CELLULITIS Presented by Wendy Gerstein, MD Thursday School
7/24/14
Slide 2
QUESTION 1 38 yo woman is evaluated in urgent care for redness
and pus that developed near a scratch on her right shin. On PE:
T=37.3 C, bp 135/75, p 78, rr 14. A 3x2 cm erythematous, warm patch
is present over the right shin with associated purulence/pus, but
no fluctuance, drainable abscess or lymphadenopathy is present. WBC
is 10k with 70% N and 30% L. She has no drug allergies. Which of
the following is the most appropriate outpatient therapy? A)
Cephalexin (Keflex) B) Dicloxacillin C)
Trimethoprim-sulfamethoxazole (Bactrim) D) Amoxicillin
Slide 3
QUESTION 2 A 27 yo male is evaluated for redness that developed
over his left forearm at the site of a mosquito bite. He is
otherwise healthy and takes no medications. PE: T= 37.2 C, bp
120/70, p 68, rr 14. There is an erythematous 3x3 cm patch on the
left forearm. The area is warm to the touch with no evidence of
purulence, fluctuance, crepitus, or lymphadenopathy. Which of the
following is the most appropriate empiric outpatient therapy? A)
Doxycycline B) Cephalexin (Keflex) C) Fluconazole D)
Trimethoprim-sulfamethoxazole (Bactrim) E) Metronidazole
Slide 4
ANSWERS Answer for question 1: C, Bactrim Answer for question
2: B, Cephalexin (Keflex) What is the one important difference
between the two cases?
Slide 5
Slide 6
CELLULITIS
Slide 7
Clinical presentation: local tenderness, pain and erythema that
rapidly increases. Borders are not elevated or sharply demarcated
(as in erysipelas). May have patchy involvement with skip areas.
Systemic manifestations include mild fever, chills and malaise, can
progress to sepsis.
Slide 8
CELLULITIS Complications can include bacteremia, abscesses,
overlying skin necrosis, muscle/joint/bone involvement. Risk
factors: lymphedema, chronic venous stasis, trauma, skin breakdown
(fungal infection), diabetes, immunosuppression, altered
anatomy/surgery. Patient who are showing systemic signs (i.e., meet
SIRS criteria) should be admitted for initial treatment with IV
antibiotics, then transition to appropriate oral therapy.
Slide 9
ORGANISMS Most common organisms: streptococci (group A
-hemolytic [GABHS] most likely) and Staphylococcus aureus. Think
strep if peau dorange skin changes and lymphangitis are present.
Think S. aureus (and CA-MRSA, MRSA) if purulence or abscess
present. Erysipelas: superficial, well-demarcated, intensely
erythematous, indurated borders. GABHS.
Slide 10
Slide 11
CELLULITIS Post-operative infections with Group A strep are
uncommon but can spread rapidly and develop into bacteremia/sepsis.
Can occur within 6-48 hours after surgery. Hypotension may be the
first signs of infection prior to cellulitis. Thin serous discharge
may be expressed from the surgical site that is gram stain positive
for streptococci.
Slide 12
CELLULITIS Diabetics: at risk for polymicrobial infections
including: GPC including S. aureus, Enterococcus, various
streptococcal species, peptostreptococcus (anaerobe). GN aerobes:
Enterobacter, Acinetobacter, and Pseudomonas. GN anaerobes:
Bacteroides
Slide 13
ANTIBIOTICS IN CELLULITIS At minimum, need empiric coverage for
strep species and S. aureus. Include a -lactam antibiotic with
activity against penicillinase- producing S. aureus (MSSA). If not
severe may treat as outpatient. Cephalexin or dicloxacillin have
good strep and MSSA coverage. Clindamycin may be used for strep and
CA-MRSA (know local antibiogram). If suspect MRSA then consider
TMP-SMX or doxycycline (can add clindamycin or amoxillin if need
improved strep coverage). May also consider Linezolid.
Slide 14
ANTIBIOTICS CONT. Inpatient antibiotic choices: Strep/MSSA
choices: nafcillin, cefazolin, clindamycin CA-MRSA/MRSA:
clindamycin (know antibiogram), vancomycin, daptomycin, linezolid,
ceftaroline. Diabetics: broaden to amp-sulbactam (moderate
infection), pip/tazobactam (severe) plus MRSA coverage. Remember
ceftriaxone does not have anaerobic coverage. Septic patient: start
broad, then narrow coverage as cultures return.
Slide 15
Slide 16
CA-MRSA/MRSA
Slide 17
MRSA CELLULITIS GUIDELINES For a cutaneous abscess incision and
drainage is the primary treatment. When is adjunct antibiotic
therapy recommend for abscesses? Severe or extensive (multiple
sites) or rapid progression in presence of cellulitis. Signs of
systemic illness. Associated comorbidities or immunosuppressed.
Extremes of age.
