8/3/2019 Cardiac Anomalies in the Fetus
http://slidepdf.com/reader/full/cardiac-anomalies-in-the-fetus 1/11
Cardiac Anomaliesin the Fetus
Christopher G. B.Turner, MDa, Wayne Tworetzky, MD
b,c,
Louise E. Wilkins-Haug, MD, PhDd, Russell W. Jennings, MD
e,f,*
As the most frequent congenital anomaly and the leading cause of death among
infants in the United States, congenital heart disease (CHD) is an attractive target
for fetal therapy. With the development of successful neonatal repair for many types
of CHD over the last 20 years, earlier postnatal therapy to restore physiologic anatomy
has been encouraged, and fetal therapy has become the next frontier. Concurrent
advances in interventional catheterization and fetal imaging provided a foundation
for the novel field of fetal cardiac intervention. This article focuses on the current status
of in utero catheter interventions for CHD with particular interest in therapy for defects
characterized by progressive stenosis or atresia of the semilunar valves, the aortic andpulmonary, with development of subsequent ventricular hypoplasia.
FETAL CIRCULATION
In the normal fetal circulation, oxygenated blood from the umbilical vein is able to
stream efficiently through the foramen ovale (FO) to the left heart and up to the brain.
The desaturated blood from the superior vena cava is directed through the ductus
arteriosus (DA) back to the placenta for reoxygenation ( Fig. 1 ). Because pulmonary
a Department of Surgery, Children’s Hospital Boston, 300 Longwood Avenue, Fegan 3, Boston,MA 02115, USAb Department of Pediatrics, Harvard Medical School, 300 Longwood Avenue, Pavillion 2,Boston, MA 02115, USAc Fetal Cardiology Program, Children’s Hospital Boston, 300 Longwood Avenue, Fegan 3,Boston, MA 02115, USAd Department of Maternal Fetal Medicine, Brigham and Women’s Hospital, 75 Francis St.,Boston, MA 02115, USAe Department of Surgery, Harvard Medical School, 300 Longwood Avenue, Pavillion 2, Boston,MA 02115, USAf
Advanced Fetal Care Center, Department of Surgery, Children’s Hospital Boston, 300Longwood Avenue, Fegan 3, Boston, MA 02115, USA* Corresponding author. Advanced Fetal Care Center, Department of Surgery, Children’sHospital Boston, 300 Longwood Avenue, Fegan 3, Boston, MA 02115.E-mail address: [email protected] (R.W. Jennings).
KEYWORDS
Congenital heart disease Fetal intervention Hypoplastic left heart syndrome Pulmonary atresia Balloon dilatation Valvuloplasty
Clin Perinatol 36 (2009) 439–449doi:10.1016/j.clp.2009.03.015 perinatology.theclinics.com
0095-5108/09/$ – see front matter ª 2009 Elsevier Inc. All rights reserved.

8/3/2019 Cardiac Anomalies in the Fetus
http://slidepdf.com/reader/full/cardiac-anomalies-in-the-fetus 2/11
vascular resistance is higher than systemic vascular resistance, blood shunts through
the DA from the right side to the left, diverting around the lungs. At the moment of birth,
however, pulmonary vascular resistance suddenly drops, the shunt reverses, andblood flows through the lungs. As the FO and DA close in the postnatal period, two
distinct circuits are formed, the pulmonary and systemic vasculatures.
With severe semilunar valve pathology, however, there is only a single functional
ventricular pump, the left ventricle in the case of pulmonary atresia (PA), and the right
ventricle in the case of aortic stenosis (AS). In these situations, the DA is essential to
continue perfusion to the systemic or pulmonary vasculature, and the FO is essential
to allow the mixture of oxygenated and deoxygenated blood in the single ventricle
system. As blood flows preferentially through the patent FO rather than the high-pres-
sure ventricle, however, the reduction in flow through the ventricle retards growth, and
in part, contributes to eventual hypoplasia.In addition to semilunar pathology, if the atrial septum is intact (IAS) or severely
stenosed, the circuit on the side of the atretic semilunar valve will become obstructed.
