
Introduction to Antineoplastic Introduction to Antineoplastic PrescribingPrescribing
Robert Bradbury, R.Ph., BCPSRobert Bradbury, R.Ph., BCPSClinical CoordinatorClinical Coordinator
H. Lee Moffitt Cancer CenterH. Lee Moffitt Cancer Center

ObjectivesObjectives
• Meet the following goals concerning antineoplastic prescribing:
– Understand the basis for chemotherapy.
– Be able to identify appropriate dosage ranges.
– Be able to identify major toxicities.
– Learn the skill of prescribing chemotherapy.
• Meet the following goals concerning antineoplastic prescribing:
– Understand the basis for chemotherapy.
– Be able to identify appropriate dosage ranges.
– Be able to identify major toxicities.
– Learn the skill of prescribing chemotherapy.

OverviewOverview
• Cell Cycle Kinetics
• Pharmacologic Classification of Antineoplastic Agents
• Review of Agents
• Review of Combination Therapy
• Cell Cycle Kinetics
• Pharmacologic Classification of Antineoplastic Agents
• Review of Agents
• Review of Combination Therapy

The Cell Cycle The Cell Cycle
G0Resting Phase
SG1
G2
M
Mitosis (Cell Division)
DNA Synthesis
PremitoticPhaseRNA Synthesis
Cell Death
Cell Maturation

Therapy ConceptsTherapy Concepts
• Phase Specific drugs – work only on a specific phase of cell growth– most effective in rapidly growing cells
• Phase Non-Specific drugs – work on more than one phase of cell growth– most effective in rapidly growing cells
• Phase Specific drugs – work only on a specific phase of cell growth– most effective in rapidly growing cells
• Phase Non-Specific drugs – work on more than one phase of cell growth– most effective in rapidly growing cells

Therapy ConceptsTherapy Concepts
• Chemotherapy Terminology
– Induction- drug therapy used as primary treatment (leukemia)
– Consolidation - drug therapy used as follow up after remission from induction (leukemia)
– Adjuvant- drug therapy after surgery or XRT
– Neo-adjuvant - drug therapy before surgery or XRT which is not adequate alone.
– Salvage - drug therapy when primary drug treatment after relapse.
• Chemotherapy Terminology
– Induction- drug therapy used as primary treatment (leukemia)
– Consolidation - drug therapy used as follow up after remission from induction (leukemia)
– Adjuvant- drug therapy after surgery or XRT
– Neo-adjuvant - drug therapy before surgery or XRT which is not adequate alone.
– Salvage - drug therapy when primary drug treatment after relapse.

Therapy ConceptsTherapy Concepts
• Chemotherapy Terminology (cont)
– Regional - drug therapy localized to a specific area (e.g. limb perfusion, intrathecal, intraperitoneal)
– Maintenance - drug therapy used to maintain stable disease or remission.
– High Dose - doses above the standard range used primarily in combo with bone marrow rescue. Assumption that dose-intensity is effective.
– Palliation - drug therapy given to reduce symptoms without an intent to cure disease.
• Chemotherapy Terminology (cont)
– Regional - drug therapy localized to a specific area (e.g. limb perfusion, intrathecal, intraperitoneal)
– Maintenance - drug therapy used to maintain stable disease or remission.
– High Dose - doses above the standard range used primarily in combo with bone marrow rescue. Assumption that dose-intensity is effective.
– Palliation - drug therapy given to reduce symptoms without an intent to cure disease.

Therapy ConceptsTherapy Concepts
• Response Criteria
– Complete Response - Complete disappearance of signs and symptoms for at least 1 month.
– Partial Response - >50% reduction of tumor mass of all measured lesions and no new lesions.
– Stable Disease - No significant change in tumor mass neither increasing or decreasing by 25%.
– Progressive Disease- More than 25% increase in tumor mass
• Response Criteria
– Complete Response - Complete disappearance of signs and symptoms for at least 1 month.
– Partial Response - >50% reduction of tumor mass of all measured lesions and no new lesions.
– Stable Disease - No significant change in tumor mass neither increasing or decreasing by 25%.
– Progressive Disease- More than 25% increase in tumor mass

Therapy ConceptsTherapy Concepts
• Gompertzian Model of Tumor Growth
– Growth rate of tumor cells decreases with time
– Response to chemotherapy is during rapid growth phase.
• Gompertzian Model of Tumor Growth
– Growth rate of tumor cells decreases with time
– Response to chemotherapy is during rapid growth phase.
Time
Rapid rate of tumor growth
Plateau

Therapy ConceptsTherapy Concepts
• Goldie-Coldman Hypothesis
– A fraction of tumor cells will develop resistance after treatment.
– This clone will continue to grow even though the patient appears to respond.
– Alternating combinations of chemotherapy agents early in treatment is necessary to prevent development resistant clones.
• Goldie-Coldman Hypothesis
– A fraction of tumor cells will develop resistance after treatment.
– This clone will continue to grow even though the patient appears to respond.
– Alternating combinations of chemotherapy agents early in treatment is necessary to prevent development resistant clones.

