Embed Size (px)
Citation preview

Dr.Hassaan Ali 20142nd workshop of ED and
Penile Prostheses 1,2 Jan 2015
Aswan Egypt

Dr.Hassaan Ali 2014
ERECTILE DYSFUNCTION PRACTICAL VIEW

Definition of ED
Epidemiology
Anatomy and Physiology of erection
Causes ED
Examination of patient with ED
Investigations
Treatment
Dr.Hassaan Ali 2014

Synonym: Impotence
Persistent or recurrent inability to obtain or
maintain penile erection (or both)
sufficient for satisfactory sexual performance, for more than 3-months
duration(1).
Dr.Hassaan Ali 2014

NO!Sexual function is an important component of
quality of life and subjective well-being.
Sexual problems affect adversely mood, well-being, and interpersonal functioning.
Nearly every man can be successfully treated.
Dr.Hassaan Ali 2014

Incidence and prevalence is high
worldwide
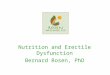
Effects up to 52% of men (40-70yrs)
Complete impotence from 5% of 40yr olds
to 15% of 70yr olds
Only 10-20% solely psychogenic
Dr.Hassaan Ali 2014

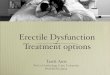
Prevalence of ED by Age and Severity (%)
Severe
Moderate
Mild or
Mild/Moderate
100%
80%
60%
40%
20%
0%
Dr.Hassaan Ali 2014

Dr.Hassaan Ali 2014

Dr.Hassaan Ali 2014

Dilatation arterioles&arteries
expanding of sinusoids
compression of subtunicalvenular plexuses
Emissary veins enclosed
increasing of intracavernouspressure to raise the penis
Dr.Hassaan Ali 2014

Transient intracorporeal pressure increase
[smooth muscle contraction]
Pressure decrease slowly
[slow reopening of the venous channels]
Pressure decrease fast
[venous outflow capacity is fully restored]
Dr.Hassaan Ali 2014

Dr.Hassaan Ali 2014

Dr.Hassaan Ali 2014

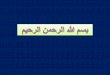
Flaccid phase (1) Minimal arterial and venous flow; b
Latent (filling) phase (2) Increased flow in the internal pudendal
artery during both systolic and diastolic phases. Decreased pressure
in the internal pudendal artery; unchanged intracavernous pressure.
Some elongation of the penis.
Tumescent phase (3) Rising intracavernous pressure until full erection
is achieved. Penis shows more expansion and elongation with
pulsation. The arterial flow rate decreases as the pressure rises..
Full erection phase (4) Intracavernous pressure can rise to as much as
80–90% of the systolic pressure. Pressure in the internal pudendal
artery increases but remains slightly below systemic pressure. Arterial
flow is much less than in the initial filling phase but is still higher than
in the flaccid phase. approach those of arterial blood.
Skeletal or rigid erection phase (5) As a result of contraction of the
ischiocavernous muscle, the intracavernous pressure rises well
above the systolic pressure, resulting in rigid erection..
Detumescent phase (6) After ejaculation or cessation of erotic stimuli,
sympathetic tonic discharge resumes, resulting in contraction of the
smooth muscles around the sinusoids and arterioles. This effectively
diminishes the arterial flow to flaccid levels,.
Dr.Hassaan Ali 2014

Supraspinal pathways
[ hypothalamus, limbic system and cerebral cortex
Parasympathetic nerves S2-4 mediate erection
Sympathetic nerves T11-L2 control ejaculation and
detumescence
Smooth muscle relaxation
Nitric oxide diffuses into cavernosal smooth muscle cells, activates Guanylate cyclase converts guanosine
triphosphate to cGMP resulting in smooth muscle
relaxation.
Effect of cGMP stopped by Phosphodiesterase type 5 which
exists primarily in corpora cavernosa
Dr.Hassaan Ali 2014

Dr.Hassaan Ali 2014

Sedentary lifestyle
Obesity
Smoking
Hypercholesterolemia
Diabetes mellitus
Dr.Hassaan Ali 2014