Slide 18
MRSA CELLULITIS GUIDELINES Abscess in area difficult to drain
(face, hand and genitalia). Associated with septic phlebitis. Lack
of response to incision and drainage.
Slide 19
MRSA CELLULITIS GUIDELINES Treatment of purulent cellulitis:
Empiric treatment for CA-MRSA/MRSA. Bactrim, clindamycin,
doxycycline or minocycline, linezolid. If need MRSA and
streptococcus coverage: clindamycin; or bactrim or doxycycline with
amoxicillin; or linezolid alone. If inpatient treat with IV
antibiotics initially: vancomycin, clindamycin, linezolid,
daptomycin, ceftaroline.
Slide 20
Slide 21
AJM 2010;123:942-950 Retrospective cohort study in 2005-2007
comparing bactrim to cephalexin to clindamycin for mild to moderate
cellulitis. 405 patients in study: Excluded patients with severe
cellulitis. MRSA recovered in 72/117 positive culture specimens.
Successful treatment TMP-SMX 138/152 (91%) Cephalexin 134/180 (74%)
Clindamycin 34/40 (85%)
Slide 22
HOW LONG TO TREAT?? IDSA guidelines: five days of treatment is
a effective as a 10 day course for uncomplicated cellulitis. Based
on a 2004 study in which 87 patients were treated with levofloxacin
500mg po qd x 5 days compared with 43 patients who received
levofloxacin for 10 days. Complete resolution on day 14 was similar
and day 28 recurrence rate was similar.
Slide 23
However levofloxacin has a longer life than -lactam antibiotics
that are used more commonly. IDSA recommends evaluation at day 5 if
resolved can stop antibiotics. If persisting, continue to 10 days.
Arch Intern Med 2004;164:1169-1674.
Slide 24
PROPHYLAXIS FOR RECURRENT CELLULITIS First identify and treat
predisposing conditions (edema, obesity, eczema, venous
insufficiency, fungal foot infections). Oral penicillin 250-500 mg
po bid for one year should be considered in patients who have >3
episodes per year despite attempts to treat or control predisposing
factors. Can continue past one year (indefinitely) if factors
persist and patient tolerating. IDSA guidelines, 2014. Based on two
studies, PATCH 1 and PATCH 2.
Slide 25
SPECIAL CIRCUMSTANCES FOR CELLULITIS Erysipelothrix
rhusiopathiae (erysipeloid) gram positive facultative anaerobic
rod. Causes an indolent cellulitis occurring in persons who handle
saltwater fish, shellfish, poultry, meat and hides. Treat with
penicillin or cephalosporin. Aeromonas hydrophila gram negative rod
that causes an acute cellulitis after laceration while swimming in
fresh water. Also associated with medicinal leeches. Treat with
ciprofloxacin +/- doxycycline.
Slide 26
SPECIAL CIRCUMSTANCES FOR CELLULITIS Vibrio vulnificus (curved
gram negative rod) causes cellulitis, bullous lesions or necrotic
ulcers after exposure to warm coastal water or exposure to
drippings from raw seafood. Infection can progress to necrosis
requiring surgical debridement. Bacteremia with septicemia can
occur after eating raw oysters, can develop associated skin
findings. Alcoholic cirrhosis, hemochromatosis and thalassemia
increase the risk of septicemia and development of necrotizing
fasciitis (due to iron overload). Treat with doxycycline plus
ceftriaxone.
Slide 27
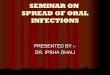
E. RHUSIOPATHIAE AND VIBRIO E. rhusiopathiae Vibrio
species
Slide 28
OTHER Animal or human bite: Clean wound, check tetanus status
of patient, rabies status of animal. Usually polymicrobial
infection due to mouth and skin flora. Empiric antibiotic coverage
with Augmentin or unasyn. Penicillin allergic : fluoroquinolone or
doxycycline (plus clindamycin or metronidazole for anaerobic
coverage).
Slide 29
Drugs 2003;63:1459-1480
Slide 30
IMMUNOSUPPRESSED (CANCER PATIENTS, AIDS, TRANSPLANT)
Differential for skin lesions much broader in this subset biopsy is
necessary is most cases, get early if possible. Need to consider
infection, drug reaction/eruption, Sweet syndrome, malignancy,
leukocytoclastic vasculitis, erythema multiforme.
Slide 31
QUESTION 3 40 yo male evaluated in ER for LUE skin infection.
He works at the VA, where he sustained a minor laceration 3 days
ago when trying to prevent a patients fall. He cleaned and bandaged
the laceration but developed purulence, surrounding tenderness, and
now with fever over last 24 hours. On exam T=38.5, bp 125/75, p 90,
rr 18. An area of purulent cellulitis measuring 4x5 cm surrounding
a 1.5 cm laceration is present. No fluctuance. Rest of exam wnl.
WBC 14k, 90% neutrophils. UA nl. Radiograph of arm only shows soft
tissue swelling.
