OCHA Evaluation of Duty of Care | 59
Annexes
OCHA Evaluation of Duty of Care | 60
7 Annexes7.1 Annex 1: TOR and Scoping DocumentTerms of ReferenceEvaluation of OCHA’s Provision of Duty of Care15 December 2017
BackgroundThe recently drafted People Strategy affirmed that OCHA is an organization that adds value to the humanitarian system through its people and talent. OCHA Functional Review concluded that, in response to the financial constraints faced by the humanitarian system and the organization itself, OCHA staff are undertaking more activities with less resources, and are feeling spread thin and stretched. Moreover, OCHA is operating in some of the most dangerous places in the world; under the new paradigm “to stay and deliver”, OCHA staff are increasingly working in environments with weak capacity of host governments, marked by the threat of conflict or terrorist activity, and in which humanitarian workers themselves have become regular targets of attacks.
Through its People Strategy, OCHA has committed to, as part of its duty of care to staff members, foster an environment that values staff as its greatest resource, promote the health, security and well-being of its people serving in all duty stations, including a healthy work-life balance, in an atmosphere that is respectful, empowering, caring and free of harassment and discrimination. The Strategy envisions an establishment of a committee tasked with the development of a concrete action plan for its implementation.
This evaluation will assess OCHA’s approaches to providing duty of care to its staff and their family members, identify areas that can be improved, and capture good practices that can be useful to OCHA in the future. Given the need for OCHA to retain and attract talent, the evaluation will identify good practices and areas for improvement in the areas of safety, security, and wellbeing of OCHA staff. The results of the evaluation will feed into the work of the People Strategy and Management Committee, as well as of the Operations and Advocacy, and Administration functions.
Purpose, Scope, and Key Evaluation IssuesThe overall purpose of the evaluation is to clarify and strengthen OCHA’s provision of duty of care towards its staff and their eligible family members, particularly those in high-risk environments. The evaluation will cover all OCHA staff, including international and national, in general service, professional, and management positions, at the headquarters and in field locations.
More specifically, the evaluation will examine:
• Overall OCHA approach and any necessary improvements to the OCHA provision of duty of care in pre-deployment, deployment and post-deployment phases, including: safety, security, training provision, gender specific requirements, diversity supporting actions, financial, logistic and HR support, provision of entitlements, standards of living, medical support (including psychosocial), post-incident response and support, and survivor and eligible family member support;
• Application of UN Policies, effectiveness and efficiency of management practices, and identification of OCHA specific duty of care requirements beyond current UN policies; with consideration of the work and likely proposals of the High-Level Committee on Management (HLCM) established Task
OCHA Evaluation of Duty of Care | 61
Force on Duty of Care; OCHA’s effectiveness in creating an atmosphere that is respectful, empowering and free of harassment and discrimination.
The evaluation will identify gaps as well as lessons learned and best practices in OCHA and other UN entities, and identify ways in which coordination, collaboration and cooperation with relevant UN departments and agencies should be strengthened.
Evaluation MethodologyThe evaluation will employ mixed methods (qualitative, quantitative, and participatory) and a number of data collection tools. Data will be derived from primary and secondary sources, including literature review, desk review of relevant documents, key informant interviews, small group discussions, and a staff survey. The evaluation team will visit three countries with OCHA operations, selected during the inception phase. Perspectives from all stakeholders will be solicited, including OCHA management and staff at headquarters and in field, as well as key relevant personnel from UNDSS, DFS, DM, UNDP, and other UN entities.
Detailed methodology, including standardized data collection instruments (staff survey, interview guides, etc.), will be developed during the inception phase of the evaluation.
All data used will be triangulated for validation. The evaluation is expected to use the evaluation criteria of Relevance, Effectiveness, Efficiency, and Impact. The applicability of these criteria will be examined in the inception phase, during which additional criteria may be proposed.
Administrative arrangementsOCHA will appoint the Evaluation Manager, who will be the main point of contact for the evaluation, coordinate and supervise evaluation processes, and ensure use of appropriate data collection and analysis methods, adherence to professional norms and standards, and quality of evaluation processes and products. The Evaluation manager will participate in the field missions.Key OCHA stakeholders identified during the inception phase will be provided an opportunity to comment on all evaluation deliverables.
Evaluation TeamThe evaluation will require services of an Evaluation Team of up to four members with the following collective experience and skills:• Extensive evaluation experience of humanitarian strategies and programmes;• Senior-level work experience with United Nations, preferably in the areas of administration,
security, and human resources;• An appropriate range of field experience;• Experience in facilitating consultative workshops involving a wide range of organizations and
participants;• Excellent writing and communication skills in English.The Evaluation Team will include a Team Leader, who is responsible for the overall conduct of the evaluation in accordance with the ToR, including:• Developing and adjusting the evaluation methodology;• Managing the evaluation team, ensuring efficient division of tasks between mission members;• Ensuring the quality of all outputs; and• Submitting all outputs in a timely manner.
OCHA Evaluation of Duty of Care | 62
Deliverables and Reporting RequirementsThe quality of the evaluation report and other deliverables will be assessed according to the UNEG Evaluation Standards and OCHA Quality Assurance system. The inception and draft reports will be produced jointly by members of the evaluation team and reflect their collective understanding of the evaluation. All deliverables listed will be written in good Standard English and follow OCHA’s guidelines on writing evaluation reports. If in the estimation of the Evaluation Manager the reports do not meet this required standard, the Evaluation Team will ensure at their own expense the editing needed to bring it to the required standard.
A. Inception ReportThe Evaluation Team will produce an inception report of up to 5,000 words (excluding annexes), setting out:• The team’s understanding of the topic of the evaluation;• Any suggested deviations from the ToR, including any additional issues raised during the initial
consultations; • Evaluation framework and first and second-level questions;• An evaluation matrix showing, for each question, the indicators proposed and sources of
information; • The evaluation criteria to be used, including the rationale for using each particular evaluation
criterion and, if needed, for rejecting any of the criteria proposed in the ToR;• Methodology, including any changes to the proposed methodology, details of gender analysis,
and the triangulation strategy;• Methodological limitations and evaluability issues and how they will be addressed;• Stakeholder analysis and a plan for their involvement in the evaluation process;• Data collection tools (interview guides, survey instruments, and/or other tools) to be employed
for the evaluation;• Data collection plan and detailed fieldwork plan; and• Draft outline for the evaluation report
B. Interim ReportThe Evaluation Team will produce a short interim report outlining the preliminary findings (in bulleted format, and not longer than 2 pages) within one week after the completion of the field missions.
C. Evaluation ReportThe Evaluation Team will produce a single report, written in a clear and accessible manner, allowing the readers to understand readily evaluation findings and their inter-relationship. The report should not exceed 15,000 words (excluding annexes) and should be comprised of:• Stand-alone Executive Summary of no more than 2500 words;• List of acronyms;• Table of contents;• Summary table linking findings, conclusions and recommendations, including where responsibility
for follow up should lie;• Literature and document review;• Methodology summary (brief, with a more detailed description provided in an annex);• Main body of the report, including findings in response to the evaluation questions, conclusions and
recommendations;
OCHA Evaluation of Duty of Care | 63
• Annexes will include: (1) ToR, (2) Detailed methodology, (3) List of persons met, (4) Team itinerary, (5) Details of any quantitative analysis undertaken, (6) Evaluation tools employed, and (7) Bibliography;
• For accuracy and credibility, recommendations should be the logical implications of the findings and conclusions. Recommendations should follow logically from the evaluation findings and conclusions and be:1. Categorised as a) Critical, b) Important, or c) Opportunity for learning.2. Relevant, realistic and useful and reflect the reality of the context in which OCHA operates;3. Clearly stated and not broad or vague;4. Realistic and reflect an understanding of OCHA and the humanitarian system and potential
constraints to follow-up;5. Suggest where responsibility for follow-up should lie and include a timeframe for follow-
up.
D. Short (4 Page) summary of the Evaluation ReportE. Power-point presentation of the Evaluation ReportF. EvidenceMatrixusedbytheteamtoderivefindingsandconclusionsG. Comments Matrix, outlining the response of the evaluation team to comments
received by stakeholders
OCHA Evaluation of Duty of Care | 64
Scoping Document
Evaluation of OCHA’s Duty of Care to StaffScope and Focus
BackgroundThis document builds on the terms of reference for OCHA’s evaluation of its duty of care to staff, and provides further detail on the scope, focus and limits of the evaluation, and key evaluation questions. It also includes some adjustments of the terms of reference.
Scope and LimitsThe overall purpose of the evaluation is to clarify and strengthen OCHA’s provision of duty of care to-wards its personnel and their eligible family members. [This is an adjustment from the terms of refer-ence, which referred to OCHA staff and eligible family members.]
The term ‘personnel’ refers to all persons, national and international, in the employ of OCHA (except those who are both locally-recruited and paid on the basis of hourly rates), together with their spouses and recognized dependents regardless of their contractual status. It also includes for example consult-ants, staff on temporary assistance contracts and interns.57
For budgetary reasons, this evaluation has to be completed within a short timeframe. This means that some aspects of duty of care, even if relevant and important, will not be included in its focus, for the simple reason that it would not be possible to examine them within the timeframe.
The evaluation scope will be OCHA’s duty of care to all OCHA personnel, including international and na-tional, in general service, professional, and management positions, at the headquarters and in field lo-cations, on permanent, continuing, fixed-term, temporary and other contracts, plus their eligible family members. The evaluation will, however, particularly focus on staff having served or serving in high-risk environments including surge deployments.
Duty of care “constitutes a non-waivable duty on the part of [OCHA and the UN] to mitigate or otherwise address foreseeable risks that may harm or injure its personnel and their eligible family members,”58 as per the definition of the UN’s High-Level Management Committee. This evaluation will focus on three aspects of duty of care: safety, security and wellbeing. The inception report will provide the working definitions of safety, security and wellbeing used for the evaluation.
The evaluation’s scope will not cover: training other than security and safety-related training, career development, recruitment, OCHA’s duty of care to “implementing partners,” i.e., humanitarian organiza-tions implementing projects with money from OCHA-managed pooled funds.
The evaluation will focus on the last three years, 2015-2017. Relevant information from previous years may however be considered, such as major security incidents or relevant data.
[57] OCHAPolicyInstructiononSecurity(28February2013)[58] UNChiefExecutivesBoardforCoordination/High-LevelCommitteeonManagement:“FinalReport:HLCMWorkingGroupon“ReconcilingDutyofCare for UN personnel while operating in high risk environments” (15 March 2016), page 3
OCHA Evaluation of Duty of Care | 65
The evaluation will identify gaps as well as lessons learned and best practices in OCHA and other UN entities, and identify ways in which coordination, collaboration and cooperation with relevant UN de-partments and agencies, should be strengthened.
As per the terms of reference, the evaluation covers three broad areas, focusing on (1) the provision of duty of care; (2) the application of policies, effectiveness and efficiency of management practices; and (3) a respectful and empowering working atmosphere.
Under these three broad areas and linked to the evaluation criteria of relevance, effectiveness, efficien-cy, connectedness [added to the four criteria of the ToRs] and impact, specific evaluation questions will include the following (these may be adjusted, with OCHA’s consent, during the inception phase):
Relevance• Does OCHA have a systematic approach to duty of care? If so, is it relevant to the achievement of
adequate duty of care of its personnel?• To what extent does OCHA systematically apply relevant UN policies, rules and regulations?• How does OCHA apply the UN’s programme criticality framework and business continuity plans,
and how does this affect duty of care?• Beyond UN policies, rules and regulations, does OCHA have specific duty of care requirements?• To what extent is duty of care adequately taken into account in the development of OCHA’s budgets?• To what extent is OCHA’s approach to post-incident/crisis support to its personnel adequate?
Effectiveness and Efficiency• Is OCHA’s provision of duty of care effective and efficient?• Is OCHA’s current approach to security management of its personnel adequate? • Is OCHA’s approach to the implementation of security measures in high risk environments adequate? • How does OCHA’s security management and duty of care approaches compare to those of similar UN
entities? Are there any lessons that OCHA can incorporate from those experiences?• Does OCHA effectively and efficiently obtain necessary security resources (e.g. armoured vehicles,
personal protection equipment)?• Pre-deployment - do OCHA personnel travelling or going to the field, including those on surge mis-
sions, receive the necessary support and preparation to be deployed?• Do staff deployed to high-risk environments receive the administrative, logistical, safety and securi-
ty, and other types of support they require? • Do OCHA staff have adequate access to medical and psychosocial care, in particular in high-risk duty
stations?• Post-deployment: do OCHA personnel receive the necessary support when completing a mission? • How does OCHA deal with security incidents? Do personnel affected by incidents and their families
receive the care and support they need?• To what extent does OCHA consider gender-specific duty of care requirements? • Does OCHA communicate with and inform staff effectively on all aspects of duty of care, in particular
the risks they take and the support services and entitlements available to them?• To what extent can OCHA improve the provision of duty of care to its personnel, and how?
Connectedness• Does OCHA ensure that the specific duty of care needs of humanitarian workers and its staff are re-
flected in UN policies, rules and regulations, e.g., via the high-level panel on duty of care?• How does OCHA coordinate its security management with the relevant security actors – UNDSS,
UNDP, DPKO missions and the UN Security Management System overall? • WhatroledoesOCHA’scivil-militarycoordinationplayinthedutyofcareofOCHApersonnel?
OCHA Evaluation of Duty of Care | 66
Impact• Do OCHA staff feel they are provided with the necessary safety and security support, in particular in
high-risk duty stations?• Are OCHA staff aware of security policies, including their own responsibilities?• Do OCHA staff feel they are provided with the necessary administrative support (financial, logistical
and human resource support, provision of entitlements)?• WhatisthestateofOCHAstaff’swellbeing?DoesOCHAdoenoughtoensureitsstaff’swellbeing?
Whatcanbeimproved?• Do OCHA staff feel they work in a respectful and empowering work environment, free of harassment
and discrimination?• Does OCHA effectively manage risks to its staff’s safety, security and wellbeing? Does OCHA work to
prevent such risks?• Do different groups of OCHA personnel—e.g. men and women, national and international staff, staff
on fixed-term and temporary appointments, staff in capital cities and sub-offices—feel they are be-ing treated fairly and equitably?
Country MissionsThe evaluation team will visit three countries affected by humanitarian crises and with OCHA opera-tions, one during the inception phase and two during the fieldwork. (In addition, there will be visits to Geneva and New York.) The countries, listed below, present a mix of the different environments in which OCHA works. It includes large and medium humanitarian crises, protracted crises and those that have recently escalated, large and small OCHA offices, a country with an integrated mission, etc.
OCHA Evaluation of Duty of Care | 67
7.2 Annex 2: Bibliography
ALNAP.(10October2016).EvaluationofHumanitarianActionGuide.Retrieved30January2018,from,https://www.alnap.org/help-library/evaluation-of-humanitarian-action-guide
Chen, Huey-Tseh. (1991). Theory Driven Evaluations. London: Sage.
Cusimano,Salvator;DosSantosCruz,CarlosAlberto&Phillip,RWilliam.(2017).ImprovingSecurityofUnitedNationsPeacekeepers:Weneedtochangethewaywearedoingbusiness.Retrieved29January2018, from https://peacekeeping.un.org/sites/default/files/improving_security_of_united_nations_peacekeepers_report.pdf
Darby,Roger&Williamson,Christine.(2012).Themanagementofemployeeriskinthehumanitarianaid and security sectors. Human Resources Development and Management, 12(3), 1-36. Retrieved 24 January2018,fromhttp://dutyofcareinternational.co.uk/
Devex.(9March2018).UNLaunchesStaffhelplinetoaddresssexualmisconductinformationgaps.Re-trieved9April2018,from,https://www.devex.com/news/un-launches-staff-helpline-to-address-sex-ual-misconduct-information-gaps-92275.
Hearns,Annette.(2017).HumanitarianAidWorkersPerceptionsofStressManagementServices.Re-trieved2April2018,from,https://scholarworks.waldenu.edu/cgi/viewcontent.cgi?article=4351&con-text=dissertations
HIPPO. (2016). Information on Standing Administrative Measures Terms of reference for review of key processes. RetrievedApril 11 2018, from, http://dag.un.org/bitstream/handle/11176/387433/HIPPO%20implementation%20May%2016.docx?sequence=4&isAllowed=y.
Hoppe,Kelsey&Williamson,Christine.(18April2016).DennisvsNorwegianRefugeeCouncil:impli-cationsfordutyofcare.RetrievedJanuary242018,fromhttps://odihpn.org/blog/dennis-vs-norwe-gian-refugee-council-implications-for-duty-of-care/
Hoppe, Kelsey. (1 June 2016). Guide: 10 ways to manage your duty of care with security manage-ment. Retrieved 24 January 2018, from http://dutyofcareinternational.co.uk/wp-content/up-loads/2018/01/10-ways-Duty-of-Care-Security-Management-1.pdf
HumanitarianWomens Network. (May 2016). Full Survey Results. Retrieved 30March 2018, from,http://humanitarianwomensnetwork.org/
Humanitarian Womens Network. (May 2016). Mission Statement. Retrieved 30 March 2018, from,http://humanitarianwomensnetwork.org/
Independent Evaluation Group. (2012). Designing a Results Framework for achieving Results: A How to Guide.Retrieved11April2018fromhttps://siteresources.worldbank.org/EXTEVACAPDEV/Resourc-es/designing_results_framework.pdf.
Insecurity Insight. Aid providers and their staff 1996-2010. Report 13-1. Switzerland. Retrieved 11 April2018from,www.insecurityinsight.org
Inter-Agency Standing Committee. (11 December 2015). Protection from Sexual Exploitation and Abuse:
OCHA Evaluation of Duty of Care | 68
StatementbytheInter-AgencyStandingCommittee.Retrieved7February2018,fromhttps://intera-gencystandingcommittee.org/system/files/principals_statement_psea_20151112_0.pdf
InternationalCivilServiceCommission.(February2018).AguidetothemobilityandHardshipschemeandrelatedarrangements.RetrievedApril112018, from.https://icsc.un.org/resources/hrpd/mah/MOBILITYENG.pdf
Joint Inspection Unit. (2011). Business continuity in the UN System. (REP/2011/6). Geneva. Retrieved 10Aprilfrom,http://www.searo.who.int/entity/emergencies/bc_unsystems.pdf.
Joint Inspection Unit. (2011). Review of the Medical Service in the United Nations System. (Rep 2011/1). Geneva.Retrieved1February2018,fromhttps://www.unjiu.org/en/reports-notes/JIU%20Products/JIU_REP_2011_1_English.pdf
Joint Inspection Unit. (2016). Safety and Security in the United Nations System. (Rep 2016/9). Gene-va.Retrieved24 January2018, fromhttps://www.unjiu.org/en/reports-notes/JIU%20Products/JIU_REP_2016_9_English.pdf
Mannet & The Boston Consulting Group. (29 July 2016). OCHA Functional Review. OCHA-internal doc-ument.
Mayne, J. (2001) “Addressing Attribution through Contribution Analysis: Using Performance Measures Sensibly”CanadianJournalofProgrammeEvaluationVol6,No.1.CanadianEvaluationSociety.
McDonald, Brendan. (31 July 2015). Humanitarian agencies need to stop failing their staff on mental health.TheGuardian.Retrieved24January2018,from,https://www.theguardian.com/global-develop-ment-professionals-network/2015/jul/31/aid-workers-casualties-mental-health
New York University Centre on International Cooperation (2014). UN Development System Risk Man-agementinFragileStates.AWhitePaperforthe2014UtsteinGroupSpringMeeting.RetrievedJanuary252018,from:http://cic.nyu.edu/sites/default/files/un_dev_risk_mgmnt_rannii_jacquand_1.pdf
OCHA (15 July 2015). Guidelines: Redeployment After Critical Incident. OCHA-internal document.
OCHA(2018).PeopleStrategy2018-2021.OCHA-internaldocument.
OCHAWelfareOffice&WebsterUniversity (June2015).OCHAWork,HealthandWell-BeingReport.OCHA-internal document.
OCHA, The Norwegian Refugee Council & Jindal School of International Affairs. (2017). Presence and Proximity:ToStayandDeliverFiveYearsOn.RetrievedJanuary29,2018,from,https://www.unocha.org/story/stay-and-deliver-five-years-risk-and-complexity-delivering-aid-highly-insecure-environ-ments
OCHA. (2011). To Stay and Deliver – Good practice for humanitarians in complex security environments. Retrieved29January2018,fromhttps://www.unocha.org/sites/unocha/files/Stay_and_Deliver.pdf
OCHA. (2013) Policy Instruction: Security. OCHA-internal document.
OCHA Evaluation of Duty of Care | 69
OCHA.(2018)StrategicPlan2018-2021.Retrieved17April2018,fromhttps://www.unocha.org/sites/unocha/files/OCHA%202018-21%20Strategic%20Plan.pdf
OCHA. (June 2017). Creating a better OCHA: Outcomes of the Design Phase of OCHA’s Change Process. OCHA-internal document.
OCHA. (May 2016). Standard Operating Procedures: OCHA PSEA Arrangements for Receiving Com-plaints,Reporting,InvestigationandVictimAssistance.OCHA-internaldocument.
OCHA.(notdated).OCHAStaffWelfareOffice–2017AnnualSummary:Ayearofchallengesandunprec-edented changes. OCHA-internal document.
Office of Administration of Justice. (2009). A guide to resolving disputes. New York. Retrieved 11 April 2018from,http://www.un.org/en/oaj/unjs/pdf/guide_to_resolving_disputes_en.pdf.
Office of Internal Oversight Services (March 2017). Audit of the Operations of the Office for the Coor-dinationofHumanitarianAffairsinEthiopia.2017/014.Retrieved30January2018,fromhttps://oios.un.org/page/download/id/704
Office of Internal Oversight Services .(17 November 2017). Audit of arrangements for staff accommoda-tion in field operations of the Office of the United Nations High Commissioner for Refugees. 2017/119. RetrievedApril102018,from,https://oios.un.org/page/download/id/758.
OfficeofInternalOversightServices.(18March2016).AuditofAdministrationofstaffcompensationclaims inNewYork. 2016/016.Retrieved11April 2018 from, https://oios.un.org/page/download/id/468
Office of Internal Oversight Services. (23 August 2016). Audit of Resource Mobilization in the Office fortheCoordinationofHumanitarianAffairs.2016/090.Retrieved11April2018from,https://oios.un.org/page/download/id/547
Office of Internal Oversight Services. (31 October 2016). Audit of management of human resources in theOffice fortheCoordinationofHumanitarianAffairs.2016/127.Retrieved29January2018from,https://oios.un.org/page/download/id/582
Patton, Michael Quinn. (2000). Utilization-focused Evaluation. London: Sage.
Patton, Michael Quinn. (2010). Qualitative Research and Evaluation. San Francisco, California: Sage.
Ratcliffe,Rebecca.(18January2018).SexualharassmentandassaultrifeatUnitedNations,staffclaim.The Guardian. Retrieved 24 January 2018, from, https://www.theguardian.com/global-develop-ment/2018/jan/18/sexual-assault-and-harassment-rife-at-united-nations-staff-claim
RedR UK, Insecurity Insight, EISF. ( September 2017). Security Incident Information Management Hand-book.Retrieved11April2018fromhttps://www.redr.org.uk/getmedia/0b2d6c98-4b60-49d2-a976-d3069ac9625e/SIIM-Handbook-Sept2017.pdf.
Reuters.(31January2018).U.N.agenciesvowtorampupfightagainstsexualharassment.Retrieved8February2018,fromhttps://www.reuters.com/article/us-global-un-harassment/u-n-agencies-vow-to-ramp-up-fight-against-sexual-harassment-idUSKBN1FK1YY
OCHA Evaluation of Duty of Care | 70
Saving Lives Together. (October 2015). A Framework for improving Security Arrangements among In-ternational Non-Governmental Organisations/International Organisations and the United Nations. Re-trieved29 January2018, fromhttps://reliefweb.int/sites/reliefweb.int/files/resources/saving_lives_together_framework_-_october_2015.pdf
Swiss Federal Department of Foreign Affairs (FDFA), Stabilization Unit (SU) , Center for International PeaceOperations(ZIF).(2017).VoluntaryGuidelinesontheDutyofCaretoSecondedCivilianPerson-nel.Retrieved3April2018,from,http://www.zif-berlin.org/fileadmin/uploads/experten-einsaetze/Voluntary_Guidelines_on_the_Duty_of_Care_to_Seconded_Civilian_Personnel_Final_170420.pdf
TheGuardian(7February2018).UN‘grosslymishandled’inquiryintoallegedsexualassault,saycam-paigners.Retrieved8February2018,fromhttps://www.theguardian.com/global-development/2018/feb/07/un-inquiry-alleged-sexual-assault-campaigners
TheGuardian. (19 January2018). Sexualharassment andassault rife atUnitedNations, staff claim.Retrieved 8 February 2018, fromhttps://www.theguardian.com/global-development/2018/jan/18/sexual-assault-and-harassment-rife-at-united-nations-staff-claim
UNHCR. (March 2017). Recruitment Brochure – General Information on Entitlements & Benefits for Inter-nationalStaff.RetrievedApril112018,from,http://www.unhcr.org/en-us/admin/jobs/4b82a19222/recruitment-brochure-general-information-entitlements-benefits-international.html
UnitedNationsChiefExecutivesBoardforCoordination.(15March2016).FinalReport:HLCMWork-ing Group on “Reconciling Duty of Care for UN personnel while operating in high risk environments. CEB/2016/HLCM/11.Retrieved8February2018,fromhttp://ficsa.org/files/HLCM11_WG_on_Recon-ciling_duty_of_care_for_UN_personnel.pdf
UnitedNationsChiefExecutivesBoardforCoordination.(17September2014).Reportof28thsessionof HLCM. “Policy on the Organizational Resilience Management System (ORMS). CEB/2014/HLCM/17. Retrieved 10 April 2018, from, https://www.unsystem.org/CEBPublicFiles/High-Level%20Commit-tee%20on%20Management/Document/CEB-2014-2%20-%20HLCM%2028%20-%20final%20re-port.pdf
UnitedNationsChiefExecutivesBoardforCoordination.(17September2014).Reportof28thsessionof HLCM. “Key Performance Indicators: Organizational Resilience Management System”. CEB/2014/HLCM/17.Add.1.Retrieved10April2018,from,https://www.unsceb.org/CEBPublicFiles/High-Lev-el%20Committee%20on%20Management/Document/ORMS%20-%20Key%20Performance%20Indi-cators.pdf
UnitedNationsChiefExecutivesBoardforCoordination.(17September2014).Reportof28thsessionof HLCM. “Organizational Resilience Management System: Maintenance, Exercise, and Review (ME&R) Regime”. CEB/2014/HLCM/17. Add.2. Retrieved 10April 2018 from, https://www.unsceb.org/CEB-PublicFiles/High-Level%20Committee%20on%20Management/Document/ORMS%20-%20Mainte-nance%2C%20Exercise%20and%20Review%20%28ME%26R%29%20Regime.pdf
United Nations Chief Executives Board for Coordination. (31 March 2015). Occupational Safety and Health(OSH)Framework.CEB/2015/HLCM/7/Rev.2.Retrieved29January2018,from,https://www.unsceb.org/CEBPublicFiles/HLCM-OSH%20Frmwk_FINAL_2015-03-31.pdf
OCHA Evaluation of Duty of Care | 71
United Nations Department for Safety and Security. (2011). United Nations Security Management Sys-tem:SecurityPolicy.Retrieved26January2018,fromhttps://www.un.org/undss/sites/www.un.org.undss/files/docs/security_policy_manual_spm_e-book_as_of_29_nov_2017_0.pdf
United Nations Ethics Office. (April 2014). The Roadmap; A staff members guide to finding the right place.Retrieved11April2018,from,http://www.un.org/en/ethics/pdf/roadmap.pdf
United Nations Evaluation Group. (2016). Norms and Standard for Evaluation. Retrieved 30 January 2018,from,https://www.alnap.org/help-library/evaluation-of-humanitarian-action-guide
United Nations Evaluation Group. (2017). Improved Quality of Evaluation Recommendations Checklist. Retrieved30January2018,fromhttp://www.unevaluation.org/document/download/2680
United Nations Evaluation Group. (2017). Principle of Stakeholder Engagement. Retrieved 30 January 2018,fromwww.uneval.org/document/download/2790
United Nations General Assembly Resolution. (1991). Strengthening of the Coordination of Humani-tarianEmergencyAssistance.A/RES/46/182.Retrieved29 January2018, fromhttp://www.un.org/documents/ga/res/46/a46r182.htm
United Nations High Commissioner for Refugees. (2013). Mental Health and Psychological Support For Staff.PDES12/2013.Retrieved26January2018,fromhttp://www.unhcr.org/51f67bdc9.pdf
United Nations High Commissioner for Refugees. (2017). Duty of Care Poster. Retrieved 29 January 2018, from, https://www.unsceb.org/CEBPublicFiles/UNHCR-Integracy%20DoC%20workshop%20May%202017%20Posters-compressed.pdf
United Nations Secretariat ( 26 October 2011). Administrative Instruction; Administration of Tempo-raryAppointments.ST/AI2010/4/Rev.1.Retrieved1April2018,from,https://hr.un.org/sites/hr.un.org/files/handbook//AI%20%202010-%204Rev1%20%20%5BAdministration%20of%20tempo-rary%20appointments%5D.doc.
UnitedNationsSecretariat.(11February2008).Secretary-Generalsbulletin:Prohibitionofdiscrimina-tion,harassment,includingsexualharassment,andabuseofauthority.Retrieved8February2018,fromhttps://undocs.org/ST/SGB/2008/5
United Nations Secretariat. (20 January 2017). Secretary-General’s bulletin: Protection against retali-ation for reporting misconduct and for cooperating with duly authorized audits or investigations. Re-trieved8February2018,fromhttps://undocs.org/ST/SGB/2017/2
United Nations Secretariat. (30 December 2016). Secretary-General’s bulletin: Staff Regulations and Rules.ST/SGB/2017/1.Retrieved8February2018,fromhttp://digitallibrary.un.org/record/855429/files/ST_SGB_2017_1-EN.pdf
United Nations Secretariat. (5 June 2017). United Nations Mandatory Learning Programmes.ST/IC/2017/17. Retrieved 7 February 2018, from https://hr.un.org/sites/hr.un.org/files/handbook//IC%20%202017%20-%2017.docx
OCHA Evaluation of Duty of Care | 72
UnitedNationsSecretariat.(8March2007).AdministrativeInstruction;MobilityandHardshipScheme.ST/AI/2007/1. Retrieved 1 February 2018, from https://hr.un.org/sites/hr.un.org/files/handbook/AI%202016%20-%206%20%5BMobility%20and%20Hardship%20Scheme%5D.doc
United Nations Secretariat. (9 October 2003). Secretary-General’s Bulletin; Special Measures for Pro-tectionfromSexualExploitationandSexualAbuse.ST/SGB/2003/13.Retrieved7February2018,fromhttps://oios.un.org/resources/2015/01/ST-SGB-2003-13.pdf
UnitedNationsSecretariat.(February2018).TakingActiononSexualHarassment.
United Nations Secretariat. (1 April 2015). Administrative instruction; Medical Insurance Plan for the locally recruited staff at designated duty stations away from Headquarters. ST/AI/ 2015/3. Retrieved 11 April 2018 from, http://www.un.org/insurance/sites/www.un.org.insurance/files/Circulars/ST.AI.2015.3%20-%20Medical%20Insurance%20Plan%20for%20UN%20locally%20recruited%20staff%20at%20ds%20away%20from%20HQs.pdf
United Nations Secretariat.(21 September 2000). Administrative instruction; Medical Evacuation. ST/AI/2000/10. Retrieved 11 April 2018, from, http://www.un.org/hr_handbook/English/sourcedocu-ments_/09administrativ_/2000_/ai200010medical-1/ai200010medical.doc
United Nations Secretariat.(26 January 2018). Administrative instruction; Medical Clearances. ST/AI/2018/4. Retrieved 11 April 2018, from, https://hr.un.org/sites/hr.un.org/files/handbook/ST.AI_.2018.4-%20Medical%20clearances.docx
UnitedNationsSecretary-General. (2February2018).Secretary-General’spressstakeout,NewYork,2 February 2017. Retrieved 8 February 2018, from https://www.un.org/sg/en/content/sg/speech-es/2018-02-02/opening-remarks-press-stakeout
United Nations Security Management System. (11 December 2015). Security Risk Management (SRM) Manual.