Therapy ConceptsTherapy Concepts
• Worst-Drug Rule - Day
– Drug A works better than drug B against a tumor.
– Use Drug B first to shrink tumor.
– Use Drug A sequentially to overcome resistance.
– Assumes all tumors of resistant clones.
– Some tumors respond best to sequential therapy allowing for sparing of toxicity.
• Worst-Drug Rule - Day
– Drug A works better than drug B against a tumor.
– Use Drug B first to shrink tumor.
– Use Drug A sequentially to overcome resistance.
– Assumes all tumors of resistant clones.
– Some tumors respond best to sequential therapy allowing for sparing of toxicity.

Combination TherapyCombination Therapy
• Goals
– Maximum cell kill with tolerable toxicity
– Broad coverage of resistant cell lines
– Prevent development of resistance
• Method
– Use only effective drugs
– Use optimal scheduling and dose
– Limit overlapping toxicities
• Goals
– Maximum cell kill with tolerable toxicity
– Broad coverage of resistant cell lines
– Prevent development of resistance
• Method
– Use only effective drugs
– Use optimal scheduling and dose
– Limit overlapping toxicities

Combination TherapyCombination Therapy
• Disadvantages
– Multiple toxicities.
– Reduction or holding of doses due to toxicity will limit effectiveness.
– Complicated to administer.
– Expensive
• Disadvantages
– Multiple toxicities.
– Reduction or holding of doses due to toxicity will limit effectiveness.
– Complicated to administer.
– Expensive

Combination Therapy Toxicity Combination Therapy Toxicity -- CAFCAF
Toxicity Responsible Drug
Alopecia C, A
Cardiotoxicity A
Cystitis C
Mucositis A, F
Myelosuppression C,A,F
Toxicity Responsible Drug
Alopecia C, A
Cardiotoxicity A
Cystitis C
Mucositis A, F
Myelosuppression C,A,F

Factors Affecting Tumor ResponseFactors Affecting Tumor Response
• Tumor Burden• Tumor Site• Tumor Heterogeneity• Drug Resistance• Dose Intensity• Patient Specific Factors• Apoptosis
• Tumor Burden• Tumor Site• Tumor Heterogeneity• Drug Resistance• Dose Intensity• Patient Specific Factors• Apoptosis

Cell Cycle Specific DrugsCell Cycle Specific Drugs
• S Phase Specific Drugs– Antimetabolites
– Folate antagonists(methotrexate)
– Purine antagonists (cladribine)
– Pyrimidine antagonists (cytrarbine,fluorouracil)
• S Phase Specific Drugs– Antimetabolites
– Folate antagonists(methotrexate)
– Purine antagonists (cladribine)
– Pyrimidine antagonists (cytrarbine,fluorouracil)

Cell Cycle Specific DrugsCell Cycle Specific Drugs
• Mitosis Phase Specific Drugs– Vinca Alkaloids (vincristine, vinblastine)– Taxanes (paclitaxel, docetaxel)
• G2 Phase Specific Agents– Topoisomerase I Inhibitors (irinotecan)– Topoisomerase II Inhibitors (etoposide)
• G1 Phase Specific Agents– Enzymes (asparaginase)
• Mitosis Phase Specific Drugs– Vinca Alkaloids (vincristine, vinblastine)– Taxanes (paclitaxel, docetaxel)
• G2 Phase Specific Agents– Topoisomerase I Inhibitors (irinotecan)– Topoisomerase II Inhibitors (etoposide)
• G1 Phase Specific Agents– Enzymes (asparaginase)

Cell Cycle NonCell Cycle Non--Specific DrugsSpecific Drugs
• Alkylating Agents– Cyclophosphamide, busulfan
• Anthracyclines– Doxorubicin, daunorubicin, idarubicin
• Antibiotics– Mitomycin, dactinomycin
• Tryosine Kinase Inhibitors– Imatinib
• Alkylating Agents– Cyclophosphamide, busulfan
• Anthracyclines– Doxorubicin, daunorubicin, idarubicin
• Antibiotics– Mitomycin, dactinomycin
• Tryosine Kinase Inhibitors– Imatinib

