Embed Size (px)
Citation preview
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 1/183
CELLULITIS
A.prof. Keam Born.Dental department of Khmer
Soviet Friendship Hospital
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 2/183
CELLULITIS OF MAXILLA
Cellulitis KWCa A painful swelling of the soft tissue of the
mouth and face resultating from a diffuse spreading of purulent
exudate along the facial planes that separate the muscle
bundles.
Cellulitis enHekItelImnusSRKb;rUbTaMgGs;. Cellulitis GacekItenA eRkamEs,k eRkam Mucosa cenøaHsac;duM b¤q¥wg nig Lymph node .
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 3/183
ETIOLOGY –
tamkarRsavRCav )anbBa¢ak;;[dwgfa 84 % énGñkCMgW Cellulitis TaMgGs; eRcIn
bNþalmkBI Odontogenic factors .
tamRbPBEdlbgá[man Infections manBIrRbePTKW ³
● local factors
● general factors
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 4/183
● local factors :
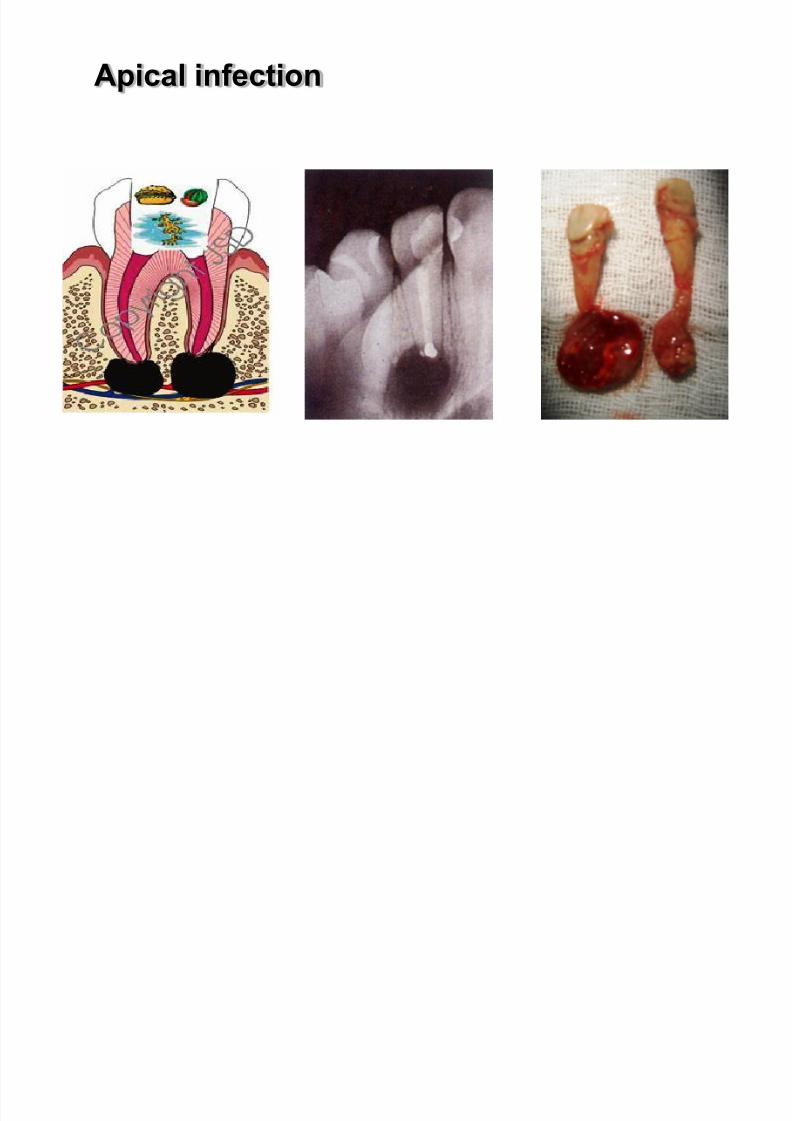
- Apical infection
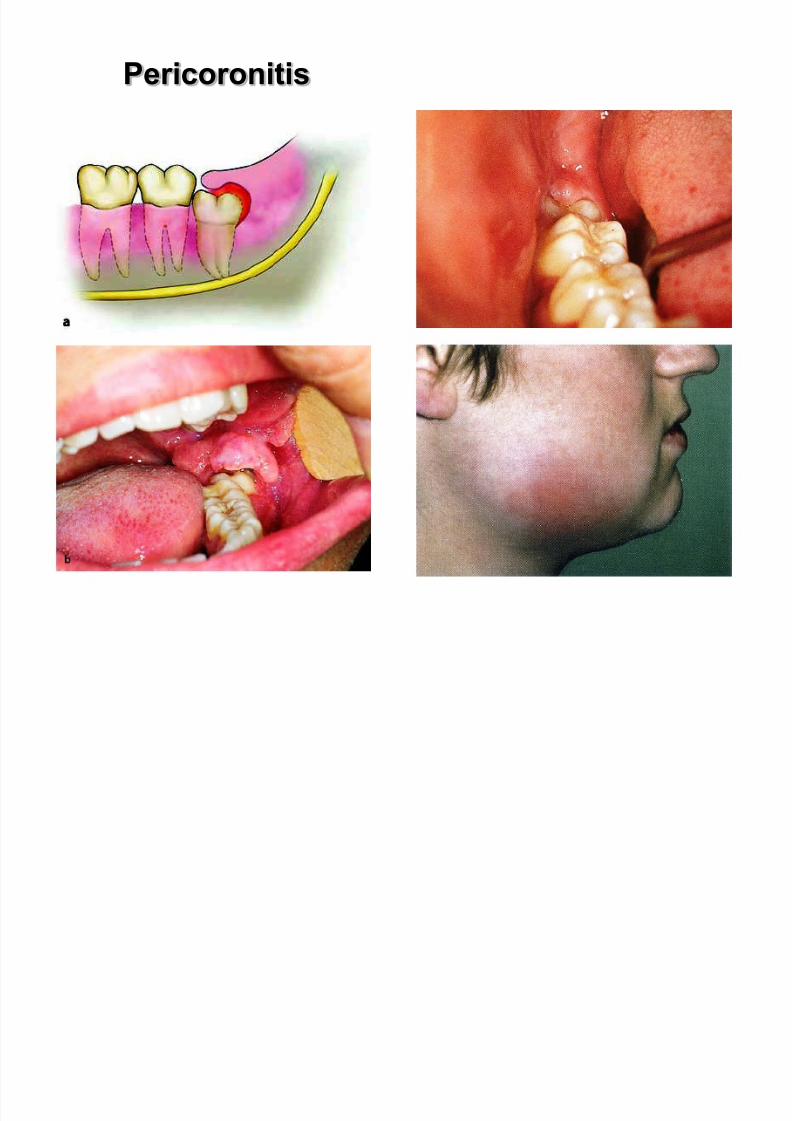
- pericoronitis
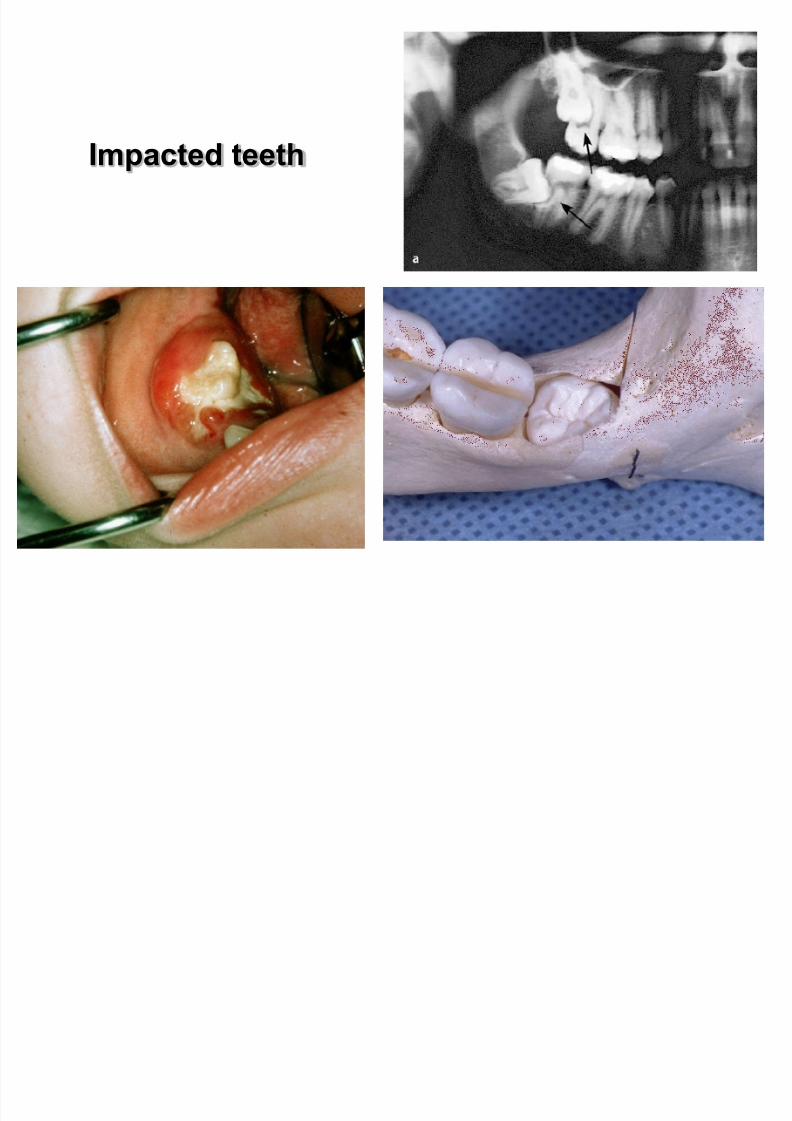
- impacted teeth
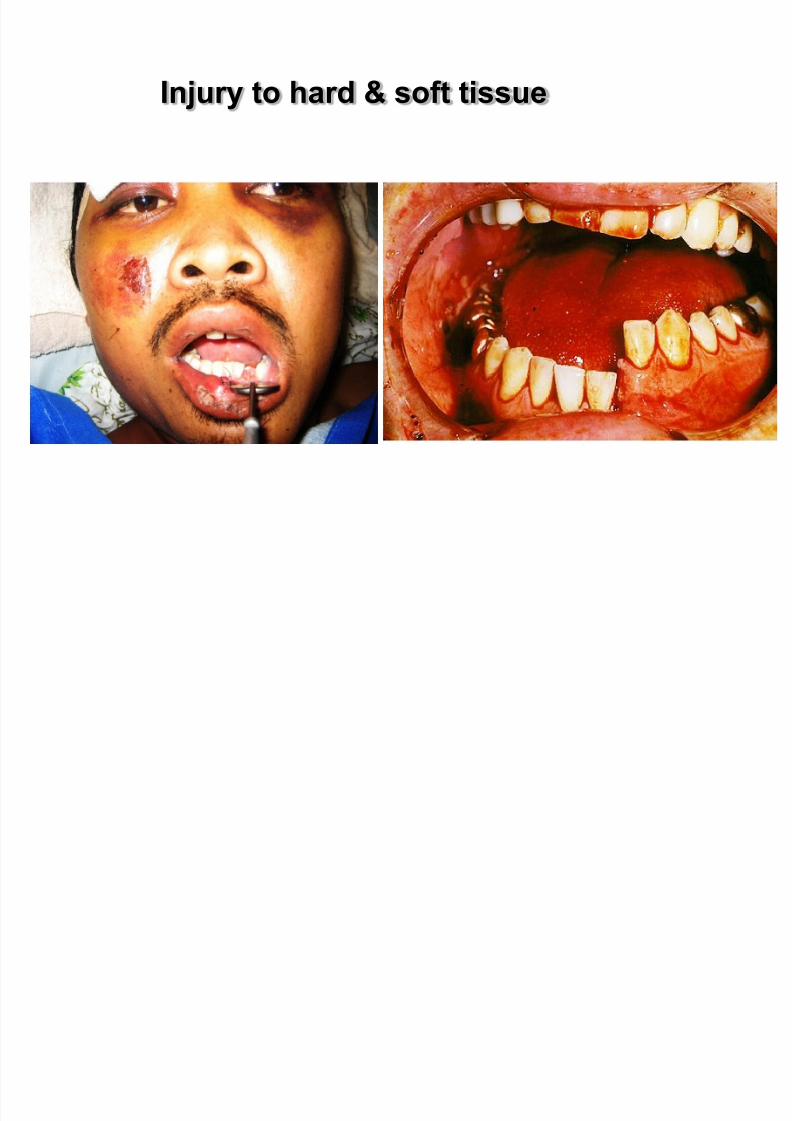
- Pus in the gingival pocket- Trauma (fracture of the facial bone,tooth extractions)
- Infected needle through infected area
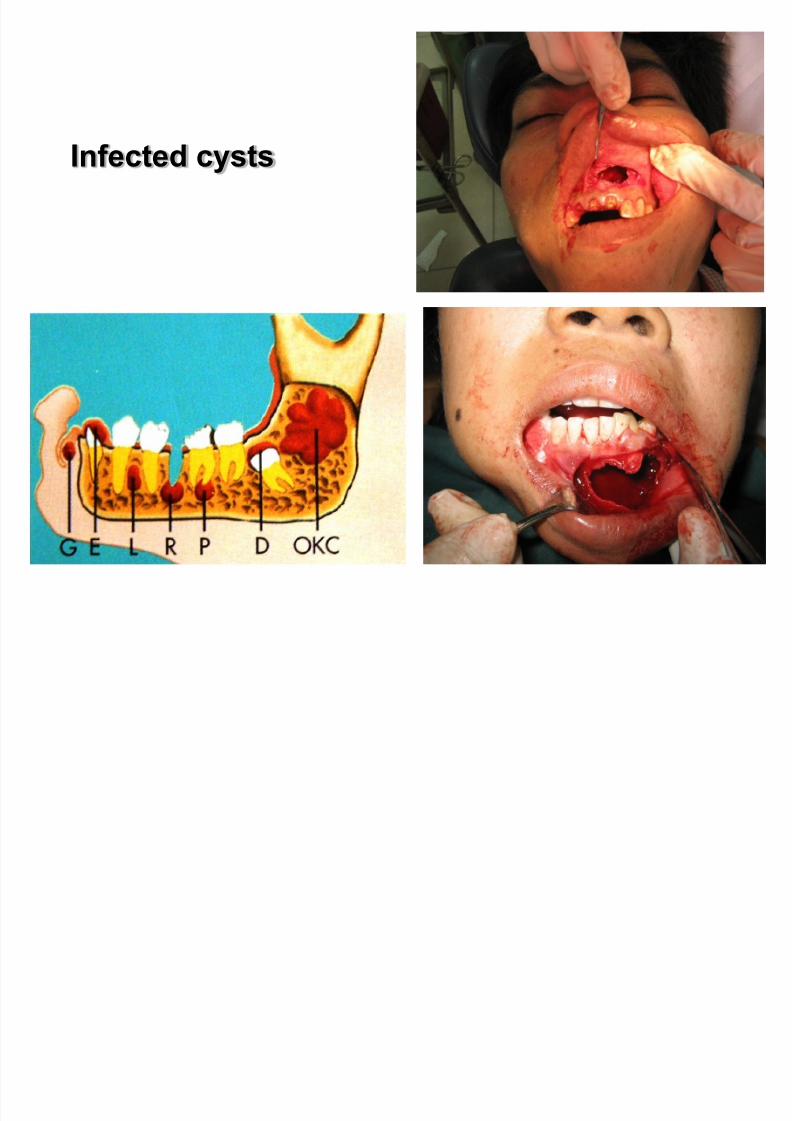
- Infected cysts
- Stomatitis
- infection of the salivary glande or lymph node
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 5/183
Apical infection
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 6/183
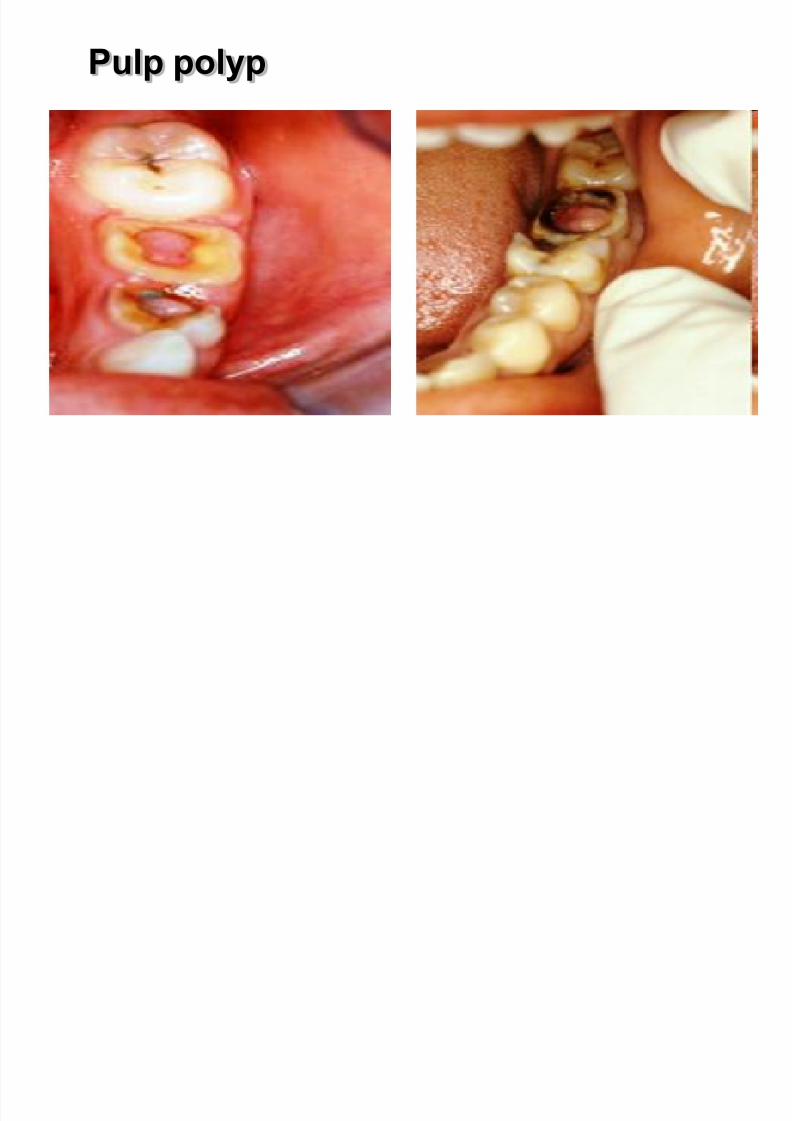
Pulp polyp
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 7/183
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 8/183
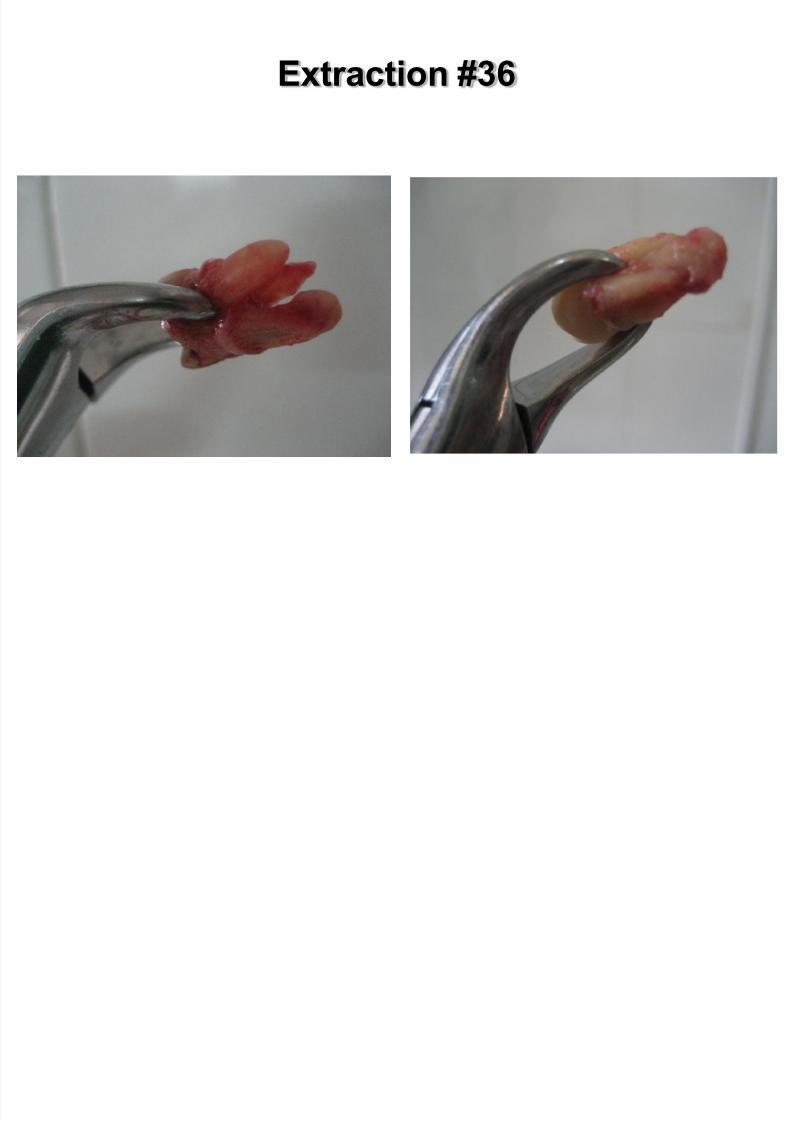
Extraction #36
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 9/183
Pathways of Odontogenic Infection
Usual cause of odontogenic infection: necrosis of tooth pulp
and bacterial invasion through the pulp chamber into deeper tissues.
Pulp necrosis results from deep decay in tooth,(inflammatory reaction).
The pulpal foramen does not allow drainage of the infectedpulp.
Further progression leads to medullary space infection andosteomyelitis.
More commonly, get fistulous tracts through alveolar bone.
Fistulous tract may penetrate oral mucosa or facial skin .

8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 10/183
Subperiosteal abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 11/183
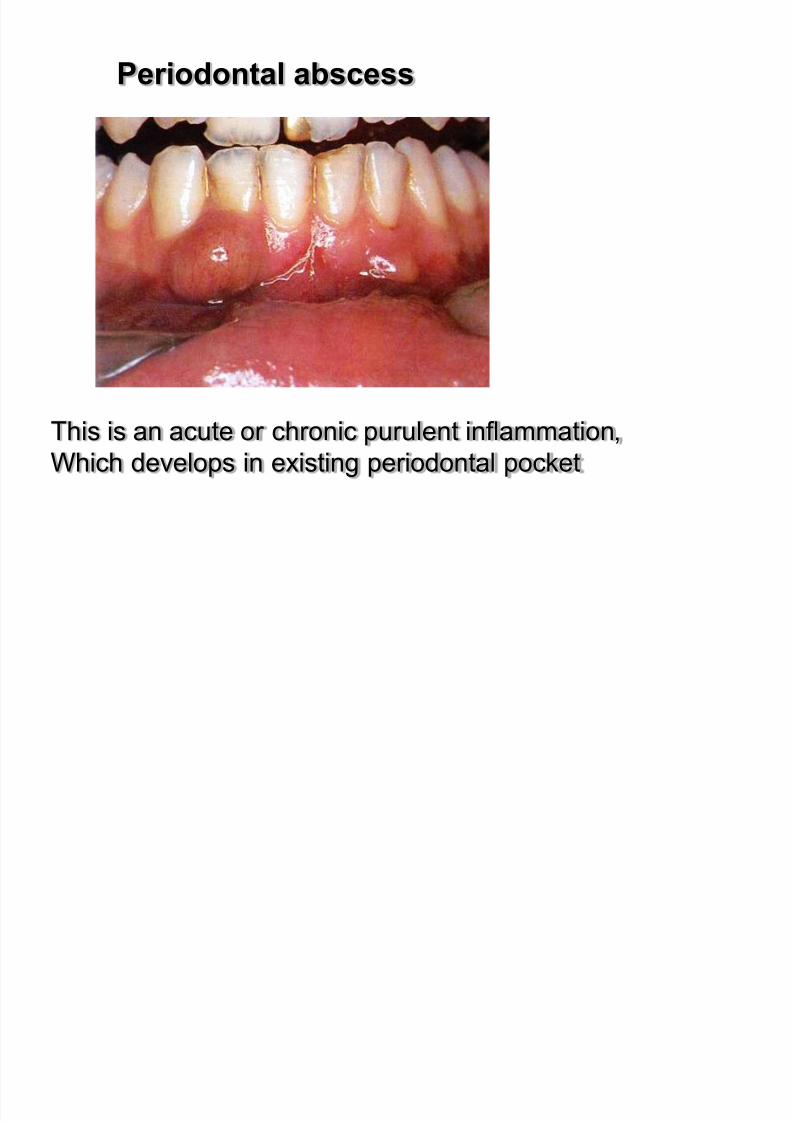
Periodontal abscess
This is an acute or chronic purulent inflammation,
Which develops in existing periodontal pocket
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 12/183
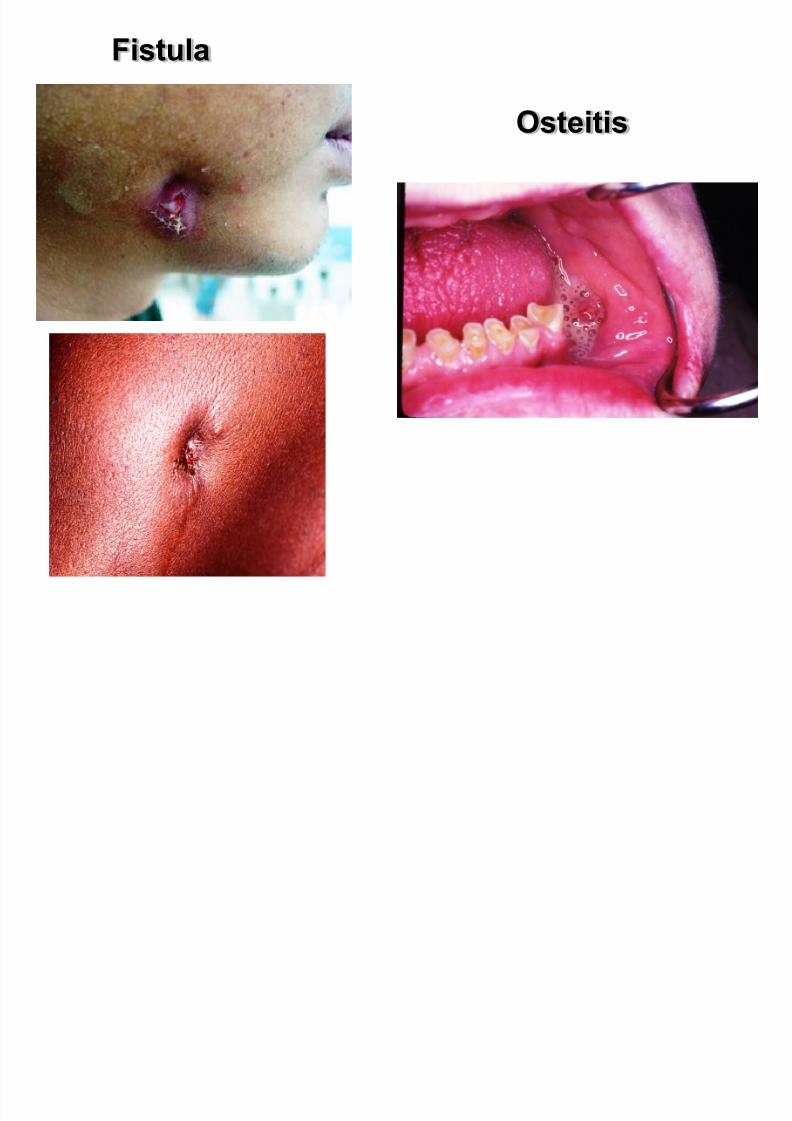
Fistula
Osteitis

8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 13/183
Periodontal abscess in the region of
the mandible second molar
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 14/183
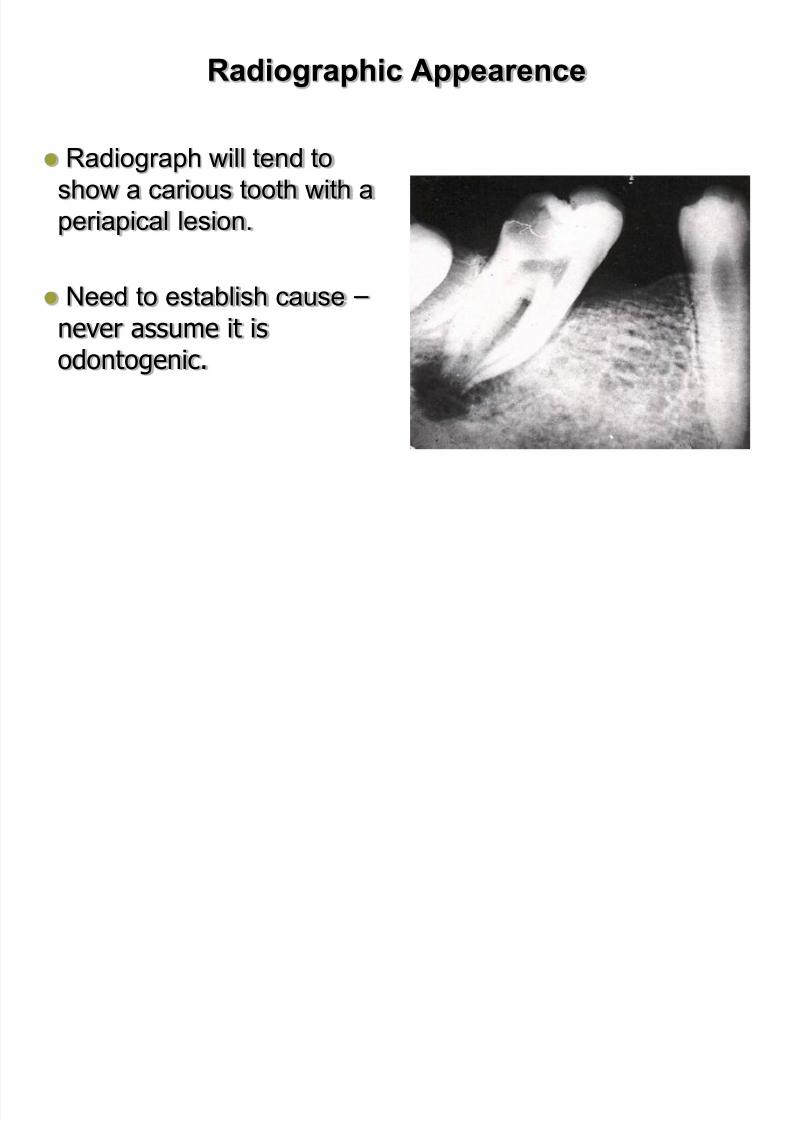
Radiographic Appearence
Radiograph will tend to
show a carious tooth with a
periapical lesion.
Need to establish cause –
never assume it isodontogenic.

8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 15/183
Fracture of facial bone
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 16/183
Injury to hard & soft tissue
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 17/183
Impacted teeth
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 18/183
Pericoronitis

8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 19/183
Stomatitis Gingivitis
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 20/183
● General factors :
Infection of maxilla , zygomatic bone or sinus:
- Osteomyelitis
- radicular cyst
- infection of salivary glands or lymph node
- O R L diseases
Cellulitis manemeraK EdlPaKeRcInCaBBYk Aerobic
bacteria
CaBiessBBYk streptococci .
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 21/183
Infected cysts
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 22/183
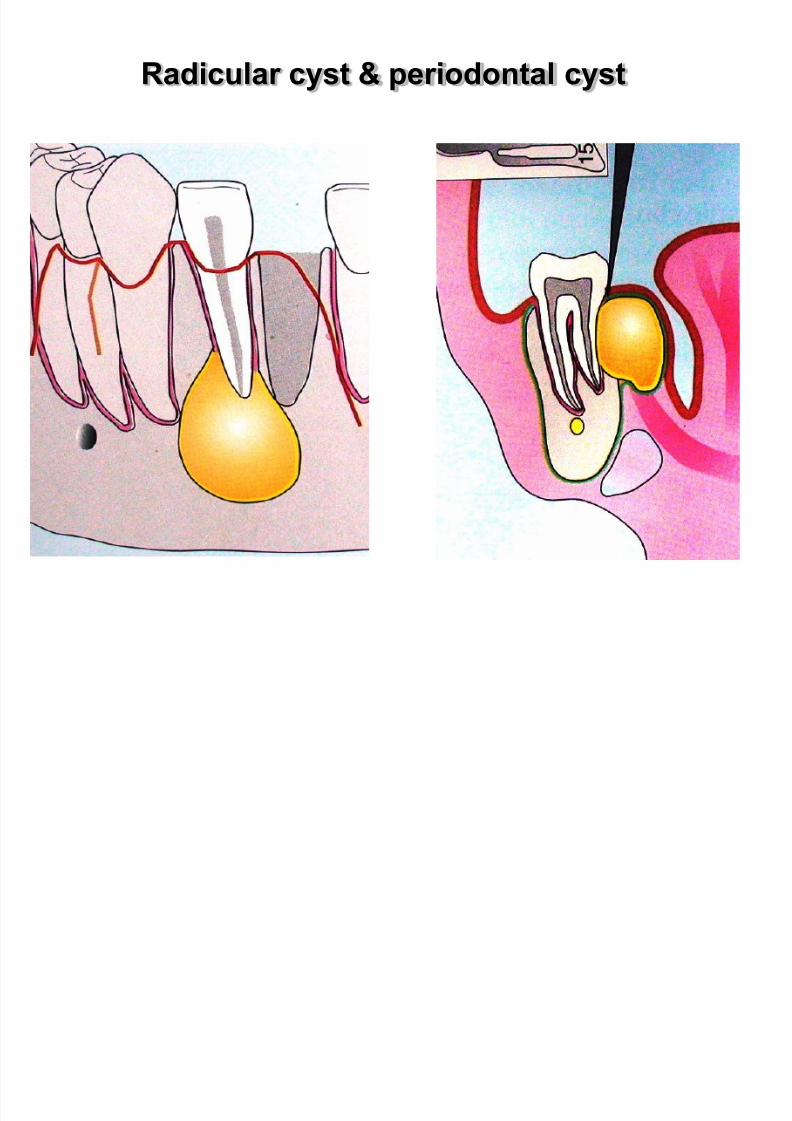
Radicular cyst & periodontal cyst
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 23/183
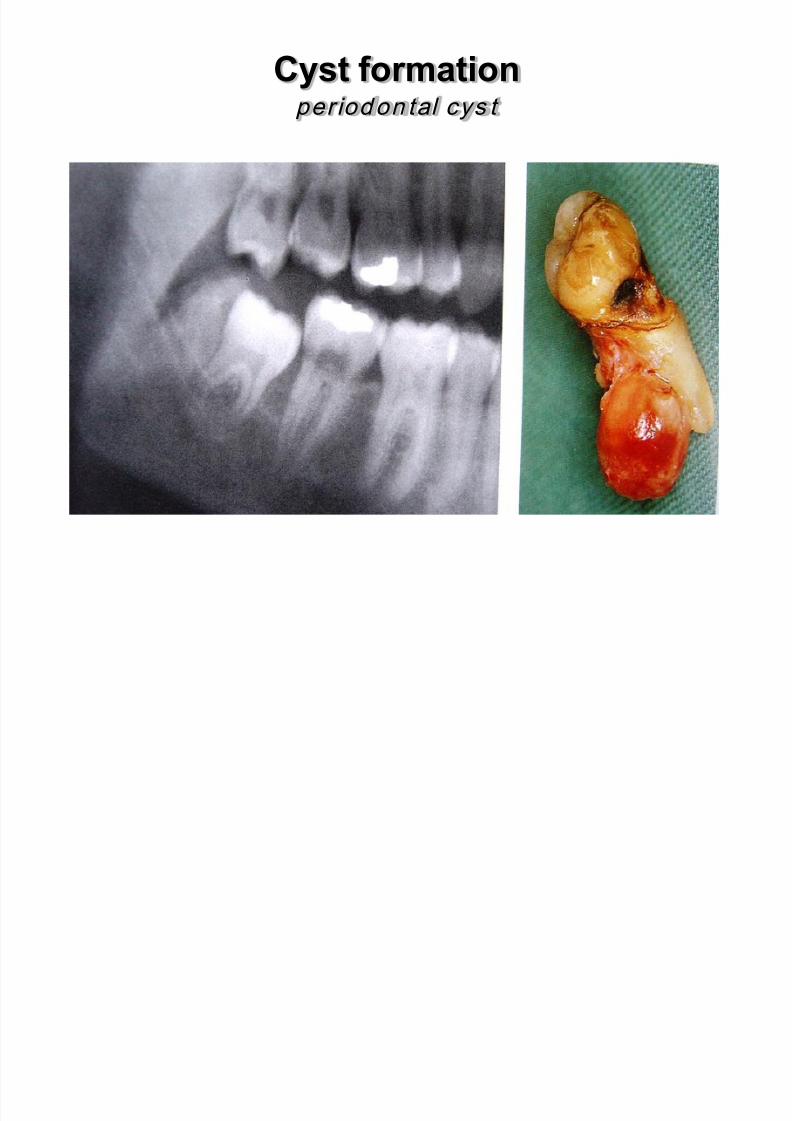
Cyst formation per iodon tal cys t
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 24/183
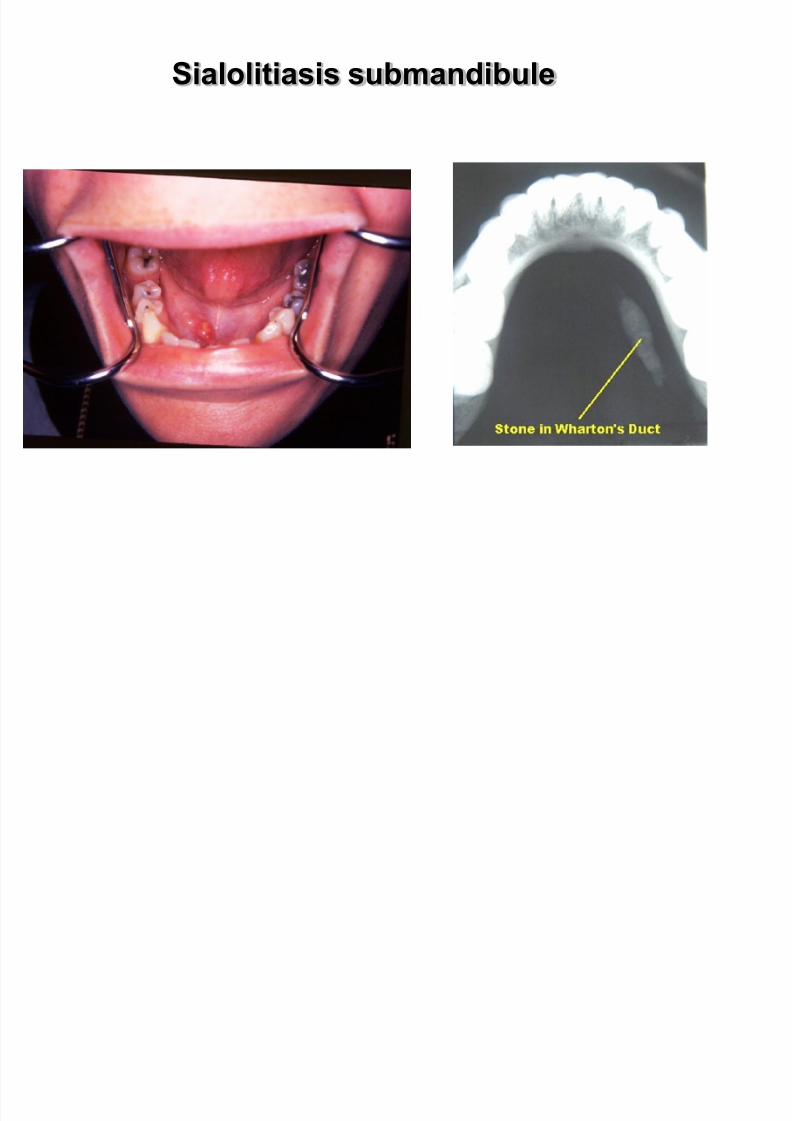
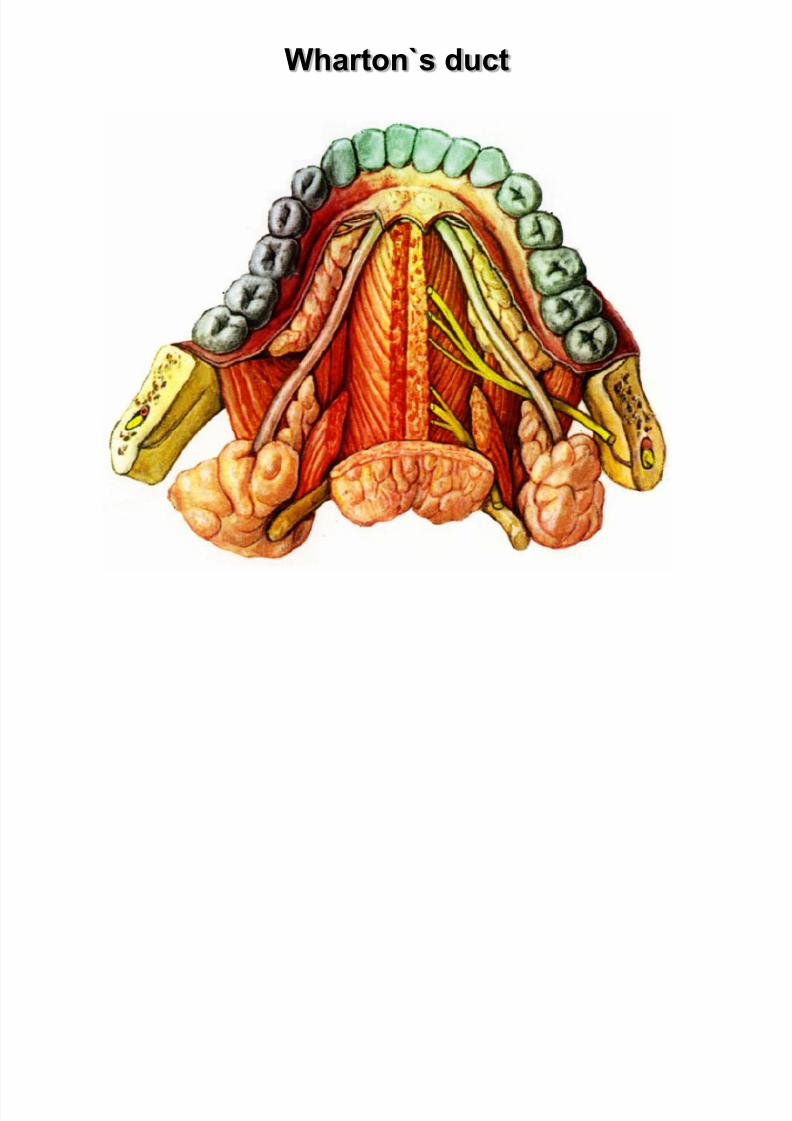
Sialolitiasis submandibule
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 25/183
Wharton`s duct
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 26/183
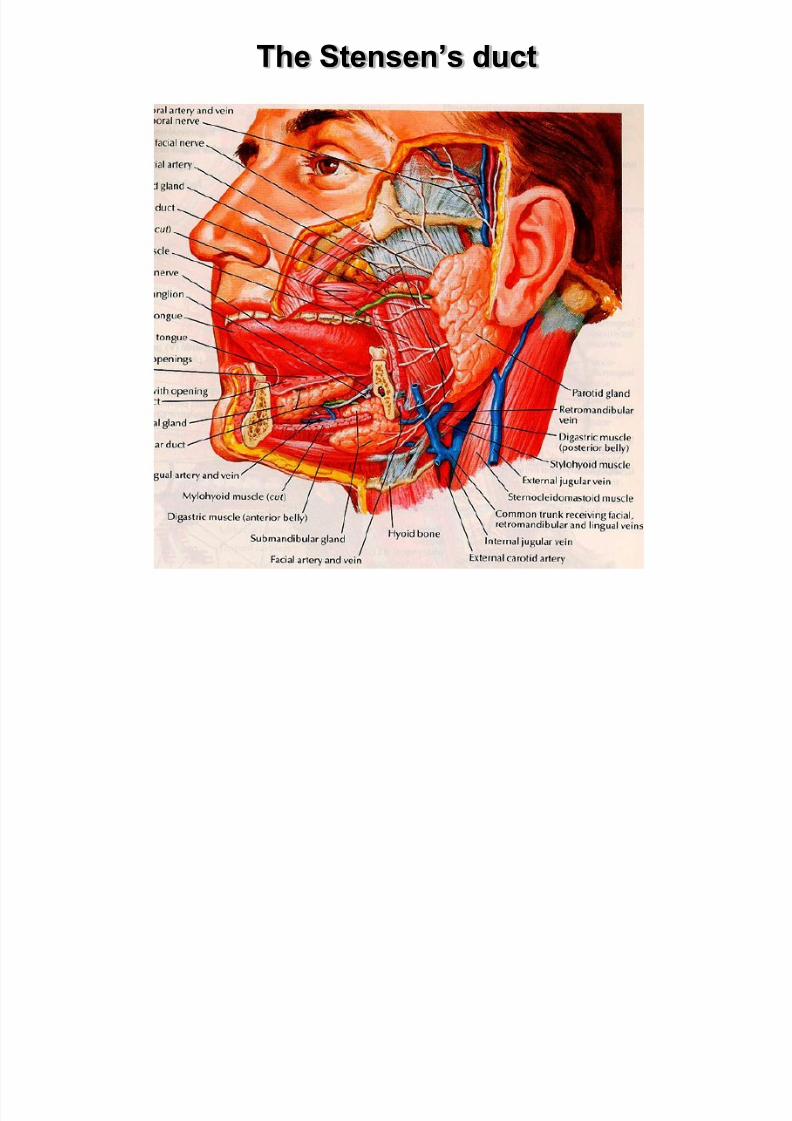
The Stensen’s duct
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 27/183
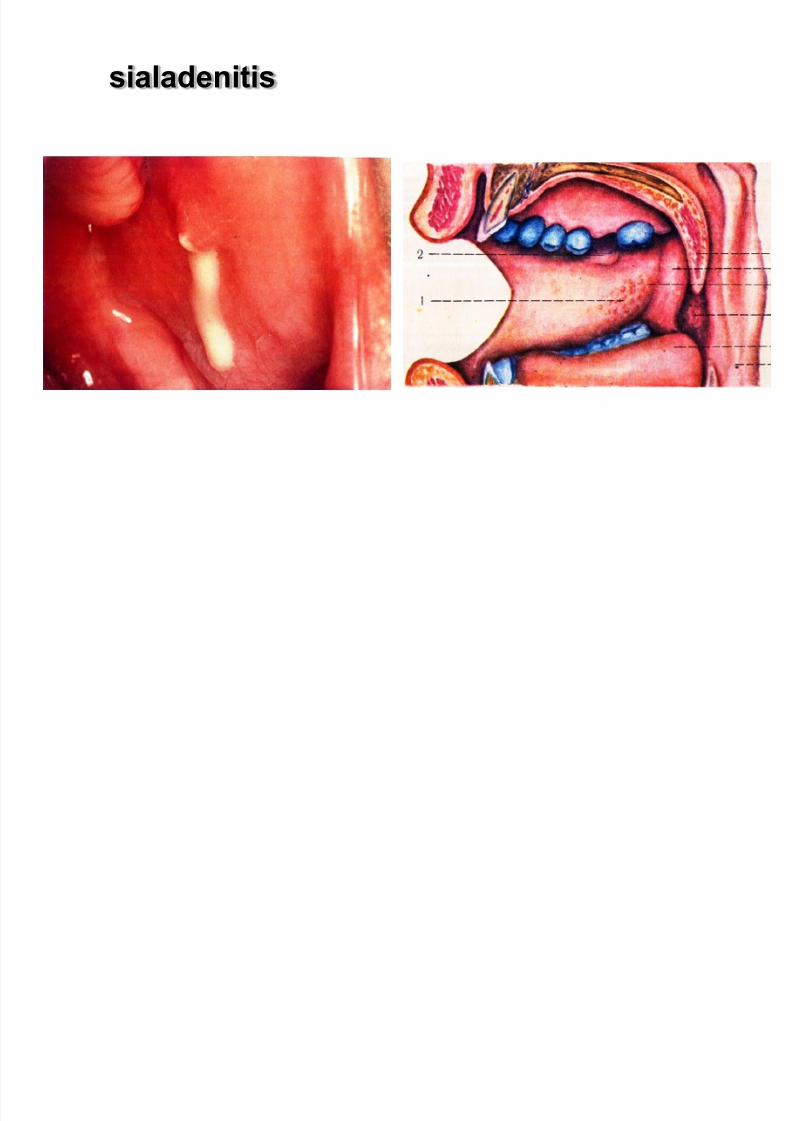
sialadenitis

