhelming period of intense
fear or discomfort
accompanied by characteristics of
the fight/flight response
Agoraphobia : Anxiety about having a panic
attack in situations where
escape might prove difficult or
embarrassing
Panic disorder: recurrent
unexpected panic attacks followed by at
least one month of persistent
concern about having another attack, constant worry about the
consequences, or a significant change in
behavior related to the attacks.
Panic Disorder
• ↑Noripinephrine activity in Locus Coeruleus
• Altered Serotonin levels
Biological
• Interoceptive Conditioning ModelBehavioral Model
• Hypersensitivity to bodily sensations• Dire Thought with Catastrophizing• Thought fuels increase in bodily
response• Vicious out-of-control cycle
Cognitive Model
Panic Attack
Happens less often with younger children
Feel very scared
Heart pounding, hard to breathe, Feel shaky,
dizzy, or sick or going crazy or bad intuition
Sometimes they avoid school or want to
stay in the house
Avoids going to school – A part of
Agrophobia
F40 - Phobic anxiety disordersF40 Phobic anxiety disorders F40.0 Agoraphobia F40.1 Social phobias F40.2 Specific (isolated) phobias F40.8 Other phobic anxiety disorders F40.9 Phobic anxiety disorder,
unspecified
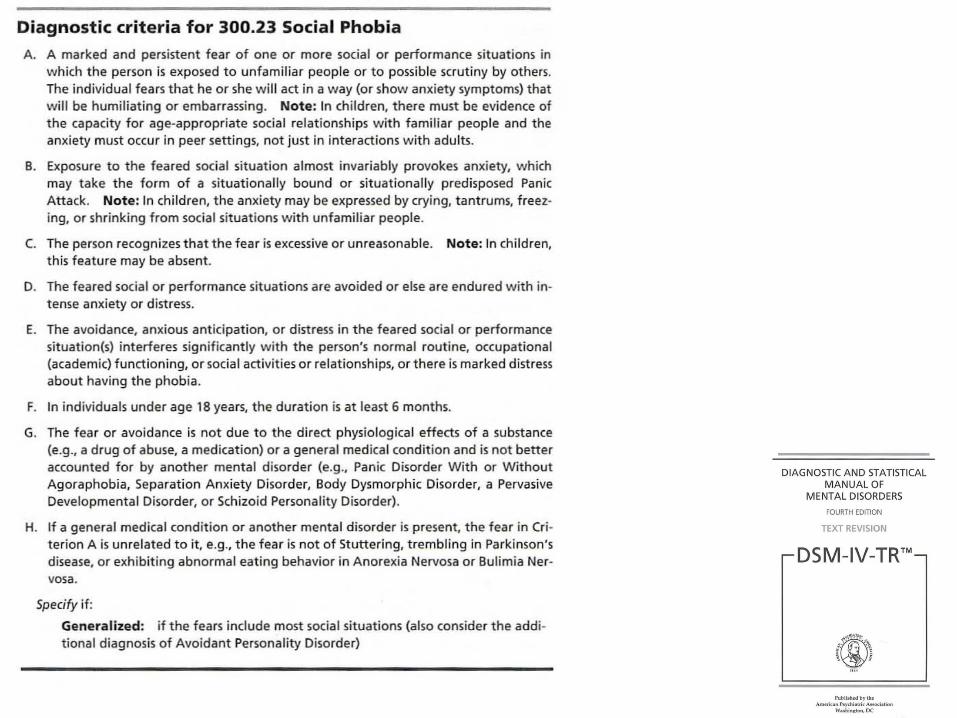
Diagnostic features of Phobias
1. Intense, persistent, irrational fear a particular
object, event or situation.
2. Response is disproportionate and leads to
avoidance of phobic object, event or situation.
3. Fear is serve enough to interfere with
everyday life. Condition may or may not be accompanied by PANIC ATTACKS
Types of Phobias
SPECIFIC PHOBIAS, of animals, events (flying), bodily (blood), situations (enclosed places).
SOCIAL PHOBIAS, of social situations, public speaking, parties, meeting new people.