In the extremely rare case of PA with a stenotic atrial septum, the fetal circulation is
impaired and often not compatible with fetal life. In the case of established hypoplastic
left heart syndrome (HLHS) with an intact atrial septum, the postnatal circulation is
impaired and not compatible with neonatal life.
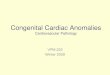
Fig. 1. Normal intracardiac fetal circulation. Physiologic shunting through the patentforamen ovale (FO) and the patent ductus arteriosus (DA). Oxygenated blood from theplacenta (red arrows ) reaches the right atrium (RA) by means of the inferior vena cava(IVC). This well-oxygenated blood is shunted preferentially from the RA across to the left
atrium (LA) through the FO and then is ejected out the left ventricle (LV) to the ascendingaorta (AO). Deoxygenated blood (blue arrows ) returning from the superior vena cava (SVC)preferentially travels from RA into the RV, then out through the main pulmonary artery(PA). Because of the high pulmonary vascular resistance in the fetal lungs, this deoxygen-ated blood bypasses lungs and enters the descending aorta by means of the DA. (From
Insaba AF. Cardiac disorders. In: Marx JA, editor. Rosen’s emergency medicine: conceptsand clinical practice. 6th edition. Philadelphia: Elsevier; 2006. p. 2568; with permission.)
Turner et al44 0

8/3/2019 Cardiac Anomalies in the Fetus
http://slidepdf.com/reader/full/cardiac-anomalies-in-the-fetus 3/11
The most common indication for a fetal cardiac intervention is to attempt to prevent
the development of right or left ventricular (LV) hypoplasia. In the approach to fetal
cardiac interventions for semilunar valve stenosis, therefore, there are two funda-
mental conditions:
One must understand the in utero characteristics of the heart defect that wouldpredict progression to ventricular hypoplasia.
One must understand the characteristics of the heart defect that indicate that an in
utero intervention might lead to improvement in cardiac growth and function.
Moreover, one needs to understand the features that indicate the heart defect is too
far advanced and that fetal intervention would be futile and provide unnecessary risk
to the mother and fetus.
DIAGNOSTIC STUDIES
Echocardiography is the preferred modality for screening and determining the severity
of semilunar valve stenosis. Color Doppler imaging can identify reduced flow through
the aortic valve and retrograde flow in the transverse aortic arch, the hallmark of
evolving HLHS in this defect. The pressure gradient across the valve is affected by
the degree of stenosis and the competitive retrograde arch flow, as well as the func-
tion of the left ventricle. A low gradient therefore may indicate a stenotic valve with
poor LV function. Other indicators of LV dysfunction and evolving HLHS include retro-
grade flow in the aortic arch supplied via the ductus arteriosus, diminished mitral valve
diastolic excursion with reduced inflow, left-to-right flow across the FO, or left-to-right
bulge of an intact atrial septum.1–4
Also, although rare, a thrombus can form in thedilated left ventricle.
Thousands of prenatal screening ultrasounds are needed to detect a small number
of cardiac defects. Despite increased screening and improved detection rates, most
cardiac defects remain undiagnosed prenatally. If CHD is suspected, the mother
should be referred to a pediatric cardiologist as soon as possible. This early referral
allows for confirmation of the diagnosis, appropriate counseling, and arrangement
for delivery and treatment at a center capable of treating complex congenital heart
defects.5,6 Early prenatal diagnosis also allows for the option of palliative or thera-
peutic in utero interventions for amenable cardiac defects.7–9 Because these therapies
are available at only a few centers, early prenatal detection is critical. Increased overallscreening rates, improved detection, and earlier referral will allow for more patients to
potentially benefit from in utero interventions.
CONGENITAL HEART DEFECTS APPROPRIATE FOR FETAL INTERVENTION
Fetal intervention offers the tantalizing possibility to reverse the pathologic process
before significant cardiac structural and functional deterioration has occurred. Early
relief of semilunar valve stenosis in utero may reverse the progression toward ventric-
ular hypoplasia.10–12 This section discusses the specific defect on the left and right
side.