OrganicI. Vasculogenic : Arteriogenic Cavernosal Mixed
II. Neurogenic
III. Anatomic
IV. Endocrinology
PsychogenicI. Generalized
A. Generalized unresponsiveness
1. Primary lack of sexual arousability 2. Aging-related decline in sexual arousability
B. Generalized inhibition 1. Chronic disorder of sexual intimacy
II. Situational
A. Partner-related 1. Lack of arousability in specific relationship 2. Lack of arousability owing to sexual object preference 3. High central inhibition owing to partner conflict or threat
B. Performance-related 1. Associated with other sexual dysfunction/s (e.g., rapid ejaculation) 2. Situational performance anxiety (e.g., fear of failure)
C. Psychological distress- or adjustment-related 1. Associated with negative mood state (e.g., depression) or major life stress (e.g., death of partner)
Mixed
Dr.Hassaan Ali 2014

Dr.Hassaan Ali 2014

Vascular
Diabetes
Medication
Pelvic Surgery,
Radiation
or TraumaNeurological Causes
Endocrine
ProblemsOther
Vascular
Diabetes
Medication
Dr.Hassaan Ali 2014

Hypertension
Smoking
Diabetes
Hyperlipidaemia
Peripheral vascular disease
Blunt perineal or pelvic trauma
Pelvic irradiation
Dr.Hassaan Ali 2014

Central:Lesions of medial preoptic nucleus, paraventicular nucleus, hippocampus
Spinal trauma
Myelodisplasia (spina bifida)
Pelvic surgery/radiotherapy
Multiple sclerosis
Intervertebral disc lesion
Peripheral neuropathies
Alcohol
Diabetes
HIV
Dr.Hassaan Ali 2014

Hypogonadism
Low testosterone
Raised SHBG
Raised Prolactin
Thyroid disease
Hypothyroidism
hyperthyroidism
Dr.Hassaan Ali 2014

Peyronie’s disease
Micropenis
Penile anomalies (hypospadias etc
Dr.Hassaan Ali 2014

AntihypertensivesThiazides
B blockers
Centrally acting drugs
AntidepressantsTricyclics
MAO inhibitors
SSRI
AnticholinergicsAtropine
AntipsychoticsPhenothiazines
AnxiolyticsBenzodiazepines
Psychotropic drugsAlcoholOpiatesAmphetaminesCocaine
Dr.Hassaan Ali 2014

I. Generalized
A. Generalized unresponsiveness
1. Primary lack of sexual arousability
2. Aging-related decline in sexual arousability
B. Generalized inhibition
1. Chronic disorder of sexual intimacy
Dr.Hassaan Ali 2014

II. Situational A. Partner-related
1. Lack of arousability in specific relationship
2. Lack of arousability owing to sexual object preference
3. High central inhibition owing to partner conflict or threat
B. Performance-related
1. Associated with other sexual dysfunction/s (e.g., rapid ejaculation)
2. Situational performance anxiety (e.g., fear of failure)
C. Psychological distress- or adjustment-related
1. Associated with negative mood state (e.g., depression) or major life stress (e.g., death of partner)
Dr.Hassaan Ali 2014

History taking (including drug intake).
physical examinations: testes, penis, signs of hypoandogenism.
Investigation
Dr.Hassaan Ali 2014

Dr.Hassaan Ali 2014

Medical
Surgical
Psychiatric
Medication
Smoking
Alcohol
Recreational drug use
Dr.Hassaan Ali 2014

International Index of Erectile Function questionnaire (IIEF) most common questionnaire
addresses erectile function, orgasmic function, desire, intercourse satisfaction, overall satisfaction
Erectile function 1,2,3,4,5,15
Intercourse satisfaction 6,7,8
Orgasmic function 9,10
Sexual desire 11,12
Overall satisfaction 13,14
Dr.Hassaan Ali 2014

International Index of Erectile Function
5-item version for quick office evaluation
Score of 5-7 sever ED
Score of 8-11 moderate
Score of 12-16 mild to moderate
Score of 17-21mild
Score of 22- 25 no ED
Dr.Hassaan Ali 2014

Gradual onset
Normal ejaculation
Normal libido
Medical risk factor
Trauma/surgery/radiotherapy to pelvis
Current medication
Lifestyle
Dr.Hassaan Ali 2014

Sudden onset
Early collapse of erection
Self stimulated or waking erections
Premature ejaculation or inability to ejaculate
Problems/change in relationship
Major life event
Psychological problems
Dr.Hassaan Ali 2014

Genitourinary examination Testes size and consistency
Secondary sexual characteristics
Penis for Peyronie’s plaques,
Pulses (femoral), BP
Rectal examination
Dr.Hassaan Ali 2014

