-
7/30/2019 l14 Cancer Chemotherapy
1/47
CANCER CHEMOTHERAPY
-
7/30/2019 l14 Cancer Chemotherapy
2/47
CANCER(neoplastic disease): disease
characterized by uncontrolled cell division,
invasion and metastasis.
Multiple factors may be involved :
*sex, age, race, genetic predisposition;
*environmental factors: radiation, chemical
carcinogens,( those in tobacco smoke), viruses ( HBV, HCV,
HIV,
EBV) etc.
-
7/30/2019 l14 Cancer Chemotherapy
3/47
Cancer treatment modalities:
- surgery, radiotherapy, chemotherapy;
CHEMOTHERAPY:
1) Primary induction therapy- primarytreatment in advanced
cancers with no otheralternative;
2) Neoadjuvant chemotherapyin localized
disease in situations when surgery/RT/bothcannot be used;
3) Adjuvant chemotherapy-to RT / surgey/both.
-
7/30/2019 l14 Cancer Chemotherapy
4/47
-The anticancer drugs:
-either kill cancer cells or modify their growth.
- most act on the proliferating population of
cells.
-they act against metabolic sites essential forcancer cell
replication
- these drugs do not specifically recognize
cancer cells and affect all proliferating cells bothnormal and
abnormal cells (they are one of the
most toxic drugs used in therapy).
-
7/30/2019 l14 Cancer Chemotherapy
5/47
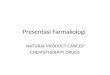
A schematic summary of cell cycle
kinetics is presented in next figure:
-
7/30/2019 l14 Cancer Chemotherapy
6/47
Anticancer drugs may be:
*CELL CYCLE SPECIFIC DRUGS (CCS):
They act specifically on cells undergoing cycling:
Antimetabolites, Bleomycin, Vinca alkaloids
*CELLCYCLE NONSPECIFIC (CCNS) DRUGS:
They act in both cycling and resting states
(alkylating agents, some antibiotics).
-
7/30/2019 l14 Cancer Chemotherapy
7/47
The role of drug combinations: - it provides maximal cell
kill;
-it provides a broader range of interactionsbetween drugs and
and tumour cells;
-it may prevent /slow development of
resistance.Principles in selecting drugs in the most
effective combination: *efficacy; * mechanism of
interactions
*toxicity; * avoidance of arbitrary
*optimum scheduling; dose changes
-
7/30/2019 l14 Cancer Chemotherapy
8/47
Eg. of drugs combinations:
ACRONYMS:
ABVD: doxorubicin(
adriamycin)+bleomycin+vinblastine+dacarbazine
MOPP : mechlorethamine+
vincristine+procarbazine+prednisone
-
7/30/2019 l14 Cancer Chemotherapy
9/47
GENERAL TOXICITY OF CYTOTOXIC
DRUGS
Tissues with rapidly multiplying cells are
affected in a dose dependent manner by
majority of drugs.
* Bone marrow: -depression with
granulocytopenia, agranulocytosis,
thrombocytopenia, aplastic
anemiainfections and bleedings are theusual complications.
-
7/30/2019 l14 Cancer Chemotherapy
10/47
Lymphoreticular tissue : lymphocytopenia and
inhibition of lymphocyte function suppression of
cell mediated and humoral immunity.The mostimportant are the
opportunistic infections with
Candida , viruses ( herpes zoster, cytomegalovirus),
pneumocystis carinii, toxoplasma gondii.
Gastrointestinal tract: stomatitis, diarrhoea,haemorrhages ,
nausea, vomiting( due to the
stimulation of the chemoreceptor trigger zone and
generation of emetic impulses from the upper
gastrointestinal tract);
Skin :alopecia due to damage to the cells in hair
follicles; dermatitis.
-
7/30/2019 l14 Cancer Chemotherapy
11/47
Gonads:inhibition of gonadal cells witholigozospermia,
inhibition of ovulation,amenorrhoea.
Foetus:cytotoxic drugs in pregnant woman:abortion, foetal death,
teratogenesis.
Carcinogenicity:secondary cancers( appear with
greater frequency many years after the use ofcytotoxic
drugs).
Hyperuricaemia:gout, urate stones.
-
7/30/2019 l14 Cancer Chemotherapy
12/47
Classification of anticancer drugs
(according to the mechanism of action)
1)Antimetabolites ;
2)Alkylating agents;
3)Antibiotics;
4)Vinca alkaloids;5)Taxanes;
6)Epipodophyllotoxin;
7)Camptothecin analogues;
8)Miscellaneous;
9) Hormones and antihormones.
-
7/30/2019 l14 Cancer Chemotherapy
13/47
1)ANTIMETABOLITES
They are structurally similar to normal DNAcomponents and they
generally inhibit synthesis ofnormal purine / pyrimidines or folic
acid or competewith them in DNA or RNA synthesis.