United Nations, Report of the Secretary General. (27 September 2017). Shifting the Management para-digmintheUnitedNations:ensuringabetterfutureforall.A/72492.Retrieved29January2018,from,https://undocs.org/A/72/492
United Nations, Report of the Secretary-General. (15 July 2015). Activities of the Office of the of the Unit-edNationsOmbudsmanandMediationServices.A/70/151.Retrieved29January2018,from,http://www.un.org/en/ga/search/view_doc.asp?symbol=A/70/151
United Nations, Report of the Secretary-General. (15 July 2016). Activities of the Office of the of the Unit-edNationsOmbudsmanandMediationServices.A/71/157.Retrieved29January2018,from,http://www.un.org/en/ga/search/view_doc.asp?symbol=A/71/157
United Nations, Report of the Secretary-General. (26 September 2017). Shifting the Management par-adigm in the United Nations: ensuring a better future for all. A/72/492.Add.1. Retrieved 29 January 2018,fromhttp://www.un.org/en/ga/search/view_doc.asp?symbol=A/72/492/Add.1
United Nations, Report of the Secretary-General. (26 September 2017). Shifting the management para-digm in the United Nations: improving and streamlining the programme planning and budgeting process. Retrieved8February2018,fromhttp://www.un.org/en/ga/search/view_doc.asp?symbol=A/72/492
OCHA Evaluation of Duty of Care | 73
UnitedNations,ReportoftheSecretary-General.(28February2017).SpecialMeasuresforProtectionfrom Sexual Exploitation and Abuse: A NewApproach. A/71/818. Retrieved 7 January 2018, from,https://conduct.unmissions.org/sites/default/files/a_71_818_1.pdf
UnitedNations.(October2017).SystemWideStrategyonGenderParity.Retrieved1February2018,from,https://www.un.int/sites/www.un.int/files/Permanent%20Missions/delegate/17-00102b_gen-der_strategy_report_13_sept_2017.pdf
Wille,ChristinaandLarissaFast.(2013).‘OperatinginInsecurity:Shiftingpatternsofviolenceagainsthumanitarian
Williamson, Christine. (14 August 2017). Understanding Informed Consent in Employment: An Es-sential Element ofDuty of Care. Retrieved 24 January 2018, from, https://www.saferedge.com/sin-gle-post/2017/08/14/Understanding-Informed-Consent-An-Essential-Element-of-Duty-of-Care
Williamson,Christine.(25July2017).Opinion:Dutyofcarestartswithrecruitment.Retrieved24Jan-uary2018,from,https://www.devex.com/news/opinion-duty-of-care-starts-with-recruitment-90701 Williamson,Christine.(June2010).Personnelmanagementandsecurity.HumanitarianExchangeMag-azine(47),14-17.Retrieved24January2018,fromhttps://odihpn.org/magazine/personnel-manage-ment-and-security/
Williamson,Christine;Colvin,Gary&McDonald,Amy.(2008).HumanResourceManagement.ROOTS12: Resourcing Organisations with Opportunities For Transformation and Sharing. Retrieved 24 Janu-ary2018, fromhttp://dutyofcareinternational.co.uk/wp-content/uploads/2017/04/ROOTS12-E-full-document.pdf
Witting,Christian.(2005).DutyofCare:AnAnalyticalApproach.OxfordJournalofLegalStudies,25(1),33-63.Retrieved24January2018,from,https://academic.oup.com/ojls/article/25/1/33/1598139
WorldHealthOrganization(2011).PsychologicalFirstAid:GuideforFieldWorkers.Retrieved11April2018,from,http://www.who.int/mental_health/publications/guide_field_workers/en/
OCHA Evaluation of Duty of Care | 74
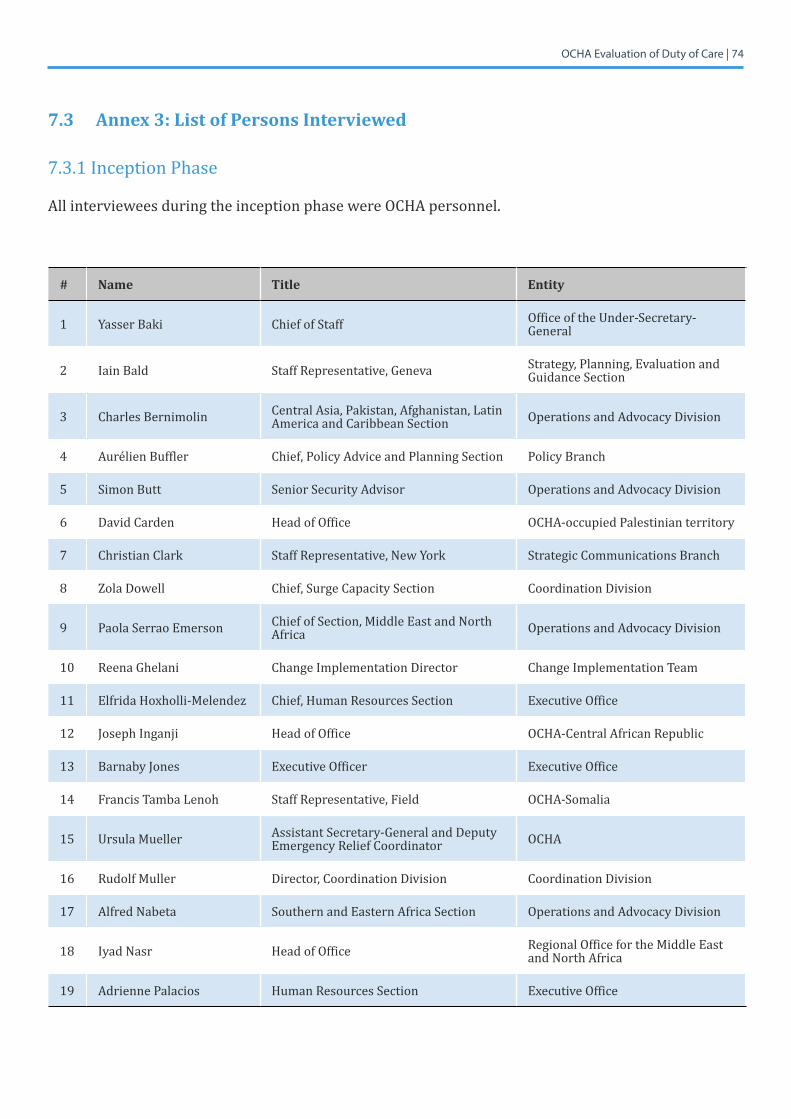
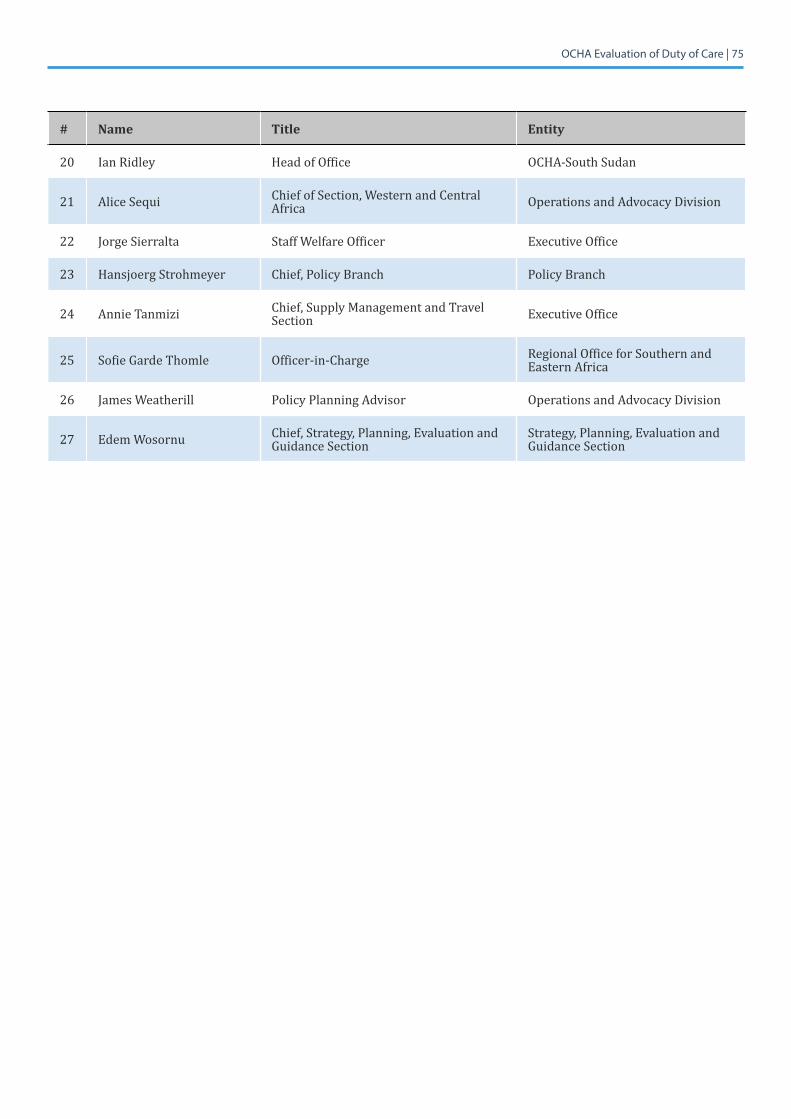
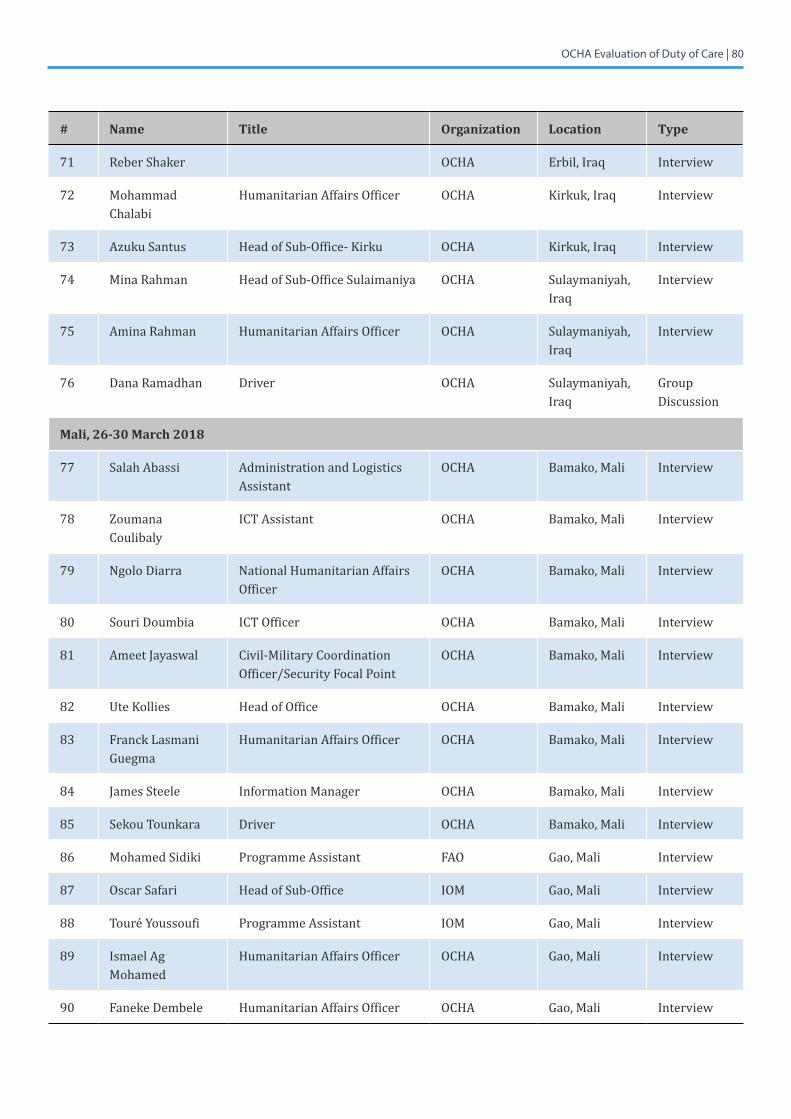
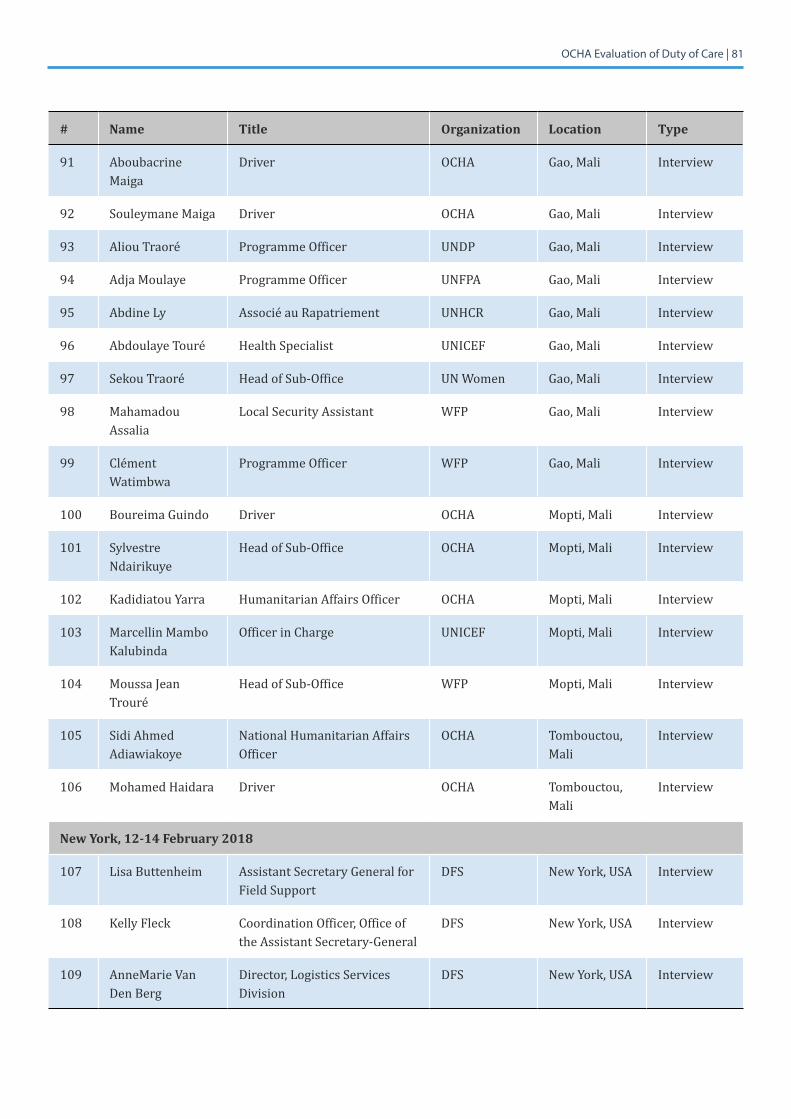
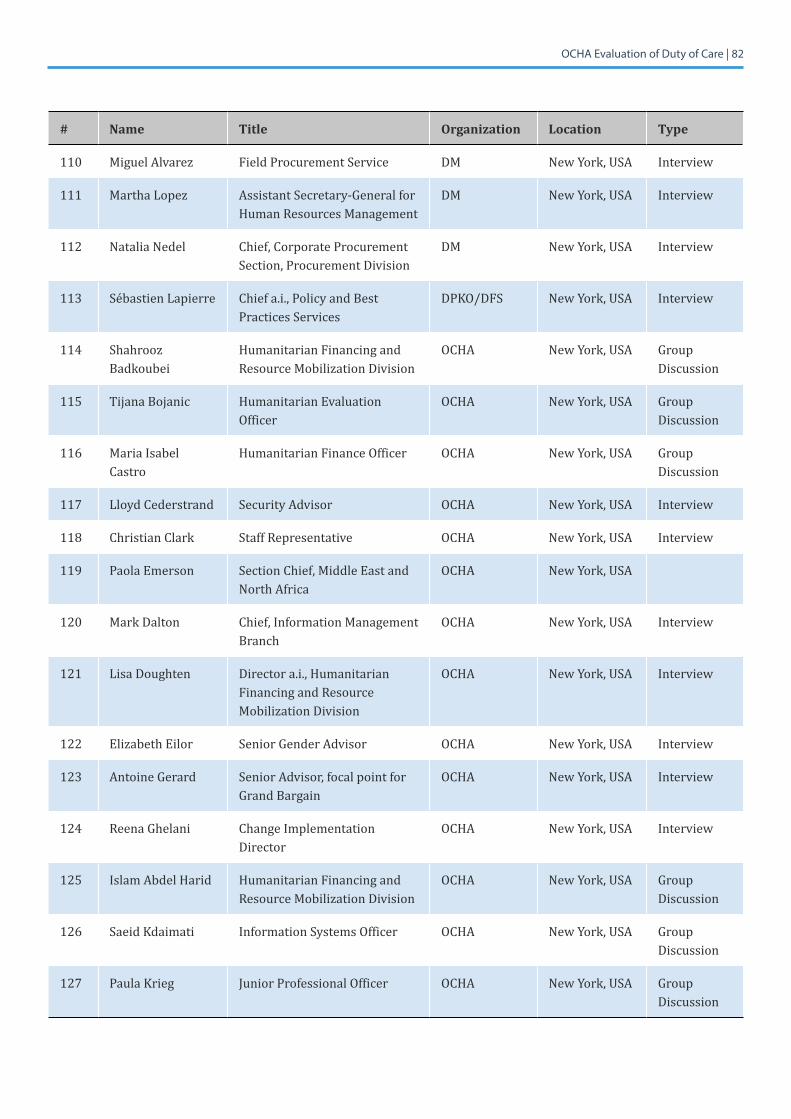
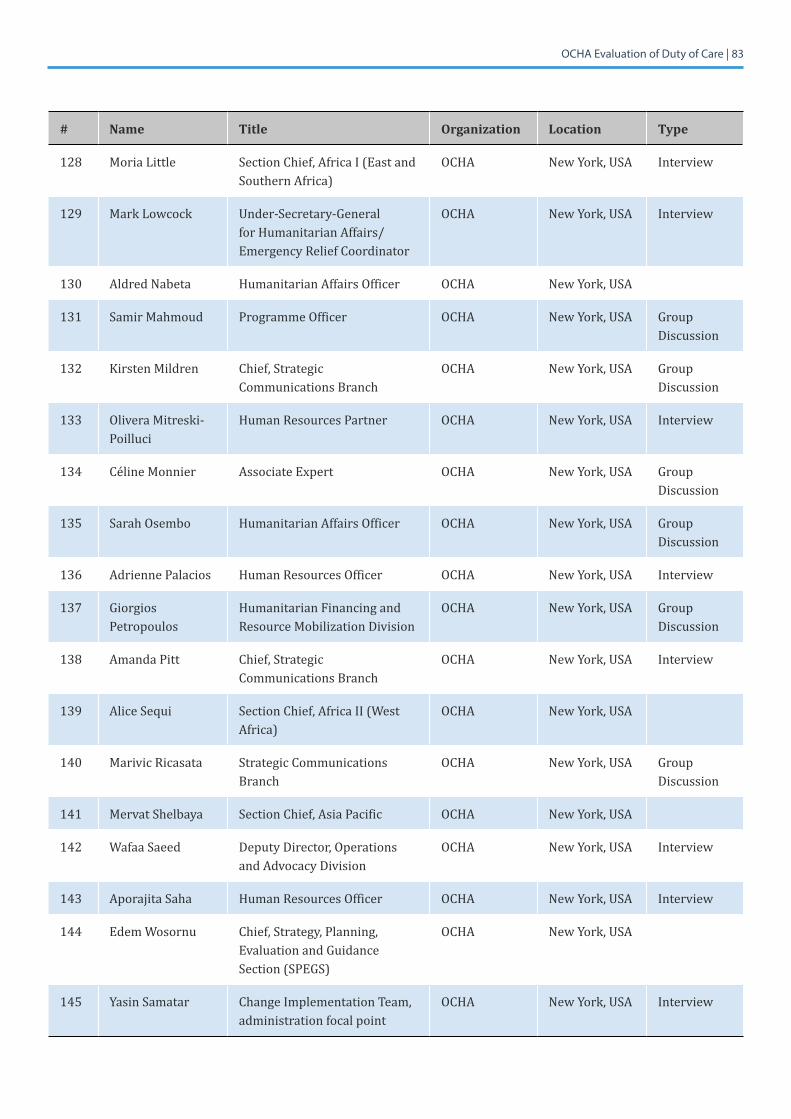
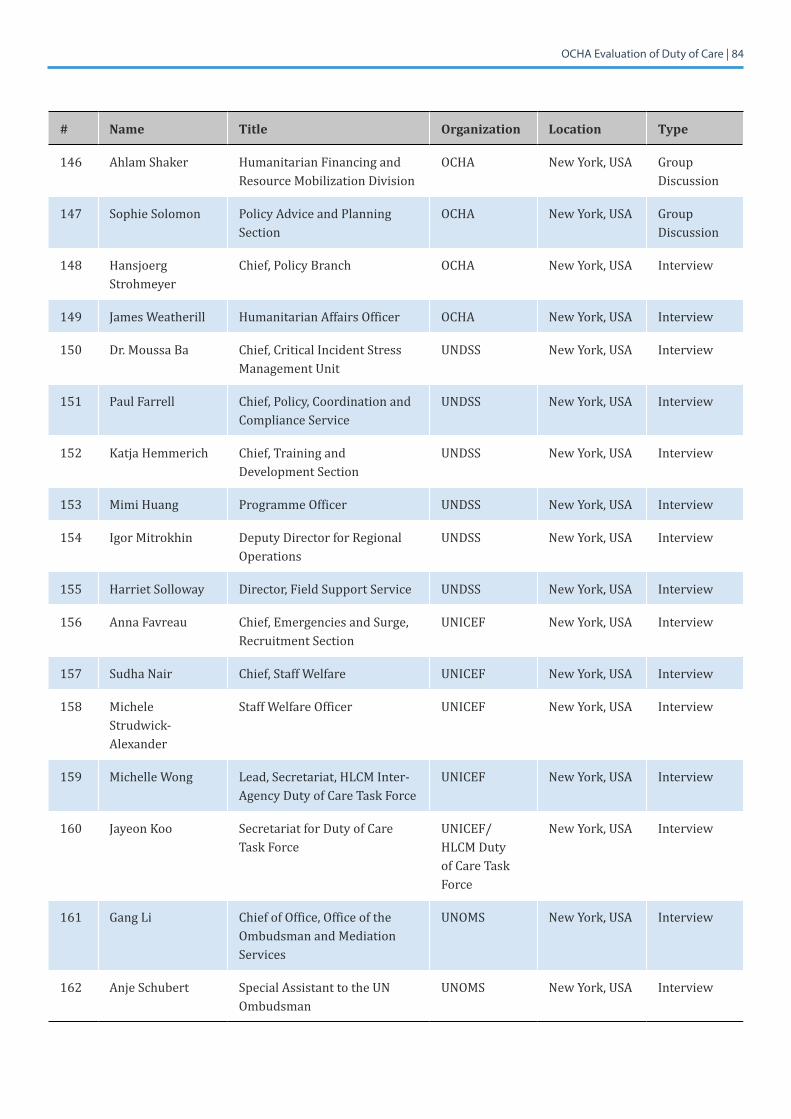
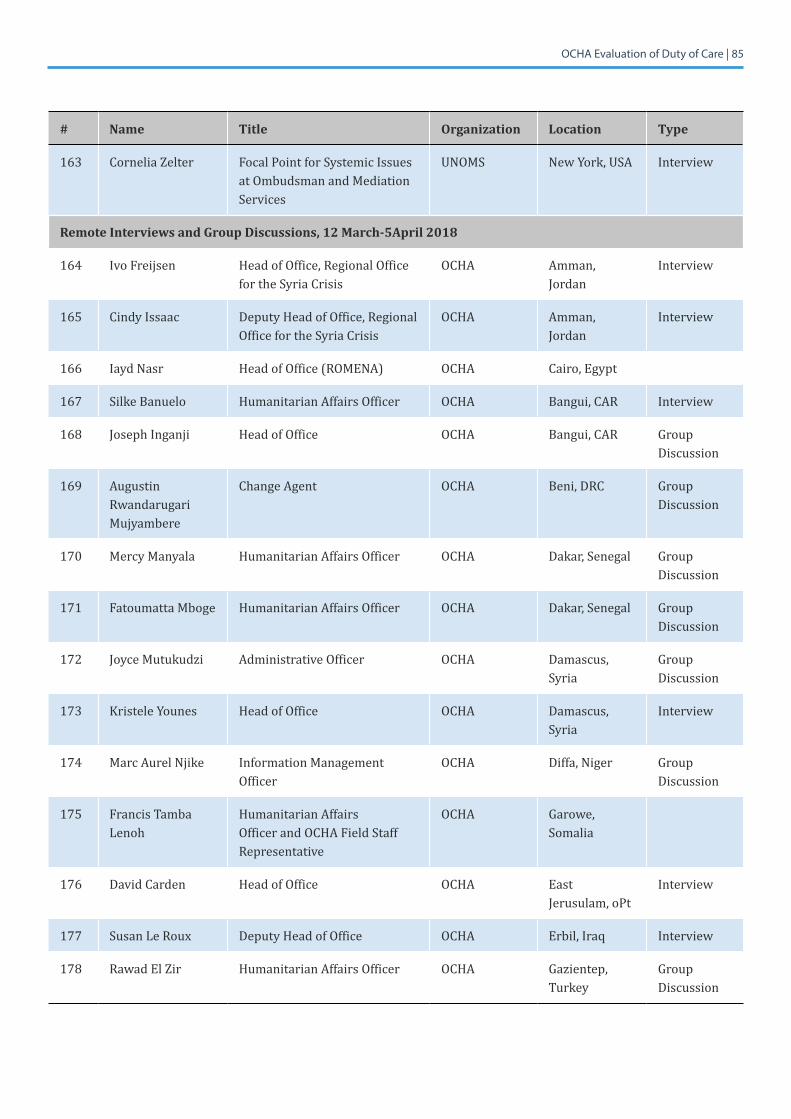
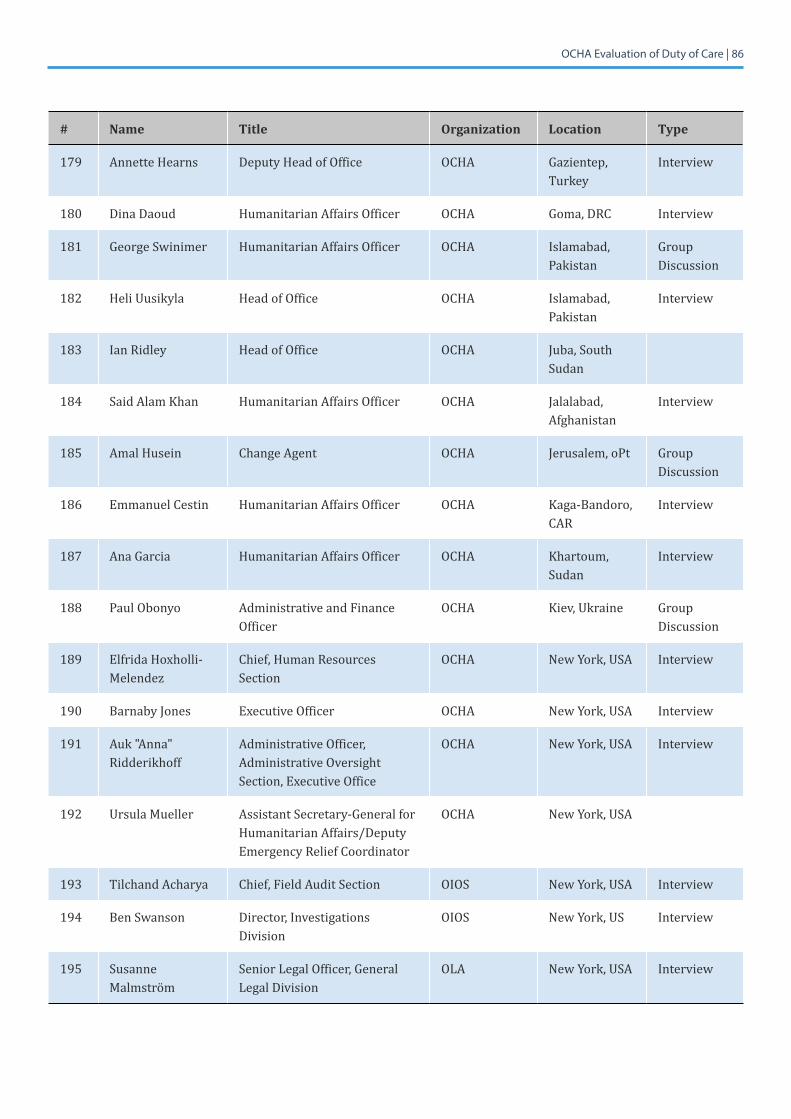
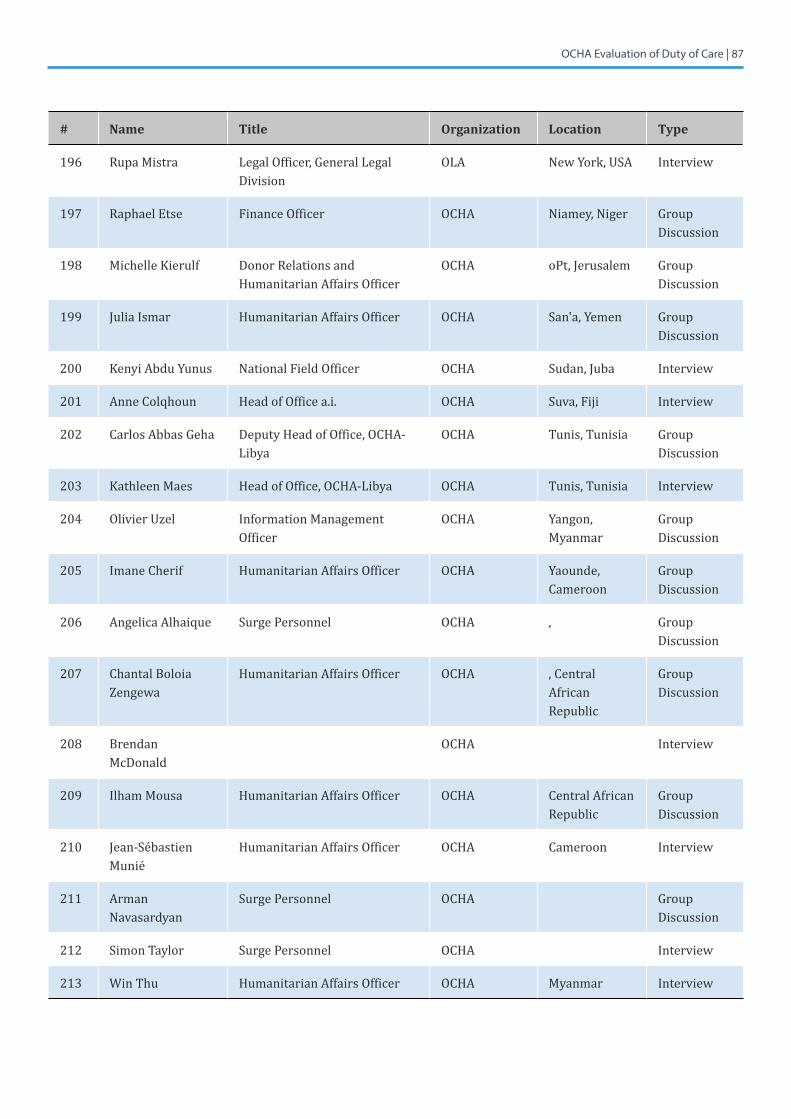
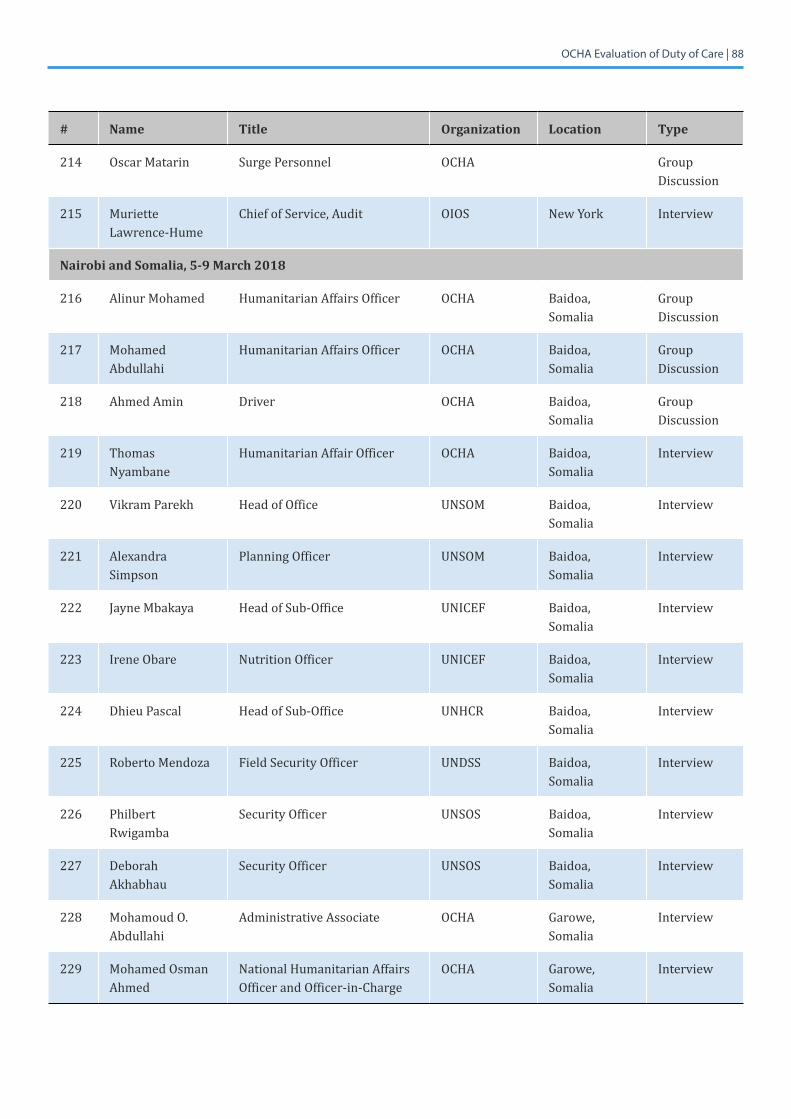
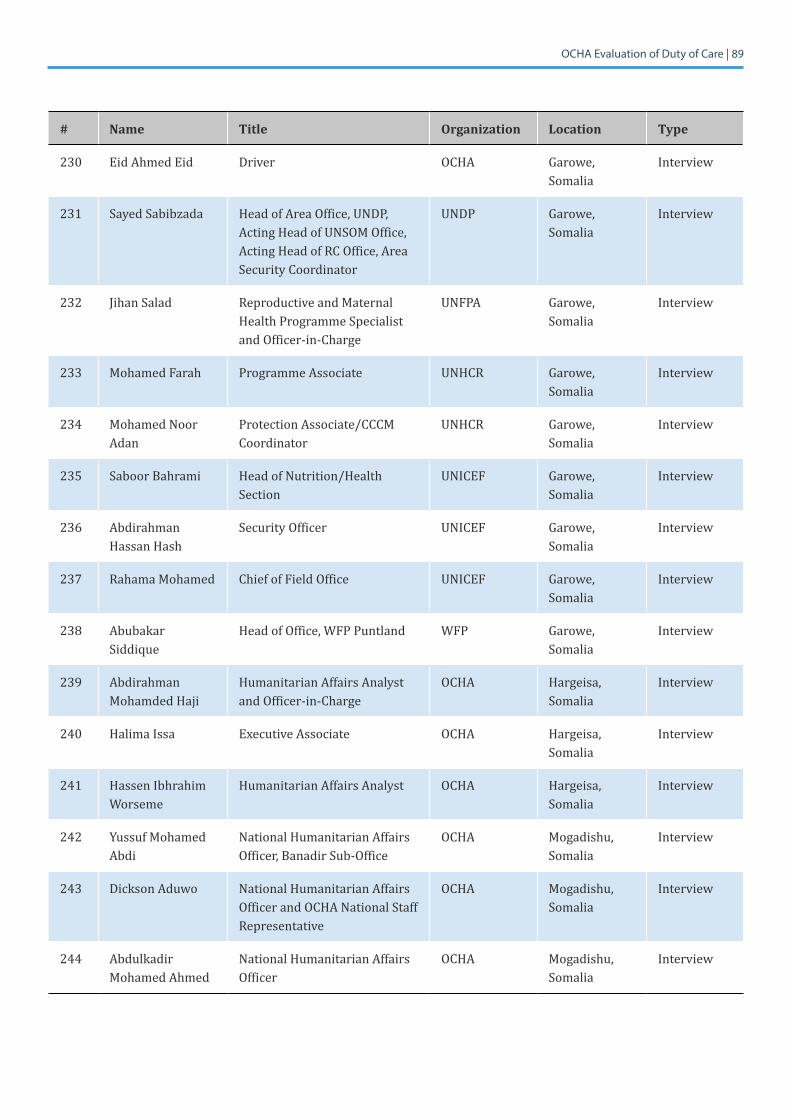
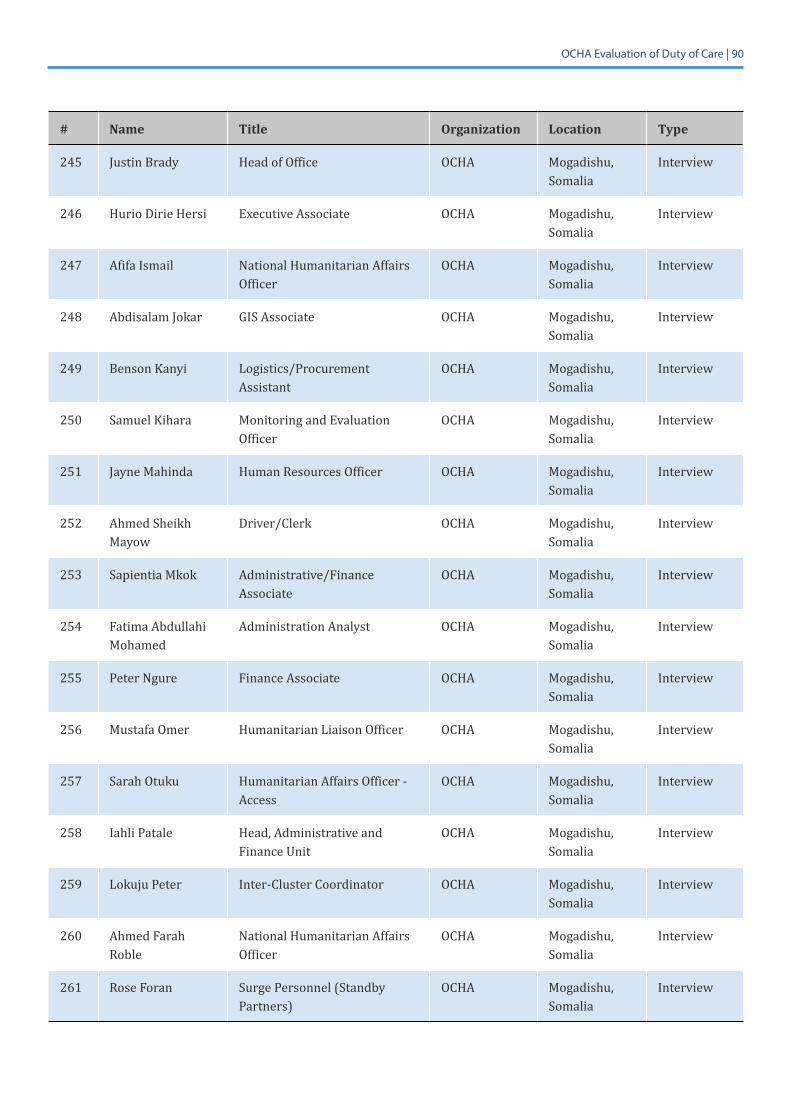
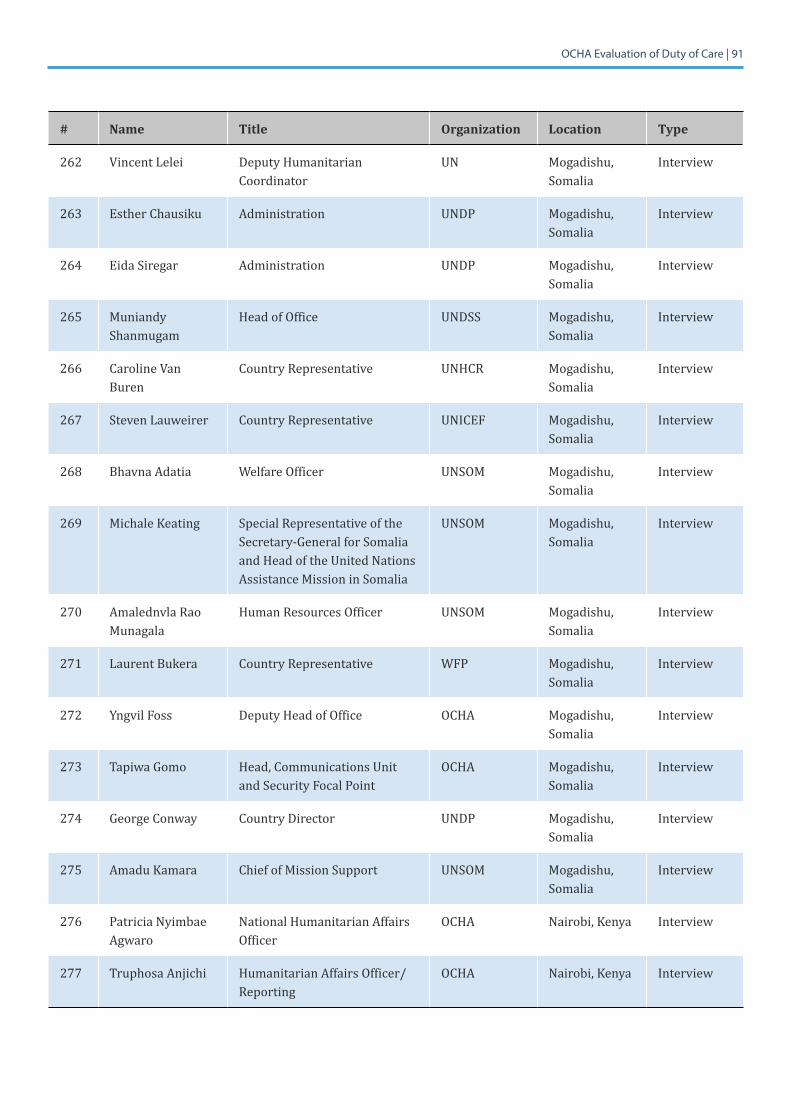
7.3 Annex 3: List of Persons Interviewed
7.3.1 Inception Phase
All interviewees during the inception phase were OCHA personnel.