Defects on the Left Side
Aortic valve defects in the fetus range from mild stenosis with an adequately sized
ventricle to severe stenosis with evolving HLHS, a term that implies that the left ventricle
is unable to sustain systemic circulation. With a patent FO, blood in the left atrium flows
Cardiac Anomalies in the Fetus 441

8/3/2019 Cardiac Anomalies in the Fetus
http://slidepdf.com/reader/full/cardiac-anomalies-in-the-fetus 4/11
preferentially to the low-pressure right atrium rather than the high-pressure left
ventricle. The resultant diminished flow through the left heart causes arrest of LV growth
and HLHS. Occasionally the left ventricle can be of normal size, but the myocardium
becomes damaged and fibrotic with significantly reduced filling and poor systolic func-
tion. In fetuses with aortic stenosis and an intact or restrictive atrial septum, there is no
low-pressure outlet for blood entering the left heart, so the left atrium and ventricle may
become severely dilated. This may lead to severe mitral regurgitation from mitral
annular dilation, with the resultant elevated pressure and compression of the right heart
causing right heart failure and hydrops fetalis. Patients with HLHS, one of the most
serious CHDs, require palliative surgery at birth to make the right ventricle the system-
ically functioning ventricle, or occasionally primary neonatal heart transplantation.
Therefore severe aortic valve stenosis with evolving HLHS is the defect for which fetal
intervention is most likely to be considered.1–3,7–9,13–15
Several centers have offered in utero aortic valvuloplasty as an alternative treatment
for midgestation fetal AS, with a high probability of progression of HLHS.7,9,14,16 The
objective of fetal aortic valvuloplasty is to relieve the obstruction to LV ejection,
thereby reducing LV work and damage, increasing flow through the left heart, and
slowing or preventing the progression to HLHS. Recent studies from the authors’
center demonstrate that fetal aortic valvuloplasty may increase blood flow through
the left heart and improve left heart growth.14,16 An oversized balloon was associated
with moderate or severe aortic regurgitation that was tolerated by the fetus and
improved through the gestation.16
To achieve maximal benefit from the procedure, it must be performed before the
occurrence of irreversible pathology. Much remains unknown with respect to the evolu-
tion of this CHD.17,18
Early attempts at fetal aortic valvuloplasties performed in the thirdtrimester were too late in gestation to reverse the disease, demonstrating that the
window for intervention must occur as early as possible during the second trimester.
Based on the current understanding of the risk–benefit ratio of fetal intervention,
fetal aortic valvuloplasty should not be performed in fetuses with AS that will not other-
wise progress to HLHS. Anatomic dimensions of left heart structures at the time of
diagnosis alone do not predict progression to HLHS. Instead, physiologic aberrations
such as reversed blood flow in the transverse aortic arch, left-to-right flow across the
FO, monophasic mitral valve inflow, and moderate-to-severe LV dysfunction in midg-
estation are important signs of evolving HLHS.19 These findings may be useful for
identifying appropriate candidates for fetal aortic valvuloplasty.The presence of an intact or highly restrictive atrial septum (I/HRAS) is a predictor
of poor outcome among patients with HLHS.20–23 Maintenance of a postnatal circu-
lation depends on an atrial septal defect (ASD) to allow the left atrium to decom-
press into the right heart. Without an adequate ASD, left atrial hypertension
prevents adequate pulmonary flow, and these infants die shortly after birth without
immediate intervention. Anatomic studies have described an intact atrial septum in
approximately 6% of patients with HLHS, and clinically deleterious restriction to
flow at the level of the atrial septum occurring in as many as 22%.24,25 In a recent
series at a major referral center with aggressive management involving prenatal
diagnosis and planned delivery, survival was only 28%.26 At the authors’ institution,a series of 24 fetuses that underwent attempted ASD creation in utero revealed that
the procedure can be performed with a high rate of technical success. Of 21 at-
tempted procedures, 19 were technically successful. Creation of a defect greater
than or equal to 3 mm was associated with better postnatal oxygenation and
less frequent need for emergent postnatal intervention, but it was not shown to
improve survival.27
Turner et al442

8/3/2019 Cardiac Anomalies in the Fetus
http://slidepdf.com/reader/full/cardiac-anomalies-in-the-fetus 5/11
Defects on the Right Side
In a similar fashion to aortic valve disease, pulmonary valve disease occupies a spec-
trum from mild stenosis to severe atresia. Pulmonary atresia with an intact ventricular
septum (PA/IVS) produces hypoplastic right heart syndrome (HRHS). Some fetuses
with severe tricuspid regurgitations may develop high central venous pressures andresultant fetal hydrops. The size and rate of growth of the fetal tricuspid valve accu-
rately predicts postnatal outcomes and may be used for selecting patients for fetal
therapy.28 In addition, a right ventricular (RV)-dependant coronary artery supply
results in increased mortality after birth and is considered the most severe form. These
infants will require a palliative circulation or transplantation. If the fetus is likely to
require single ventricle palliation after birth, some fetuses with PA/IVS are appropriate
candidates for fetal intervention.