Laboratory Investigation
complete blood count,
urinalysis,
renal function,
lipid profile,
fasting blood sugar,
thyroid function.
Routine endocrinologic testing remains
controversial
Dr.Hassaan Ali 2014

1-Young patients who have always had
difficulty in obtaining and/or sustaining
an erection
2-Patients with a history of trauma
3-Where an abnormality of the testes or
penis is found on examination.
4-Patients unresponsive to medical
therapies that may desire surgical
treatment for ED.
Dr.Hassaan Ali 2014

1-Nocturnal penile tumescence and rigidity (NPTR)
2-vascular studies:Combined intracavernous injection & stimulation (CIS)
Duplex ultrasound
Dynamic infusion cavernosometry & cavernosography (DICC)
Selective penile angiography
3-neurological studies (e.g. bulbocavernosusreflex latency,nerve conduction studies);
4-endocrinological studies;
5-specialised psycho diagnostic evaluation.
Dr.Hassaan Ali 2014

3 B
.
4 B
4 B
GRLE Recommendations for the diagnostic work-up
B3Clinical use of a validated questionnaire related
to ED may help assess all sexual function
domains and the effect of a specific treatment
modality.
B3Physical examination is needed in the initial
assessment of ED to identify underlying medical
conditions associated with ED
B4Routine laboratory tests, including glucose-lipid
profile and total testosterone, are required to
identify and treat any reversible risk factors and
modifiable lifestyle factors.
B4 Specific diagnostic tests are indicated by only a
few conditions.
Dr.Hassaan Ali 2014

Total tumescence time 20% of night at puberty Adults – 27 minutes/nigh
RigiScan - 1985Monitors radial rigidity, tumescence, number, duration of erectile events
Portable – can use at home
Can record 3 different nights up to 10 hrs each
Results
Radial rigidity >70% = good erection
<40% = flaccid penis
Normal = 3-6 erections/night, 10-15 minutes per episode NEVA
deviceUses electrobioimpedance to assess volumetric changes in penis during nocturnal erections
Undetectable alternating current from glans to hip electrodes
Penile base electrode measures impedance & changes in penile length
Mean volume change in controls = 213% increase (14.4 mL)
Dr.Hassaan Ali 2014

Inject vasodilator, stimulate,
Bypasses neurologic & hormonal influences to evaluate vascular status
Use:
alprostodil 10-20ug
papaverine & phentolamine (Bimix 0.3 mL)
Trimix 0.3 mL
27 or 29g needle, compress for 5 min after injection
Normal results = normal venous occlusion
False negative up to 20% w/ borderline arterial flow
Dr.Hassaan Ali 2014

Penile blood flow study (CIS & blood flow measurement by US) is most reliable & least invasive evidence based assessment of EDRed = towards probe
Blue = away from probe
Can visualize dorsal & cavernous arteries in real time
Can diagnose high flow priapism
TechniqueMeasure flow velocities 5-10 min after injection
Rate erectile quality
Look at both cavernous arteries & diameters
Asymmetric cavernous arterial flow >10cm/s or reversal of flow across a collateral may mean atherosclerotic lesion
Dr.Hassaan Ali 2014

Peak Systolic Velocity (PSV)PSV < 25 correlates with abnormal pudendalarteriography
Severe unilateral arterial insufficiency >10 cm/s asymmetry
Severe vascular ED, diameter increase is <75%, diameter rarely exceeds 0.7 mmHigh systolic flow (>25 cm/s)
Persistent end-diastolic flow (EDV) (>5 cm/s)
Resistive Index (RI)RI = PSV – EDV/PSVMeasure 20 min after injection & stimulation
RI > 0.9 normal
RI < 0.75 venous leakage
Dr.Hassaan Ali 2014

Intracavernosal injection with color duplex Doppler ultrasound Most informative diagnostic test
Least invasive for vascular ED, high vs. low flow priapism, Peyronie’s plaque
Useful measurements
PSV, cavernous artery diameter, EDV, RI
PSV <25 = severe cavernous artery insufficiency
PSV >35 = normal inflow
Negative relationship between age & PSV
Dr.Hassaan Ali 2014