# Name Title Entity
1 Yasser Baki Chief of Staff Office of the Under-Secretary-General
2 Iain Bald Staff Representative, Geneva Strategy, Planning, Evaluation and Guidance Section
3 Charles Bernimolin Central Asia, Pakistan, Afghanistan, Latin America and Caribbean Section Operations and Advocacy Division
4 Aurélien Buffler Chief, Policy Advice and Planning Section Policy Branch
5 Simon Butt Senior Security Advisor Operations and Advocacy Division
6 David Carden Head of Office OCHA-occupied Palestinian territory
7 Christian Clark Staff Representative, New York Strategic Communications Branch
8 Zola Dowell Chief, Surge Capacity Section Coordination Division
9 Paola Serrao Emerson Chief of Section, Middle East and North Africa Operations and Advocacy Division
10 Reena Ghelani Change Implementation Director Change Implementation Team
11 Elfrida Hoxholli-Melendez Chief, Human Resources Section Executive Office
12 Joseph Inganji Head of Office OCHA-Central African Republic
13 Barnaby Jones Executive Officer Executive Office
14 Francis Tamba Lenoh Staff Representative, Field OCHA-Somalia
15 Ursula Mueller Assistant Secretary-General and Deputy Emergency Relief Coordinator OCHA
16 Rudolf Muller Director, Coordination Division Coordination Division
17 Alfred Nabeta Southern and Eastern Africa Section Operations and Advocacy Division
18 Iyad Nasr Head of Office Regional Office for the Middle East and North Africa
19 Adrienne Palacios Human Resources Section Executive Office
OCHA Evaluation of Duty of Care | 75
# Name Title Entity
20 Ian Ridley Head of Office OCHA-South Sudan
21 Alice Sequi ChiefofSection,WesternandCentralAfrica Operations and Advocacy Division
22 Jorge Sierralta StaffWelfareOfficer Executive Office
23 Hansjoerg Strohmeyer Chief, Policy Branch Policy Branch
24 Annie Tanmizi Chief, Supply Management and Travel Section Executive Office
25 Sofie Garde Thomle Officer-in-Charge Regional Office for Southern and Eastern Africa
26 JamesWeatherill Policy Planning Advisor Operations and Advocacy Division
27 EdemWosornu Chief, Strategy, Planning, Evaluation and Guidance Section
Strategy, Planning, Evaluation and Guidance Section

OCHA Evaluation of Duty of Care | 76
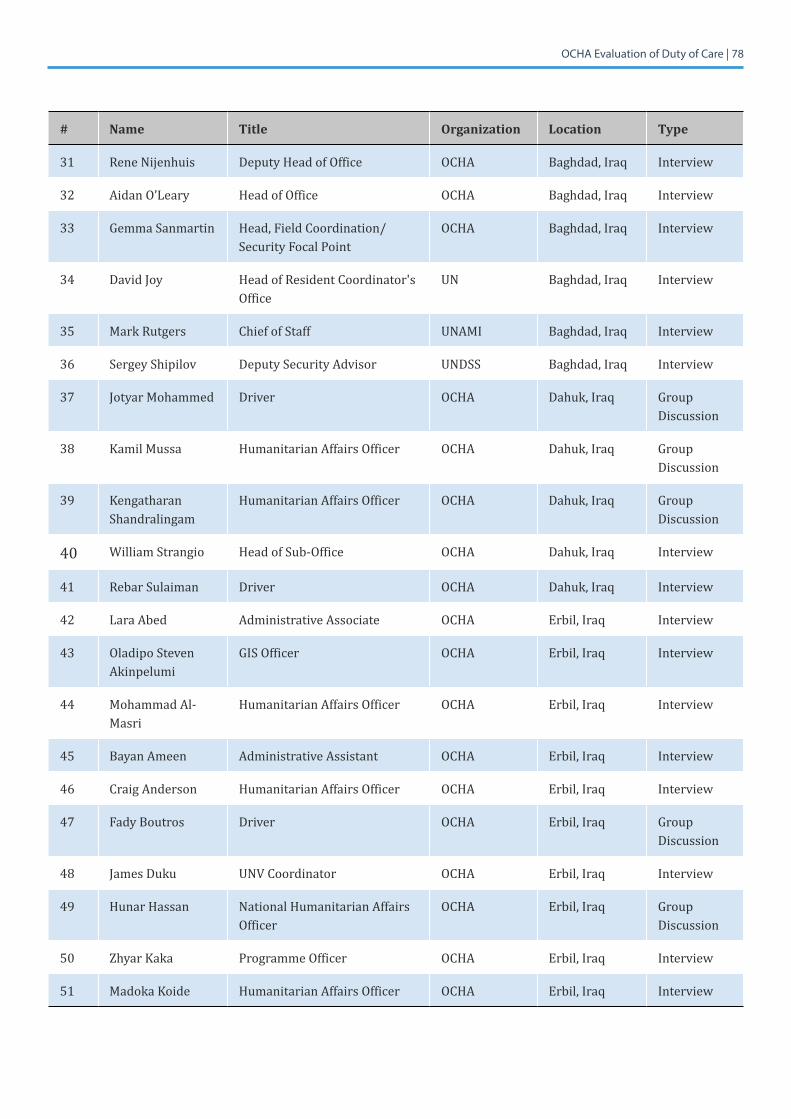
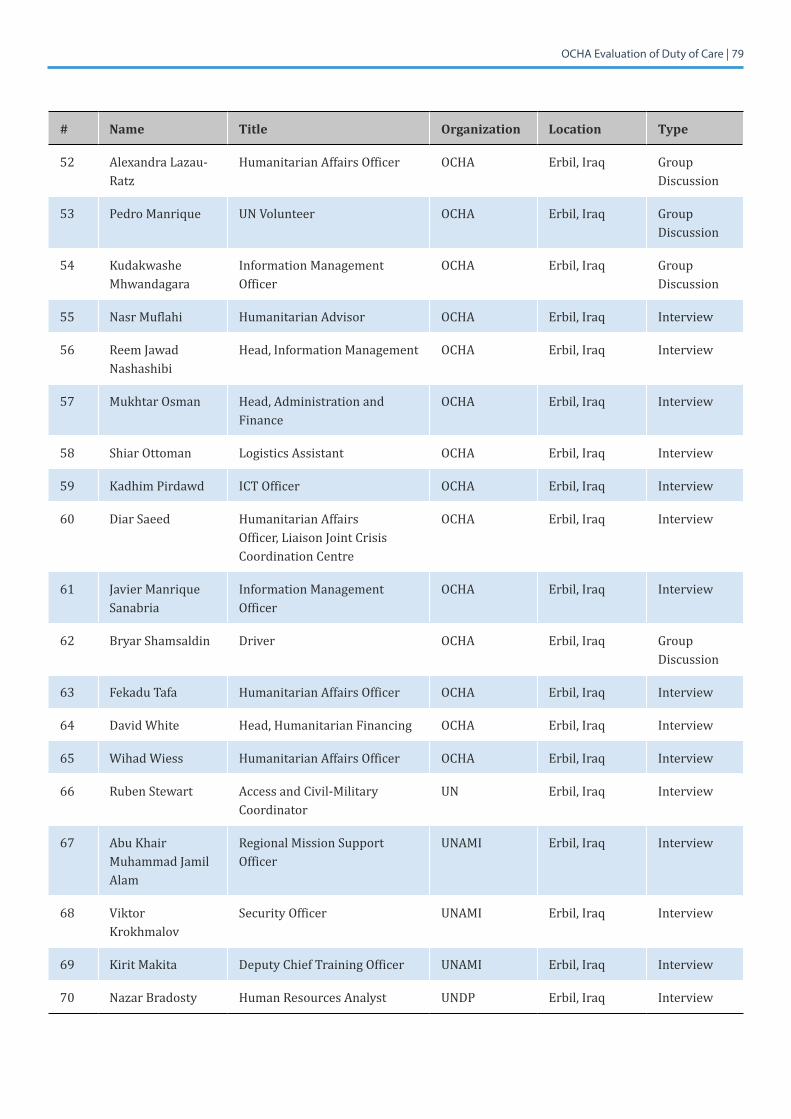
7.3.2 Data Collection Phase
In addition to the people listed below, a number of interviewees asked to remain anonymous.
# Name Title Organization Location Type
Geneva, 26-28 March 2018
1 Dr. Pascal Achard Medical Director UN Medical Service
Geneva, Switzerland
Interview
2 Dr. Rao Sekander Director, UN Medical Service UN Medical Service
Geneva, Switzerland
Interview
3 Dr. Jennifer Underhill
UN Medical Service - Surge UN Medical Service
Geneva, Switzerland
Interview
4 Tensai Asfaw Head of Desk, Donor Relations Section
OCHA Geneva, Switzerland
Group Discussion
5 Iain Bald Staff Representative OCHA Geneva, Switzerland
Interview
6 Monique Bouvoir Programme Assistant OCHA Geneva, Switzerland
Group Discussion
7 Alan Butterfield OIC, Surge Capacity Section OCHA Geneva, Switzerland
Interview
8 WendyCue Chief, a.i., IASC secretariat OCHA Geneva, Switzerland
Interview
9 Ana Maria Donamaria
Administration Assistant OCHA Geneva, Switzerland
Group Discussion
10 Zola Dowell Chief, Surge Capacity Section OCHA Geneva, Switzerland
Interview
11 Merete Johansson Chief of Section, Operations and Advocacy Division
OCHA Geneva, Switzerland
Interview
12 Jesper Lund Chief, Emergency Response Support Branch and INSARAG Secretariat
OCHA Geneva, Switzerland
Interview
13 Johanna Medina Staff Assistant OCHA Geneva, Switzerland
Group Discussion
14 Janette Moritz Staff Development Officer (Training)
OCHA Geneva, Switzerland
Interview

OCHA Evaluation of Duty of Care | 77
# Name Title Organization Location Type
15 Rudolf Muller Director, Coordination Division OCHA Geneva, Switzerland
Interview
16 Janet Puhalovic Humanitarian Affairs Officer OCHA Geneva, Switzerland
Group Discussion
17 Jorge Sierralta Staff Counsellor OCHA Geneva, Switzerland
Interview
18 Justyna Susla Humanitarian Affairs Officer OCHA Geneva, Switzerland
Group Discussion
19 Annie Tanmizi Chief, Supply Management and Travel Section
OCHA Geneva, Switzerland
Interview
20 Katherine Tapia Barron
Assistant Deputy, Supply Management and Travel Section
OCHA Geneva, Switzerland
Interview
21 Cecile Thibaud Administration Assistant OCHA Geneva, Switzerland
Group Discussion
22 JeanVerheyden Chief, Donor Relations Section OCHA Geneva, Switzerland
Interview
23 AndrewWylie Chief, Assessment, Planning and Monitoring Branch
OCHA Geneva, Switzerland
Interview
24 Dr. Ling Kituyi Head,StaffHealthandWelfareService, and HLCM Duty of Care Task Force
UNHCR Geneva, Switzerland
Interview
25 Stephen Farrell Chief, Purchase and Procurement Section
UNOG Geneva, Switzerland
Interview
Iraq, 12-16 March 2018
26 Scott Bohlinger Director INSO Baghdad, Iraq Interview
27 Yasir Al Azawi Administrative and Finance Associate/Security Focal Point for National Staff
OCHA Baghdad, Iraq Interview
28 Roberto Colangelo Special Assistant to the Head of Office
OCHA Baghdad, Iraq Interview
29 Bruce Koepke Humanitarian Affairs Officer OCHA Baghdad, Iraq Interview
30 Hani Mohammed Mahdi
Humanitarian Affairs Officer/Government Liaison
OCHA Baghdad, Iraq Interview
OCHA Evaluation of Duty of Care | 78
# Name Title Organization Location Type
31 Rene Nijenhuis Deputy Head of Office OCHA Baghdad, Iraq Interview
32 Aidan O’Leary Head of Office OCHA Baghdad, Iraq Interview
33 Gemma Sanmartin Head, Field Coordination/ Security Focal Point
OCHA Baghdad, Iraq Interview
34 David Joy Head of Resident Coordinator's Office
UN Baghdad, Iraq Interview
35 Mark Rutgers Chief of Staff UNAMI Baghdad, Iraq Interview
36 Sergey Shipilov Deputy Security Advisor UNDSS Baghdad, Iraq Interview
37 Jotyar Mohammed Driver OCHA Dahuk, Iraq Group Discussion
38 Kamil Mussa Humanitarian Affairs Officer OCHA Dahuk, Iraq Group Discussion
39 Kengatharan Shandralingam
Humanitarian Affairs Officer OCHA Dahuk, Iraq Group Discussion
40 WilliamStrangio Head of Sub-Office OCHA Dahuk, Iraq Interview
41 Rebar Sulaiman Driver OCHA Dahuk, Iraq Interview
42 Lara Abed Administrative Associate OCHA Erbil, Iraq Interview
43 Oladipo Steven Akinpelumi
GIS Officer OCHA Erbil, Iraq Interview
44 Mohammad Al-Masri
Humanitarian Affairs Officer OCHA Erbil, Iraq Interview
45 Bayan Ameen Administrative Assistant OCHA Erbil, Iraq Interview
46 Craig Anderson Humanitarian Affairs Officer OCHA Erbil, Iraq Interview
47 Fady Boutros Driver OCHA Erbil, Iraq Group Discussion
48 James Duku UNVCoordinator OCHA Erbil, Iraq Interview
49 Hunar Hassan National Humanitarian Affairs Officer
OCHA Erbil, Iraq Group Discussion
50 Zhyar Kaka Programme Officer OCHA Erbil, Iraq Interview
51 Madoka Koide Humanitarian Affairs Officer OCHA Erbil, Iraq Interview
OCHA Evaluation of Duty of Care | 79
# Name Title Organization Location Type
52 Alexandra Lazau-Ratz
Humanitarian Affairs Officer OCHA Erbil, Iraq Group Discussion
53 Pedro Manrique UNVolunteer OCHA Erbil, Iraq Group Discussion
54 Kudakwashe Mhwandagara
Information Management Officer
OCHA Erbil, Iraq Group Discussion
55 Nasr Muflahi Humanitarian Advisor OCHA Erbil, Iraq Interview
56 Reem Jawad Nashashibi
Head, Information Management OCHA Erbil, Iraq Interview
57 Mukhtar Osman Head, Administration and Finance
OCHA Erbil, Iraq Interview
58 Shiar Ottoman Logistics Assistant OCHA Erbil, Iraq Interview
59 Kadhim Pirdawd ICT Officer OCHA Erbil, Iraq Interview
60 Diar Saeed Humanitarian Affairs Officer, Liaison Joint Crisis Coordination Centre
OCHA Erbil, Iraq Interview
61 Javier Manrique Sanabria
Information Management Officer
OCHA Erbil, Iraq Interview
62 Bryar Shamsaldin Driver OCHA Erbil, Iraq Group Discussion
63 Fekadu Tafa Humanitarian Affairs Officer OCHA Erbil, Iraq Interview
64 DavidWhite Head, Humanitarian Financing OCHA Erbil, Iraq Interview
65 WihadWiess Humanitarian Affairs Officer OCHA Erbil, Iraq Interview
66 Ruben Stewart Access and Civil-Military Coordinator
UN Erbil, Iraq Interview
67 Abu Khair Muhammad Jamil Alam
Regional Mission Support Officer
UNAMI Erbil, Iraq Interview
68 ViktorKrokhmalov
Security Officer UNAMI Erbil, Iraq Interview
69 Kirit Makita Deputy Chief Training Officer UNAMI Erbil, Iraq Interview
70 Nazar Bradosty Human Resources Analyst UNDP Erbil, Iraq Interview
OCHA Evaluation of Duty of Care | 80
# Name Title Organization Location Type
71 Reber Shaker OCHA Erbil, Iraq Interview
72 Mohammad Chalabi
Humanitarian Affairs Officer OCHA Kirkuk, Iraq Interview
73 Azuku Santus Head of Sub-Office- Kirku OCHA Kirkuk, Iraq Interview
74 Mina Rahman Head of Sub-Office Sulaimaniya OCHA Sulaymaniyah, Iraq
Interview
75 Amina Rahman Humanitarian Affairs Officer OCHA Sulaymaniyah, Iraq
Interview
76 Dana Ramadhan Driver OCHA Sulaymaniyah, Iraq
Group Discussion
Mali, 26-30 March 2018
77 Salah Abassi Administration and Logistics Assistant
OCHA Bamako, Mali Interview
78 Zoumana Coulibaly
ICT Assistant OCHA Bamako, Mali Interview
79 Ngolo Diarra National Humanitarian Affairs Officer
OCHA Bamako, Mali Interview
80 Souri Doumbia ICT Officer OCHA Bamako, Mali Interview
81 Ameet Jayaswal Civil-Military Coordination Officer/Security Focal Point
OCHA Bamako, Mali Interview
82 Ute Kollies Head of Office OCHA Bamako, Mali Interview
83 Franck Lasmani Guegma
Humanitarian Affairs Officer OCHA Bamako, Mali Interview
84 James Steele Information Manager OCHA Bamako, Mali Interview
85 Sekou Tounkara Driver OCHA Bamako, Mali Interview
86 Mohamed Sidiki Programme Assistant FAO Gao, Mali Interview
87 Oscar Safari Head of Sub-Office IOM Gao, Mali Interview
88 Touré Youssoufi Programme Assistant IOM Gao, Mali Interview
89 Ismael Ag Mohamed
Humanitarian Affairs Officer OCHA Gao, Mali Interview
90 Faneke Dembele Humanitarian Affairs Officer OCHA Gao, Mali Interview
OCHA Evaluation of Duty of Care | 81
# Name Title Organization Location Type
91 Aboubacrine Maiga
Driver OCHA Gao, Mali Interview
92 Souleymane Maiga Driver OCHA Gao, Mali Interview
93 Aliou Traoré Programme Officer UNDP Gao, Mali Interview
94 Adja Moulaye Programme Officer UNFPA Gao, Mali Interview
95 Abdine Ly Associé au Rapatriement UNHCR Gao, Mali Interview
96 Abdoulaye Touré Health Specialist UNICEF Gao, Mali Interview
97 Sekou Traoré Head of Sub-Office UNWomen Gao, Mali Interview
98 Mahamadou Assalia
Local Security Assistant WFP Gao, Mali Interview
99 Clément Watimbwa
Programme Officer WFP Gao, Mali Interview
100 Boureima Guindo Driver OCHA Mopti, Mali Interview
101 Sylvestre Ndairikuye
Head of Sub-Office OCHA Mopti, Mali Interview
102 Kadidiatou Yarra Humanitarian Affairs Officer OCHA Mopti, Mali Interview
103 Marcellin Mambo Kalubinda
Officer in Charge UNICEF Mopti, Mali Interview
104 Moussa Jean Trouré
Head of Sub-Office WFP Mopti, Mali Interview
105 Sidi Ahmed Adiawiakoye
National Humanitarian Affairs Officer
OCHA Tombouctou, Mali
Interview
106 Mohamed Haidara Driver OCHA Tombouctou, Mali
Interview
New York, 12-14 February 2018
107 Lisa Buttenheim Assistant Secretary General for Field Support
DFS New York, USA Interview
108 Kelly Fleck Coordination Officer, Office of the Assistant Secretary-General
DFS New York, USA Interview
109 AnneMarieVanDen Berg
Director, Logistics Services Division
DFS New York, USA Interview
OCHA Evaluation of Duty of Care | 82
# Name Title Organization Location Type
110 Miguel Alvarez Field Procurement Service DM New York, USA Interview
111 Martha Lopez Assistant Secretary-General for Human Resources Management
DM New York, USA Interview
112 Natalia Nedel Chief, Corporate Procurement Section, Procurement Division
DM New York, USA Interview
113 Sébastien Lapierre Chief a.i., Policy and Best Practices Services
DPKO/DFS New York, USA Interview
114 Shahrooz Badkoubei
Humanitarian Financing and Resource Mobilization Division
OCHA New York, USA Group Discussion
115 Tijana Bojanic Humanitarian Evaluation Officer
OCHA New York, USA Group Discussion
116 Maria Isabel Castro
Humanitarian Finance Officer OCHA New York, USA Group Discussion
117 Lloyd Cederstrand Security Advisor OCHA New York, USA Interview
118 Christian Clark Staff Representative OCHA New York, USA Interview
119 Paola Emerson Section Chief, Middle East and North Africa
OCHA New York, USA
120 Mark Dalton Chief, Information Management Branch
OCHA New York, USA Interview
121 Lisa Doughten Director a.i., Humanitarian Financing and Resource Mobilization Division
OCHA New York, USA Interview
122 Elizabeth Eilor Senior Gender Advisor OCHA New York, USA Interview
123 Antoine Gerard Senior Advisor, focal point for Grand Bargain
OCHA New York, USA Interview
124 Reena Ghelani Change Implementation Director
OCHA New York, USA Interview
125 Islam Abdel Harid Humanitarian Financing and Resource Mobilization Division
OCHA New York, USA Group Discussion
126 Saeid Kdaimati Information Systems Officer OCHA New York, USA Group Discussion
127 Paula Krieg Junior Professional Officer OCHA New York, USA Group Discussion
OCHA Evaluation of Duty of Care | 83
# Name Title Organization Location Type
128 Moria Little Section Chief, Africa I (East and Southern Africa)
OCHA New York, USA Interview
129 Mark Lowcock Under-Secretary-General for Humanitarian Affairs/Emergency Relief Coordinator
OCHA New York, USA Interview
130 Aldred Nabeta Humanitarian Affairs Officer OCHA New York, USA
131 Samir Mahmoud Programme Officer OCHA New York, USA Group Discussion
132 Kirsten Mildren Chief, Strategic Communications Branch
OCHA New York, USA Group Discussion
133 Olivera Mitreski-Poilluci
Human Resources Partner OCHA New York, USA Interview
134 Céline Monnier Associate Expert OCHA New York, USA Group Discussion
135 Sarah Osembo Humanitarian Affairs Officer OCHA New York, USA Group Discussion
136 Adrienne Palacios Human Resources Officer OCHA New York, USA Interview
137 Giorgios Petropoulos
Humanitarian Financing and Resource Mobilization Division
OCHA New York, USA Group Discussion
138 Amanda Pitt Chief, Strategic Communications Branch
OCHA New York, USA Interview
139 Alice Sequi SectionChief,AfricaII(WestAfrica)
OCHA New York, USA
140 Marivic Ricasata Strategic Communications Branch
OCHA New York, USA Group Discussion
141 Mervat Shelbaya Section Chief, Asia Pacific OCHA New York, USA
142 WafaaSaeed Deputy Director, Operations and Advocacy Division
OCHA New York, USA Interview
143 Aporajita Saha Human Resources Officer OCHA New York, USA Interview
144 EdemWosornu Chief, Strategy, Planning, Evaluation and Guidance Section (SPEGS)
OCHA New York, USA
145 Yasin Samatar Change Implementation Team, administration focal point
OCHA New York, USA Interview
OCHA Evaluation of Duty of Care | 84
# Name Title Organization Location Type
146 Ahlam Shaker Humanitarian Financing and Resource Mobilization Division
OCHA New York, USA Group Discussion
147 Sophie Solomon Policy Advice and Planning Section
OCHA New York, USA Group Discussion
148 Hansjoerg Strohmeyer
Chief, Policy Branch OCHA New York, USA Interview
149 JamesWeatherill Humanitarian Affairs Officer OCHA New York, USA Interview
150 Dr. Moussa Ba Chief, Critical Incident Stress Management Unit
UNDSS New York, USA Interview
151 Paul Farrell Chief, Policy, Coordination and Compliance Service
UNDSS New York, USA Interview
152 Katja Hemmerich Chief, Training and Development Section
UNDSS New York, USA Interview
153 Mimi Huang Programme Officer UNDSS New York, USA Interview
154 Igor Mitrokhin Deputy Director for Regional Operations
UNDSS New York, USA Interview
155 Harriet Solloway Director, Field Support Service UNDSS New York, USA Interview
156 Anna Favreau Chief, Emergencies and Surge, Recruitment Section
UNICEF New York, USA Interview
157 Sudha Nair Chief,StaffWelfare UNICEF New York, USA Interview
158 Michele Strudwick-Alexander
StaffWelfareOfficer UNICEF New York, USA Interview
159 MichelleWong Lead, Secretariat, HLCM Inter-Agency Duty of Care Task Force
UNICEF New York, USA Interview
160 Jayeon Koo Secretariat for Duty of Care Task Force
UNICEF/HLCM Duty of Care Task Force
New York, USA Interview
161 Gang Li Chief of Office, Office of the Ombudsman and Mediation Services
UNOMS New York, USA Interview
162 Anje Schubert Special Assistant to the UN Ombudsman
UNOMS New York, USA Interview
OCHA Evaluation of Duty of Care | 85
# Name Title Organization Location Type
163 Cornelia Zelter Focal Point for Systemic Issues at Ombudsman and Mediation Services
UNOMS New York, USA Interview
Remote Interviews and Group Discussions, 12 March-5April 2018
164 Ivo Freijsen Head of Office, Regional Office for the Syria Crisis
OCHA Amman, Jordan
Interview
165 Cindy Issaac Deputy Head of Office, Regional Office for the Syria Crisis
OCHA Amman, Jordan
Interview
166 Iayd Nasr Head of Office (ROMENA) OCHA Cairo, Egypt
167 Silke Banuelo Humanitarian Affairs Officer OCHA Bangui, CAR Interview
168 Joseph Inganji Head of Office OCHA Bangui, CAR Group Discussion
169 Augustin Rwandarugari Mujyambere
Change Agent OCHA Beni, DRC Group Discussion
170 Mercy Manyala Humanitarian Affairs Officer OCHA Dakar, Senegal Group Discussion
171 Fatoumatta Mboge Humanitarian Affairs Officer OCHA Dakar, Senegal Group Discussion
172 Joyce Mutukudzi Administrative Officer OCHA Damascus, Syria
Group Discussion
173 Kristele Younes Head of Office OCHA Damascus, Syria
Interview
174 Marc Aurel Njike Information Management Officer
OCHA Diffa, Niger Group Discussion
175 Francis Tamba Lenoh
Humanitarian Affairs Officer and OCHA Field Staff Representative
OCHA Garowe, Somalia
176 David Carden Head of Office OCHA East Jerusulam, oPt
Interview
177 Susan Le Roux Deputy Head of Office OCHA Erbil, Iraq Interview
178 Rawad El Zir Humanitarian Affairs Officer OCHA Gazientep, Turkey
Group Discussion
OCHA Evaluation of Duty of Care | 86
# Name Title Organization Location Type
179 Annette Hearns Deputy Head of Office OCHA Gazientep, Turkey
Interview
180 Dina Daoud Humanitarian Affairs Officer OCHA Goma, DRC Interview
181 George Swinimer Humanitarian Affairs Officer OCHA Islamabad, Pakistan
Group Discussion
182 Heli Uusikyla Head of Office OCHA Islamabad, Pakistan
Interview
183 Ian Ridley Head of Office OCHA Juba, South Sudan
184 Said Alam Khan Humanitarian Affairs Officer OCHA Jalalabad, Afghanistan
Interview
185 Amal Husein Change Agent OCHA Jerusalem, oPt Group Discussion
186 Emmanuel Cestin Humanitarian Affairs Officer OCHA Kaga-Bandoro, CAR
Interview
187 Ana Garcia Humanitarian Affairs Officer OCHA Khartoum, Sudan
Interview
188 Paul Obonyo Administrative and Finance Officer
OCHA Kiev, Ukraine Group Discussion
189 Elfrida Hoxholli-Melendez
Chief, Human Resources Section
OCHA New York, USA Interview
190 Barnaby Jones Executive Officer OCHA New York, USA Interview
191 Auk "Anna" Ridderikhoff
Administrative Officer, Administrative Oversight Section, Executive Office
OCHA New York, USA Interview
192 Ursula Mueller Assistant Secretary-General for Humanitarian Affairs/Deputy Emergency Relief Coordinator
OCHA New York, USA
193 Tilchand Acharya Chief, Field Audit Section OIOS New York, USA Interview
194 Ben Swanson Director, Investigations Division
OIOS New York, US Interview
195 Susanne Malmström
Senior Legal Officer, General Legal Division
OLA New York, USA Interview
OCHA Evaluation of Duty of Care | 87
# Name Title Organization Location Type
196 Rupa Mistra Legal Officer, General Legal Division
OLA New York, USA Interview
197 Raphael Etse Finance Officer OCHA Niamey, Niger Group Discussion
198 Michelle Kierulf Donor Relations and Humanitarian Affairs Officer
OCHA oPt, Jerusalem Group Discussion
199 Julia Ismar Humanitarian Affairs Officer OCHA San'a, Yemen Group Discussion