8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 28/183
Lymph node
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 29/183
MICROBIOLOGY OF ODONTOGENIC INFECTIONS
Usually caused by endogenous bacteria Aerobic bacteria alone rarely causative agents
Streptococcus species are usually the etiologic organisms if
aerobic bacteria present
Half odontogenic infections: anaerobes Most odontogenic infections due to mixed flora
Mixed infections may have 5-10 organisms present
Bacterial composition :
1. 5%-aerobic bacteria
2. 60%-anaerobic bacteria
3. 35% mixed aerobic and anaerobic bacteria
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 30/183
Local symptoms
Pain.The severity of the pain depends on the stage of development of the inflammation.In the initial phase thepain is dull and continous and worsens duringpercussion of the responsible tooth and when it comesinto contact with antagonist teeth
Edema.Edema appears intraorally or extraorally and itusually has a buccal localization and more rarely palatalor lingual.
Usually the edema is soft with redness of the skin.
Other symptoms.There is a sense elongation of theresponsible tooth,slight mobility and difficulty inswollowing.

8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 31/183
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 32/183
Systemic symptoms
fever ( to 39 –40 °C )
chill
malaise with pain in muscles and joints
anorexia, insomnia, nausea, and vomiting
Complications :
trismus, lymphadenitis at the respective lymph nodes
osteomyelitis
bacteremia,
septicemia.
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 33/183
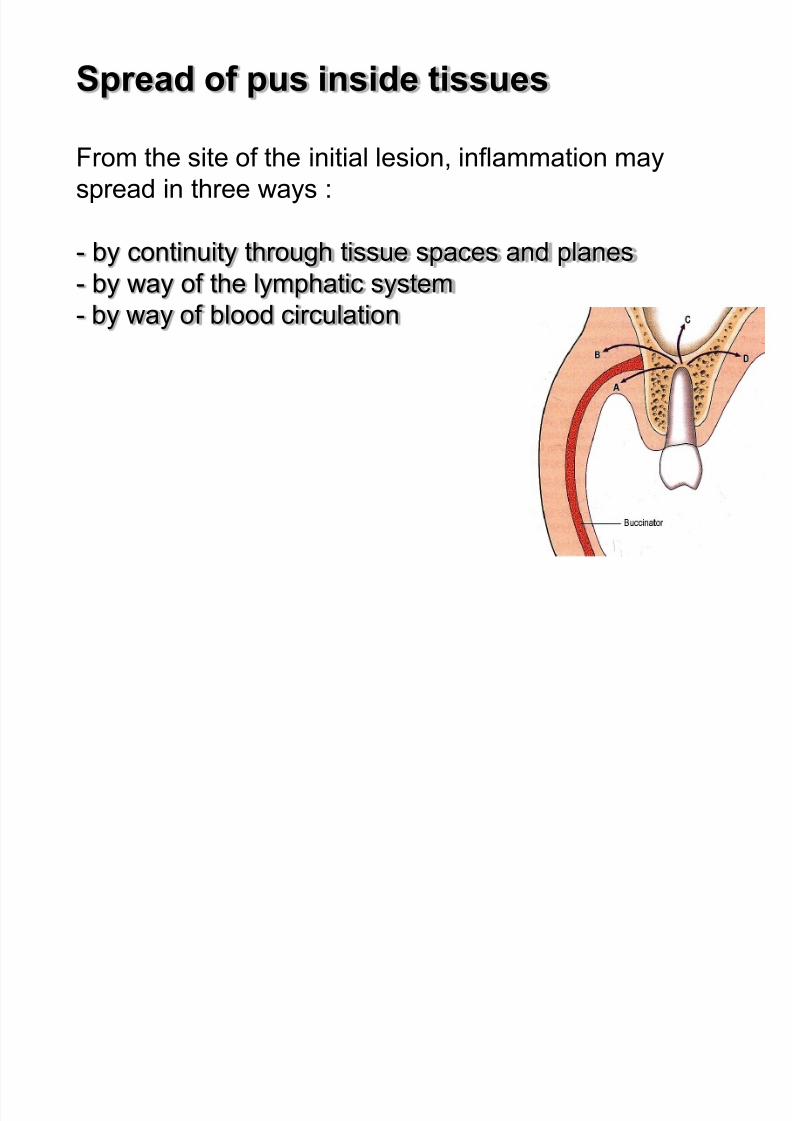
Spread of pus inside tissues
From the site of the initial lesion, inflammation may
spread in three ways :
- by continuity through tissue spaces and planes
- by way of the lymphatic system- by way of blood circulation
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 34/183
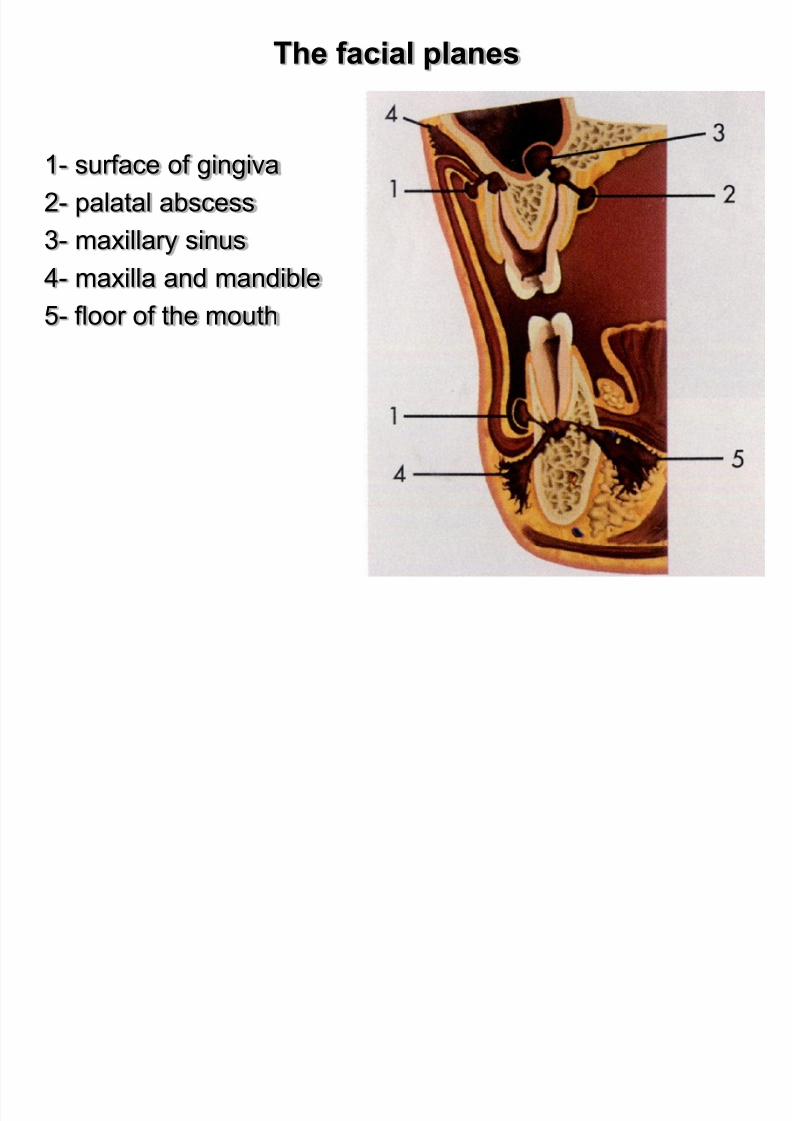
The facial planes
1- surface of gingiva
2- palatal abscess
3- maxillary sinus
4- maxilla and mandible5- floor of the mouth
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 35/183
Fascial Spaces
Fascial planes offer anatomic highways for infection tospread superficial to deep planes
Antibiotic availability in fascial spaces is limited due topoor vascularity
Treatment of fascial space infections depends on I and D
Fascial spaces are contiguous and infection readilyspreads from one space to another (open primary and
secondary spaces)
Despite I and D the etiologic agent (tooth) must beremoved
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 36/183
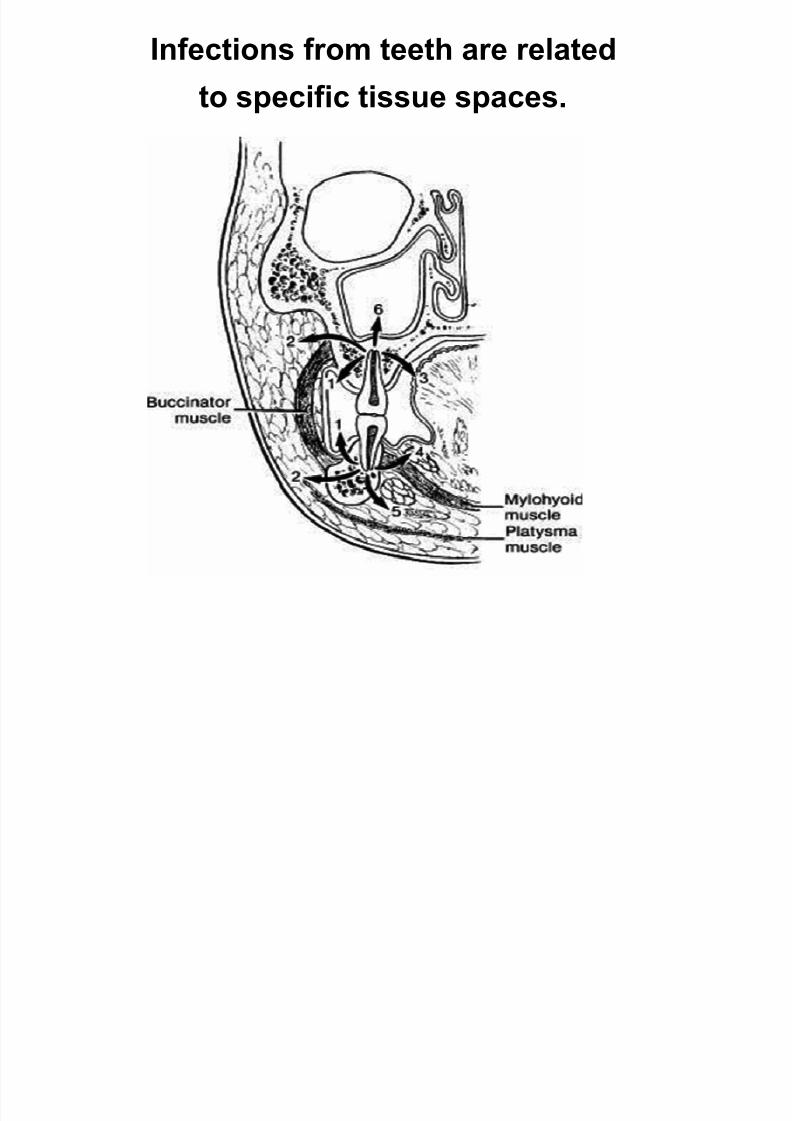
Infections from teeth are related
to specific tissue spaces.
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 37/183
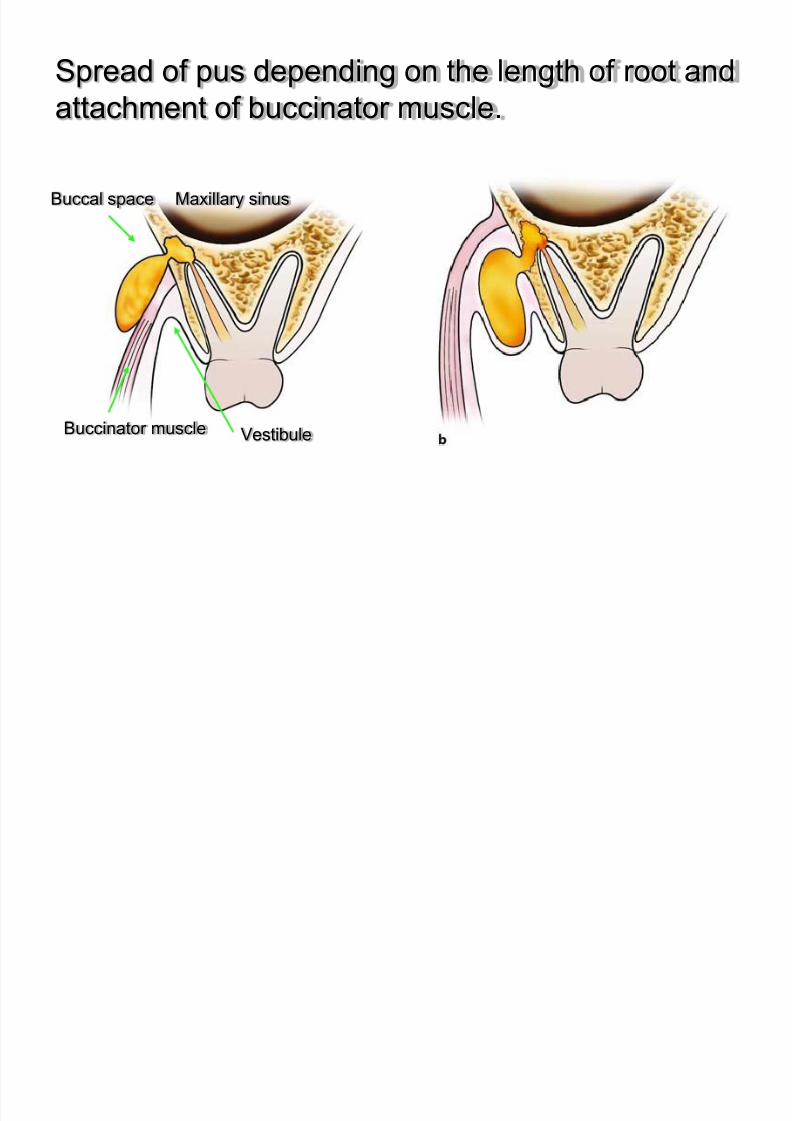
Spread of pus depending on the length of root and
attachment of buccinator muscle.
Buccal space
Buccinator muscle
Maxillary sinus
Vestibule
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 38/183
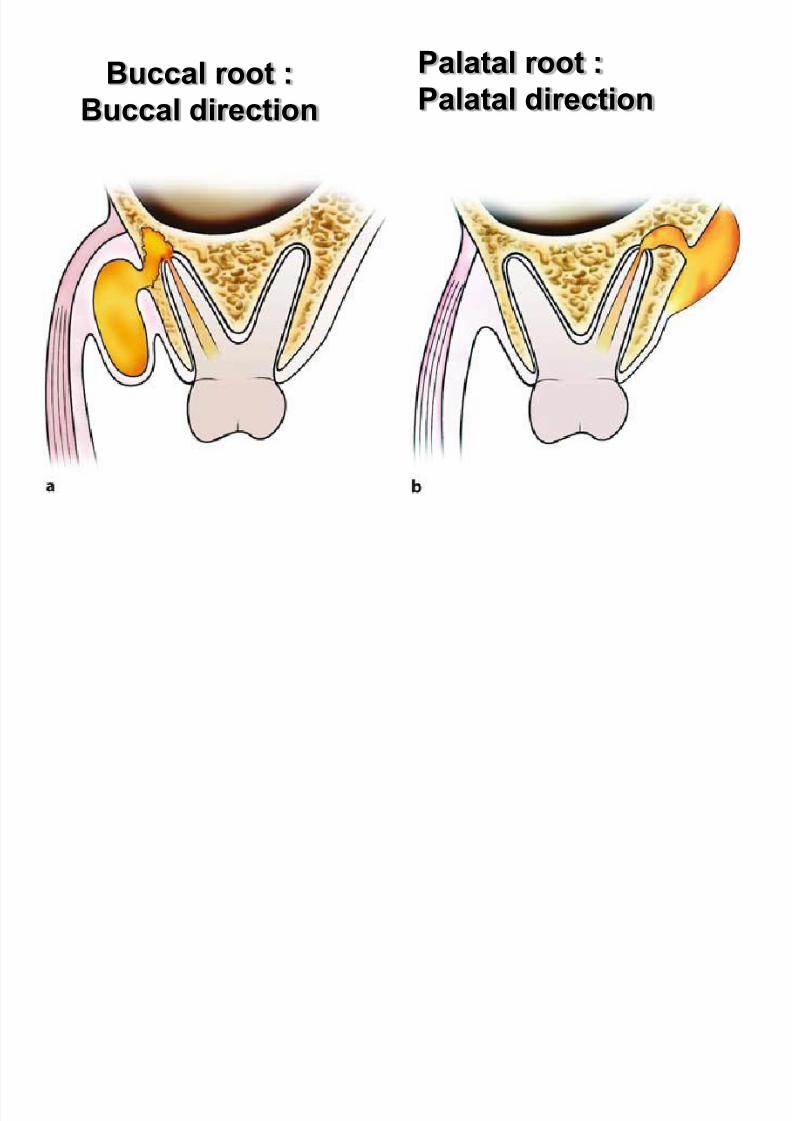
Buccal root :
Buccal direction
Palatal root :
Palatal direction
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 39/183
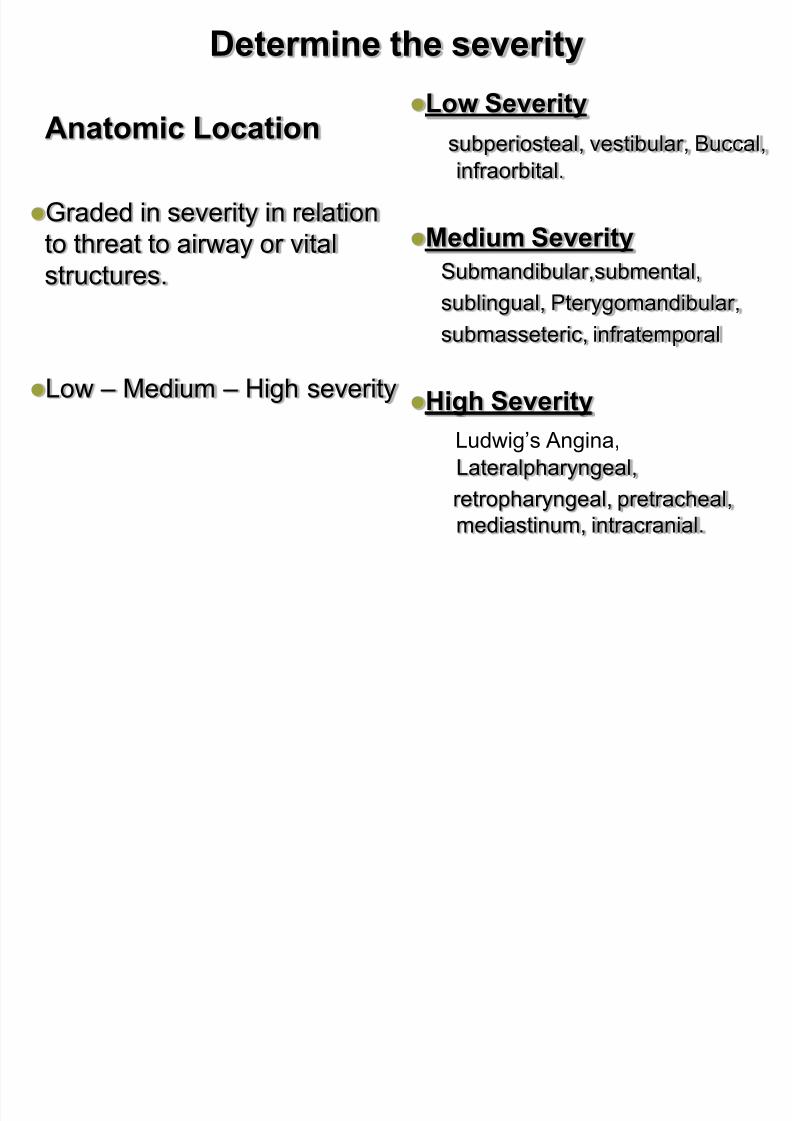
Determine the severity
Anatomic Location
Graded in severity in relation
to threat to airway or vital
structures.
Low – Medium – High severity
Low Severity
subperiosteal, vestibular, Buccal,infraorbital.
Medium Severity
Submandibular,submental,sublingual, Pterygomandibular,
submasseteric, infratemporal
High Severity
Ludwig’s Angina,
Lateralpharyngeal,
retropharyngeal, pretracheal,
mediastinum, intracranial.
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 40/183
I- Low Severity
Abscess of base of upper lip
Subperiosteal abscess
Vestibular abscess
Intraalveolar abscess of maxilla& mandible Infraorbital ascess
Buccal abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 41/183
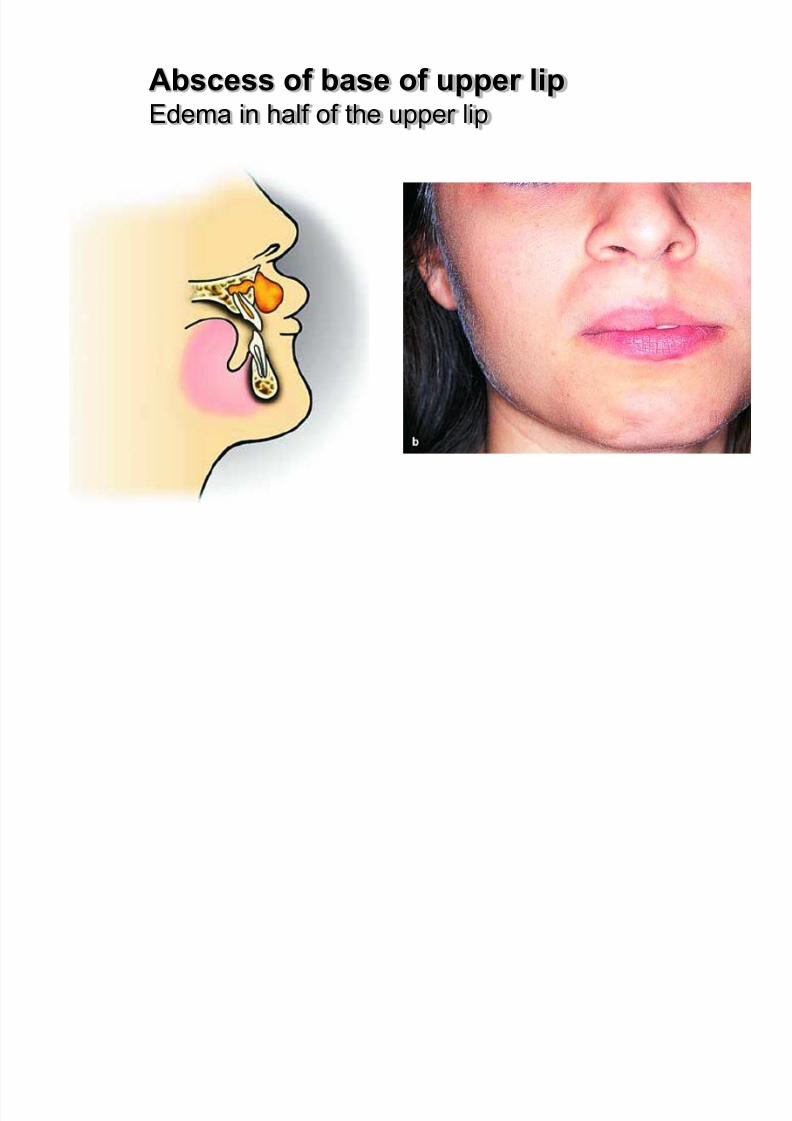
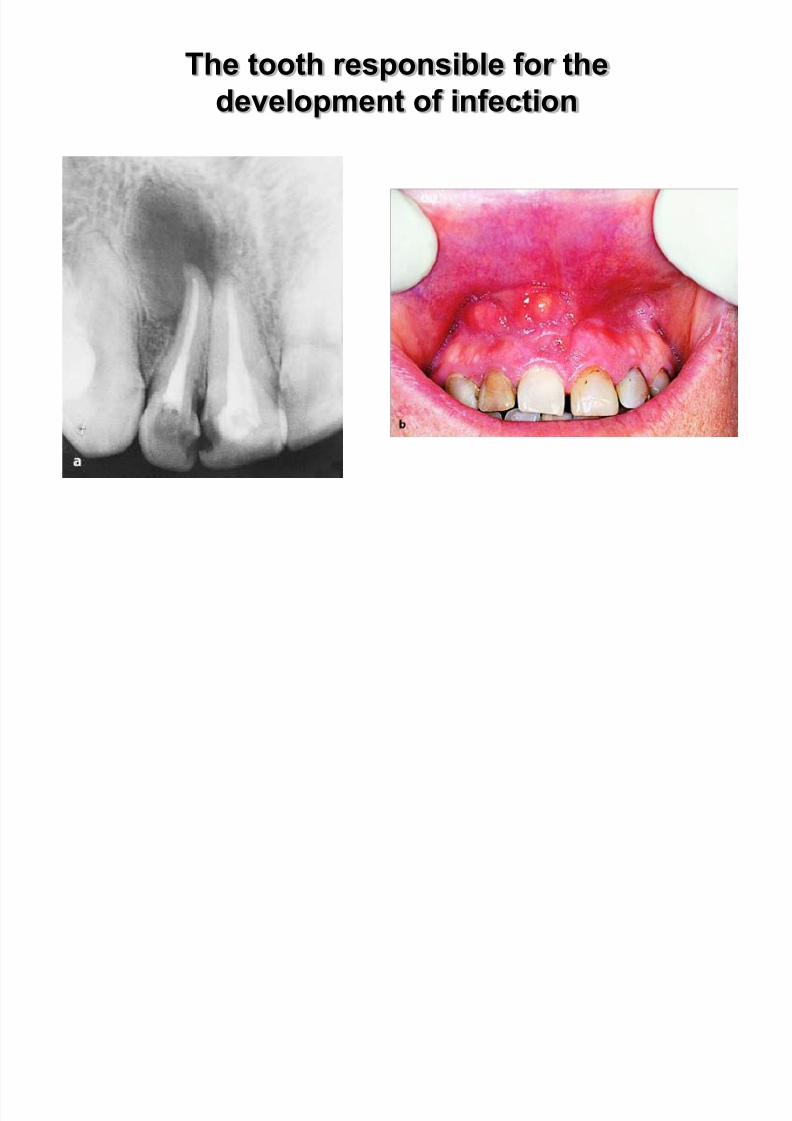
a-Abscess of base of upper lip
This abscess develops the loose connective tissue of thebase of the upper lip at the anterior region of the maxilla,
beneath the pearshaped aperture.
Etiology :It is usually caused by infected root canals of maxillary
anterior teeth.
Clinical :- the swelling and protrusion of the upper lip
- obliteration of the depth of the mucolabial fold
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 42/183
Abscess of base of upper lipEdema in half of the upper lip
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 43/183
The tooth responsible for the
development of infection
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 44/183
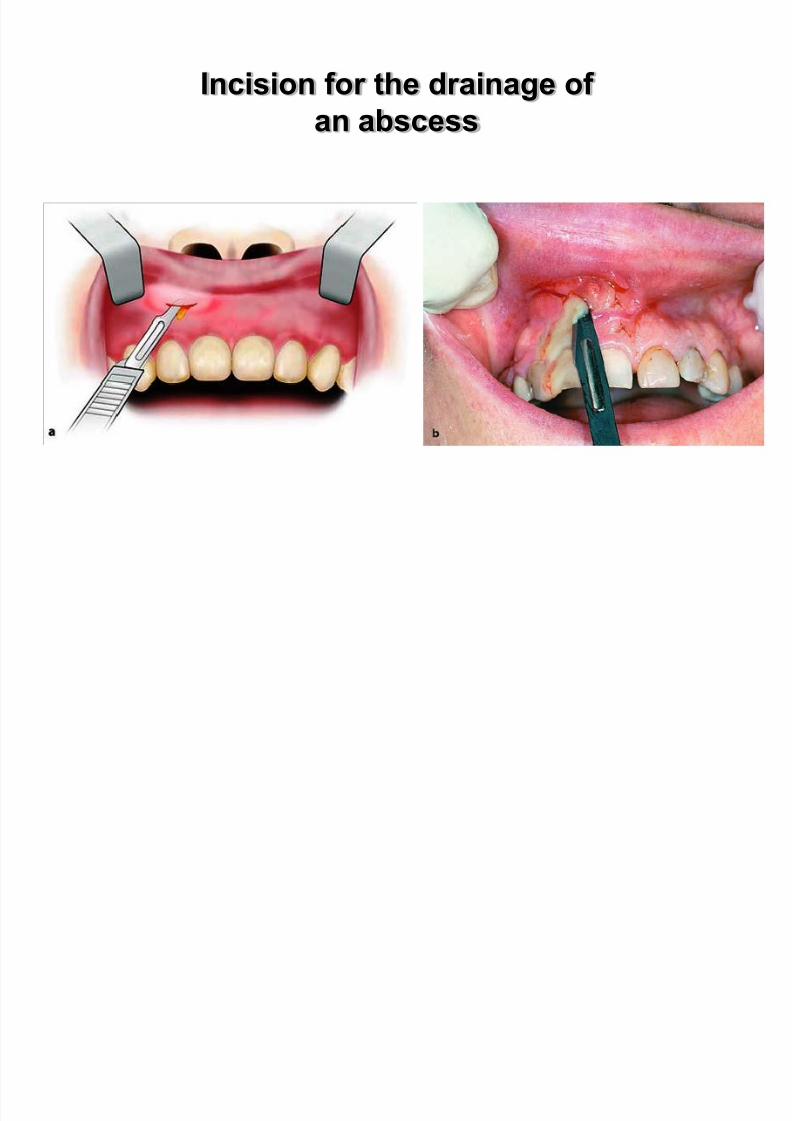
Incision for the drainage of
an abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 45/183
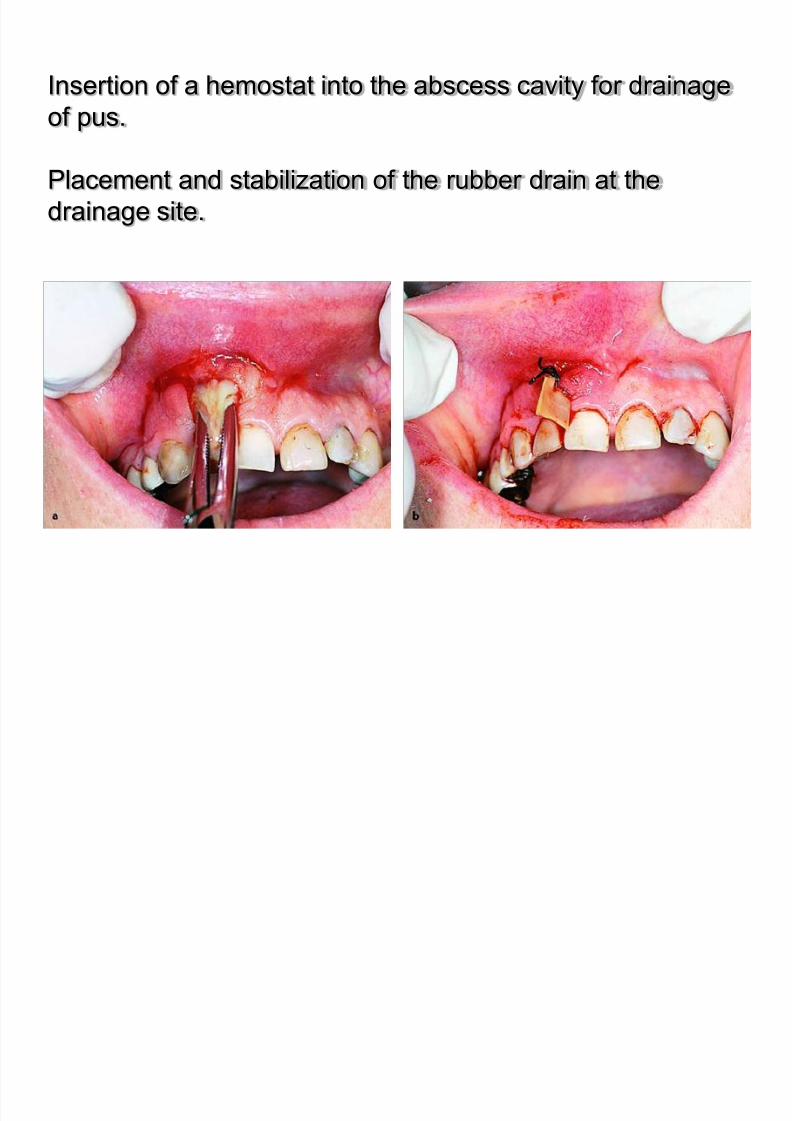
Insertion of a hemostat into the abscess cavity for drainage
of pus.
Placement and stabilization of the rubber drain at the
drainage site.
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 46/183
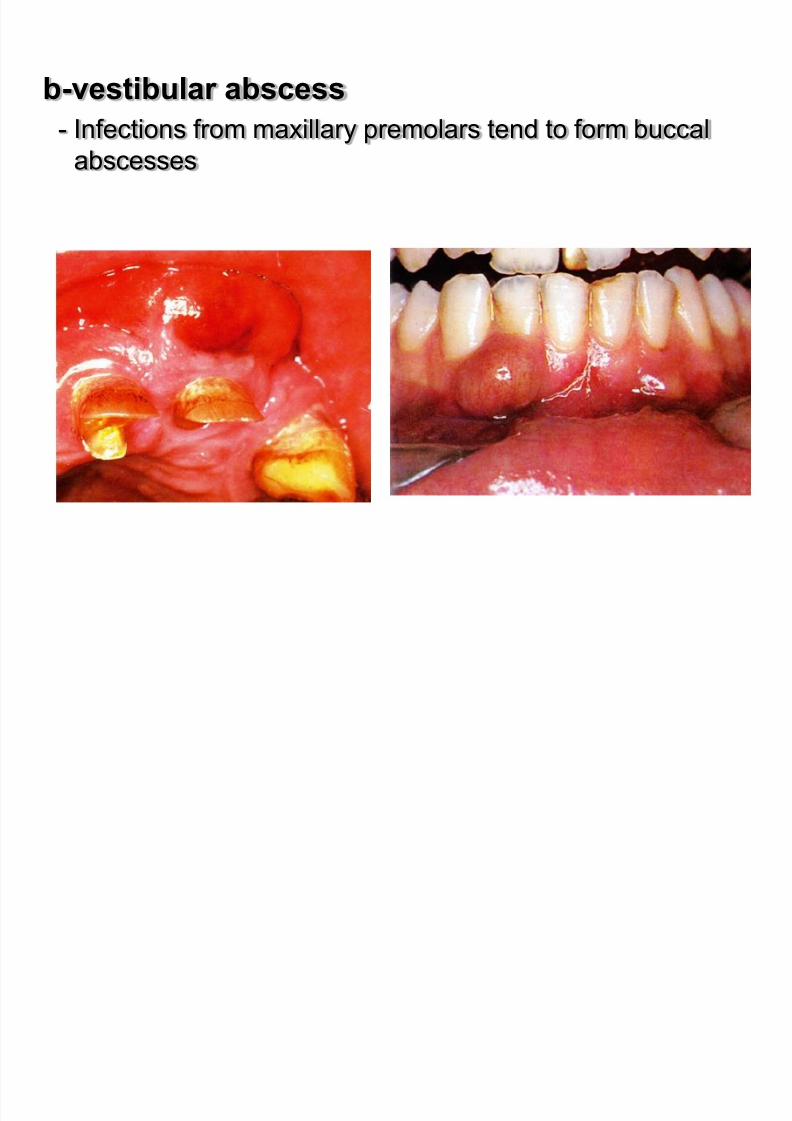
b-vestibular abscess
- Infections from maxillary premolars tend to form buccal
abscesses
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 47/183
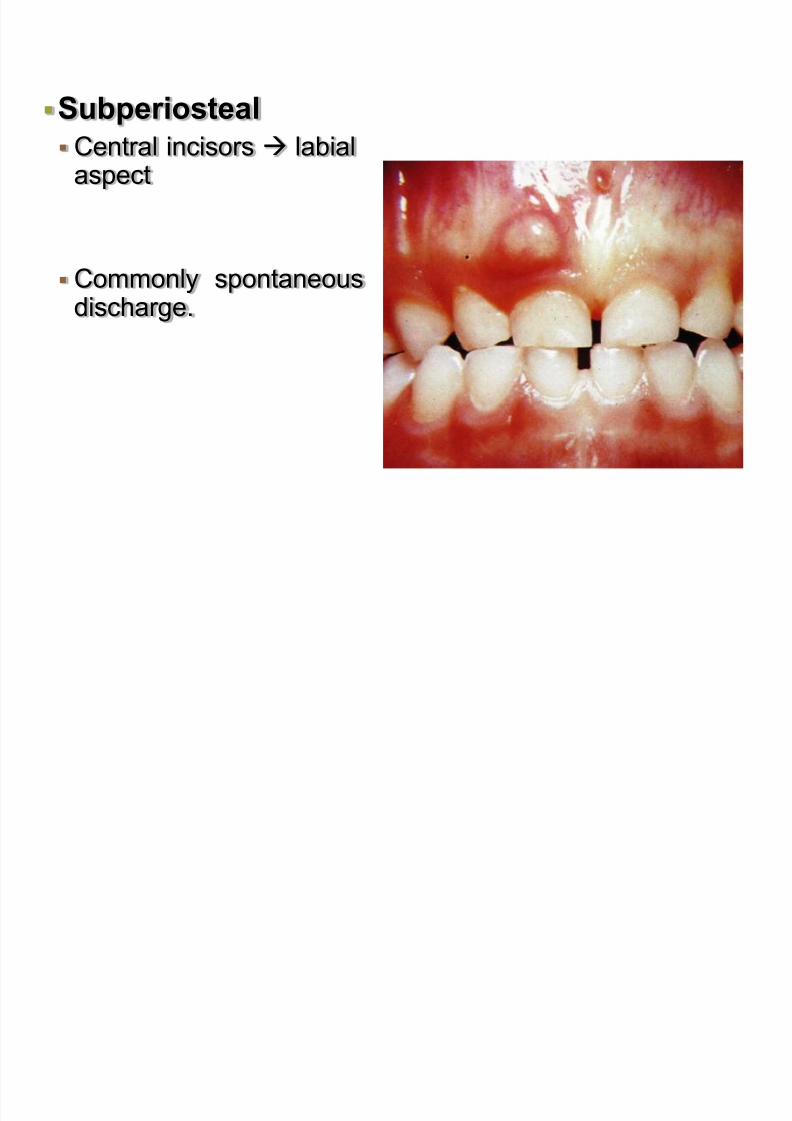
Subperiosteal
Central incisors labialaspect
Commonly spontaneousdischarge.