AGORAPHOBIA, of public crowded places (not open spaces), of leaving safety of home
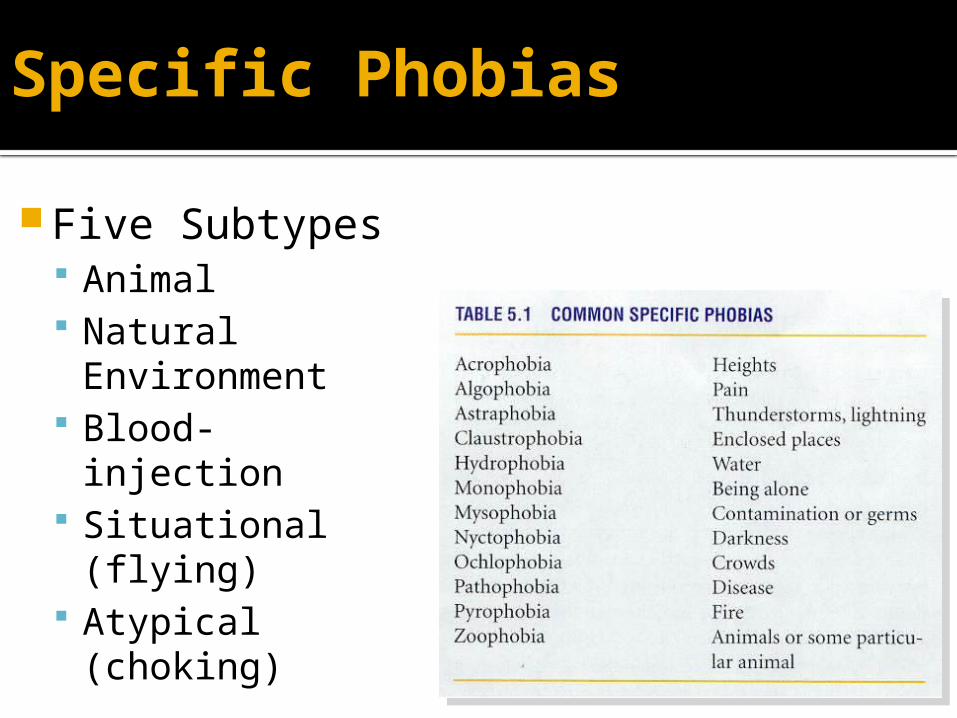
Specific Phobias
Five Subtypes Animal Natural
Environment Blood-injection Situational
(flying) Atypical
(choking)
Explanation
Biological
Evolution Theory
Genetics Theory
Vulnerability theory
Social Anxiety/Social Phobia
Happens more in teens than in young children
Fear and worry about social situations
Going to school
Speaking in class
Social events including recess and lunch
Shy, self-conscious
Easily embarrassed
These kids tend to be sensitive to criticism and
find it hard to be assertive
Treatment
CBT
SSRIs
Definition
Obsessions – persistent, recurring, unwanted cognitions, usually unrealistic or irrational. eg – contamination by germs
Compulsions – repetitive, ritualistic behaviours that reduce the anxiety associated with the obsessive thoughts. eg: repetitive hand washing / cleaning
Obsessive-Compulsive Disorder
Obsessions &/or Compulsions x 1hr/day
Rituals can get very elaborate and family’s
can get involved
Mild OC symptoms are very common
peak in early adolescents-19%
most resolve spontaneously
OCD ExplanationExplanation Behavioral
Two process theory of MowrerClassical Conditioning
Operant Conditioning
Cognitive BiasHyper-vigilance
Catastrophic Misinterpretation
Memory Problems
Psychodynamic Fixation – Anal stageUnconscious Conflict
Reaction formation
Obsessive-Compulsive Disorder In early childhood or adolescence.
Have frequent uncontrollable thoughts (obsessions)
They don’t like these thoughts, or do not care
Perform certain behaviors or rituals to try and prevent something bad from happening (or to get rid of thoughts)
Examples are: handwashing a lot if there is a fear of germs; checking that doors are locked; special touching rituals
Neurobiology of OCD
PET scans demonstrate hypermetabolism of
orbital frontal cortex and caudate nucleus;
normalizes with response to treatment
Structural and functional MRI scans
demonstrate abnormalities of cortical/basal
ganglia function (subtle abnormalities only)
Neuropsychological deficits, particularly in
executive functioningFrom: Rapoport & Wise
Pediatric
Autoimmune
Neuropsychiatric
Disorders
Associated with
Streptococcal infections
Treatment
CBT
Clompranine
SRI
SSRI
Post Traumatic Stress Disorder
Symptoms start after a physical or emotional trauma or very frightening event
Can be marked by several of Behavioral changes Repetitive play Zoning out, numbing of feelings Jumpiness and watchfulness of surroundings Nightmares and sleep problems “Flashbacks”
Not very common in young children
Acute Stress Reaction
A transient disorder of significant severity
In an individual without any previous mental
disorder
In response to exceptional physical and/or
psychological stress.