200 Kenyi Abdu Yunus National Field Officer OCHA Sudan, Juba Interview
201 Anne Colqhoun Head of Office a.i. OCHA Suva, Fiji Interview
202 Carlos Abbas Geha Deputy Head of Office, OCHA-Libya
OCHA Tunis, Tunisia Group Discussion
203 Kathleen Maes Head of Office, OCHA-Libya OCHA Tunis, Tunisia Interview
204 Olivier Uzel Information Management Officer
OCHA Yangon, Myanmar
Group Discussion
205 Imane Cherif Humanitarian Affairs Officer OCHA Yaounde, Cameroon
Group Discussion
206 Angelica Alhaique Surge Personnel OCHA , Group Discussion
207 Chantal Boloia Zengewa
Humanitarian Affairs Officer OCHA , Central African Republic
Group Discussion
208 Brendan McDonald
OCHA Interview
209 Ilham Mousa Humanitarian Affairs Officer OCHA Central African Republic
Group Discussion
210 Jean-Sébastien Munié
Humanitarian Affairs Officer OCHA Cameroon Interview
211 Arman Navasardyan
Surge Personnel OCHA Group Discussion
212 Simon Taylor Surge Personnel OCHA Interview
213 WinThu Humanitarian Affairs Officer OCHA Myanmar Interview
OCHA Evaluation of Duty of Care | 88
# Name Title Organization Location Type
214 Oscar Matarin Surge Personnel OCHA Group Discussion
215 Muriette Lawrence-Hume
Chief of Service, Audit OIOS New York Interview
Nairobi and Somalia, 5-9 March 2018
216 Alinur Mohamed Humanitarian Affairs Officer OCHA Baidoa, Somalia
Group Discussion
217 Mohamed Abdullahi
Humanitarian Affairs Officer OCHA Baidoa, Somalia
Group Discussion
218 Ahmed Amin Driver OCHA Baidoa, Somalia
Group Discussion
219 Thomas Nyambane
Humanitarian Affair Officer OCHA Baidoa, Somalia
Interview
220 VikramParekh Head of Office UNSOM Baidoa, Somalia
Interview
221 Alexandra Simpson
Planning Officer UNSOM Baidoa, Somalia
Interview
222 Jayne Mbakaya Head of Sub-Office UNICEF Baidoa, Somalia
Interview
223 Irene Obare Nutrition Officer UNICEF Baidoa, Somalia
Interview
224 Dhieu Pascal Head of Sub-Office UNHCR Baidoa, Somalia
Interview
225 Roberto Mendoza Field Security Officer UNDSS Baidoa, Somalia
Interview
226 Philbert Rwigamba
Security Officer UNSOS Baidoa, Somalia
Interview
227 Deborah Akhabhau
Security Officer UNSOS Baidoa, Somalia
Interview
228 Mohamoud O. Abdullahi
Administrative Associate OCHA Garowe, Somalia
Interview
229 Mohamed Osman Ahmed
National Humanitarian Affairs Officer and Officer-in-Charge
OCHA Garowe, Somalia
Interview
OCHA Evaluation of Duty of Care | 89
# Name Title Organization Location Type
230 Eid Ahmed Eid Driver OCHA Garowe, Somalia
Interview
231 Sayed Sabibzada Head of Area Office, UNDP, Acting Head of UNSOM Office, Acting Head of RC Office, Area Security Coordinator
UNDP Garowe, Somalia
Interview
232 Jihan Salad Reproductive and Maternal Health Programme Specialist and Officer-in-Charge
UNFPA Garowe, Somalia
Interview
233 Mohamed Farah Programme Associate UNHCR Garowe, Somalia
Interview
234 Mohamed Noor Adan
Protection Associate/CCCM Coordinator
UNHCR Garowe, Somalia
Interview
235 Saboor Bahrami Head of Nutrition/Health Section
UNICEF Garowe, Somalia
Interview
236 Abdirahman Hassan Hash
Security Officer UNICEF Garowe, Somalia
Interview
237 Rahama Mohamed Chief of Field Office UNICEF Garowe, Somalia
Interview
238 Abubakar Siddique
HeadofOffice,WFPPuntland WFP Garowe, Somalia
Interview
239 Abdirahman Mohamded Haji
Humanitarian Affairs Analyst and Officer-in-Charge
OCHA Hargeisa, Somalia
Interview
240 Halima Issa Executive Associate OCHA Hargeisa, Somalia
Interview
241 Hassen Ibhrahim Worseme
Humanitarian Affairs Analyst OCHA Hargeisa, Somalia
Interview
242 Yussuf Mohamed Abdi
National Humanitarian Affairs Officer, Banadir Sub-Office
OCHA Mogadishu, Somalia
Interview
243 Dickson Aduwo National Humanitarian Affairs Officer and OCHA National Staff Representative
OCHA Mogadishu, Somalia
Interview
244 Abdulkadir Mohamed Ahmed
National Humanitarian Affairs Officer
OCHA Mogadishu, Somalia
Interview
OCHA Evaluation of Duty of Care | 90
# Name Title Organization Location Type
245 Justin Brady Head of Office OCHA Mogadishu, Somalia
Interview
246 Hurio Dirie Hersi Executive Associate OCHA Mogadishu, Somalia
Interview
247 Afifa Ismail National Humanitarian Affairs Officer
OCHA Mogadishu, Somalia
Interview
248 Abdisalam Jokar GIS Associate OCHA Mogadishu, Somalia
Interview
249 Benson Kanyi Logistics/Procurement Assistant
OCHA Mogadishu, Somalia
Interview
250 Samuel Kihara Monitoring and Evaluation Officer
OCHA Mogadishu, Somalia
Interview
251 Jayne Mahinda Human Resources Officer OCHA Mogadishu, Somalia
Interview
252 Ahmed Sheikh Mayow
Driver/Clerk OCHA Mogadishu, Somalia
Interview
253 Sapientia Mkok Administrative/Finance Associate
OCHA Mogadishu, Somalia
Interview
254 Fatima Abdullahi Mohamed
Administration Analyst OCHA Mogadishu, Somalia
Interview
255 Peter Ngure Finance Associate OCHA Mogadishu, Somalia
Interview
256 Mustafa Omer Humanitarian Liaison Officer OCHA Mogadishu, Somalia
Interview
257 Sarah Otuku Humanitarian Affairs Officer - Access
OCHA Mogadishu, Somalia
Interview
258 Iahli Patale Head, Administrative and Finance Unit
OCHA Mogadishu, Somalia
Interview
259 Lokuju Peter Inter-Cluster Coordinator OCHA Mogadishu, Somalia
Interview
260 Ahmed Farah Roble
National Humanitarian Affairs Officer
OCHA Mogadishu, Somalia
Interview
261 Rose Foran Surge Personnel (Standby Partners)
OCHA Mogadishu, Somalia
Interview
OCHA Evaluation of Duty of Care | 91
# Name Title Organization Location Type
262 VincentLelei Deputy Humanitarian Coordinator
UN Mogadishu, Somalia
Interview
263 Esther Chausiku Administration UNDP Mogadishu, Somalia
Interview
264 Eida Siregar Administration UNDP Mogadishu, Somalia
Interview
265 Muniandy Shanmugam
Head of Office UNDSS Mogadishu, Somalia
Interview
266 CarolineVanBuren
Country Representative UNHCR Mogadishu, Somalia
Interview
267 Steven Lauweirer Country Representative UNICEF Mogadishu, Somalia
Interview
268 Bhavna Adatia WelfareOfficer UNSOM Mogadishu, Somalia
Interview
269 Michale Keating Special Representative of the Secretary-General for Somalia and Head of the United Nations Assistance Mission in Somalia
UNSOM Mogadishu, Somalia
Interview
270 Amalednvla Rao Munagala
Human Resources Officer UNSOM Mogadishu, Somalia
Interview
271 Laurent Bukera Country Representative WFP Mogadishu, Somalia
Interview
272 Yngvil Foss Deputy Head of Office OCHA Mogadishu, Somalia
Interview
273 Tapiwa Gomo Head, Communications Unit and Security Focal Point
OCHA Mogadishu, Somalia
Interview
274 George Conway Country Director UNDP Mogadishu, Somalia
Interview
275 Amadu Kamara Chief of Mission Support UNSOM Mogadishu, Somalia
Interview
276 Patricia Nyimbae Agwaro
National Humanitarian Affairs Officer
OCHA Nairobi, Kenya Interview
277 Truphosa Anjichi Humanitarian Affairs Officer/Reporting
OCHA Nairobi, Kenya Interview
OCHA Evaluation of Duty of Care | 92
# Name Title Organization Location Type
278 Gemma Connell Head of Office, Regional Office for Southern and Eastern Africa
OCHA Nairobi, Kenya Interview
279 Sophie Garde Thomle
Deputy Head of Office, Regional Office for Southern and Eastern Africa
OCHA Nairobi, Kenya Interview
280 Ayub Gitonga Information Management Officer
OCHA Nairobi, Kenya Group Discussion
281 Michael Kahara Graphics Designer OCHA Nairobi, Kenya Group Discussion
282 Matija Kovac Humanitarian Affairs Officer/Pooled Fund Manager
OCHA Nairobi, Kenya Interview
283 Helen Masibo Executive Assistant OCHA Nairobi, Kenya Group Discussion
284 Adnan Mohammed
Head of Administration OCHA Nairobi, Kenya Interview
285 Erin Mooney Senior Protection Advisor, ProCap
OCHA Nairobi, Kenya Group Discussion
286 Boniface Munywoki
IT Associate OCHA Nairobi, Kenya Group Discussion
287 Dirk-Jan Omtzigt Head, Information Management and Analysis Unit
OCHA Nairobi, Kenya Group Discussion
288 Autumn Peterson Humanitarian Affairs Officer OCHA Nairobi, Kenya Group Discussion
289 Giovanni Quacquarella
Humanitarian Affairs Officer and Security Focal Point
OCHA Nairobi, Kenya Interview
290 Max Schott Deputy Head of Office OCHA Nairobi, Kenya Interview
291 Guiomar Pau Sole Head, Communications Unit OCHA Nairobi, Kenya Group Discussion

OCHA Evaluation of Duty of Care | 93
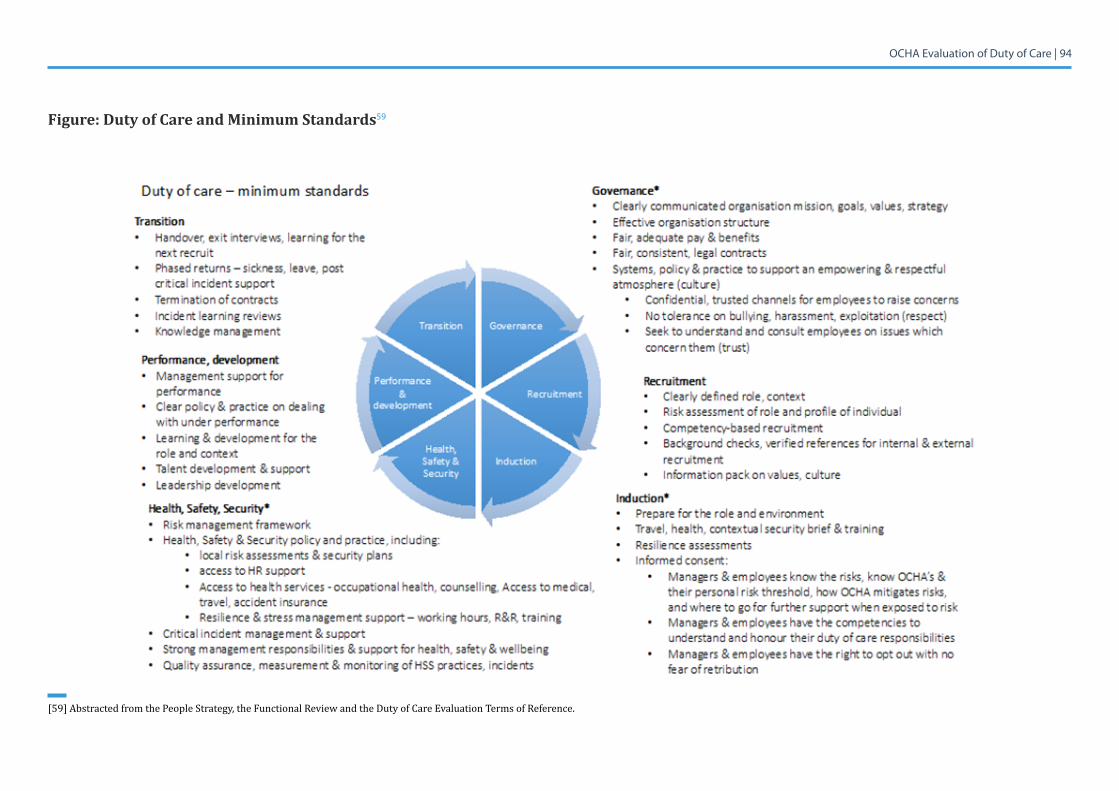
7.4 Annex 4: Conceptual Framework for Duty of Care
Conceptual Framework: Duty of care from a historical and legal perspective is about how to reasona-bly prevent harm and neglect (negligence) of an individual an organization has a degree of control over or proximity to. How far the organization should go to prevent harm and neglect depends on what is deemed good and reasonable practice in the circumstances. In high-risk environments, organizations are expected to enhance their standards and go above and beyond the minimum.
The following model describes some of the minimum standards of duty of care required for OCHA to meet its intention outlined in the People Strategy, i.e., the standards it has set for itself. The scope of the TOR for this evaluation focussed primarily on three of the areas in the model – governance (partial), induction (partial) and health, safety and security. The standards set out below are not exhaustive.
OCHA Evaluation of Duty of Care | 94
Figure: Duty of Care and Minimum Standards59
[59]AbstractedfromthePeopleStrategy,theFunctionalReviewandtheDutyofCareEvaluationTermsofReference.
OCHA Evaluation of Duty of Care | 95
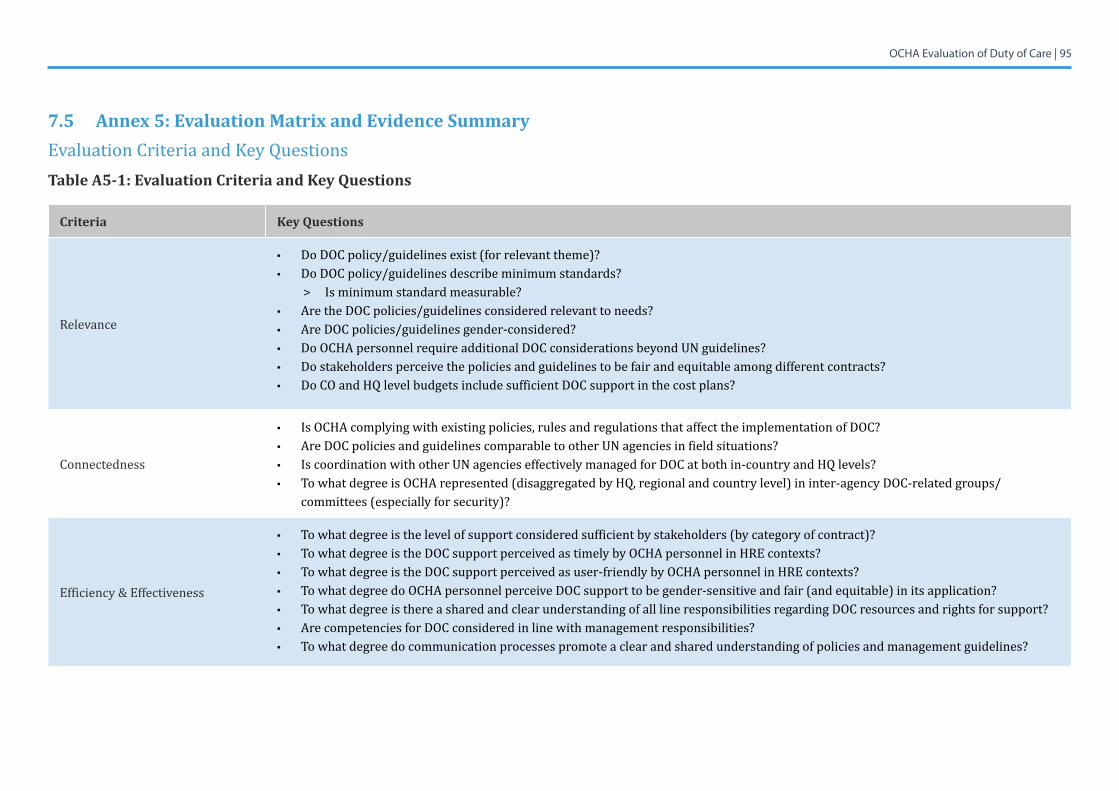
7.5 Annex 5: Evaluation Matrix and Evidence SummaryEvaluation Criteria and Key QuestionsTable A5-1: Evaluation Criteria and Key Questions
Criteria Key Questions
Relevance
• Do DOC policy/guidelines exist (for relevant theme)?• Do DOC policy/guidelines describe minimum standards? > Is minimum standard measurable?• Are the DOC policies/guidelines considered relevant to needs?• Are DOC policies/guidelines gender-considered?• Do OCHA personnel require additional DOC considerations beyond UN guidelines?• Do stakeholders perceive the policies and guidelines to be fair and equitable among different contracts?• Do CO and HQ level budgets include sufficient DOC support in the cost plans?
Connectedness
• Is OCHA complying with existing policies, rules and regulations that affect the implementation of DOC?• Are DOC policies and guidelines comparable to other UN agencies in field situations?• Is coordination with other UN agencies effectively managed for DOC at both in-country and HQ levels?• To what degree is OCHA represented (disaggregated by HQ, regional and country level) in inter-agency DOC-related groups/
committees (especially for security)?
Efficiency & Effectiveness
• To what degree is the level of support considered sufficient by stakeholders (by category of contract)?• To what degree is the DOC support perceived as timely by OCHA personnel in HRE contexts?• To what degree is the DOC support perceived as user-friendly by OCHA personnel in HRE contexts?• To what degree do OCHA personnel perceive DOC support to be gender-sensitive and fair (and equitable) in its application? • To what degree is there a shared and clear understanding of all line responsibilities regarding DOC resources and rights for support?• Are competencies for DOC considered in line with management responsibilities?• To what degree do communication processes promote a clear and shared understanding of policies and management guidelines?
OCHA Evaluation of Duty of Care | 96
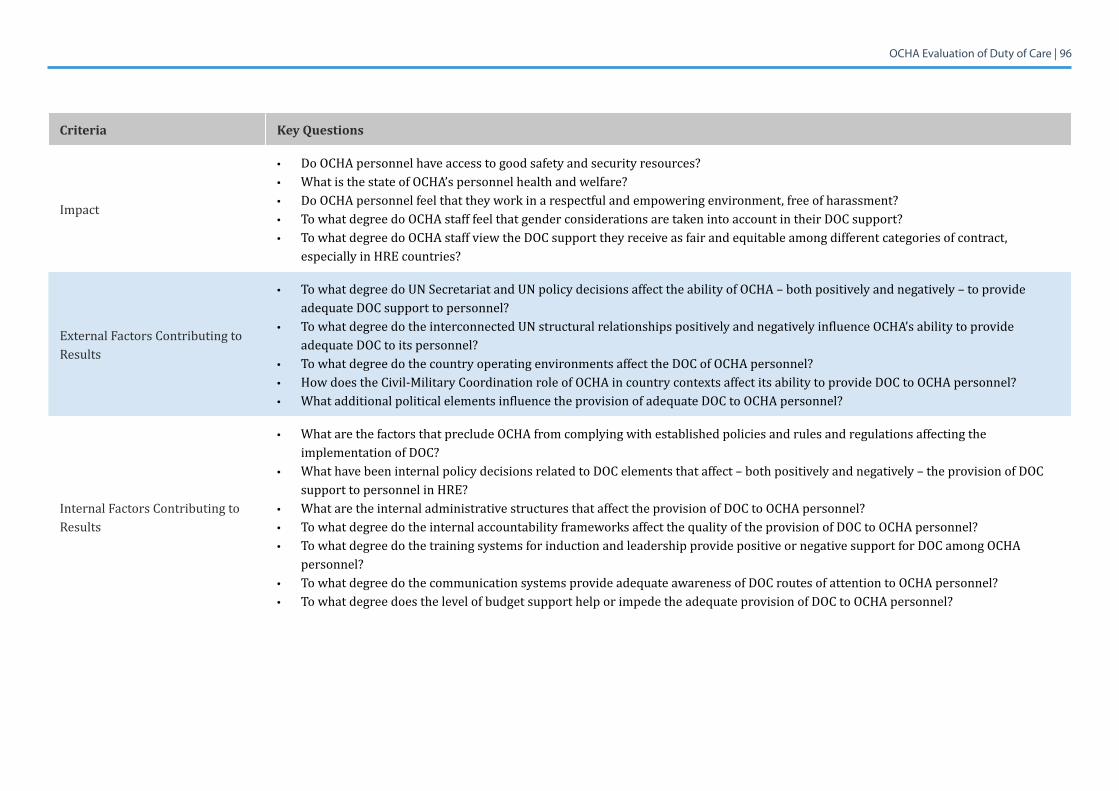
Criteria Key Questions
Impact
• Do OCHA personnel have access to good safety and security resources?• WhatisthestateofOCHA’spersonnelhealthandwelfare?• Do OCHA personnel feel that they work in a respectful and empowering environment, free of harassment?• To what degree do OCHA staff feel that gender considerations are taken into account in their DOC support?• To what degree do OCHA staff view the DOC support they receive as fair and equitable among different categories of contract,
especially in HRE countries?
External Factors Contributing to Results
• To what degree do UN Secretariat and UN policy decisions affect the ability of OCHA – both positively and negatively – to provide adequate DOC support to personnel?
• To what degree do the interconnected UN structural relationships positively and negatively influence OCHA’s ability to provide adequate DOC to its personnel?
• To what degree do the country operating environments affect the DOC of OCHA personnel?• How does the Civil-Military Coordination role of OCHA in country contexts affect its ability to provide DOC to OCHA personnel?• WhatadditionalpoliticalelementsinfluencetheprovisionofadequateDOCtoOCHApersonnel?
Internal Factors Contributing to Results
• WhatarethefactorsthatprecludeOCHAfromcomplyingwithestablishedpoliciesandrulesandregulationsaffectingtheimplementation of DOC?
• WhathavebeeninternalpolicydecisionsrelatedtoDOCelementsthataffect–bothpositivelyandnegatively–theprovisionofDOCsupport to personnel in HRE?
• WhataretheinternaladministrativestructuresthataffecttheprovisionofDOCtoOCHApersonnel?• To what degree do the internal accountability frameworks affect the quality of the provision of DOC to OCHA personnel?• To what degree do the training systems for induction and leadership provide positive or negative support for DOC among OCHA
personnel?• To what degree do the communication systems provide adequate awareness of DOC routes of attention to OCHA personnel? • To what degree does the level of budget support help or impede the adequate provision of DOC to OCHA personnel?
OCHA Evaluation of Duty of Care | 97
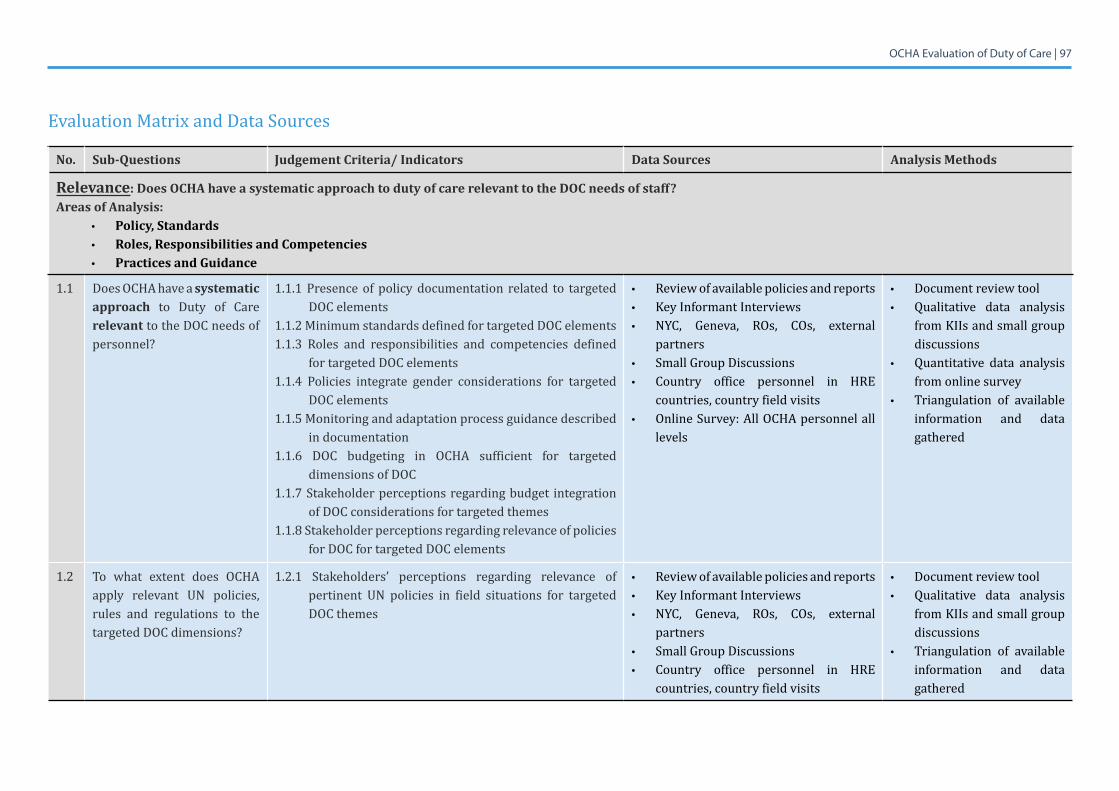
Evaluation Matrix and Data Sources
No. Sub-Questions Judgement Criteria/ Indicators Data Sources Analysis Methods
Relevance: Does OCHA have a systematic approach to duty of care relevant to the DOC needs of staff?Areas of Analysis:
• Policy, Standards• Roles, Responsibilities and Competencies• Practices and Guidance
1.1 Does OCHA have a systematic approach to Duty of Care relevant to the DOC needs of personnel?
1.1.1 Presence of policy documentation related to targeted DOC elements
1.1.2 Minimum standards defined for targeted DOC elements1.1.3 Roles and responsibilities and competencies defined
for targeted DOC elements1.1.4 Policies integrate gender considerations for targeted
DOC elements1.1.5 Monitoring and adaptation process guidance described
in documentation1.1.6 DOC budgeting in OCHA sufficient for targeted
dimensions of DOC1.1.7 Stakeholder perceptions regarding budget integration
of DOC considerations for targeted themes1.1.8Stakeholderperceptionsregardingrelevanceofpolicies
for DOC for targeted DOC elements
• Review of available policies and reports• Key Informant Interviews• NYC, Geneva, ROs, COs, external
partners• Small Group Discussions• Country office personnel in HRE
countries, country field visits• Online Survey: All OCHA personnel all
levels
• Document review tool• Qualitative data analysis
from KIIs and small group discussions
• Quantitative data analysis from online survey
• Triangulation of available information and data gathered
1.2 To what extent does OCHA apply relevant UN policies, rules and regulations to the targeted DOC dimensions?
1.2.1 Stakeholders’ perceptions regarding relevance of pertinent UN policies in field situations for targeted DOC themes
• Review of available policies and reports• Key Informant Interviews• NYC, Geneva, ROs, COs, external
partners• Small Group Discussions• Country office personnel in HRE
countries, country field visits
• Document review tool• Qualitative data analysis
from KIIs and small group discussions
• Triangulation of available information and data gathered
OCHA Evaluation of Duty of Care | 98
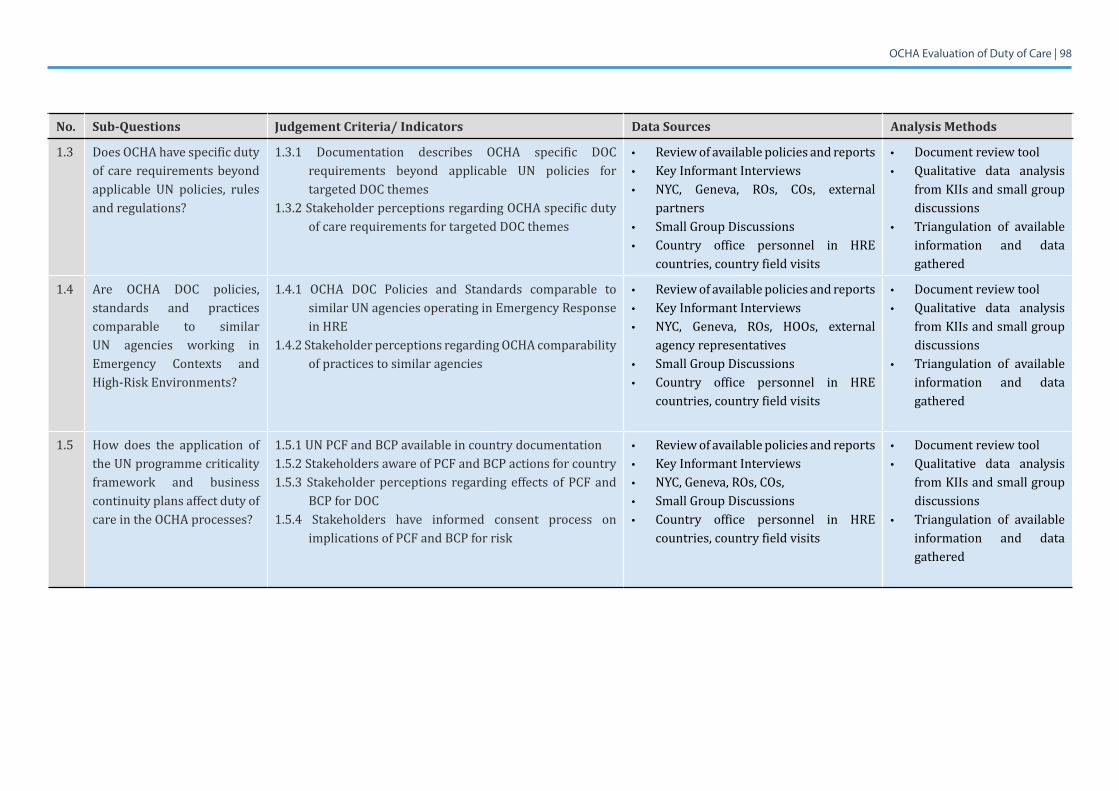
No. Sub-Questions Judgement Criteria/ Indicators Data Sources Analysis Methods
1.3 Does OCHA have specific duty of care requirements beyond applicable UN policies, rules and regulations?
1.3.1 Documentation describes OCHA specific DOC requirements beyond applicable UN policies for targeted DOC themes
1.3.2 Stakeholder perceptions regarding OCHA specific duty of care requirements for targeted DOC themes
• Review of available policies and reports• Key Informant Interviews• NYC, Geneva, ROs, COs, external
partners• Small Group Discussions• Country office personnel in HRE
countries, country field visits
• Document review tool• Qualitative data analysis
from KIIs and small group discussions
• Triangulation of available information and data gathered
1.4 Are OCHA DOC policies, standards and practices comparable to similar UN agencies working in Emergency Contexts and High-Risk Environments?
1.4.1 OCHA DOC Policies and Standards comparable to similar UN agencies operating in Emergency Response in HRE
1.4.2 Stakeholder perceptions regarding OCHA comparability of practices to similar agencies
• Review of available policies and reports• Key Informant Interviews• NYC, Geneva, ROs, HOOs, external
agency representatives• Small Group Discussions• Country office personnel in HRE
countries, country field visits
• Document review tool• Qualitative data analysis
from KIIs and small group discussions
• Triangulation of available information and data gathered
1.5 How does the application of the UN programme criticality framework and business continuity plans affect duty of care in the OCHA processes?
1.5.1 UN PCF and BCP available in country documentation1.5.2 Stakeholders aware of PCF and BCP actions for country 1.5.3 Stakeholder perceptions regarding effects of PCF and
BCP for DOC1.5.4 Stakeholders have informed consent process on
implications of PCF and BCP for risk
• Review of available policies and reports• Key Informant Interviews• NYC, Geneva, ROs, COs, • Small Group Discussions• Country office personnel in HRE
countries, country field visits
• Document review tool• Qualitative data analysis
from KIIs and small group discussions
• Triangulation of available information and data gathered
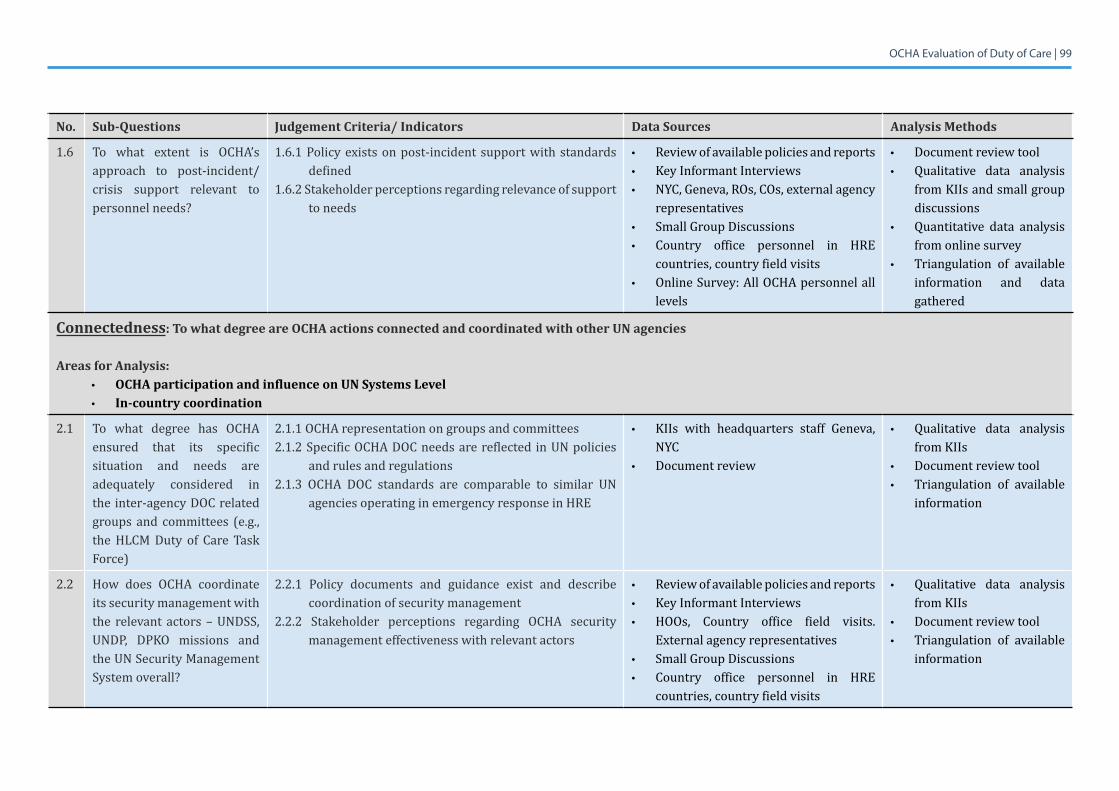
OCHA Evaluation of Duty of Care | 99
No. Sub-Questions Judgement Criteria/ Indicators Data Sources Analysis Methods
1.6 To what extent is OCHA’s approach to post-incident/crisis support relevant to personnel needs?
1.6.1 Policy exists on post-incident support with standards defined
1.6.2 Stakeholder perceptions regarding relevance of support to needs
• Review of available policies and reports• Key Informant Interviews• NYC, Geneva, ROs, COs, external agency
representatives • Small Group Discussions• Country office personnel in HRE
countries, country field visits• Online Survey: All OCHA personnel all
levels
• Document review tool• Qualitative data analysis
from KIIs and small group discussions
• Quantitative data analysis from online survey
• Triangulation of available information and data gathered
Connectedness: To what degree are OCHA actions connected and coordinated with other UN agencies
Areas for Analysis:• OCHA participation and influence on UN Systems Level• In-country coordination
2.1 To what degree has OCHA ensured that its specific situation and needs are adequately considered in the inter-agency DOC related groups and committees (e.g., the HLCM Duty of Care Task Force)
2.1.1 OCHA representation on groups and committees2.1.2 Specific OCHA DOC needs are reflected in UN policies
and rules and regulations2.1.3 OCHA DOC standards are comparable to similar UN
agencies operating in emergency response in HRE
• KIIs with headquarters staff Geneva, NYC
• Document review
• Qualitative data analysis from KIIs
• Document review tool • Triangulation of available
information
2.2 How does OCHA coordinate its security management with the relevant actors – UNDSS, UNDP, DPKO missions and the UN Security Management System overall?