Cavernous arterial occlusion pressureBasically penile blood pressure measurement – 1989
TechniqueInject vasodilator
infuse saline into corpora to get pressure > systolic BP
apply Doppler to penile base
Pressure when cavernous arterial flow becomes detectable is cavernous artery systolic occlusion pressure (CASOP)
Gradient between cavernous & brachial artery pressure <35 & equal pressure on L & R is normalPharmacologic ArteriographyTechniqueInject vasodilatorCannulate internal pudendal arteryInject contrastLook at anatomy of iliac, internal pudendal, penile arteriesAberrant anatomy in 50% of normal volunteersUseful for anatomy, not functionIndication:Young pt w/ ED due to traumatic arterial disruption or perineal compression injury. Essential for planning reconstruction
Dr.Hassaan Ali 2014

Pharmacologic Cavernosometry & CavernosographyCavernosometry
Saline infusion while monitoring intracavernouspressure
Assesses penile outflow
Cavernosography
Infusion of contrast into corpora after vasodilator induced erection
Good for young men who may be candidates for penile vascular operations
Dr.Hassaan Ali 2014

Penile Brachial Pressure Index
Inaccurate
Penile Plethysmography
Penile pulse volume recording
Infrared Spectrophotometry
Radioisotopic Penography
MRA
Cavernous Smooth Muscle Content
Dr.Hassaan Ali 2014

Only certain types of ED have the potential to be cured with specific treatments:General Measures
Smoking cessation
Reduce alcohol
Weight loss
Exercise
Hormonal: testosterone failure – give testosterone
contraindicated in men (prostate carcinoma or with symptoms of prostatism.)
Post-traumatic arteriogenic: surgical penile revascularization has a 60-70% long-term success
Psychogenic: underlying problem, sex therapy/counselling, phosphodiesterase type-5 inhibitors (sildenafil, tadalafil, vardenafil)
Dr.Hassaan Ali 2014

PDE-5 inhibitors potentiate NO’s effect
Do not increase NO levelsNeed sexual stimulation for PDE-5 inhibitors to work
Sildenafil (Viagra)
FDA approved 1998
Vardenafil (Levitra)
FDA approved 8/2003
Tadalafil (Cialis)
FDA approved
11/2003
Dr.Hassaan Ali 2014

TadalafilVardenafilSildenafil
15 min – 2 hr15 min – 1 hr15 min - 1
hrOnset of Action
17.5 hr4-5 hr3-5 hrHalf-life
Not tested15%40%Bioavailability
No effect↓↓ Absorption↓↓
AbsorptionFatty Food
YesYesYesHA, flushing, dyspepsia
YesRare RareBachache, Myalgia
RareRareYesBlurred/Blue vision
NoYesNoPrecaution w/
antiarrhythmics
YesYesYesContraindication w/
nitratesDr.Hassaan Ali 2014

Newer agents Avanafil
Post Radical Prostatectomy
Diabetes
Acts 15 min
No effect with food
Dr.Hassaan Ali 2014

25-50% placebo responseAcupuncture – psychogenic EDAndrostenedione – may benefit men w/ low testosterone, lowers HDL 10%Ginko biloba – may have blood-thinning effectKorean red ginseng – may benefitL-Arginine – precursor to Nitric Oxide, may lower BPYohimbine – most supplements contain little or none, can have serious side effectsZinc – good if low zinc, can be immunosuppressive
Dr.Hassaan Ali 2014

Plastic cylinder connected to vacuum
generating source place constriction ring
after engorgement
Remove ring within 30 min
Satisfaction rate 68-83%
Adverse effects:pain, petechiae,
bruising,
numbness
Dr.Hassaan Ali 2014

Papaverine
Phentolamine (alpha1 & alpha2-antagonist)
Alprostadil (Caverject & Edex 2-40mcg) -
Prostaglandin E1
CombinationsPapaverine + Phentolamine
Papaverine + Phentolamine + Alprostadil
Dr.Hassaan Ali 2014

Isolated from opium poppy
Inhibitory effect on PDE, increased cAMP & cGMP, blocks calcium channels
1-2 hr half-life
Good
Low cost
Stable at room temp
Bad
Priapism (up to 35%)
Corporal fibrosis (1-33%) due to acidity
<55% effective
Not FDA approved
Dr.Hassaan Ali 2014

alpha1 & alpha2-antagonist
Side effects
Hypotension
Reflex tachycardia
Nasal congestion
GI upset
30 min half-life
Increases corporal blood flow, but does not
cause significant increase in intracavernous
pressure
Dr.Hassaan Ali 2014

