Causal relationship between occupational dysfunction anddepression in healthcare workers: A study using structuralequation modelMutsumi Teraoka, Makoto Kyougoku
Purpose: The purpose of this study is to identify the impacts of occupational dysfunctionon depression in healthcare workers (nurses, physical therapists, and occupationaltherapists) in hospitals.Methods: Healthcare workers responded to a questionnaire based on the Classificationand Assessment of Occupational Dysfunction (CAOD) and Center for Epidemiologic StudiesDepression Scale (CES-D). CAOD and CES-D were examined using the following methods:descriptive statistics, exploratory factor analysis (EFA), confirmatory factor analysis (CFA),and a causal sequence model.Results: CFA of CAOD had 16 items and 5 factors (CFI=0.958, TLI=0.946, RMSEA=0.092).CFA of CES-D had 20 items and 4 factors (CFI=0.950, TLI=0.942, RMSEA=0.060). Theresults suggest that occupational dysfunction had positive causal effects on depression(CFI=0.926, TLI=0.920, RMSEA=0.059).Conclusion: This model refers to the relationship between depression and occupationaldysfunction. Therefore, assessment and intervention on classification of occupationaldysfunction for healthcare workers would be beneficial in the prevention of depression.
PeerJ PrePrints | http://dx.doi.org/10.7287/peerj.preprints.787v1 | CC-BY 4.0 Open Access | rec: 13 Jan 2015, publ: 13 Jan 2015
PrePrin
ts
1
Title: Causal relationship between occupational dysfunction and depression in
healthcare workers: A study using structural equation modeling
Authors: Mutsumi Teraoka 1, 2, Makoto Kyougoku 3
Affiliations:
1 Doctor Course, Graduate School of Health Sciences, KIBI International University,
Okayama, Japan
2 Oosugi Hospital, Okayama, Japan
3 Department of Occupational Therapy, School of Health Sciences, KIBI International
University, Okayama, Japan
Location:
8, Iga-machi, Takahashi city, Okayama, 716-8508, Japan
Corresponding Author
Name: Mutsumi Teraoka
Email: [email protected]
Phone: +81-866-22-9091
Competing Interests
The authors have declared that no competing interests exist.
PeerJ PrePrints | http://dx.doi.org/10.7287/peerj.preprints.787v1 | CC-BY 4.0 Open Access | rec: 13 Jan 2015, publ: 13 Jan 2015
PrePrin
ts
2
Introduction
Occupational dysfunction is recognized as a major health-related problem in
workers by occupational therapists (Maynard 1986; Scaffa & Reitz 2013). Occupational
dysfunction is defined as a category of difficulties faced by individuals when
performing daily activities in the work environment, including occupational
marginalization, occupational imbalance, occupational alienation, and occupational
deprivation (Teraoka 2014). Occupational marginalization is defined as not being
afforded the opportunity to engage in daily activities (Townsend & Wilcock 2004).
Occupational imbalance is defined as a loss of balance in the engagement of daily
activities (Anaby et al. 2010). Occupational alienation is defined as not satisfying one’s
inner needs through daily activities (Bryant et al. 2004). Occupational deprivation is
defined as a loss of choice and opportunities in daily activities, which are beyond the
control of the individual(Whiteford 2000). These problems are recognized as
health-related risk factors for workers.
It has been pointed out that occupational dysfunction arises without apparent
medical disease (Kyougoku 2010). According to an estimate of an observational study
on workers without obvious medical disease, 36% of workers have some occupational
dysfunction (Akiyama 2010). Regarding occupational alienation, 43% of workers have
reported experiencing a serious problem (Akiyama 2010). In other words, workers have
reported experiencing psychological stress. Moreover, a report found that occupational
dysfunction was observed in 75.4% of rehabilitation therapists in hospitals without
obvious medical disease, and occupational dysfunction showed a correlation with job
stress (Miyake 2014). Previous study indicates that healthcare workers experience
occupational dysfunction and various levels of stress more frequently than other
professionals (Akiyama 2010; Miyake 2014).
Healthcare workers have high rates of anxiety, burnout, depression, substance
abuse, and suicide related to strong stress levels on the job (Dyrbye et al. 2008; Harry
2013). In particular, depression is caused by an increase in job stress, and is recognized
worldwide as a major health-related problem (Irvine 1997; Van Praag 2004). In Japan,
more than 60% of workers are reported to suffer from stress (Honda et al. 2014). In
Japanese society, there is a recognized association between depressive mood and
PeerJ PrePrints | http://dx.doi.org/10.7287/peerj.preprints.787v1 | CC-BY 4.0 Open Access | rec: 13 Jan 2015, publ: 13 Jan 2015
PrePrin
ts
3
subsequent suicide among workers (Takeuchi & Nakao 2013; Tamakoshi et al. 2000).
One of the causes of depression in workers is attributed to difficult working conditions,
such as heavy overtime work, understaffing, time pressure, relationship problems, and
cost-cutting (Denton et al. 2002; Kato et al. 2014; Schaefer & Moos 1993; Seki &
Yamazaki 2006). Many Japanese workers are workaholics, which leads to fatigue, and
this is also one of the causes of depression (Matsudaira et al. 2013; Seki & Yamazaki
2006). There has been concern about depression, especially among healthcare workers,
because depression is one of the most common work-related health problems in
healthcare (Health 2008).
