Case 5
Call For A Slide Seminar Of African Cases (…And Not Only…)
06/09/2017
João Fraga, Paula Serra, Catarina Cerdeira, Ana Catarina Lai, Maria Beatriz Pimentão, Rui Almeida, Helder Moreira, BrunoFernandes, Graça Fernandes, Raquel Pina

Enterprise | Interest
Nothing to declare.

Clinical history
Male, 39 years old
Chronic alcoholism (120g / day)
No history of chronic liver disease / portal hypertension
Symptoms: morning nausea and vomiting
201720152011
Primary Health Care
CHUC
40 years
Symptoms: matinal nausea and vomiting
2012
Abdominal ultrasound: "Moderate volumeperitoneal effusion surrounding the liver andalso in the pelvic excavation."
Upper abdominal CT: "Peritoneal effusion in the upperabdomen; subperitoneal thickening of the mesenteryroot and densification of the great epiploon "
IPORefractory ascitis of
unknown cause

Clinical history201720152011
Primary Health Care
CHUC
2012
43 years
Symptoms: abdominal pain(1 month duration)
Physical examination: bulky andpainful abdomen
Toraco-abdomino-pelvic CT:“Massive peritoneal effusion in all quadrants of the abdomen. Densification of the large omentum.
Peritoneal carcinomatosis can not be excluded. "
No analytical changes

Smear (Papanicolau 200x)
Biopsy (HE 100x)
Cell-Block (HE 100x)
Cyt
olo
gy Histo
logy
Gastroenterology - diagnostic paracentesis andperitoneal biopsy

BerEp4 100x
Calretinin 100x
EMA 100x
Caldesmon 100x
Ki-67 100x
Immunohistochemistry
Cell-block
Desmin 100x
Calretinin 100x
Ki-67 100x
BiopsyBerEp4 100x
Differential diagnosisReactive mesothelial proliferation
Mesothelioma
Metastatic disease

Follow-up
Clinical diagnosis of "Ascites of indeterminate cause"
Medicated with furosemide 40id, spironolactone 100id and alcohol cessation
Clinical history review: No exposure to asbestos

Clinical history
45 years
Symptoms: abdominalpain and distension, increscendo in the lastmonths
Abdominal ultrasound: "Massive peritoneal
effusion in all quadrants of the abdomen, free aspect"
No analytical changes
201720152011
Primary Health Care
CHUC
2012Regular evacuation paracentesis

Laparoscopy: • Thick, congestive peritoneum• Large ascitic effusion, dispersed
throughout all quadrants - aspiration of about 15L with harvest for cytologicalstudy
• Performed appendectomy + epiplon biopsy + parietal peritoneum biopsypsy
Clinical history
201720152011
Primary Health Care
CHUC
2012Regular evacuation paracentesis
Right iliac fossa Right hypochondrium

Cytology
Smear (Giemsa 100x) Cell-Block (HE 100x)

BerEp4 100x Calretinin 200x
EMA 100x
WT1 100x
Ki-67 (12%) 200x
Immunohistochemistry
Differential diagnosisReactive mesothelial proliferation
Mesothelioma
Metastatic disease

Histology
HE 20x
Ileocecal appendix
HE 200x
Appendicectomy -
pinkish, mat serosa

Histology
HE 40x
Epiploon Parietal peritoneum
HE 40x
Epiploon biopsy – witish, homogeneous, firm tissue Parietal peritoneum biopsy - white-pinkish, homogeneous and elastic tissue

CK 5,6 40x
BerEp4 40xCalretinin 40x EMA 40x
p53 200x Desmin 200x
Immunohistochemistry
Differential diagnosis
Reactive mesothelial proliferation
Well-differentiated papillary mesothelioma
Diffuse malignant peritoneal mesothelioma
Metastatic disease