Cell Cycle NonCell Cycle Non--Specific DrugsSpecific Drugs
• Biologic Agents– Immunomodulators (Interferon, Interleukin-2)
• Monoclonal Antibodies– Rituximab, Trastuzumab Gemtuzumab Ozogamicin,
Alemtuzumab, Ibritumomab Tiuxetan Yttrium-90, Cetuximab, Bevacizumab
• Hormones– Tamoxifen, leuprolide, flutamide
• Biologic Agents– Immunomodulators (Interferon, Interleukin-2)
• Monoclonal Antibodies– Rituximab, Trastuzumab Gemtuzumab Ozogamicin,
Alemtuzumab, Ibritumomab Tiuxetan Yttrium-90, Cetuximab, Bevacizumab
• Hormones– Tamoxifen, leuprolide, flutamide

Alkylating Agents Alkylating Agents
• Mechanism: Bind to DNA causing breaks• Cell Cycle Non-Specific• Major Toxicity: Myelosuppression, alopecia• Examples:
– Busulfan (Myleran)– Dacarbazine (DTIC)– Cyclophosphamide, Ifosfamide– Melphalan
• Mechanism: Bind to DNA causing breaks• Cell Cycle Non-Specific• Major Toxicity: Myelosuppression, alopecia• Examples:
– Busulfan (Myleran)– Dacarbazine (DTIC)– Cyclophosphamide, Ifosfamide– Melphalan

Busulfan ( Myleran)Busulfan ( Myleran)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
1.8mg/m2PO daily or 0.06 mg/kg one time.
BMT: 4mg/kg/d PO3.2mg/kg/d IV
CMLCLLBMT
Myelosuppression Pulmonary fibrosisCNS Hepatic (VOD)

Dacarbazine (DTIC)Dacarbazine (DTIC)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
250mg/m2x 5 days
SarcomaMelanoma
MyelosuppressionPhotosensitivityFlu-like symptomN/VIrritant Hepatic (vascular)VOD

Cyclophosphamide (Cytoxan)Cyclophosphamide (Cytoxan)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
IV:500-2000mgper m2
Max: 100mg/kg/48H
PO:50-400mg/m2daily
ALLBreastCLLNHLHodgkins
MyelosuppressionN/VCardiac (HD)Hemm. CystitisSIADH

Ifosfamide (Ifex)Ifosfamide (Ifex)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
1-2gm/m2daily x 4IV Only
SarcomaNHLOvarianTesticular
MyelosuppressionN/VHemm. Cystitis(Requires Mesna)CNS

Melphalan (Alkeran)Melphalan (Alkeran)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
Oral: 9mg/m2Daily PO
BMT:50-140mg/m2 IV
Isolated LimbPerfusion: 0.8-1.5mg/kg
M.MyleomaBreast OvarianMelanoma
MyelosuppressionSecondary leukemiaPulmonary fibrosis

Other Alkylating AgentsOther Alkylating Agents
• Procarbazine(Matulane)
• Chlorambucil (Leukeran)
• Mechlorethamine (Mustargen)
• Procarbazine(Matulane)
• Chlorambucil (Leukeran)
• Mechlorethamine (Mustargen)

NitrosoureasNitrosoureas
• Mechanism: Bind to DNA causing breaks• Cell Cycle Non-Specific• Examples
– Carmustine (BCNU)– Lomustine (CeeNu)– Streptozocin (Zanosar)
• Mechanism: Bind to DNA causing breaks• Cell Cycle Non-Specific• Examples
– Carmustine (BCNU)– Lomustine (CeeNu)– Streptozocin (Zanosar)

Carmustine (BCNU)Carmustine (BCNU)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
75-100mg/m2/dayx 2days
CNS TumorsSarcomaHodgkinsNHL
Delayed Myelosuppression(6 week nadir)N/VPulmonary fibrosis

Platinum AnaloguesPlatinum Analogues
• Mechanism: Form Crosslinks in DNA,RNA• Cell Cycle Non-Specific• Major Toxicity: Renal and N/V• Examples:
– Cisplatin (Platinol)– Carboplatin (Paraplatin)
• Mechanism: Form Crosslinks in DNA,RNA• Cell Cycle Non-Specific• Major Toxicity: Renal and N/V• Examples:
– Cisplatin (Platinol)– Carboplatin (Paraplatin)

Cisplatin (Platinol)Cisplatin (Platinol)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
60-100 mg/m2I V q 21 days
LungTesticularHead & NeckBladderOvarian
Renal- hydrateElectrolyte AbnormalityN/V - SeverePeripheral NeuropathyOtotoxicity

Carboplatin ( Paraplatin)Carboplatin ( Paraplatin)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
300-400mg/m2 IVorAUC Dose5-7mg/mlxminDose = AUC(CrCl+25)
LungTesticularHead & NeckBreastBladderOvarian
MyelosuppressionN/VCNS Hypersensitivity

Oxaliplatin (Eloxatin®)Oxaliplatin (Eloxatin®)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
85mg/m2 IVover 2 hoursevery 2 weekscombined with5FU+ LV
Colon 90% NeuropathyMyelosuppression