However, no previous study has examined the impact of occupational
dysfunction on depression. A case study and theoretical study on occupational therapy
have suggested a causal linkage between occupational dysfunction and depression (Ishii
2010; Kyougoku 2010). As stated above, it has been pointed out that occupational
dysfunction arises without medical disease (Kyougoku 2010). In fact, workers without
medical disease have presented with occupational dysfunction (Akiyama 2010; Miyake
2014). Therefore, occupational dysfunction has the possibility to antedate the
appearance of depression in workers. We hypothesize that occupational dysfunction as
assessed by the Classification and Assessment of Occupational Dysfunction (CAOD) is
associated with the Center for Epidemiological Studies Depression Scale (CES-D). The
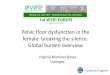
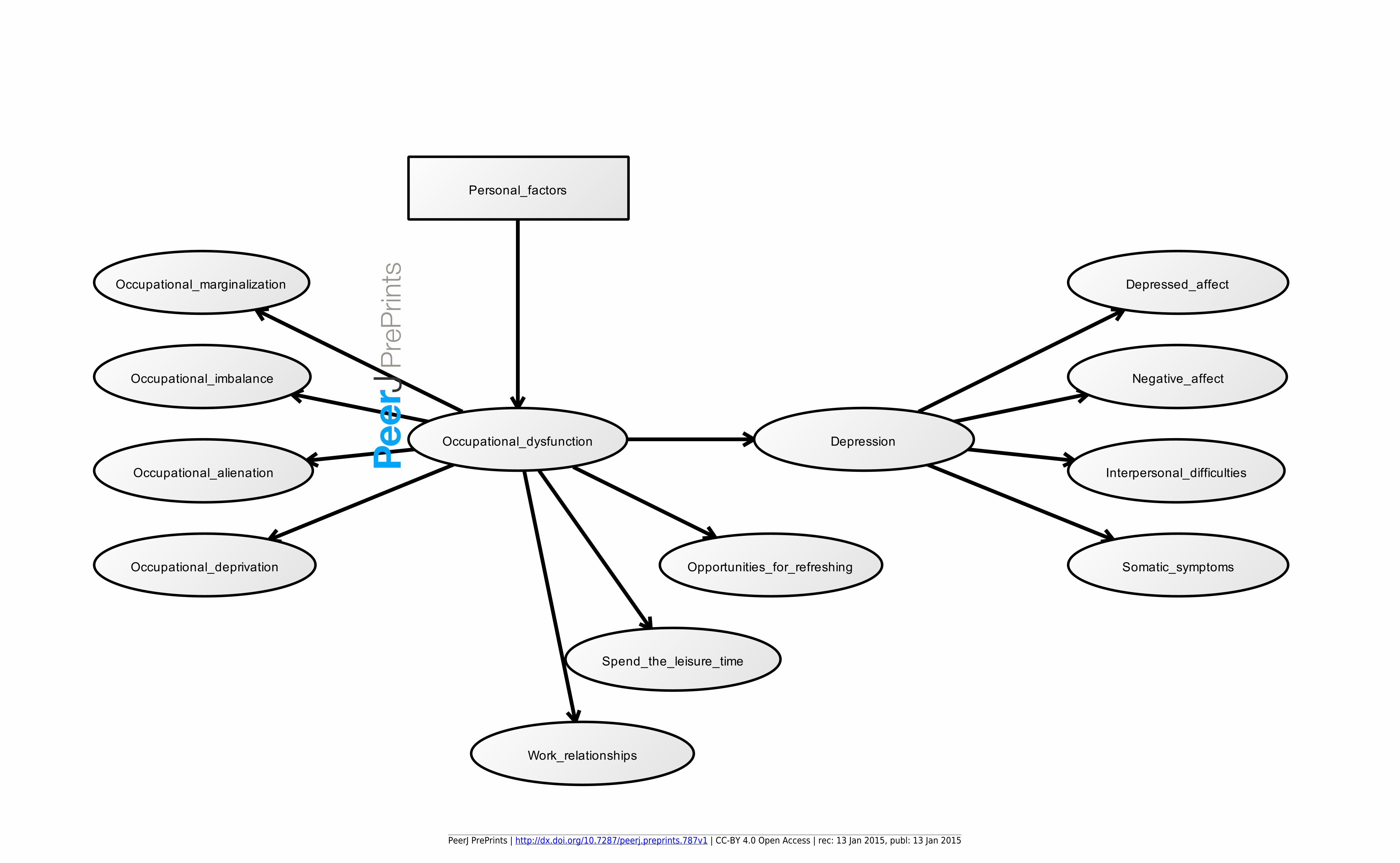
hypothesized model is shown in Figure 1. In other words, our model posits that the
occurrence of occupational dysfunction in healthcare workers facilitates depression.
Moreover, we surmise that occupational dysfunction in healthcare workers influences
depression-related factors, including opportunities for opportunities for refreshing
changes and methods of spending leisure time, and work relationships. In addition, we
postulate that occupational dysfunction in healthcare workers is influenced partly by
personal factors (such as age, years of work experience, and job category). The
significance of this study will be providing insights into the causes of depression.
In summary, this study aims to test the hypothesis that depression is
influenced by occupational dysfunction in healthcare workers.
PeerJ PrePrints | http://dx.doi.org/10.7287/peerj.preprints.787v1 | CC-BY 4.0 Open Access | rec: 13 Jan 2015, publ: 13 Jan 2015
PrePrin
ts
4
Methods
Ethics statement
The Ethics Committee of Kibi International University approved the research
protocol (Nos. 13−30). We provided the participants with a letter explaining the outline
and purposes of the study and obtained their informed consent. Participants had the
right to drop out of the study without reason. We regarded return of the survey form as
consent for participation in this study. Survey forms were sent back anonymously in
sealed envelopes.
Participants
There were a total of 911 participants (463 nurses, 239 physical therapists,
and 209 occupational therapists).
Measures
Participant Profiles: Demographic data were obtained from participants. We assessed
gender, age, years of work experience, job category, taking a leave of absence, vacation,
work relationships, marital status, work schedule, drinking, and smoking.
CAOD (Miyake 2014): CAOD was measured using occupational dysfunction,
including occupational marginalization (6 items), occupational imbalance (4 items),
occupational alienation (3 items), and occupational deprivation (3 items), based on
OBP2.0. CAOD contains 16 items on a 7-point Likert scale (1 = strongly disagree, 7 =
strongly agree). CAOD has been widely used as an assessment tool for occupational
dysfunction.
CES-D (Shima 1985): CES-D was measured based on the level of depression
experienced within the past week using 20 items on four subscales - depressed affect (7
items), negative affect (4 items), interpersonal difficulties (2 items), and somatic
PeerJ PrePrints | http://dx.doi.org/10.7287/peerj.preprints.787v1 | CC-BY 4.0 Open Access | rec: 13 Jan 2015, publ: 13 Jan 2015
PrePrin
ts
5
symptoms (7 items) - with a 4-point response (0 = none of the time, 3 = all of the
time). In epidemiologic studies, CES-D has been used worldwide as an assessment tool
for depression. Among the negative affect-related items, 4 were originally regarded as
related to a positive affect. In the present study, the 4 items were inversely scored to
make this point more comprehensible.
Statistical Analysis
SPSS Statistics (http://www.spss.com) was used for the sample characteristics.
Mplus 7.3 (http://www.statmodel.com) was used for structural equation modeling
(SEM). SEM is a comprehensive statistical analysis for the integration of path analysis
and factor analysis (Ullman & Bentler 2003). SEM offers the advantage of
identification of causal relationships (Ullman & Bentler 2003).
Sample Characteristics: The demographics of participants were summarized using
descriptive analyses. The normal distribution of all scores was examined using the
Kolmogorov-Smirnov test (p>0.05).
Structural validity: The factor structure of CAOD and CES-D were determined by
confirmatory factor analysis (CFA) of SEM, using a robust weighted least squares
factoring method (WLSMV) with missing data (Asparouhov & Muthén 2010). If an
unacceptable model fit was found due to CAF, we performed EFA using WLSMV with
missing data. EFA adopted the same model-data fit assessment as CFA. Based on the
results of EFA, once again, we performed a CFA using WLSMV with missing data. We
used three indexes for assessment of model-data fit (Kline 1986; Tabachnick & Fidell
2007). The first index was the root mean square error of approximation (RMSEA).
Critical values of RMSEA from 0.08 to 0.10 showed a mediocre fit, and below 0.08
indicated a good fit (MacCallum et al. 1996). The second and third indexes were the
comparative fit index (CFI), and the Tucker–Lewis index (TLI), both with critical
values above 0.95 (Kline 2011).
Testing the causal relationship: We analyzed the relationship using SEM. The
analyses examining the effects of occupational dysfunction on depression were
PeerJ PrePrints | http://dx.doi.org/10.7287/peerj.preprints.787v1 | CC-BY 4.0 Open Access | rec: 13 Jan 2015, publ: 13 Jan 2015
PrePrin
ts
6
performed for causal structures as indicated in Figure 1. We assessed the model fit of
the hypothesized relationship between latent variables (occupational dysfunction,
depression) to data by SEM. To account for the contexts, personal variables (such as
age and gender) and depression-related variables (such as opportunities for refreshing
changes and methods of spending leisure time, work relationships) were included in the
model. The indirect effect estimates were calculated to test whether or not occupational
dysfunction was indirectly associated with subscales of CES-D (depressed affect,
negative affect, interpersonal difficulties, and somatic symptoms) via depression. When
modifying the model based on the results of SEM, the modification indexes, model fit,
standardized estimates, 95% confidence intervals, and standard errors were considered
while taking the hypothesis into account. SEM was performed without special
limitations. All items were treated as categorical data. An estimator was used for
WLMSV with missing data. Goodness of model fit index was evaluated using CFI, TLI,
and RMSEA. Critical values of RMSEA from 0.08 to 0.10 showed a mediocre fit, and
below 0.08 indicated a good fit (MacCallum et al. 1996). The second and third indexes
were the comparative fit index (CFI), and the Tucker–Lewis index (TLI), both with
critical values above 0.95 (Kline 2011).