Acute Stress Reaction
SYMPTOMS
Initial state of „daze” Constriction of the field
of consciousness Narrowing of attention, Inability to comprehend
stimuli Disorientation Withdrawal from the
surrounding situation Agitation and
overactivity.
AUTONOMIC SIGNS
Tachycardia sweating or flushing Appear within minutes
of the impact Disappear within
several hours, maximally 2—3 d
Post-traumatic Stress Disorder (PTSD)
A delayed and/or protracted response to a stressful event
of an exceptionally threatening or catastrophic nature.
The three major elements of PTSD include
1)Re-experiencing the trauma through dreams or recurrent
and intrusive thoughts (“flashbacks”)
2)showing emotional numbing such as feeling detached
from others
3)Having symptoms of autonomic hyperarousal such as
irritability and exaggerated startle response, insomnia
PTSD
Fear/avoidance of cues - original trauma.
Excessive use of alcohol and drugs may
be a complicating factor.
The lifetime prevalence is estimated at
about 0.5% in men and 1.2% in women.
TREATMENT
Psychotherapeutic CBT
Psychodynamic therapy Attachment based therapy
Psychopharmacology
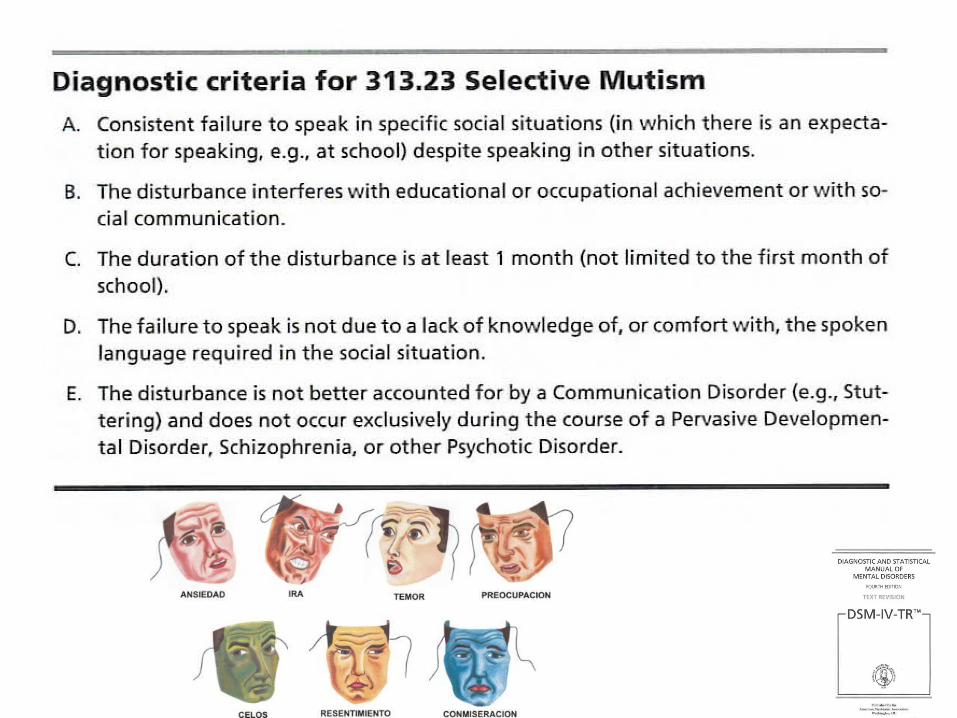
Selective Mutism
May not talk to anyone who is not close to them
They may look down, withdraw, turn red if
required to talk
Often they whisper if they do speak in a
situation
Up to 2% of school age children
Some kids outgrow it
Pharmocotherapy
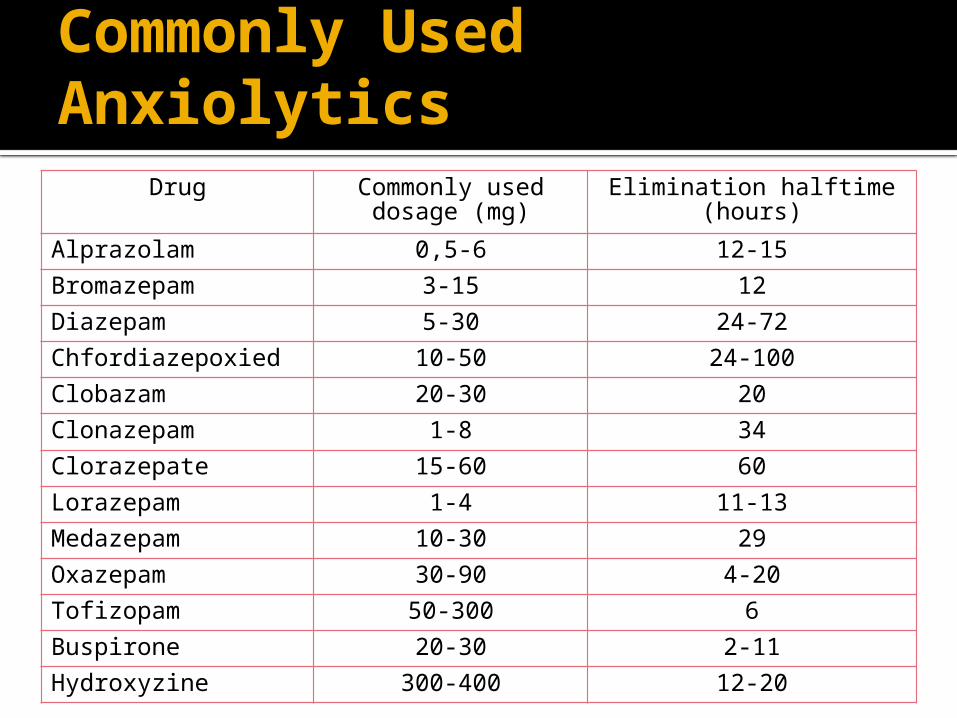
Commonly Used Anxiolytics
Drug Commonly used dosage (mg)
Elimination halftime (hours)
Alprazolam 0,5-6 12-15
Bromazepam 3-15 12
Diazepam 5-30 24-72
Chfordiazepoxied 10-50 24-100
Clobazam 20-30 20
Clonazepam 1-8 34
Clorazepate 15-60 60
Lorazepam 1-4 11-13
Medazepam 10-30 29
Oxazepam 30-90 4-20
Tofizopam 50-300 6
Buspirone 20-30 2-11
Hydroxyzine 300-400 12-20
Evidence for therapies – AHCPRAgency of Health Care Policy and Research
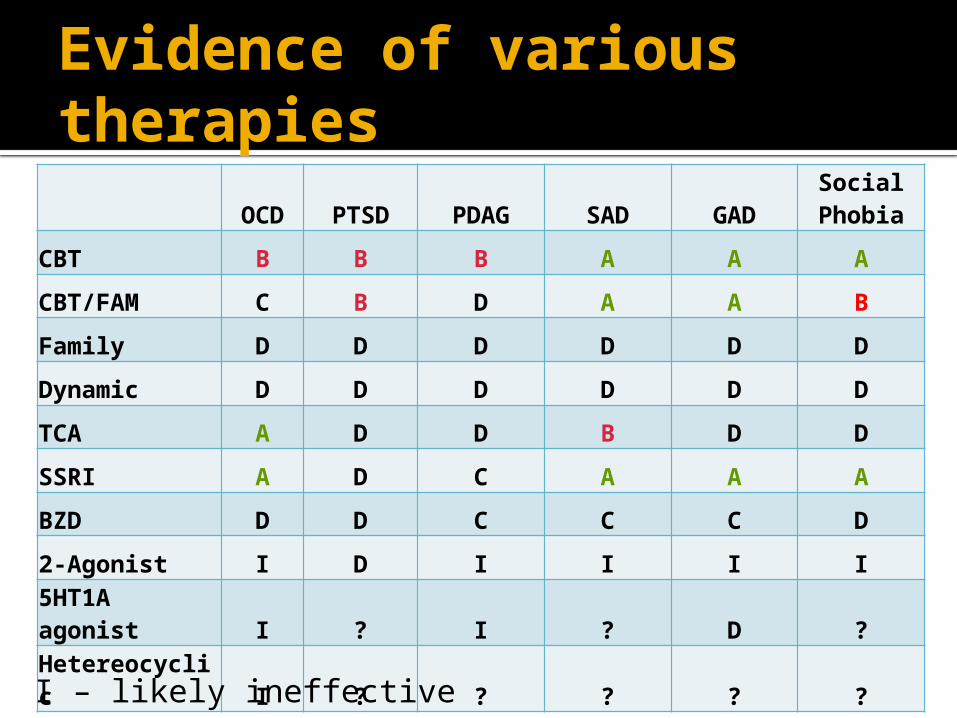
Evidence of various therapies
OCD PTSD PDAG SAD GADSocial Phobia
CBT B B B A A A
CBT/FAM C B D A A B
Family D D D D D D
Dynamic D D D D D D
TCA A D D B D D
SSRI A D C A A A
BZD D D C C C D
2-Agonist I D I I I I5HT1A agonist I ? I ? D ?Hetereocyclic I ? ? ? ? ?