Unlike the left ventricle, the right ventricle has some capacity to grow postnatally,
and RV decompression in infancy allows the potential for RV growth. RV decompres-
sion in utero presumably also should lead to RV growth. Several attempts have beenmade at treating this defect in utero, but there have been no reports in which the infant
did not require postnatal surgery also.29–31 Further evolution in the technique for right-
sided heart interventions is needed, which may also benefit additional defects such as
tetralogy of Fallot with pulmonary atresia and hypoplastic pulmonary arteries.
PROCEDURE
Technique
Several techniques have been attempted for fetal balloon valvuloplasty. The least
invasive involves maternal sedation with percutaneous access to the fetus, as origi-nally described by Allan.7–9 A more invasive technique involves a laparotomy to
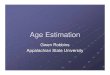
Fig. 2. Ideal fetal position and cannula course for aortic valvuloplasty. Course of cannulacorresponds to unobstructed pathway from maternal abdomen to left ventricle apex toaortic valve. (From Tworetzky W, Wilkins-Haug L, Jennings RW, et al. Balloon dilation ofsevere aortic stenosis in the fetus: potential for prevention of hypoplastic left heartsyndrome: candidate selection, technique, and results of successful intervention. Circulation2004;110(15):2127; with permission.)
Cardiac Anomalies in the Fetus 443

8/3/2019 Cardiac Anomalies in the Fetus
http://slidepdf.com/reader/full/cardiac-anomalies-in-the-fetus 6/11
expose the uterus, which allows for easier manipulation of the fetus, improved ultra-
sound image quality, and shorter distance to the fetal heart. The most invasive tech-
nique involves a uterine incision and fetal exposure, which allows for femoral and
carotid artery access.32 The more invasive techniques offer direct contact and the
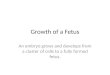
Fig. 3. Ultrasound images of percutaneous in utero aortic valvuloplasty for aortic stenosis.( A) Aortic valve flow before intervention. (B) Alignment of needle. (C ) Guide wire acrossaortic valve in ascending aorta. (D) Inflated balloon across the aortic valve. (E ) Aortic valveflow after intervention.
Turner et al44 4

8/3/2019 Cardiac Anomalies in the Fetus
http://slidepdf.com/reader/full/cardiac-anomalies-in-the-fetus 7/11
possibility of improved technical success, but these benefits occur at the cost of
increased maternal morbidity and premature delivery. Therefore, less-invasive percu-
taneous techniques when possible are preferable.
Techniques at Children’s Hospital Boston and Brigham and Women’s Hospital have
evolved with the collaboration of many departments. Percutaneous transthoracic cardiac
puncture has been most effective, with minimal maternal risk.The access point to thefetal
heart depends on the type of procedure. All procedures are performed under two-dimen-
sional ultrasound guidance. The needle used to access the fetal heart is preferably as
small as possible, such as a 19G cannula. A minilaparotomy is performed to expose
the uterus only if certain factors require it, such as fetal position, anterior placenta, and
maternal body habitus.