Slide 32
QUESTION 3 CONTINUED Which of the following beta-lactam
antibiotics is most appropriate for treatment of this infection? A)
Meropenem B) Oxacillin C) Zosyn (pip/tazobactam) D) Ceftaroline E)
Ceftriaxone
Slide 33
QUESTION 3 CONTINUED Correct answer is D, ceftaroline need MRSA
coverage due to purulence, health-care associated. Vancomycin would
have been correct if offered as a choice.
Slide 34
Slide 35
NECROTIZING FASCIITIS Deep tissue infection that spreads
rapidly along fascial planes. Clinical features that suggest a
necrotizing infection include: Severe constant pain, pain out of
proportion to exam. Bullae: related to occlusion of deep blood
vessels that traverse the fascia or muscles. Skin necrosis or
ecchymosis that precedes the skin necrosis. Gas in the soft
tissues. Edema that extends beyond the margin of the erythema.
Cutaneous anesthesia. Systemic toxicity (fever, leukocytosis,
delirium, renal failure). Rapid spread, especially concerning if on
antibiotic therapy. Subcutaneous tissues feels wooden-hard.
Slide 36
Slide 37
Slide 38
NECROTIZING FASCIITIS
Slide 39
Slide 40
Type I- Polymicrobial Includes at least one anaerobic species,
commonly Bacteroides or Peptostreptococcus; Plus one or more
facultative anaerobic species such as streptococci; Plus members of
Enterobacteriaceae (E. coli, Enterobacter, Klebsiella, Proteus.
Associated with: Surgical procedures involving the bowel or
penetrating abdominal trauma. Decubitus ulcer or a perianal
abscess. Site of injection in IVDA. Spread from a Bartholin abscess
or minor vulvovaginal infection.
Slide 41
NECROTIZING FASCIITIS Type II (aka hemolytic streptococcal
gangrene): Group A streptococci are isolated either alone or with
S. aureus Usually involves the limbs with 2/3 in the lower
extremities. Associated with underlying disease: DM
Arteriosclerotic vascular disease Venous insufficiency with edema
Chronic vascular ulcer Post varicella infection commonly due to S.
pyogenes Mortality is high- 50-70% in patients with hypotension and
organ failure. Lancet 1994;344:1111-5
Slide 42
NECROTIZING FASCIITIS Type III- Gram negative monomicrobial
Vibrio spp V. damselae and V. vulnificus Mortality of 30-40%
despite prompt diagnosis and aggressive therapy. (J of Hos Infec
2010;75:249-257) Type IV- Fungal Cases of candida NF very rare,
mostly in immunocompromised. Zygomycotic NF (Mucor and Rhizopus
spp) affect immunocompetent patients after severe trauma. Burns or
trauma wounds with aspergillus or zygomycetes should be consider
infected (not just colonized). (J of Hos Infec 2010;75:249-
257
Slide 43
NECROTIZING FASCIITIS Determinants of mortality Retrospective
study in 2005 in Taiwan. Studied both type I and type II
necrotizing fasciitis. 87 pts. Found increased mortality with: Age
>60 2 comorbidities, especially DM and liver disease
Thrombocytopenia Abnormal liver function tests Increased BUN and Cr
Low serum albumin level Patients who underwent emergent debridement
in
Slide 44
NECROTIZING FASCIITIS Studies CT scan or MRI may show edema
and/or gas extending along the fascial plane. In practice, clinical
judgment is the most important element of diagnosis. Cultures
obtained from deep tissue during surgery are helpful. Skin cultures
usually contaminated with skin flora.
Slide 45
Slide 46
NECROTIZING FASCIITIS Treatment: Surgical intervention: No
response to antibiotic therapy. Profound toxicity with fever,
hypotension, or advancement of skin and soft-tissue infection
during antibiotic therapy. Local wound shows any necrosis with easy
dissection along fascia by blunt instrument. Any soft tissue
infection accompanied by gas. Most patients with necrotizing
fasciitis should return to the OR within 24-36 hours after first
debridement and daily thereafter until surgical team finds no
further need for debridement.
Slide 47
NECROTIZING FASCIITIS Empiric coverage: very broad
Piperacillin-tazobactam, plus vancomycin OR Meropenem/imipenem plus
vancomycin. PCN allergy: Cefotaxime, plus metronidazole or
clindamycin, plus vancomycin. Severe PCN allergy: clindamycin or
metronidazole, plus aminoglycoside or fluoroquinolone, plus
vancomycin.
Slide 48
NECROTIZING FASCIITIS Streptococci infections PCN: most
streptococci are susceptible in the US. Clindamycin: in vitro
studies demonstrate both toxin suppression and modulation of
cytokine TNF production. Give both initially.
Slide 49
NECROTIZING FASCIITIS IVIG not enough evidence to recommend
therapy. HBO hyperbaric oxygen not enough evidence to recommend
therapy.