AnthracyclinesAnthracyclines
• Mechanism: Intercalate DNA base pairs• Cell Cycle Non-Specific• Major Toxicity: Cardiac, Vesicant, Alopecia• Examples:
– Doxorubicin (Adriamycin)– Daunorubicin (Cerubidine)– Idarubicin (Idamycin)– Epirubicin (Ellence)– Mitoxantrone (Novantrone)
• Mechanism: Intercalate DNA base pairs• Cell Cycle Non-Specific• Major Toxicity: Cardiac, Vesicant, Alopecia• Examples:
– Doxorubicin (Adriamycin)– Daunorubicin (Cerubidine)– Idarubicin (Idamycin)– Epirubicin (Ellence)– Mitoxantrone (Novantrone)

Doxorubicin (Adriamycin)Doxorubicin (Adriamycin)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
60-100mg/m2 IV Q21 days
MAX:450mg/m2with XRT300mg/m2
BreastBladderNHLHodgkinsSarcomaMyelomaLungAML
MyelosuppressionCardiac ToxicityN/VMucositisVesicant

Daunorubicin (Cerubidine)Daunorubicin (Cerubidine)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
30-60mg/m2/dayx3-5 days
MAX:550mg/m2in adults
AMLALLNHLWilm’s TumorNeuroblastoma
MyelosuppressionCardiac ToxicityN/VMucositisVesicant

Idarubicin (Idamycin)Idarubicin (Idamycin)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
12 mg/m2/dayx 3 days
MAX:120mg/m2
AMLALL
MyelosuppressionN/VCardiacVesicant

Epirubicin (Ellence)Epirubicin (Ellence)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
IV:60-100mg/m2IVP MAX:700mg/m2
Breast CardiacMyelosuppressionN/VAlopeciaVesicant
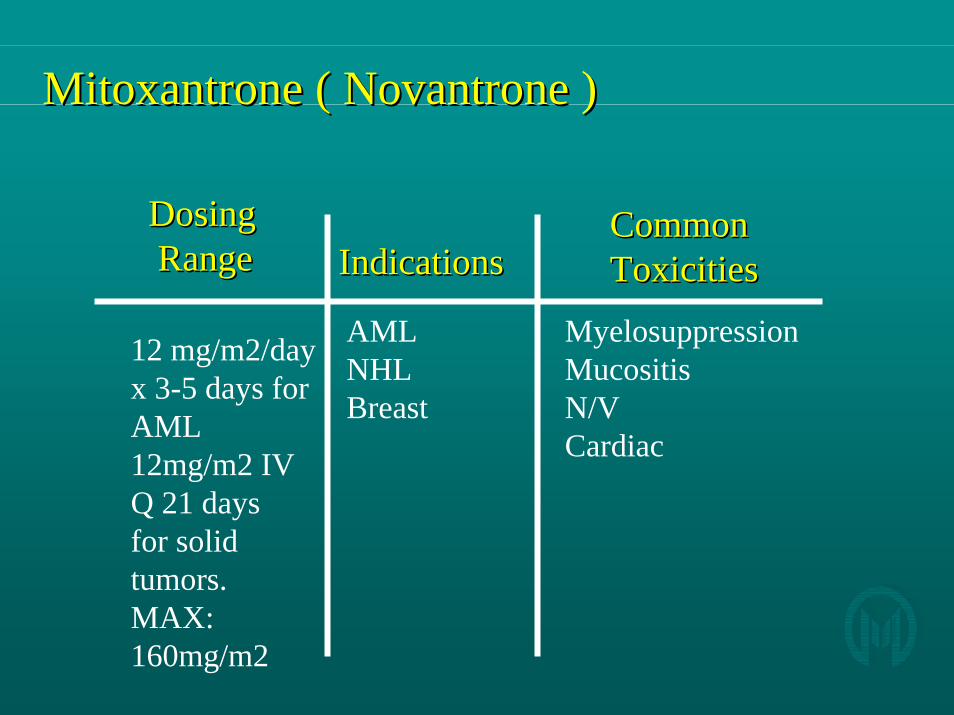
Mitoxantrone ( Novantrone )Mitoxantrone ( Novantrone )
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
12 mg/m2/dayx 3-5 days forAML12mg/m2 IVQ 21 daysfor solid tumors.MAX:160mg/m2
AMLNHLBreast
MyelosuppressionMucositisN/VCardiac

CardiotoxicityCardiotoxicity
Agent EKGCHG
Arrhythmia CHF Myopathy
DoxorubicinDaunorubici
++ ++ +++ +++
Idarubicin ++ ++ ++ ++Epirubicin + + ++ ++Mitoxantrone + ++ +CytoxanIfosfamide
++ ++
Paclitaxel ++ ++
Agent EKGCHG
Arrhythmia CHF Myopathy
DoxorubicinDaunorubici
++ ++ +++ +++
Idarubicin ++ ++ ++ ++Epirubicin + + ++ ++Mitoxantrone + ++ +CytoxanIfosfamide
++ ++
Paclitaxel ++ ++