For aortic balloon valvuloplasty, the large dilated left ventricle is the most easily ac-
cessed structure with proximity to the aortic valve. The cannula and stylet needle are
advanced through the maternal abdomen, uterine wall, and fetal chest wall ( Fig. 2 ).
The cannula, guide wires, and balloon shafts are premeasured and marked, allowing
positioning within the fetal heart by both external measurements and ultrasound
imaging. Correct fetal positioning is critical; the left ventricle is entered only when:
The left chest is anterior.
There are no limbs between the uterine wall and apex.
The apex is within 9 cm of the abdominal wall.
The outflow track is parallel to the cannula course.
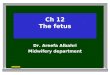
Fig. 4. Ultrasound images of percutaneous in utero pulmonary valvuloplasty for pulmonaryatresia with intact ventricular septum. ( A) Needle aimed at pulmonary valve. (B) Guide wireacross pulmonary valve in pulmonary artery. (C ) Inflated balloon across the pulmonary valve.(D) Pulmonary valve flow after intervention.
Cardiac Anomalies in the Fetus 445

8/3/2019 Cardiac Anomalies in the Fetus
http://slidepdf.com/reader/full/cardiac-anomalies-in-the-fetus 8/11
The balloon valvuloplasty itself is performed with a small coronary artery balloon
over a thin, floppy-tipped guide wire. The balloon is inflated with pressure gauges to
precise inflation diameters. Flow across the dilated aortic valve is confirmed with
echocardiography ( Fig. 3 ).
For pulmonary balloon valvuloplasty, the right ventricle is accessed, although it
makes a more difficult target than the left because of small size, complex geometry,
and valvular atresia. The same principles of measurement and position are used.
Flow across the dilated pulmonary valve is confirmed with echocardiography
( Fig. 4 ).
For atrial septoplasty, the right atrium is accessed through the right chest wall. An
unobstructed line is identified from the fetal right atrium, through the left atrium, and
into a left pulmonary vein. An 18G or 19G introducer cannula on a sharp metal obtu-
rator is advanced into the right atrium and against the atrial septum. The septum is
punctured by the tip of the introducer or, more commonly, with a 22G Chiba needle
(Cook Incorporated, Bloomington, IN). A wire then is introduced into the left atrium
or a pulmonary vein, and the Chiba needle is exchanged for a balloon angioplasty
catheter. The balloon is inflated fully several times before the cannula is removed.
Flow across the new atrial septal defect is confirmed with echocardiography ( Fig. 5 ).
Anesthesia
Anesthesia is a necessary element of any of these procedures. Although maternal
sedation is possible, inhaled anesthetic allows for maximal uterine relaxation and
easy conversion to an open procedure if necessary. Additional fetal anesthesia is
Fig. 5. Ultrasound images of percutaneous in utero atrial septoplasty for hypoplastic leftheart syndrome. ( A) Needle penetrating left atrium from right atrium. (B) Balloon acrossatrial septum. (C ) Atrial septum flow after intervention.
Turner et al44 6

8/3/2019 Cardiac Anomalies in the Fetus
http://slidepdf.com/reader/full/cardiac-anomalies-in-the-fetus 9/11
administered through an intramuscular injection, which allows for fetal manipulation
and optimal positioning. At Children’s Hospital Boston, a combination of fentanyl,
pancuronium, and atropine are used. Atropine counteracts the bradycardia that can
occur with fetal and uterine manipulation.
COMPLICATIONS
Fetal complications are usually treatable. Bradycardia is common with needle access
to the ventricle, occurring in about 50% of cases, and uncommon with needle access
to the atrium. The arrhythmia resolves by stopping manipulations or with intracardiac
administration of epinephrine, either into the muscle or by direct injection. Pericardial
effusions are also common and, if moderate to large, they can be drained successfully.
Low maternal complication rates also have been possible with in utero catheter
interventions. Despite well-executed procedures and extensive preprocedure evalua-
tion to exclude maternal contraindications, complications from the anesthesia, lapa-rotomy, and uterine manipulation do occur. A sick fetus can cause premature labor
or the maternal mirror syndrome, which resembles preeclampsia and requires delivery
of the fetus.