Diagnosis
Diffuse malignant peritoneal mesothelioma, epithelioid, with tubulo-papillary pattern, involving serosa and subserosa of the ileo-cecal
appendix, mesoappendix, epiploon and peritoneum
Follow-up Patient proposed for intraperitonealchemotherapy
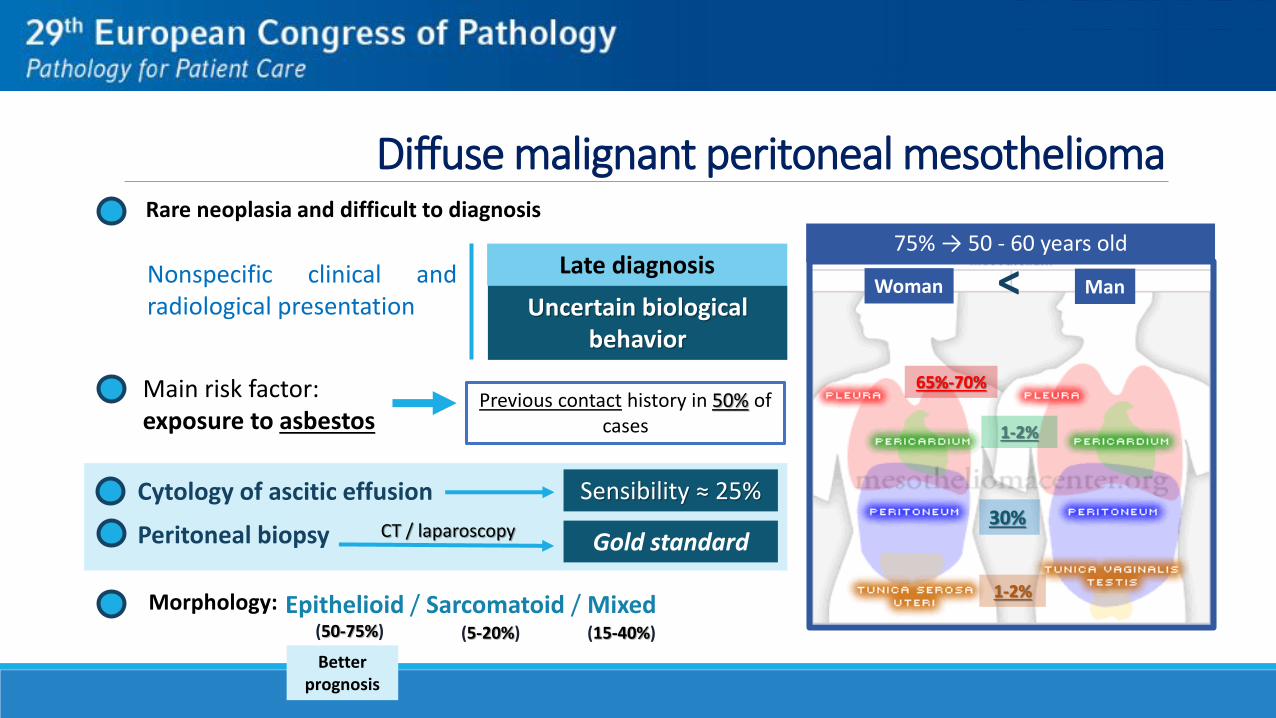
Diffuse malignant peritoneal mesothelioma
Main risk factor: exposure to asbestos
Previous contact history in 50% of cases
65%-70%
30%
1-2%
1-2%
Nonspecific clinical andradiological presentation
Late diagnosis
Uncertain biological behavior
Cytology of ascitic effusion Sensibility ≈ 25%
Peritoneal biopsy CT / laparoscopyGold standard
<75% → 50 - 60 years old
Morphology: Epithelioid / Sarcomatoid / Mixed(50-75%) (5-20%) (15-40%)
Rare neoplasia and difficult to diagnosis
Woman Man
Better prognosis

Thank You
Recommended

![Arun Agrawal - Accountability in Decentralization [a Framework With South Asian and West African Cases]](https://img.pdfslide.us/doc/110x75/5572144b497959fc0b9434b8/arun-agrawal-accountability-in-decentralization-a-framework-with-south-asian.jpg)