Results
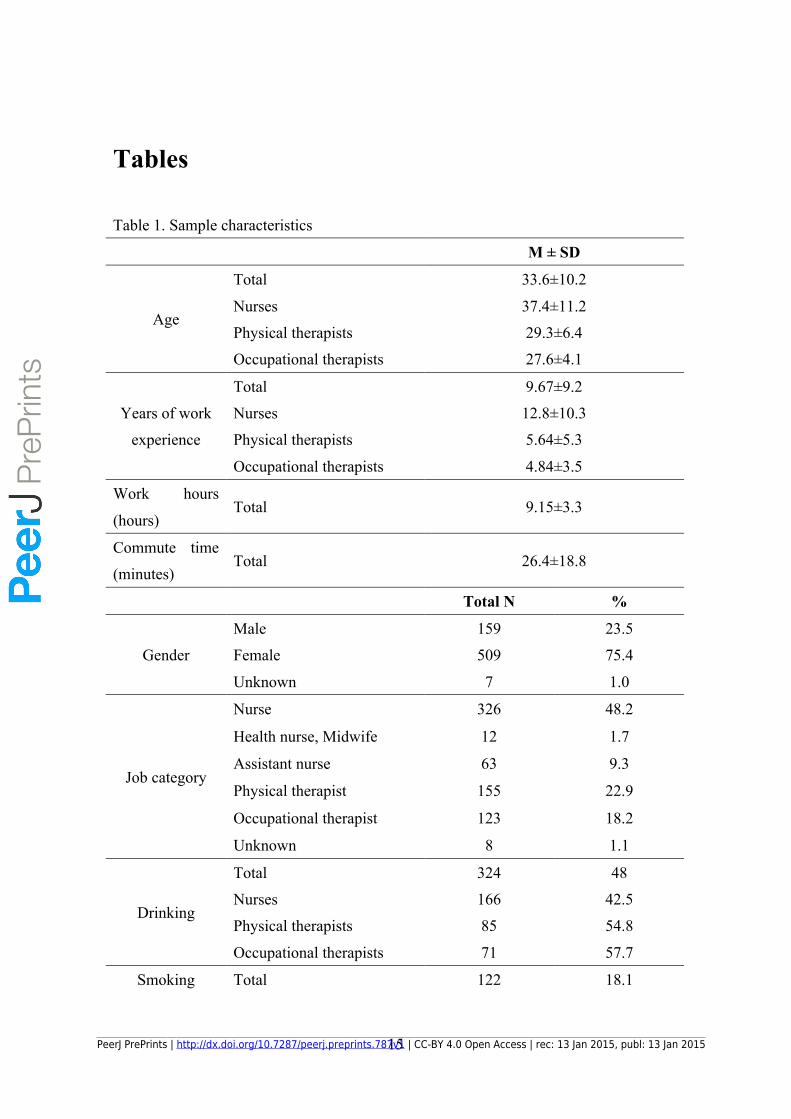
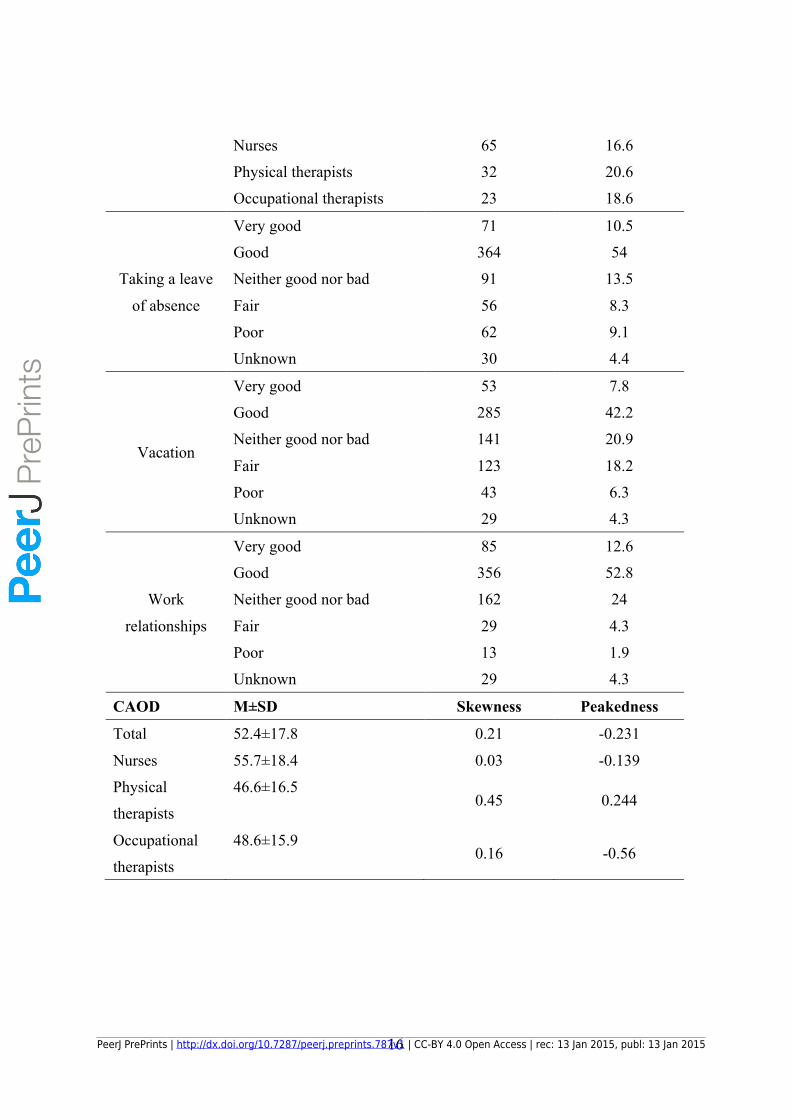
Sample Characteristics
Table 1 shows the results of sample characteristics. In this study, a total of
674 participants (388 nurses (including 11 public health nurses and midwives and 63
assistant nurses), 155 physical therapists, 123 occupational therapists, and 8 unknowns)
participated (73% response rate), including 159 males, 509 females, and 6 unknowns,
with an average age of 33.6 ± 10.2 years. The Kolmogorov-Smirnov test showed that all
scores had normal distribution.
