CANCER CHEMOTHERAPY
PRINCIPLES
DR RASHA HAGGAG


Characteristics of Cancer Cells
• The problem:
– Cancer cells divide rapidly (cell cycle is accelerated)
– They are “immortal”– Cell-cell communication is altered– uncontrolled proliferation– invasiveness – Ability to metastasise

Cell Cycle = Growth, Division


• After completion of mitosis, the resulting daughter cells have two options:
• (1) they can either enter G1 & repeat the cycle or • (2) they can go into G0 and not participate in the cell
cycle.• The ratio of proliferating cells to cells in G0, is called
the growth fraction.
• A tissue with a large percentage of proliferating cells & few cells in G0 has a high growth fraction.
• • Conversely, a tissue composed of mostly of cells in G0
has a low growth fraction.


• Cell Cycle Specific Drugs:
• Antimetabolites• Bleomycin peptide antibiotics• Vinca alkaloids
• Cell Cycle non-Specific Drugs:
• Alkylating agents• Antibiotics (Dactinomycin)• Cisplatin
Chemotherapeutic Agents
Effective for high growth-fraction-malignancies, such as hematologic cancers.
Effective for both low-growth (solid tumors) and high growth fraction malignancies

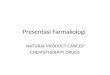
Log kill hypothesis
• According to the log-kill hypothesis, chemotherapeutic agents kill a constant fraction of cells (first order kinetics), rather than a specific number of cells, after each dose
1. Solid cancer tumors - generally have a low growth fraction thus respond poorly to chemotherapy & in most cases need to be removed by surgery
2. Disseminated cancers- generally have a high growth fraction & generally respond well to chemotherapy

Log kill hypothesis:

Clinical Implications of Fractional Cell Kill

Role of Chemotherapy in Cancer Treatment
(1) Metastatic Cancer: Palliative or
Curative Chemotherapy
(2) Adjuvant Chemotherapy:
to eradicate or control micro-metastasis
(3) Neo-adjuvant Chemotherapy:
to make Surgery of RT possible
to alleviate surgical damage
to eradicate micro-metastasis
(4) Hematological Malignancies:
Primary Treatment

ANTICANCER DRUGS

1. Alkylating agents:
• Major interaction: Alkylation of DNA
• Binds to nucleophilic groups on various cell constituents. Including DNA
• These drugs react with carboxyl, sulfhydryl, amino, hydroxyl, and phosphate groups of cellular
constituents. • Primary DNA alkylation site: N7 position of guanine
(other sites as well) • Major Toxicity: bone marrow suppression
Chemotherapeutic Agents
CyclophosphamaideCarboplatinCisplatinOxaliplatinDacarbazine

Chemotherapeutic Agents2. Antimetabolites:
•Structurally related to normal compounds that exist within the cell.
•Interfere with the availability of normal purine or pyrimidine nucleotide precursors, either by inhibiting their synthesis or by competing with them in DNA or RNA synthesis.
•Their maximal cytotoxic effects are in S-phase and therefore are cell-cycle specific.
5-Fluoro UracilGemcitabineCyterabineMethotrexate

3. Microtubule Inhibitors:
• These are plant-derived substances .
• Cause cytotoxicity by affecting the equilibrium between the polymerized and depolymerized forms of the microtubules.
• Vinca alkaloids inhibit microtubule polymerization and increase microtubule disassembly. The mitotic spindle apparatus is disrupted, and segregation of chromosomes in metaphase is arrested.
Chemotherapeutic Agents
Vinca AlkaloidsVincristine VinblastineVinorelbine
TaxanesPaclitaxelDocetaxel

4. Antineoplastic Antibiotics:
• Interacts with DNA, leading to disruption of DNA function.
• Also Inhibit topoisomerases (I and II) and produce free radicals.
• Cell-cycle nonspecific.
• Eg: Actinomycin D binds with double-stranded DNA and blocks the action of RNA polymerase, which prevents DNA transcription.
Chemotherapeutic Agents
BleomycinDoxorubicinDactinomycinDaunorubicin

5. Hormonal Agents:
• Commonly involves the use of glucocorticoids.• Direct antitumor effects are related to their
lympholytic properties;.• Glucocorticoids can inhibit mitosis, RNA synthesis,
and protein synthesis in sensitive lymphocytes.
• Considered cell-cycle nonspecific . • Resistance to a given glucocorticoid may develop
rapidly and typically extends to other glucocorticoids.
Chemotherapeutic Agents
PrednisoneTamoxifenEstrogensFlutamideNilutamideBicalutamide