8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 48/183
Subperiosteal abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 49/183
Subperiosteal abscess
The subperiosteal abscess involves limitedaccumulation of pus that is semi-fluctuant.
It is located between bone and the periosteum,at
the buccal,palatal,or lingual region,relative to the
tooth responsible for the infection.
Clinical :
- Mild edema
- severe pain due to tension of the periosteum- sensitivity during palpation
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 50/183
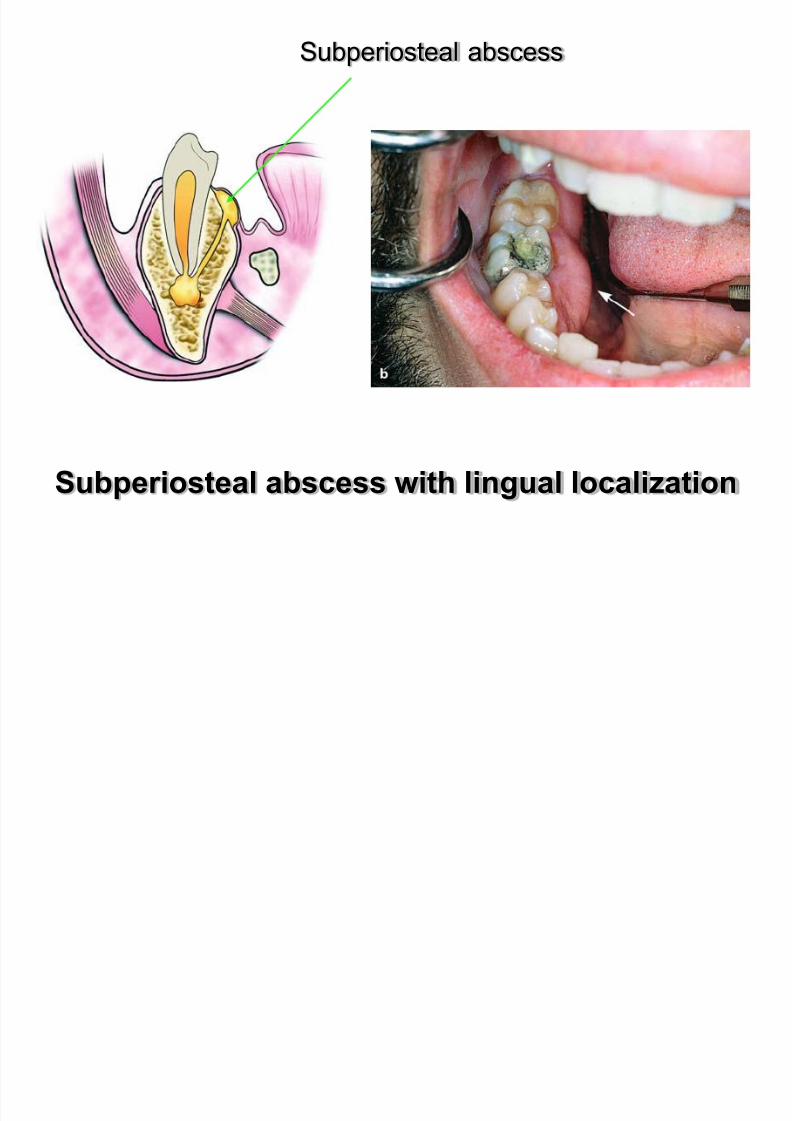
Subperiosteal abscess with lingual localization
Subperiosteal abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 51/183
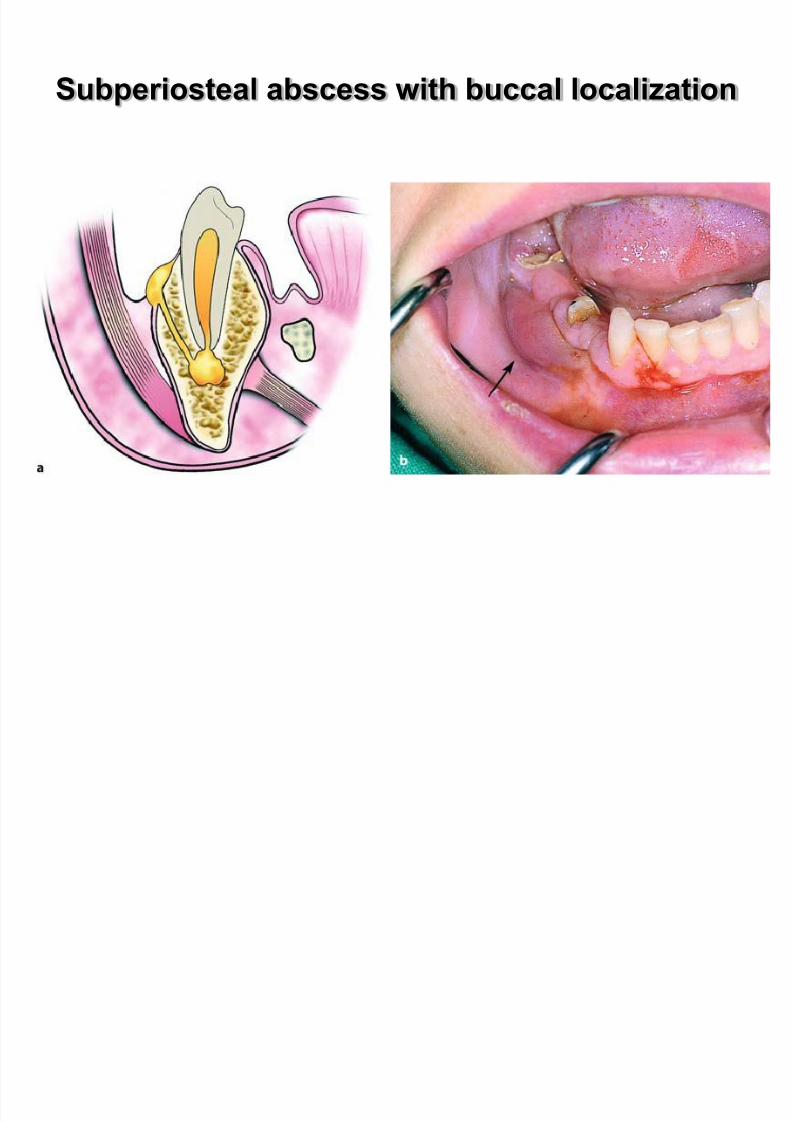
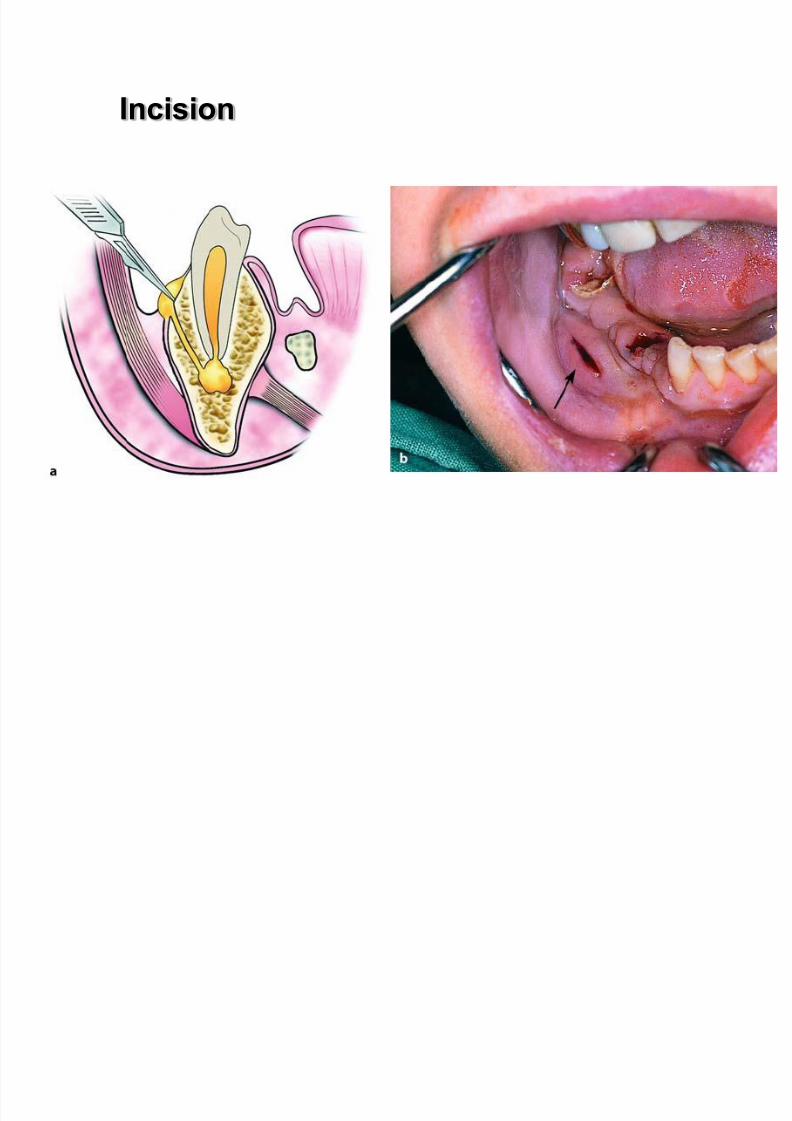
Subperiosteal abscess with buccal localization
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 52/183
Incision
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 53/183
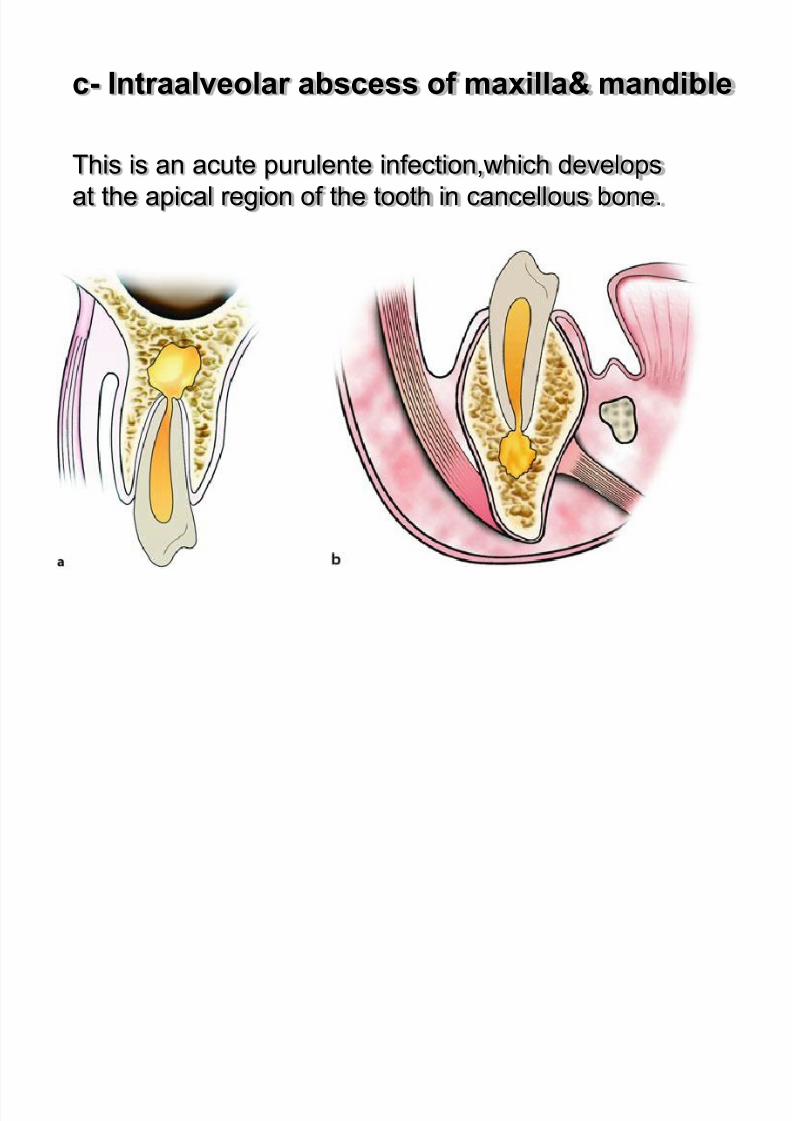
c- Intraalveolar abscess of maxilla& mandible
This is an acute purulente infection,which develops
at the apical region of the tooth in cancellous bone.
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 54/183
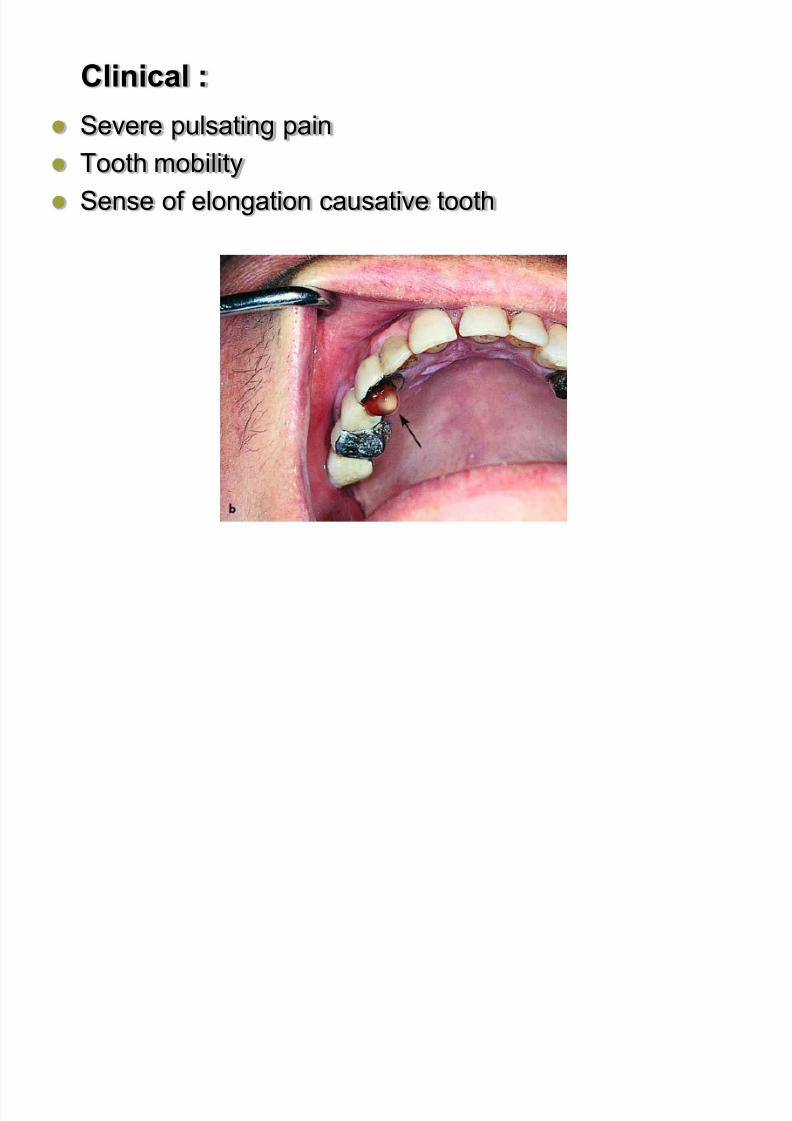
Clinical :
Severe pulsating pain
Tooth mobility
Sense of elongation causative tooth
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 55/183
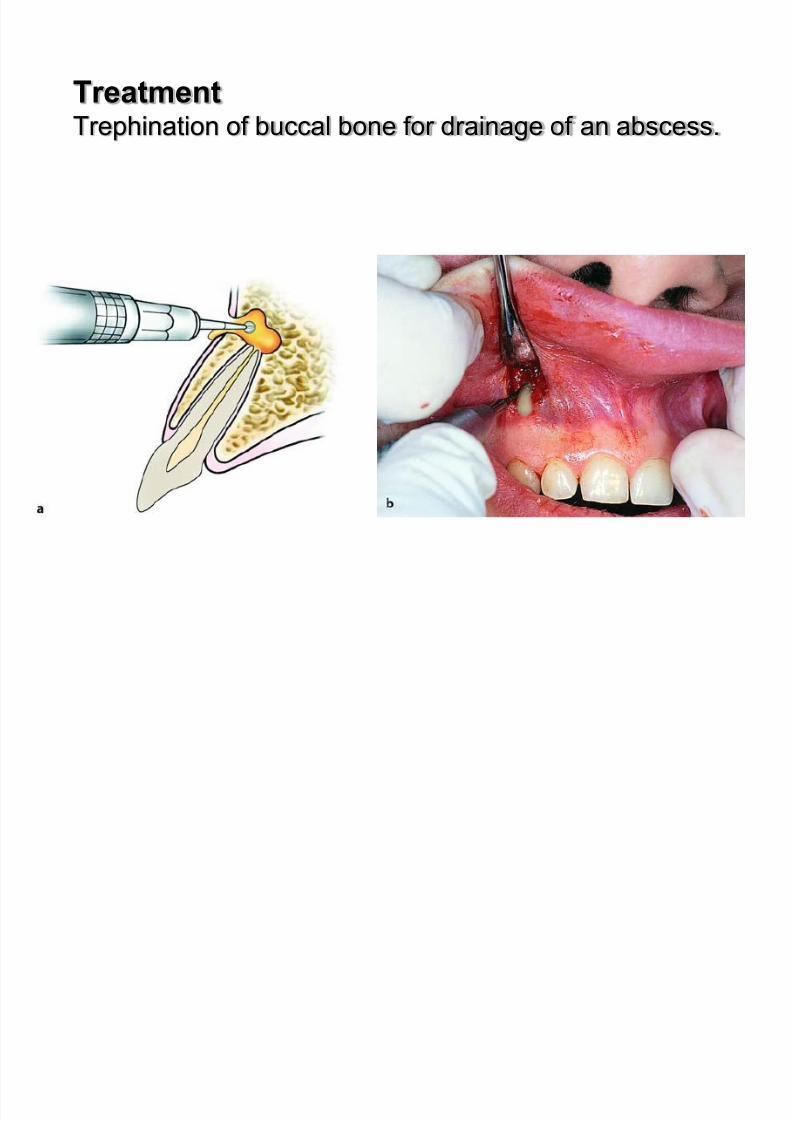
TreatmentTrephination of buccal bone for drainage of an abscess.
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 56/183
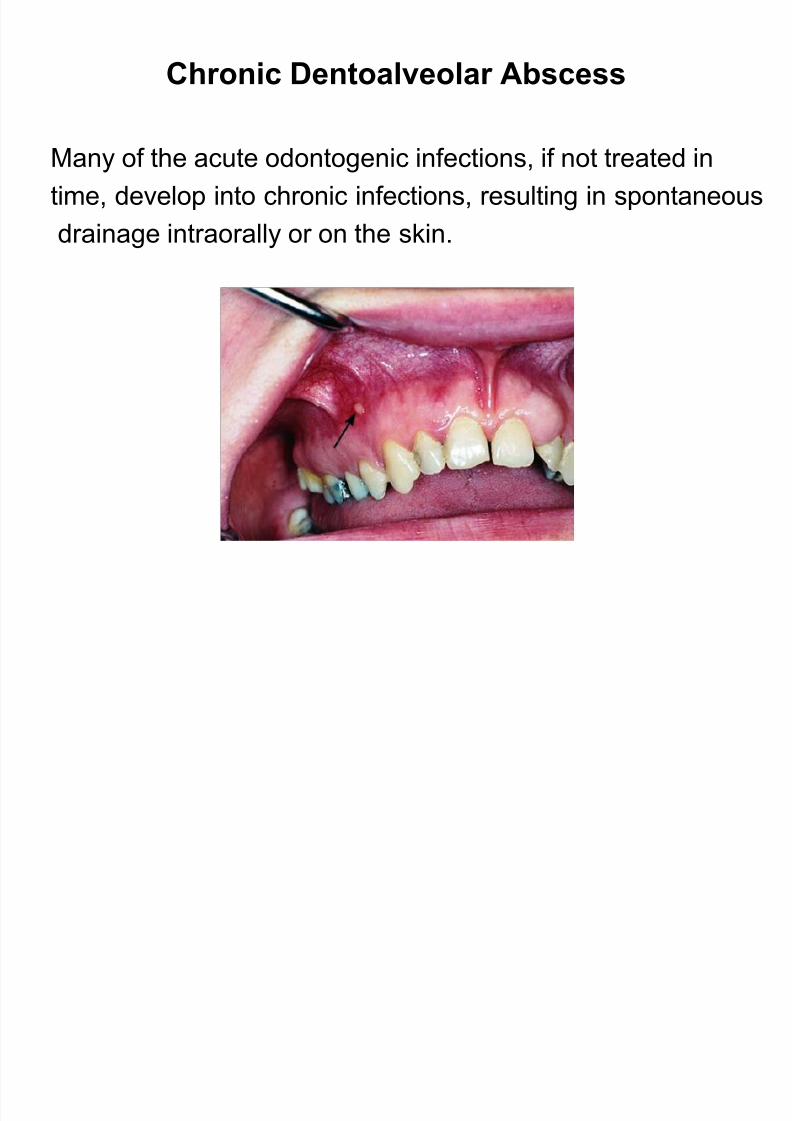
Chronic Dentoalveolar Abscess
Many of the acute odontogenic infections, if not treated in
time, develop into chronic infections, resulting in spontaneous
drainage intraorally or on the skin.

8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 57/183
Chronic dentoalveolar abscess with drainage, through a
fistula, at the buccal mucosa of the mandible and at the
mucosa of the palate
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 58/183
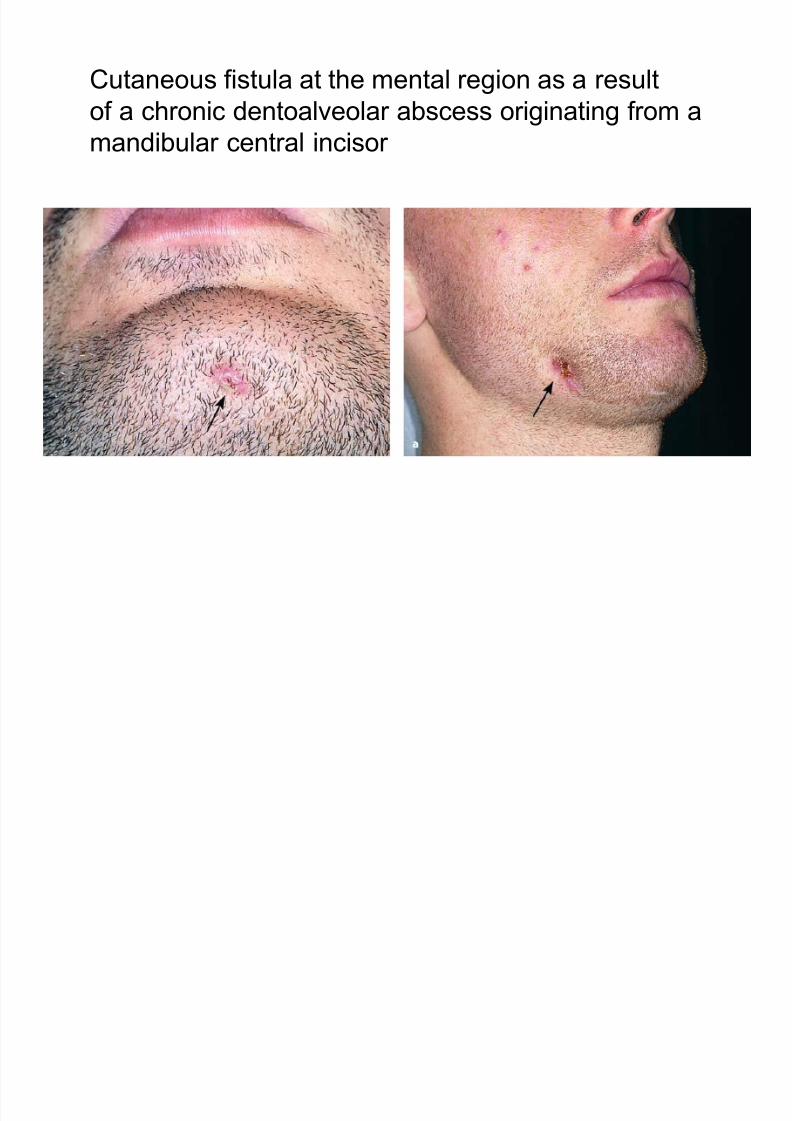
Cutaneous fistula at the mental region as a result
of a chronic dentoalveolar abscess originating from a
mandibular central incisor
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 59/183
Treatment
Treatment consists of eliminating the infection from the
responsible tooth with endodontic therapy or in conjunctionWith surgical treatment (apicoectomy),when endodontic therapy
alone does not produce the desired results.
Usually in intraoral fistulas, the fistulous tract disappears a fewdays after endodontic therapy begins,without requiring
intervention for excision of the opening.
In extraoral fistulas, though, after treating the infected site, thefistulous tract must be excised as far as the bone cavity and,
after debridement,must be sutured tightly.
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 60/183
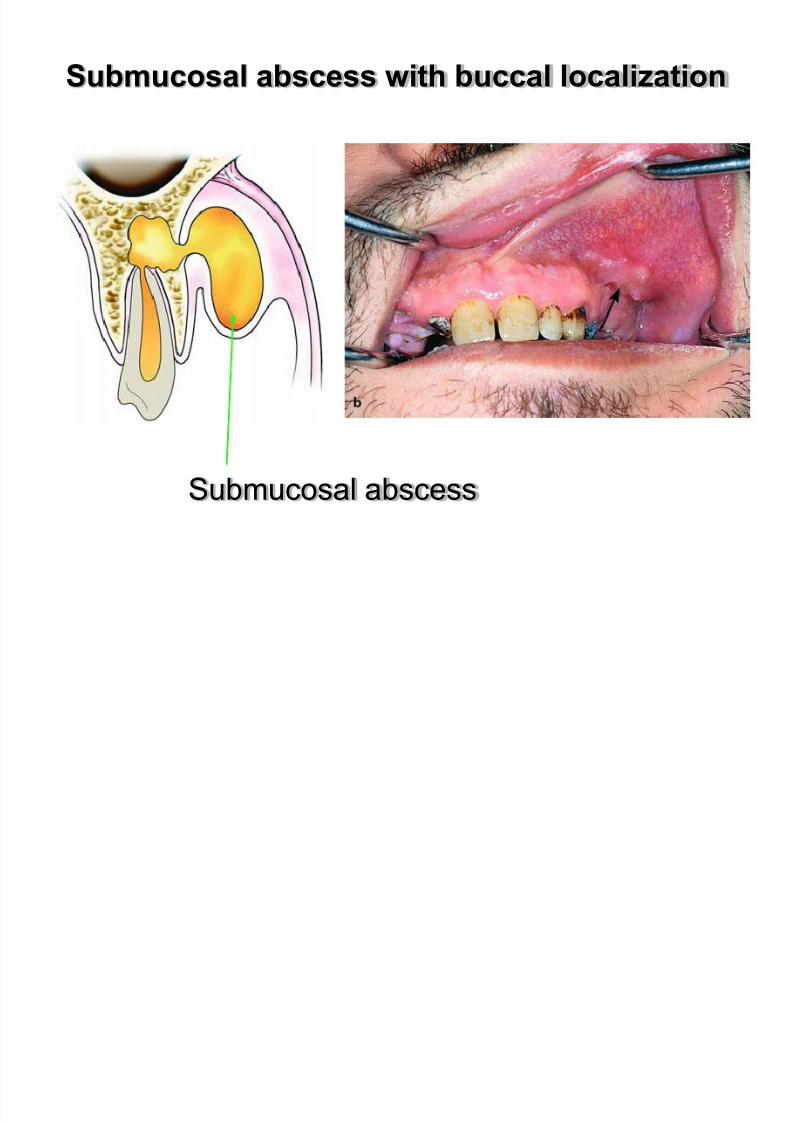
d-Submucosal abscess
Submucosal abscess is located exactly underneath the
buccal and labial vestibular mucosa of the maxilla or
mandible,as well as the palatal or lingual region,respective to
the tooth responsible for the infection.
Clinical :
- sweeling of the mucosa with obvious fluctuation
- the mucosa appears reddish
- obliteration of the mucobuccal fold in the area of infection
- sensitivity during palpation
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 61/183
Submucosal abscess with buccal localization
Submucosal abscess
b l b f h ill i h
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 62/183
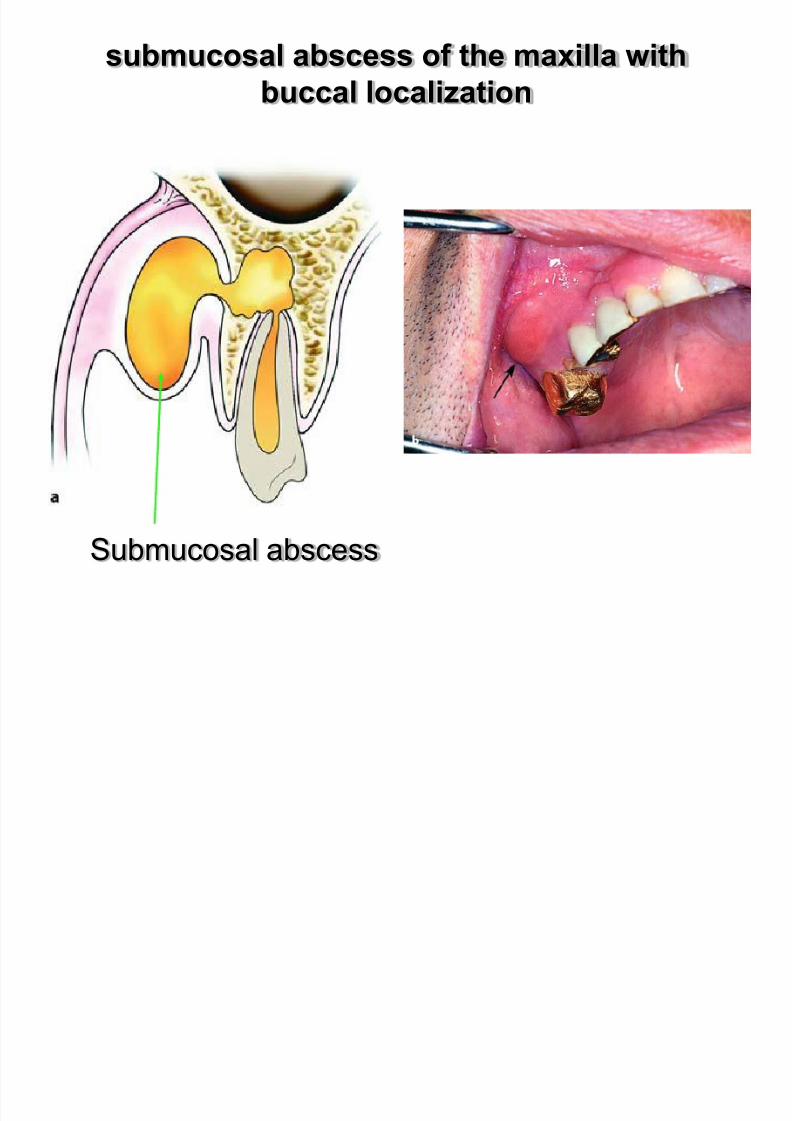
submucosal abscess of the maxilla with
buccal localization
Submucosal abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 63/183
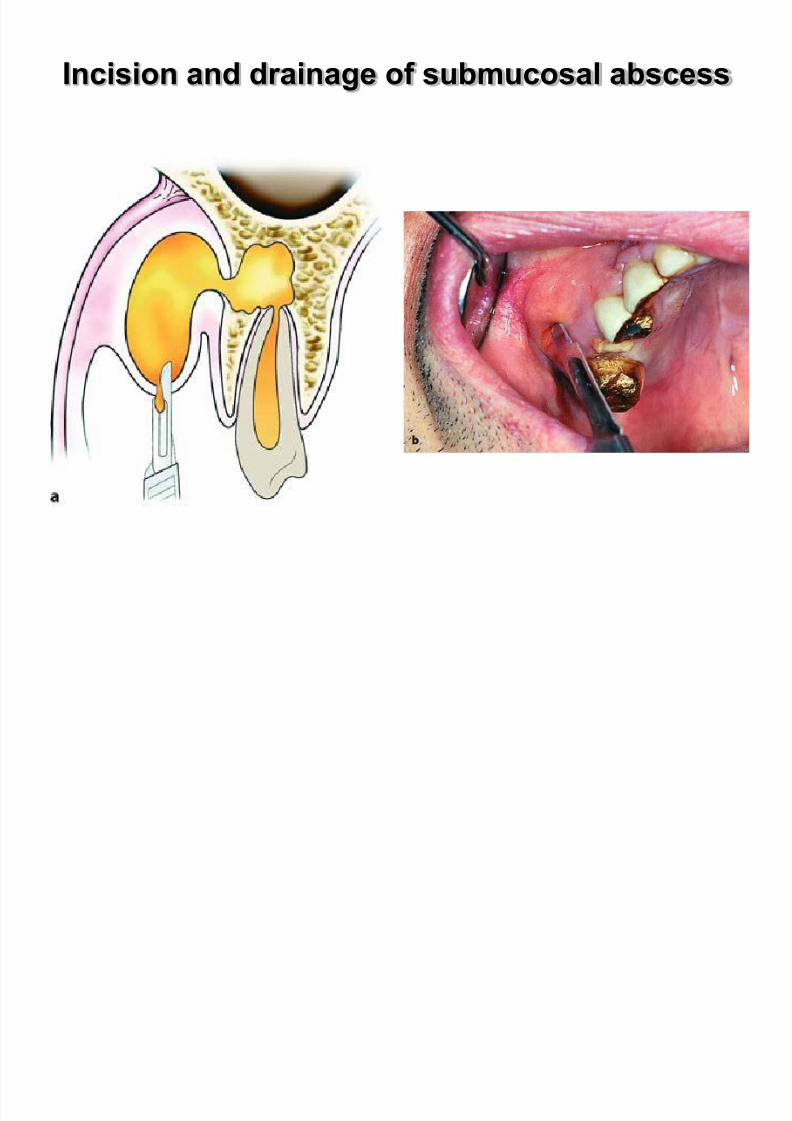
Incision and drainage of submucosal abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 64/183
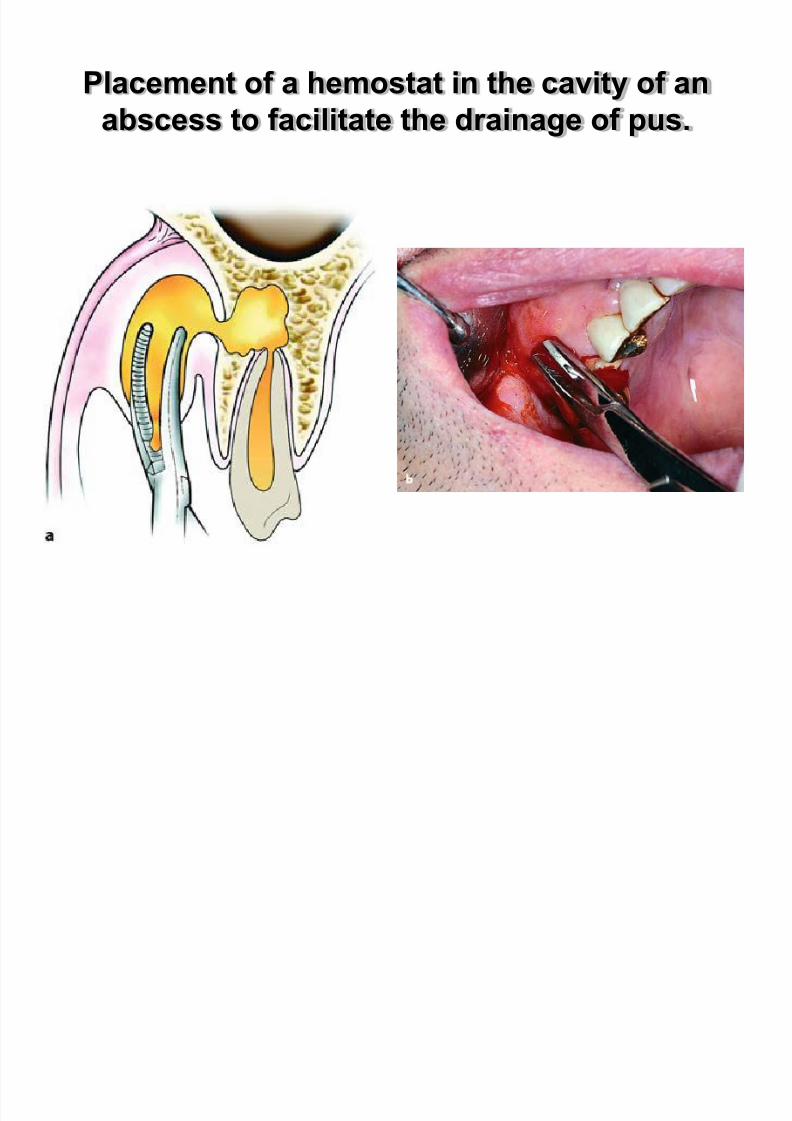
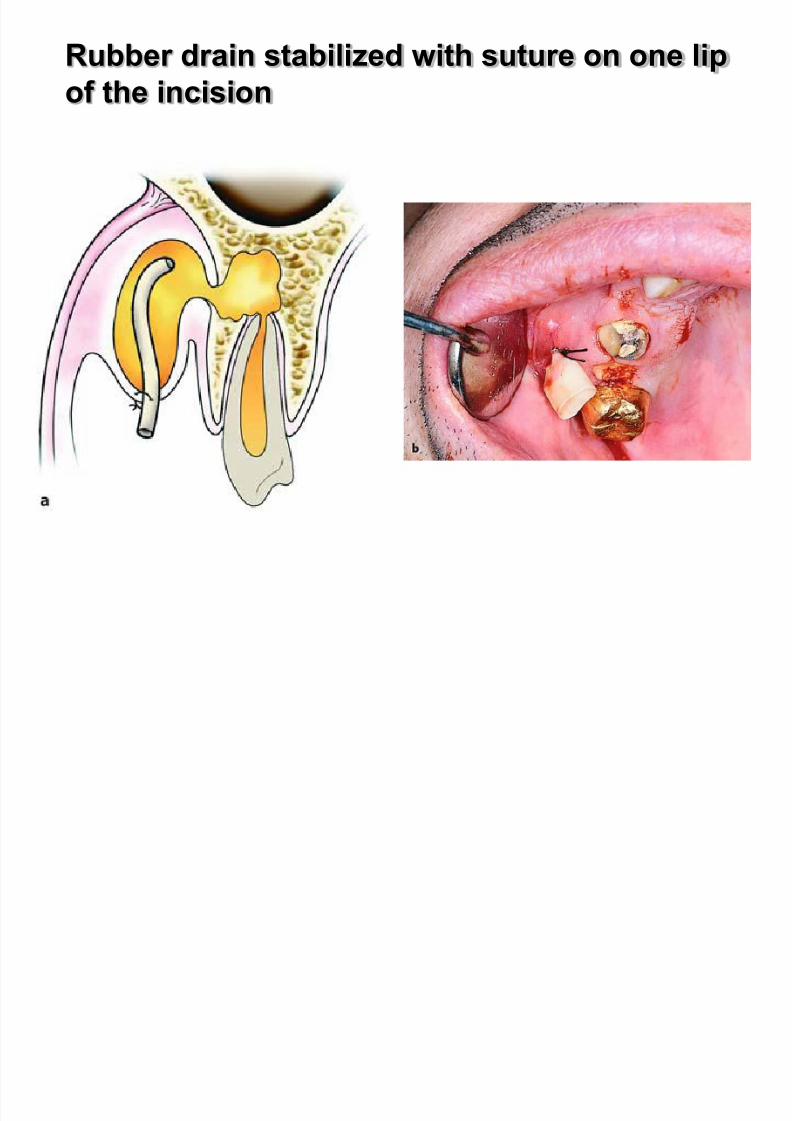
Placement of a hemostat in the cavity of an
abscess to facilitate the drainage of pus.
R bb d i t bili d ith t li
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 65/183
Rubber drain stabilized with suture on one lip
of the incision
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 66/183
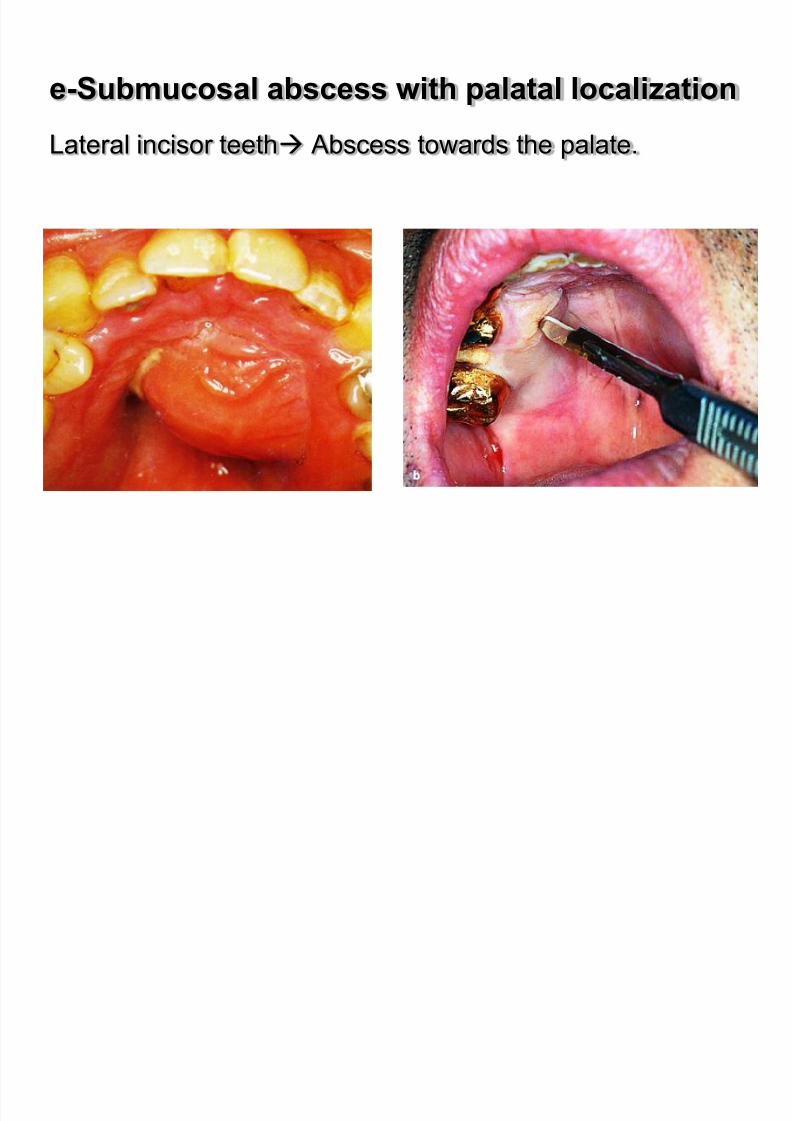
e-Submucosal abscess with palatal localization
Lateral incisor teeth Abscess towards the palate.
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 67/183
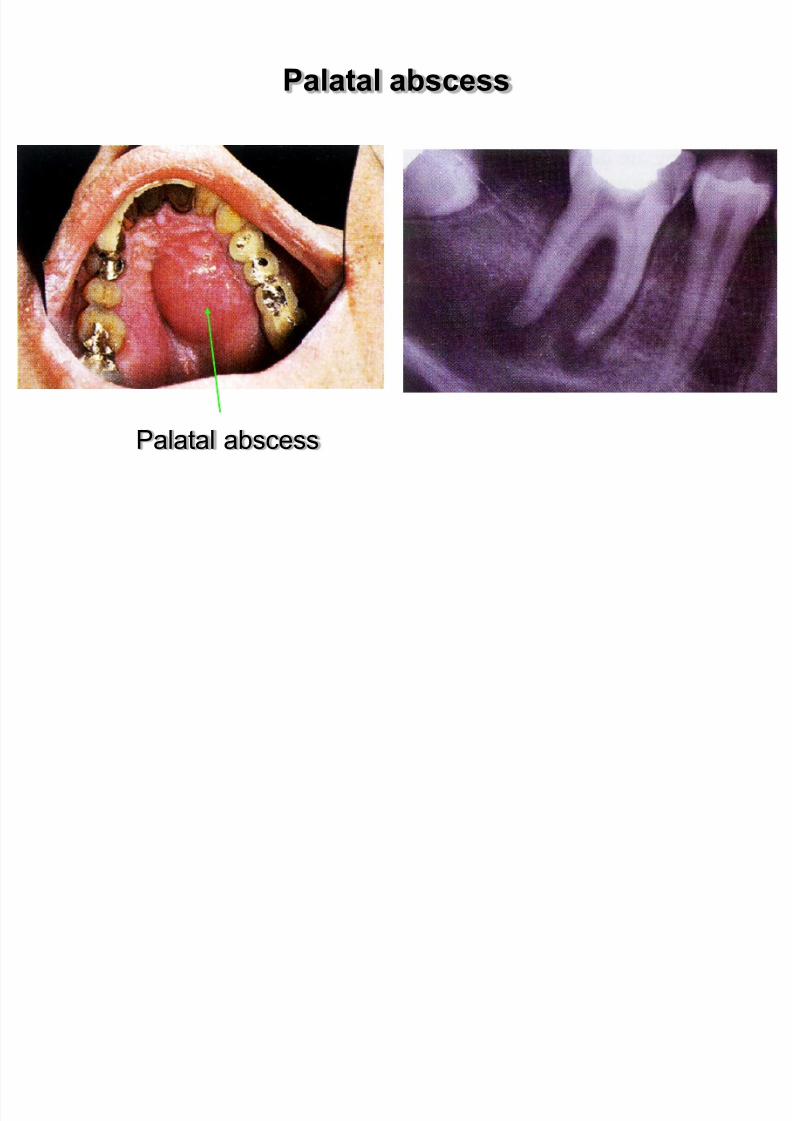
Palatal abscess
Palatal abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 68/183
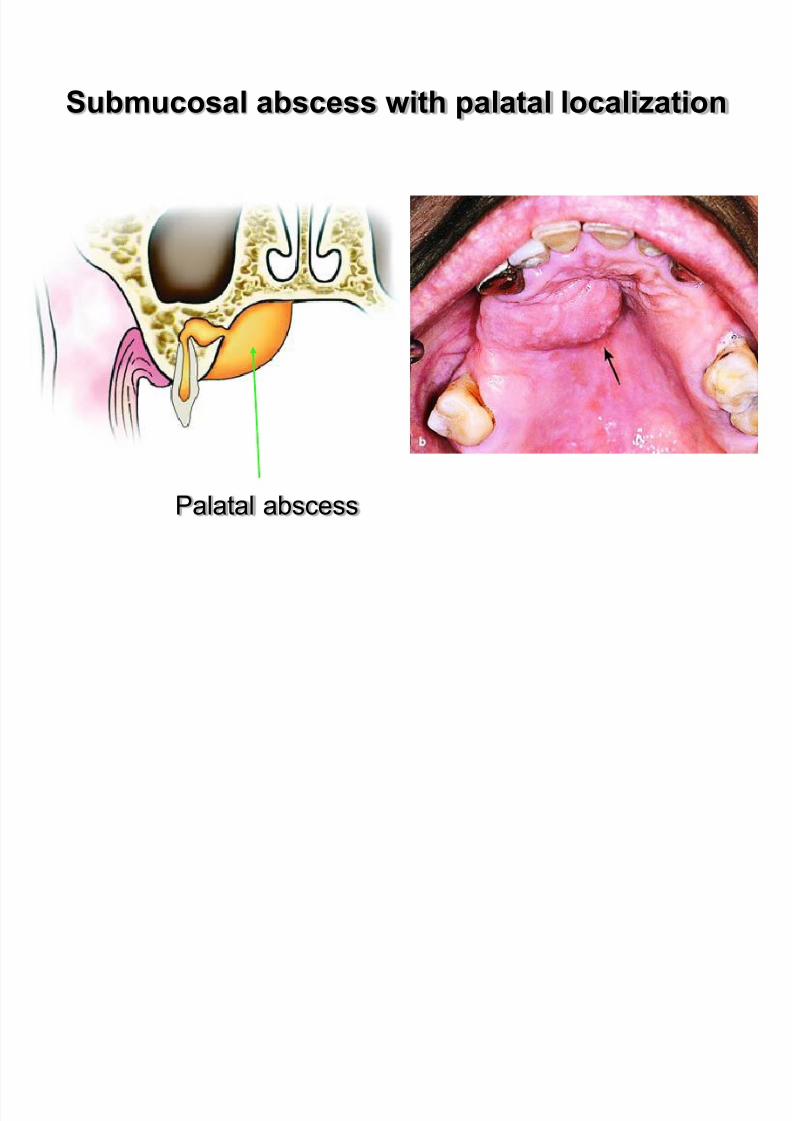
Submucosal abscess with palatal localization
Palatal abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 69/183
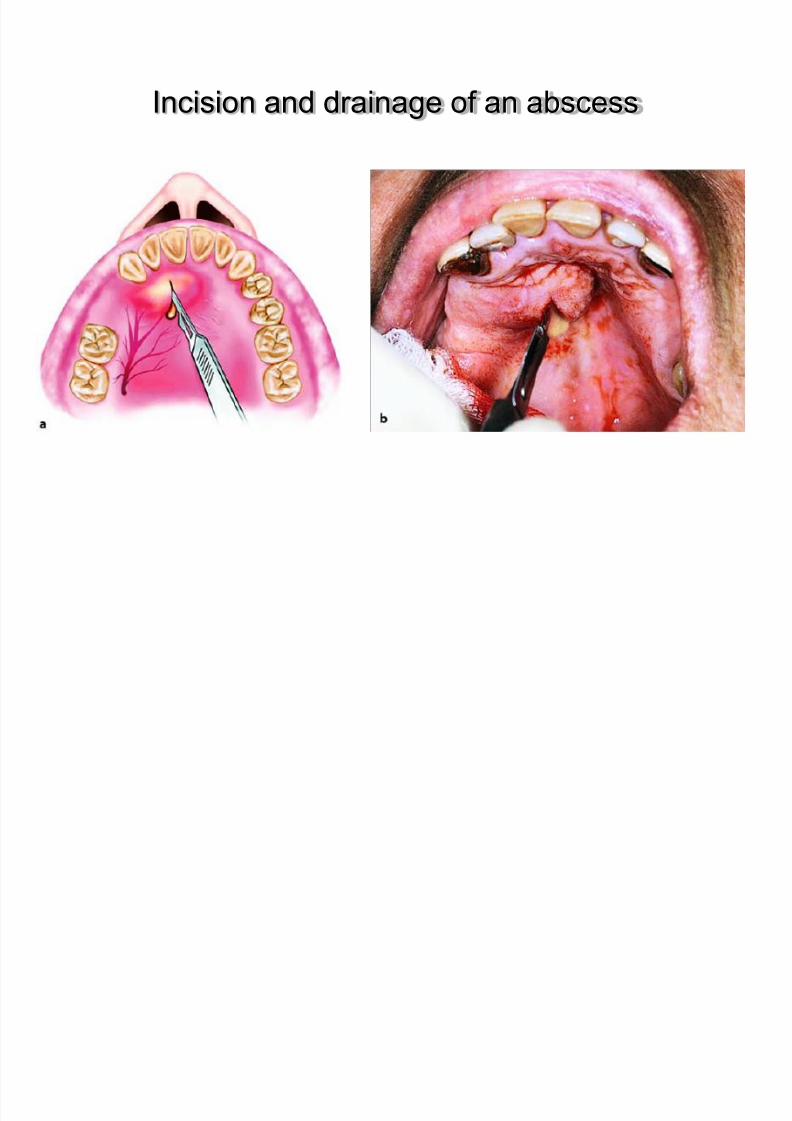
Incision and drainage of an abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 70/183
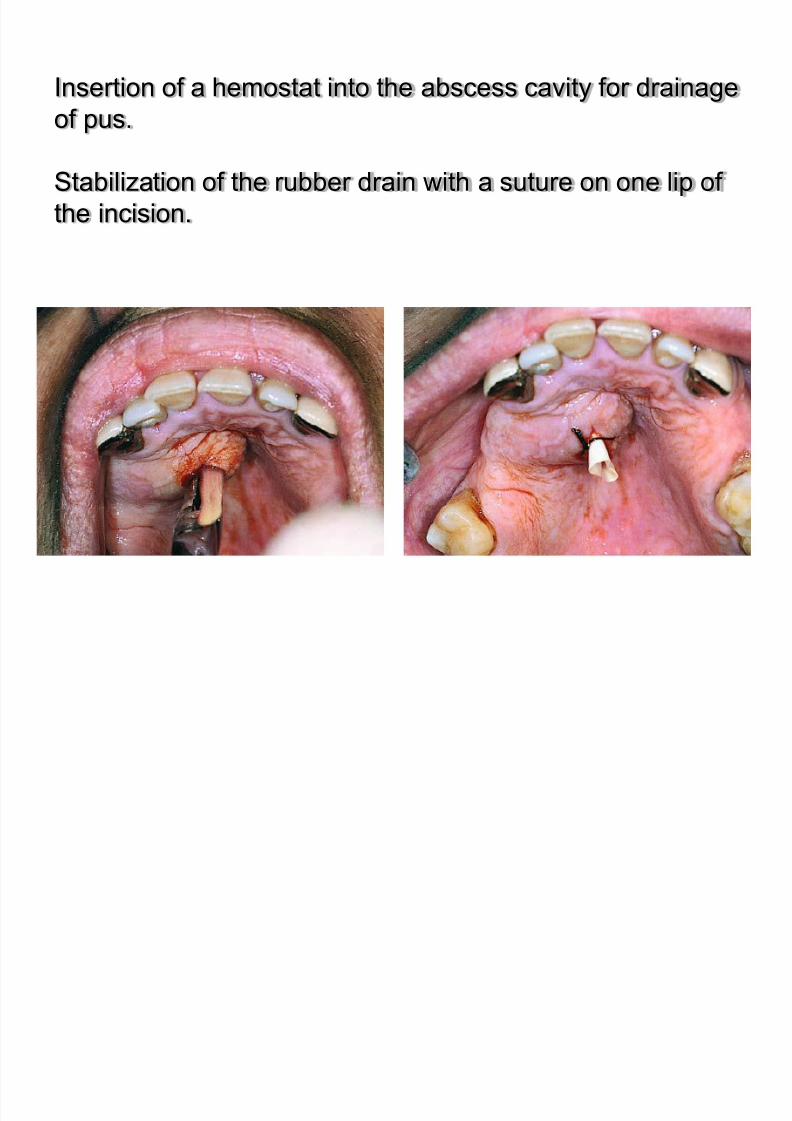
Insertion of a hemostat into the abscess cavity for drainage
of pus.
Stabilization of the rubber drain with a suture on one lip of
the incision.
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 71/183
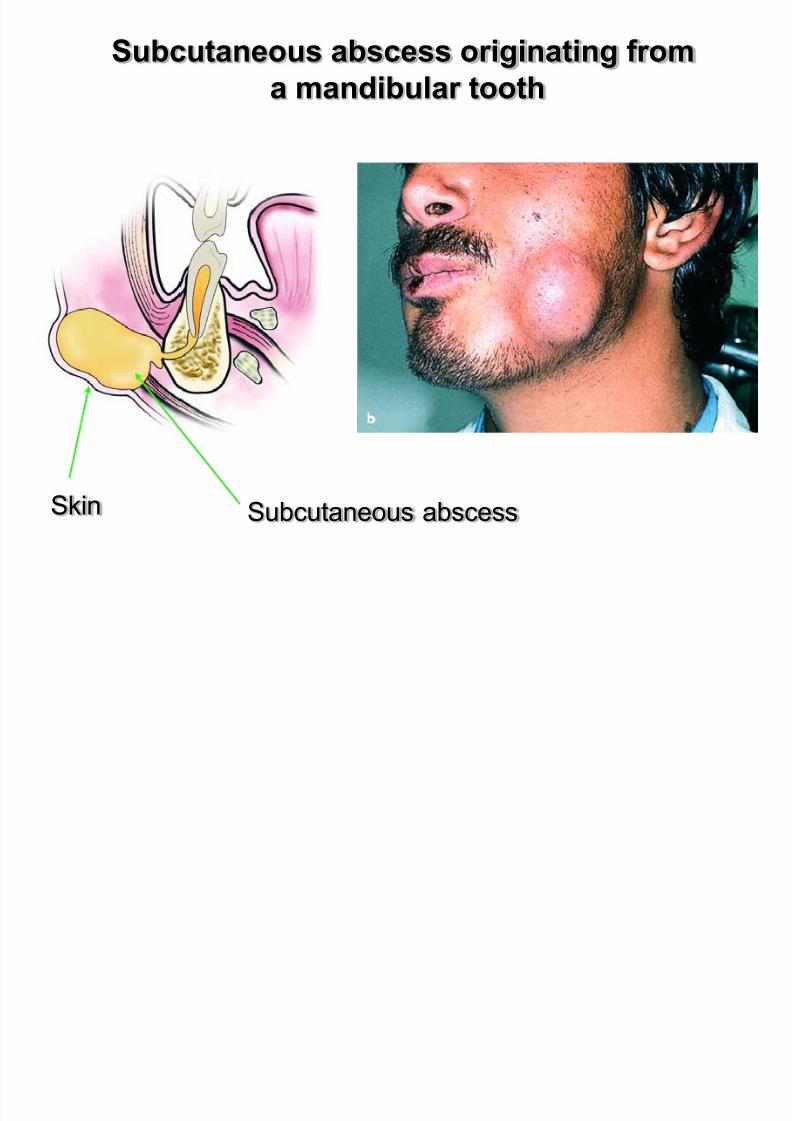
f- Subcutaneous abscess
This abscess is localized in various areas of the face
underneath the skin,with characteristic swelling that usually
fluctuates.
Clinical :
- edema
- the skin appears reddish
Subcutaneous abscess originating from
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 72/183
Subcutaneous abscess originating from
a mandibular tooth
Subcutaneous abscessSkin