Structural validity of CAOD
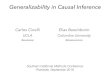
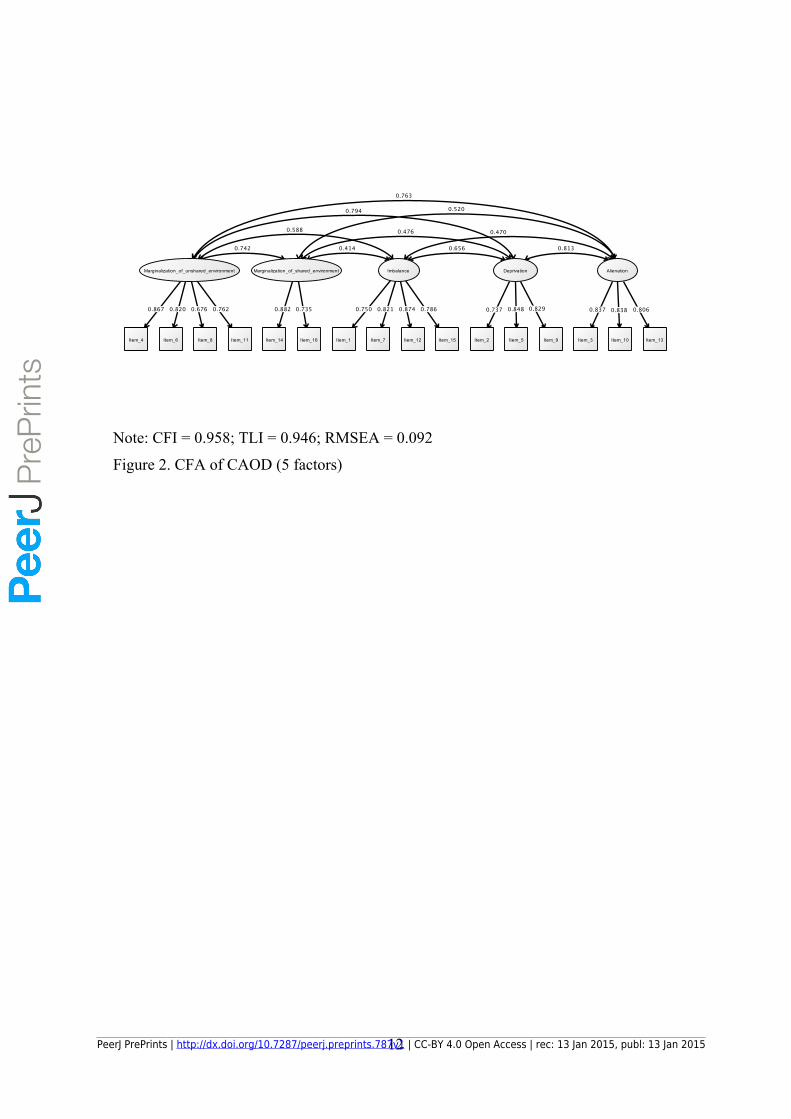
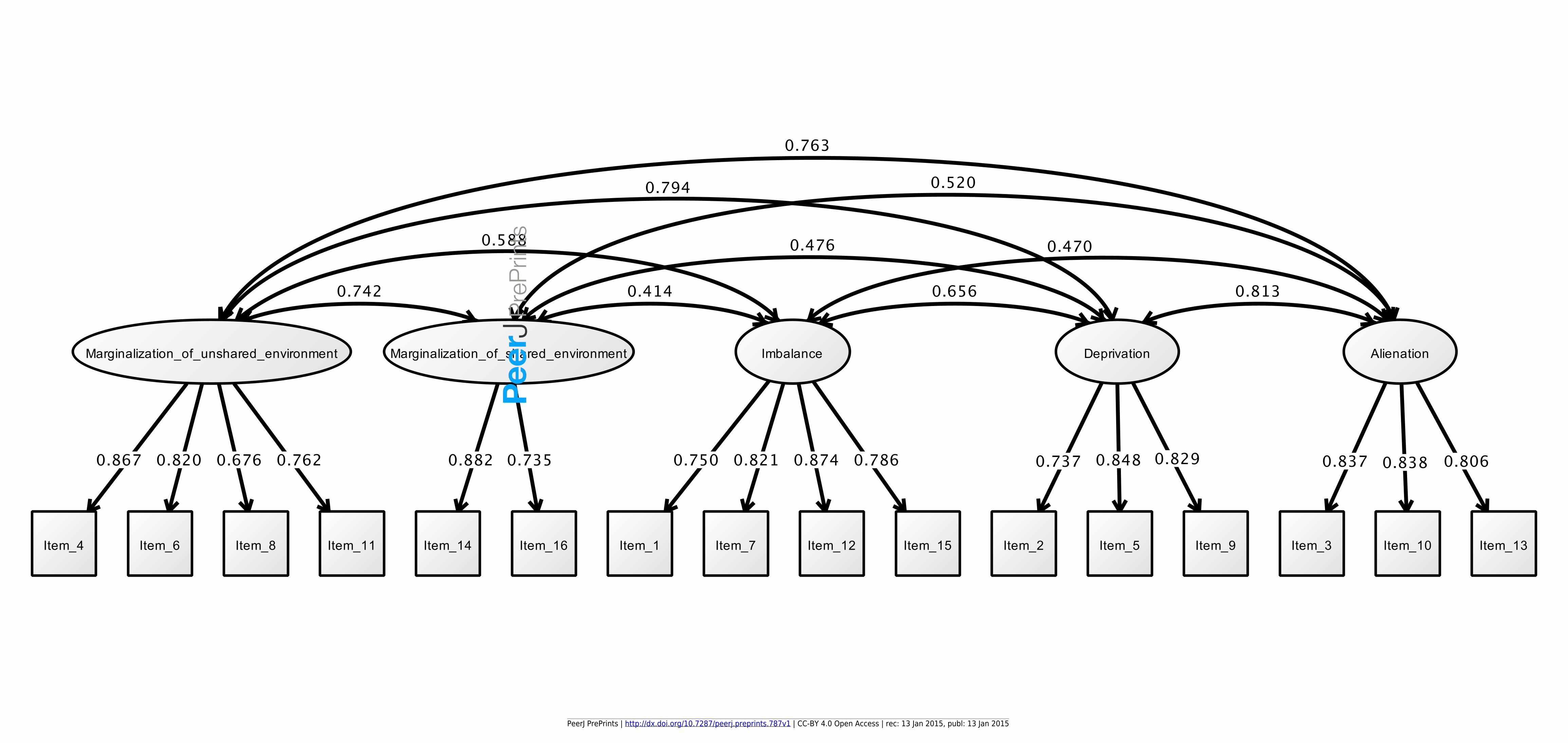
Figure 2 shows the results of CFA of CAOD. First, CFA was estimated to be a poor
PeerJ PrePrints | http://dx.doi.org/10.7287/peerj.preprints.787v1 | CC-BY 4.0 Open Access | rec: 13 Jan 2015, publ: 13 Jan 2015
PrePrin
ts
7
estimate of RMSEA of model fit (RMSEA = 0.104, CFI = 0.943, and TLI = 0.931).
Therefore, we performed EFA, we performed EFA, and found that the CAOD consisted
of 16 items of 5 factors, including occupational marginalization of shared environment
(2 items), occupational marginalization of unshared environment (4 items), occupational
imbalance (4 items), occupational alienation (3 items), and occupational deprivation (3
items). The indexes for this model were RMSEA = 0.066, CFI = 0.988, and TLI = 0.972.
Based on EFA, CFA of CAOD was determined a good estimate of model fit (RMSEA =
0.092, CFI = 0.958, and TLI = 0.946).