(Caverject & Edex 2-40mcg) - Prostaglandin E1
Exogenous form of a naturally occurring fatty acid
Causes smooth muscle relaxation, vasodilation, inhibition of platelet aggregation by elevating cAMP
Metabolized by prostaglandin-15-hydroxydehydrogenase in corpora cavernosa
96% locally metabolized after 60 min
Side effects
Pain at injection site or during erection
Hematoma
Priapism
Much lower incidence of fibrosis
Once reconstituted into liquid from powder, has shortened half-life if not refrigerated
Dr.Hassaan Ali 2014

Papaverine + Phentolamine
Papaverine + Phentolamine + Alprostadil
Lower incidence of painful erection
As effective as alprostadil alone
Good for failed therapy or painful erection w/ PGE1
Serious side effects
Priapism
Fibrosis
Contraindications
Sickle cell
Schizophrenia
Other severe psychiatric disorders
Severe systemic illness
Dr.Hassaan Ali 2014

Intraurethral suppositories
“MUSE” (Medicated urethral system for erectionAlprostadil (125mg,
250mg, 500mg,1g
Dr.Hassaan Ali 2014

TypesMalleable prosthesisADV: Low Mechanic Failure / Ease of useDISADV: Constant rigidity / ▲ Erosion Risk
Positional prosthesisSemiRigid – Articulating Segments
Better to maintain up/down positions
2 – piece inflatable prosthesisADV: Ease of implantationDISADV: ▲ Mechanical Failure Risk
Dr.Hassaan Ali 2014

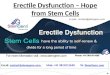
3 – piece inflatable penis
Most closely resembles natural flaccidity
and erection
Provide penile girth expansion and rigidity
Dr.Hassaan Ali 2014

Dr.Hassaan Ali 2014

Dr.Hassaan Ali 2014

Subcoronal – malleable or positional
Infrapubic - reservoir placement under direct
vision
Penoscrotal – better corporeal exposure, no
dorsal nerve injury, pump fixation possible
Dr.Hassaan Ali 2014

Dr.Hassaan Ali 2014

Foley removed next day
Antibiotic for 1 week
Oral narcotic used for 1 week
Restrict lifting activities if reservoir present
Have pts practice pumping 1 month after
sx
Dr.Hassaan Ali 2014

INFECTIONS – No significant illness, but to eradicate infection, removal of prosthesis is required.
To avoid it:
-Delay implanation if UTI or cutaneous inf
-Shave day of surgery
-Prevent by 10 minute skin prep
-Gent vancomycin
-Silicone has a sterile charge and should be irrigated
Dr.Hassaan Ali 2014

Infections occur either
1st few weeks - gram negative
After 6 months – gram positive Staph epi
Role of diabetes is controversial as related to
infection probability
EARLY INFECTIONS
Swelling, erythema, tenderness, drainage
Occasional fever
LATE INFECTIONS
Skin may be adherent to pump
Erosion is evidence of infection
REMOVE ALL COMPONENTS
Dr.Hassaan Ali 2014

Re-Implant?To minimize scarring of corporeal dilation, perform as soon as possible to PREVENT SCARRING AND PENILE SHORTENING
Rifampin/Minocycline coated prosthesis showed less infection rate than hydrophilic
coated devices.
IF mechanical failure, usually after 5 years
Dr.Hassaan Ali 2014

If dilator perforates proximal corpora, use a
larger dilator & allow perforation to heal
If dilator perforates urethra, ABANDON
PROCEDURE; place catheter 7-10 days
Can avoid by keeping tip of dilator under
dorsolateral surface of corpus cavernosum
If erosion of one cylinder:
REMOVE THAT CYLINDER. OK w/ one
Dr.Hassaan Ali 2014

“Concorde” type glans after placement b/c of
undersized, or inadequate dilation
SST DEFORMITY
Oversized cylinders cause pain and can erode
Dr.Hassaan Ali 2014

Peyronie’s disease
Scarring in tunic albuginea
Corporoplasty likely needed if length and girth
expanders used
If relaxing incision are done and gap is greater
than 1 cm, must cllose to prevent herniation
of cylinders
Dr.Hassaan Ali 2014

thanks
Dr.Hassaan Ali 2014