8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 73/183
Subcutaneous abscess

8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 74/183
Peripheral infiltration anesthesia of healthy tissues
surrounding inflammation
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 75/183
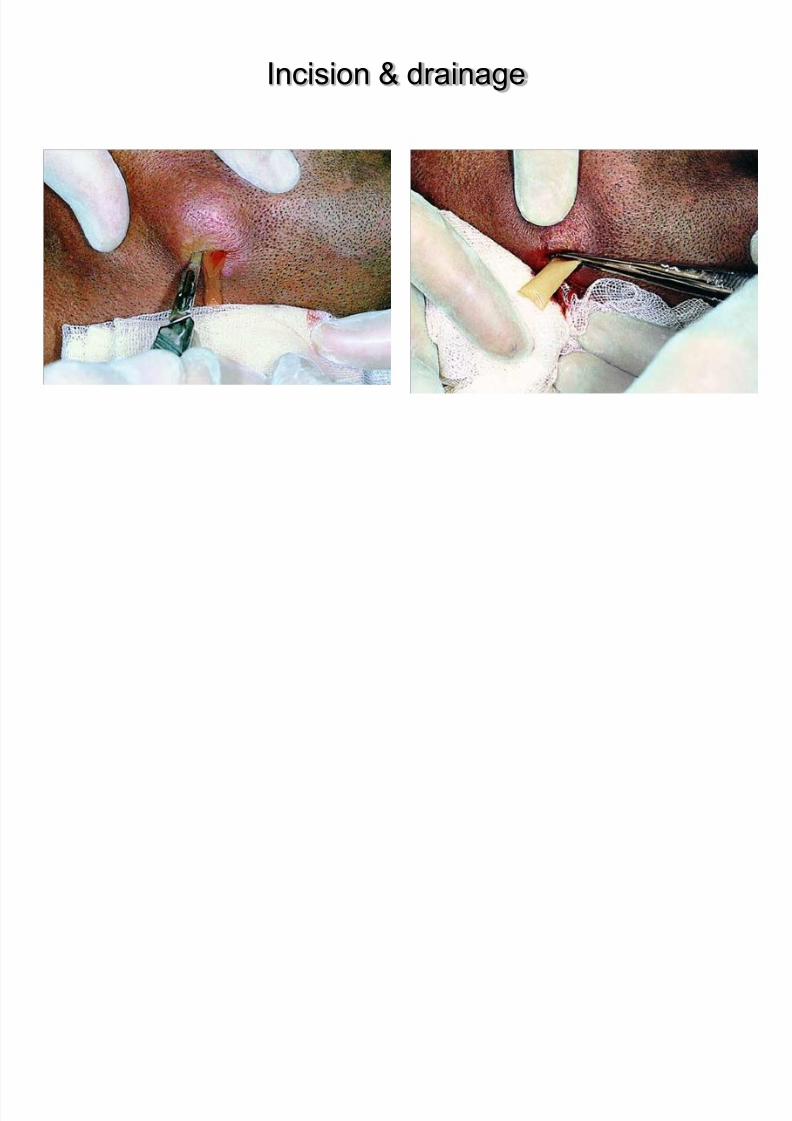
Incision & drainage
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 76/183
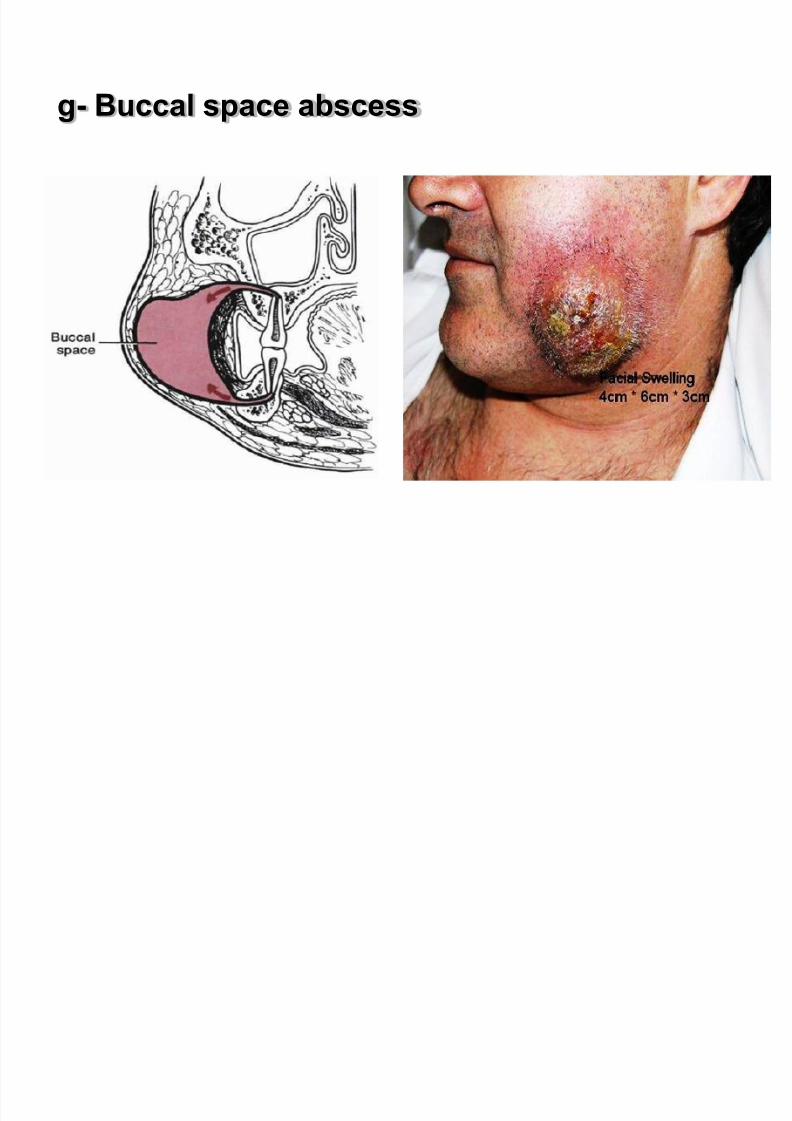
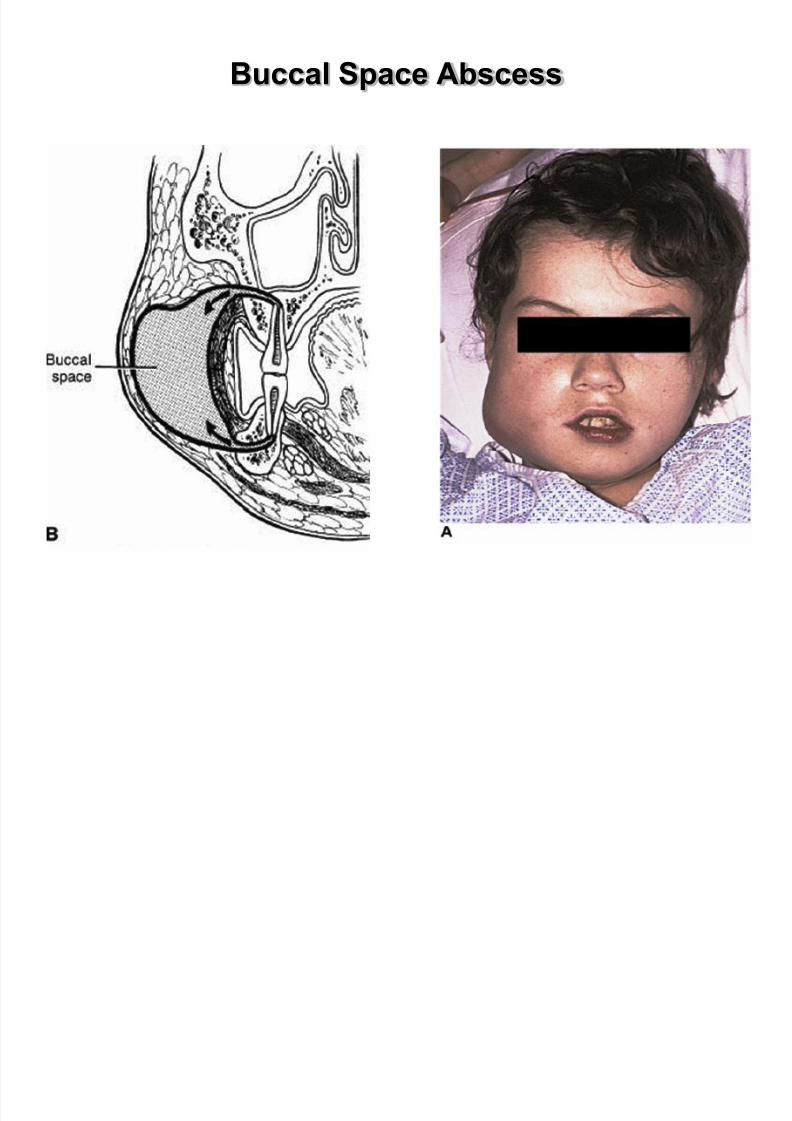
g- Buccal space abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 77/183
Buccal Space
1. Boundaries:
1. Lateral-Skin of the face
2. Medial-Buccinator muscle
2. Both a primary mandibular and maxillary space
3. Most infections caused by posterior maxillary teeth
Buccal Space Abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 78/183
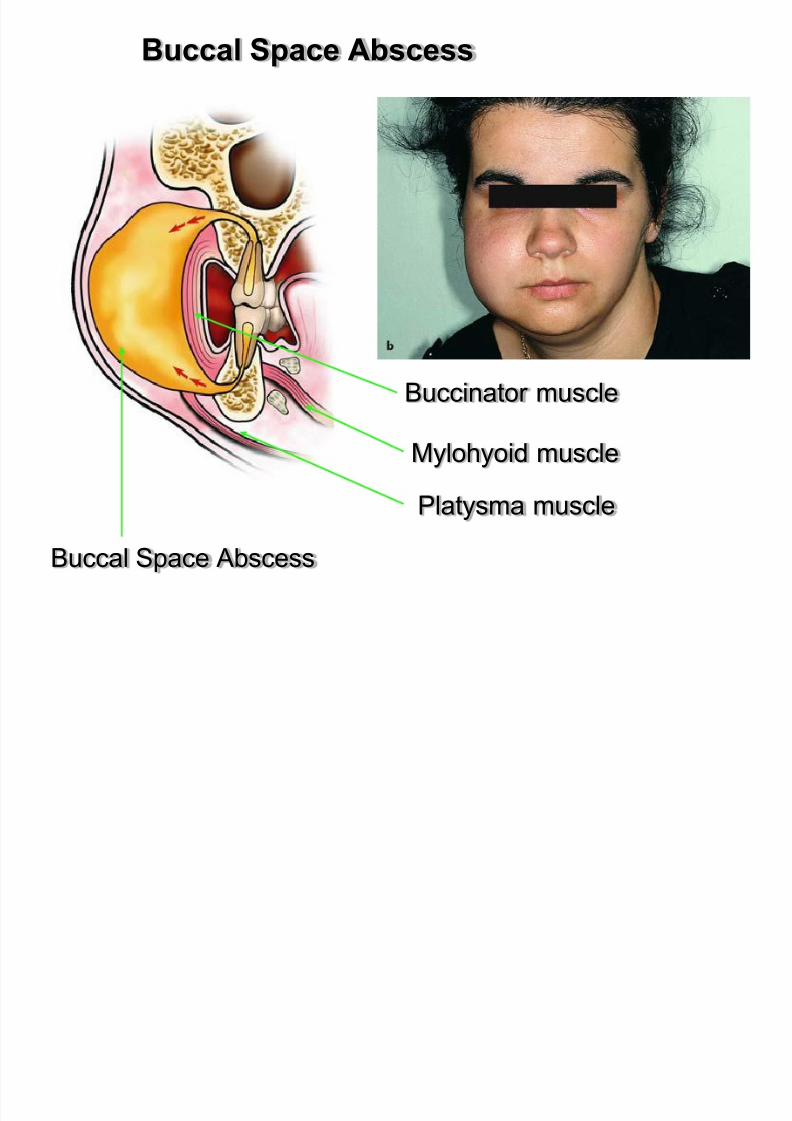
Buccal Space Abscess
Buccal Space Abscess
Buccinator muscle
Platysma muscle
Mylohyoid muscle
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 79/183
Buccal Space Abscess

8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 80/183
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 81/183
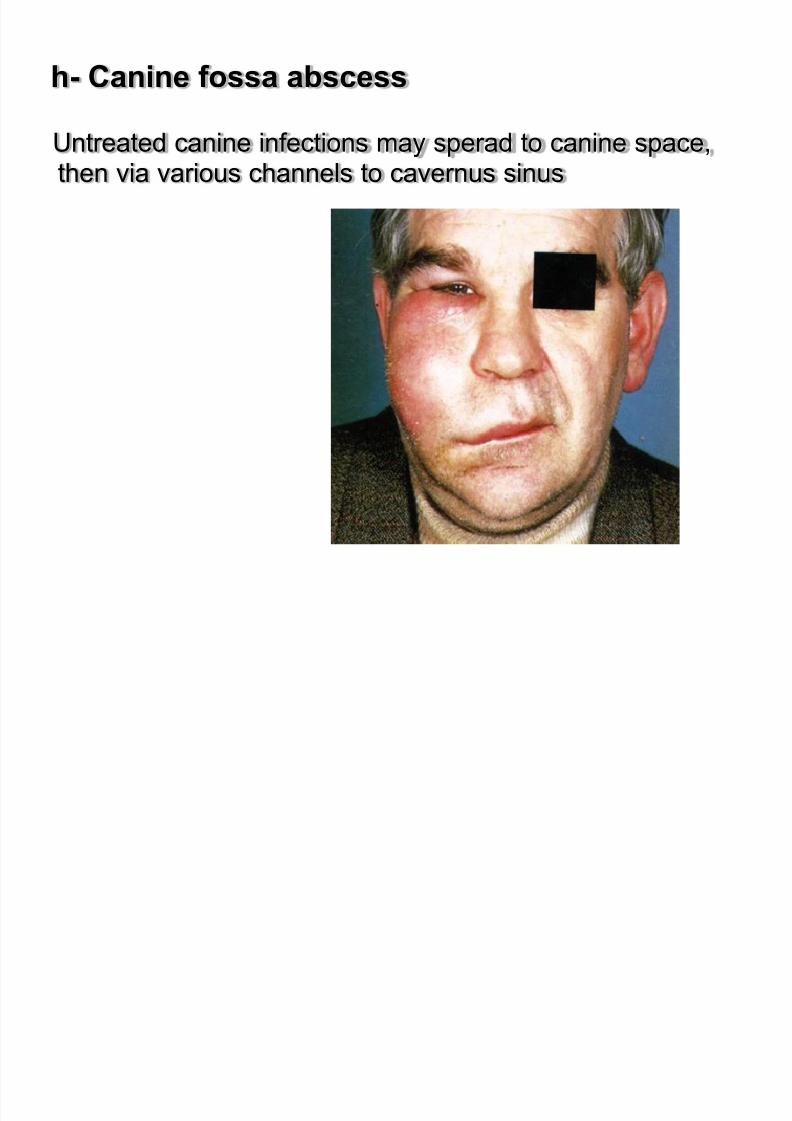
h- Canine fossa abscess
Untreated canine infections may sperad to canine space,then via various channels to cavernus sinus
Canine fossa abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 82/183
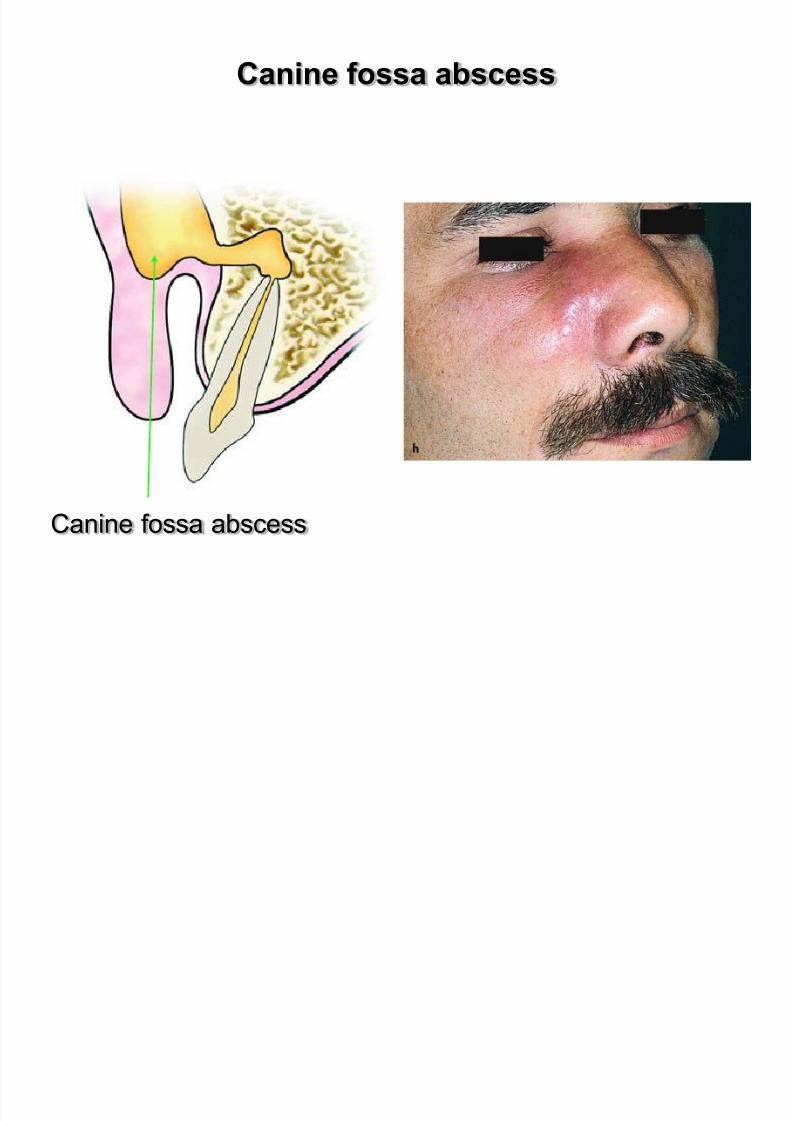
Canine fossa abscess
The canine fossa,which is where this type of abcess
develops, is a small space between the levator labiisuperioris and the levator anguli oris muscle.
Etiology : Infected root canals of premolars and canine of
the maxilla are considered to be responsible for thedevelopment of abscesses of the canina fossa.
Clinical :
- edema,localized in the infraorbital region,medial canthusof the eye,lower eyelid and nose.
- painful during palpation.
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 83/183
Canine fossa abscess
Canine fossa abscess

8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 84/183
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 85/183
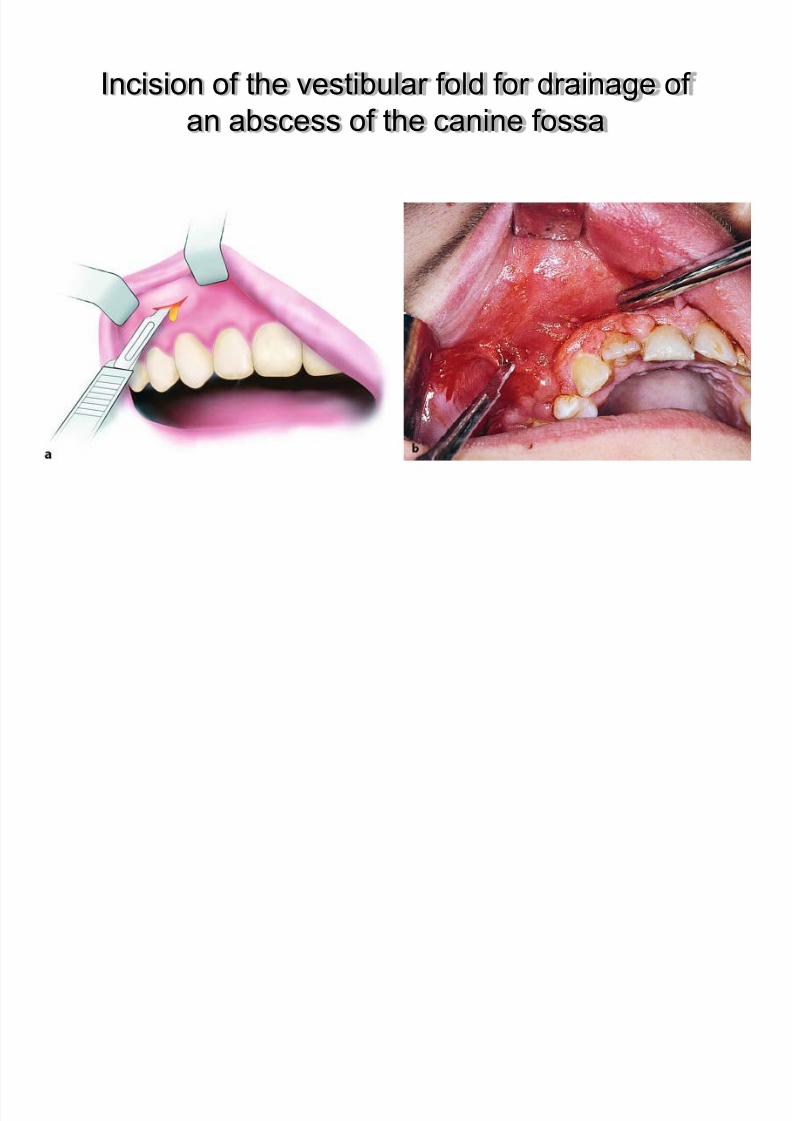
Incision of the vestibular fold for drainage of
an abscess of the canine fossa
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 86/183
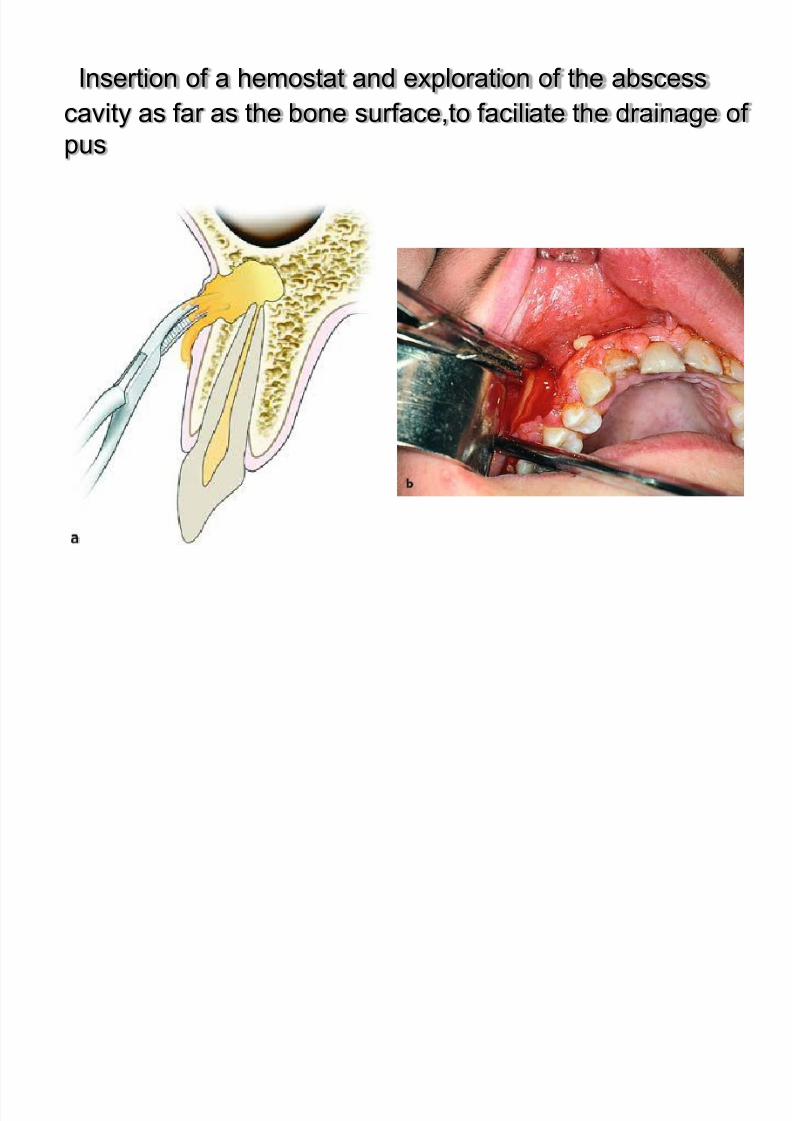
Insertion of a hemostat and exploration of the abscess
cavity as far as the bone surface,to faciliate the drainage of
pus
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 87/183
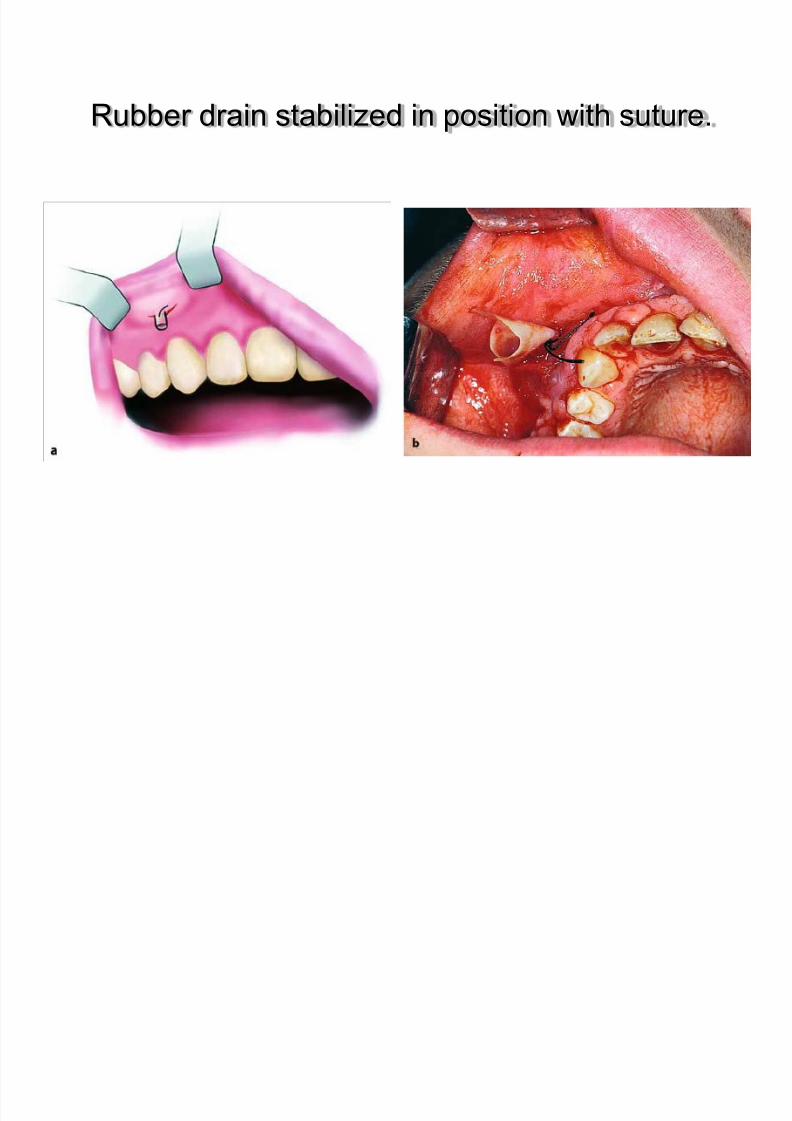
Rubber drain stabilized in position with suture.
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 88/183
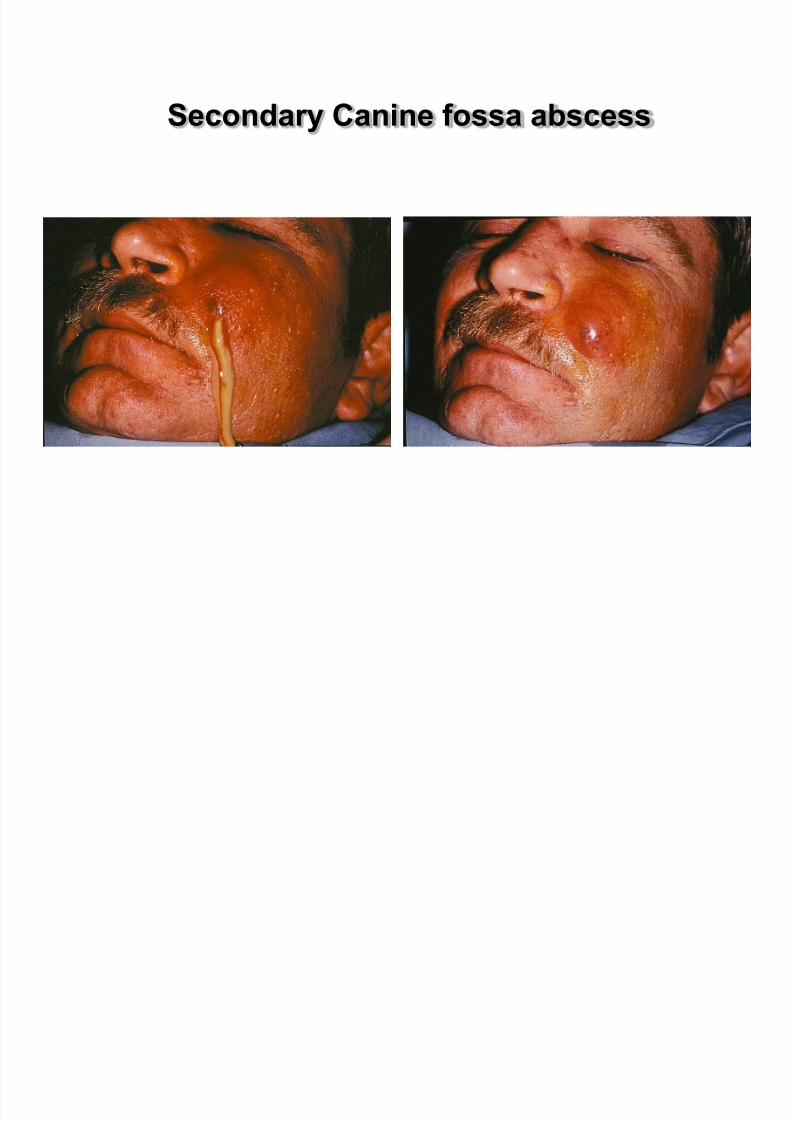
Secondary Canine fossa abscess
P i ill
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 89/183
Primary maxillary space
(canine, buccal, and infratemporal space) involvement can
ascend to cause orbital cellulitis (preseptal or postseptal)or cavernous sinus thrombosis
1. Ocular findings include erythema and swelling of theeyelids, and ophthalmoplegia
2. Cavernous sinus thrombosis1. Can result from hematogenous spread of
odontogenic infections
2. Bacterial routes of spread:1. Posterior: via pterygoid plexus or emissary veins
2. Anterior: via angular vein and inferior or superior ophthalmicveins to the cavernous sinus
3. Veins of the face and orbit valve less so retrograde flow canoccur
O bit l Ab