Structural validity of CES-D
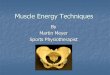
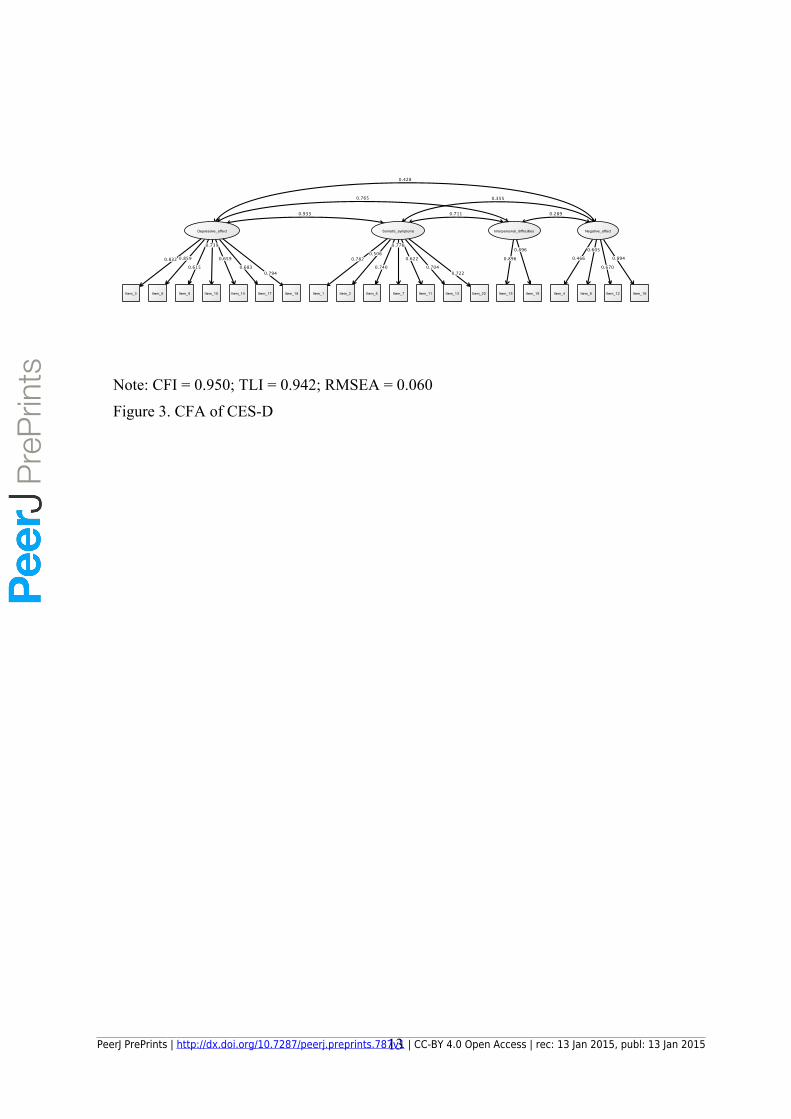
Figure 3 shows the results of CFA of CES-D. The CFA model for the latent
factors of CES-D exhibited good fit of depressed affect, negative affect, interpersonal
difficulties, and somatic symptoms (RMSEA = 0.060, CFI = 0.950, and TLI = 0.942).
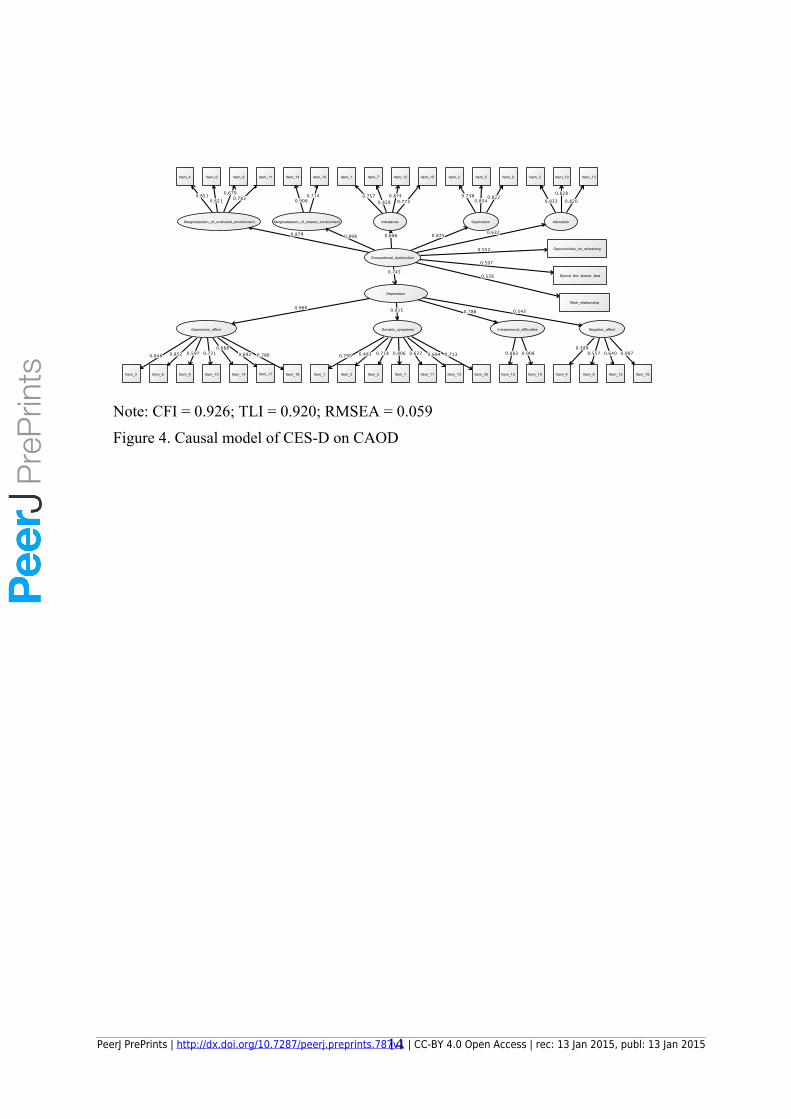
Hypothesized model
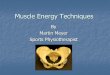
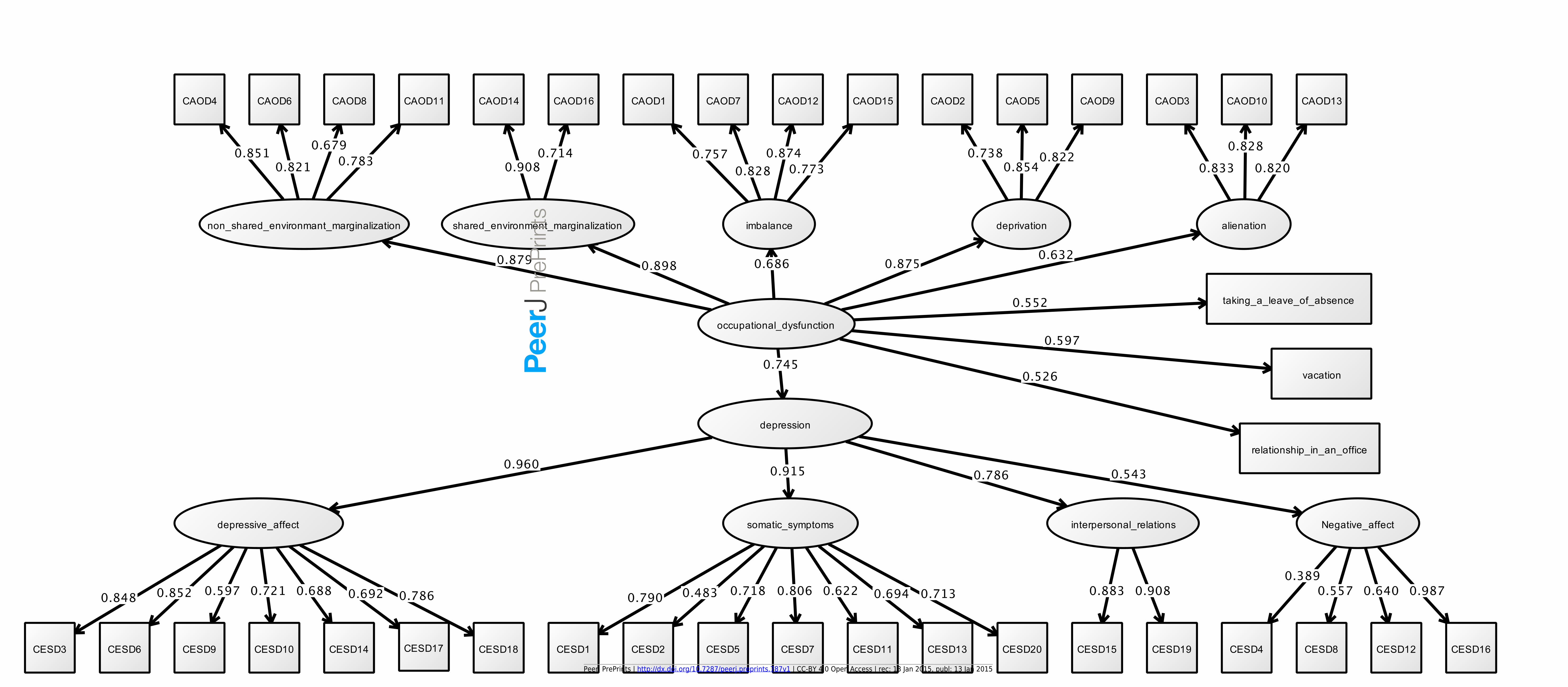
Figure 4 shows the results of the final model. The hypothesized model
exhibited excellent fit (RMSEA=0.059, CFI=0.926, TLI=0.920). In this model,
occupational dysfunction was significantly positively associated with depression
(standardized direct effect = 0.745, S.E. = 0.021, Est./S.E. = 34.634, P-Value = 0.000,
95% CI = 0.703; 0.787). Indirect effect of occupational dysfunction on depression
symptoms was significant for the following indicators: depressed affect (standardized
indirect effect = 0.715, S.E. = 0.024, Est./S.E. = 29.618, P-Value = 0.000, 95% CI =
0.667; 0.762), negative affect (standardized indirect effect = 0.404, S.E. = 0.033,
Est./S.E. = 12.070, P-Value = 0.000, 95% CI = 0.526; 0.645), interpersonal difficulties
(standardized indirect effect = 0.585, S.E. = 0.030, Est./S.E. = 19.301, P-Value = 0.000,