2.2.1 Policy documents and guidance exist and describe coordination of security management
2.2.2 Stakeholder perceptions regarding OCHA security management effectiveness with relevant actors
• Review of available policies and reports• Key Informant Interviews• HOOs, Country office field visits.
External agency representatives• Small Group Discussions• Country office personnel in HRE
countries, country field visits
• Qualitative data analysis from KIIs
• Document review tool• Triangulation of available
information
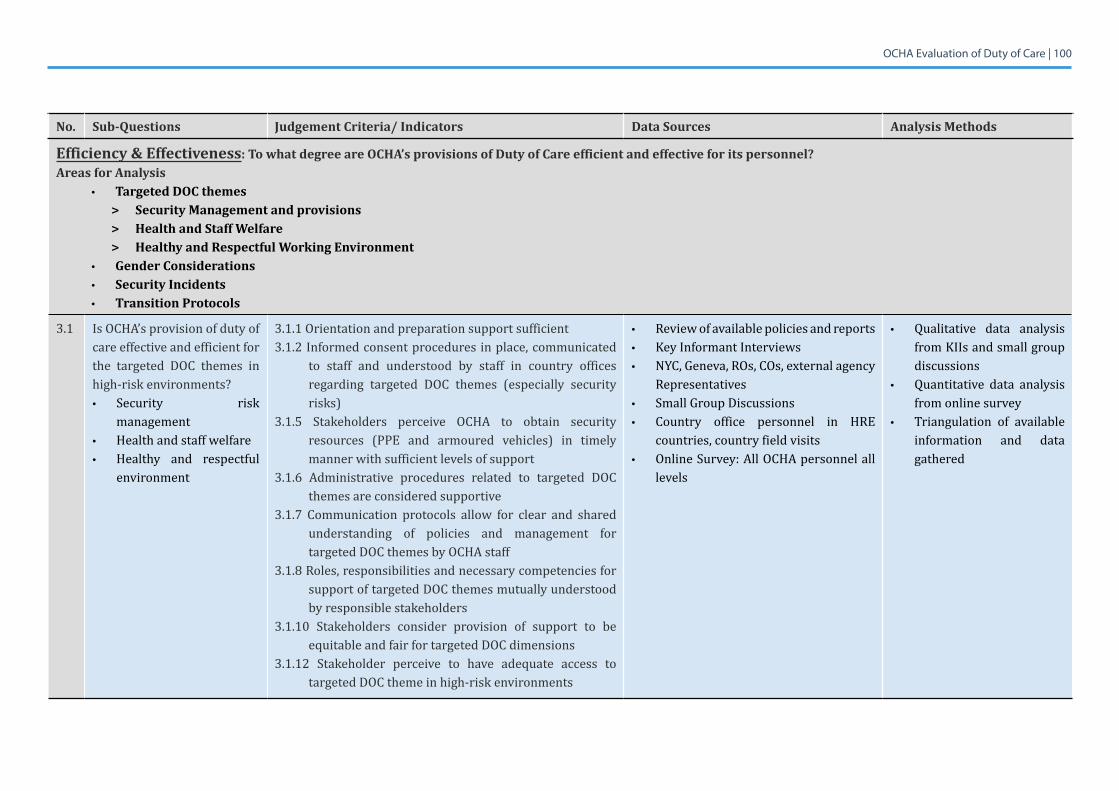
OCHA Evaluation of Duty of Care | 100
No. Sub-Questions Judgement Criteria/ Indicators Data Sources Analysis Methods
Efficiency & Effectiveness: To what degree are OCHA’s provisions of Duty of Care efficient and effective for its personnel?Areas for Analysis
• Targeted DOC themes> Security Management and provisions> Health and Staff Welfare > Healthy and Respectful Working Environment
• Gender Considerations• Security Incidents• Transition Protocols
3.1 Is OCHA’s provision of duty of care effective and efficient for the targeted DOC themes in high-risk environments?• Security risk
management • Health and staff welfare• Healthy and respectful
environment
3.1.1 Orientation and preparation support sufficient 3.1.2 Informed consent procedures in place, communicated
to staff and understood by staff in country offices regarding targeted DOC themes (especially security risks)
3.1.5 Stakeholders perceive OCHA to obtain security resources (PPE and armoured vehicles) in timely manner with sufficient levels of support
3.1.6 Administrative procedures related to targeted DOC themes are considered supportive
3.1.7 Communication protocols allow for clear and shared understanding of policies and management for targeted DOC themes by OCHA staff
3.1.8Roles,responsibilitiesandnecessarycompetenciesforsupport of targeted DOC themes mutually understood by responsible stakeholders
3.1.10 Stakeholders consider provision of support to be equitable and fair for targeted DOC dimensions
3.1.12 Stakeholder perceive to have adequate access to targeted DOC theme in high-risk environments
• Review of available policies and reports• Key Informant Interviews• NYC, Geneva, ROs, COs, external agency
Representatives• Small Group Discussions• Country office personnel in HRE
countries, country field visits• Online Survey: All OCHA personnel all
levels
• Qualitative data analysis from KIIs and small group discussions
• Quantitative data analysis from online survey
• Triangulation of available information and data gathered
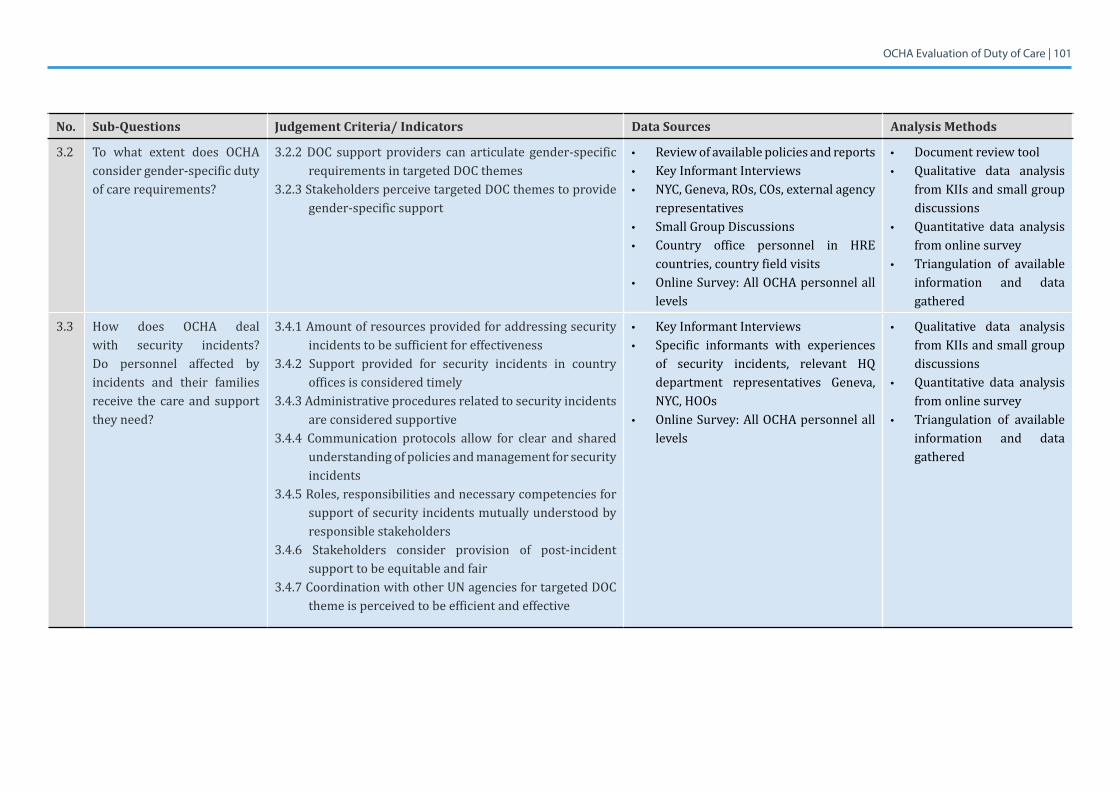
OCHA Evaluation of Duty of Care | 101
No. Sub-Questions Judgement Criteria/ Indicators Data Sources Analysis Methods
3.2 To what extent does OCHA consider gender-specific duty of care requirements?
3.2.2 DOC support providers can articulate gender-specific requirements in targeted DOC themes
3.2.3 Stakeholders perceive targeted DOC themes to provide gender-specific support
• Review of available policies and reports• Key Informant Interviews• NYC, Geneva, ROs, COs, external agency
representatives• Small Group Discussions• Country office personnel in HRE
countries, country field visits• Online Survey: All OCHA personnel all
levels
• Document review tool• Qualitative data analysis
from KIIs and small group discussions
• Quantitative data analysis from online survey
• Triangulation of available information and data gathered
3.3 How does OCHA deal with security incidents? Do personnel affected by incidents and their families receive the care and support they need?
3.4.1 Amount of resources provided for addressing security incidents to be sufficient for effectiveness
3.4.2 Support provided for security incidents in country offices is considered timely
3.4.3 Administrative procedures related to security incidents are considered supportive
3.4.4 Communication protocols allow for clear and shared understanding of policies and management for security incidents
3.4.5 Roles, responsibilities and necessary competencies for support of security incidents mutually understood by responsible stakeholders
3.4.6 Stakeholders consider provision of post-incident support to be equitable and fair
3.4.7 Coordination with other UN agencies for targeted DOC theme is perceived to be efficient and effective
• Key Informant Interviews• Specific informants with experiences
of security incidents, relevant HQ department representatives Geneva, NYC, HOOs
• Online Survey: All OCHA personnel all levels
• Qualitative data analysis from KIIs and small group discussions
• Quantitative data analysis from online survey
• Triangulation of available information and data gathered
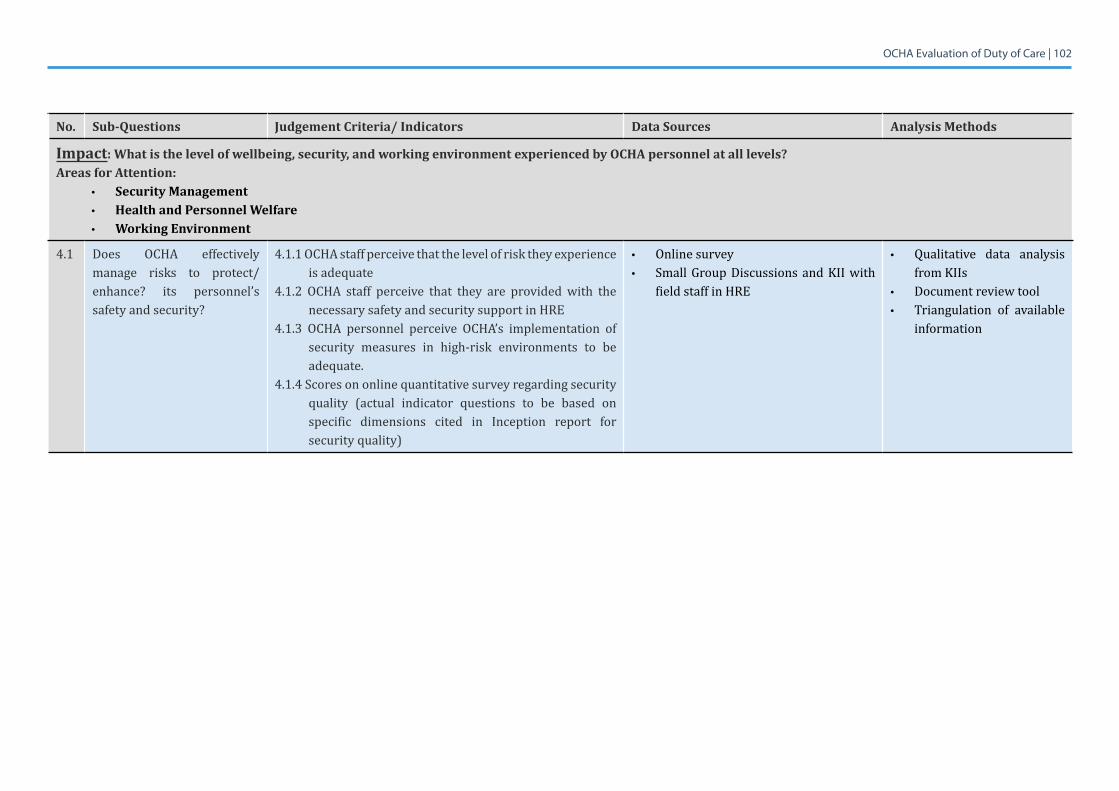
OCHA Evaluation of Duty of Care | 102
No. Sub-Questions Judgement Criteria/ Indicators Data Sources Analysis Methods
Impact: What is the level of wellbeing, security, and working environment experienced by OCHA personnel at all levels?Areas for Attention:
• Security Management• Health and Personnel Welfare• Working Environment
4.1 Does OCHA effectively manage risks to protect/enhance? its personnel’s safety and security?
4.1.1 OCHA staff perceive that the level of risk they experience is adequate
4.1.2 OCHA staff perceive that they are provided with the necessary safety and security support in HRE
4.1.3 OCHA personnel perceive OCHA’s implementation of security measures in high-risk environments to be adequate.
4.1.4 Scores on online quantitative survey regarding security quality (actual indicator questions to be based on specific dimensions cited in Inception report for security quality)
• Online survey• Small Group Discussions and KII with
field staff in HRE
• Qualitative data analysis from KIIs
• Document review tool• Triangulation of available
information
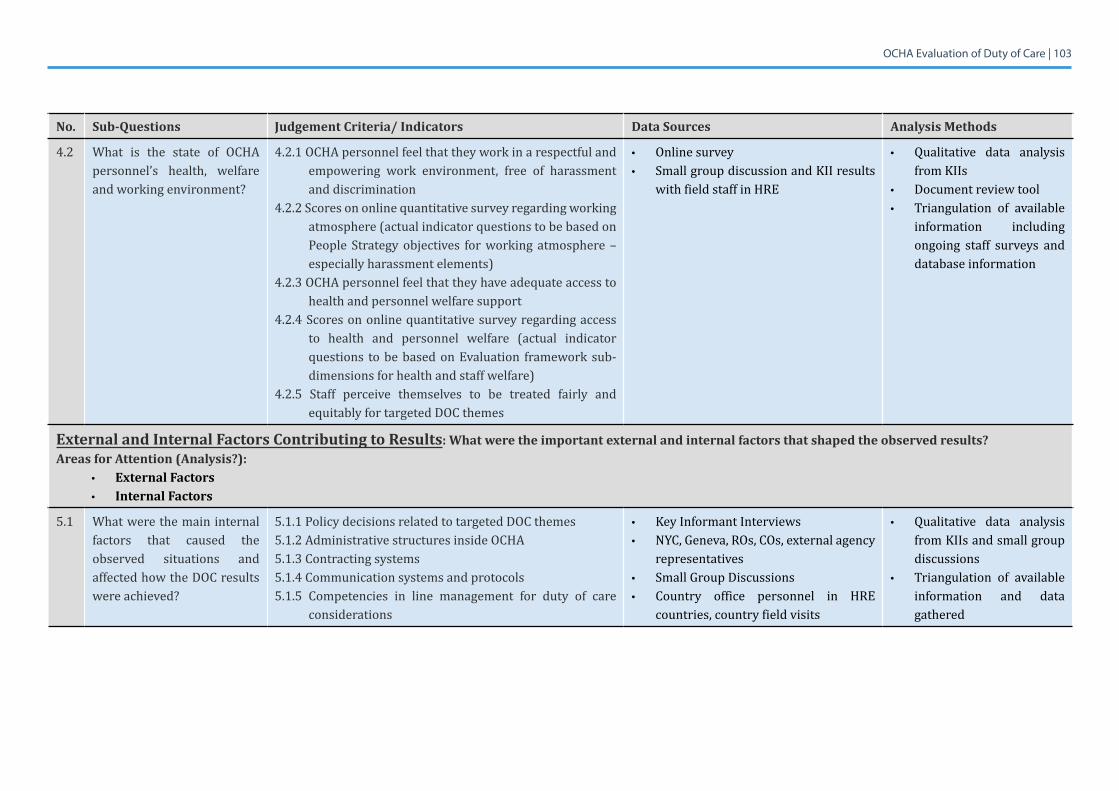
OCHA Evaluation of Duty of Care | 103
No. Sub-Questions Judgement Criteria/ Indicators Data Sources Analysis Methods
4.2 What is the state of OCHApersonnel’s health, welfare and working environment?
4.2.1 OCHA personnel feel that they work in a respectful and empowering work environment, free of harassment and discrimination
4.2.2 Scores on online quantitative survey regarding working atmosphere (actual indicator questions to be based on People Strategy objectives for working atmosphere – especially harassment elements)
4.2.3 OCHA personnel feel that they have adequate access to health and personnel welfare support
4.2.4 Scores on online quantitative survey regarding access to health and personnel welfare (actual indicator questions to be based on Evaluation framework sub-dimensions for health and staff welfare)
4.2.5 Staff perceive themselves to be treated fairly and equitably for targeted DOC themes
• Online survey• Small group discussion and KII results
with field staff in HRE
• Qualitative data analysis from KIIs
• Document review tool • Triangulation of available
information including ongoing staff surveys and database information
External and Internal Factors Contributing to Results: What were the important external and internal factors that shaped the observed results?Areas for Attention (Analysis?):
• External Factors• Internal Factors
5.1 Whatwerethemaininternalfactors that caused the observed situations and affected how the DOC results were achieved?
5.1.1 Policy decisions related to targeted DOC themes5.1.2 Administrative structures inside OCHA5.1.3 Contracting systems5.1.4 Communication systems and protocols5.1.5 Competencies in line management for duty of care
considerations
• Key Informant Interviews• NYC, Geneva, ROs, COs, external agency
representatives• Small Group Discussions• Country office personnel in HRE
countries, country field visits
• Qualitative data analysis from KIIs and small group discussions
• Triangulation of available information and data gathered
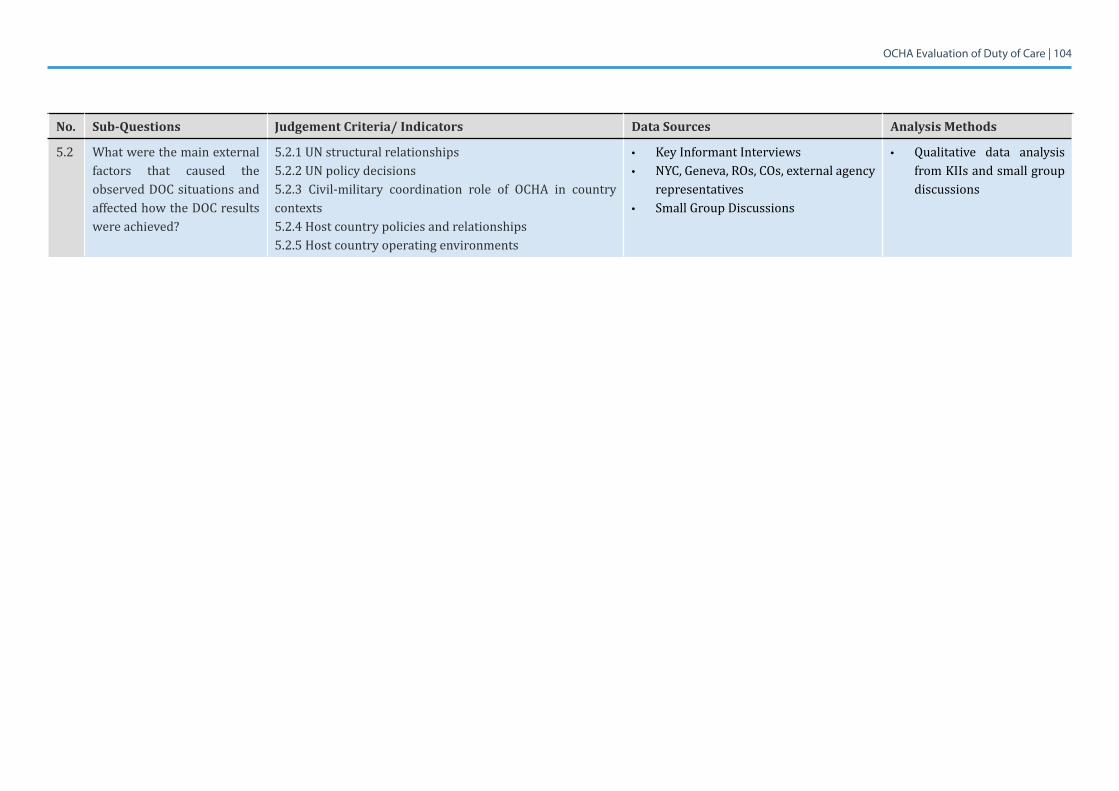
OCHA Evaluation of Duty of Care | 104
No. Sub-Questions Judgement Criteria/ Indicators Data Sources Analysis Methods
5.2 Whatwerethemainexternalfactors that caused the observed DOC situations and affected how the DOC results were achieved?
5.2.1 UN structural relationships5.2.2 UN policy decisions5.2.3 Civil-military coordination role of OCHA in country contexts5.2.4 Host country policies and relationships5.2.5 Host country operating environments
• Key Informant Interviews• NYC, Geneva, ROs, COs, external agency
representatives• Small Group Discussions
• Qualitative data analysis from KIIs and small group discussions
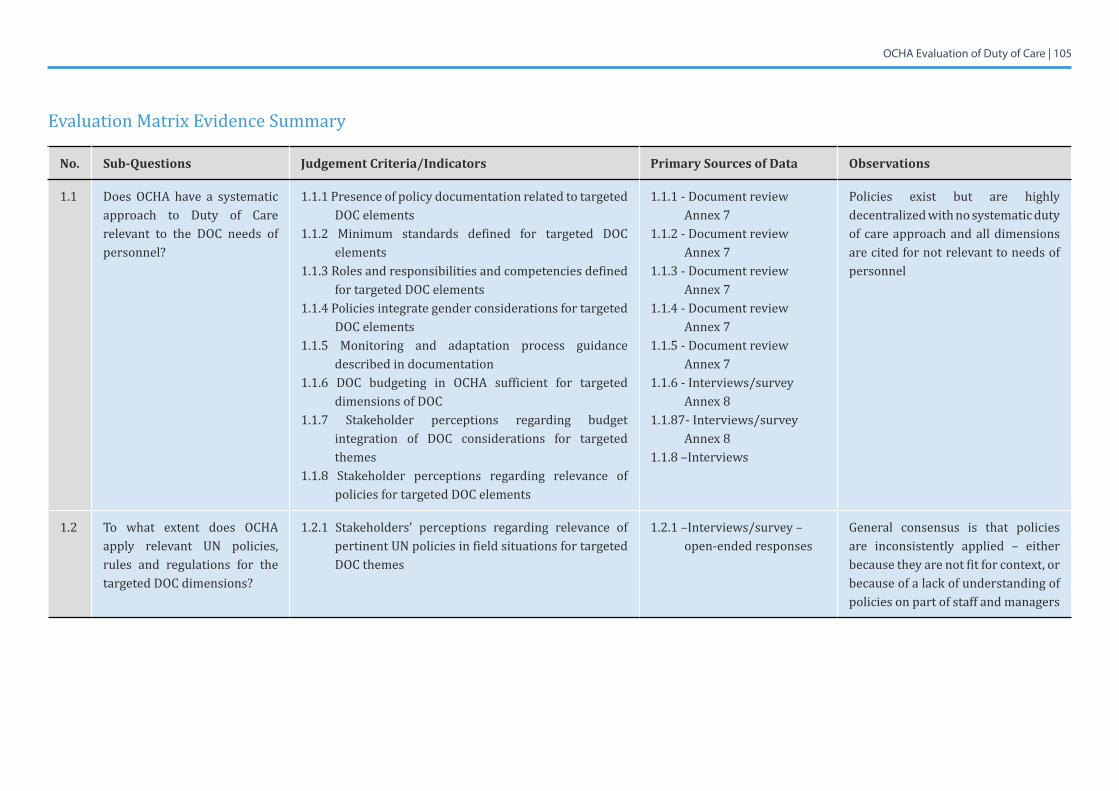
OCHA Evaluation of Duty of Care | 105
Evaluation Matrix Evidence Summary
No. Sub-Questions Judgement Criteria/Indicators Primary Sources of Data Observations
1.1 Does OCHA have a systematic approach to Duty of Care relevant to the DOC needs of personnel?
1.1.1 Presence of policy documentation related to targeted DOC elements
1.1.2 Minimum standards defined for targeted DOC elements
1.1.3 Roles and responsibilities and competencies defined for targeted DOC elements
1.1.4 Policies integrate gender considerations for targeted DOC elements
1.1.5 Monitoring and adaptation process guidance described in documentation
1.1.6 DOC budgeting in OCHA sufficient for targeted dimensions of DOC
1.1.7 Stakeholder perceptions regarding budget integration of DOC considerations for targeted themes
1.1.8 Stakeholder perceptions regarding relevance ofpolicies for targeted DOC elements
1.1.1 - Document review Annex 7
1.1.2 - Document review Annex 7
1.1.3 - Document review Annex 7
1.1.4 - Document review Annex 7
1.1.5 - Document review Annex 7
1.1.6 - Interviews/survey Annex8
1.1.87-Interviews/surveyAnnex8
1.1.8–Interviews
Policies exist but are highly decentralized with no systematic duty of care approach and all dimensions are cited for not relevant to needs of personnel
1.2 To what extent does OCHA apply relevant UN policies, rules and regulations for the targeted DOC dimensions?
1.2.1 Stakeholders’ perceptions regarding relevance of pertinent UN policies in field situations for targeted DOC themes
1.2.1 –Interviews/survey – open-ended responses
General consensus is that policies are inconsistently applied – either because they are not fit for context, or because of a lack of understanding of policies on part of staff and managers
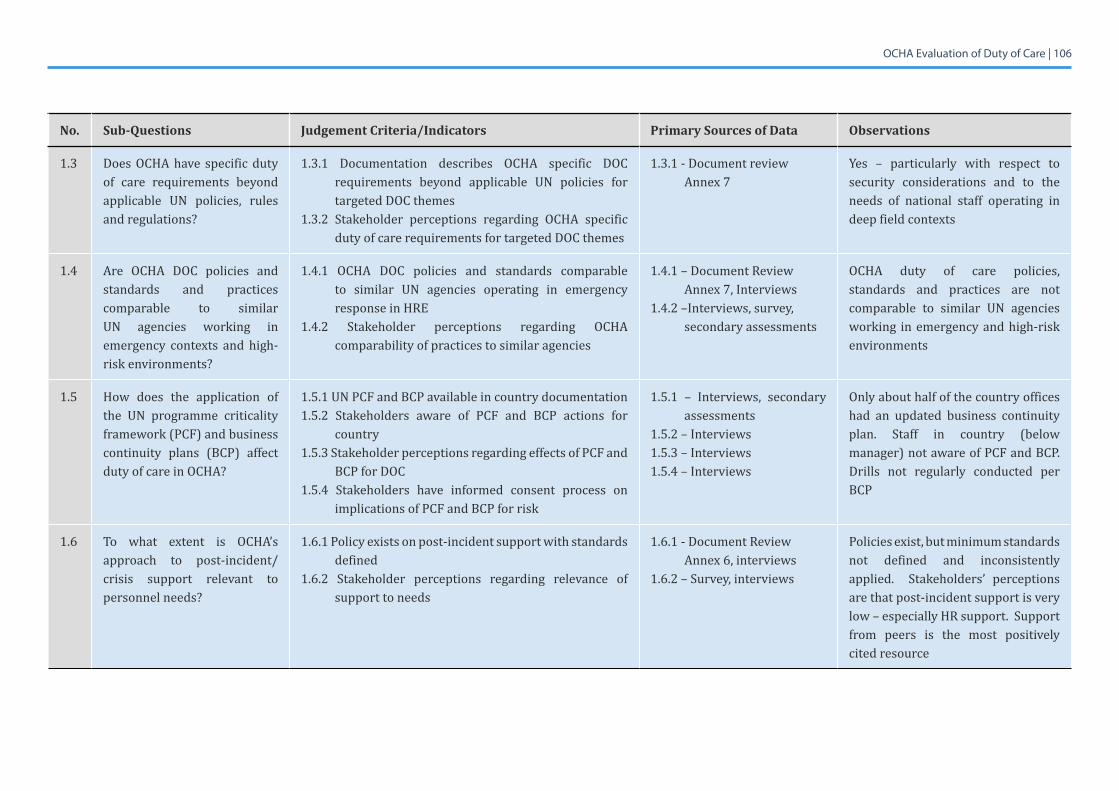
OCHA Evaluation of Duty of Care | 106
No. Sub-Questions Judgement Criteria/Indicators Primary Sources of Data Observations
1.3 Does OCHA have specific duty of care requirements beyond applicable UN policies, rules and regulations?
1.3.1 Documentation describes OCHA specific DOC requirements beyond applicable UN policies for targeted DOC themes
1.3.2 Stakeholder perceptions regarding OCHA specific duty of care requirements for targeted DOC themes
1.3.1 - Document review Annex 7
Yes – particularly with respect to security considerations and to the needs of national staff operating in deep field contexts
1.4 Are OCHA DOC policies and standards and practices comparable to similar UN agencies working in emergency contexts and high-risk environments?
1.4.1 OCHA DOC policies and standards comparable to similar UN agencies operating in emergency response in HRE
1.4.2 Stakeholder perceptions regarding OCHA comparability of practices to similar agencies
1.4.1 – Document Review Annex 7, Interviews
1.4.2 –Interviews, survey, secondary assessments
OCHA duty of care policies, standards and practices are not comparable to similar UN agencies working in emergency and high-risk environments
1.5 How does the application of the UN programme criticality framework (PCF) and business continuity plans (BCP) affect duty of care in OCHA?
1.5.1 UN PCF and BCP available in country documentation1.5.2 Stakeholders aware of PCF and BCP actions for
country 1.5.3 Stakeholder perceptions regarding effects of PCF and
BCP for DOC1.5.4 Stakeholders have informed consent process on
implications of PCF and BCP for risk
1.5.1 – Interviews, secondary assessments
1.5.2 – Interviews1.5.3 – Interviews1.5.4 – Interviews
Only about half of the country offices had an updated business continuity plan. Staff in country (below manager) not aware of PCF and BCP. Drills not regularly conducted per BCP
1.6 To what extent is OCHA’s approach to post-incident/crisis support relevant to personnel needs?
1.6.1 Policy exists on post-incident support with standards defined
1.6.2 Stakeholder perceptions regarding relevance of support to needs
1.6.1 - Document Review Annex 6, interviews
1.6.2 – Survey, interviews
Policies exist, but minimum standards not defined and inconsistently applied. Stakeholders’ perceptions are that post-incident support is very low – especially HR support. Support from peers is the most positively cited resource
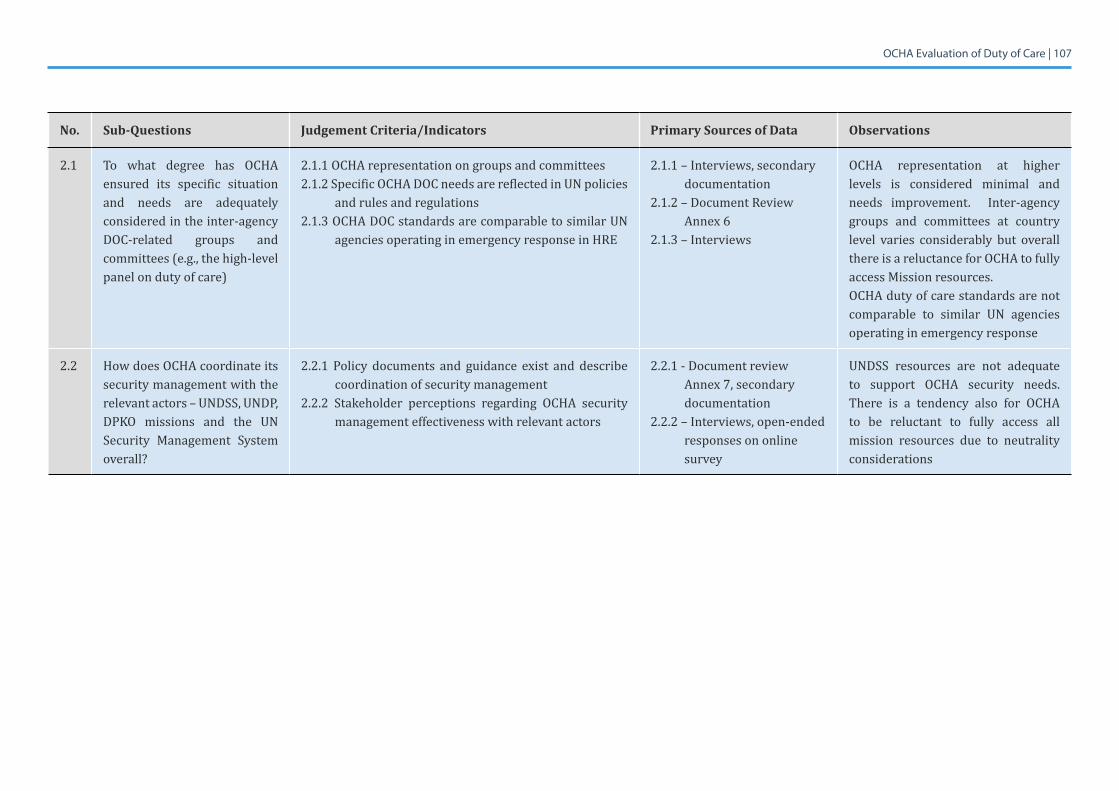
OCHA Evaluation of Duty of Care | 107
No. Sub-Questions Judgement Criteria/Indicators Primary Sources of Data Observations
2.1 To what degree has OCHA ensured its specific situation and needs are adequately considered in the inter-agency DOC-related groups and committees (e.g., the high-level panel on duty of care)
2.1.1 OCHA representation on groups and committees2.1.2 Specific OCHA DOC needs are reflected in UN policies
and rules and regulations2.1.3 OCHA DOC standards are comparable to similar UN
agencies operating in emergency response in HRE
2.1.1 – Interviews, secondary documentation
2.1.2 – Document Review Annex 6
2.1.3 – Interviews
OCHA representation at higher levels is considered minimal and needs improvement. Inter-agency groups and committees at country level varies considerably but overall there is a reluctance for OCHA to fully access Mission resources.OCHA duty of care standards are not comparable to similar UN agencies operating in emergency response
2.2 How does OCHA coordinate its security management with the relevant actors – UNDSS, UNDP, DPKO missions and the UN Security Management System overall?