They act especially in S phase.
a)Folic acid antagonists
b)Purine antagonists
c)Pyrimidine antagonists
-
7/30/2019 l14 Cancer Chemotherapy
14/47
a)Folic acid antagonistsMethotrexate : inhibition of
dihydrofolate reductase
decreased DNA synthesis and cell death. It also affects RNA
synthesis and protein synthesis
-
7/30/2019 l14 Cancer Chemotherapy
15/47
-orally or i.v.
*acute leukemias in childrens in maintainingremission ;
*choriocarcinoma,
*breast cancer, head, neck, bladder cancerlung carcinoma and in
high doses inosteogenic sarcomas.
*immunosuppressant.
-Major toxicity: on bone marrow.!The toxic effects on normal
cells may be
reduced by administration ofFolinic acid(Leucovorin).
-
7/30/2019 l14 Cancer Chemotherapy
16/47
b)Purine antagonists Mercaptopurine (6MP) ) a structural
analog
of hypoxanthine
Thioguanine (6TG) a structural analog of
guanine
-
7/30/2019 l14 Cancer Chemotherapy
17/47
Mercaptopurine (6MP) )
* a structural analog of hypoxanthine
* It is converted to nucleotide form inhibitseveral enzymes
involved in purine metabolism,with inhibition ofpurine ring.
Clinical uses: *the maintenance of the remission ofchildhood
acute leukemia; myelogenousleukemia,granulocytic leukemia.
Side effects: *bone marrow depression.
*Hyperuricaemia, hepatotoxicity;*6MP causes more nausea and
vomiting than 6-TG
-
7/30/2019 l14 Cancer Chemotherapy
18/47
Thioguanine (6TG) a structural analog ofguanine
Clinical uses: in acute myelogenous leukemia(+cytarabine and
daunorubicin)
Acute lymphoblastic leukemia.
Side effects:
* bone marrow depression.
*Hyperuricaemia
In acute leukemia, both have been used incombination regimens to
induce remission and 6-MP to maintain it.
-
7/30/2019 l14 Cancer Chemotherapy
19/47
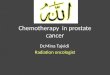
c)Pyrimidine antagonists
Fluorouracil (5-FU) -a pyrimidine analog
It is converted in the body to the
corresponding nucleotide which inhibits
thymidylate synthetase critical for the
synthesis of thymine nucleotides inhibition
of DNA synthesis.
-
7/30/2019 l14 Cancer Chemotherapy
20/47
-
7/30/2019 l14 Cancer Chemotherapy
21/47
Clinical uses: orally, i.v. and topically.
* slowly growing solid tumors (breast, ovarian,
pancreatic, colorectal,urinary, liver), i.v.
* skin cancers topically (premalignant keratoses,
cutaneous basal cell carcinomas).
Side effects:
* bone marrow depression, severe ulceration of
the oral and GI mucosa, neurotoxicity.
-
7/30/2019 l14 Cancer Chemotherapy
22/47
Cytarabine
*i.v.,in acute myelogenous leukemia(in
combination)
*Hodgkins disease and non Hodgkin lymphoma.
* bone marrow depression
-
7/30/2019 l14 Cancer Chemotherapy
23/47
2)ALKYLATING AGENTS
1.Nitrogen mustards:
mechloretammine,cyclophosphamide,
chlorambucil, melphalan
2.Nitrosoureas: carmustine, lomustine,
semustine
3.Alkyl sulfones: Busulfan
4. Triazenes: Dacarbazine
-
7/30/2019 l14 Cancer Chemotherapy
24/47
They exert their cytotoxic effects by covalently binding to
various cellular constituents. The major reaction is alkylation
of
N7 (nitrogen position 7) of guanine within DNA.
-
7/30/2019 l14 Cancer Chemotherapy
25/47
1.Nitrogen mustards
Mechlorethamine*Hodgkins disease as a part of MOPP
regimen(vincristine, procarbazine, prednisone)
and non Hlymphomas.It is given i.v.
*It causes severe bone marrow depression,
nausea, vomiting.
-
7/30/2019 l14 Cancer Chemotherapy
26/47
CyclophosphamideIt is inactive as such and must be activated
tocytotoxic forms (aldophosphamide, phosphoramide
mustard and acrolein) in the liver by microsomalenzymes.
Clinical uses:
* ovarian and breast cancers, H disease, lung cancer;
it is used orally or i.v., alone or as a part of a regimen.*as
immunosuppressant
Side effects:
-hemorrhagic cystitis (caused by chemical irritation of
the bladder mucosa by acrolein);-alopecia, nausea, vomiting,
diarrhea;
-prolonged treatment can produce interstitialpulmonary fibrosis
and cardiomyopathy.