AntibioticsAntibiotics
• Mechanism: DNA breakage• Cell Cycle Non-Specific• Major Toxicity: Pulmonary and Renal• Examples:
– Mitomycin– Bleomycin
• Mechanism: DNA breakage• Cell Cycle Non-Specific• Major Toxicity: Pulmonary and Renal• Examples:
– Mitomycin– Bleomycin

Mitomycin (Mutamycin)Mitomycin (Mutamycin)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
10-20mg/m2 Q6 weeksMAX: 60mg/m2 Total
BladderBreastLung
MyelosuppressionHUS(dose related)Pulmonary(avoid high O2 levels)Vesicant

Bleomycin (Blenoxane)Bleomycin (Blenoxane)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
10-20 U/m2IV or IM 1-2 x per week
Pleurodesis:60 unitsMAX:400 U Total
TesticularNHLMalignantPleuralEffusions
Pulmonary fibrosis(avoid high O2 levels)AnaphylaxisFeverHyperpimentation

Pulmonary ToxicityPulmonary Toxicity
• Bleomycin– Avoid high 02 concentrations for several weeks post chemo– Incidence is 1-3% when doses >400 units– Symptoms include dyspnea and dry cough
• Carmustine– 20-30% lung fibrosis with doses >600mg/m2
• Mitomycin C– Incidence 3-12% when doses exceed 60 mg
• Busulfan– Incidence of fibrosis 3% when >500mg
• Bleomycin– Avoid high 02 concentrations for several weeks post chemo– Incidence is 1-3% when doses >400 units– Symptoms include dyspnea and dry cough
• Carmustine– 20-30% lung fibrosis with doses >600mg/m2
• Mitomycin C– Incidence 3-12% when doses exceed 60 mg
• Busulfan– Incidence of fibrosis 3% when >500mg

Antimetabolites: Folate AntagonistsAntimetabolites: Folate Antagonists
• Mechanism: Blocks tetrahydrofolic acid production
• Cell Cycle Specific: S Phase• Major Toxicity: Myelosuppression & GI• Example
– Methotrexate– Edatrexate– Pemetrexed
• Mechanism: Blocks tetrahydrofolic acid production
• Cell Cycle Specific: S Phase• Major Toxicity: Myelosuppression & GI• Example
– Methotrexate– Edatrexate– Pemetrexed

Methotrexate (Mexate, MTX)Methotrexate (Mexate, MTX)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
Low:10-100mg/m2Inter: 1-2 g/m2High:10-12 g/m2Intrathecal:12mg
BreastNHLSarcomaALL
MyelosuppressionMucositisRadiation SensitizerRenal- alkalinize urineCNS
(Leucovorin Rescue)

Pemetrexed ( Alimta)Pemetrexed ( Alimta)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
500mg/m2Every 21 days
Requires FolicAcid and B12Supplements
MesotheliomaNSCLC
Neutropenia 24%N/V 30%Fatigue 25%

Antimetabolites: Pyrimidine AntagonistsAntimetabolites: Pyrimidine Antagonists
• Mechanism: Block DNA production• Cell Cycle Specific: S Phase• Major Toxicity: Myelosuppression • Examples
– Cytarabine– Fluorouracil– Capecitabine– Gemcitabine
• Mechanism: Block DNA production• Cell Cycle Specific: S Phase• Major Toxicity: Myelosuppression • Examples
– Cytarabine– Fluorouracil– Capecitabine– Gemcitabine

Cytarabine ( Cytosar, AraCytarabine ( Cytosar, Ara--C)C)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
100-200mg/m2/dayx 5-7 daysCIVI 1-3 g/m2 Q12 hrs bolus10-30mg/m2intrathecal
AMLALLCMLNHL
MyelosuppressionCerebellar (High Dose)Ocular (High Dose)PulmonaryHepatic (VOD)

Fluorouracil (5Fluorouracil (5--FU, Adrucil)FU, Adrucil)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
IV:400 - 500mg/m2 weekly
300-1000mg/m2/dayx 5-7 days
ColonBreastHead & NeckGastric
MyelosuppressionMucositis (CIVI)DiarrheaCardiacRashCNS

Capecitabine (Xeloda)Capecitabine (Xeloda)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
Oral:1250mg/m2BID x 14 daysWith 1-2 weekrest
BreastColon
DiarrheaHand/Foot Syndrome

Gemcitabine (Gemzar)Gemcitabine (Gemzar)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
IV:1000mg/m2over 30 minweekly X 3
PancreaticBreastLung
MyelosuppressionN/VRashHepatic