SUMMARY
On the frontier of pediatric cardiology, fetal cardiac interventions for CHD offer a prom-
ising therapeutic option for those conditions with significant morbidity and mortality
from current palliative operations. Early detection and referral of all fetuses with sus-
pected CHD would increase the number of patients that may benefit. Concurrent
multidisciplinary collaboration between perinatologists, cardiologists, fetal surgeons,
and anesthesiologists will improve patient selection criteria, techniques for safe
access to the fetus, the performance of the procedure, and perioperative care.
REFERENCES
1. Sharland GK, Chita SK, Fagg NL, et al. Left ventricular dysfunction in the fetus:
relation to aortic valve anomalies and endocardial fibroelastosis. Br Heart J
1991;66(6):419–24.2. McCaffrey FM, Sherman FS. Prenatal diagnosis of severe aortic stenosis. Pediatr
Cardiol 1997;18(4):276–81.
3. Simpson JM, Sharland GK. Natural history and outcome of aortic stenosis diag-
nosed prenatally. Heart 1997;77(3):205–10.
4. Berning RA, Silverman NH, Villegas M, et al. Reversed shunting across the ductus
arteriosus or atrial septum in utero heralds severe congenital heart disease. J Am
Coll Cardiol 1996;27(2):481–6.
5. Tworetzky W, McElhinney DB, Reddy VM, et al. Improved surgical outcome after
fetal diagnosis of hypoplastic left heart syndrome. Circulation 2001;103(9):
1269–73.6. Bonnet D, Coltri A, Butera G, et al. Detection of transposition of the great arteries
in fetuses reduces neonatal morbidity and mortality. Circulation 1999;99(7):916–8.
7. Maxwell D, Allan L, Tynan MJ. Balloon dilatation of the aortic valve in the fetus:
a report of two cases. Br Heart J 1991;65(5):256–8.
8. Allan LD, Maxwell DJ, Carminati M, et al. Survival after fetal aortic balloon valvo-
plasty. Ultrasound Obstet Gynecol 1995;5(2):90–1.
Cardiac Anomalies in the Fetus 447

8/3/2019 Cardiac Anomalies in the Fetus
http://slidepdf.com/reader/full/cardiac-anomalies-in-the-fetus 10/11
9. Kohl T, Sharland G, Allan LD, et al. World experience of percutaneous ultrasound-
guided balloon valvuloplasty in human fetuses with severe aortic valve obstruc-
tion. Am J Cardiol 2000;85(10):1230–3.
10. Tweddell JS, Hoffman GM, Mussatto KA, et al. Improved survival of patients
undergoing palliation of hypoplastic left heart syndrome: lessons learned from
115 consecutive patients. Circulation 2002;106(12 Suppl 1):I82–9.
11. Fishman NH, Hof RB, Rudolph AM, et al. Models of congenital heart disease in
fetal lambs. Circulation 1978;58(2):354–64.
12. Hornberger LK, Sanders SP, Rein AJ, et al. Left heart obstructive lesions and left
ventricular growth in the midtrimester fetus. A longitudinal study. Circulation 1995;
92(6):1531–8.
13. Daubeney PE, Sharland GK, Cook AC, et al. Pulmonary atresia with intact ventric-
ular septum: impact of fetal echocardiography on incidence at birth and post-
natal outcome. UK and Eire Collaborative Study of Pulmonary Atresia with
Intact Ventricular Septum. Circulation 1998;98(6):562–6.
14. Tworetzky W, Wilkins-Haug L, Jennings RW, et al. Balloon dilation of severe
aortic stenosis in the fetus: potential for prevention of hypoplastic left heart
syndrome: candidate selection, technique, and results of successful intervention.
Circulation 2004;110(15):2125–31.
15. Vida VL, Bacha EA, Larrazabal A, et al. Hypoplastic left heart syndrome with
intact or highly restrictive atrial septum: surgical experience from a single center.