8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 90/183
Orbital Abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 91/183
II-Moderate Severity
Submental
Submandibular
Sublingual
Submasseteric space,Pterygomandibular
Superficial and deep temporal
spaces
Why are these moderate?
Because they can hinder
access to airway due to
trismus or swelling.
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 92/183
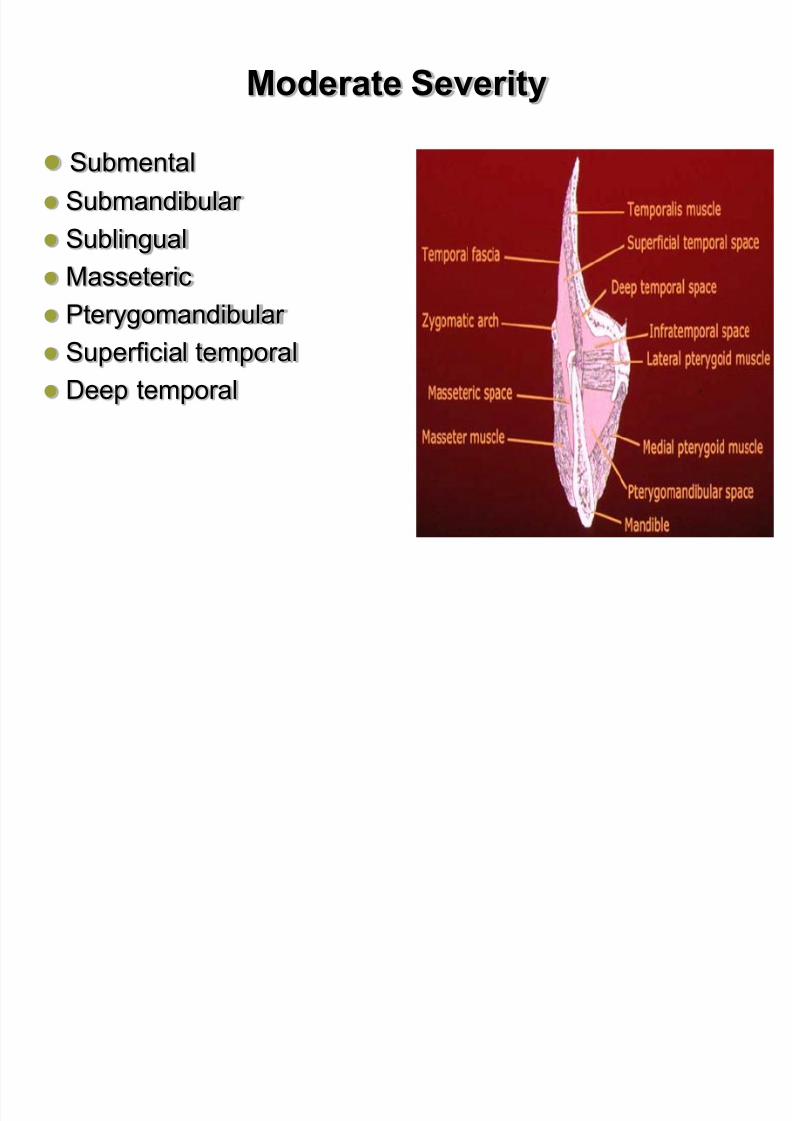
Moderate Severity
Submental
Submandibular
Sublingual
Masseteric
Pterygomandibular
Superficial temporal
Deep temporal
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 93/183
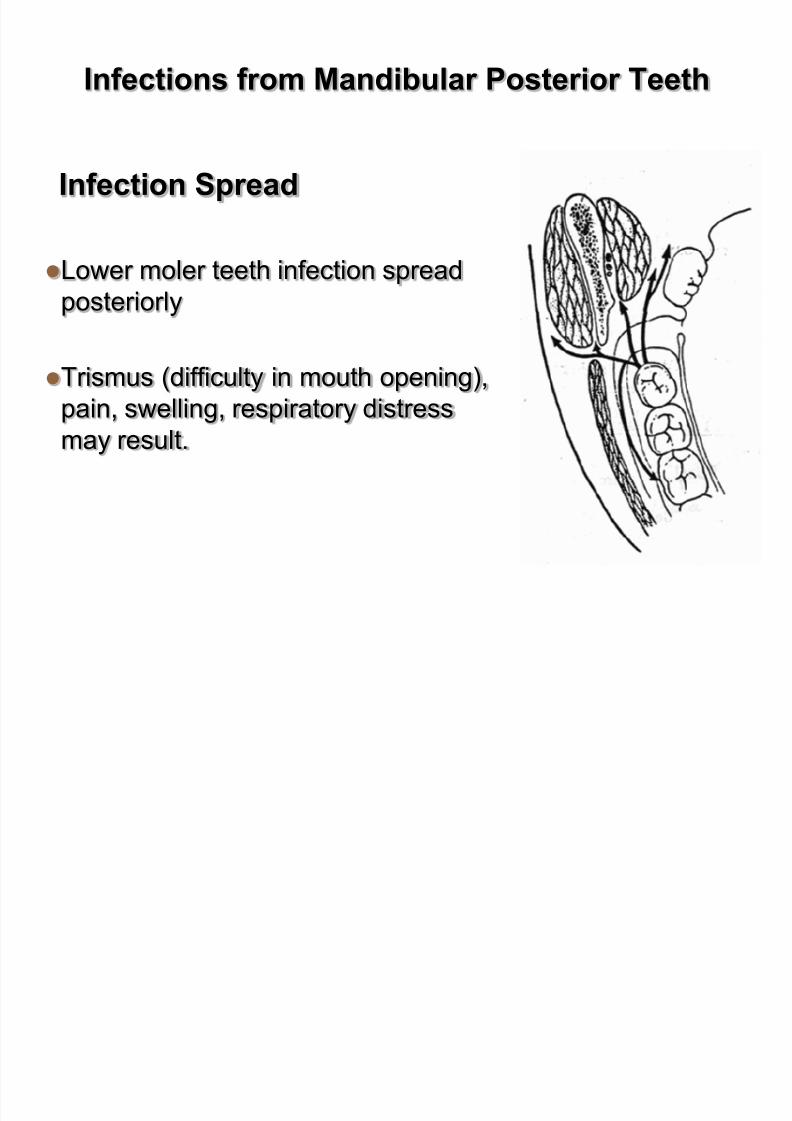
Infections from Mandibular Posterior Teeth
Infection Spread
Lower moler teeth infection spread
posteriorly
Trismus (difficulty in mouth opening),
pain, swelling, respiratory distress
may result.
Moderate Severity
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 94/183
Moderate Severity
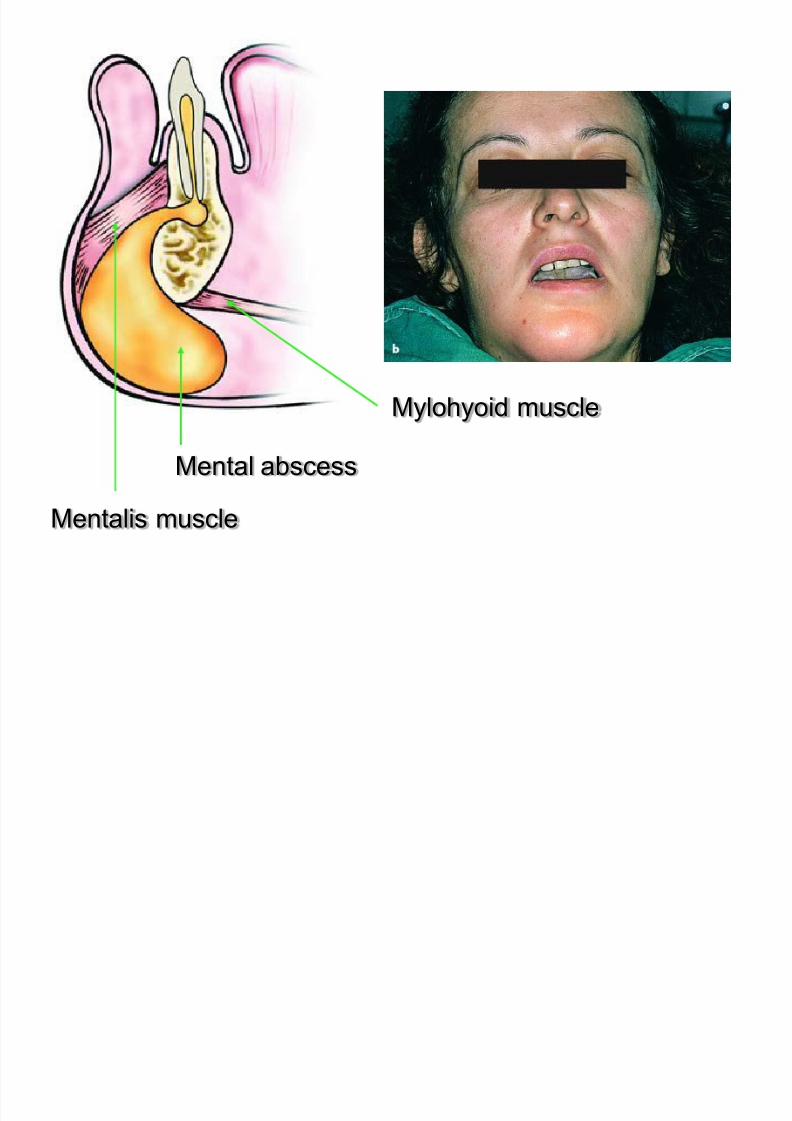
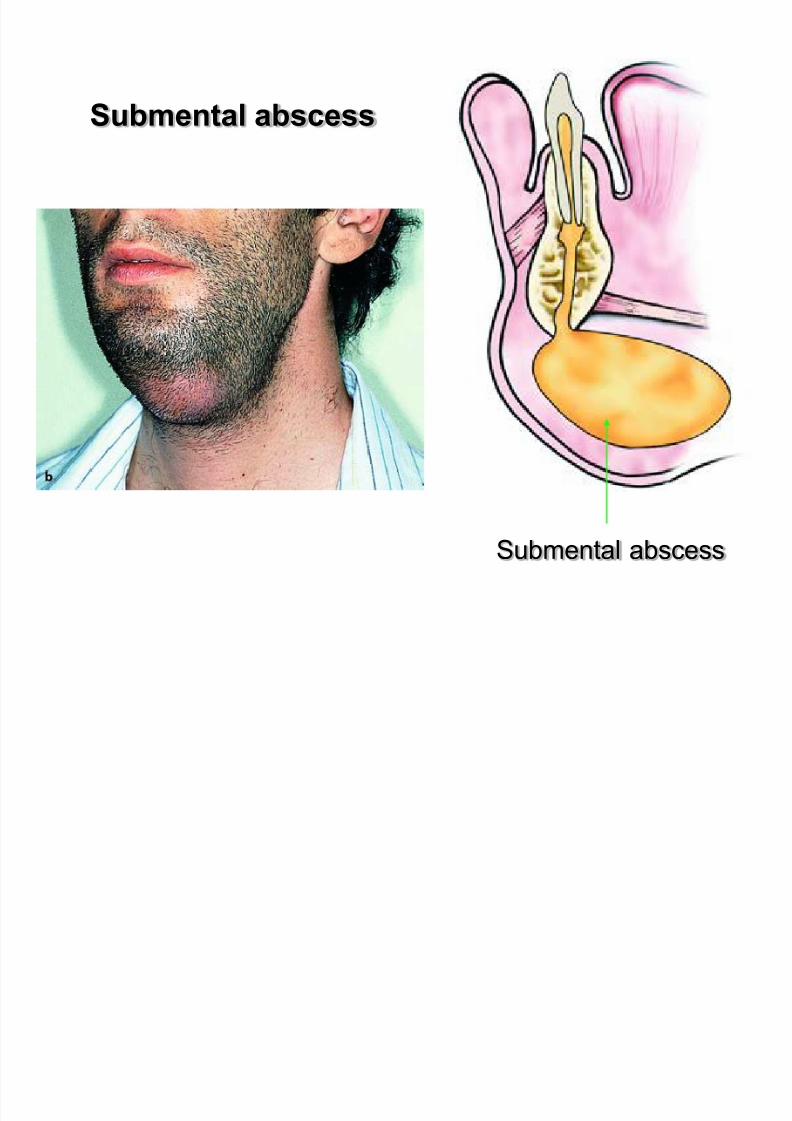
a-Mental abscessThe accumulation of pus in this space is located at the
anterior region of the mandible,near the bone,and,more
specifically,underneath the mentalis muscle,with spreat
of the infection towards the symphysis menti.
Clinical :
- firm and painful swelling in the area of the chin
- the skin becomes shiny and red
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 95/183
Mylohyoid muscle
Mental abscess
Mentalis muscle
b- Submental space
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 96/183
b Submental space
1- Infection can result directly due to infected mandibular
incisor or indirectly from the submandibular space
2- Space located between the anterior bellies of the
digastric muscle laterally, deeply by the mylohyoid muscle,
and superiorly by the deep cervical fascia, the platysmamuscle, the superficial cervical fascia, and the skin.
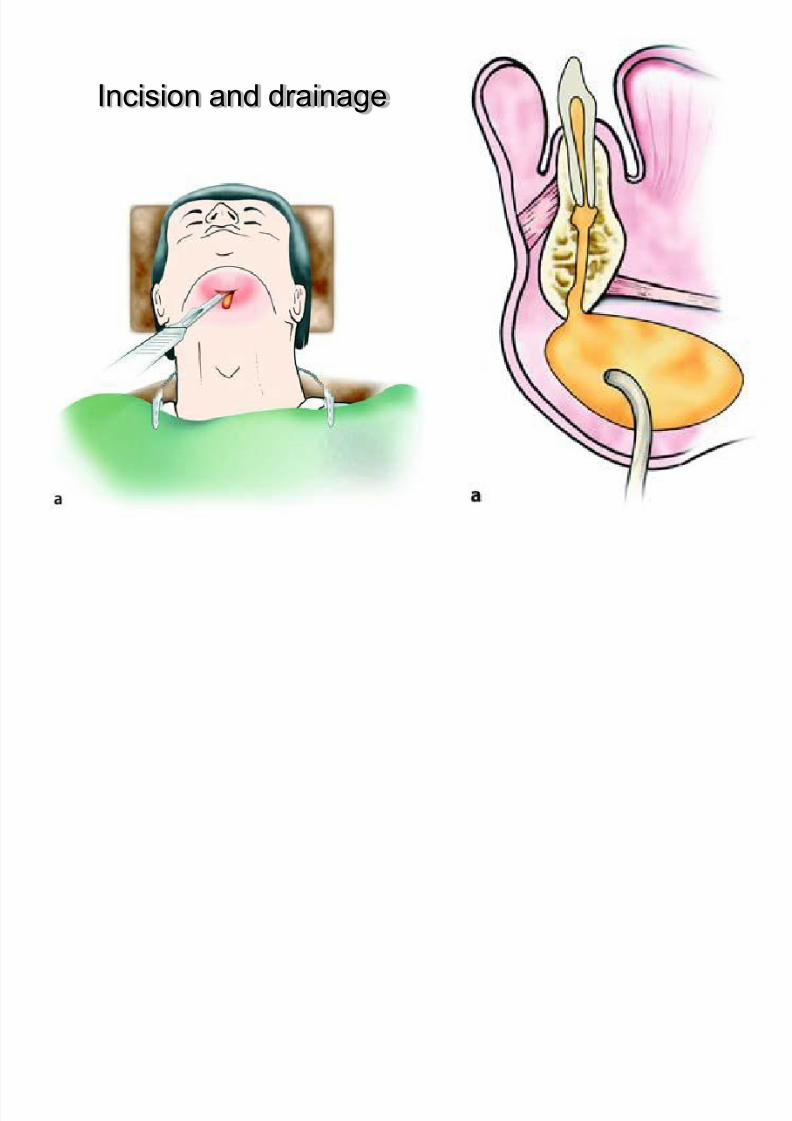
3- Dependent drainage of this space is performed by
placing a horizontal incision in the most dependent area
of the swelling extraorally with a cosmetic scar being the
result
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 97/183
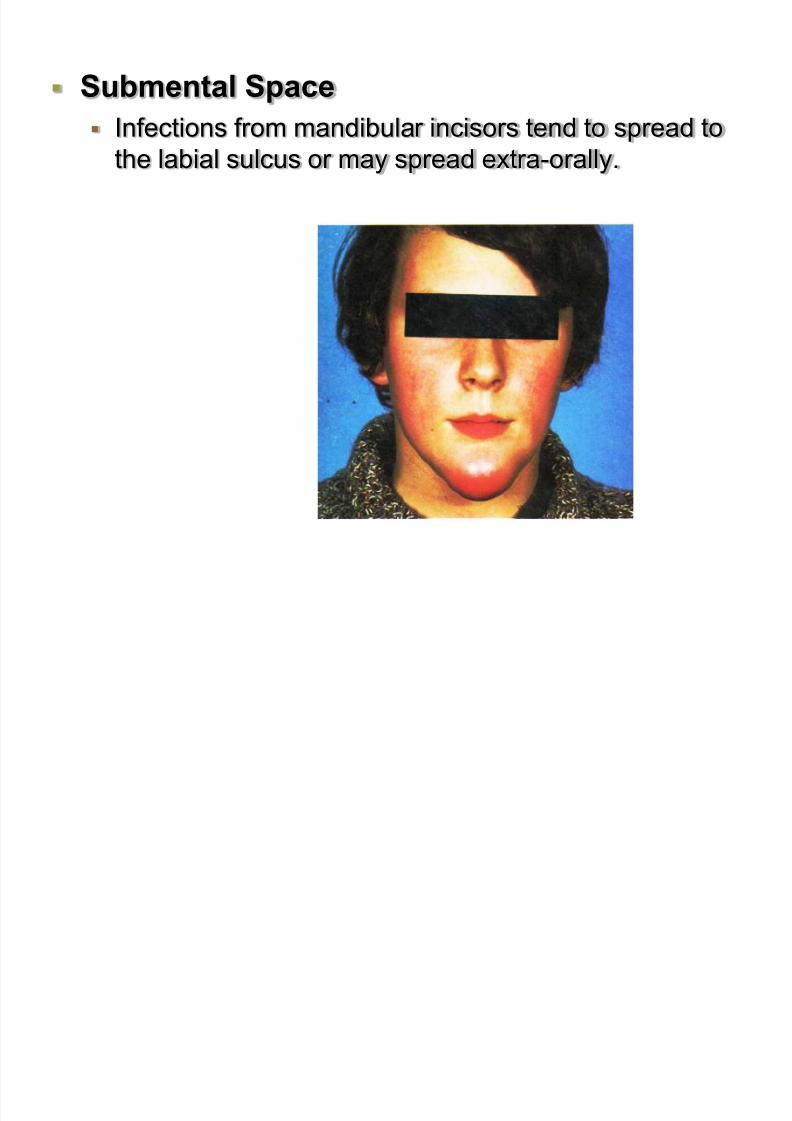
Submental Space Infections from mandibular incisors tend to spread to
the labial sulcus or may spread extra-orally.
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 98/183
Submental abscess
Submental abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 99/183
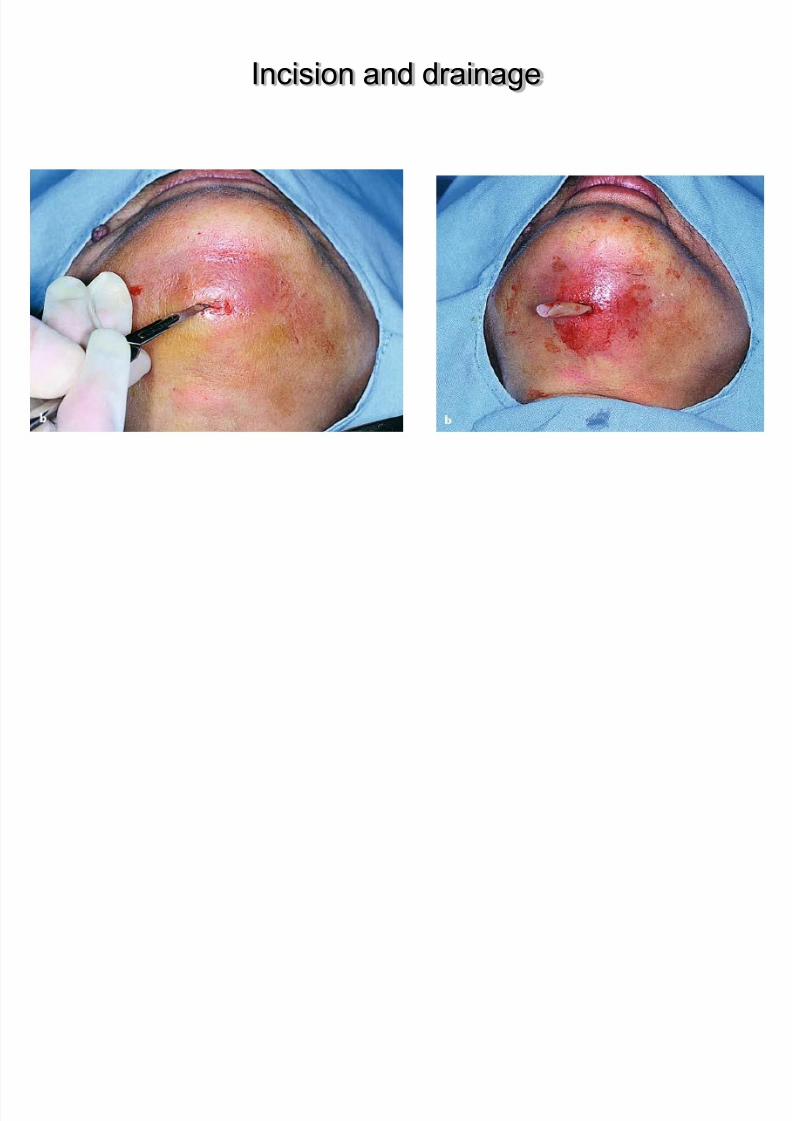
Incision and drainage
Incision and drainage
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 100/183
Incision and drainage
d Submandibular abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 101/183
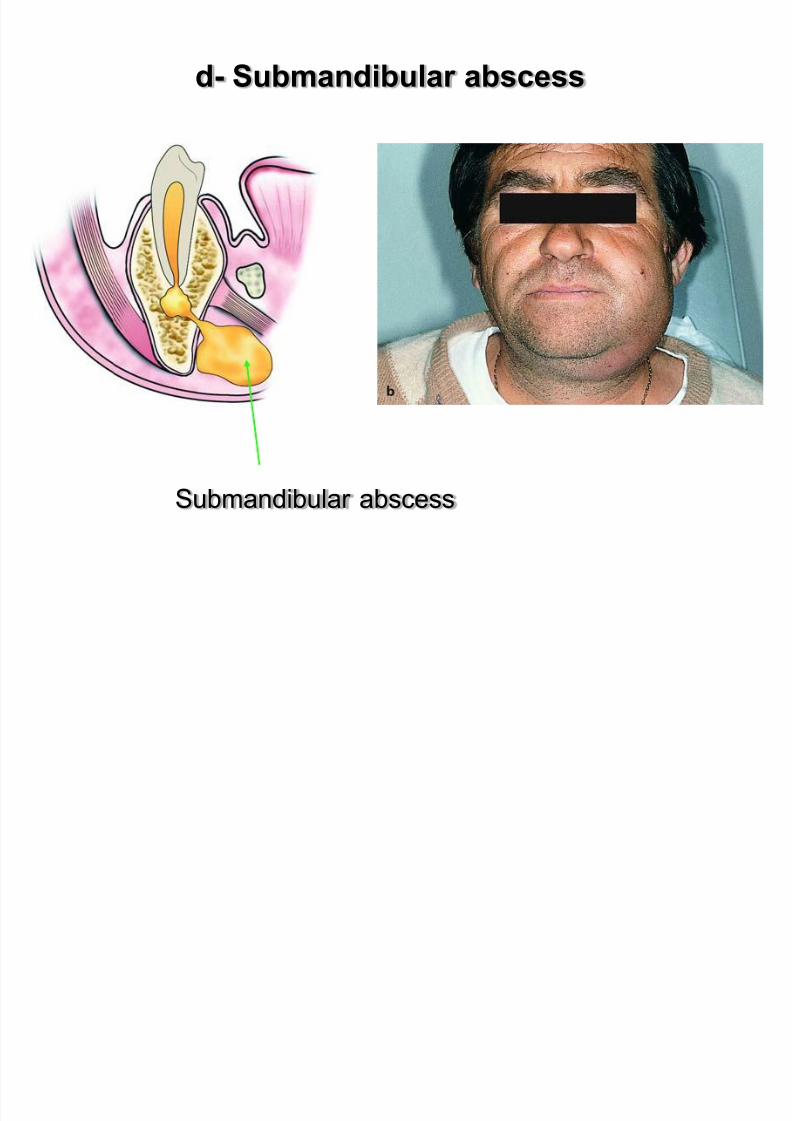
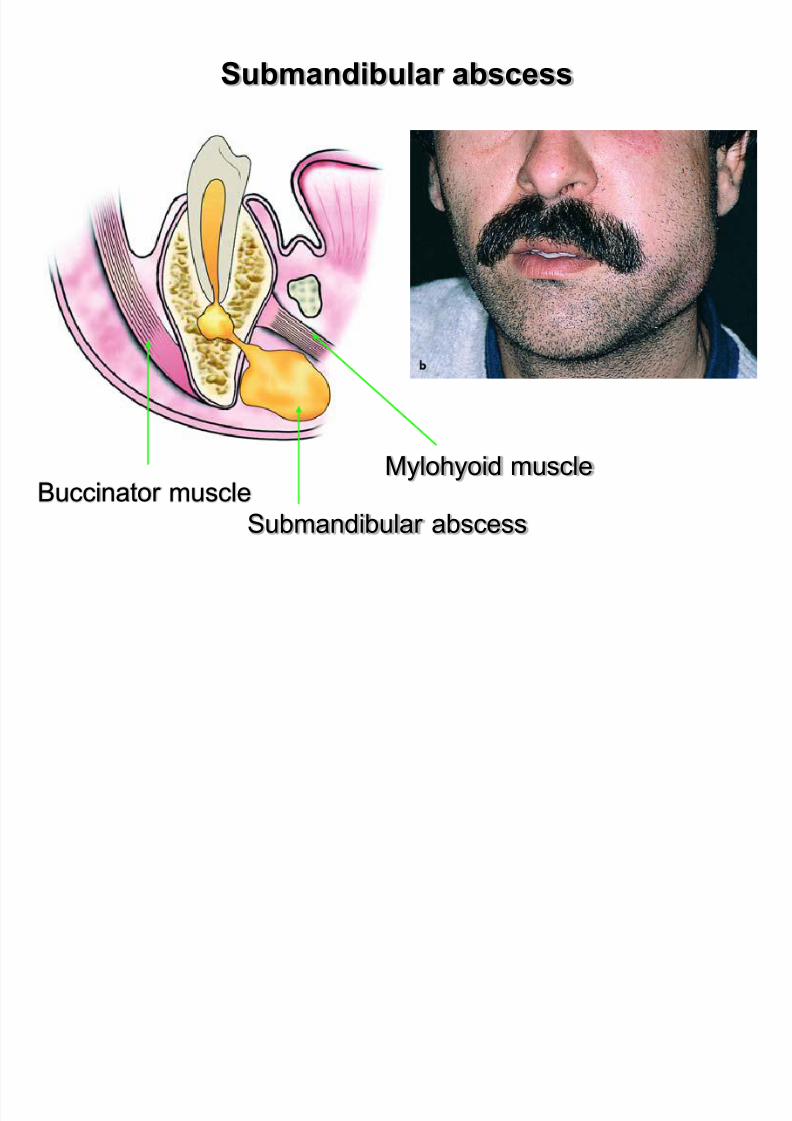
d- Submandibular abscess
Submandibular abscess
Submandibular abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 102/183
Submandibular abscess
Submandibular abscess
Mylohyoid muscleBuccinator muscle
Submandibular space
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 103/183
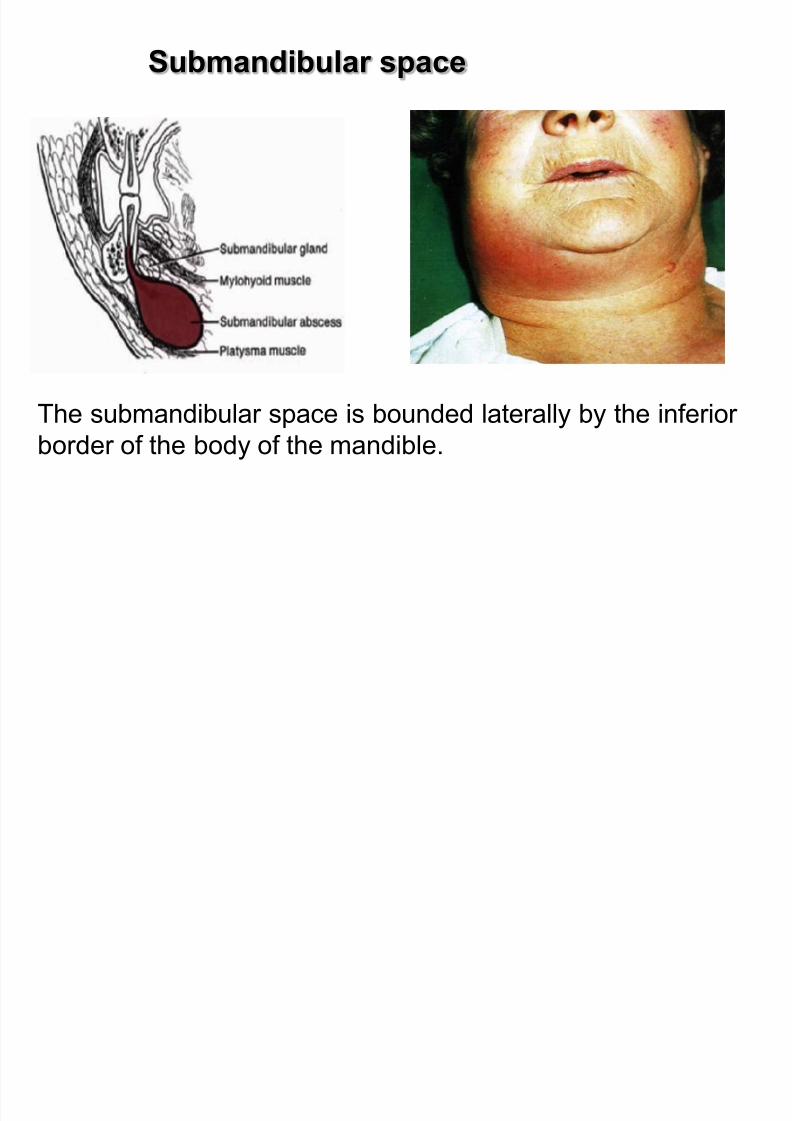
p
The submandibular space is bounded laterally by the inferior
border of the body of the mandible.
Boundaries:
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 104/183
Boundaries:
medially by the anterior belly of the digastric muscle
posteriorly by the stylohyoid ligament and the posterior
belly of the digastric muscle
superiorly by the mylohyoid and hyoglossus muscles
inferiorly by the superficial layer of the deep cervical fascia
Submandibular Space Abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 105/183
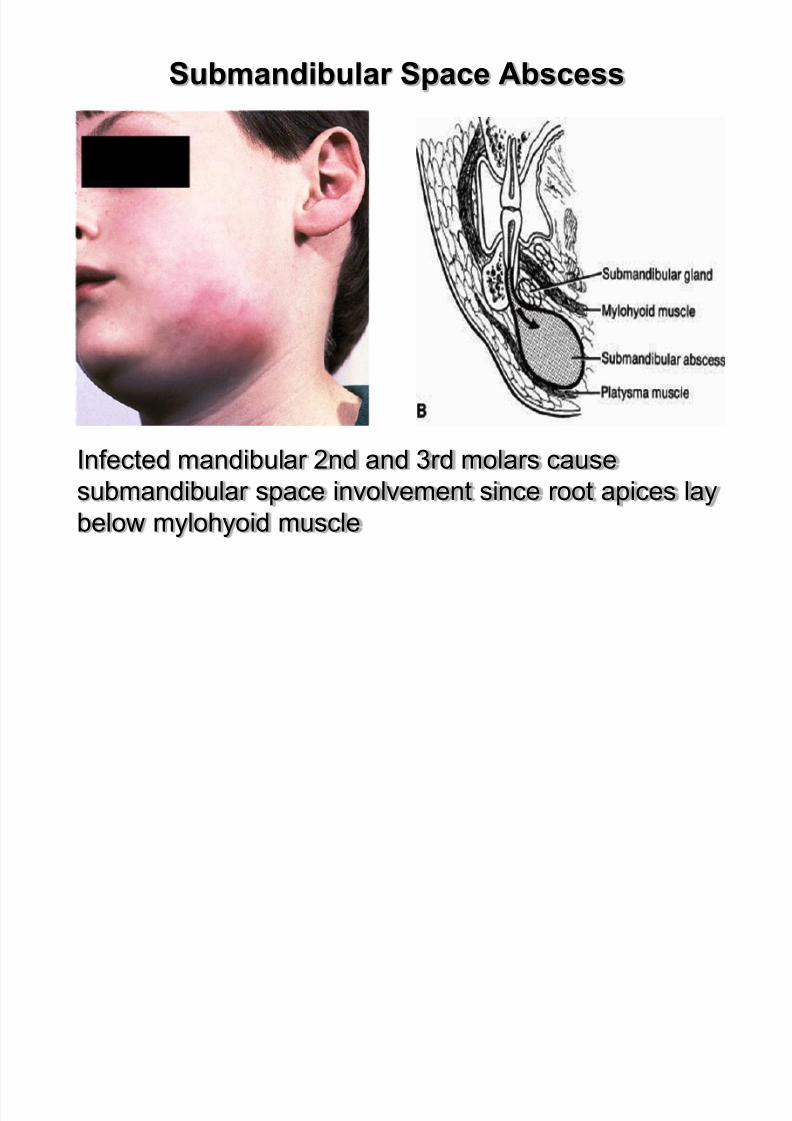
Submandibular Space Abscess
Infected mandibular 2nd and 3rd molars cause
submandibular space involvement since root apices lay
below mylohyoid muscle
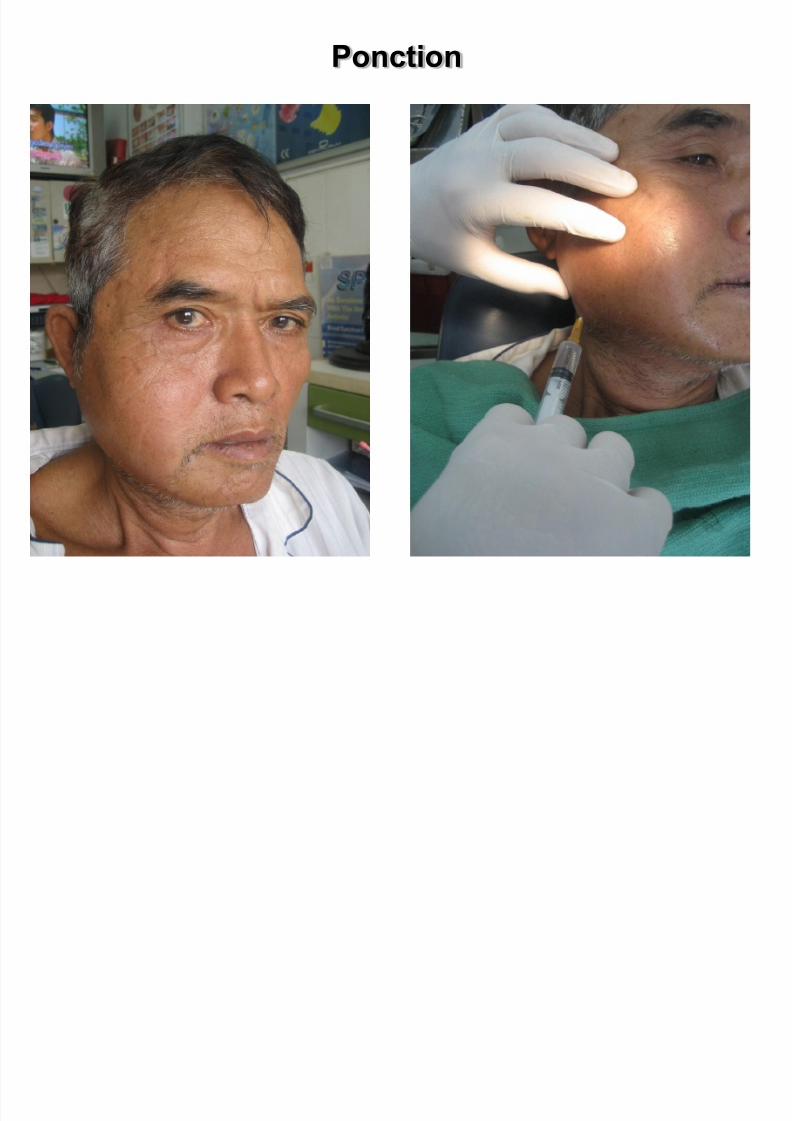
Ponction
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 106/183