2.2.1 Policy documents and guidance exist and describe coordination of security management
2.2.2 Stakeholder perceptions regarding OCHA security management effectiveness with relevant actors
2.2.1 - Document review Annex 7, secondary documentation
2.2.2 – Interviews, open-ended responses on online survey
UNDSS resources are not adequate to support OCHA security needs. There is a tendency also for OCHA to be reluctant to fully access all mission resources due to neutrality considerations
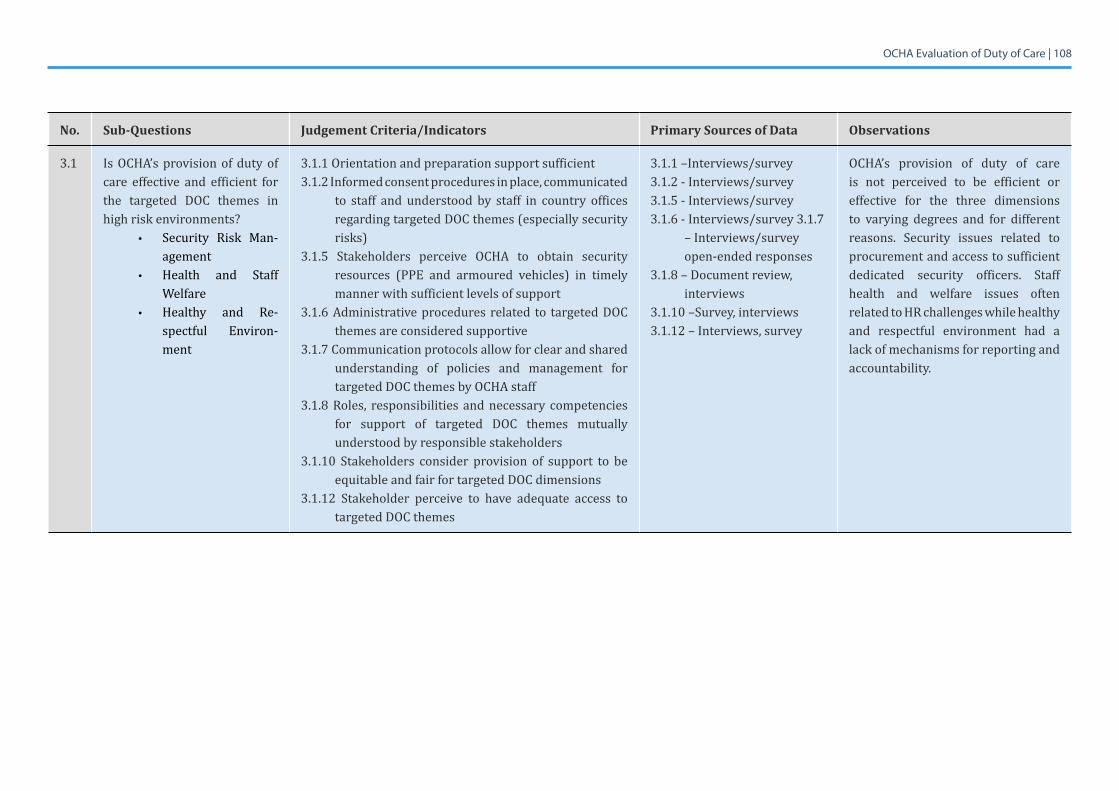
OCHA Evaluation of Duty of Care | 108
No. Sub-Questions Judgement Criteria/Indicators Primary Sources of Data Observations
3.1 Is OCHA’s provision of duty of care effective and efficient for the targeted DOC themes in high risk environments?
• Security Risk Man-agement
• Health and Staff Welfare
• Healthy and Re-spectful Environ-ment
3.1.1 Orientation and preparation support sufficient 3.1.2 Informed consent procedures in place, communicated
to staff and understood by staff in country offices regarding targeted DOC themes (especially security risks)
3.1.5 Stakeholders perceive OCHA to obtain security resources (PPE and armoured vehicles) in timely manner with sufficient levels of support
3.1.6 Administrative procedures related to targeted DOC themes are considered supportive
3.1.7 Communication protocols allow for clear and shared understanding of policies and management for targeted DOC themes by OCHA staff
3.1.8Roles, responsibilitiesandnecessary competenciesfor support of targeted DOC themes mutually understood by responsible stakeholders
3.1.10 Stakeholders consider provision of support to be equitable and fair for targeted DOC dimensions
3.1.12 Stakeholder perceive to have adequate access to targeted DOC themes
3.1.1 –Interviews/survey 3.1.2 - Interviews/survey3.1.5 - Interviews/survey3.1.6 - Interviews/survey 3.1.7
– Interviews/survey open-ended responses
3.1.8–Documentreview,interviews
3.1.10 –Survey, interviews3.1.12 – Interviews, survey
OCHA’s provision of duty of care is not perceived to be efficient or effective for the three dimensions to varying degrees and for different reasons. Security issues related to procurement and access to sufficient dedicated security officers. Staff health and welfare issues often related to HR challenges while healthy and respectful environment had a lack of mechanisms for reporting and accountability.
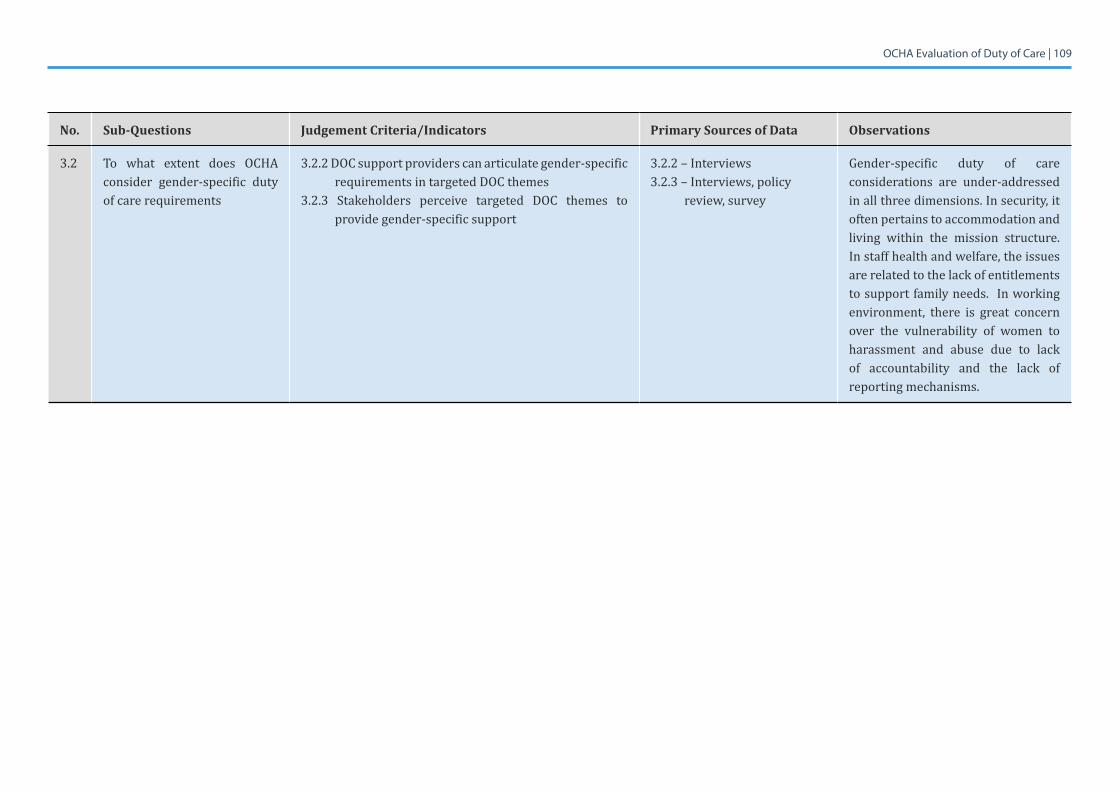
OCHA Evaluation of Duty of Care | 109
No. Sub-Questions Judgement Criteria/Indicators Primary Sources of Data Observations
3.2 To what extent does OCHA consider gender-specific duty of care requirements
3.2.2 DOC support providers can articulate gender-specific requirements in targeted DOC themes
3.2.3 Stakeholders perceive targeted DOC themes to provide gender-specific support
3.2.2 – Interviews3.2.3 – Interviews, policy
review, survey
Gender-specific duty of care considerations are under-addressed in all three dimensions. In security, it often pertains to accommodation and living within the mission structure. In staff health and welfare, the issues are related to the lack of entitlements to support family needs. In working environment, there is great concern over the vulnerability of women to harassment and abuse due to lack of accountability and the lack of reporting mechanisms.
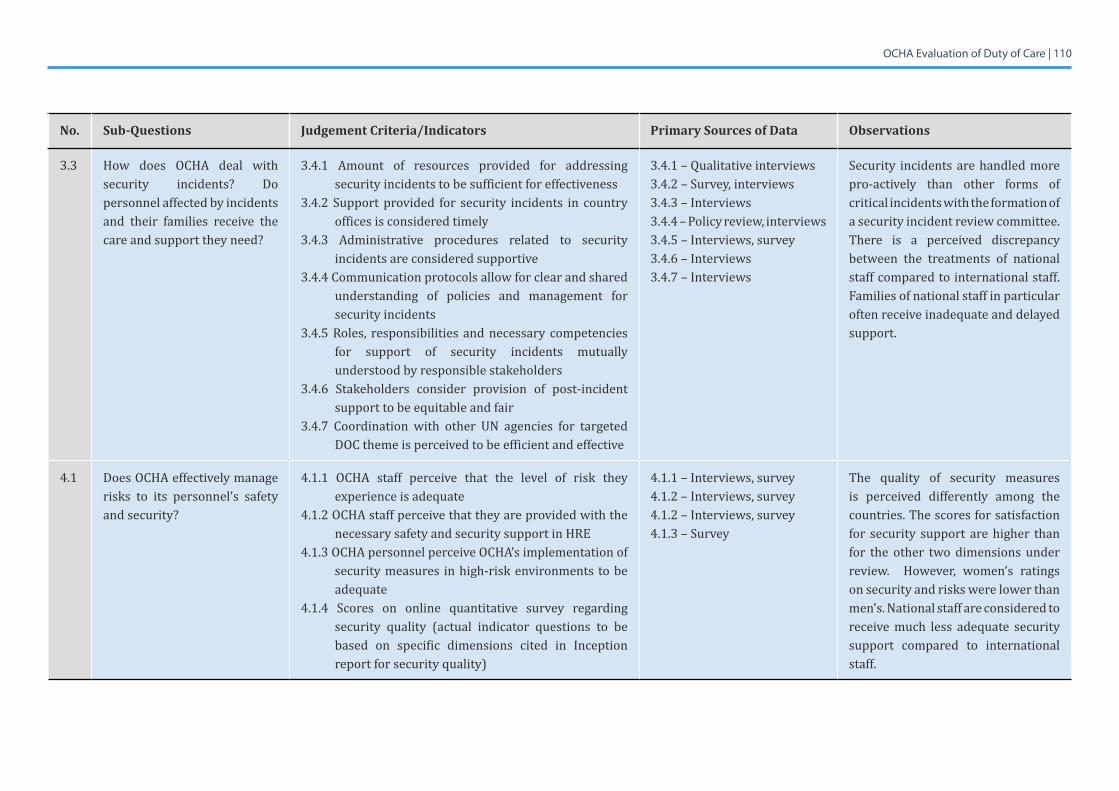
OCHA Evaluation of Duty of Care | 110
No. Sub-Questions Judgement Criteria/Indicators Primary Sources of Data Observations
3.3 How does OCHA deal with security incidents? Do personnel affected by incidents and their families receive the care and support they need?
3.4.1 Amount of resources provided for addressing security incidents to be sufficient for effectiveness
3.4.2 Support provided for security incidents in country offices is considered timely
3.4.3 Administrative procedures related to security incidents are considered supportive
3.4.4 Communication protocols allow for clear and shared understanding of policies and management for security incidents
3.4.5 Roles, responsibilities and necessary competencies for support of security incidents mutually understood by responsible stakeholders
3.4.6 Stakeholders consider provision of post-incident support to be equitable and fair
3.4.7 Coordination with other UN agencies for targeted DOC theme is perceived to be efficient and effective
3.4.1 – Qualitative interviews3.4.2 – Survey, interviews3.4.3 – Interviews3.4.4 – Policy review, interviews3.4.5 – Interviews, survey3.4.6 – Interviews3.4.7 – Interviews
Security incidents are handled more pro-actively than other forms of critical incidents with the formation of a security incident review committee. There is a perceived discrepancy between the treatments of national staff compared to international staff. Families of national staff in particular often receive inadequate and delayed support.
4.1 Does OCHA effectively manage risks to its personnel’s safety and security?
4.1.1 OCHA staff perceive that the level of risk they experience is adequate
4.1.2 OCHA staff perceive that they are provided with the necessary safety and security support in HRE
4.1.3 OCHA personnel perceive OCHA’s implementation of security measures in high-risk environments to be adequate
4.1.4 Scores on online quantitative survey regarding security quality (actual indicator questions to be based on specific dimensions cited in Inception report for security quality)
4.1.1 – Interviews, survey4.1.2 – Interviews, survey4.1.2 – Interviews, survey4.1.3 – Survey
The quality of security measures is perceived differently among the countries. The scores for satisfaction for security support are higher than for the other two dimensions under review. However, women’s ratings on security and risks were lower than men’s. National staff are considered to receive much less adequate security support compared to international staff.
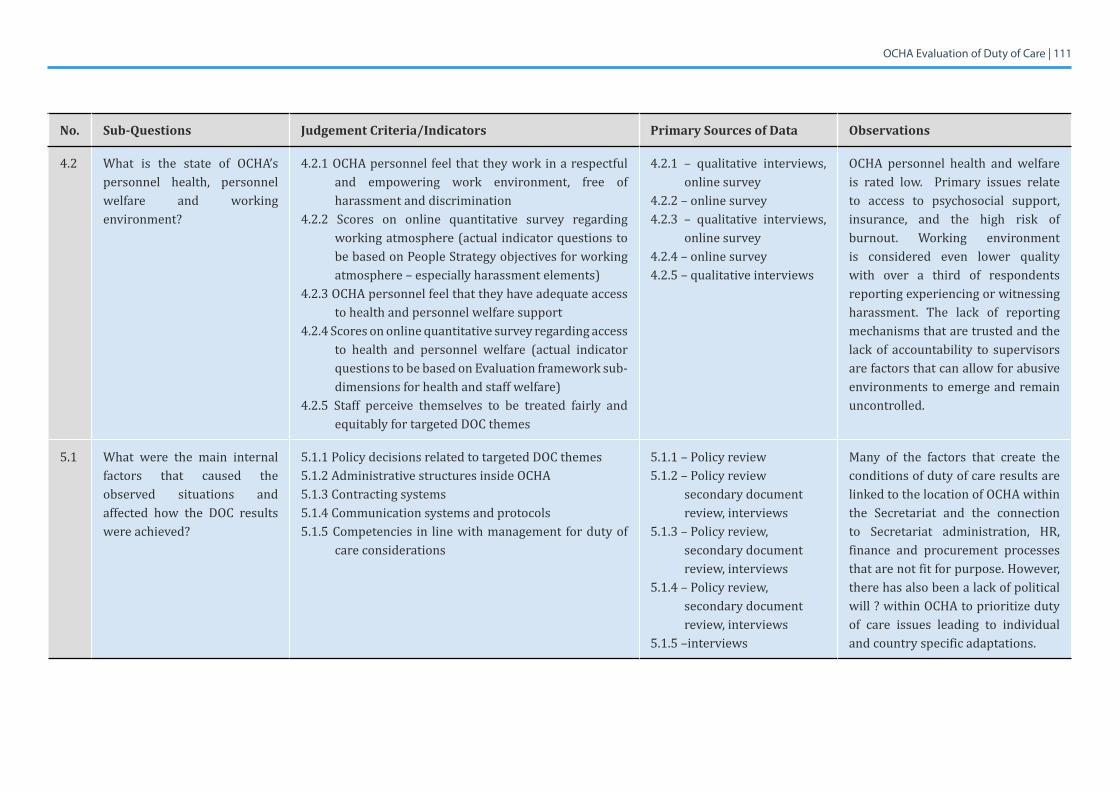
OCHA Evaluation of Duty of Care | 111
No. Sub-Questions Judgement Criteria/Indicators Primary Sources of Data Observations
4.2 What is the state of OCHA’spersonnel health, personnel welfare and working environment?
4.2.1 OCHA personnel feel that they work in a respectful and empowering work environment, free of harassment and discrimination
4.2.2 Scores on online quantitative survey regarding working atmosphere (actual indicator questions to be based on People Strategy objectives for working atmosphere – especially harassment elements)
4.2.3 OCHA personnel feel that they have adequate access to health and personnel welfare support
4.2.4 Scores on online quantitative survey regarding access to health and personnel welfare (actual indicator questions to be based on Evaluation framework sub-dimensions for health and staff welfare)
4.2.5 Staff perceive themselves to be treated fairly and equitably for targeted DOC themes
4.2.1 – qualitative interviews, online survey
4.2.2 – online survey4.2.3 – qualitative interviews,
online survey4.2.4 – online survey4.2.5 – qualitative interviews
OCHA personnel health and welfare is rated low. Primary issues relate to access to psychosocial support, insurance, and the high risk of burnout. Working environmentis considered even lower quality with over a third of respondents reporting experiencing or witnessing harassment. The lack of reporting mechanisms that are trusted and the lack of accountability to supervisors are factors that can allow for abusive environments to emerge and remain uncontrolled.
5.1 What were the main internalfactors that caused the observed situations and affected how the DOC results were achieved?
5.1.1 Policy decisions related to targeted DOC themes5.1.2 Administrative structures inside OCHA5.1.3 Contracting systems5.1.4 Communication systems and protocols5.1.5 Competencies in line with management for duty of
care considerations
5.1.1 – Policy review5.1.2 – Policy review
secondary document review, interviews
5.1.3 – Policy review, secondary document review, interviews
5.1.4 – Policy review, secondary document review, interviews
5.1.5 –interviews
Many of the factors that create the conditions of duty of care results are linked to the location of OCHA within the Secretariat and the connection to Secretariat administration, HR, finance and procurement processes that are not fit for purpose. However, there has also been a lack of political will ? within OCHA to prioritize duty of care issues leading to individual and country specific adaptations.
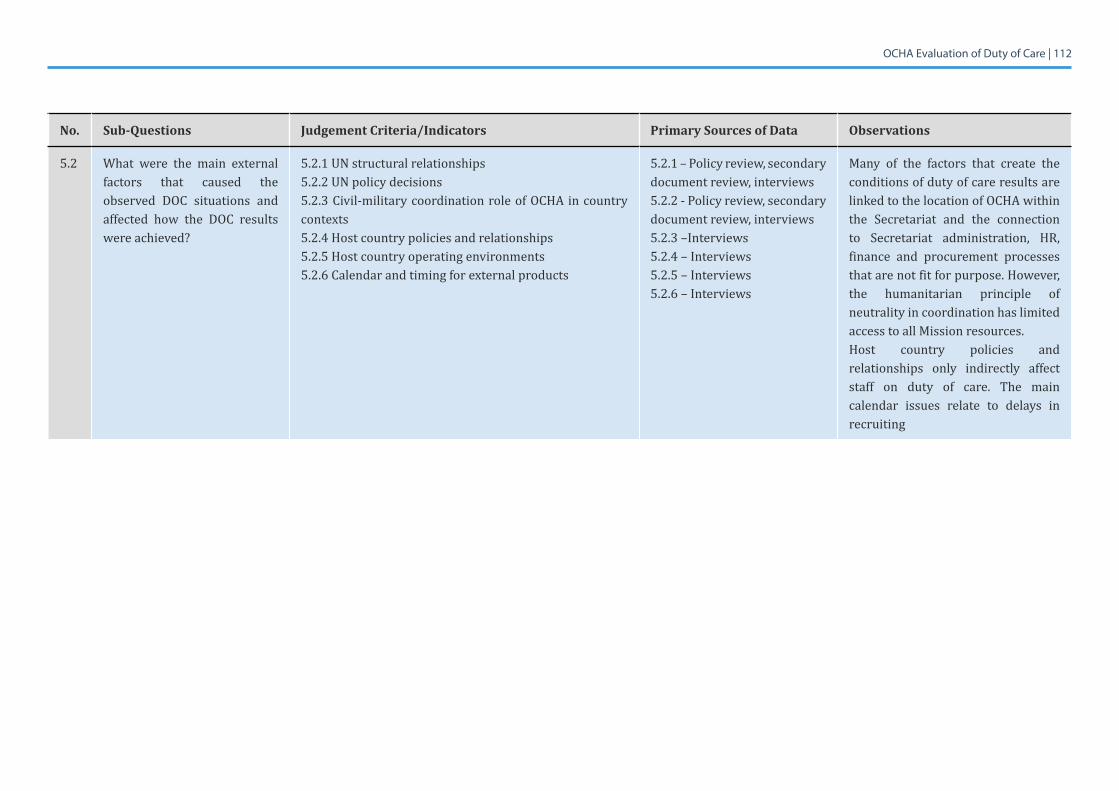
OCHA Evaluation of Duty of Care | 112
No. Sub-Questions Judgement Criteria/Indicators Primary Sources of Data Observations
5.2 What were the main externalfactors that caused the observed DOC situations and affected how the DOC results were achieved?
5.2.1 UN structural relationships5.2.2 UN policy decisions5.2.3 Civil-military coordination role of OCHA in country contexts5.2.4 Host country policies and relationships5.2.5 Host country operating environments5.2.6 Calendar and timing for external products
5.2.1 – Policy review, secondary document review, interviews5.2.2 - Policy review, secondary document review, interviews5.2.3 –Interviews5.2.4 – Interviews5.2.5 – Interviews5.2.6 – Interviews
Many of the factors that create the conditions of duty of care results are linked to the location of OCHA within the Secretariat and the connection to Secretariat administration, HR, finance and procurement processes that are not fit for purpose. However, the humanitarian principle of neutrality in coordination has limited access to all Mission resources. Host country policies and relationships only indirectly affect staff on duty of care. The main calendar issues relate to delays in recruiting
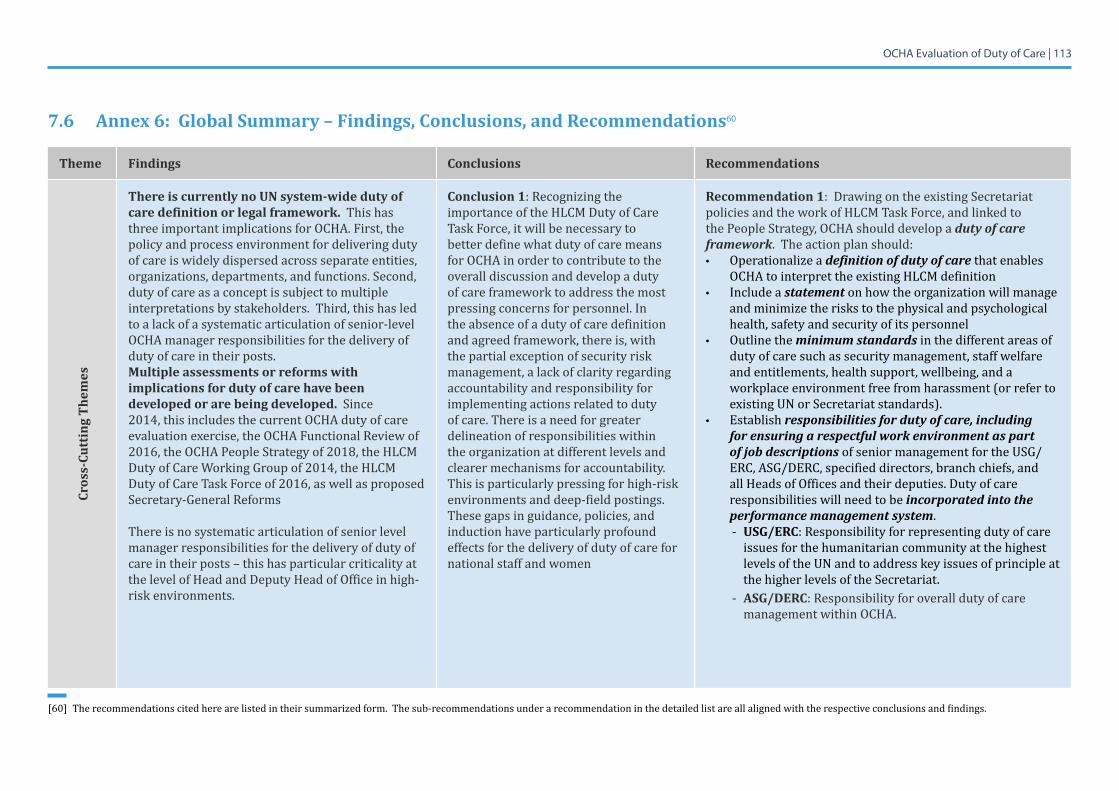
OCHA Evaluation of Duty of Care | 113
7.6 Annex 6: Global Summary – Findings, Conclusions, and Recommendations60
Theme Findings Conclusions Recommendations
Cros
s-Cu
ttin
g Th
emes
There is currently no UN system-wide duty of care definition or legal framework. This has three important implications for OCHA. First, the policy and process environment for delivering duty of care is widely dispersed across separate entities, organizations, departments, and functions. Second, duty of care as a concept is subject to multiple interpretations by stakeholders. Third, this has led to a lack of a systematic articulation of senior-level OCHA manager responsibilities for the delivery of duty of care in their posts.Multiple assessments or reforms with implications for duty of care have been developed or are being developed. Since 2014, this includes the current OCHA duty of care evaluation exercise, the OCHA Functional Review of 2016,theOCHAPeopleStrategyof2018,theHLCMDutyofCareWorkingGroupof2014,theHLCMDuty of Care Task Force of 2016, as well as proposed Secretary-General Reforms
There is no systematic articulation of senior level manager responsibilities for the delivery of duty of care in their posts – this has particular criticality at the level of Head and Deputy Head of Office in high-risk environments.
Conclusion 1: Recognizing the importance of the HLCM Duty of Care Task Force, it will be necessary to better define what duty of care means for OCHA in order to contribute to the overall discussion and develop a duty of care framework to address the most pressing concerns for personnel. In the absence of a duty of care definition and agreed framework, there is, with the partial exception of security risk management, a lack of clarity regarding accountability and responsibility for implementing actions related to duty of care. There is a need for greater delineation of responsibilities within the organization at different levels and clearer mechanisms for accountability. This is particularly pressing for high-risk environments and deep-field postings. These gaps in guidance, policies, and induction have particularly profound effects for the delivery of duty of care for national staff and women
Recommendation 1: Drawing on the existing Secretariat policies and the work of HLCM Task Force, and linked to the People Strategy, OCHA should develop a duty of care framework. The action plan should:• Operationalize a definition of duty of care that enables
OCHA to interpret the existing HLCM definition • Include a statement on how the organization will manage
and minimize the risks to the physical and psychological health, safety and security of its personnel
• Outline the minimum standards in the different areas of duty of care such as security management, staff welfare and entitlements, health support, wellbeing, and a workplace environment free from harassment (or refer to existing UN or Secretariat standards).
• Establish responsibilities for duty of care, including for ensuring a respectful work environment as part of job descriptions of senior management for the USG/ERC, ASG/DERC, specified directors, branch chiefs, and all Heads of Offices and their deputies. Duty of care responsibilities will need to be incorporated into the performance management system.- USG/ERC: Responsibility for representing duty of care
issues for the humanitarian community at the highest levels of the UN and to address key issues of principle at the higher levels of the Secretariat.
- ASG/DERC: Responsibility for overall duty of care management within OCHA.
[60] Therecommendationscitedherearelistedintheirsummarizedform.Thesub-recommendationsunderarecommendationinthedetailedlistareallalignedwiththerespectiveconclusionsandfindings.
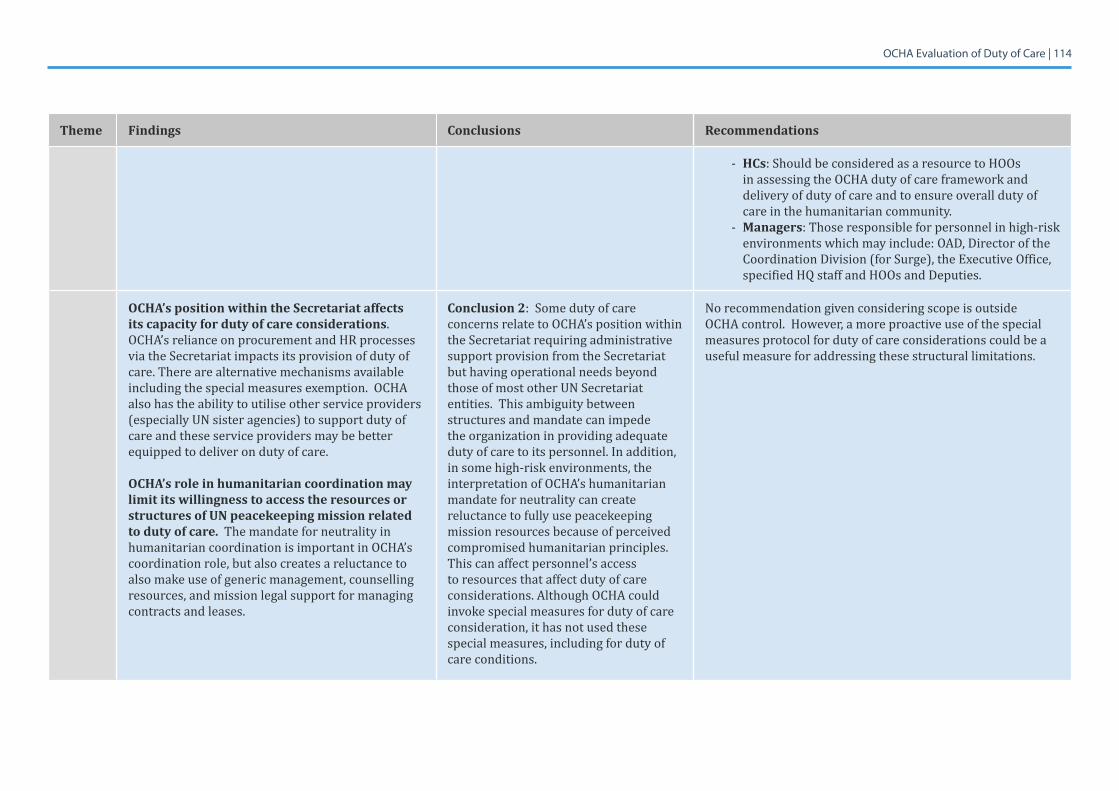
OCHA Evaluation of Duty of Care | 114
Theme Findings Conclusions Recommendations
- HCs: Should be considered as a resource to HOOs in assessing the OCHA duty of care framework and delivery of duty of care and to ensure overall duty of care in the humanitarian community.
- Managers: Those responsible for personnel in high-risk environments which may include: OAD, Director of the Coordination Division (for Surge), the Executive Office, specified HQ staff and HOOs and Deputies.
OCHA’s position within the Secretariat affects its capacity for duty of care considerations. OCHA’s reliance on procurement and HR processes via the Secretariat impacts its provision of duty of care. There are alternative mechanisms available including the special measures exemption. OCHA also has the ability to utilise other service providers (especially UN sister agencies) to support duty of care and these service providers may be better equipped to deliver on duty of care.
OCHA’s role in humanitarian coordination may limit its willingness to access the resources or structures of UN peacekeeping mission related to duty of care. The mandate for neutrality in humanitarian coordination is important in OCHA’s coordination role, but also creates a reluctance to also make use of generic management, counselling resources, and mission legal support for managing contracts and leases.
Conclusion 2: Some duty of care concerns relate to OCHA’s position within the Secretariat requiring administrative support provision from the Secretariat but having operational needs beyond those of most other UN Secretariat entities. This ambiguity between structures and mandate can impede the organization in providing adequate duty of care to its personnel. In addition, in some high-risk environments, the interpretation of OCHA’s humanitarian mandate for neutrality can create reluctance to fully use peacekeeping mission resources because of perceived compromised humanitarian principles. This can affect personnel’s access to resources that affect duty of care considerations. Although OCHA could invoke special measures for duty of care consideration, it has not used these special measures, including for duty of care conditions.
No recommendation given considering scope is outside OCHA control. However, a more proactive use of the special measures protocol for duty of care considerations could be a useful measure for addressing these structural limitations.
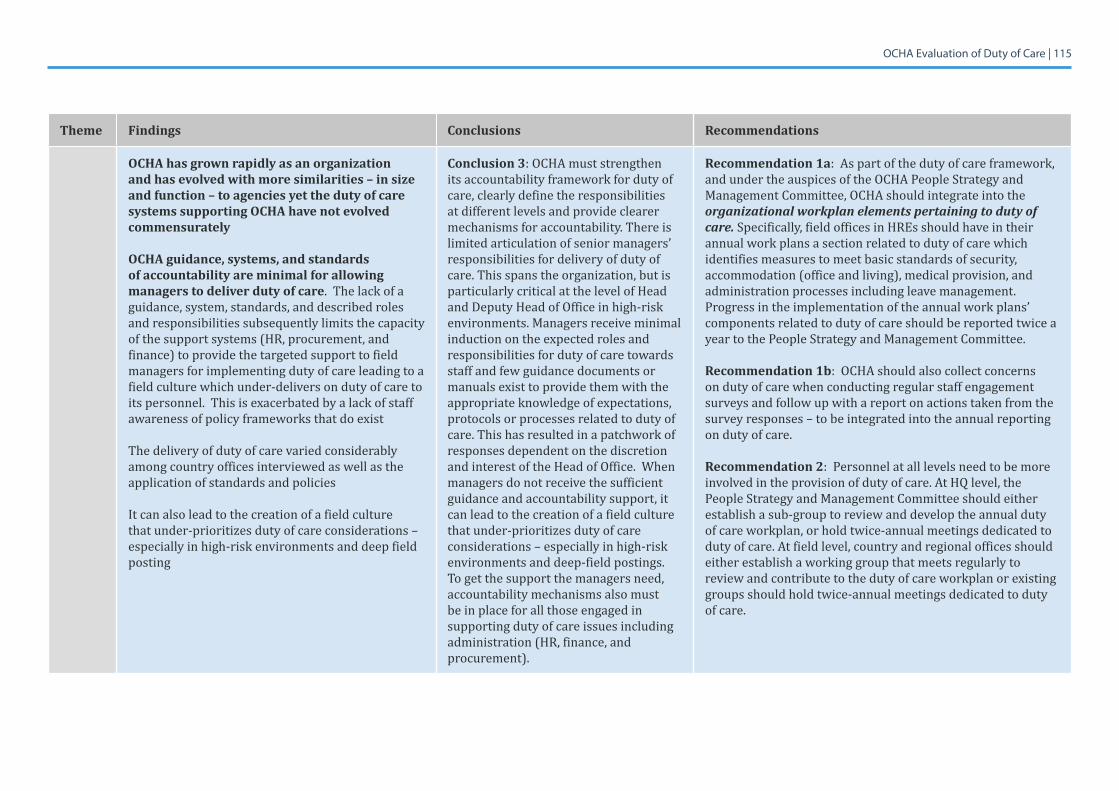
OCHA Evaluation of Duty of Care | 115
Theme Findings Conclusions Recommendations
OCHA has grown rapidly as an organization and has evolved with more similarities – in size and function – to agencies yet the duty of care systems supporting OCHA have not evolved commensurately
OCHA guidance, systems, and standards of accountability are minimal for allowing managers to deliver duty of care. The lack of a guidance, system, standards, and described roles and responsibilities subsequently limits the capacity of the support systems (HR, procurement, and finance) to provide the targeted support to field managers for implementing duty of care leading to a field culture which under-delivers on duty of care to its personnel. This is exacerbated by a lack of staff awareness of policy frameworks that do exist
The delivery of duty of care varied considerably among country offices interviewed as well as the application of standards and policies
It can also lead to the creation of a field culture that under-prioritizes duty of care considerations – especially in high-risk environments and deep field posting
Conclusion 3: OCHA must strengthen its accountability framework for duty of care, clearly define the responsibilities at different levels and provide clearer mechanisms for accountability. There is limited articulation of senior managers’ responsibilities for delivery of duty of care. This spans the organization, but is particularly critical at the level of Head and Deputy Head of Office in high-risk environments. Managers receive minimal induction on the expected roles and responsibilities for duty of care towards staff and few guidance documents or manuals exist to provide them with the appropriate knowledge of expectations, protocols or processes related to duty of care. This has resulted in a patchwork of responses dependent on the discretion andinterestoftheHeadofOffice.Whenmanagers do not receive the sufficient guidance and accountability support, it can lead to the creation of a field culture that under-prioritizes duty of care considerations – especially in high-risk environments and deep-field postings. To get the support the managers need, accountability mechanisms also must be in place for all those engaged in supporting duty of care issues including administration (HR, finance, and procurement).