95% CI = 0.526; 0.645), and somatic symptoms (standardized indirect effect = 0.681,
S.E. = 0.024, Est./S.E. = 28.175, P-Value = 0.000, 95% CI = 0.634; 0.729). In other
words, the symptoms of depression increased with the deterioration of occupational
dysfunction. In addition, the effects of occupational dysfunction on depression-related
factors were significant for the following indicators: opportunities for refreshing
changes (standardized direct effect = 0.552, S.E. = 0.030, Est./S.E. = 18.515, P-Value =
PeerJ PrePrints | http://dx.doi.org/10.7287/peerj.preprints.787v1 | CC-BY 4.0 Open Access | rec: 13 Jan 2015, publ: 13 Jan 2015
PrePrin
ts
8
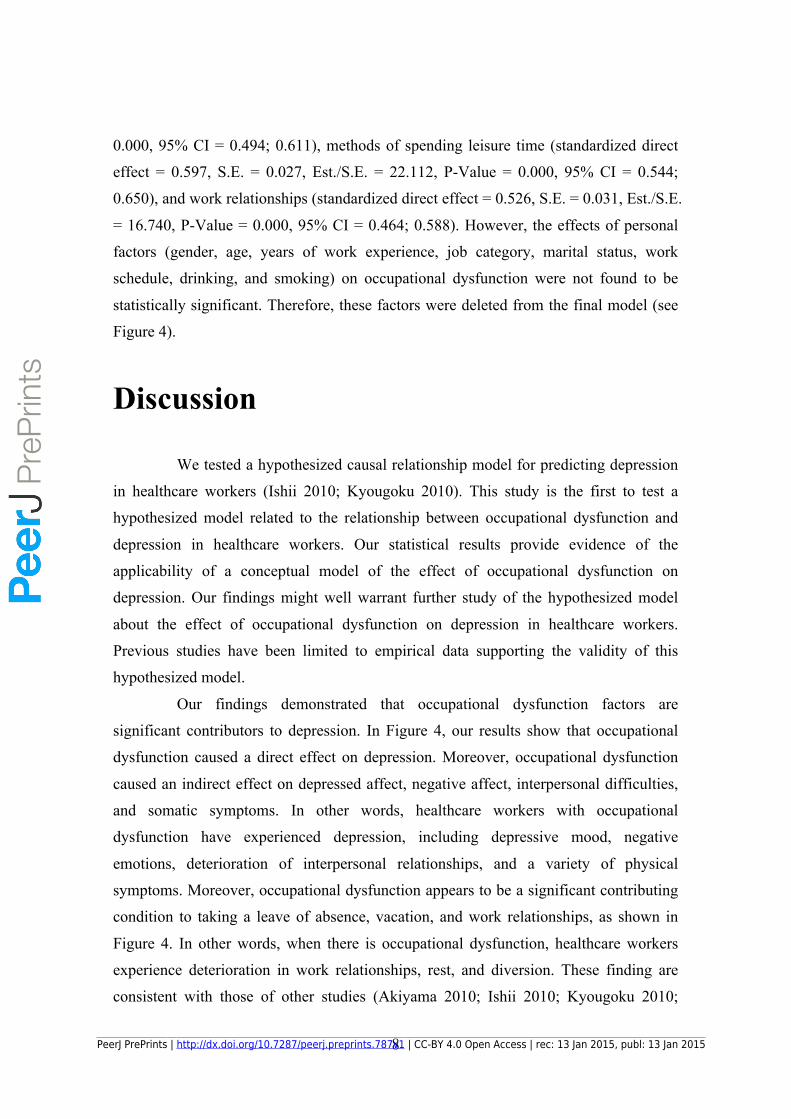
0.000, 95% CI = 0.494; 0.611), methods of spending leisure time (standardized direct
effect = 0.597, S.E. = 0.027, Est./S.E. = 22.112, P-Value = 0.000, 95% CI = 0.544;
0.650), and work relationships (standardized direct effect = 0.526, S.E. = 0.031, Est./S.E.
= 16.740, P-Value = 0.000, 95% CI = 0.464; 0.588). However, the effects of personal
factors (gender, age, years of work experience, job category, marital status, work
schedule, drinking, and smoking) on occupational dysfunction were not found to be
statistically significant. Therefore, these factors were deleted from the final model (see
Figure 4).