-
7/30/2019 l14 Cancer Chemotherapy
27/47
Chlorambucil:
It is a very slow acting alkylating agent
*the drug of choice for long term maintenance
therapy for chronic lymphatic leukemia (incombination with
prednisone). It is administeredorally.
Melphalan
* multiple myeloma, breast, ovarian cancer ;
* Bone marrow depression
-
7/30/2019 l14 Cancer Chemotherapy
28/47
2.Nitrosoureas: carmustine, lomustine,
semustine
They are highly lipid soluble and cross the
blood brain barrier making them useful in
malignancies of the CNS (meningeal leukemia
and brain tumors).
They cause delayed bone marrow
depression(it takes nearly 6 weeks to
develop).
-
7/30/2019 l14 Cancer Chemotherapy
29/47
3.Alkyl sulfones: Busulfan
It is the drug of choice for chronic myeloid
leukemia. It is given orally.Side effects: -endocrine
dysfunction(adrenalinsufficiency);pulmonary fibrosis is a
specificsideeffect;skinpigmentation;myelosuppression
;hyperuricaemia.4. Triazenes: Dacarbazine
They have primary inhibitory action on RNA andprotein
synthesis.It is activated in the liver.
Its most important indication is malignantmelanoma. It is
administered i.v.
It causes marked nausea, vomiting,myelosuppression.
-
7/30/2019 l14 Cancer Chemotherapy
30/47
ANTIBIOTICS
*Dactinomycin (Actinomycin D)
*Antracyclines : Doxorubicine ,Daunorubicine
Mitoxantrone
*Bleomycin
*Plicamycin
*Mitomycin C
-
7/30/2019 l14 Cancer Chemotherapy
31/47
*Dactinomycin (Actinomycin D)
-Wilms tumour, rhabdomyosarcoma, Ewings
sarcoma, soft tissues sarcomas, Kaposis
sarcomas, i.v. (with surgery and Vincristine)
(+/- RT)
-as immunosuppressive agent
- The major side effect: bone marrow
depression.
-
7/30/2019 l14 Cancer Chemotherapy
32/47
*Antracyclines
-Doxorubicine: Hodgkins (H) disease ( ABVDregimen), solid tumors
(of the breast,ovary,endometrium, testicle , stomach, liver ,
lung) and acute leukemia;i.v.It causes
irreversibledose-dependent cardiotoxicity.
-Daunorubicine- used in acute myeloid leukemias;it causes bone
marrow depression, GI
disturbances, alopecia.-Mitoxantrone-analogue of doxorubicine ,
used in
prosatate cancer
-
7/30/2019 l14 Cancer Chemotherapy
33/47
*Bleomycin
-testicular carcinoma(+Cisplatin and Vinblastine)
- H disease and nonH lymphomas and
carcinomas of the head, neck, skin,
genitourinary tract;
- It has mucocutaneous toxicity and causes
pulmonary fibrosis
-
7/30/2019 l14 Cancer Chemotherapy
34/47
*Plicamycin:
-embryonal testicular cancer, disseminated cancers
-highly toxic drug
*Mitomycin C
-resistant cancers of stomach, colon, cervix, rectum,
bladder.
-It causes bone marrow and gastrointestinal toxicity.
-
7/30/2019 l14 Cancer Chemotherapy
35/47
VINCA ROSEA ALKALOIDS:
VINBLASTINE AND VINCRISTINE
Vincristine(i.v. route):- derived from the periwinkle plant
Vinca
Rosea.
Clinical uses:
-childhood acute lymphoblastic leukemia,
-H disease and nonH lymphomas(MOPP regimen), s
-solid tumors in children and tumors of the breast, lung in
adults.
Adverse effects: peripheral neuropathy, alopecia, GI
disturbances, autonomic nervous system dysfunctions.Vinblastine(
i.v.) : used in metastatic testicular carcinoma( in
combination) and H disease; it causes bone marrow depression
( leucopenia)
Vinorelbine : lung, ovarian,breast cancers.
-
7/30/2019 l14 Cancer Chemotherapy
36/47
Mechanism of action:
inhibit tubulin polymerization which disrupts
assembly of microtubules an important part ofthe cytoskeleton
and the mitotic spindle
mitotic arrest in metaphasecell death.
-
7/30/2019 l14 Cancer Chemotherapy
37/47
TAXANES
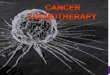
Mechanism of action:
They function as mitotic
spindle poisons : they
bind to microtubules with
enhancement of tubulin
polimerization finally
inhibition of mitosis andcell division.
-
7/30/2019 l14 Cancer Chemotherapy
38/47
Paclitaxel
- by i.v. infusion
-metastatic ovarian and breast carcinoma after failure offirst
line chemotherapy and relapse cases;
-advanced cases of head,neck cancer, small cell lungcancer,
esophageal carcinoma.