Recommendation 1a: As part of the duty of care framework, and under the auspices of the OCHA People Strategy and Management Committee, OCHA should integrate into the organizational workplan elements pertaining to duty of care. Specifically, field offices in HREs should have in their annual work plans a section related to duty of care which identifies measures to meet basic standards of security, accommodation (office and living), medical provision, and administration processes including leave management. Progress in the implementation of the annual work plans’ components related to duty of care should be reported twice a year to the People Strategy and Management Committee.
Recommendation 1b: OCHA should also collect concerns on duty of care when conducting regular staff engagement surveys and follow up with a report on actions taken from the survey responses – to be integrated into the annual reporting on duty of care.
Recommendation 2: Personnel at all levels need to be more involved in the provision of duty of care. At HQ level, the People Strategy and Management Committee should either establish a sub-group to review and develop the annual duty of care workplan, or hold twice-annual meetings dedicated to duty of care. At field level, country and regional offices should either establish a working group that meets regularly to review and contribute to the duty of care workplan or existing groups should hold twice-annual meetings dedicated to duty of care.
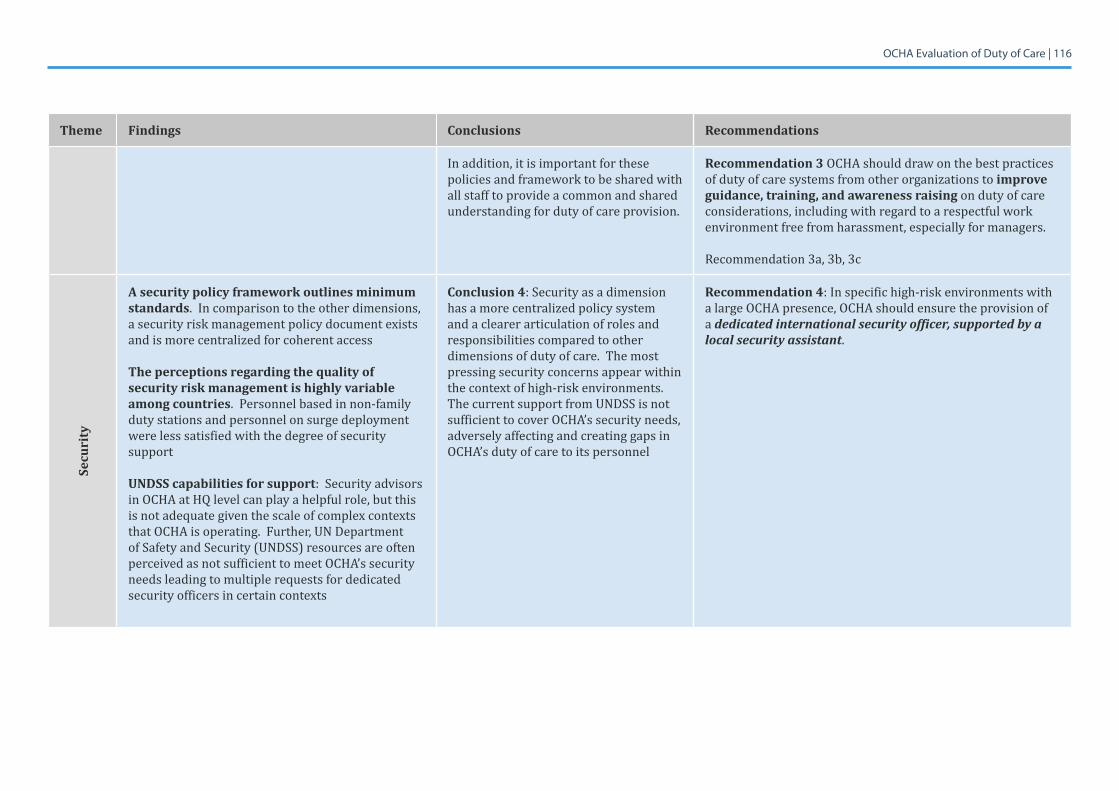
OCHA Evaluation of Duty of Care | 116
Theme Findings Conclusions Recommendations
In addition, it is important for these policies and framework to be shared with all staff to provide a common and shared understanding for duty of care provision.
Recommendation 3 OCHA should draw on the best practices of duty of care systems from other organizations to improve guidance, training, and awareness raising on duty of care considerations, including with regard to a respectful work environment free from harassment, especially for managers.
Recommendation 3a, 3b, 3c
Secu
rity
A security policy framework outlines minimum standards. In comparison to the other dimensions, a security risk management policy document exists and is more centralized for coherent access
The perceptions regarding the quality of security risk management is highly variable among countries. Personnel based in non-family duty stations and personnel on surge deployment were less satisfied with the degree of security support
UNDSS capabilities for support: Security advisors in OCHA at HQ level can play a helpful role, but this is not adequate given the scale of complex contexts that OCHA is operating. Further, UN Department of Safety and Security (UNDSS) resources are often perceived as not sufficient to meet OCHA’s security needs leading to multiple requests for dedicated security officers in certain contexts
Conclusion 4: Security as a dimension has a more centralized policy system and a clearer articulation of roles and responsibilities compared to other dimensions of duty of care. The most pressing security concerns appear within the context of high-risk environments. The current support from UNDSS is not sufficient to cover OCHA’s security needs, adversely affecting and creating gaps in OCHA’s duty of care to its personnel
Recommendation 4: In specific high-risk environments with a large OCHA presence, OCHA should ensure the provision of a dedicated international security officer, supported by a local security assistant.
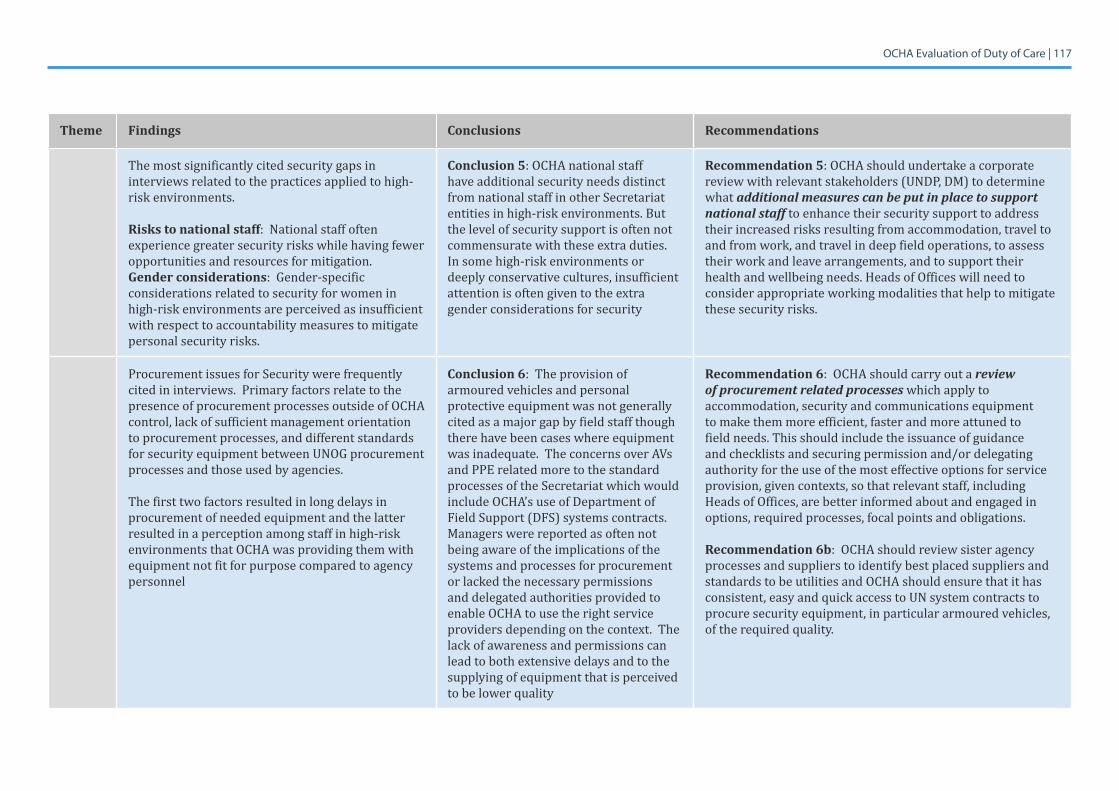
OCHA Evaluation of Duty of Care | 117
Theme Findings Conclusions Recommendations
The most significantly cited security gaps in interviews related to the practices applied to high-risk environments.
Risks to national staff: National staff often experience greater security risks while having fewer opportunities and resources for mitigation.Gender considerations: Gender-specific considerations related to security for women in high-risk environments are perceived as insufficient with respect to accountability measures to mitigate personal security risks.
Conclusion 5: OCHA national staff have additional security needs distinct from national staff in other Secretariat entities in high-risk environments. But the level of security support is often not commensurate with these extra duties. In some high-risk environments or deeply conservative cultures, insufficient attention is often given to the extra gender considerations for security
Recommendation 5: OCHA should undertake a corporate review with relevant stakeholders (UNDP, DM) to determine what additional measures can be put in place to support national staff to enhance their security support to address their increased risks resulting from accommodation, travel to and from work, and travel in deep field operations, to assess their work and leave arrangements, and to support their health and wellbeing needs. Heads of Offices will need to consider appropriate working modalities that help to mitigate these security risks.
Procurement issues for Security were frequently cited in interviews. Primary factors relate to the presence of procurement processes outside of OCHA control, lack of sufficient management orientation to procurement processes, and different standards for security equipment between UNOG procurement processes and those used by agencies.
The first two factors resulted in long delays in procurement of needed equipment and the latter resulted in a perception among staff in high-risk environments that OCHA was providing them with equipment not fit for purpose compared to agency personnel
Conclusion 6: The provision of armoured vehicles and personal protective equipment was not generally cited as a major gap by field staff though there have been cases where equipment wasinadequate.TheconcernsoverAVsand PPE related more to the standard processes of the Secretariat which would include OCHA’s use of Department of Field Support (DFS) systems contracts. Managers were reported as often not being aware of the implications of the systems and processes for procurement or lacked the necessary permissions and delegated authorities provided to enable OCHA to use the right service providers depending on the context. The lack of awareness and permissions can lead to both extensive delays and to the supplying of equipment that is perceived to be lower quality
Recommendation 6: OCHA should carry out a review of procurement related processes which apply to accommodation, security and communications equipment to make them more efficient, faster and more attuned to field needs. This should include the issuance of guidance and checklists and securing permission and/or delegating authority for the use of the most effective options for service provision, given contexts, so that relevant staff, including Heads of Offices, are better informed about and engaged in options, required processes, focal points and obligations.
Recommendation 6b: OCHA should review sister agency processes and suppliers to identify best placed suppliers and standards to be utilities and OCHA should ensure that it has consistent, easy and quick access to UN system contracts to procure security equipment, in particular armoured vehicles, of the required quality.
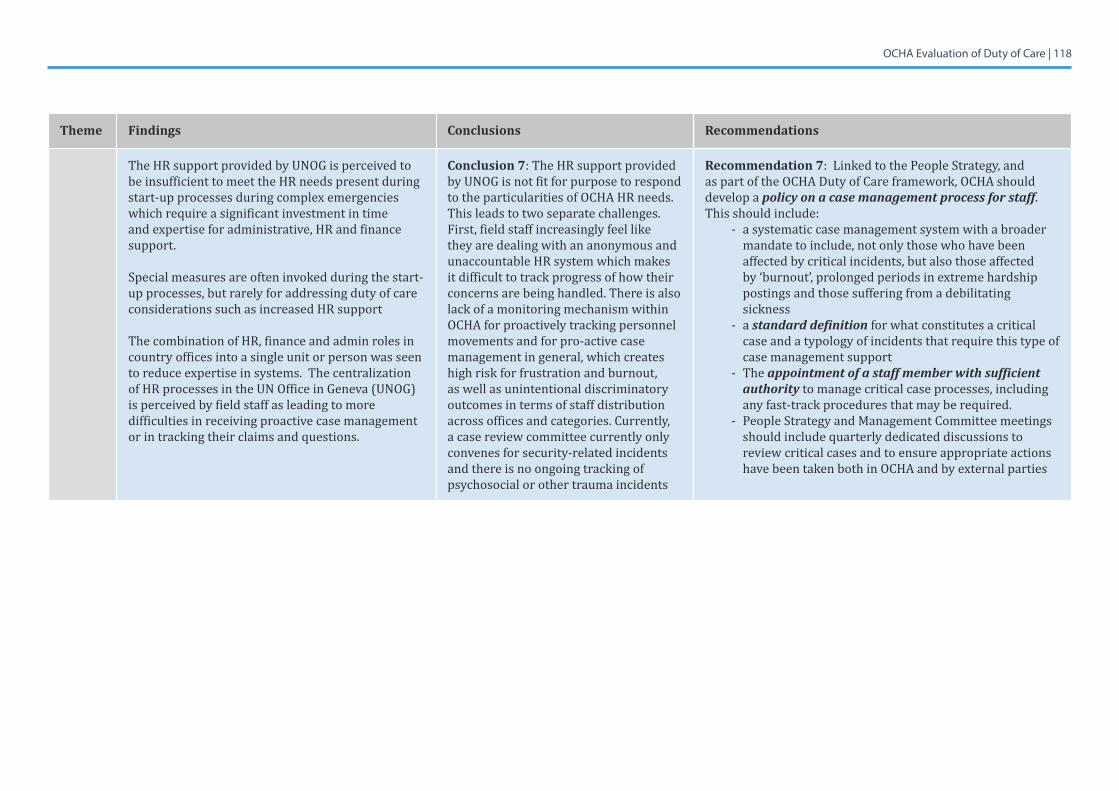
OCHA Evaluation of Duty of Care | 118
Theme Findings Conclusions Recommendations
The HR support provided by UNOG is perceived to be insufficient to meet the HR needs present during start-up processes during complex emergencies which require a significant investment in time and expertise for administrative, HR and finance support.
Special measures are often invoked during the start-up processes, but rarely for addressing duty of care considerations such as increased HR support
The combination of HR, finance and admin roles in country offices into a single unit or person was seen to reduce expertise in systems. The centralization of HR processes in the UN Office in Geneva (UNOG) is perceived by field staff as leading to more difficulties in receiving proactive case management or in tracking their claims and questions.
Conclusion 7: The HR support provided by UNOG is not fit for purpose to respond to the particularities of OCHA HR needs. This leads to two separate challenges. First, field staff increasingly feel like they are dealing with an anonymous and unaccountable HR system which makes it difficult to track progress of how their concerns are being handled. There is also lack of a monitoring mechanism within OCHA for proactively tracking personnel movements and for pro-active case management in general, which creates high risk for frustration and burnout, as well as unintentional discriminatory outcomes in terms of staff distribution across offices and categories. Currently, a case review committee currently only convenes for security-related incidents and there is no ongoing tracking of psychosocial or other trauma incidents
Recommendation 7: Linked to the People Strategy, and as part of the OCHA Duty of Care framework, OCHA should develop a policy on a case management process for staff. This should include:
- a systematic case management system with a broader mandate to include, not only those who have been affected by critical incidents, but also those affected by ‘burnout’, prolonged periods in extreme hardship postings and those suffering from a debilitating sickness
- a standard definition for what constitutes a critical case and a typology of incidents that require this type of case management support
- The appointment of a staff member with sufficient authority to manage critical case processes, including any fast-track procedures that may be required.
- People Strategy and Management Committee meetings should include quarterly dedicated discussions to review critical cases and to ensure appropriate actions have been taken both in OCHA and by external parties
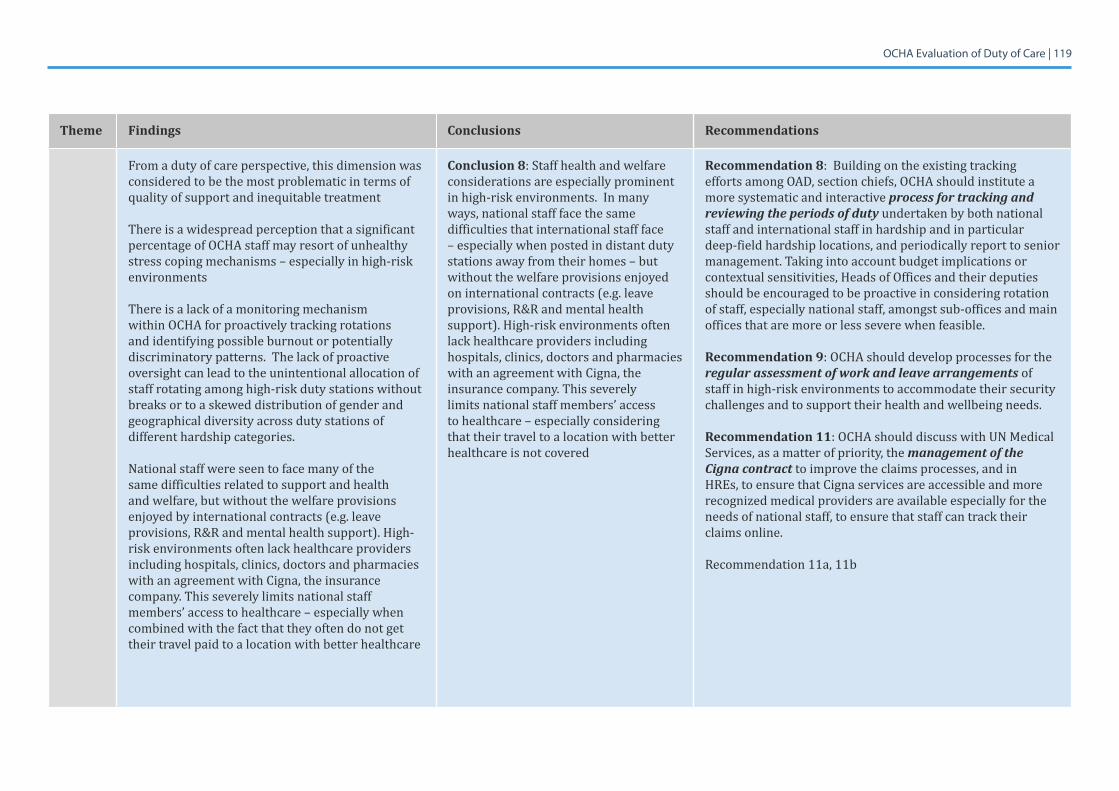
OCHA Evaluation of Duty of Care | 119
Theme Findings Conclusions Recommendations
From a duty of care perspective, this dimension was considered to be the most problematic in terms of quality of support and inequitable treatment
There is a widespread perception that a significant percentage of OCHA staff may resort of unhealthy stress coping mechanisms – especially in high-risk environments
There is a lack of a monitoring mechanism within OCHA for proactively tracking rotations and identifying possible burnout or potentially discriminatory patterns. The lack of proactive oversight can lead to the unintentional allocation of staff rotating among high-risk duty stations without breaks or to a skewed distribution of gender and geographical diversity across duty stations of different hardship categories.
National staff were seen to face many of the same difficulties related to support and health and welfare, but without the welfare provisions enjoyed by international contracts (e.g. leave provisions, R&R and mental health support). High-risk environments often lack healthcare providers including hospitals, clinics, doctors and pharmacies with an agreement with Cigna, the insurance company. This severely limits national staff members’ access to healthcare – especially when combined with the fact that they often do not get their travel paid to a location with better healthcare
Conclusion 8: Staff health and welfare considerations are especially prominent in high-risk environments. In many ways, national staff face the same difficulties that international staff face – especially when posted in distant duty stations away from their homes – but without the welfare provisions enjoyed on international contracts (e.g. leave provisions, R&R and mental health support). High-risk environments often lack healthcare providers including hospitals, clinics, doctors and pharmacies with an agreement with Cigna, the insurance company. This severely limits national staff members’ access to healthcare – especially considering that their travel to a location with better healthcare is not covered
Recommendation 8: Building on the existing tracking efforts among OAD, section chiefs, OCHA should institute a more systematic and interactive process for tracking and reviewing the periods of duty undertaken by both national staff and international staff in hardship and in particular deep-field hardship locations, and periodically report to senior management. Taking into account budget implications or contextual sensitivities, Heads of Offices and their deputies should be encouraged to be proactive in considering rotation of staff, especially national staff, amongst sub-offices and main offices that are more or less severe when feasible.
Recommendation 9: OCHA should develop processes for the regular assessment of work and leave arrangements of staff in high-risk environments to accommodate their security challenges and to support their health and wellbeing needs.
Recommendation 11: OCHA should discuss with UN Medical Services, as a matter of priority, the management of the Cigna contract to improve the claims processes, and in HREs, to ensure that Cigna services are accessible and more recognized medical providers are available especially for the needs of national staff, to ensure that staff can track their claims online.
Recommendation 11a, 11b
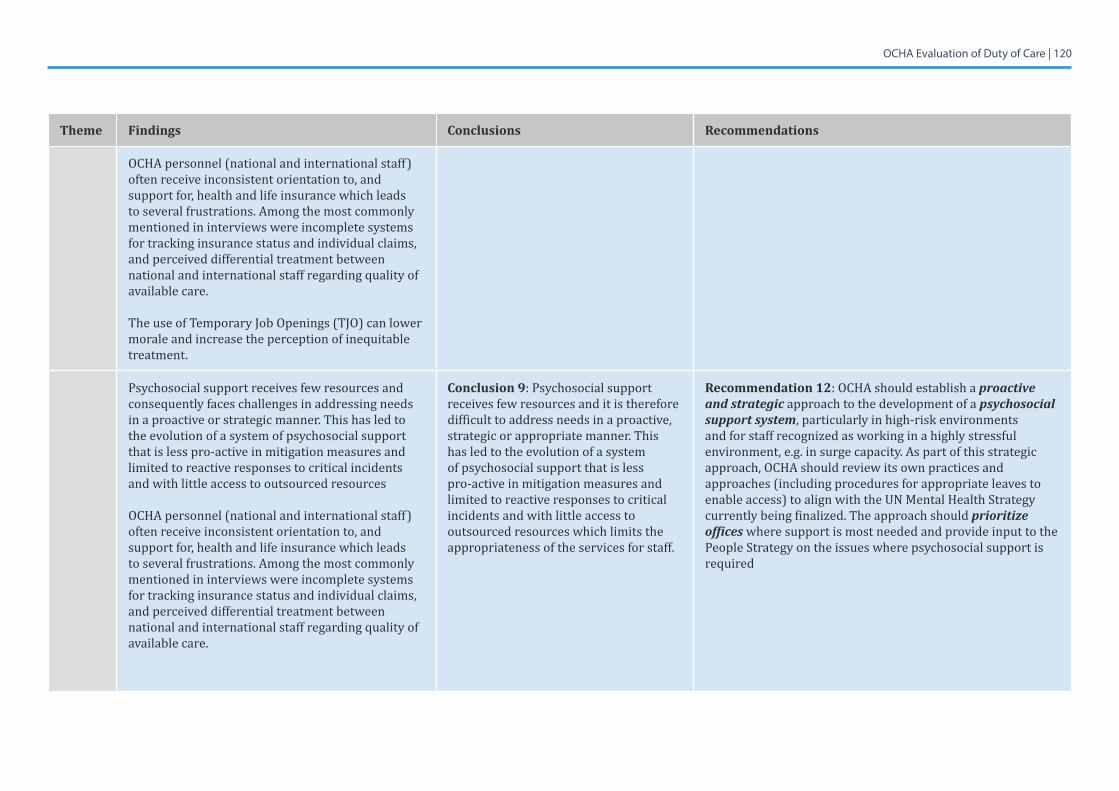
OCHA Evaluation of Duty of Care | 120
Theme Findings Conclusions Recommendations
OCHA personnel (national and international staff) often receive inconsistent orientation to, and support for, health and life insurance which leads to several frustrations. Among the most commonly mentioned in interviews were incomplete systems for tracking insurance status and individual claims, and perceived differential treatment between national and international staff regarding quality of available care.
The use of Temporary Job Openings (TJO) can lower morale and increase the perception of inequitable treatment.
Psychosocial support receives few resources and consequently faces challenges in addressing needs in a proactive or strategic manner. This has led to the evolution of a system of psychosocial support that is less pro-active in mitigation measures and limited to reactive responses to critical incidents and with little access to outsourced resources
OCHA personnel (national and international staff) often receive inconsistent orientation to, and support for, health and life insurance which leads to several frustrations. Among the most commonly mentioned in interviews were incomplete systems for tracking insurance status and individual claims, and perceived differential treatment between national and international staff regarding quality of available care.
Conclusion 9: Psychosocial support receives few resources and it is therefore difficult to address needs in a proactive, strategic or appropriate manner. This has led to the evolution of a system of psychosocial support that is less pro-active in mitigation measures and limited to reactive responses to critical incidents and with little access to outsourced resources which limits the appropriateness of the services for staff.
Recommendation 12: OCHA should establish a proactive and strategic approach to the development of a psychosocial support system, particularly in high-risk environments and for staff recognized as working in a highly stressful environment, e.g. in surge capacity. As part of this strategic approach, OCHA should review its own practices and approaches (including procedures for appropriate leaves to enable access) to align with the UN Mental Health Strategy currently being finalized. The approach should prioritize offices where support is most needed and provide input to the People Strategy on the issues where psychosocial support is required
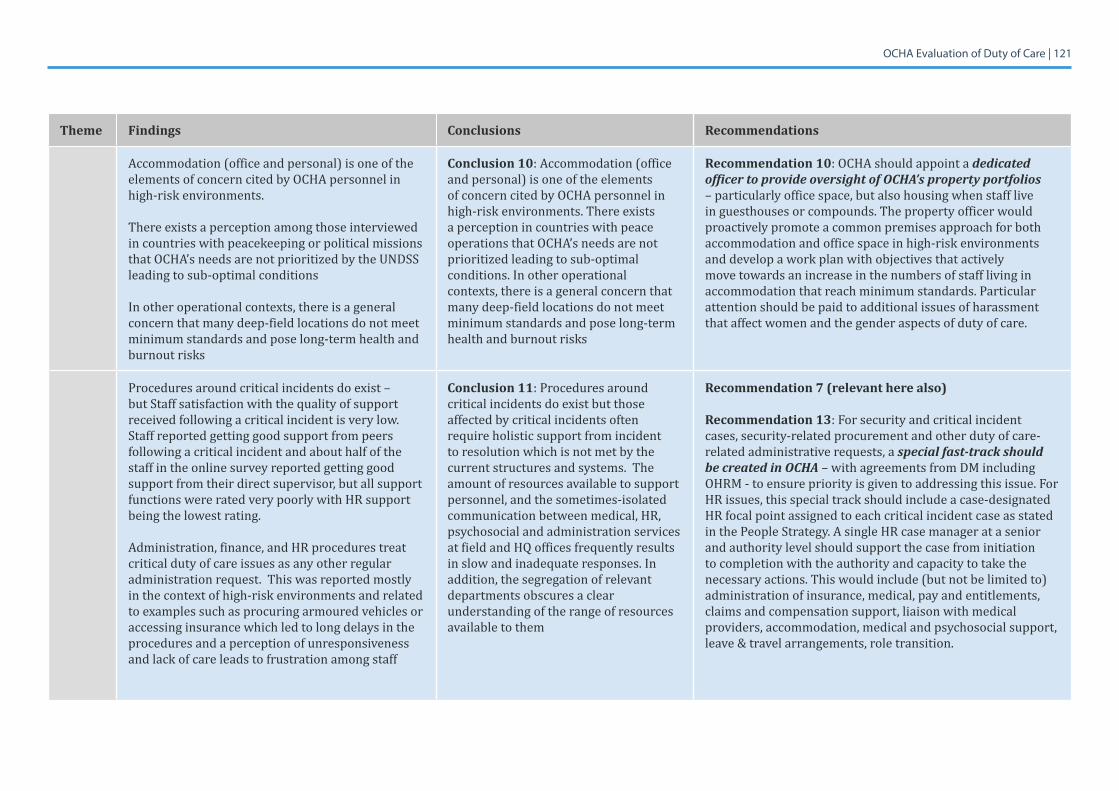
OCHA Evaluation of Duty of Care | 121
Theme Findings Conclusions Recommendations
Accommodation (office and personal) is one of the elements of concern cited by OCHA personnel in high-risk environments.
There exists a perception among those interviewed in countries with peacekeeping or political missions that OCHA’s needs are not prioritized by the UNDSS leading to sub-optimal conditions
In other operational contexts, there is a general concern that many deep-field locations do not meet minimum standards and pose long-term health and burnout risks
Conclusion 10: Accommodation (office and personal) is one of the elements of concern cited by OCHA personnel in high-risk environments. There exists a perception in countries with peace operations that OCHA’s needs are not prioritized leading to sub-optimal conditions. In other operational contexts, there is a general concern that many deep-field locations do not meet minimum standards and pose long-term health and burnout risks
Recommendation 10: OCHA should appoint a dedicated officer to provide oversight of OCHA’s property portfolios – particularly office space, but also housing when staff live in guesthouses or compounds. The property officer would proactively promote a common premises approach for both accommodation and office space in high-risk environments and develop a work plan with objectives that actively move towards an increase in the numbers of staff living in accommodation that reach minimum standards. Particular attention should be paid to additional issues of harassment that affect women and the gender aspects of duty of care.
Procedures around critical incidents do exist – but Staff satisfaction with the quality of support received following a critical incident is very low. Staff reported getting good support from peers following a critical incident and about half of the staff in the online survey reported getting good support from their direct supervisor, but all support functions were rated very poorly with HR support being the lowest rating.
Administration, finance, and HR procedures treat critical duty of care issues as any other regular administration request. This was reported mostly in the context of high-risk environments and related to examples such as procuring armoured vehicles or accessing insurance which led to long delays in the procedures and a perception of unresponsiveness and lack of care leads to frustration among staff
Conclusion 11: Procedures around critical incidents do exist but those affected by critical incidents often require holistic support from incident to resolution which is not met by the current structures and systems. The amount of resources available to support personnel, and the sometimes-isolated communication between medical, HR, psychosocial and administration services at field and HQ offices frequently results in slow and inadequate responses. In addition, the segregation of relevant departments obscures a clear understanding of the range of resources available to them
Recommendation 7 (relevant here also)
Recommendation 13: For security and critical incident cases, security-related procurement and other duty of care-related administrative requests, a special fast-track should be created in OCHA – with agreements from DM including OHRM - to ensure priority is given to addressing this issue. For HR issues, this special track should include a case-designated HR focal point assigned to each critical incident case as stated in the People Strategy. A single HR case manager at a senior and authority level should support the case from initiation to completion with the authority and capacity to take the necessary actions. This would include (but not be limited to) administration of insurance, medical, pay and entitlements, claims and compensation support, liaison with medical providers, accommodation, medical and psychosocial support, leave & travel arrangements, role transition.
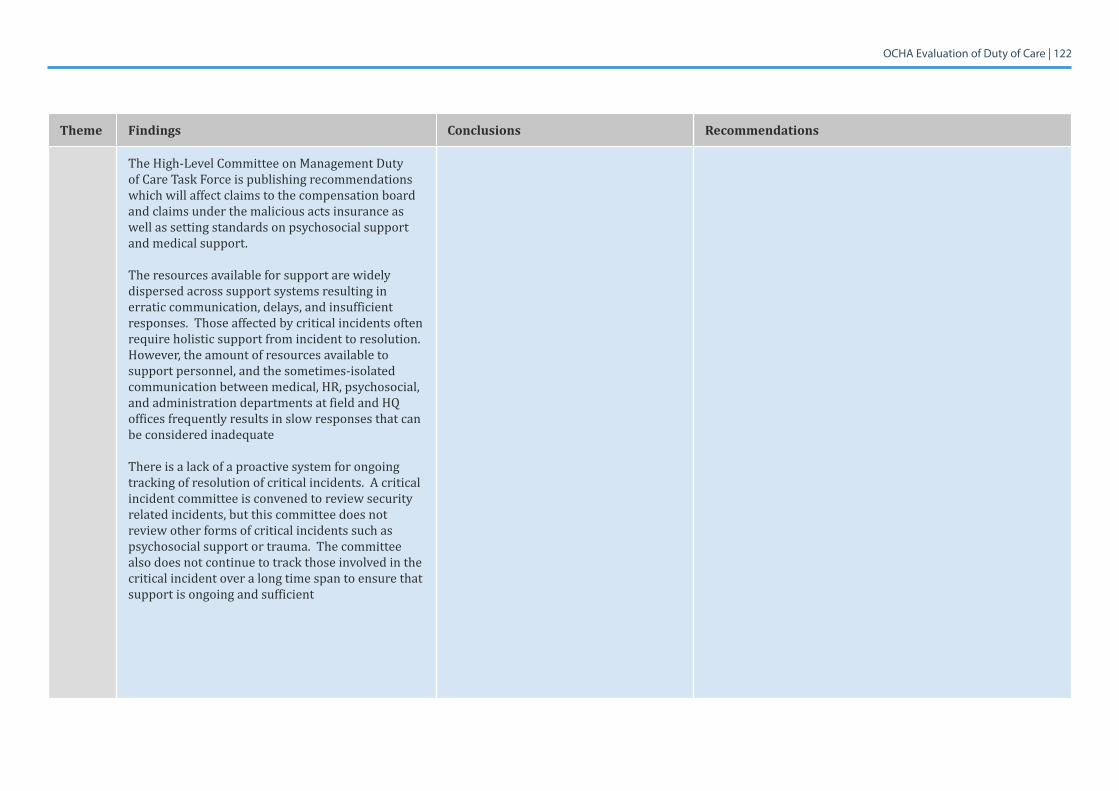
OCHA Evaluation of Duty of Care | 122
Theme Findings Conclusions Recommendations
The High-Level Committee on Management Duty of Care Task Force is publishing recommendations which will affect claims to the compensation board and claims under the malicious acts insurance as well as setting standards on psychosocial support and medical support.
