Embed Size (px)
Citation preview

Depression and anxiety
in childhood
Dr Brendan Belsham
Child and adolescent psychiatrist
www.drbelsham.com

Lund
beck
Janssen Novartis Lilly Cipla Adcock Mylan
Speakers
honoraria xx
Conferences x x x x x x
Advisory
boardsx x x
Disclosures
Pharma
plan

What is abnormal? Normal temperament
Cultural thresholds for abnormality
Normal reactions to stressful environments The home
The school
Adjustment disorder The development of emotional or behavioural symptoms (including
inattentiveness and hyperactivity) occurring within 3 months of a stressor
once the stressor has terminated, the symptoms do not persist for more than an additional 6 months
Abnormal reactions to stressors: PTSD
Various disorders

Normal temperament
Behaviours or traits appearing in the first year of life, which are
stable across time and across situations
They are innate, inborn, genetic
These traits are normal!

Dimensions of temperament
1. Mood
The prevailing mood of the child
2. Approach-withdrawel
The child’s characteristic response to a new situation or strangers
3. Adaptability
How the child copes with transitions and changes
4. Intensity
The energy level of a response, whether positive or negative
5. Persistence Continuing with activities in the face of obstacles
Thomas and Chess, 1963

Attachment
The close emotional bonds of affection that develop between
infants and primary caregivers (mothers)
A biological phenomenon
Occurs in a critical window period, 18-24 months
Securely attached children have:
Increased attention spans (Maslin-Cole and Spieker, 1990)
Greater persistence in problem-solving (Matas et al, 1978)
Better delay of gratification (Olsen et al, 1990)
Better social interactions (Lyons-Ruth et al, 1993)
Less chance of later anxiety disorders, depression

Healthy attachment:
Requires a mother who is
Consistently present
Attuned to the infant’s needs for eye contact,
focused attention, physical affection, stimulation
Cannot occur if the mother is
Unavailable
Erratic
Unpredictable
(NB post-natal depression)

Types of disorders: Categorical
NormalDisorder

Level of impairment
normal disorder
Types of disorders: Dimensional
Number and intensity of symptoms
Zone of ambiguity

So when is it a disorder?
Developmental appropriateness
Situational appropriateness
Symptom count
Chronicity of symptoms
Number of settings in which the symptoms occur
Family history of mental illness
Functional impairment

Anxiety levels
Level of functioning

Prevalence of anxiety disorders
■ 15-20% of youth have an anxiety disorder
■ The most frequent psychiatric disorders in children and adolescents
■ majority of anxiety disorders have their onset in childhood and
adolescence
■ …earliest of all forms of psychopathology
■ Less than one-fifth of affected youth ever receive treatment
■ Overall girls>boys, by adolescence, 2-3:1

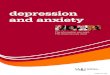
Aetiology of anxiety disorders
Genetic vulnerability
Environment
Gene-environment interactions

Gene
expression
Environment
DNA methylation
Inherited
genome
CLINICAL
DISORDER

Features common to anxiety disorders
Avoidance behavior
Frequent midline physical complaints:
headaches, tummy aches, nausea, butterflies
Catastrophic thinking
Impaired functioning:
Classroom performance
Social interactions
Sporting performance
Sleep disturbance
Subjective distress

Anxiety Disorders of Childhood
■ Generalised Anxiety Disorder
■ Separation Anxiety Disorder
■ Social anxiety disorder (social phobia)
■ Selective mutism
■ Panic Disorder
■ Agoraphobia
■ Specific phobia
■ Obsessive Compulsive Disorder
■ PTSD
‘paediatric anxiety
disorder triad’

Post Traumatic Stress Disorder
■ Exposure to an event involving real or threatened death, serious injury or sexual violence, associated with:
1) Re-experiencing phenomena:
■ Memories, nightmares, flashbacks, severe physical reactions
2) Avoidance symptoms
3) Negative cognitions and mood
4) Changes in arousal or reactivity
■ exaggerated startle response
■ hyperactivity
■ inattentiveness

Post Traumatic Stress Disorder
■ DSM 5 introduces new developmental subtype:
■ PTSD in preschool children:
■ Makes allowance for:
■ Type of trauma (dog bites, invasive medical procedures)
■ Observed affect with intrusion symptoms
■ Avoidance symptoms: constricted play
■ Arousal symptoms: extreme temper tantrums

■ Risk of PTSD in those with ADHD 4x greater
than controls
■ ADHD associated with fear circuitry
abnormalities which may predispose to ADHD (ventromedial prefrontal cortex, hippocampus)
■ Faulty processing of the trauma?