8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 107/183
Clinical :
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 108/183
- moderate swelling at the submandibular area
- edema that is indurated
- redness of the overlying skin
- pain during palpation
- moderate trismus due to involvement of the medial
pterygoid muscle.
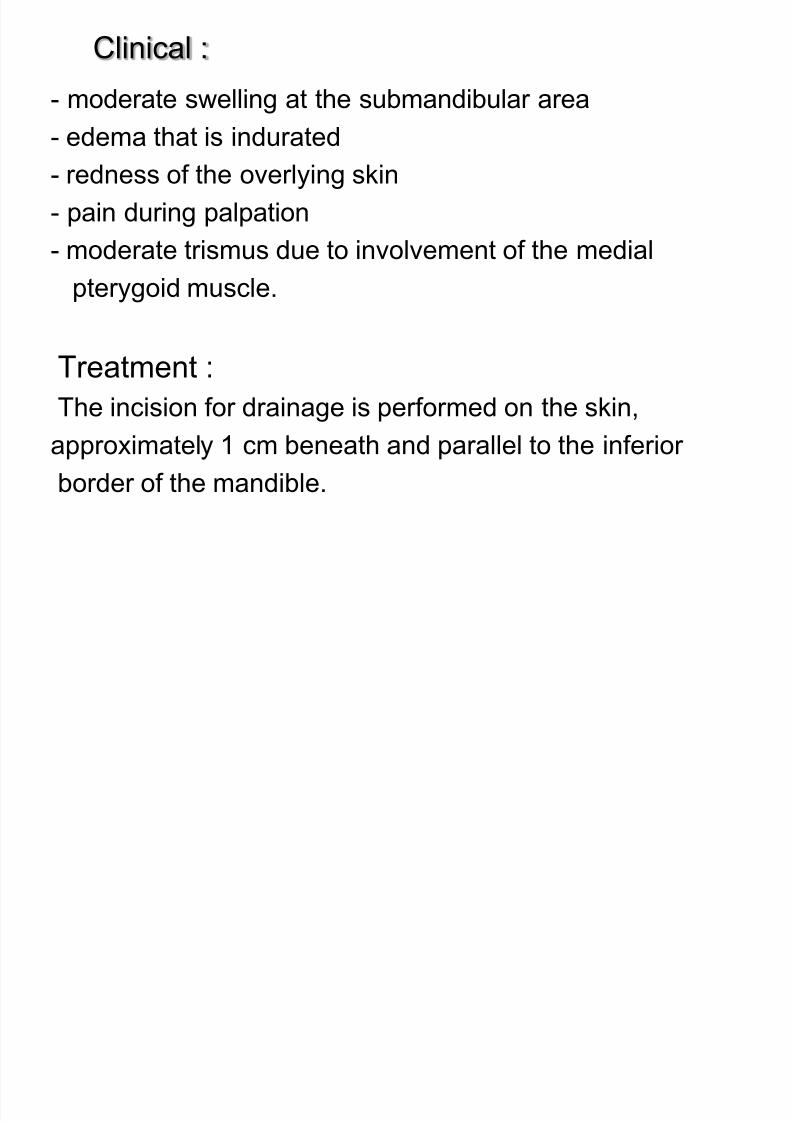
Treatment :
The incision for drainage is performed on the skin,
approximately 1 cm beneath and parallel to the inferior
border of the mandible.
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 109/183
Incision & drainage
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 110/183
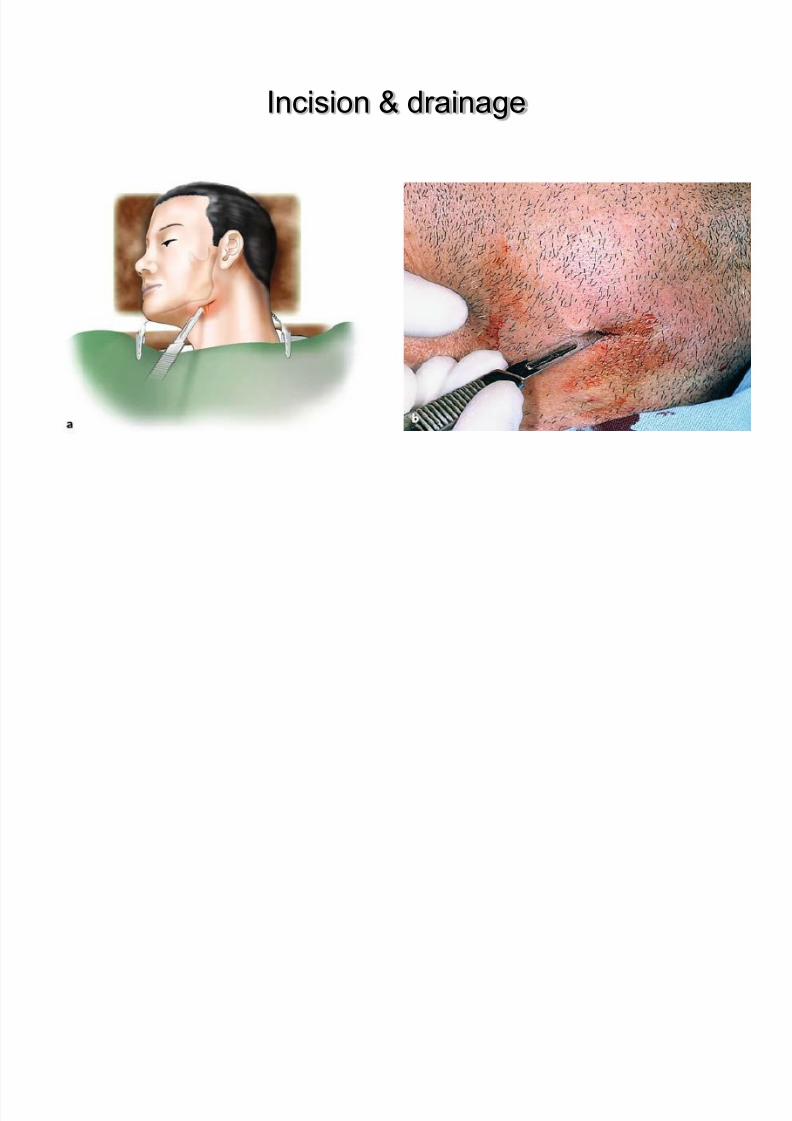
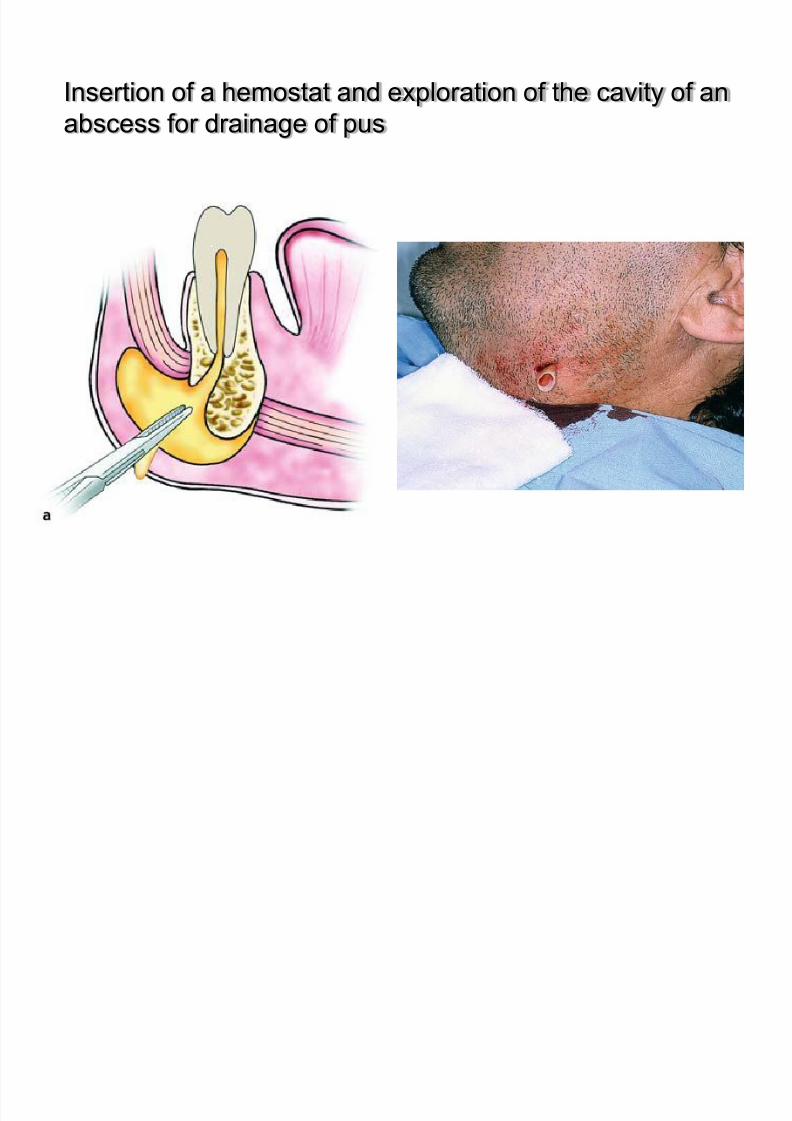
Insertion of a hemostat and exploration of the cavity of an
abscess for drainage of pus

8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 111/183
TECHNIQUE OF INCISION

8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 112/183
Secondary Mandibular Spaces
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 113/183
Secondary Mandibular Spaces
Referred to as secondary spaces since they are infected after involvement of primary mandibular spaces
Failure to treat a primary space infection or a compromisedhost results in secondary space involvement
Connective tissue fascia has poor blood supply hencetreatment usually surgical to drain purulent exudates
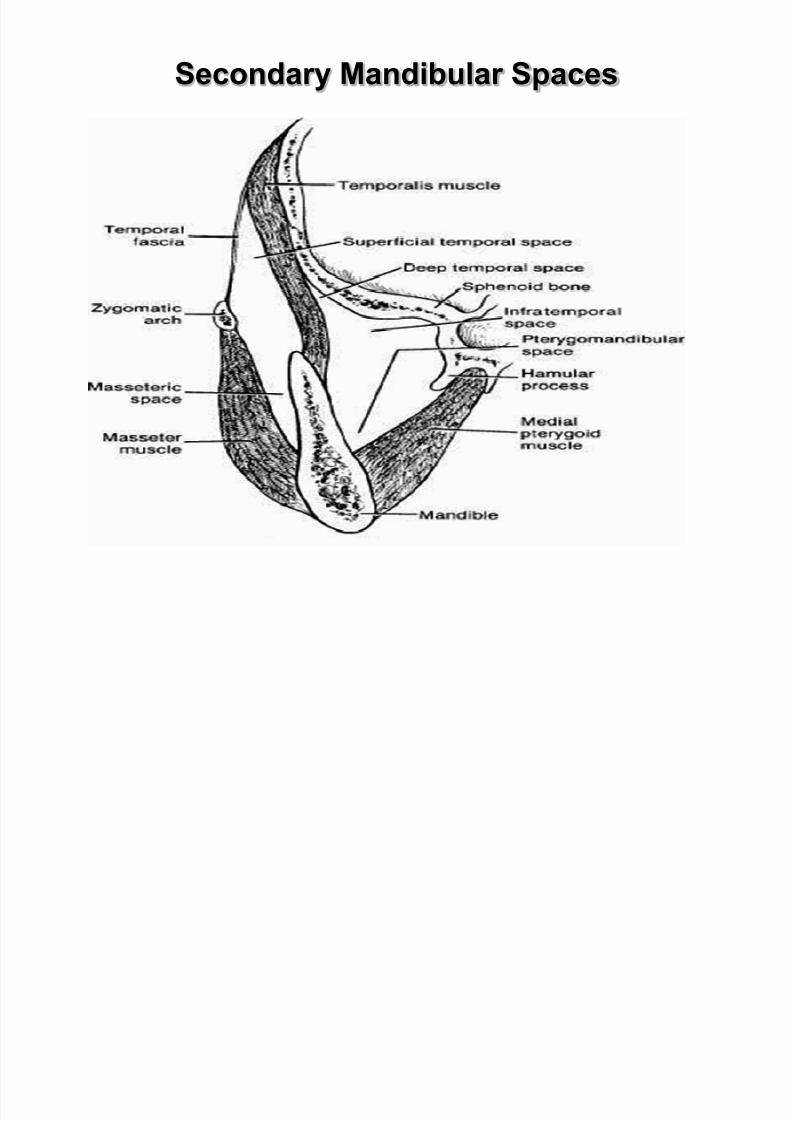
The secondary mandibular spaces include the masseteric,pterygomandibular, and temporal spaces
Secondary Mandibular Spaces
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 114/183
Secondary Mandibular Spaces
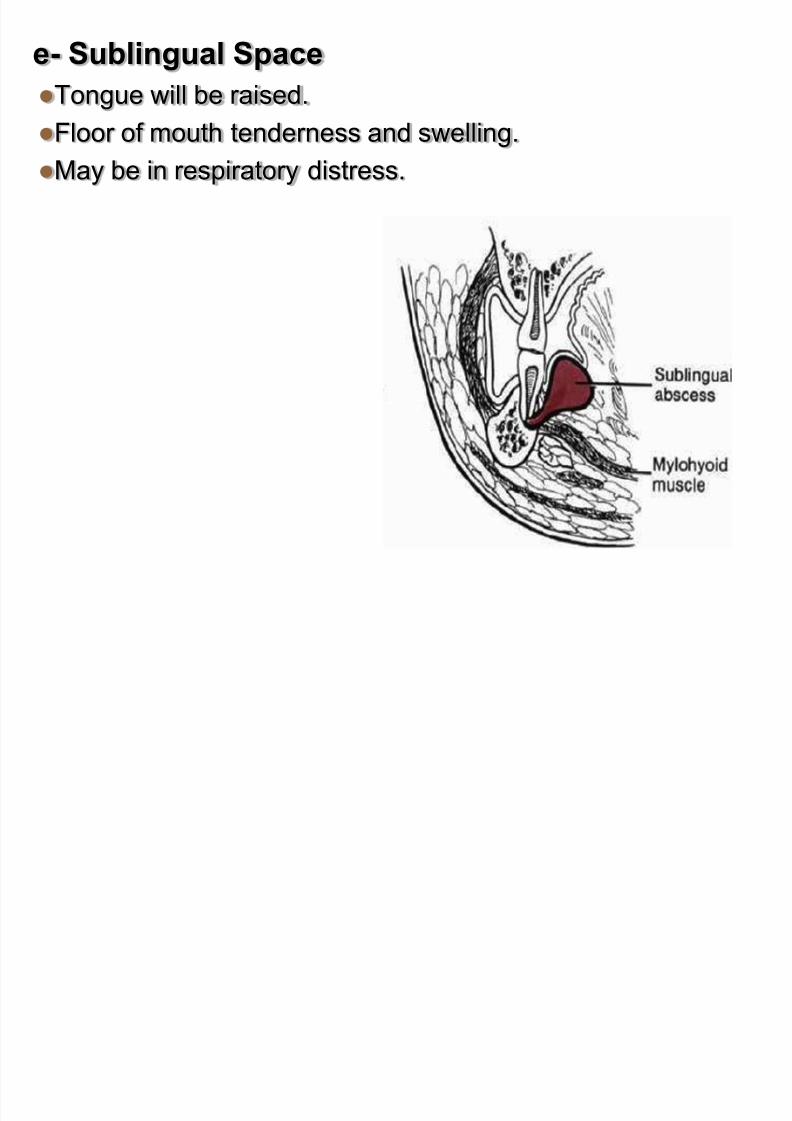
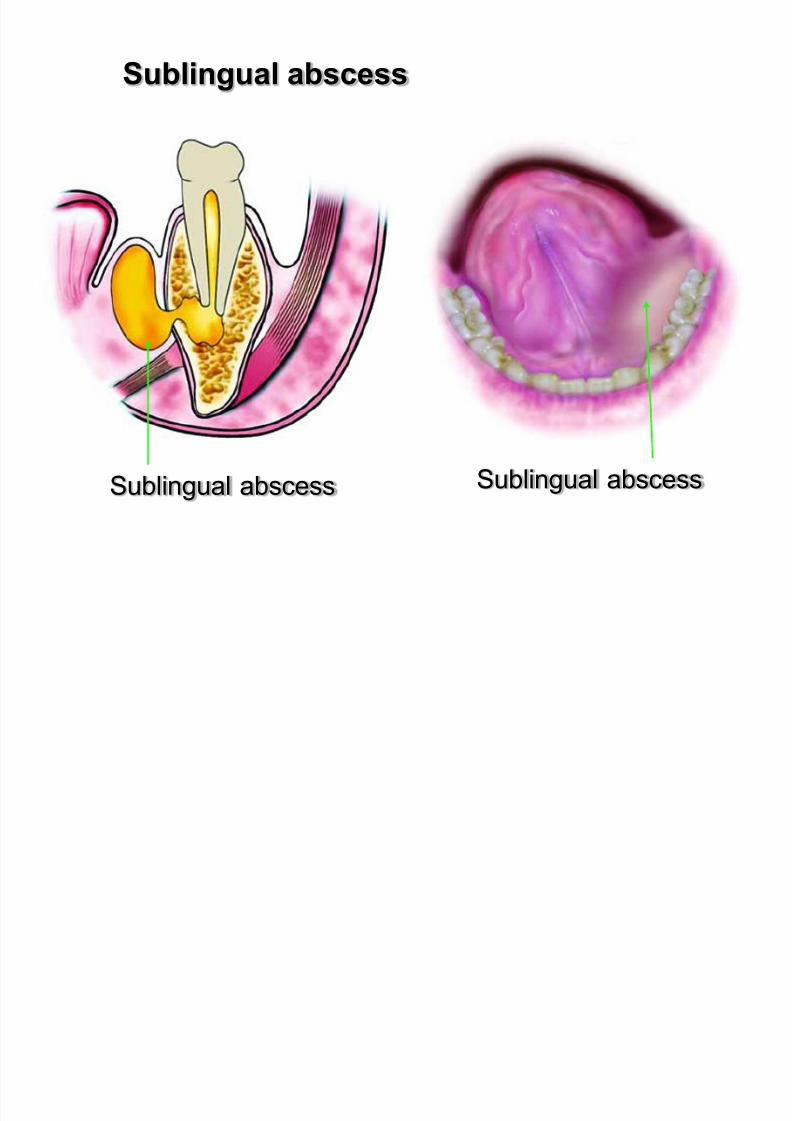
e- Sublingual Space
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 115/183
Tongue will be raised.
Floor of mouth tenderness and swelling.
May be in respiratory distress.
Sublingual Space
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 116/183
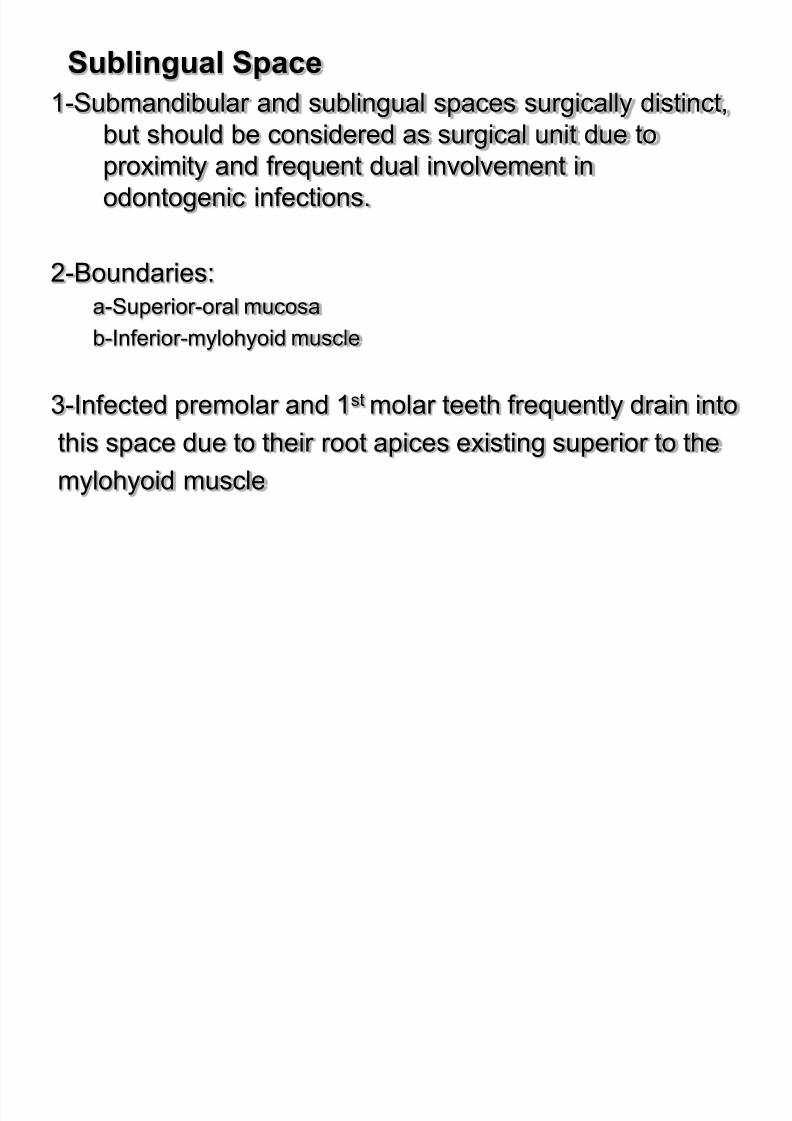
1-Submandibular and sublingual spaces surgically distinct,
but should be considered as surgical unit due to
proximity and frequent dual involvement inodontogenic infections.
2-Boundaries:
a-Superior-oral mucosa
b-Inferior-mylohyoid muscle
3-Infected premolar and 1st molar teeth frequently drain into
this space due to their root apices existing superior to the
mylohyoid muscle
Sublingual abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 117/183
g
Sublingual abscessSublingual abscess
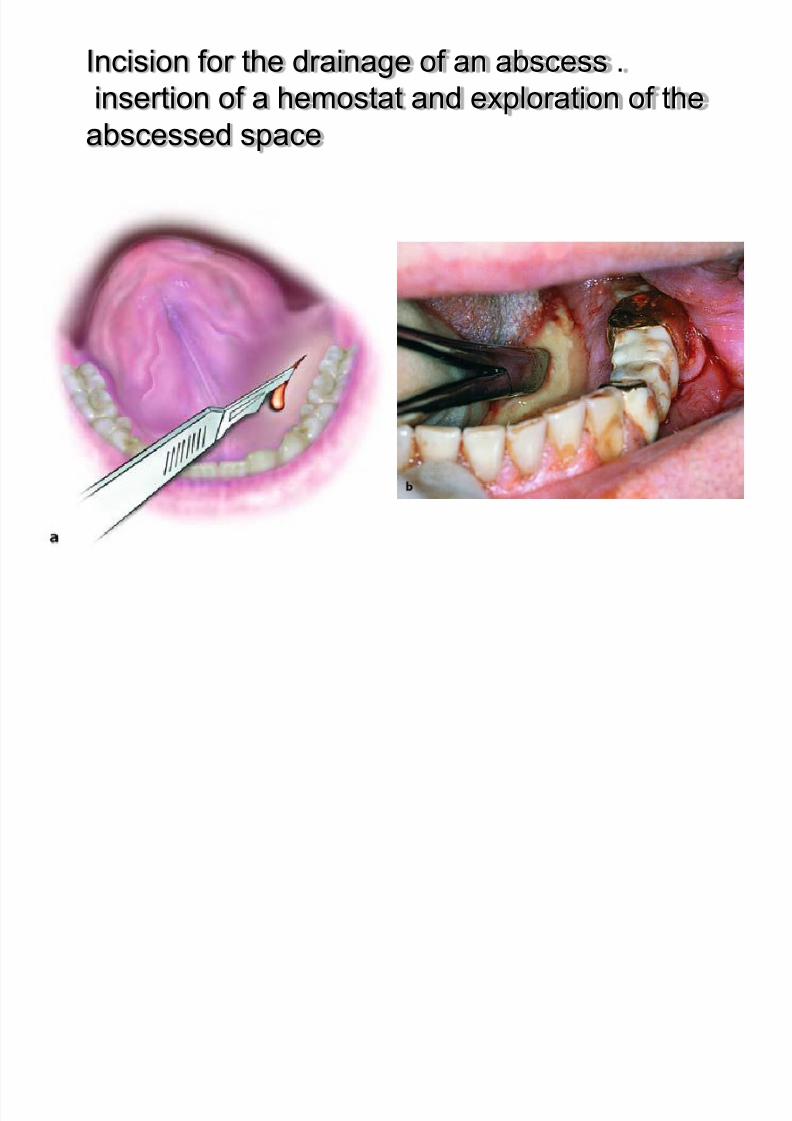
Incision for the drainage of an abscess .
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 118/183
insertion of a hemostat and exploration of the
abscessed space
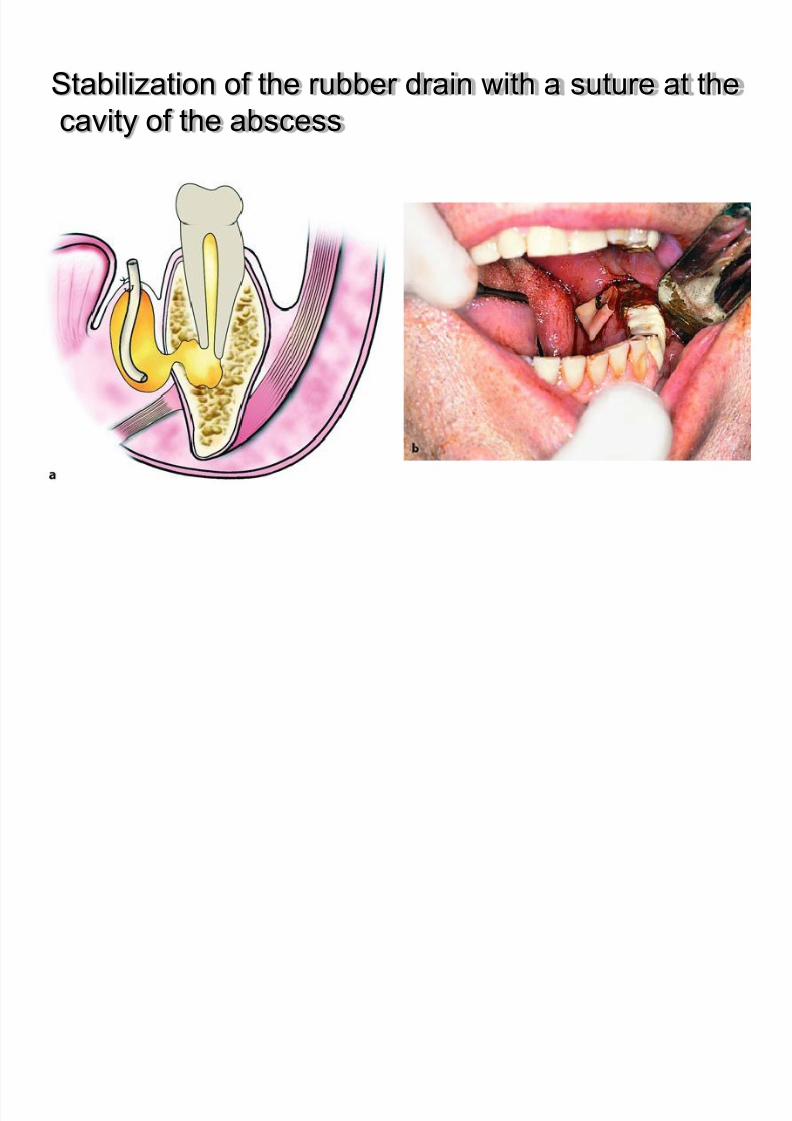
Stabilization of the rubber drain with a suture at the
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 119/183
Stabilization of the rubber drain with a suture at the
cavity of the abscess
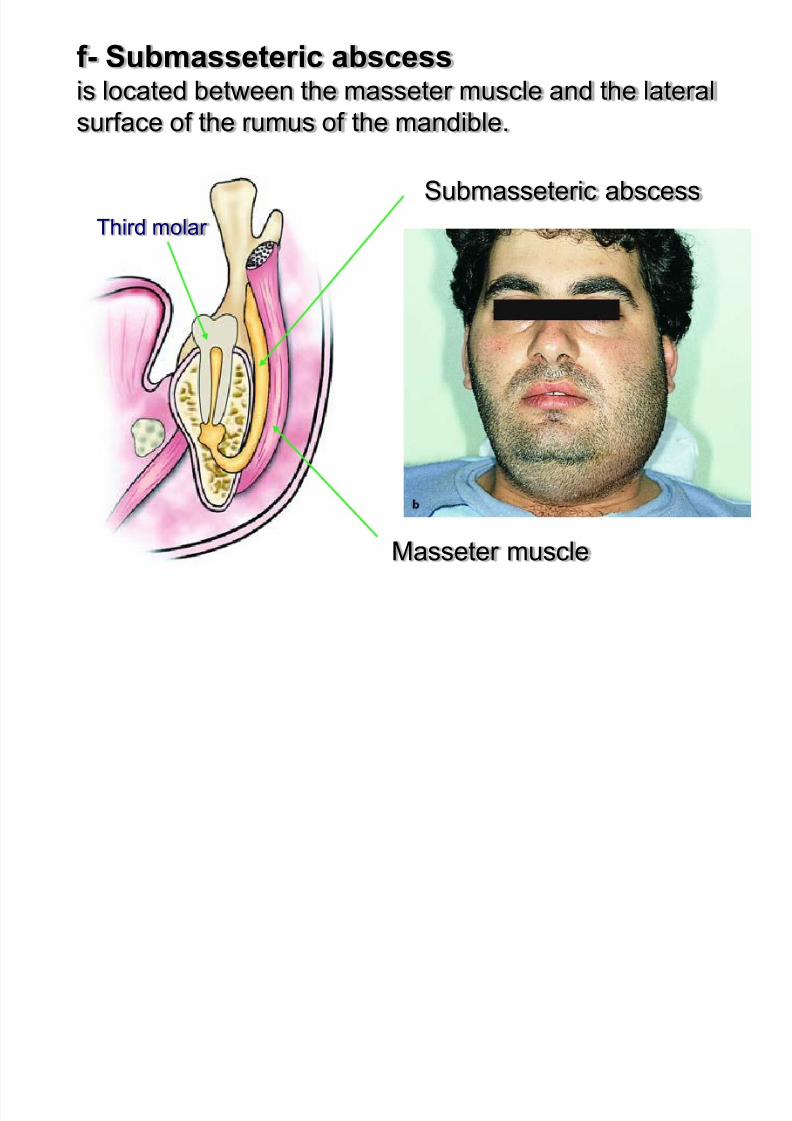
f- Submasseteric abscessis located between the masseter muscle and the lateral
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 120/183
is located between the masseter muscle and the lateral
surface of the rumus of the mandible.
Masseter muscle
Submasseteric abscess
Third molar
Masseteric Space
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 121/183
Masseteric Space
1-Located between lateral aspect of the mandible and
the masseter muscle
2-Involvement of this space generally occurs frombuccal space primary involvement
3-Signs of involvement of the masseteric space include
trismus and posterior-inferior face swelling
g- Pterygomandibulary abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 122/183
g yg y
Location :between medial aspect of the mandible and the medial
pterygoid muscle (communicates with infratemporal spaces)
Etiology :
- infection of mandibular third molars (pericoronitis)
- the result of an inferior alveolar nerve block
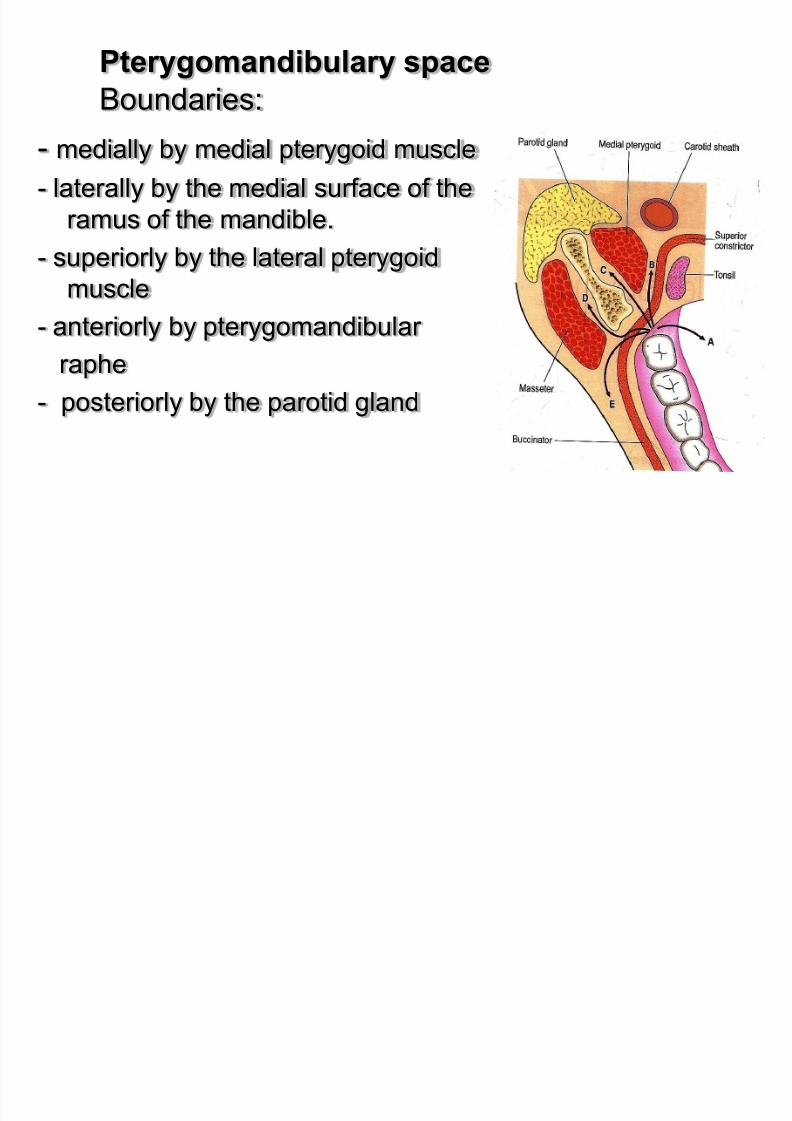
Pterygomandibulary space B d i
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 123/183
Boundaries:
- medially by medial pterygoid muscle- laterally by the medial surface of the
ramus of the mandible.
- superiorly by the lateral pterygoid
muscle- anteriorly by pterygomandibular
raphe
- posteriorly by the parotid gland
P tid l d
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 124/183
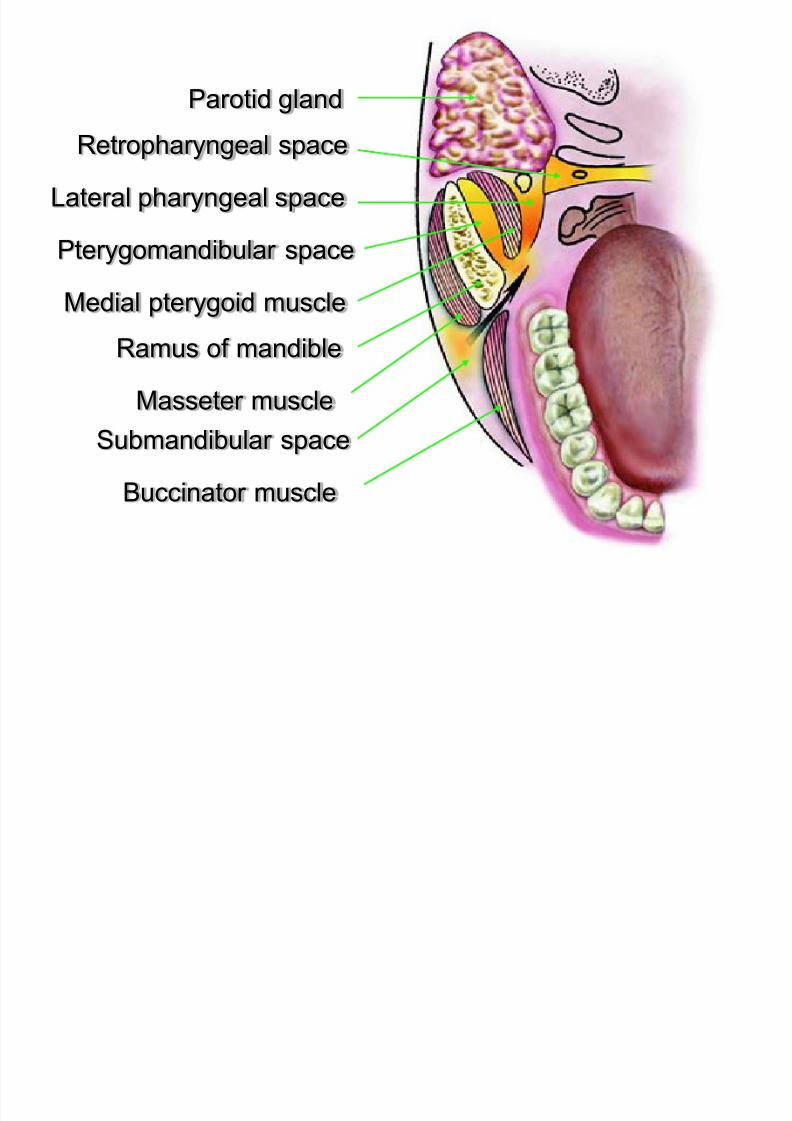
Parotid gland
Retropharyngeal space
Medial pterygoid muscle
Pterygomandibular space
Masseter muscle
Ramus of mandible
Lateral pharyngeal space
Submandibular space
Buccinator muscle
Clinical :
t i d li ht t l d b th th
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 125/183
- severe trismus and slight extraoral edema beneath the
angle of the mandible
- edema of the soft palate
- displacement of the uvula and lateral pharyngeal wall
- difficulty in swollowing
Treatment :
The incision for drainage is performed on the mucosa of the
oral cavity and,more specifically,along the mesial temporal
crest.The incision must be 1,5 cm long and 3-4 mm deep.
Incision for drainage of a
pterygomandibular abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 126/183
pterygomandibular abscess
2ndary infection results from spread from the sublingual and
submandibular spaces
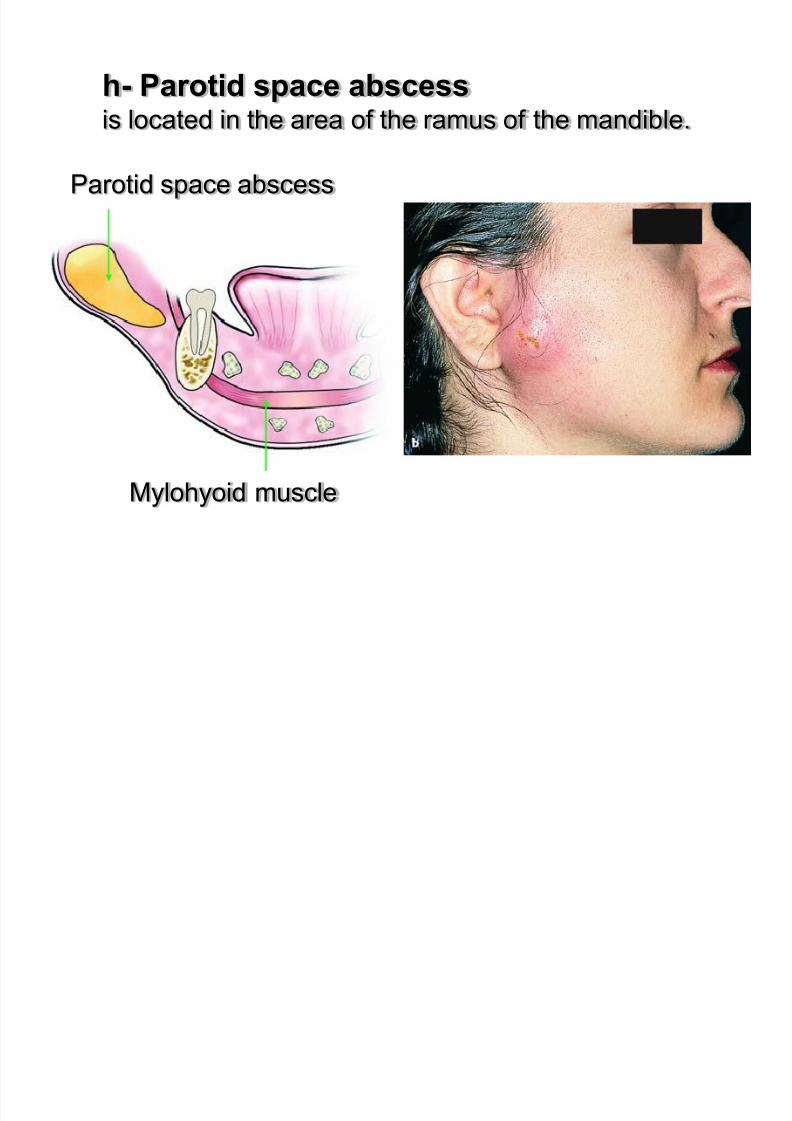
h- Parotid space abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 127/183
h Parotid space abscessis located in the area of the ramus of the mandible.
Mylohyoid muscle
Parotid space abscess
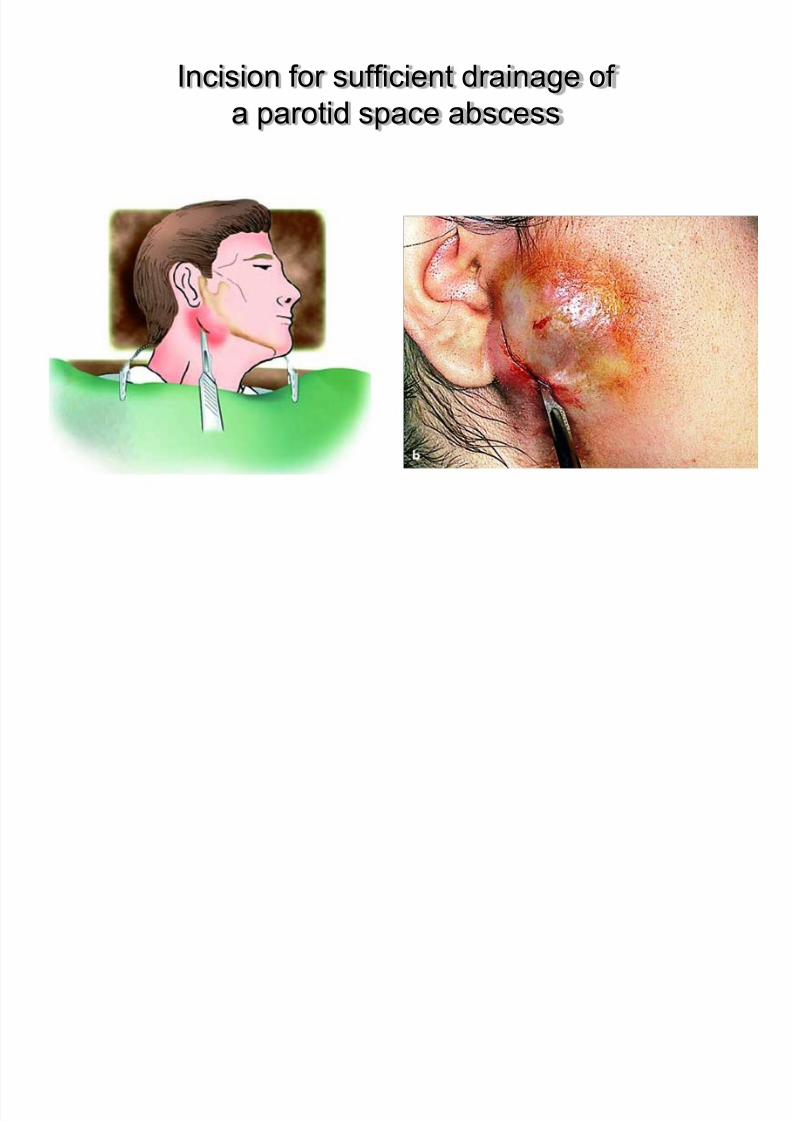
Incision for sufficient drainage of
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 128/183
a parotid space abscess
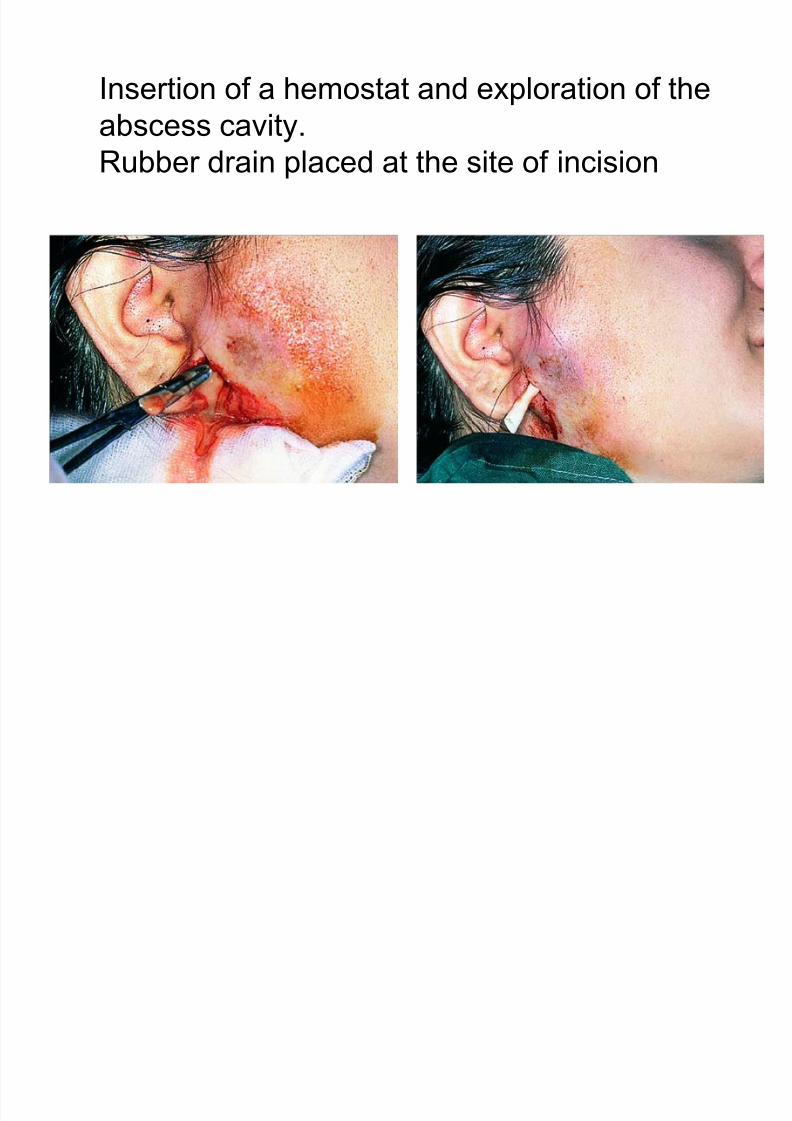
Insertion of a hemostat and exploration of the
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 129/183
Insertion of a hemostat and exploration of the
abscess cavity.
Rubber drain placed at the site of incision
Temporal Space
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 130/183
1-Location: posterior and superior to the masseteric and
pterygomandibular spaces
2-Bounded laterally by the temporalis fascia and
medially by the temporal bone
3-Two components :
1. Superficial temporal space: located between temporal
fascia and temporalis muscle
2. Deep temporal space: located between the temporalis
muscle and the temporal bone
1. Continuous with the infratemporal space
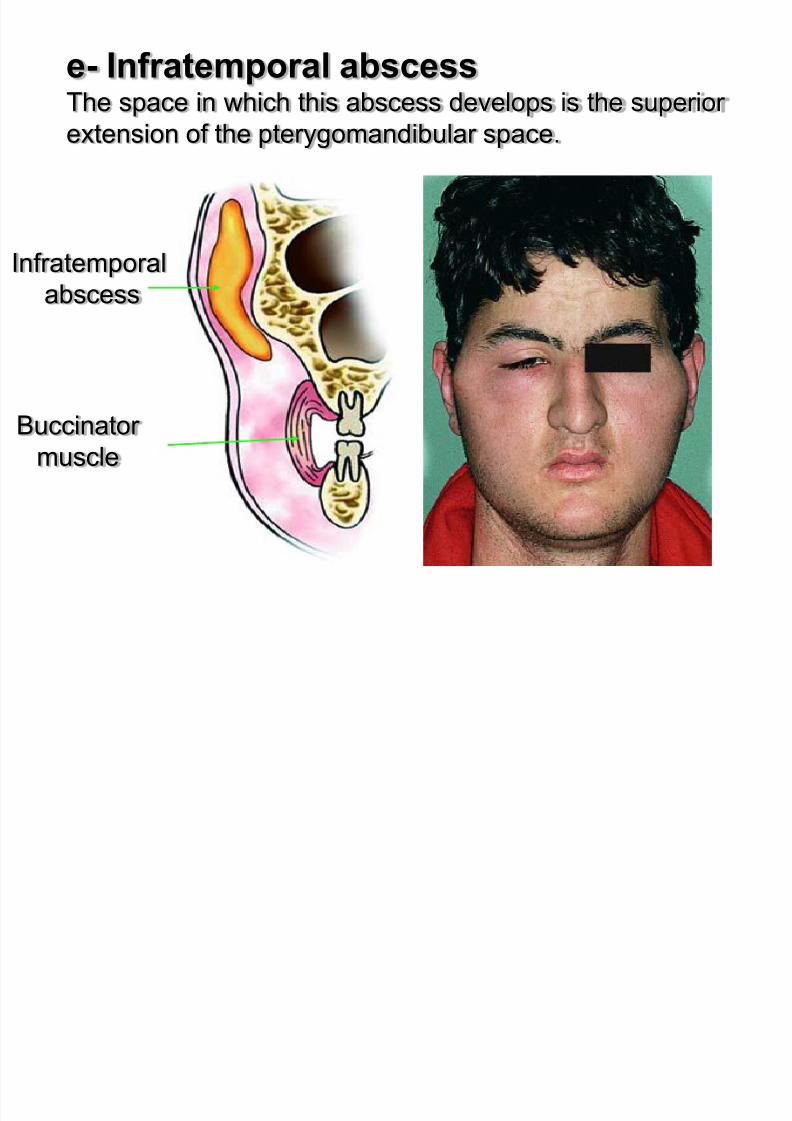
e- Infratemporal abscessTh i hi h thi b d l i th i
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 131/183
The space in which this abscess develops is the superior
extension of the pterygomandibular space.
Infratemporal
abscess
Buccinator muscle
Infratemporal Space
1 Location: posterior to the maxilla
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 132/183
1-Location: posterior to the maxilla
2-Boundaries:
1. Medial : lateral plate of the pterygoid process of the sphenoid
bone
2. Superior : skull base
3. Lateral : infratemporal space is continuous with the deeptemporal space
3-Rare involvement with odontogenic infections, but when
occurs related to 3rd
maxillary molar infections
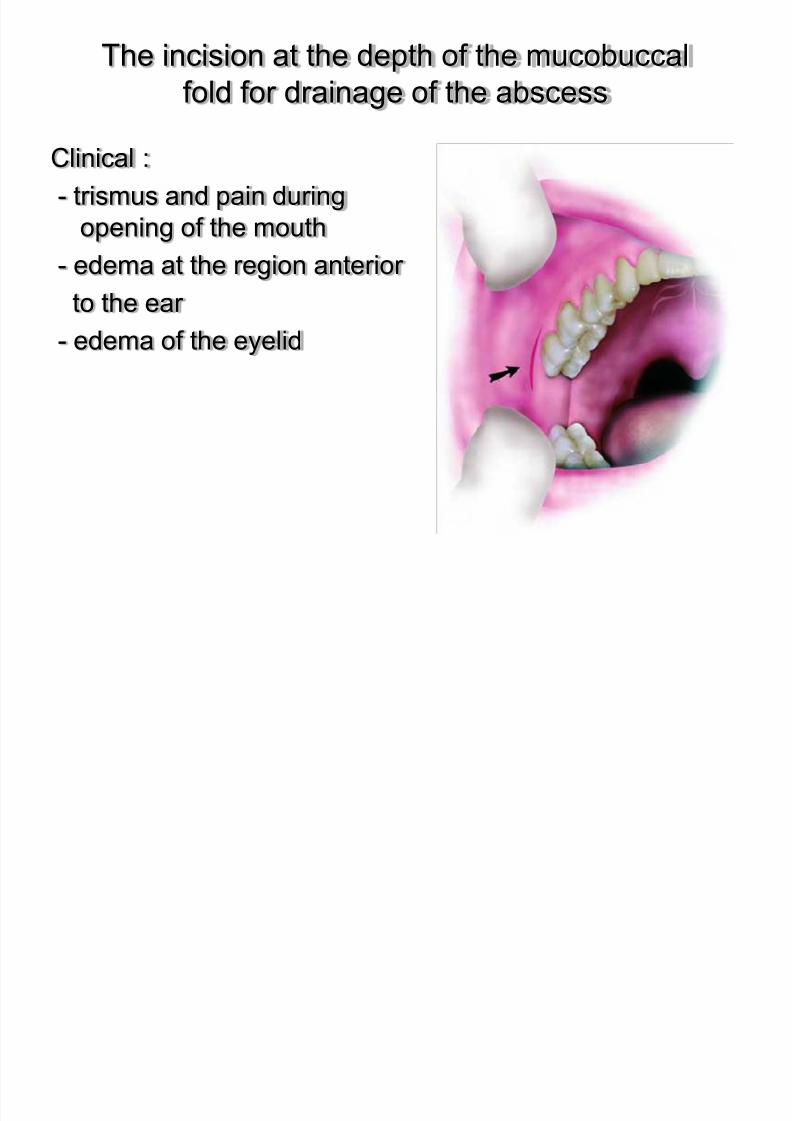
The incision at the depth of the mucobuccal
fold for drainage of the abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 133/183
fold for drainage of the abscess
Clinical :- trismus and pain during
opening of the mouth
- edema at the region anterior
to the ear
- edema of the eyelid
III- High Severity
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 134/183
Cellulitis (Phlegmon) Ludwig’s angina
Lateral Pharyngeal Space Abscess
Retropharyngeal Abscess
Cellulitis (Phlegmon)
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 135/183
Anatomic Location. This condition is an acute, diffuse inflammatory infiltration
of the loose connective tissue found underneath the skin.
It is believed today that cellulitis and phlegmon areinterchangeable terms.
The term cellulitis has prevailed and so the term phlegmon
has just about been abandoned.
Etiology.
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 136/183
It may be the result of any infected tooth and is usuallydue to a mixed infection.
The microorganisms thought to be responsible are
aerobic and anaerobic streptococci and staphylococci.
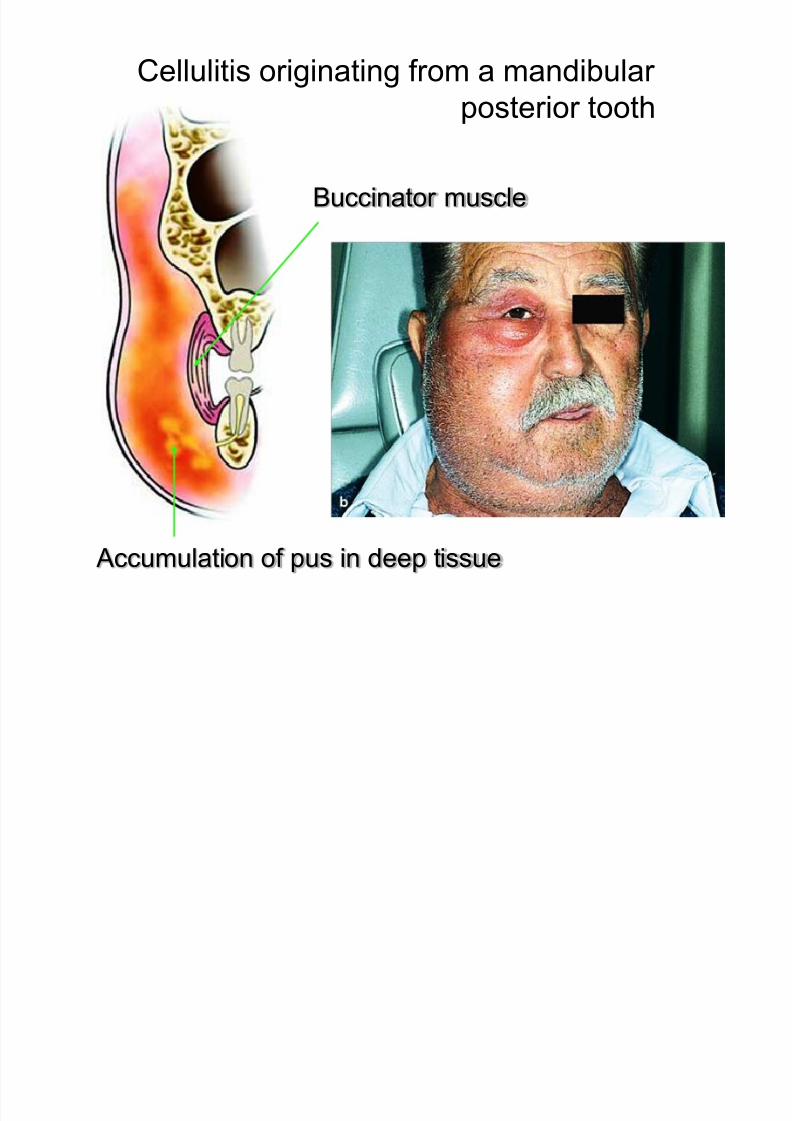
Cellulitis originating from a mandibular
t i t th
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 137/183
posterior tooth
Accumulation of pus in deep tissue
Buccinator muscle
Clinical :
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 138/183
extensive swelling of the right side, resulting in severe
disfigurement of the face Edema.The edema may present in various areas of the
face and its localization depends on the infected tooth
responsible.
headache reddish skin.
In the initial stage, cellulitis feels soft or doughy during
palpation, without pus present, while in more advanced
stages, a board-like induration appears,whichmay leadto suppuration.
At this stage, the pus is localized in small focal sites in
th d ti
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 139/183
the deep tissue.
Treatment :
large doses of antibiotics are administered (penicillin or
ampicillin parenterally).
Drainage may be performed in one or more sites tofacilitate evacuation of the exudate.
In grave cases admission of the patient to a hospital is
recommended.
Cellulitis
Diff ll liti