- It causes myelosuppression, neuropathy.
Docetaxel-It is a more potent congener of paclitaxel-same
clinical uses
- It causes neutropenia
-
7/30/2019 l14 Cancer Chemotherapy
39/47
EPIPODOPHYLLOTOXINS
ETOPOSIDE and TENIPOSIDE are semisynthetic glycosidesof the
activepodophyllotoxin extracted from the mandrakeplant.
Mechanism of action: at low c% they block cells at the
S-G2interface ; at high c% they cause G
2
arrest; they stimulateDNA topoisomerase II to cleave DNA.
Etoposide : used in lung, prostate, testicular carcinomas
( orally and i.v.).
It causes GI irritation, bone marrow depression(dose
limiting
leucopenia), alopecia; Teniposide resistant acute lymphoblastic
leukemia.
It causes bone marrow depression (leucopenia),
alopecia,gastrointestinal disturbances.
CAMPTOTHECIN ANALOGUES
-
7/30/2019 l14 Cancer Chemotherapy
40/47
CAMPTOTHECIN ANALOGUESTopotecan and Irinotecan: semisynthetic
analogues of
camptothecin, an antitumour principle obtained
from a Chinese tree.
They inhibit the activity of topoizomerase I , the key
enzyme responsible for cutting and religating single
DNA strandsDNA damage. Topotecan- metastatic carcinoma of ovary
and small
cell lung cancer after primary chemotherapy has
failed. The major toxicity is bone marrow depression
(specially neutropenia).
Irinotecan prodrug decarboxylated in the liver to
the active metabolite ;used in metastatic / advanced
colorectal carcinoma, lung/cervix/ovary cancers etc.
-
7/30/2019 l14 Cancer Chemotherapy
41/47
MISCELLANEOUS
L-ASPARAGINASE- from E. coli
- degrades L-asparagine to L-aspartic acid,depriving cancer
cells of an essential metabolite
and may cause cell deathClinical uses: childhood lymphoblastic
leukemia
Side effects:-liver damage, -pancreatitis,-CNSsymptoms,-allergic
reactions (being a foreign
protein).
-
7/30/2019 l14 Cancer Chemotherapy
42/47
CISPLATINis an inorganic platinum complex.
Mechanism of action :-similar to that of alkylatingagents.
Clinical uses: testicular tumors - alone/incombination,ovarian
carcinoma, bladder
carcinoma.
Side effects: renal dose dependent dysfunction;
nausea,vomiting;acoustic nerve dysfunction.
-
7/30/2019 l14 Cancer Chemotherapy
43/47
CARBOPLATIN- chemically related to cisplatin
-it is used alone in persistent or recurrent
ovarian carcinoma (i.v.)
-it causes dose- dependent marrow depression
(thrombocytopenia)
-
7/30/2019 l14 Cancer Chemotherapy
44/47
PROCARBAZINE : inactive as such
After metabolic activation it depolymerizes DNAand causes
chromosomal damage. Inhibitionof nucleic acid synthesis also
occur.
It is a component of MOPP regimen for
Hodgkins disease non Hodgkin lymphomasand oat cell carcinoma of
lung. It is givenorally.
Side effects:vomiting, leucopenia,thrombocytopenia,
dermatitis.
-
7/30/2019 l14 Cancer Chemotherapy
45/47
HORMONES and ANTIHORMONES
1.SEX HORMONES
They are used in hormone dependent cancers to
change the hormonal balance.
-androgens:testosterone propionate:in advancedbreast cancer with
metastasis;
-antiandrogens: -Flutamide: antagonizes androgen
action on prostate carcinoma and has palliative
effect in advanced or metastatic cases.
-
7/30/2019 l14 Cancer Chemotherapy
46/47
-estrogens: -diethylstilbestrol/ ethynylestradiol:
carcinoma prostate;
-antiestrogens:Tamoxifen- it is effective in breast
cancer in both pre as well as postmenopausalwomen; also
effective in carcinoma of
endometrium
-progestins: hydroxyprogesterone: someadvanced,recurrent (after
surgery or radiotherapy) and
metastatic endometrial carcinoma
-
7/30/2019 l14 Cancer Chemotherapy
47/47
2. ADRENAL CORTICOSTEROIDSParticularly the glucocorticoid
analogues
(hydrocortisone, prednisone)have been usefulin acute childhood
leukemia, lymphomas, andother hematological cancers and in
advancedbreast cancer.
3 . GOSERELIN ACETATE ; LEUPROLIDEThey are synthetic peptide
analogues of naturally
GR hormones.
They inhibit the release of follicle stimulating
hormone(FSH) and luteinizing hormone (LH), withreduced
testicular androgen synthesis.They areused in metastatic prostate
carcinoma.