Antimetabolites: Purine AntagonistsAntimetabolites: Purine Antagonists
• Mechanism: Block DNA production• Cell Cycle Specific: S Phase• Major Toxicity: Myelosuppression • Examples
– Cladribine– Fludarabine– Mercaptopurine
• Mechanism: Block DNA production• Cell Cycle Specific: S Phase• Major Toxicity: Myelosuppression • Examples
– Cladribine– Fludarabine– Mercaptopurine

Cladribine (2Cladribine (2--CDA, Leustatin)CDA, Leustatin)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
0.1mg/kgdaily x 7CIVI
Hairy CellLeukemiaNHLCLLWaldenstrom
MyelosuppressionFeverRash

Fludarabine (Fludara)Fludarabine (Fludara)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
IV:25mg/m2daily x 5
NHLCLLAML
MyelosuppressionEncephalopathyPulmonary

Mercaptopurine (Purinethol, 6Mercaptopurine (Purinethol, 6--MP)MP)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
PO:70-100mg/m2or 2.5mg/kgdaily
HodgkinsALLCMLNHLAML
MyelosuppressionHepatic (VOD)
Interacts withAllopurinol

Vinca AlkaloidsVinca Alkaloids
• Mechanism: Inhibits spindle formation• Cell Cycle Specific: M Phase• Major Toxicity: Neuropathy, alopecia, vesicants• Examples
– Vincristine– Vinblastine– Vinorelbine
• Mechanism: Inhibits spindle formation• Cell Cycle Specific: M Phase• Major Toxicity: Neuropathy, alopecia, vesicants• Examples
– Vincristine– Vinblastine– Vinorelbine

Vincristine (Oncovin)Vincristine (Oncovin)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
IV:0.4-1.4mg/m2weeklyMAX: 2mgweekly
ALLNHLCLLBreastHodgkinsNeuroblastoma
NeuropathyConstipationIleusVesicantSIADH
DEATH with overdoseor intrathecal use

Vinblastine (Velban)Vinblastine (Velban)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
IV:4-10mg/m2weekly
HodgkinsNHLCMLBreast
MyelosuppressionNeuropathyVesicant

Vinorelbine (Navelbine)Vinorelbine (Navelbine)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
IV30mg/m2weekly
BreastNSCLCOvarian
MyelosuppressionNeuropathyConstipationSIADHVesicant (flush vein)

Vesicants Vesicants IrritantsIrritants
• Dactinomycin• Daunorubicin• Doxorubicin• Epirubicin• Idarubicin• Mechlorethamine• Mitomycin C• Dactinomycin • Vincristine• Vinblastine• Vinorelbine
• Dactinomycin• Daunorubicin• Doxorubicin• Epirubicin• Idarubicin• Mechlorethamine• Mitomycin C• Dactinomycin • Vincristine• Vinblastine• Vinorelbine
• Cisplatin
• Carboplatin
• Docetaxel
• Etoposide
• Mitoxantrone
• Paclitaxel
• Teniposide
• Cisplatin
• Carboplatin
• Docetaxel
• Etoposide
• Mitoxantrone
• Paclitaxel
• Teniposide

ExtravasationExtravasation

Treatment of ExtravasationsTreatment of Extravasations
• Stop Infusion• Leave catheter in place• Remove tubing• Aspirate as much as possible from site• Instill antidote if indicated• Remove needle• Inject SQ antidote into site in 3-6 areas around site
– Sodium thiosulfate 1/6 M for mechlorethamine,cisplatin, carboplatin– Hyaluronidase 150-900 units for vinca alkaloids
• Apply cold compress 45 minutes on 15 min off for 24 hr• Apply warm compress for vincas, etoposide and taxanes
• Stop Infusion• Leave catheter in place• Remove tubing• Aspirate as much as possible from site• Instill antidote if indicated• Remove needle• Inject SQ antidote into site in 3-6 areas around site
– Sodium thiosulfate 1/6 M for mechlorethamine,cisplatin, carboplatin– Hyaluronidase 150-900 units for vinca alkaloids
• Apply cold compress 45 minutes on 15 min off for 24 hr• Apply warm compress for vincas, etoposide and taxanes

Topoisomerase Topoisomerase I Inhibitors:I Inhibitors:CamptothecinsCamptothecins• Mechanism: Inhibit Topoisomerase I• Cell Cycle Specific: G2 Phase• Major Toxicity:Diarrhea,Myelosuppression• Examples
– Irinotecan– Topotecan
• Mechanism: Inhibit Topoisomerase I• Cell Cycle Specific: G2 Phase• Major Toxicity:Diarrhea,Myelosuppression• Examples
– Irinotecan– Topotecan

Irinotecan Irinotecan ((CamptosarCamptosar, CPT, CPT--11)11)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
IV: 125mg/m2 weekly x 4 Or 350mg/m2Q 21 days
ColonSCLCPancreaticGastric
Diarrhea(Loperamide)MyelosuppressionFlushingN/VAlopecia