I – likely ineffective
References March RS. Diagnosis and treatment of the childhood-onset
anxiety disorders. Anxiety Disorders Association of America, 2008.
Piacentini J, Roblek T. Recognizing and childhood anxiety disorders. West J Med 2002;176:149-51.
Keeton CP, KolosAC, Walkup JT. Pediatric generalized anxiety disorder: epidemiology, diagnosis and management. Paedr Drugs 2009; 11:171-83.
Cox GR, Fisher CA, De Silva S, Phelan M, Akinwale OP, Simmons MB, Hetrick SE. Interventions for preventing relapse and recurrence of a depressive disorder in children and adolescents. Cochrane Database of Systematic Reviews 2012;11: CD007504. DOI: 10.1002/14651858.CD007504
James AACJ, Soler A, Weatherall RRW. Cognitive behavioural therapy for anxiety disorders in children and adolescents.Cochrane Database of Systematic Reviews 2005, Issue 4. Art. No.: CD004690. DOI: 10.1002/14651858.CD004690.pub2
Ipser JC, Stein DJ, Hawkridge S, Hoppe L. Pharmacotherapy for anxiety disorders in children and adolescents. Cochrane Database of Systematic Reviews 2009, Issue 3. Art. No.: CD005170. DOI: 10.1002/14651858.CD005170.pub2.
Scott S. Classification of psychiatric disorders in childhood and adolescence: building castles in the sand? Advances in Psychiatric treatment 2002;8:205–213.
Greenberg MT, Domitrovich C, Bumbarger B. The Prevention of Mental Disorders in School-Aged Children: Current State of the Field. Prevention and Treatment 2001;4: Article 1
Kessler RC, Amminger GP, Aguilar-Gaxiola S, Alonso J, Lee S, Ustun TB. Age of onset of mental disorders: A review of recent literature. Curr Opin Psychiatry. 2007 July ; 20(4): 359–364.
Costello EJ, Mustillo S, Erkanli A, Keeler G, Angold A. Prevalence and development of psyhciatric disorders in childhood and adolescence. Arch Gen Psychiatry 2003;60:837-44.
Krauss H, Buraczyńska-Andrzejewska B, Piątek J, Sosnowski P, Mikrut K, Głowacki M, Misterska E, Żukiewicz-Sobczak W, Zwoliński J. Occurrence of neurotic and anxiety disorders in rural schoolchildren and the role of physical exercise as a method to support their treatment. Ann Agric nviron Med. 2012; 19(3): 351-356.
Rachford BK. NEUROTIC DISORDERS Of CHILDHOOD INCLUDING A STUDY Of AUTO And INTESTINAL INTOXICATIONS, CHRONIC ANAEMIA, FEVER, ECLAMPSIA, EPILEPSY,MIGRAINE, CHOREA, HYSTERIA,ASTHMA,ETC. New York, EB treat and company, 1905
DSM-IV – TR, 2000 Sadock. Comprehensive textbook of Psychiatry. Oxford Textbook of Psychiatry. Infographics and Photographs: Google images Infographics and Photographs: Google images Anxiety disorders in childhood. Moories TL, Mark SJ. , 2nd edition Rutters. Child and adolescent psychiatry, 5th Edition Clinical child psychiatry. William A Klykylo, Jerald Kay
THANK YOU
Recommended