Discussion
We tested a hypothesized causal relationship model for predicting depression
in healthcare workers (Ishii 2010; Kyougoku 2010). This study is the first to test a
hypothesized model related to the relationship between occupational dysfunction and
depression in healthcare workers. Our statistical results provide evidence of the
applicability of a conceptual model of the effect of occupational dysfunction on
depression. Our findings might well warrant further study of the hypothesized model
about the effect of occupational dysfunction on depression in healthcare workers.
Previous studies have been limited to empirical data supporting the validity of this
hypothesized model.
Our findings demonstrated that occupational dysfunction factors are
significant contributors to depression. In Figure 4, our results show that occupational
dysfunction caused a direct effect on depression. Moreover, occupational dysfunction
caused an indirect effect on depressed affect, negative affect, interpersonal difficulties,
and somatic symptoms. In other words, healthcare workers with occupational
dysfunction have experienced depression, including depressive mood, negative
emotions, deterioration of interpersonal relationships, and a variety of physical
symptoms. Moreover, occupational dysfunction appears to be a significant contributing
condition to taking a leave of absence, vacation, and work relationships, as shown in
Figure 4. In other words, when there is occupational dysfunction, healthcare workers
experience deterioration in work relationships, rest, and diversion. These finding are
consistent with those of other studies (Akiyama 2010; Ishii 2010; Kyougoku 2010;
PeerJ PrePrints | http://dx.doi.org/10.7287/peerj.preprints.787v1 | CC-BY 4.0 Open Access | rec: 13 Jan 2015, publ: 13 Jan 2015
PrePrin
ts
9
Miyake 2014).
Moreover, the results of CFA indicated a good factor structure for CAOD and CES-D.
In Figure 2, the results of CFA of CAOD indicated good model fit on the five-factor
structure, unlike a previous study (Miyake 2014). In Figure 2, major factors of
occupational dysfunction contributing to the development of depression were
occupational marginalization of shared environment, occupational marginalization of
unshared environment, and occupational deprivation. These kinds of occupational
dysfunction might be matters of special importance in the prevention of depression in
healthcare workers. In Figure 3, CFA also showed that the factor structure of CES-D
was appropriate. Thus, the factor structure of the CES-D was similar to those shown in
previous studies (Shima 1985).
Therefore, these results suggest it might be possible to prevent the occurrence
of depression by early detection and rapid treatment of occupational dysfunction. For
example, CAOD can be applied to healthcare workers to identify occupational
dysfunction. After completing CAOD, healthcare workers and occupational therapists
can discuss the responses to gain a better understanding of the occupational dysfunction.
When there is occupational dysfunction, occupational therapists can provide healthcare
workers with counseling and advice (Law et al. 1998; Law et al. 2002; Scaffa et al.
2010). Consequently, they may be able to treat the depression to a certain extent.
The first limitation of this study is an inferred causal effect with low power by
a cross-sectional design. Future research is necessary to confirm this relationship by a
longitudinal design. A second limitation is that the conclusions are limited to some
extent, as the participants were chosen from among nurses, physical therapists, and
occupational therapists, owing to some constraints. Future research with different
subjects, such as physicians, psychologists, and pharmacists, is necessary.
Conclusions
We conducted a comprehensive examination on occupational dysfunction and
depression in healthcare workers. The statistical results supported the hypothesis that
occupational dysfunction influences depression. In addition, the results of this study
suggest that occupational dysfunction influences taking a leave of absence, vacation,
PeerJ PrePrints | http://dx.doi.org/10.7287/peerj.preprints.787v1 | CC-BY 4.0 Open Access | rec: 13 Jan 2015, publ: 13 Jan 2015
PrePrin
ts
10
and work relationships. The findings of this study have beneficial value for industrial
health.
PeerJ PrePrints | http://dx.doi.org/10.7287/peerj.preprints.787v1 | CC-BY 4.0 Open Access | rec: 13 Jan 2015, publ: 13 Jan 2015
PrePrin
ts

11
Figures
Figure 1. Hypothesized model
PeerJ PrePrints | http://dx.doi.org/10.7287/peerj.preprints.787v1 | CC-BY 4.0 Open Access | rec: 13 Jan 2015, publ: 13 Jan 2015
PrePrin
ts
12
Note: CFI = 0.958; TLI = 0.946; RMSEA = 0.092
Figure 2. CFA of CAOD (5 factors)
PeerJ PrePrints | http://dx.doi.org/10.7287/peerj.preprints.787v1 | CC-BY 4.0 Open Access | rec: 13 Jan 2015, publ: 13 Jan 2015
PrePrin
ts
13
Note: CFI = 0.950; TLI = 0.942; RMSEA = 0.060
Figure 3. CFA of CES-D
PeerJ PrePrints | http://dx.doi.org/10.7287/peerj.preprints.787v1 | CC-BY 4.0 Open Access | rec: 13 Jan 2015, publ: 13 Jan 2015
PrePrin
ts
14
Note: CFI = 0.926; TLI = 0.920; RMSEA = 0.059
Figure 4. Causal model of CES-D on CAOD
PeerJ PrePrints | http://dx.doi.org/10.7287/peerj.preprints.787v1 | CC-BY 4.0 Open Access | rec: 13 Jan 2015, publ: 13 Jan 2015
PrePrin
ts
15
Tables
Table 1. Sample characteristics
M ± SD
Age
Total 33.6±10.2
Nurses 37.4±11.2
Physical therapists 29.3±6.4
Occupational therapists 27.6±4.1
Years of work
experience
Total 9.67±9.2
Nurses 12.8±10.3
Physical therapists 5.64±5.3
Occupational therapists 4.84±3.5
Work hours
(hours) Total 9.15±3.3
Commute time
(minutes) Total 26.4±18.8
Total N %
Gender
Male 159 23.5
Female 509 75.4
Unknown 7 1.0
Job category
Nurse 326 48.2
Health nurse, Midwife 12 1.7
Assistant nurse 63 9.3
Physical therapist 155 22.9
Occupational therapist 123 18.2
Unknown 8 1.1
Drinking
Total 324 48
Nurses 166 42.5
Physical therapists 85 54.8
Occupational therapists 71 57.7
Smoking Total 122 18.1
PeerJ PrePrints | http://dx.doi.org/10.7287/peerj.preprints.787v1 | CC-BY 4.0 Open Access | rec: 13 Jan 2015, publ: 13 Jan 2015
PrePrin
ts
16
Nurses 65 16.6
Physical therapists 32 20.6
Occupational therapists 23 18.6
Taking a leave
of absence
Very good 71 10.5
Good 364 54
Neither good nor bad 91 13.5
Fair 56 8.3
Poor 62 9.1
Unknown 30 4.4
Vacation
Very good 53 7.8
Good 285 42.2
Neither good nor bad 141 20.9
Fair 123 18.2
Poor 43 6.3
Unknown 29 4.3
Work
relationships
Very good 85 12.6
Good 356 52.8
Neither good nor bad 162 24
Fair 29 4.3
Poor 13 1.9
Unknown 29 4.3
CAOD M±SD Skewness Peakedness
Total 52.4±17.8 0.21 -0.231
Nurses 55.7±18.4 0.03 -0.139
Physical
therapists
46.6±16.5 0.45 0.244
Occupational
therapists
48.6±15.9 0.16 -0.56
PeerJ PrePrints | http://dx.doi.org/10.7287/peerj.preprints.787v1 | CC-BY 4.0 Open Access | rec: 13 Jan 2015, publ: 13 Jan 2015
PrePrin
ts
17
References Akiyama E, Kyougoku, M. 2010. Examination of occupational dysfunction in workers:
using occupational self assessment version2 (OSA2). Sogo Rehabilitation
38:373-379.