• Antibodies that are made in the lab rather than by a person's own immune system.
• Directed at specific targets and often have fewer adverse effects.
• Designed to recognise and find specific abnormal proteins on cancer cells.
• Each monoclonal antibody recognizes one particular protein.
Chemotherapeutic Agents
Rituximab TrastuzumabCetuximabBevacizumab
6. Monoclonal Antibodies:

• Three types of monoclonal A-bodies:
1. Trigger the immune system to attack and kill cancer cells. E.g. Rituximab (Mabthera)
2. Stop cancer cells from taking up proteins E.g. Trastuzumab (Herceptin).
3. Carry cancer drugs or radiation to directly to cancer cells These are called conjugated MABs.
E.g. Ibritumomab (Zevalin)
Chemotherapeutic Agents
Rituximab TrastuzumabCetuximabBevacizumab

Combination Chemotherapy
• Rationale:– minimize resistance– maximize synergy/additivity– avoid drugs of overlapping toxicity– biochemical considerations

Combination Chemotherapy
• Rationale:–biochemical considerations:
• addition of an agent to overcome drug resistance (eg MDR inhibitor & vinca alkaloid)
• cooperative inhibition (eg leucovorin & 5FU)• inhibition of drug breakdown (eg DPD inhibitor
& 5FU)• rescue host from toxic effects of drug (eg
leucovorin following high-dose methotrexate)


ROUTES OF ADMINISTRATION
• Intravenous • Oral• Intraperitoneal Therapy• Intrathecal and Intraventricular Therapy• Intra-arterial Therapy• Prolonged Intravenous Infusion Chemotherapy• Other Routes of Administration: Intravesical therapy
Intrapleurally

Dosing Chemotherapeutics
• Body surface area• mg/kg• Total dose• Dose to pharmacokinetic target
– AUC.– Therapeutic monitoring laboratory capability
required.

• DRUG INTERACTIONS WITH CHEMOTHERAPEUTIC
AGENTS

Interactions with METHOTREXATE
• Aspirin, Cotrimoxazole, Penicillin, Nsaids (Indomethacin, Ketoprofen);
Inhibition Of Tubular Secretion Of Methotrexate :
Prolonged Excretion Of Methotrexate And Enhanced Toxicity.

Interactions with 6-MERCAPTOPURINE
• 6-mercaptopurine (6-MP) or azathioprine with ALLOPURINOL.
• 6-MP (or azathioprine) toxicity (thrombocytopenia, granulocytopenia) is enhanced and may be fatal.
• The dose of 6-MP or azathioprine should be decreased to one-third to one-fourth the normal amount when allopurinol is used concurrently

Interactions with PHENYTOIN
• The initial decrease in phenytoin concentration shortly after receiving various chemotherapeutic agents and dose increase leads to phenytoin toxicity.
• Phenytoin should have blood concentrations measured 24-72 hours after receiving chemotherapy and adjust the dose accordingly.

TOXICITIES OF SOME ANTICANCER
DRUGS

ADR of Antineoplastic Drugs in Humans Tissue Undesirable Effects
Bone marrow Leukopenia and resulting infections
Immunosuppression
Thrombocytopenia
Anemia
GI tract Oral or intestinal ulceration
Diarrhea
Hair follicles Alopecia
Gonads Menstrual irregularities, including premature
menarche; impaired spermatogenesis
Wounds Impaired healing
Fetus Teratogenesis (especially during first trimester)

Distinctive Toxicities of Some Anticancer DrugsToxicity Drug(s)
Renal Cisplatin,* methotrexate
Hepatic 6-MP, busulfan, cyclophosphamide
Pulmonary Bleomycin,* busulfan, procarbazine
Cardiac Doxorubicin, daunorubicin
Neurologic Vincristine,* cisplatin, paclitaxel
Immunosuppressive
Cyclophosphamide, cytarabine, dactinomycin, methotrexate
Other Cyclophosphamide (hemorrhagic cystitis); procarbazine (leukemia); asparaginase* (pancreatitis)
*Less Bone marrow suppression – “marrow sparing”

Prevention or Management of Drug Induced toxicities
• The toxicities of some anticancer drugs can be well anticipated and hence be prevented by giving proper medications
E.g. • mesna is given to prevent hemorrhagic
cystitis by cyclophosphamide• Dexrazoxane, is used to reduce the risk of
anthracycline-induced cardiomyopathy

•Dose Modifications

Dosage Modification for Myelosuppression
PLATELET COUNT(x 109/L)
ABSOLUTE NEUTROPHIL (ANC)*(x 109/L)
> 1.8 1.5-1.8 1.0-1.5 <1.0
> 10070-10050-70<50
100%75%50%0%
75%75%50%0%
50%50%50%0%
0%0%0%0%


• BCCA Protocol Summary for Adjuvant Therapy for Breast Cancer:
using Doxorubicin and Cyclophosphamide



Recommended