Are Primary Care Physicians Ready to Practice in a Consumer-Driven Environment?Results of a National Survey
Giridhar Mallya, M.D.Robert Wood Johnson Clinical Scholars Program
Leonard Davis Institute of Health EconomicsUniversity of Pennsylvania

Why focus on primary care physicians?
• CDHP benefit design is complicated
• Many common primary care services are not exempt from deductible
• Cost and quality information are limited
• Clinical decision-making is difficult
• Primary care doctors are a source of guidance

Aims
• To assess primary care physicians’• Knowledge of CDHP cost-sharing and savings accounts
• Readiness to advise patients on costs and budgeting for medical needs
• Attitudes with regard to quality-of-care information
• To compare physicians with and without CDHP enrollees in their practices

Methods
• Mailed survey of 1500 nationally-representative primary care physicians
• May-June 2007• GPs, FPs, general internists• $2 incentive with first mailing; 2 non-repsonse mailings
• 4-page questionnaire about CDHPs• CDHP knowledge• Brief description of plans• Advice on costs, budgeting• Attitudes regarding quality-of-care information

Methods
• 5-item response frames collapsed into 3 categories for analysis
• Descriptive statistics
• Multivariate regression for comparison of physicians with and without CDHP patients
• Adjusted for age, gender, specialty, board certification, practice size, academic affiliation, percent Medicaid, and geographic region

Results
• 49% adjusted response rate (528/1076)• 124 not primary care physicians
• 300 with undeliverable or inaccurate addresses
• Respondents more likely to be:• Female (32% vs. 27%, p=0.04)
• Board certified (86% vs. 81%, p=0.02)
• Family physicians/general practitioners (59% vs. 49%, p=0.002)
• No differences based on age or region

Experience with CDHPs
• 41% (210/528) of physicians had CDHP enrollees in their practices
• CDHP enrollees comprised a median of 5% of practice panels
• Interquartile range, 3%-7%
• Physicians with CDHP patients were less likely to care for a high percentage of Medicaid patients and less likely to be from the Northeast

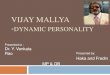
Knowledge of CDHPs
Low
Low
Low
Low
Medium
Medium
Medium
Medium
High
High
High
High
0% 20% 40% 60% 80% 100%
How money is spentfrom medical savings
account
How money iscontributed to
medical savingsaccount
Out-of-pocket costsfor CDHP enrollees
CDHPs in general

Knowledge among physicians with CDHP patients
• More likely to have high knowledge of: • CDHPs in general (5.31, 3.29-8.58)
• Patient cost-sharing in CDHPs ( 3.34, 2.12-5.26)
• How money is contributed to savings account (2.76, 1.85-4.14) • How money is spent from savings accounts (2.47, 1.66-3.68)
• 21% with low knowledge of CDHPs in general• 24% with low knowledge of cost-sharing • 18% with low knowledge of MSA contributions

Readiness to advise patients on financial matters
Ready or somewhat ready
Readiness to discuss:
Costs of medical care (in general) 73 (69-77)
Cost-effectiveness of medical care 76 (73-80)
Medical budgeting 48 (43-52)
Readiness to advise patients on the specific costs of:
Office visits 85 (82-88)
Medications 79 (76-83)
Laboratory tests 67 (63-71)
Radiologic studies 54 (50-59)
Specialist consultation 38 (33-42)
Hospital costs 33 (29-37)Notes: Percentage and 95% CI

Readiness among physicians with CDHP patients
• More ready to discuss costs of• Medical care in general (2.33, 1.48-3.68) • Medical budgeting (1.99, 1.35-2.92)
• No more ready to advise patients on costs of 5/6 specific services
• Office visits, lab tests, radiologic studies, specialty consultation, and hospitalization
• More ready with regard to costs of medications (1.68, 1.03-2.71)

Role of quality-of-care information in patient decision-making
Agree or strongly agree
Quality-of-care information should factor into patients’ choice of: (%)
Hospitals 45 (41-49)
Specialists 41 (37-45)
Patients can generally trust the quality-of-care information provided by: (%)
Government websites 21 (17-24)
Insurer websites 8 (6-10)Notes: Percentage and 95% CI

Role of quality-of-care information among physicians with CDHP patients
• No more likely to believe quality-of-care information should factor into patients’ choice of hospitals or specialists
• No more likely to trust quality-of-care information from government or insurer websites

Conclusions
• Physician knowledge of CDHP cost-sharing and savings accounts is limited
• Lesser but still significant extent among those with CDHP patients
• Generally ready to discuss issues of cost, but many not ready to advise patients on medical budgeting and the costs of certain common services
• Trust in quality-of-care information is very low and patients’ use of this information is not broadly supported

Implications
• Potential for poor decision-making• Non-exempt services, non-guaranteed employer contributions
• Limited time, disjointed decisions
• Low-income enrollees
• Possible tension in doctor-patient relationship, confusion for patients
• Track knowledge, adherence, outcomes
• Develop educational interventions for physicians and patients
• Expand access to standardized, point-of-care cost info
• Encourage doctor-patient dialogue about quality information and physician involvement in development of quality metrics

Co-Investigators
• Craig Pollack, MD, MHS• University of Pennsylvania, Robert Wood Johnson Clinical
Scholars Program, Philadelphia VA Hospital, Leonard Davis Institute of Health Economics
• Dan Polsky, PhD• University of Pennsylvania, Division of General Internal
Medicine, Leonard Davis Institute of Health Economics


Limitations
• Response bias• Board certification associated with higher knowledge
• Physician self-report rather than testing• Patients have resources other than physicians• Plan prevalence is still limited
• Skewed enrollment
• Physicians with CDHP enrollees: what’s the directionality?• Physicians’ roles: agency vs. aspiration
Recommended