Topotecan Topotecan ((HycamtinHycamtin))
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
1.5mg/m2daily x5
LungOvarian
MyelosuppressionDiarrheaHeadache

DiarrheaDiarrhea
• Causative agents
– Irinotecan
– Topotecan
– Cytarabine
– Fluorouracil
– Methotrexate
– Gemcitabine
• Causative agents
– Irinotecan
– Topotecan
– Cytarabine
– Fluorouracil
– Methotrexate
– Gemcitabine
• Treatment
– Loperamide
– Octreotide
• Treatment
– Loperamide
– Octreotide

Topoisomerase Topoisomerase II Inhibitors:II Inhibitors:EpipodophyllotoxinsEpipodophyllotoxins• Mechanism: Inhibit Topoisomerase II• Cell Cycle Specific: G2 Phase• Major Toxicity: Myelosuppression,
Mucositis• Examples
– Etoposide– Teniposide
• Mechanism: Inhibit Topoisomerase II• Cell Cycle Specific: G2 Phase• Major Toxicity: Myelosuppression,
Mucositis• Examples
– Etoposide– Teniposide

Etoposide Etoposide ((VepesidVepesid))
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
IV:30-120mg/m2/dayx 1-5 daysPO:50% Absorbed.50-100mg/m2 daily
LungNHLBreastAMLALL
MyelosuppressionMucositisAlopecia Infusion-related:Hypotension

Teniposide Teniposide ((VumonVumon))
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
IV:ALL:165mg/m2twice a week
Solid Tumors:60-90mg/m2
ALLNeuroblastomaNHL
MyelosuppressionMucositis

TaxanesTaxanes
• Mechanism: Stabilizes Microtubules• Cell Cycle Specific: M Phase• Major Toxicity: Myelosuppression,
Neuropathy, Allergic Reactions, Alopecia• Examples
– Paclitaxel– Docetaxel
• Mechanism: Stabilizes Microtubules• Cell Cycle Specific: M Phase• Major Toxicity: Myelosuppression,
Neuropathy, Allergic Reactions, Alopecia• Examples
– Paclitaxel– Docetaxel

Paclitaxel Paclitaxel ((TaxolTaxol))
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
IV:135-250mg/m2Q21 daysor80mg/m2weekly
BreastLungOvarianHead & NeckBladder
MyelosuppressionHypersensitivityNeuropathyMyalgiaAlopecia

Docetaxel Docetaxel ((TaxotereTaxotere))
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
60-100mg/m2Q 21 days
BreastLungH+NOvarian
MyelosuppressionPleural EffusionsPeripheral EdemaAngioedemaHypersensitivityMucositisAlopecia

ImmunomodulatorsImmunomodulators
• Mechanism: Enhance immune function• Cell Cycle Non- Specific • Major Toxicity:Myalgia, hypotension• Examples
– Interferon– Aldesleukin (IL-2)
• Mechanism: Enhance immune function• Cell Cycle Non- Specific • Major Toxicity:Myalgia, hypotension• Examples
– Interferon– Aldesleukin (IL-2)

Interferon (Interferon (Roferon Roferon A, A, Intron Intron A)A)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
IM or SQ:3-10 MillionUnits 3 timesa week.
MelanomaCML
Flu SymptomsMyalgiaFeverN/V, AnorexiaDepressionCough

Aldesleukin Aldesleukin ( ( ProleukinProleukin, IL, IL--2)2)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
IV: High-dose600,000 Units/Kg Q 8 HrsLow-dose2million/m2daily x 4 as CIVI
Renal CellMelanoma
Hypotension ( with high dose) Fever, chills Edema, EffusionsLiver Toxocity

Monoclonal AntibodiesMonoclonal Antibodies
• Mechanism: Destroy specific cells with antigenic markers
• Cell Cycle Non- Specific • Major Toxicity: Infusion-related toxicity• Examples:
– Rituximab– Trastuzumab– Gemtuzumab Ozogamicin– Alemtuzumab– Ibritumomab Tiuxetan Yttrium-90– Cetuximab– Bevacizumab
• Mechanism: Destroy specific cells with antigenic markers
• Cell Cycle Non- Specific • Major Toxicity: Infusion-related toxicity• Examples:
– Rituximab– Trastuzumab– Gemtuzumab Ozogamicin– Alemtuzumab– Ibritumomab Tiuxetan Yttrium-90– Cetuximab– Bevacizumab

Rituximab Rituximab ( ( RituxanRituxan))
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
IV:375mg/m2slowly Q week
NHL(CD-20 +)
Fever, chills(1st infusion worst)HypotensionBronchospasmTLS (large tumor)