Conditions commonly comorbid with anxiety
■ Another anxiety disorder
■ Learning disorder
■ Depression
■ ADHD
■ 23-33% of children with ADHD have an anxiety disorder

The school refusing child
One of the few emergencies in child psychiatry
Possible causes
Depression
Anxiety Disorders
Separation Anxiety D
Social Anxiety D
OCD
Bullying
Undiagnosed learning disorder

Screening for anxiety disorders
May present with:
Frequent need for reassurance
Unable to work independently
Avoidance behaviour
Frequent absenteeism
Underachieving child
Sometimes difficult, oppositional behaviour
Teachers and parents need to have a high index of suspicion
Talk to the child
Use developmentally appropriate language


Parent or teacher concerned
Speak to parent
monitor
Refer psychologist
Refer child/adolescent
psychiatrist (or adult
psychiatrist if >13)resolution

Treatment of childhood anxiety disorders
Early intervention is crucial
Psychoeducation
Addressing the environment Return to school is a priority
Alternative school placement?
Addressing family issues Parental psychopathology
Abuse
Cognitive behavioural therapy
Psychodynamic (play therapy)
Mindfulness therapies
Family-based interventions
Medication

Medication for childhood anxiety disorders
Usually once less invasive strategies have been attempted and failed
Selective serotonin uptake inhibitors (SSRI’s) are first line
May require augmentation, eg risperidone (Risperdal):
But associated with hormonal side-effects (increased prolactin)
Also with long-term side-effects (tardive dyskinesia)
Tricylic antidepressants (eg imipramine, Tofranil)

Medication for childhood anxiety disorders
Selective serotonin uptake inhibitors (SSRI)
Fluoxetine (Prozac, Lorien, Nuzak)
Fluvoxamine (Luvox)
Paroxetine (Aropax)
Sertraline (Zoloft, Sertra)
Citalopram (Cipramil, Cilift)
Escitalopram (Cipralex, Lexamil)
Little evidence for one over the other in various anxiety disorders

Course of anxiety disorders
May remit but mostly chronic
Early onset anxiety disorders (<13 years of age) have a tendency to
follow a chronic course, and to have a more disabling and severe
character
Increased risk of later:
Depression
Substance abuse
Suicide attempts
Poorer long term functioning:
physical health, interpersonal, educational, financial

Childhood depression
Prevalence
2% of children
4-8% of adolescents
5-10% of children and adolescents have subsyndromal depression
Gender ratio
1:1 in childhood
1:2 in adolescence

In the prevalence of depression increasing?
Yes:
Each successive generation after 1940 is at greater risk of
depression, with onset at younger age, than the previous
generation
Why??

Why do children get depressed?
Genetic risk
Adoption studies, Twin studies
The single most predictive factor
Environmental stressors affect onset and recurrences:
Losses
Neglect
Abuse
Ongoing conflict and frustration
But the effect of these stressors depends on the child’s attributional style
Interaction between genetic and environmental factors

Why do children get depressed?
Comorbid conditions
Anxiety disorders
Persistent depressive disorder
ADHD
Substance abuse
Medical illness
Diabetes

The South African context
Violence
Poverty
Migrant labour
HIV epidemic
Child-headed homes
Inadequate education
Good Childhood Survey
South Africa ranked 13th out of 15


DSM5 Major Depressive Disorder (MDD) Depressed or irritable mood; AND
Reduced interest or enjoyment of activities; plus 4 or more of : Diminished ability to think or concentrate
Markedly reduced energy levels
Insomnia or excessive sleeping
Decreased or increased appetite, or excessive weight gain or weight loss (or failure to achieve expected weight gain)
Psychomotor agitation or psychomotor slowing
Feelings of guilt or excessive worthlessness
Recurrent thought of death, suicidal thinking or suicidal behaviour
These symptoms must persist for 2 weeks or more
and cause significant functional impairment