8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 140/183
Diffuse cellulitis
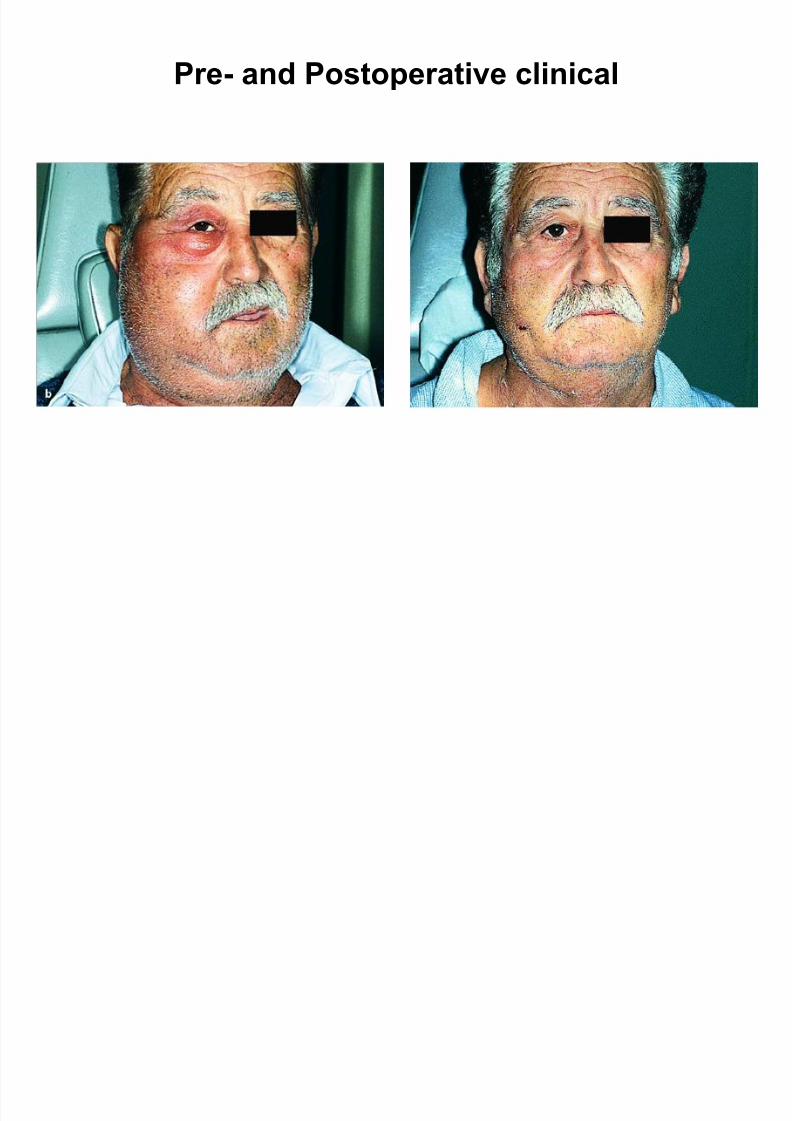
Pre- and Postoperative clinical
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 141/183
Pre-and Postoperative clinical

8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 142/183
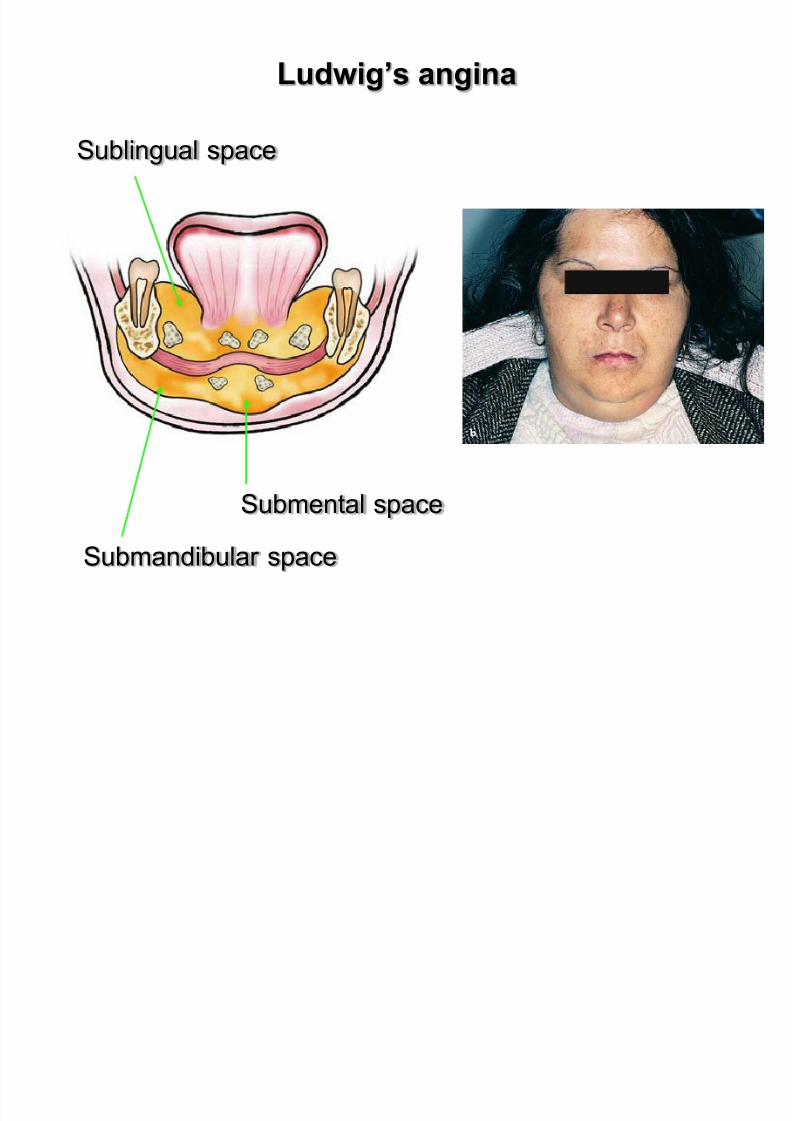
Ludwig’s angina
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 143/183
Ludwig’s Angina is a grave acute cellular infection and ischaracterized by bilateral involvement of the submandibular
and sublingual spaces as well as the submental space.
Abstract Ludwig’s Angina is a rapid progressive cellulitisof the submandibular , sublingual and submental spaces,with potential for significant upper airway obstruction.
First described by Wilhelm Fredrick Von Ludwig in 1836,
then by Camerer in 1837.
Ludwig’s angina
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 144/183
Submandibular space
Sublingual space
Submental space
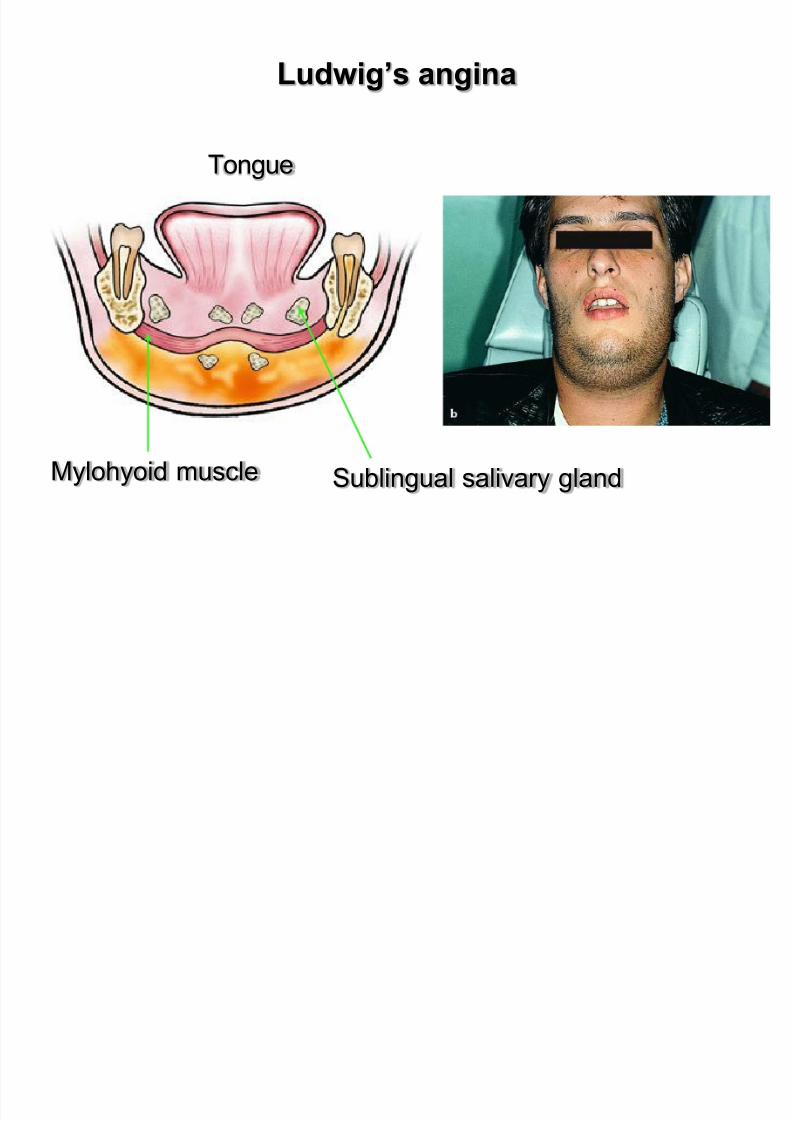
Ludwig’s angina
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 145/183
Tongue
Mylohyoid muscle Sublingual salivary gland
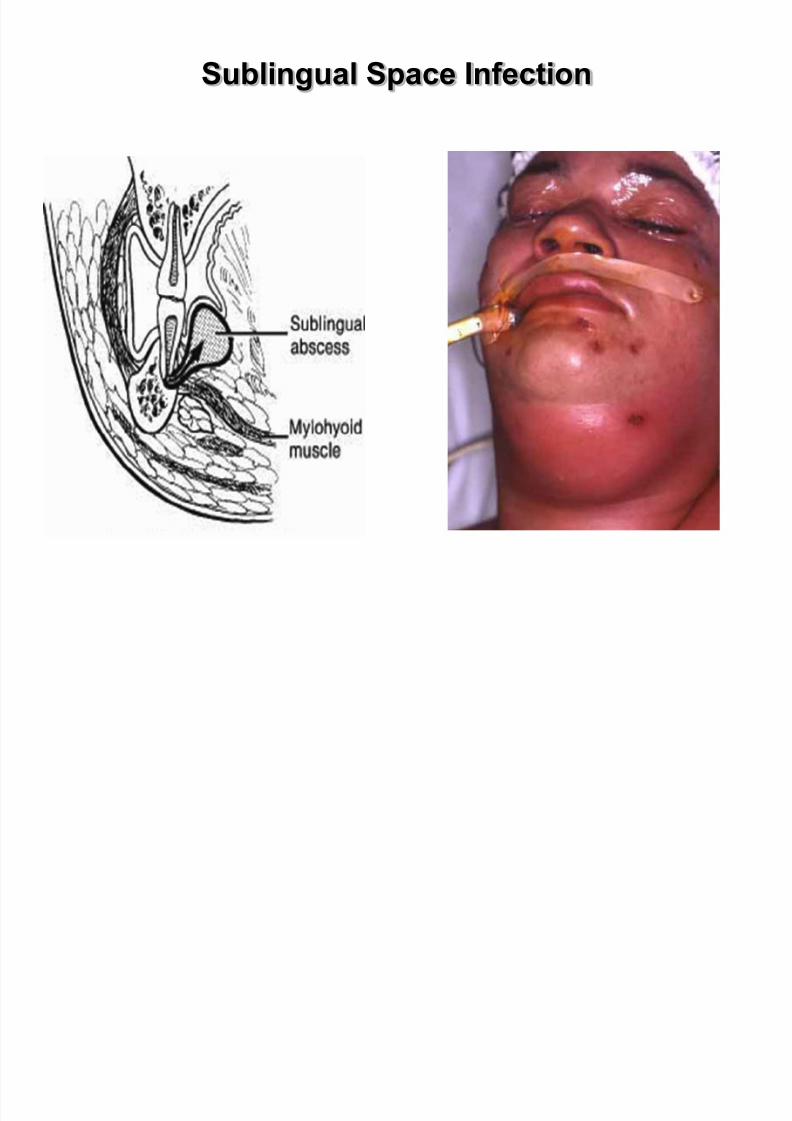
Sublingual Space Infection
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 146/183
Ludwig’s angina
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 147/183
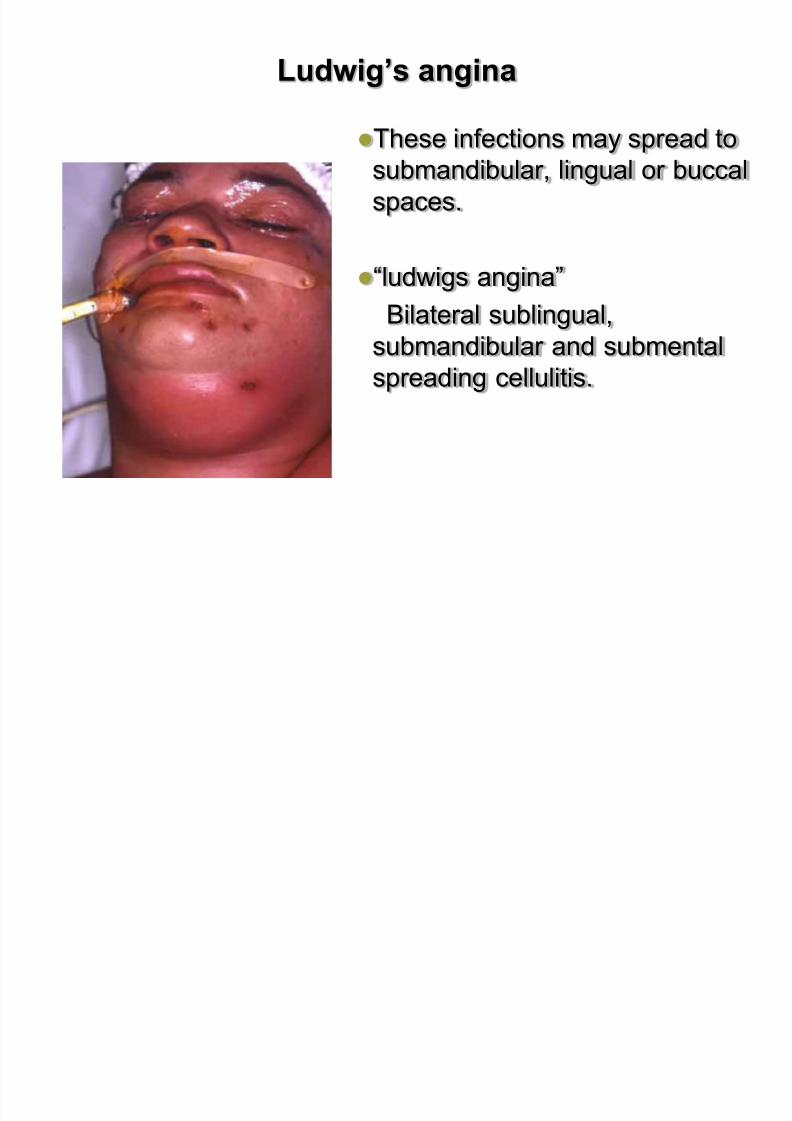
These infections may spread to
submandibular, lingual or buccalspaces.
“ludwigs angina”
Bilateral sublingual,
submandibular and submental
spreading cellulitis.
Etiology.
The most frequent cause of the disease is
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 148/183
The most frequent cause of the disease is
periapical or periodontal infection of mandibular
teeth, especially of those whose apices are found beneath
the mylohyoid muscle.
Clinical. Severe pain
severe difficulty in swallowing, speaking and breathing,
drooling of saliva
elevated temperature
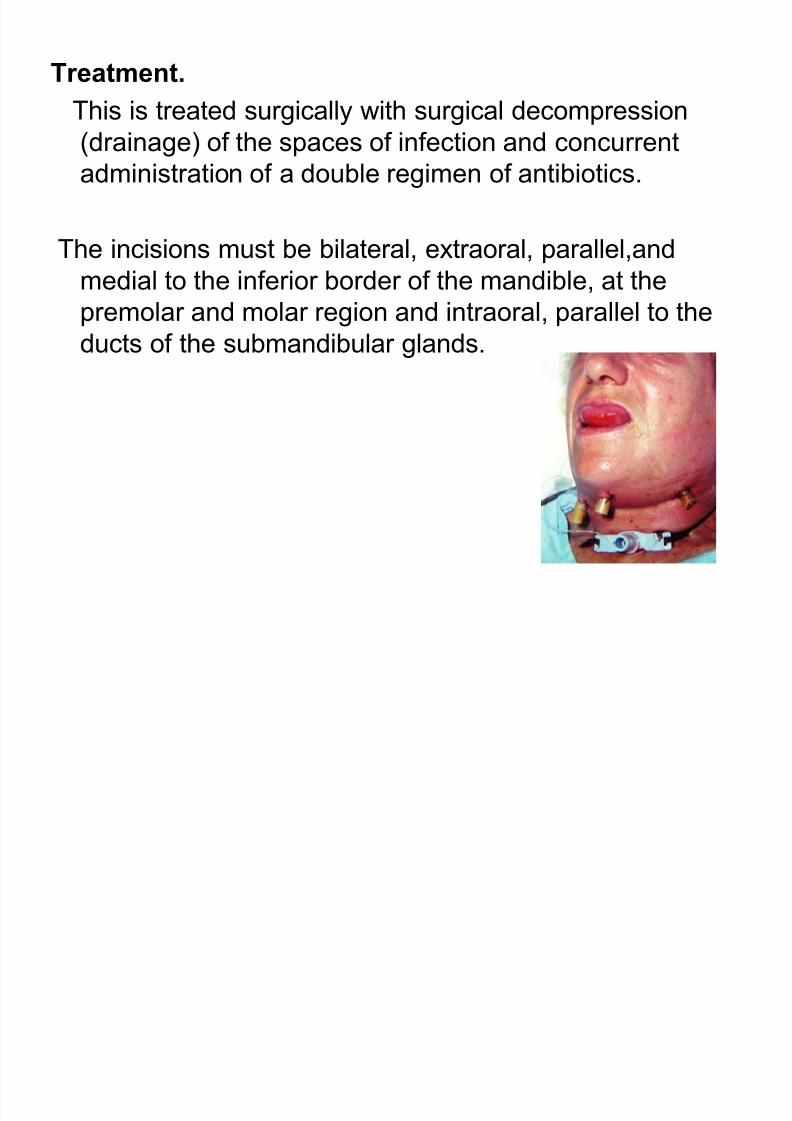
Treatment.
This is treated surgically with surgical decompression
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 149/183
This is treated surgically with surgical decompression
(drainage) of the spaces of infection and concurrent
administration of a double regimen of antibiotics.
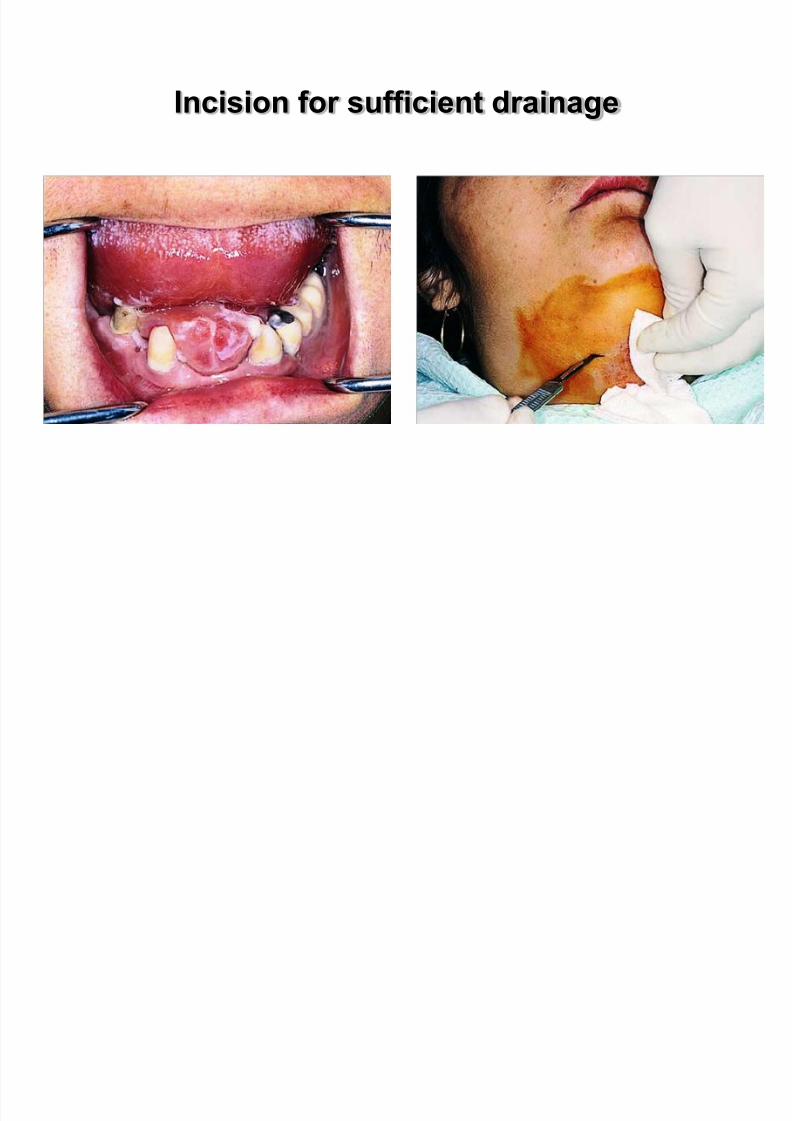
The incisions must be bilateral, extraoral, parallel,and
medial to the inferior border of the mandible, at the
premolar and molar region and intraoral, parallel to the
ducts of the submandibular glands.
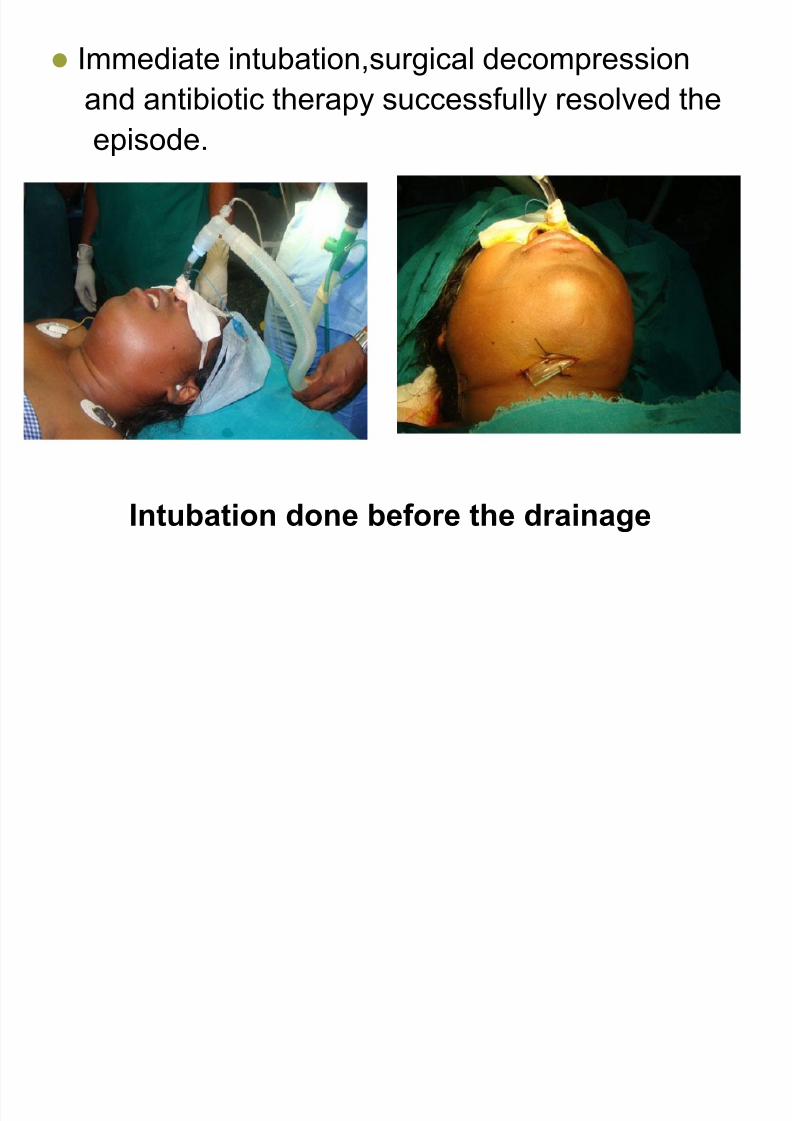
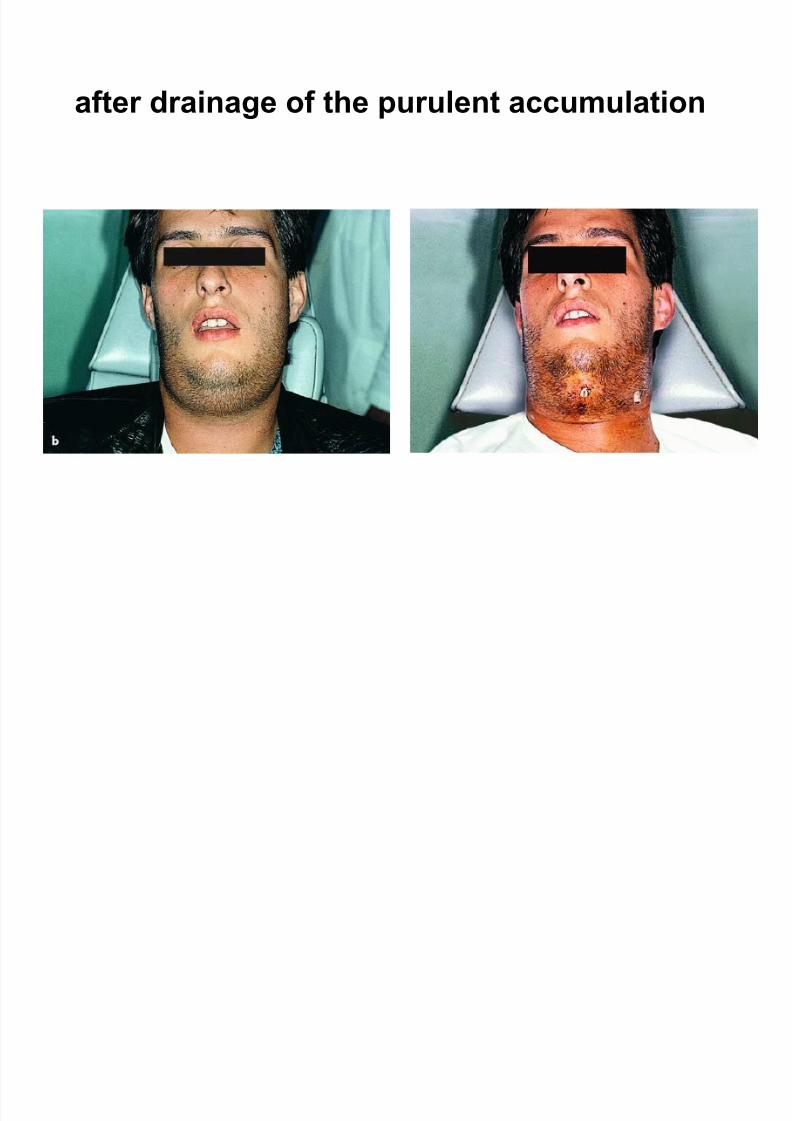
Immediate intubation,surgical decompression
and antibiotic therapy successfully resolved the
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 150/183
Intubation done before the drainage
a d a t b ot c t e apy success u y eso ed t e
episode.
Incision for sufficient drainage
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 151/183
Incision for sufficient drainage
Pre-and Postoperative clinical

8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 152/183
Pre and Postoperative clinical
after drainage of the purulent accumulation
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 153/183
after drainage of the purulent accumulation
Masseteric, pterygomandibular, and temporal spaces
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 154/183
p yg p p
referred to as masticator space due to delineation by
the muscles of mastication
1. Communicate freely with one another and are
simultaneously involved
Primary Maxillary Spaces
C i S
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 155/183
Canine Space
1. Location: between the levator anguli oris and thelevator labii superioris muscles
2. Involvement primarily due to maxillary canine toothinfection
3. Long root allows erosion through the alveolar bone of
the maxilla4. Signs:
1. Obliteration of the nasolabial fold
2. Superior extension can involve lower eyelid
Buccal Space1. Posterior maxillary teeth are source of most buccal
space infections
2. Results when infection erodes through bone superior to attachment of buccinator muscle
Deep Neck Spaces
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 156/183
Extension of odontogenic infections beyond the primary
spaces of maxilla and mandible is uncommon.
When occurs upper airway compromise and descending
mediastinitis are possible adverse sequelae.
Posterior spread of ptyerygomandibular space infection is
to lateral pharyngeal space.
Lateral Pharyngeal space
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 157/183
Shape of an inverted cone with its base at the skullbase and its apex at the hyoid bone.
Location: medial to the medial pterygoid muscle and
lateral to the superior pharyngeal constrictor muscle.
Anterior: pterygomandibular raphe.
Posterior: prevertebral fascia.
Lateral pharyngeal space communicates with
t h l