TrastuzumabTrastuzumab ((HerceptinHerceptin))
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
IV:Load: 4mg/kgover 90 min.
Maint: 2mg/kgover 30 min.Q week
Breast(Her-2 overexpression)
Fever, Chills(1st Infusion)Cardiac (CHF)√ MUGAN/V, DiarrheaRash

Gemtuzumab Ozogamicin Gemtuzumab Ozogamicin ((MylotargMylotarg))
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
IV:9mg/m2 over 2 hourson Day 1 and15.
AML for patients>60 year
Fever, Chills,Hypotension,Neutropenia, Thrombocytopenia,Anemia,Tumor Lysis

Alemtuzumab Alemtuzumab ((CampathCampath))
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
IV:3mg IV dailyover 2 hoursthen 10mg daily,then 30mg 3x a week
Anti CD-52B-cell CLLfailed Fludarabine
Fever, Chills,Hypotension,Neutropenia, Thrombocytopenia,Anemia,Tumor LysisHSV AND PCP x 2months

Ibritumomab Tiuxetan Ibritumomab Tiuxetan YY--90 (90 (ZevalinZevalin))RadioimmunotherapyRadioimmunotherapy
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
IV:0.3 -0.4mCi/kgonce
Refractorylow-grade CD20+NHL
Neutropenia 63%, Thrombocytopenia 60%,Anemia 17%

CetuximabCetuximab ((ErbituxErbitux))
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
IV:400mg/m2Over 2 hrs x1, Then250mg/m2 Over 1 hrWeekly.
EGFR +ColorectalIrinotecan refractory
Infusion Reaction 3%Bronchospasm, AnaphylaxisInter. Lung Dis. 1%Severe Acne 14%Fever 5%

Bevacizumab Bevacizumab ((AvastinAvastin))
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
IV:5mg/kg Over 90 min.every14 days.
MetastaticColorectalAnti-VEGF
Infusion ReactionsGI Perforation 2%HemorrhageNephrotic SyndromeCHF 14%Neutropenia 21%Hypertension 60%

Tyrosine Tyrosine Kinase Kinase InhibitorInhibitor
• Mechanism: Inhibits tyrosine kinase regulation of cell growth
• Cell Cycle Non- Specific • Major Toxicity: Variable• Examples:
– Imatinib– Erlotinib
• Mechanism: Inhibits tyrosine kinase regulation of cell growth
• Cell Cycle Non- Specific • Major Toxicity: Variable• Examples:
– Imatinib– Erlotinib

ImatinibImatinib ( ( GleevecGleevec))
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
PO: 400 -800mg daily
CML: Ph +,chronic,acceleratedphases,and blast crisis
Neutropenia 33-60%Thrombocytopenia 16- 60%Anemia 4-50%Hepatotoxicity 1-3%Fluid Retention1-5%

ErlotinibErlotinib ((TarcevaTarceva))
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
PO: 100-150mg daily
NSCLCPancreatic
Interstitial Lung Disease 1%Hepatotoxicity RashFatigue

Hormonal AgentsHormonal Agents• Mechanism: Block or prevent hormonal
effects on tumor cells• Cell Cycle Non- Specific • Major Toxicity: Hormonal dysfunction• Examples:
– Tamoxifen – Leuprolide– Bicalutimide
• Mechanism: Block or prevent hormonal effects on tumor cells
• Cell Cycle Non- Specific • Major Toxicity: Hormonal dysfunction• Examples:
– Tamoxifen – Leuprolide– Bicalutimide

Tamoxifen (Nolvadex)Tamoxifen (Nolvadex)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
PO:10-20mg POBID
Breast Hot FlashesN/VFlare ReactionVTECategory D:PRF

AnastrazoleAnastrazole ((ArimidexArimidex))
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
PO:1mg daily
Breast Hot FlashesN/VFlare ReactionVTEPreg Category D:

Leuprolide (Lupron)Leuprolide (Lupron)
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
IM:7.5mg monthly or 22.5mg q3months
Prostate Hot flashesImpotenceDecreased LibidoTumor Flare

FlutamideFlutamide ((EulexinEulexin ))
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
PO:250mg tid
Prostate HepatotoxicityGynecomastiaDiarrheaMyalgia

BicalutamideBicalutamide ((CasodexCasodex))
IndicationsIndicationsDosingDosingRangeRange
Common Common ToxicitiesToxicities
PO:50-150 mg daily
Prostate HepatotoxicityGynecomastiaDiarrheaMyalgia

Calculations:Calculations:
Height (cm) x Weight (Kg)3600
BSA (m2) =
Body Surface AreaBody Surface Area
Estimated Estimated Creatinine Creatinine ClearanceClearanceGFR Males = (140-age) x Weight ( Kg)
72 x SCrGFR Females = GFR Males X 0.85
Recommended

