Important differences from adult depression
Mood may be depressed or irritable
May display behavioural symptoms rather than verbalizing sadness
Low frustration tolerance
Tantrums
Social withdrawal
Less appetite and sleep disturbance

Other common symptoms of childhood
depression
School refusal, or frequent absenteeism from
school
Academic underachievement
Frequent physical complaints
Frequent complaints of boredom
Reckless behaviour (‘masked depression’) in
adolescents

Dysthymic disorder
Now known as Persistent Depressive Disorder
Consists of a persistent, long-term change in mood (depressed
mood or irritability for >1 year)
Less intense but more chronic than major depressive disorder
As impairing or more impairing than MDD
Often overlooked

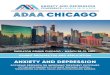
Internalising and externalising disorders
EXTERNALISING INTERNALISING
•ADHD
•Oppositional
defiant d.
•Anxiety disorders
•Depression


Depression: differential diagnosis
Persistent depressive disorder
Anxiety
ADHD
Oppositional Defiant Disorder
Substance abuse
Medical disorders
Bereavement
Adjustment disorder

Psychotic depression
Presence of hallucinations
May include command hallucinations (suicide)
Less commonly delusions
Associated with:
family history bipolar disorder
More severe depression
Resistance to antidepressants
Increased risk of bipolar dis

Prognosis
20-60% probability of recurrence within 1-2 years after remission
70% recur after 5 years
Higher risk for suicide
Higher risk for substance abuse
20-40% will develop bipolar disorder, especially if:
Family loading for bipolar
Psychotic depression
Pharmacologically - induced manic symptoms

Childhood Bipolar Disorder
Recurrent episodes of depression and
MANIA:
Grandiosity
Less need for sleep
Flight of ideas/ racing thoughts
Excessive involvement in pleasurable activities

Level of impairment normal disorder
What about sub-syndromal conditions?
Number and intensity of symptoms
x
Significant impairment
High genetic loading
Increased risk for MDD
Increased risk for suicide

Suicidal children
60% of depressed youth think about suicide, 30% will make
suicide attempt
Suicide in South African children aged 10-14 has more than
doubled in the past 15 years
Completed suicide very rare in preteens

Risk factors for youth suicide
Previous suicide attempts (especially multiple attempts)
Comorbid psychiatric disorders
Anxiety disorder is a risk factor for suicide even in the absence of
depression
Impulsivity and aggression
Availability of lethal agents
Exposure to negative events
Family history of suicide

Cutting
Genuine attempt?
Depression, other mood disorder
Relief from emotional pain?
Endorphin release
“I just want to feel something”
Personality disorder (Borderline)
Copy-cat?

Treatment of childhood depression
Admission?
Psychoeducation
Supportive management
Family involvement
School involvement
Individual psychotherapy

Medication in childhood depression
High placebo response rate (30-60%; eg tricyclic antidepressants
have not been shown to be superior to placebo)
SSRI’s the gold-standard:
Fluoxetine (Prozac) FDA approved
Recent controversy around induction of suicidality
Atypical antipsychotics (eg risperidone):
For psychotic depression
As an augmentation strategy
Treat comorbid conditions

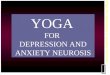
receptor
Serotonin
SERT
the serotonergic synapse
Direction of transmission

Side-effects of SSRI’s GIT
Nausea, vomiting
Diarrhoea
Stomach cramps
Headaches
Tiredness
Sleep disturbance
Appetite disturbance, weight gain
Behavioural activation (may only emerge 3 months after treatment) Disinhibition, Defiance, Impulsivity, Insomnia
Mania
Treatment-emergent suicidality

Monitoring medication
Requires good communication between:
Home (both homes where relevant)
School
Doctor
Other professionals
Monitor clinical response
Duration of treatment

Take-home messages
Anxiety and depression are common in childhood
… especially in South Africa
Often unrecognized
… especially in South Africa
A source of significant morbidity
Effective treatments are available