Anaby D, Jarus T, Backman CL, and Zumbo BD. 2010. The role of occupational
characteristics and occupational imbalance in explaining well-being. Applied
Research in Quality of Life 5:81-104.
Asparouhov T, and Muthén B. 2010. Weighted least squares estimation with missing
data. MplusTechnical Appendix.
Bryant W, Craik C, and McKay EA. 2004. Living in a glasshouse: exploring
occupational alienation. Canadian Journal of Occupational Therapy
71:282-289.
Denton M, Zeytinoglu IU, Davies S, and Lian J. 2002. Job stress and job dissatisfaction
of home care workers in the context of health care restructuring. International
Journal of Health Services 32:327-357.
Dyrbye LN, Thomas MR, Massie FS, Power DV, Eacker A, Harper W, Durning S,
Moutier C, Szydlo DW, and Novotny PJ. 2008. Burnout and suicidal ideation
among US medical students. Annals of internal medicine 149:334-341.
Harry E. 2013. Stress and the healthcare worker. As complicated or as simple as fear
and hope. The Journal of medical practice management: MPM 30:28-30.
Health NIfOSa. 2008. Exposure to stress: occupational hazards in hospitals. Cincinnati:
National Institute for Occupational Safety and Health.
Honda A, Date Y, Abe Y, Aoyagi K, and Honda S. 2014. Work-related Stress,
Caregiver Role, and Depressive Symptoms among Japanese Workers. Saf
Health Work 5:7-12.
Irvine D. 1997. The performance of doctors. I: Professionalism and self regulation in a
changing world. BMJ: British Medical Journal 314:1540.
Ishii Y, Kyougoku, M., Nagao S. 2010. Occupational therapy of mental health. Tokyo:
Chuohoki.
Kato R, Haruyama Y, Endo M, Tsutsumi A, and Muto T. 2014. Heavy overtime work
and depressive disorder among male workers. Occupational Medicine:kqu120.
Kline P. 1986. A handbook of test construction: Introduction to psychometric design:
PeerJ PrePrints | http://dx.doi.org/10.7287/peerj.preprints.787v1 | CC-BY 4.0 Open Access | rec: 13 Jan 2015, publ: 13 Jan 2015
PrePrin
ts
18
Methuen.
Kline RB. 2011. Principles and practice of structural equation modeling: Guilford
press.
Kyougoku M. 2010. Unstructured assessment for occupational therapy, 4 condition
method. Tokyo: Seisin-shoboo.
Law M, Steinwender S, and Leclair L. 1998. Occupation, health and well-being.
Canadian Journal of Occupational Therapy 65:81-91.
Law MC, Baum CM, and Baptiste S. 2002. Occupation-based practice: Fostering
performance and participation: Slack Incorporated.
MacCallum RC, Browne MW, and Sugawara HM. 1996. Power analysis and
determination of sample size for covariance structure modeling. Psychological
methods 1:130.
Matsudaira K, Shimazu A, Fujii T, Kubota K, Sawada T, Kikuchi N, and Takahashi M.
2013. Workaholism as a Risk Factor for Depressive Mood, Disabling Back Pain,
and Sickness Absence. PLoS One 8:e75140.
Maynard M. 1986. Health promotion through employee assistance programs: a role for
occupational therapists. The American journal of occupational therapy: official
publication of the American Occupational Therapy Association 40:771-776.
Miyake Y, Teraoka, M., Ogino, K., Kyougoku, M. 2014. Survey of the classification of
occupational dysfunction among japanese rehabilitation therapists and the
association of occupational dysfunction with job strain. Journal of Preventive
Medicine 9:93-100.
Scaffa ME, and Reitz SM. 2013. Occupational Therapy Community-Based Practice
Settings: FA Davis.
Scaffa ME, Reitz SM, and Pizzi M. 2010. Occupational therapy in the promotion of
health and wellness: FA Davis Company Philadelphia, PA.
Schaefer JA, and Moos RH. 1993. Relationship, task and system stressors in the health
care workplace. Journal of Community & Applied Social Psychology 3:285-298.
Seki Y, and Yamazaki Y. 2006. Effects of working conditions on intravenous
medication errors in a Japanese hospital. Journal of nursing management
14:128-139.
Shima S, Shikano, T, Kitamura, T., Asai, M. 1985. New self-rating scales for
depression. Clinical Psychiatry 27:717-723.
PeerJ PrePrints | http://dx.doi.org/10.7287/peerj.preprints.787v1 | CC-BY 4.0 Open Access | rec: 13 Jan 2015, publ: 13 Jan 2015
PrePrin
ts
19
Tabachnick BG, and Fidell LS. 2007. Using multivariate statistics, 5th ed. Toront:
Allyn and Bacon.
Takeuchi T, and Nakao M. 2013. The relationship between suicidal ideation and
symptoms of depression in Japanese workers: a cross-sectional study. BMJ
Open 3:e003643.
Tamakoshi A, Ohno Y, Yamada T, Aoki K, Hamajima N, Wada M, Kawamura T,
Wakai K, and Lin YS. 2000. Depressive mood and suicide among middle-aged
workers: findings from a prospective cohort study in Nagoya, Japan. Journal of
epidemiology/Japan Epidemiological Association 10:173-178.
Teraoka M, Kyougoku, M. 2014. Development of occupation-based practice 2.0 that
integrates occupation based-practice and dissolution approach for belief conflict.
Japanese occupationai therapy researh 33:249-258.
Townsend E, and Wilcock AA. 2004. Occupational justice and client-centred practice: a
dialogue in progress. Canadian Journal of Occupational Therapy 71:75-87.
Ullman JB, and Bentler PM. 2003. Structural equation modeling: Wiley Online Library.
Van Praag HM. 2004. Can stress cause depression? Progress in
Neuro-Psychopharmacology and Biological Psychiatry 28:891-907.
Whiteford G. 2000. Occupational deprivation: Global challenge in the new millennium.
The British Journal of Occupational Therapy 63:200-204.
PeerJ PrePrints | http://dx.doi.org/10.7287/peerj.preprints.787v1 | CC-BY 4.0 Open Access | rec: 13 Jan 2015, publ: 13 Jan 2015
PrePrin
ts
PeerJ PrePrints | http://dx.doi.org/10.7287/peerj.preprints.787v1 | CC-BY 4.0 Open Access | rec: 13 Jan 2015, publ: 13 Jan 2015
PrePrin
ts
PeerJ PrePrints | http://dx.doi.org/10.7287/peerj.preprints.787v1 | CC-BY 4.0 Open Access | rec: 13 Jan 2015, publ: 13 Jan 2015
PrePrin
ts

PeerJ PrePrints | http://dx.doi.org/10.7287/peerj.preprints.787v1 | CC-BY 4.0 Open Access | rec: 13 Jan 2015, publ: 13 Jan 2015
PrePrin
ts
PeerJ PrePrints | http://dx.doi.org/10.7287/peerj.preprints.787v1 | CC-BY 4.0 Open Access | rec: 13 Jan 2015, publ: 13 Jan 2015
PrePrin
ts
Recommended