8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 158/183
retropharyngeal space.
The styloid process separates posterior compartment of
the lateral pharyngeal space that contains the great
vessels from the anterior space.
Clinical presentation
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 159/183
1. Severe trismus
2. Lateral swelling of the neck3. Bulging of the lateral pharyngeal wall
4. Rapid progression of infection in this space is common
5. Posterior compartment involvement can result in
thrombosis of the internal jugular vein, erosion of thecarotid artery or its branches, and interference with
cranial nerves IX to XII
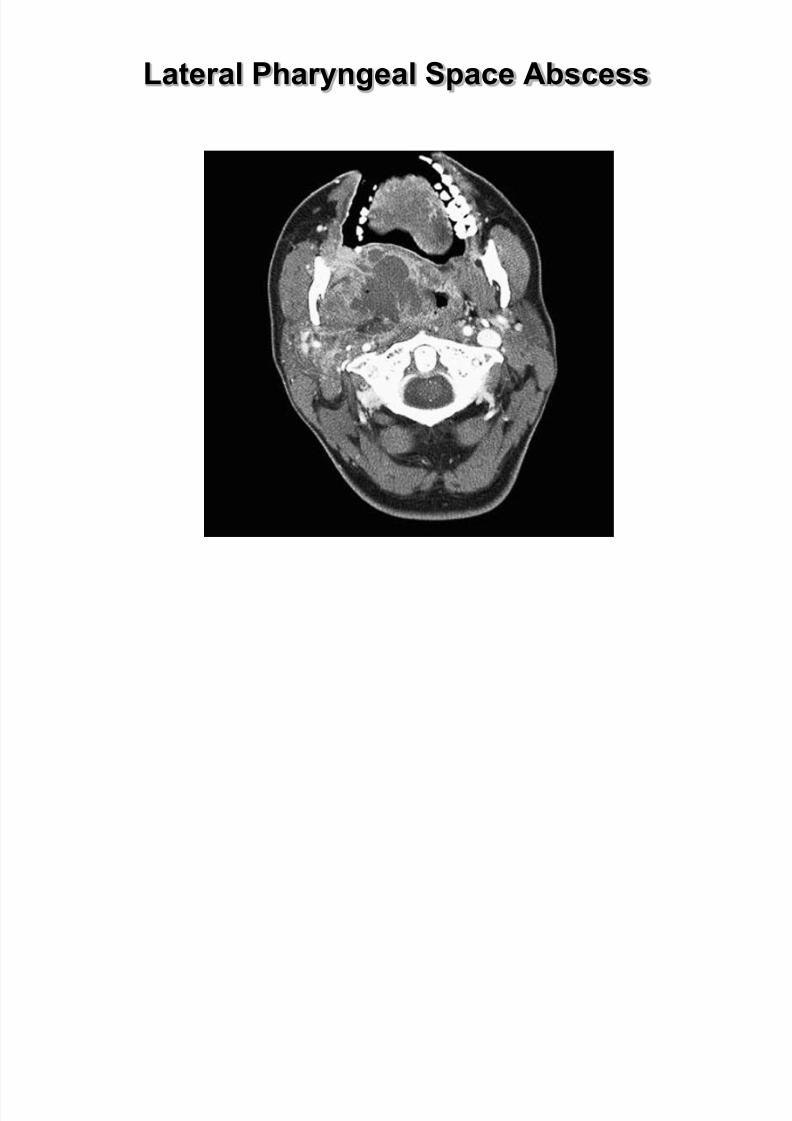
Lateral Pharyngeal Space Abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 160/183
Retropharyngeal Space
1. Posteromedial to lateral pharyngeal space and anterior
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 161/183
p y g p
to the prevertebral space
2. Anterior: superior pharyngeal constrictor muscle
3. Posterior: alar layer of prevertebral fascia
4. Extends from skull base superiorly to C7 to T1 inferiorly
5. Retropharyngeal space infections can spread to
mediastinum
6. Other complications of retropharyngeal space
involvement:
1. Airway obstruction
2. Aspiration of pus in the event of spontaneous rupture
3. Rupture can occur during endotracheal intubation
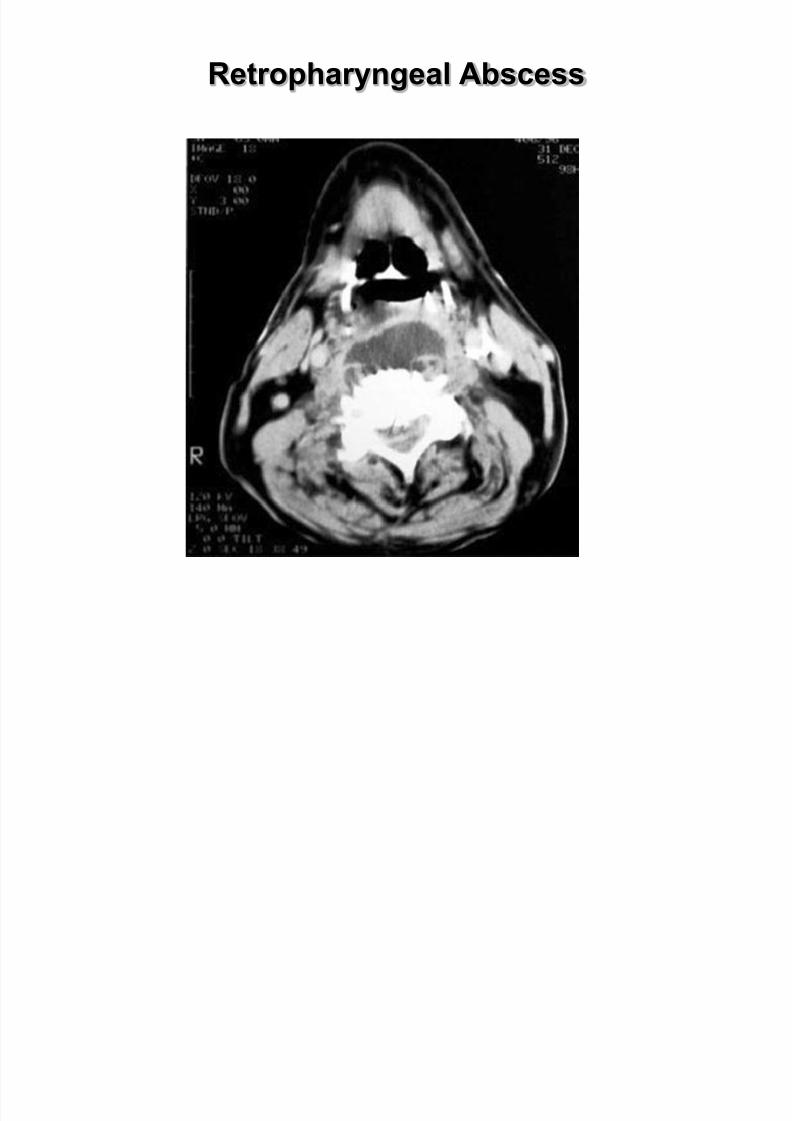
Retropharyngeal Abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 162/183
Prevertebral Space
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 163/183
Prevertebral Space
1. Potential space between two layers of prevertebralfascia (alar and prevertebral layers)
2. Extends from skull base superiorly to the diaphragm
inferiorly
3. Mediastinitis is concern with prevertebral spaceinfections similarly to retropharyngeal space infections
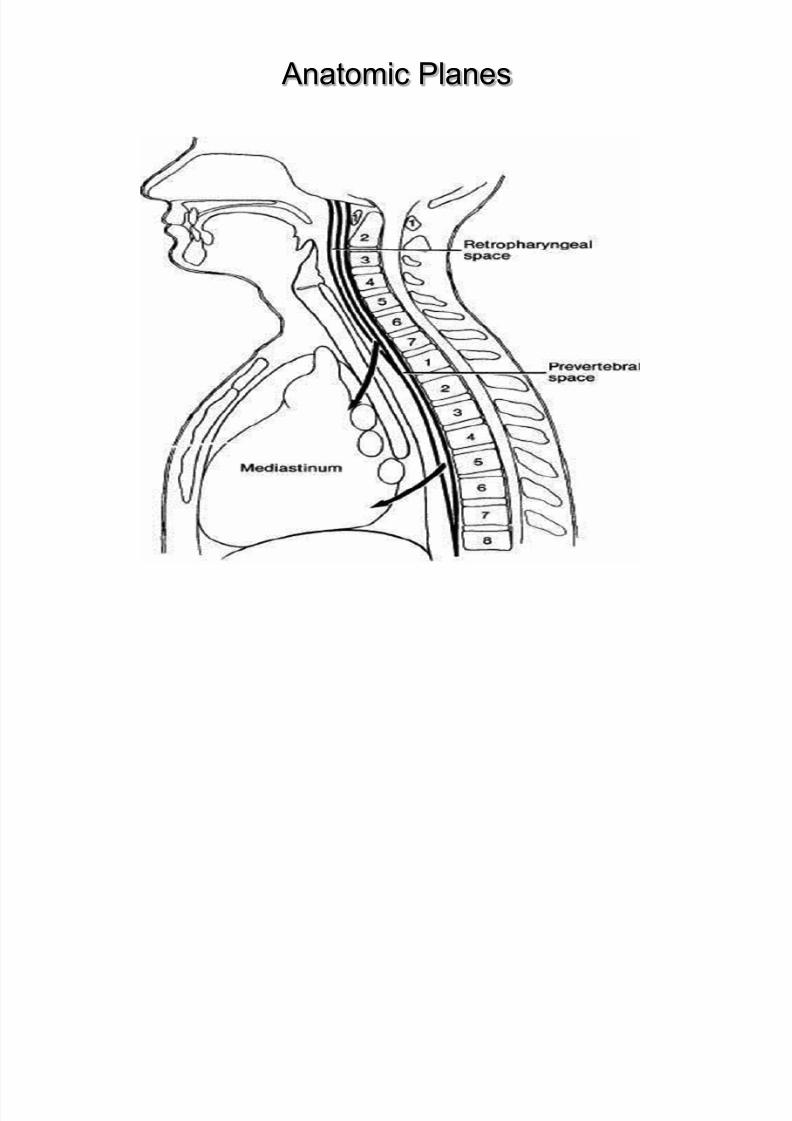
Anatomic Planes
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 164/183
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 165/183
Management of Odontogenic Infections
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 166/183
Goals of management of odontogenic infection:
1. Airway protection
2. Surgical drainage
3. Medical support of the patient4. Identification of etiologic bacteria
5. Selection of appropriate antibiotic therapy
Technique:
1 Small incision are made in a dependent area

8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 167/183
1. Small incision are made in a dependent area
2. Placement of a hemostat in the abscess cavity with entryinto all loculations of the abscess
3. Penrose drains inserted into cavity to allow for
postoperative drainage of the abscess
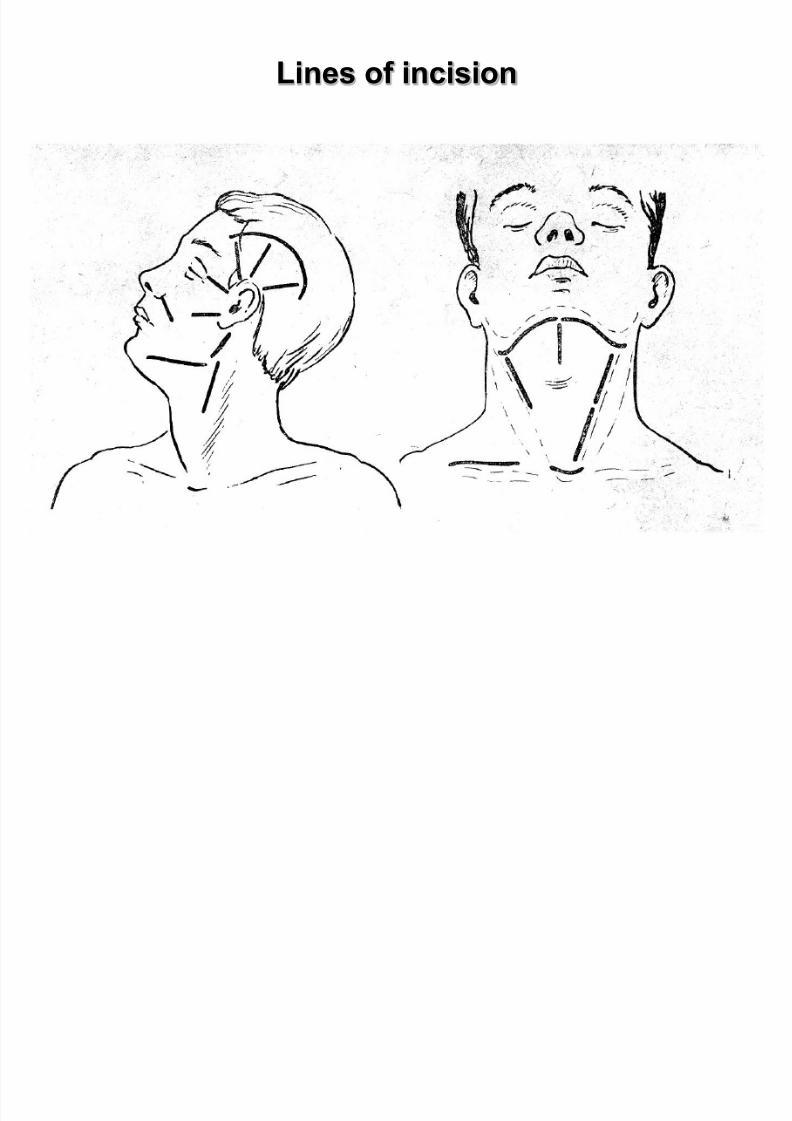
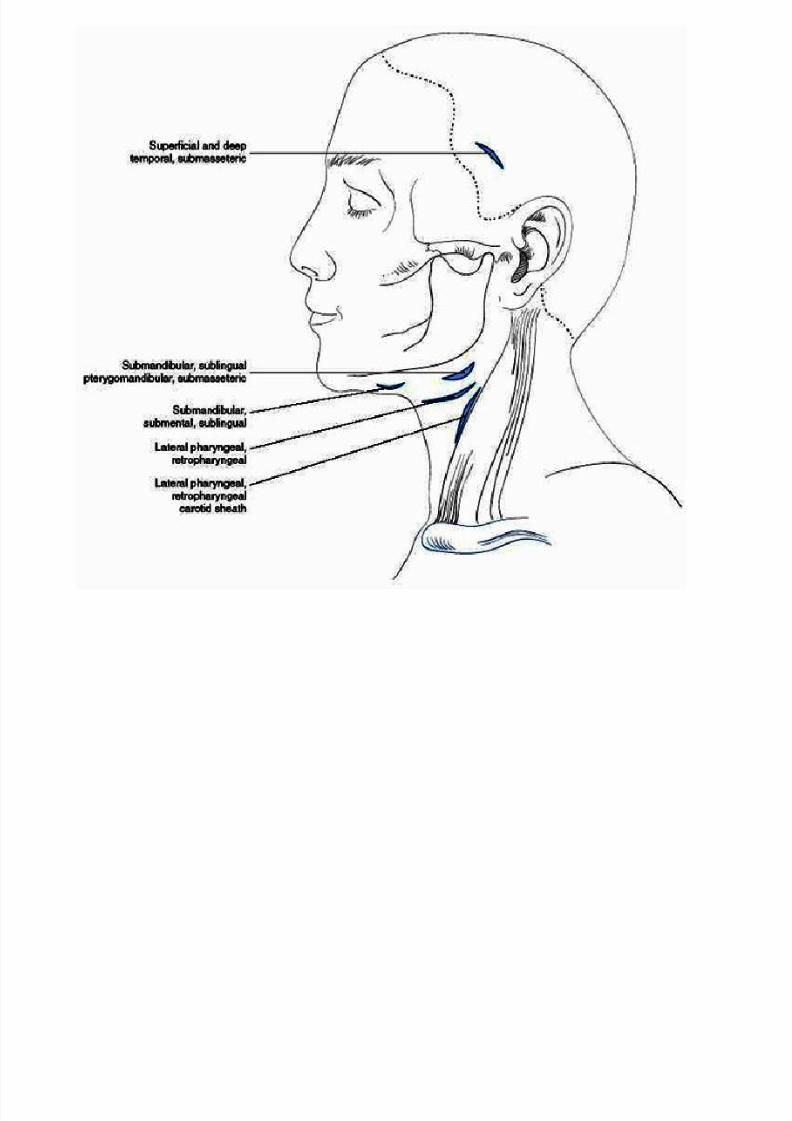
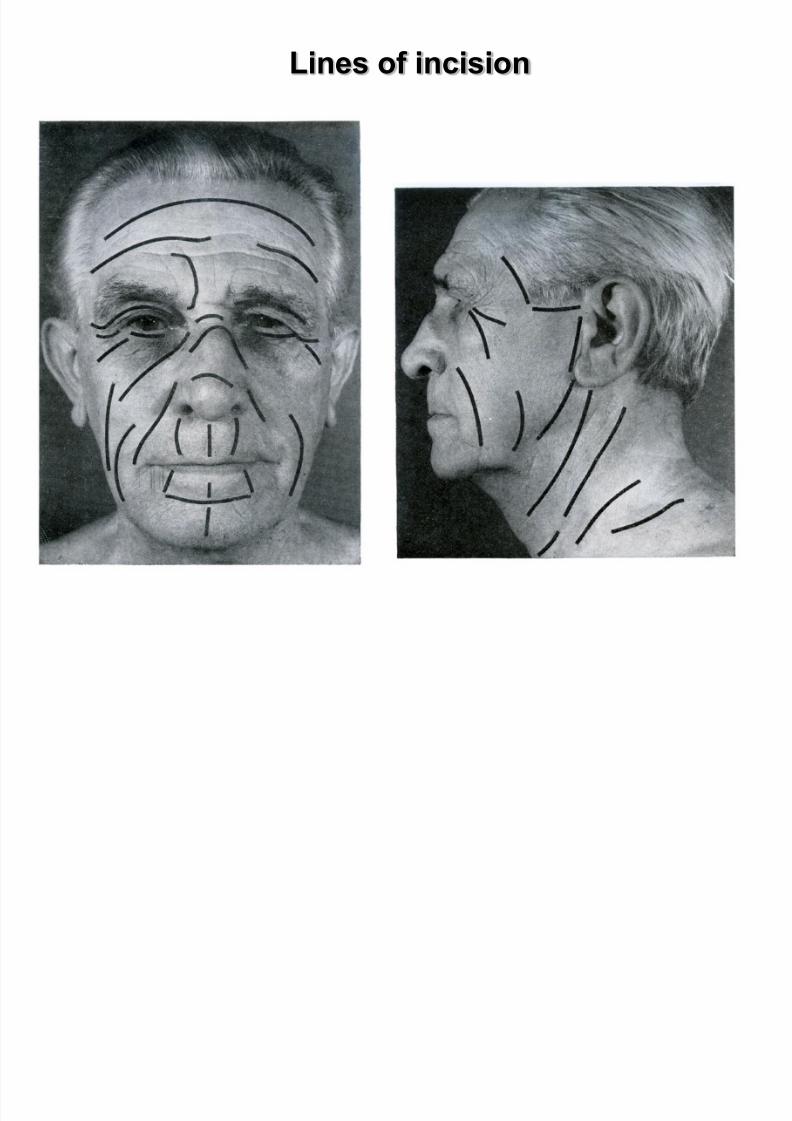
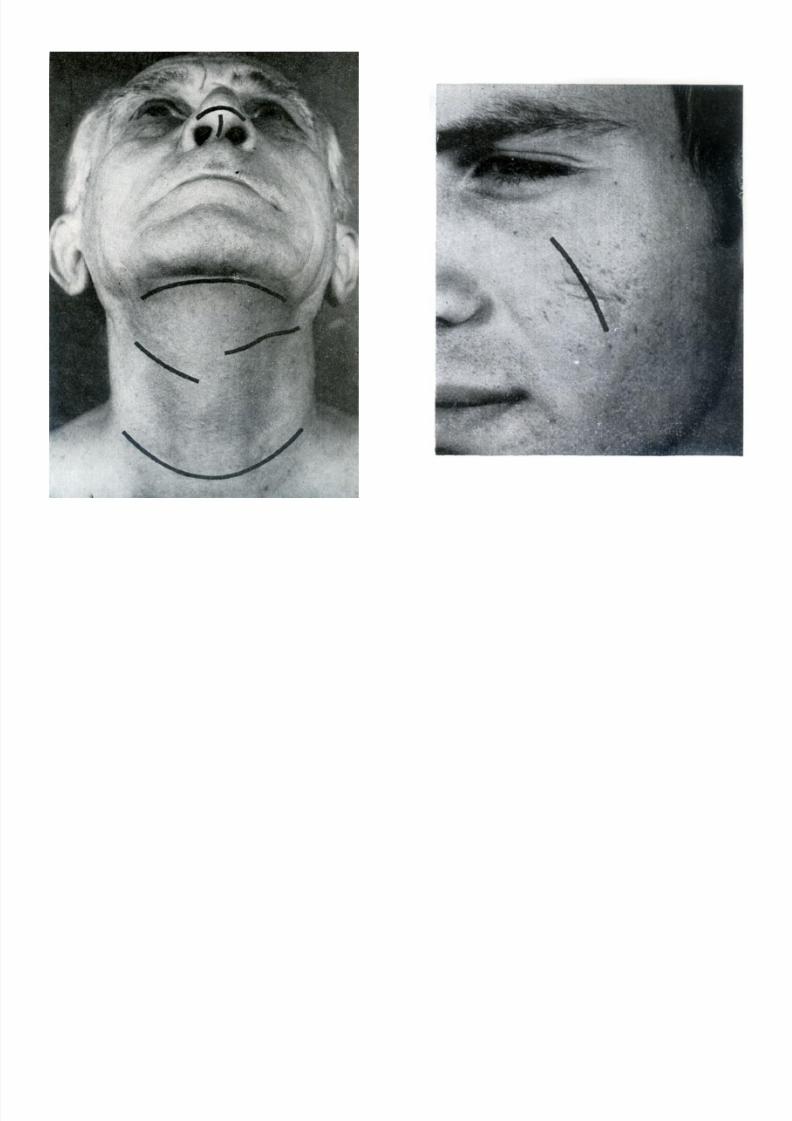
Lines of incision
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 168/183
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 169/183
Lines of incision
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 170/183
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 171/183
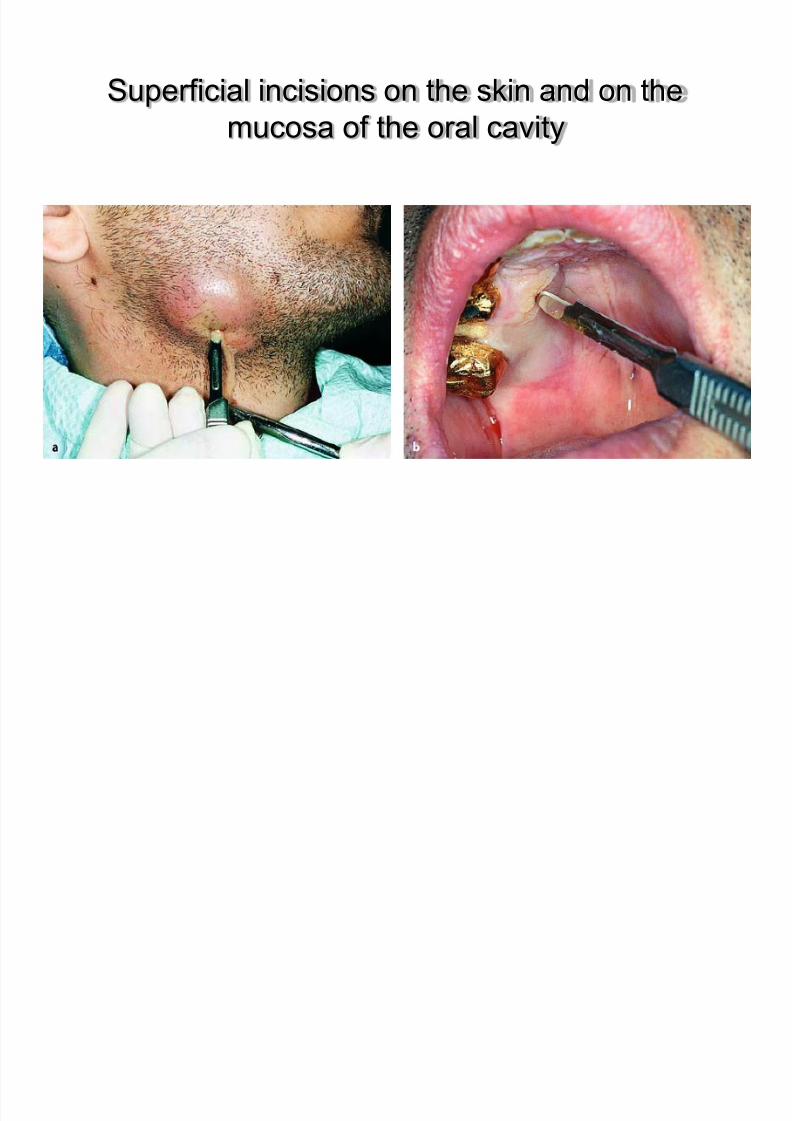
Superficial incisions on the skin and on the
mucosa of the oral cavity
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 172/183
mucosa of the oral cavity
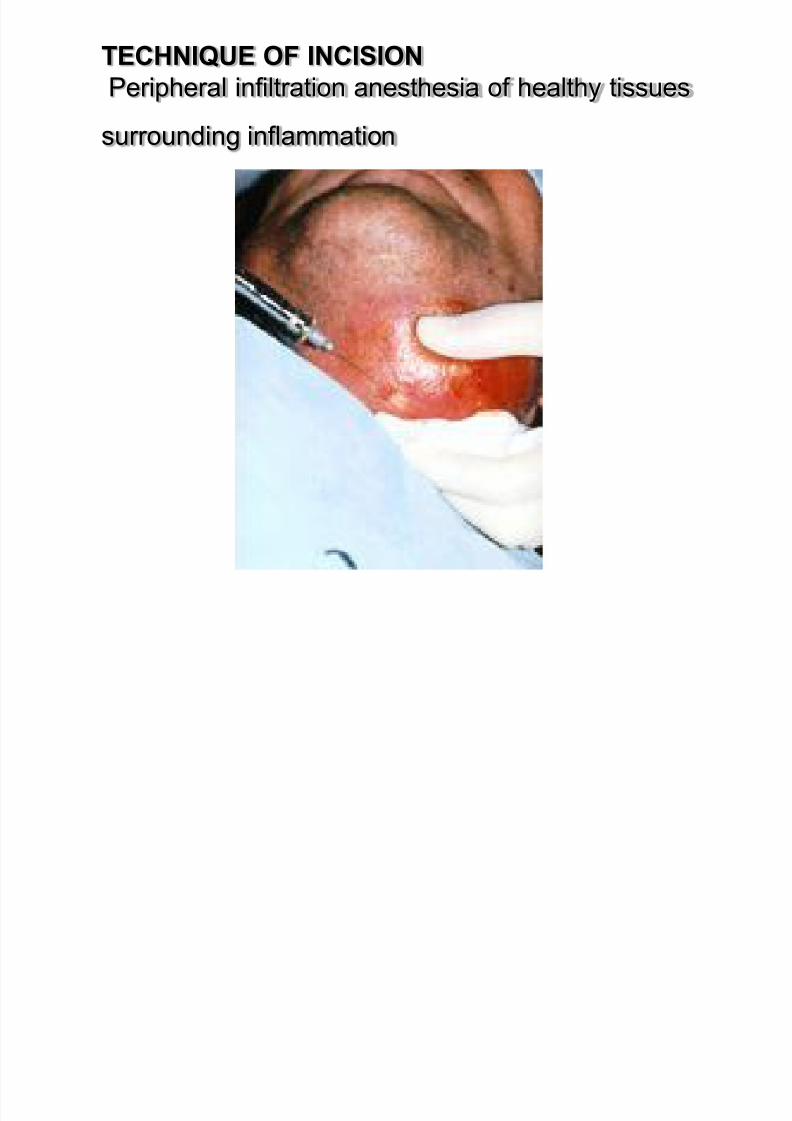
TECHNIQUE OF INCISION
Peripheral infiltration anesthesia of healthy tissues
di i fl ti
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 173/183
surrounding inflammation
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 174/183
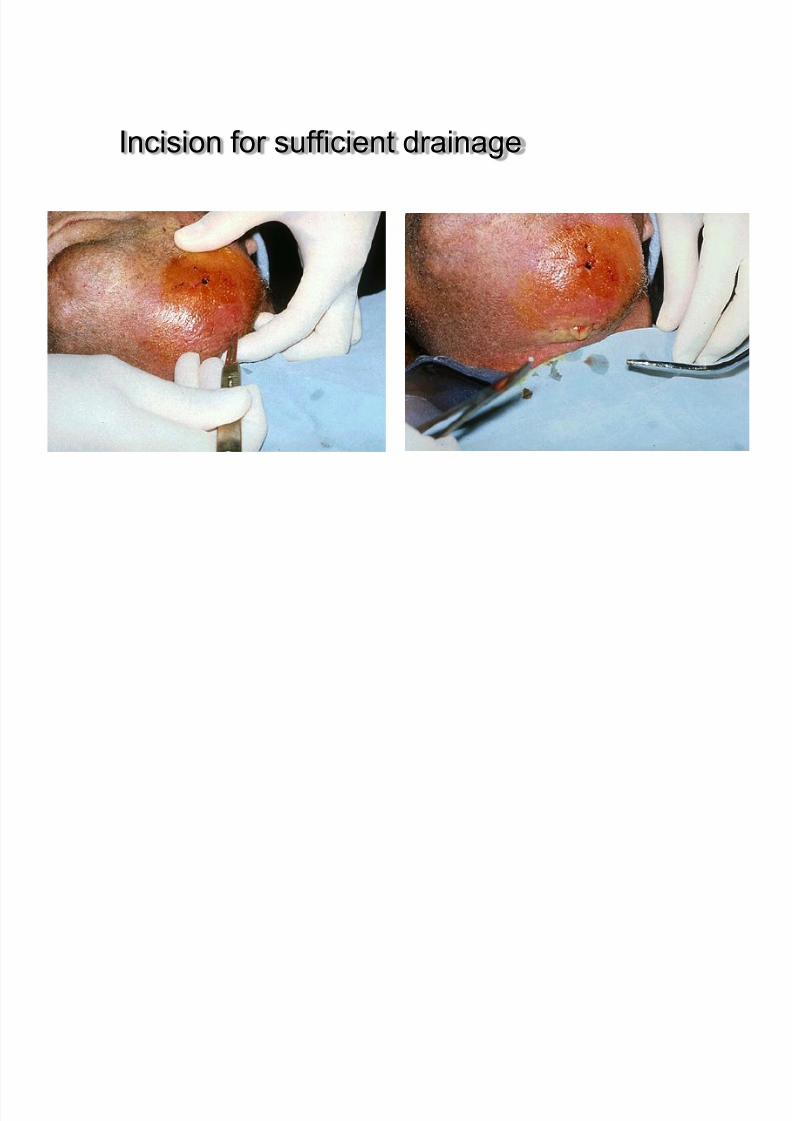
Incision for sufficient drainage
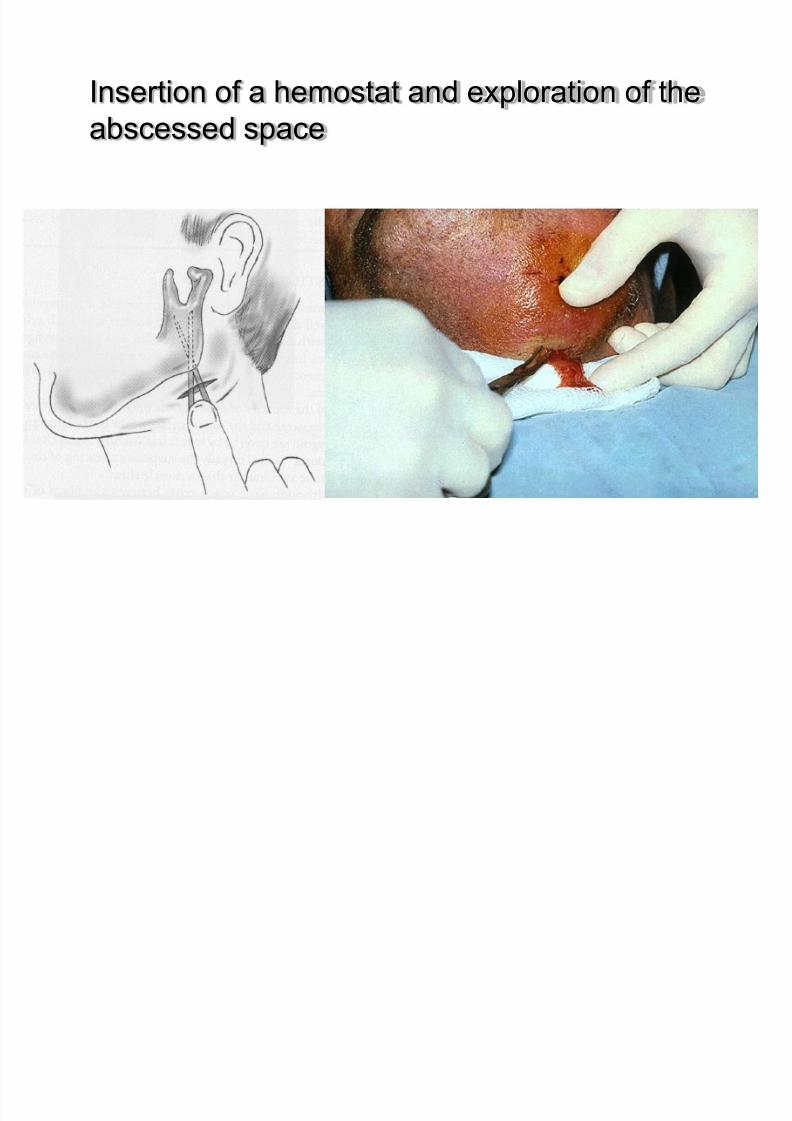
Insertion of a hemostat and exploration of the
abscessed space
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 175/183
abscessed space
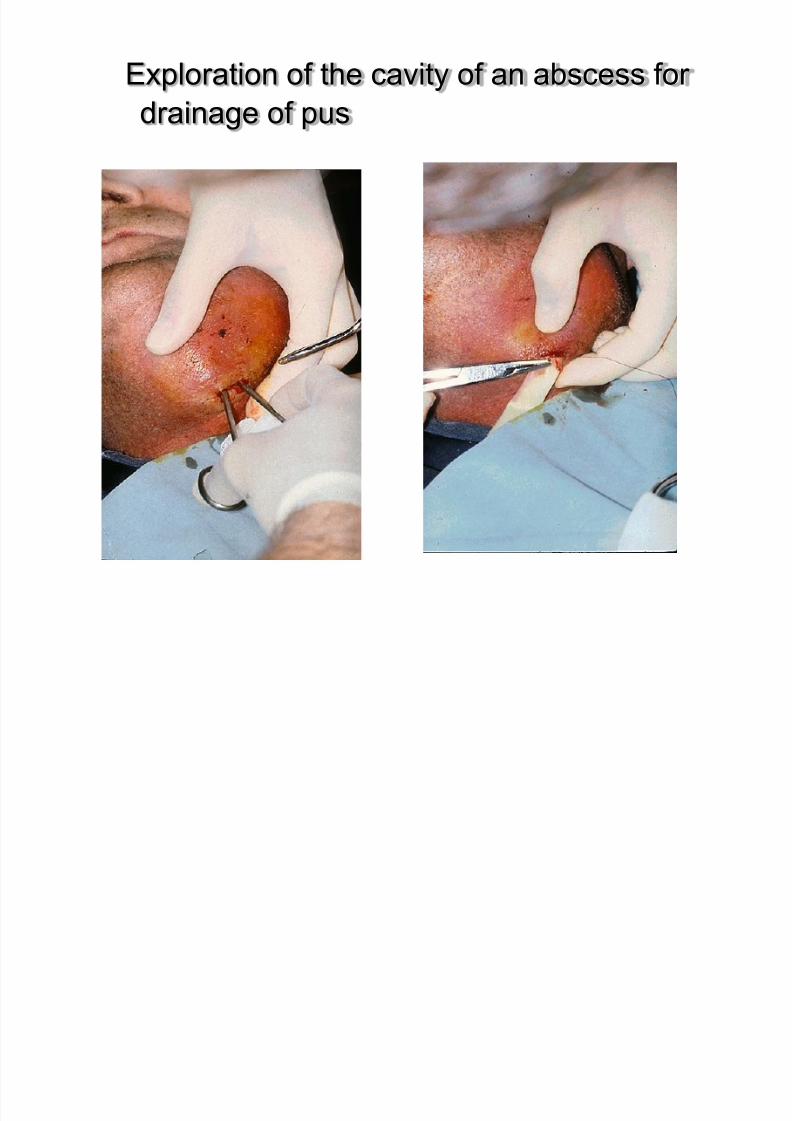
Exploration of the cavity of an abscess for
drainage of pus
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 176/183
g p
Rubber drain stabilized in position with suture.

8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 177/183
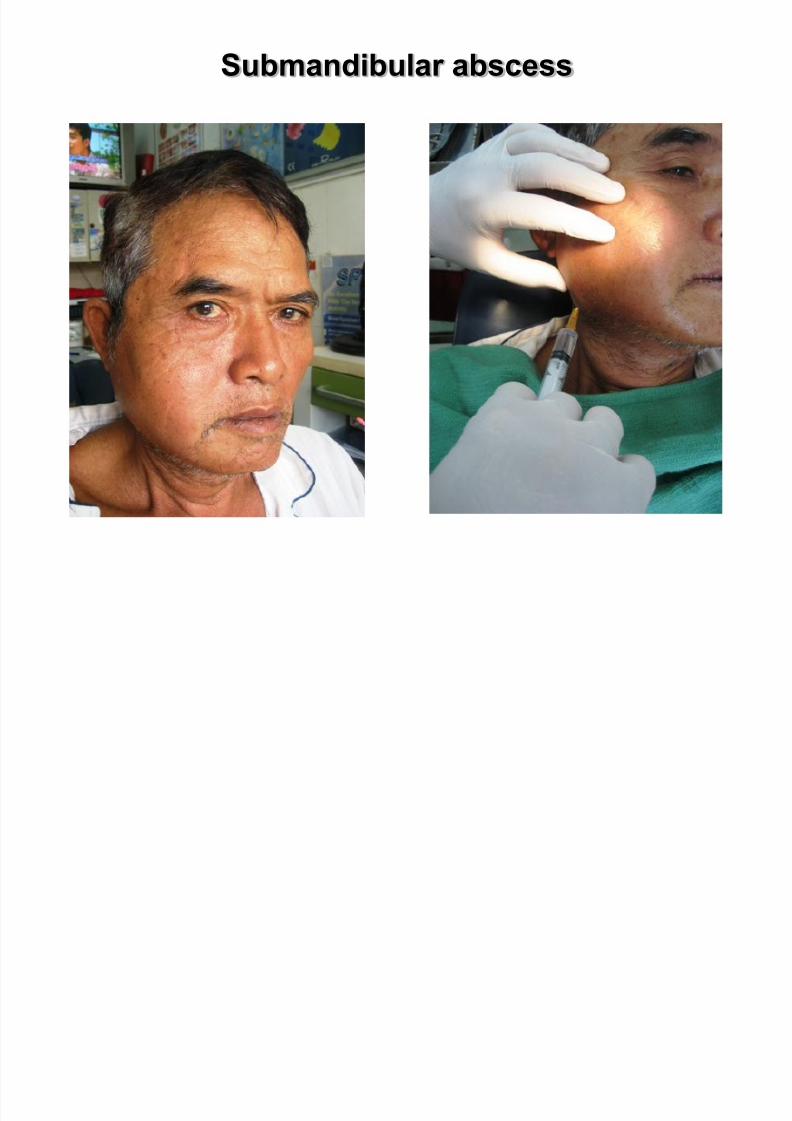
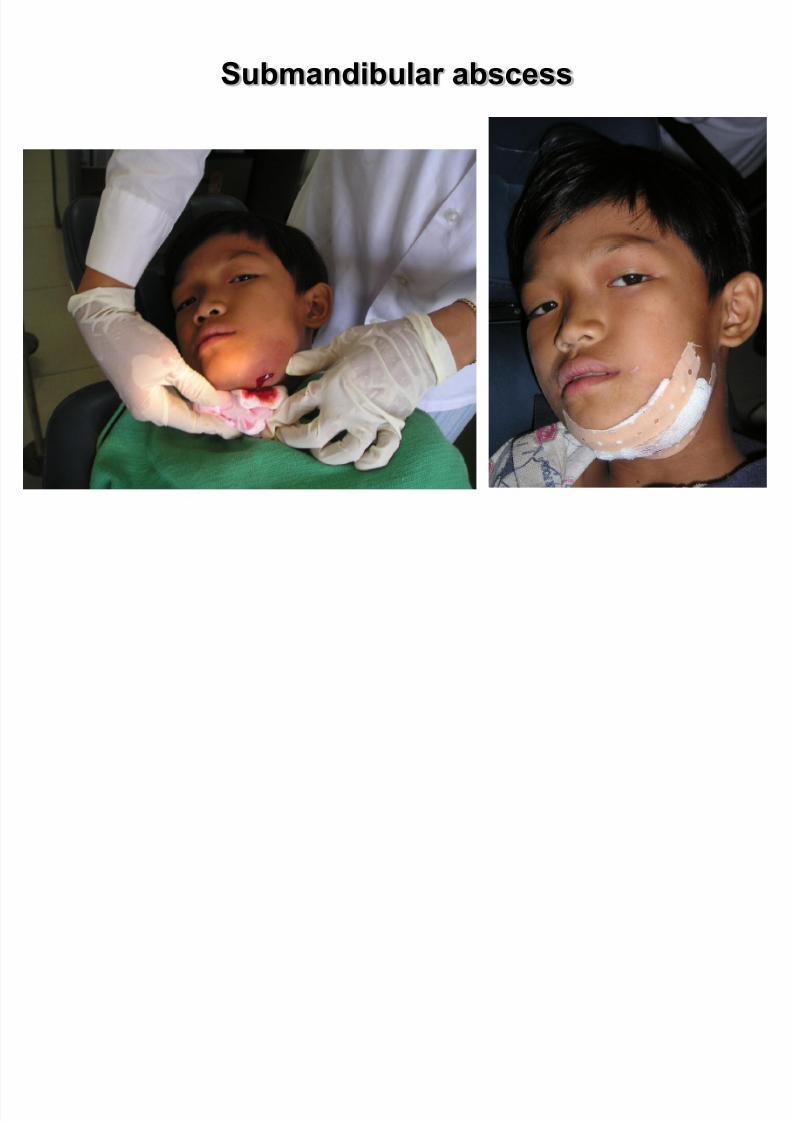
Submandibular abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 178/183

8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 179/183
Submandibular abscess
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 180/183

8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 181/183
Selection of antibiotic therapy
1. Parenteral penicillin
2 M t id l i bi ti ith i illi b
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 182/183
2. Metronidazole in combination with penicillin can be
used in severe infections3. Clindamycin for penicillin-allergic patients
4. Cephalosporins (first-generation cephalosporins)
5. Antibiotics do not substitute for incision and drainage
in cases of significant odontogenic infections
6. Causes for clinical failure include inadequate
drainage or antibiotic resistance
7. Mediastinal involvement should prompt CT scan of
the chest and cardiothoracic surgery consultation
8/22/2019 CELLulitis 1
http://slidepdf.com/reader/full/cellulitis-1 183/183
Th k !