Ann Thorac Surg 2007;84(2):581–5 [discussion: 586].
16. Marshall AC, Tworetzky W, Bergersen L, et al. Aortic valvuloplasty in the fetus:
technical characteristics of successful balloon dilation. J Pediatr 2005;147(4):
535–9.17. Sinclair BG, Sandor GG, Farquharson DF. Effectiveness of primary level antenatal
screening for severe congenital heart disease: a population-based assessment.
J Perinatol 1996;16(5):336–40.
18. Carvalho JS, Mavrides E, Shinebourne EA, et al. Improving the effectiveness of
routine prenatal screening for major congenital heart defects. Heart 2002;88(4):
387–91.
19. Makikallio K, McElhinney DB, Levine JC, et al. Fetal aortic valve stenosis and the
evolution of hypoplastic left heart syndrome: patient selection for fetal interven-
tion. Circulation 2006;113(11):1401–5.
20. Photiadis J, Urban AE, Sinzobahamvya N, et al. Restrictive left atrial outflowadversely affects outcome after the modified Norwood procedure. Eur J Cardio-
thorac Surg 2005;27(6):962–7.
21. Stasik CN, Gelehrter S, Goldberg CS, et al. Current outcomes and risk factors for
the Norwood procedure. J Thorac Cardiovasc Surg 2006;131(2):412–7.
22. Daebritz SH, Nollert GD, Zurakowski D, et al. Results of Norwood stage I opera-
tion: comparison of hypoplastic left heart syndrome with other malformations.
J Thorac Cardiovasc Surg 2000;119(2):358–67.
23. Canter CE, Moorehead S, Huddleston CB, et al. Restrictive atrial septal commu-
nication as a determinant of outcome of cardiac transplantation for hypoplastic
left heart syndrome. Circulation 1993;88(5 Pt 2):II456–60.24. Forbess JM, Cook N, Roth SJ, et al. Ten-year institutional experience with pallia-
tive surgery for hypoplastic left heart syndrome. Risk factors related to stage I
mortality. Circulation 1995;92(Suppl 9):II262–6.
25. Rychik J, Rome JJ, Collins MH, et al. The hypoplastic left heart syndrome with
intact atrial septum: atrial morphology, pulmonary vascular histopathology, and
outcome. J Am Coll Cardiol 1999;34(2):554–60.
Turner et al44 8

8/3/2019 Cardiac Anomalies in the Fetus
http://slidepdf.com/reader/full/cardiac-anomalies-in-the-fetus 11/11
26. Glatz JA, Tabbutt S, Gaynor JW, et al. Hypoplastic left heart syndrome with atrial
level restriction in the era of prenatal diagnosis. Ann Thorac Surg 2007;84(5):
1633–8.
27. Marshall AC, Levine J, Morash D, et al. Results of in utero atrial septoplasty in
fetuses with hypoplastic left heart syndrome. Prenat Diagn 2008;28(11):1023–8.
28. Salvin JW, McElhinney DB, Colan SD, et al. Fetal tricuspid valve size and growth
as predictors of outcome in pulmonary atresia with intact ventricular septum.
Pediatrics 2006;118(2):e415–20.
29. Arzt W, Tulzer G, Aigner M, et al. Invasive intrauterine treatment of pulmonary
atresia/intact ventricular septum with heart failure. Ultrasound Obstet Gynecol
2003;21(2):186–8.
30. Tulzer G, Arzt W, Franklin RC, et al. Fetal pulmonary valvuloplasty for critical
pulmonary stenosis or atresia with intact septum. Lancet 2002;360(9345):1567–8.
31. Galindo A, Gutierrez-Larraya F, Velasco JM, et al. Pulmonary balloon valvulo-
plasty in a fetus with critical pulmonary stenosis/atresia with intact ventricular
septum and heart failure. Fetal Diagn Ther 2006;21(1):100–4.
32. Adzick NS, Harrison MR. Fetal surgical therapy. Lancet 1994;343(8902):897–902.
Cardiac Anomalies in the Fetus 449
Recommended