The resources available for support are widely dispersed across support systems resulting in erratic communication, delays, and insufficient responses. Those affected by critical incidents often require holistic support from incident to resolution. However, the amount of resources available to support personnel, and the sometimes-isolated communication between medical, HR, psychosocial, and administration departments at field and HQ offices frequently results in slow responses that can be considered inadequate
There is a lack of a proactive system for ongoing tracking of resolution of critical incidents. A critical incident committee is convened to review security related incidents, but this committee does not review other forms of critical incidents such as psychosocial support or trauma. The committee also does not continue to track those involved in the critical incident over a long time span to ensure that support is ongoing and sufficient
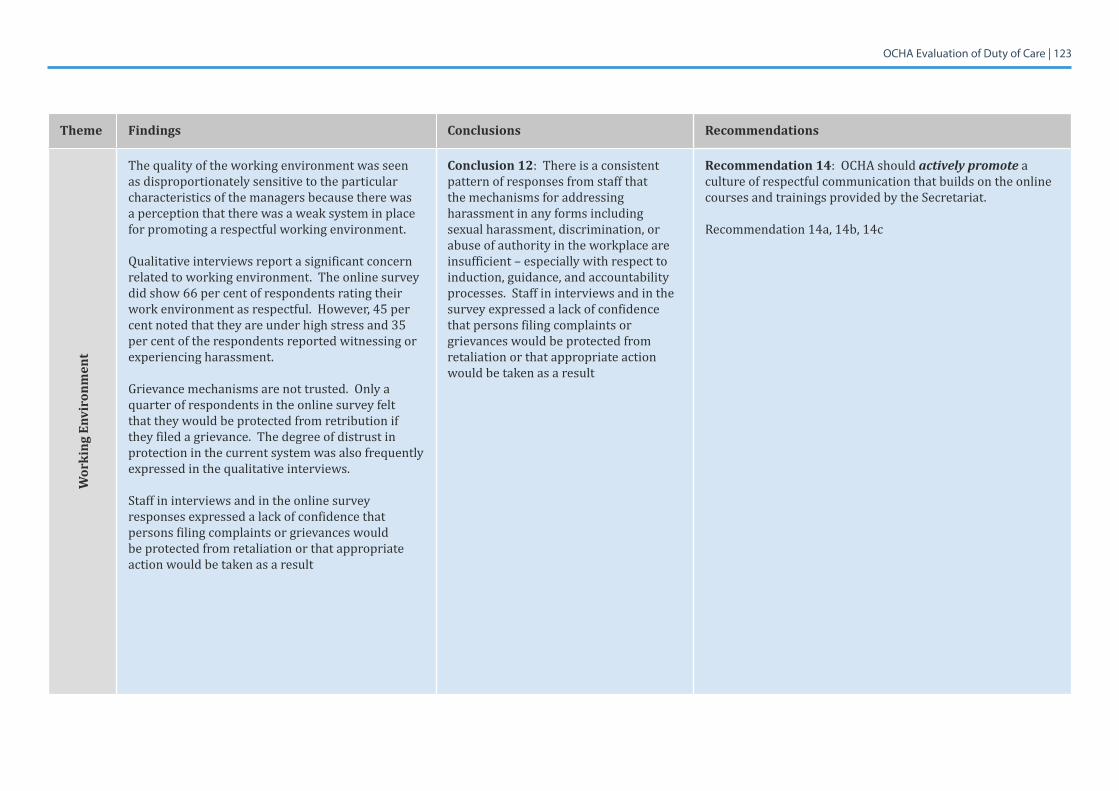
OCHA Evaluation of Duty of Care | 123
Theme Findings Conclusions Recommendations
Wor
king
Env
iron
men
t
The quality of the working environment was seen as disproportionately sensitive to the particular characteristics of the managers because there was a perception that there was a weak system in place for promoting a respectful working environment.
Qualitative interviews report a significant concern related to working environment. The online survey did show 66 per cent of respondents rating their work environment as respectful. However, 45 per cent noted that they are under high stress and 35 per cent of the respondents reported witnessing or experiencing harassment.
Grievance mechanisms are not trusted. Only a quarter of respondents in the online survey felt that they would be protected from retribution if they filed a grievance. The degree of distrust in protection in the current system was also frequently expressed in the qualitative interviews.
Staff in interviews and in the online survey responses expressed a lack of confidence that persons filing complaints or grievances would be protected from retaliation or that appropriate action would be taken as a result
Conclusion 12: There is a consistent pattern of responses from staff that the mechanisms for addressing harassment in any forms including sexual harassment, discrimination, or abuse of authority in the workplace are insufficient – especially with respect to induction, guidance, and accountability processes. Staff in interviews and in the survey expressed a lack of confidence that persons filing complaints or grievances would be protected from retaliation or that appropriate action would be taken as a result
Recommendation 14: OCHA should actively promote a culture of respectful communication that builds on the online courses and trainings provided by the Secretariat.
Recommendation 14a, 14b, 14c
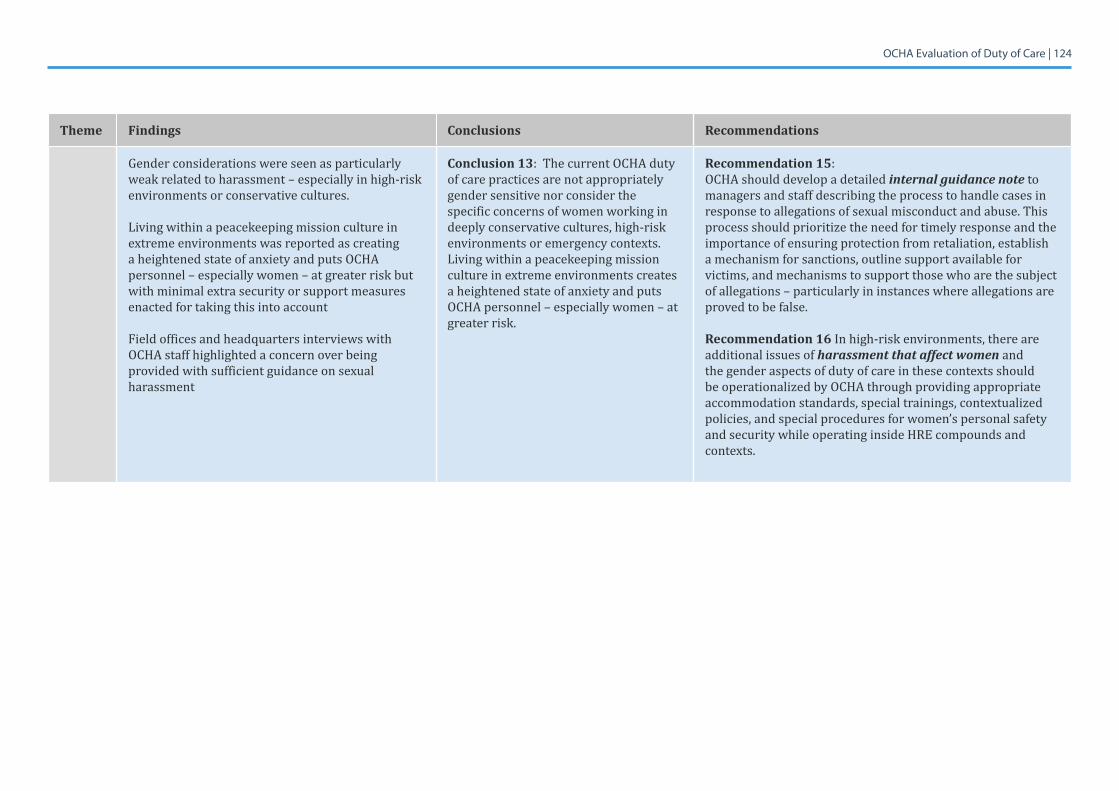
OCHA Evaluation of Duty of Care | 124
Theme Findings Conclusions Recommendations
Gender considerations were seen as particularly weak related to harassment – especially in high-risk environments or conservative cultures.
Living within a peacekeeping mission culture in extreme environments was reported as creating a heightened state of anxiety and puts OCHA personnel – especially women – at greater risk but with minimal extra security or support measures enacted for taking this into account
Field offices and headquarters interviews with OCHA staff highlighted a concern over being provided with sufficient guidance on sexual harassment
Conclusion 13: The current OCHA duty of care practices are not appropriately gender sensitive nor consider the specific concerns of women working in deeply conservative cultures, high-risk environments or emergency contexts. Living within a peacekeeping mission culture in extreme environments creates a heightened state of anxiety and puts OCHA personnel – especially women – at greater risk.
Recommendation 15: OCHA should develop a detailed internal guidance note to managers and staff describing the process to handle cases in response to allegations of sexual misconduct and abuse. This process should prioritize the need for timely response and the importance of ensuring protection from retaliation, establish a mechanism for sanctions, outline support available for victims, and mechanisms to support those who are the subject of allegations – particularly in instances where allegations are proved to be false.
Recommendation 16 In high-risk environments, there are additional issues of harassment that affect women and the gender aspects of duty of care in these contexts should be operationalized by OCHA through providing appropriate accommodation standards, special trainings, contextualized policies, and special procedures for women’s personal safety and security while operating inside HRE compounds and contexts.
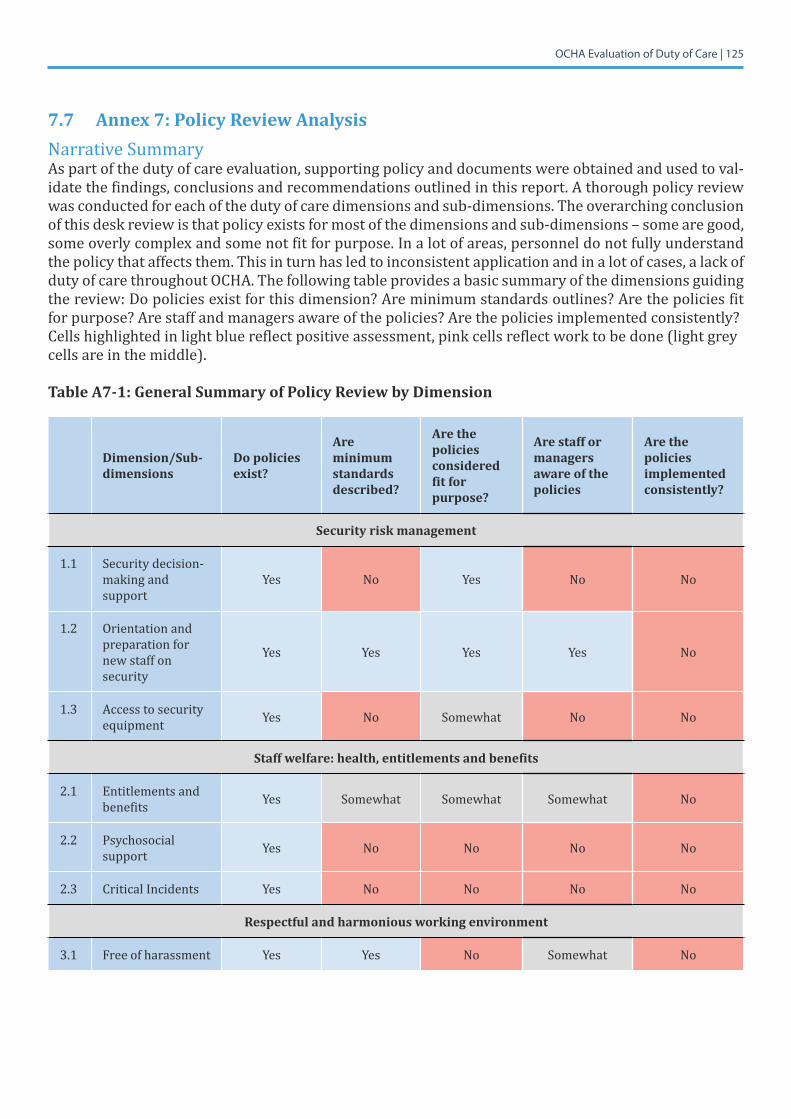
OCHA Evaluation of Duty of Care | 125
7.7 Annex 7: Policy Review AnalysisNarrative SummaryAs part of the duty of care evaluation, supporting policy and documents were obtained and used to val-idate the findings, conclusions and recommendations outlined in this report. A thorough policy review was conducted for each of the duty of care dimensions and sub-dimensions. The overarching conclusion of this desk review is that policy exists for most of the dimensions and sub-dimensions – some are good, some overly complex and some not fit for purpose. In a lot of areas, personnel do not fully understand the policy that affects them. This in turn has led to inconsistent application and in a lot of cases, a lack of duty of care throughout OCHA. The following table provides a basic summary of the dimensions guiding the review: Do policies exist for this dimension? Are minimum standards outlines? Are the policies fit for purpose? Are staff and managers aware of the policies? Are the policies implemented consistently? Cells highlighted in light blue reflect positive assessment, pink cells reflect work to be done (light grey cells are in the middle).
Table A7-1: General Summary of Policy Review by Dimension
Dimension/Sub-dimensions
Do policies exist?
Are minimum standards described?
Are the policies considered fit for purpose?
Are staff or managers aware of the policies
Are the policies implemented consistently?
Security risk management
1.1 Security decision-making and support
Yes No Yes No No
1.2 Orientation and preparation for new staff on security
Yes Yes Yes Yes No
1.3 Access to security equipment Yes No Somewhat No No
Staff welfare: health, entitlements and benefits
2.1 Entitlements and benefits Yes Somewhat Somewhat Somewhat No
2.2 Psychosocial support Yes No No No No
2.3 Critical Incidents Yes No No No No
Respectful and harmonious working environment
3.1 Free of harassment Yes Yes No Somewhat No
OCHA Evaluation of Duty of Care | 126
Duty of care definition
The legal definition for duty of care for the UN, as set out in the UN Staff Rules and Regulations, Article 1:
1.1 (c) The Secretary-General shall ensure that the rights and duties of staff members, as set out in the Charter and the Staff Regulations and Rules and in the relevant resolutions and decisions of the General Assembly, are respected; 1.2 (c) General rights and obligations: Staff members are subject to the authority of the Secretary-General and to assignment by him or her to any of the activities or offices of the United Nations. In exercising this authority, the Secretary-General shall seek to ensure, having regard to the circumstances, that all neces-sary safety and security arrangements are made for staff carrying out the responsibilities entrusted to them.
Dimension 1: Security Risk Management
1.1 Security decision-making & support (including access to security equipment)OCHA has a clear framework, policy and minimum standards in place on safety and security (including access to security equipment), that outlines clear accountabilities and responsibilities. Security man-agement has the strongest policy standards out of all the dimensions studied, but the standard to which they are embedded and understood with staff is inconsistent and below the standard the policy aspires to.
In 2011, OCHA published a landmark study ‘To Stay and Deliver’, which collected and documented hu-manitarian organisation’s good practices in deploying and delivering relief in highly insecure environ-ments and is fully supported by the Secretary-General. The study emphasizes the shift from avoiding risks to managing risks, and demonstrates how the risks to aid workers have increased over the years.
The UNSMS Security Policy, OCHA Policy Instruction on Security and the UN Convention on the Safety and Security of UN Personnel include policy and guidance for field security, managing critical incidents, and the UNDSS Trust Fund helps combat risky behaviours. A security guide also exists for women.
MOSS was discontinued in 2017 and replaced with the Security Risk Management Measures from the SRM process. The oversight process for the new MOSS is being established so no reporting beyond self-reporting of offices is currently available.
An integral part of the Organizational Resilience Management System (ORMS) is Business Continuity Management (BCM) to ensure the continued delivery of defined essential and time-critical business services in a crisis. It is mandatory for duty stations at all levels (HQ, regional, country) to develop and implement a site- and organization-specific BCP framework of procedures, policies, organizational structures and preparedness measures which, in addition to ensuring continuity of critical functions and programmes, accounts for health and safety of staff and dependents and coordination with local authorities, the UN system and key partners.
The BCP does not cover security measures but its annex contains a list of critical staff and provides key information (business processes, mitigation strategies, core documents) on critical functions and ser-vices in the areas of IT, Financing, Security, Common Services, Procurement, and HR. To identify critical functions in a duty station, a Programme Criticality assessment is mandatory in areas with risk levels “very high” and “high”.
OCHA Evaluation of Duty of Care | 127
1.2 Orientation and preparation for new staff on securityThe security advice and support for personnel is standardised in the UN Security Management System, Security Policy Manual, together with training for managers.
The ASG sent a memorandum in 2017 on the United Nations mandatory learning programme, which lists the learning staff and managers must undertake, including basic security in the field, advanced security in the field (for non-HQ duty stations and missions), safe and secure approaches in field envi-ronments (on arrival in duty stations), gender, prevention of workplace harassment, sexual harassment and abuse of authority in the workplace.
The courses where staff are truly monitored are the basic and advanced online security modules, as without these certificates of completion a staff member cannot travel and SSAFE training for those go-ing to high-risk duty stations are mandatory ?. The general induction is a list of resources and online courses available to all staff, which staff self-manage – it is not clear how involved the manager is with the overall induction process. There is also no opportunity for OCHA to collect informed consent when the mode of delivery is online and self-taught modules.
Dimension 2: Staff Welfare: health, entitlements and benefitsThe majority of policy for staff entitlements and benefits is outlined in the UN Staff Regulations and Rules of the United Nations 2017. The pay and entitlement provisions have clear policy and guidelines. The areas in this dimension that warrant particular attention are:
AccommodationThere are guidelines on occupational standards but the evaluation team were unable to locate specific rules on standards for living quarters. Reports from UNSOM and OIOS have both made the development of a comprehensive accommodation master plan a key recommendation.
Medical provisionMedical policy plans with minimum standards exist for international and national staff, overseen and managed by UN Medical Services. However, these standards are not consistently adhered to in the field. National staff have lower standards and this is more apparent with critical illness and medevacs. The contract with the health insurance provider also requires immediate attention and better management.
Mobility & rotationThe UN Staff Rules and Regulations states that the purpose of staff selection and mobility management is to promote greater movement and rotation between headquarters and regional commissions. The field mobility scheme in OCHA is no longer in use. There is no current practice or standard which pro-vides for mobility and rotation leading to staff working in highly stressful environments for prolonged periods of time, leading to sickness, burn out and a demotivated work force and high staff turnover.
Danger payPolicy exists for both international and national staff. International staff receive $1,600/month. Nation-al staff receive 30 per cent of a mid-point salary.
Psychosocial supportThe evaluation team could not locate a policy on psychosocial support. There are several guides and booklets on stress management and ‘burn out’ but no policies or standards. This sub-dimension is of critical concern. The UN Mental Health Strategic Plan outlines a collaborative system-wide response to the mental health and wellbeing needs of staff. It is unclear when this will be implemented and be able to have a profound impact on OCHA staff.
OCHA Evaluation of Duty of Care | 128
The UNSMS Security Policy Manual provides a policy for critical incidents and the Critical Incident Stress Management Unit serves as the central body for managing critical incidents and ensuring the provision of psycho-social services in the event of a critical incident, in accordance with the principles of imme-diacy, proximity and availability of high quality professional services. The evaluation team interviewed cases where the care and support given to affected individuals was well below this standard.
Managers require more discretion with leave management. The complexities of the different leave poli-cies can adversely impact each other e.g. sick leave can impact R&R qualification.
The data OCHA keeps on critical incidents could be vastly improved. The information the evaluation team obtained could not be used to help review practices and implement preventative measures for the future. It is recommended that more data is collected on gender, category of staff and type of incident. A new Security Incident Information Management Handbook has just been developed for the sector by RedR UK and EISF and can be obtained from their respective websites free of charge.
Temporary contracts (TJOs)Policy exists for the use of TJOs but it is often abused in terms of length of service. The number of TJOs working in higher risk environments on less benefits than their fixed-term counterparts is high.
Respectful and harmonious working environment
Free from harassmentPolicy exists that outlines the UN’s stance on harassment, and a helpline for sexual harassment com-plaintshasbeenrecentlyputinplacefollowingtheSG’sbulletininFebruary2018.Staffaremeanttoattend mandatory inductions on this issue, however, on the whole, staff are left to familiarise themselves with this sensitive topic. Reporting mechanisms exist however according to our findings and to OIOS, who are qualified to investigate these concerns, they are not trusted. It is also not clear how a victim would be supported with a claim, psychologically and practically; a very critical duty of care issue.
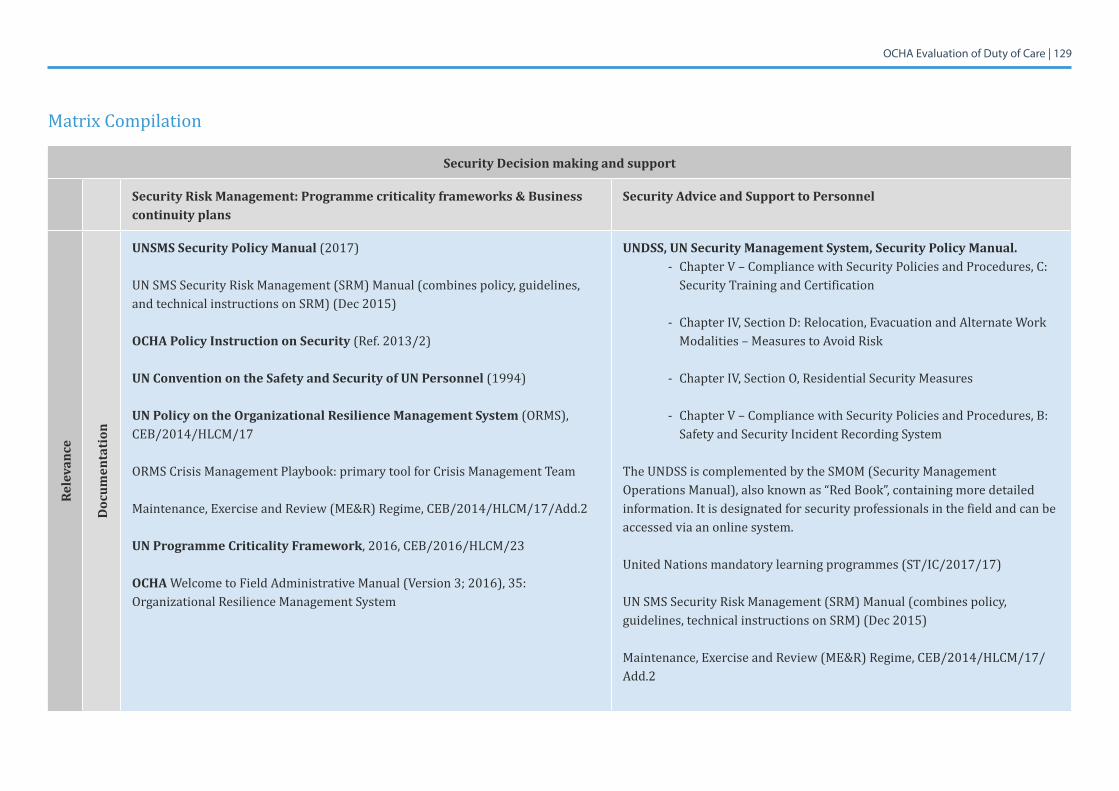
OCHA Evaluation of Duty of Care | 129
Matrix Compilation
Security Decision making and support
Security Risk Management: Programme criticality frameworks & Business continuity plans
Security Advice and Support to Personnel
Rele
vanc
e
Doc
umen
tati
on
UNSMS Security Policy Manual (2017)
UN SMS Security Risk Management (SRM) Manual (combines policy, guidelines, and technical instructions on SRM) (Dec 2015)
OCHA Policy Instruction on Security (Ref. 2013/2)
UN Convention on the Safety and Security of UN Personnel (1994)
UN Policy on the Organizational Resilience Management System (ORMS), CEB/2014/HLCM/17
ORMS Crisis Management Playbook: primary tool for Crisis Management Team
Maintenance, Exercise and Review (ME&R) Regime, CEB/2014/HLCM/17/Add.2
UN Programme Criticality Framework, 2016, CEB/2016/HLCM/23
OCHA WelcometoFieldAdministrativeManual(Version3;2016),35:Organizational Resilience Management System
UNDSS, UN Security Management System, Security Policy Manual. - ChapterV–CompliancewithSecurityPoliciesandProcedures,C:
Security Training and Certification
- ChapterIV,SectionD:Relocation,EvacuationandAlternateWorkModalities – Measures to Avoid Risk
- ChapterIV,SectionO,ResidentialSecurityMeasures
- ChapterV–CompliancewithSecurityPoliciesandProcedures,B:Safety and Security Incident Recording System
The UNDSS is complemented by the SMOM (Security Management Operations Manual), also known as “Red Book”, containing more detailed information. It is designated for security professionals in the field and can be accessed via an online system.
United Nations mandatory learning programmes (ST/IC/2017/17)
UN SMS Security Risk Management (SRM) Manual (combines policy, guidelines, technical instructions on SRM) (Dec 2015)
Maintenance, Exercise and Review (ME&R) Regime, CEB/2014/HLCM/17/Add.2
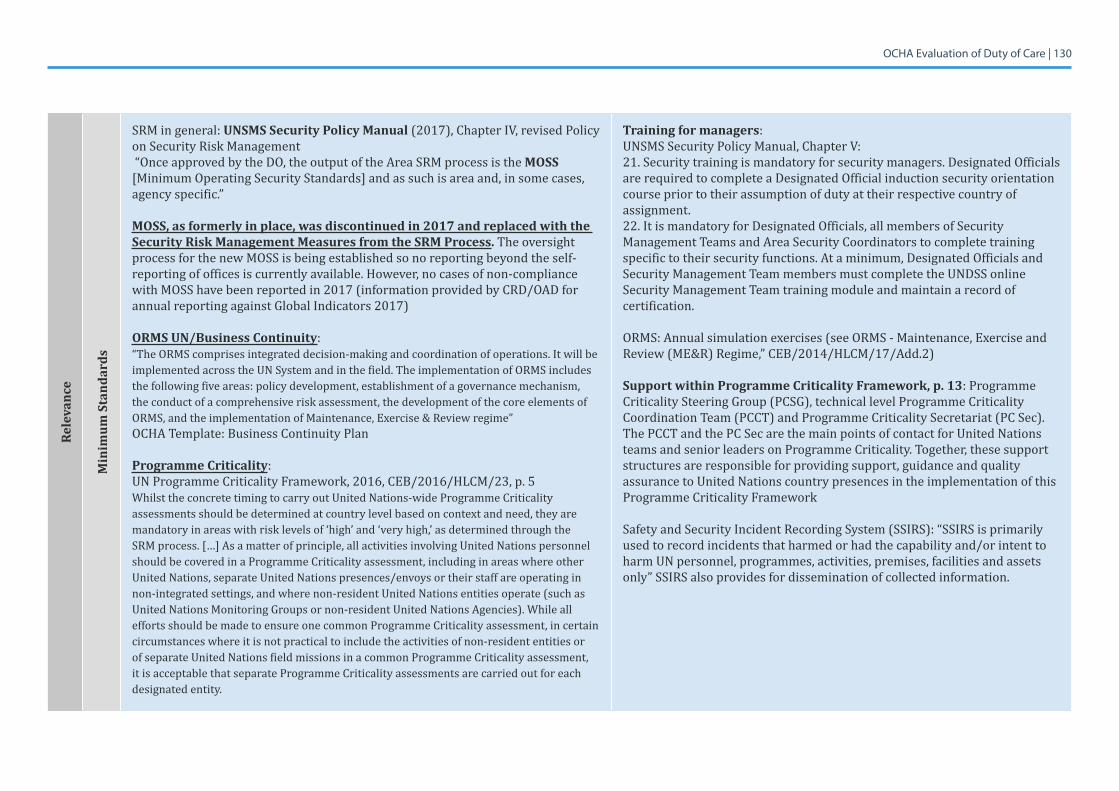
OCHA Evaluation of Duty of Care | 130Re
leva
nce
Min
imum
Sta
ndar
ds
SRM in general: UNSMS Security Policy Manual (2017),ChapterIV,revisedPolicyon Security Risk Management “Once approved by the DO, the output of the Area SRM process is the MOSS [Minimum Operating Security Standards] and as such is area and, in some cases, agency specific.”
MOSS, as formerly in place, was discontinued in 2017 and replaced with the Security Risk Management Measures from the SRM Process. The oversight process for the new MOSS is being established so no reporting beyond the self-reporting of offices is currently available. However, no cases of non-compliance with MOSS have been reported in 2017 (information provided by CRD/OAD for annual reporting against Global Indicators 2017)
ORMS UN/Business Continuity:“The ORMS comprises integrated decision-making and coordination of operations. It will be implemented across the UN System and in the field. The implementation of ORMS includes the following five areas: policy development, establishment of a governance mechanism, the conduct of a comprehensive risk assessment, the development of the core elements of ORMS, and the implementation of Maintenance, Exercise & Review regime” OCHA Template: Business Continuity Plan
Programme Criticality:UN Programme Criticality Framework, 2016, CEB/2016/HLCM/23, p. 5WhilsttheconcretetimingtocarryoutUnitedNations-wideProgrammeCriticalityassessments should be determined at country level based on context and need, they are mandatory in areas with risk levels of ‘high’ and ‘very high,’ as determined through the SRM process. […] As a matter of principle, all activities involving United Nations personnel should be covered in a Programme Criticality assessment, including in areas where other United Nations, separate United Nations presences/envoys or their staff are operating in non-integrated settings, and where non-resident United Nations entities operate (such as UnitedNationsMonitoringGroupsornon-residentUnitedNationsAgencies).Whileallefforts should be made to ensure one common Programme Criticality assessment, in certain circumstances where it is not practical to include the activities of non-resident entities or of separate United Nations field missions in a common Programme Criticality assessment, it is acceptable that separate Programme Criticality assessments are carried out for each designated entity.
Training for managers:UNSMSSecurityPolicyManual,ChapterV:21. Security training is mandatory for security managers. Designated Officials are required to complete a Designated Official induction security orientation course prior to their assumption of duty at their respective country of assignment. 22. It is mandatory for Designated Officials, all members of Security Management Teams and Area Security Coordinators to complete training specific to their security functions. At a minimum, Designated Officials and Security Management Team members must complete the UNDSS online Security Management Team training module and maintain a record of certification.
ORMS: Annual simulation exercises (see ORMS - Maintenance, Exercise and Review (ME&R) Regime,” CEB/2014/HLCM/17/Add.2)
Support within Programme Criticality Framework, p. 13: Programme Criticality Steering Group (PCSG), technical level Programme Criticality Coordination Team (PCCT) and Programme Criticality Secretariat (PC Sec). The PCCT and the PC Sec are the main points of contact for United Nations teams and senior leaders on Programme Criticality. Together, these support structures are responsible for providing support, guidance and quality assurance to United Nations country presences in the implementation of this Programme Criticality Framework
Safety and Security Incident Recording System (SSIRS): “SSIRS is primarily used to record incidents that harmed or had the capability and/or intent to harm UN personnel, programmes, activities, premises, facilities and assets only” SSIRS also provides for dissemination of collected information.
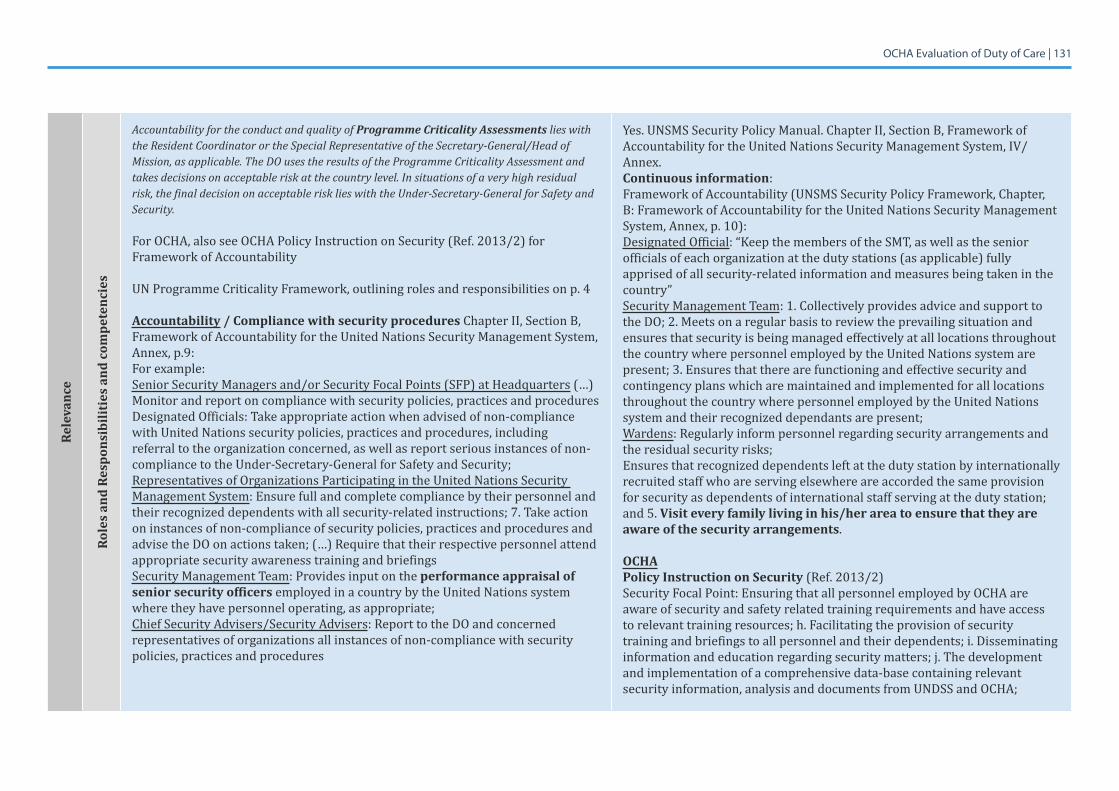
OCHA Evaluation of Duty of Care | 131Re
leva
nce
Role
s an
d Re
spon
sibi
litie
s an
d co
mpe
tenc
ies
Accountability for the conduct and quality of Programme Criticality Assessments lies with the Resident Coordinator or the Special Representative of the Secretary-General/Head of Mission, as applicable. The DO uses the results of the Programme Criticality Assessment and takes decisions on acceptable risk at the country level. In situations of a very high residual risk, the final decision on acceptable risk lies with the Under-Secretary-General for Safety and Security.
For OCHA, also see OCHA Policy Instruction on Security (Ref. 2013/2) for Framework of Accountability
UN Programme Criticality Framework, outlining roles and responsibilities on p. 4
Accountability / Compliance with security procedures Chapter II, Section B, Framework of Accountability for the United Nations Security Management System, Annex, p.9:For example:Senior Security Managers and/or Security Focal Points (SFP) at Headquarters (…) Monitor and report on compliance with security policies, practices and procedures Designated Officials: Take appropriate action when advised of non-compliance with United Nations security policies, practices and procedures, including referral to the organization concerned, as well as report serious instances of non-compliance to the Under-Secretary-General for Safety and Security;Representatives of Organizations Participating in the United Nations Security Management System: Ensure full and complete compliance by their personnel and their recognized dependents with all security-related instructions; 7. Take action on instances of non-compliance of security policies, practices and procedures and advise the DO on actions taken; (…) Require that their respective personnel attend appropriate security awareness training and briefingsSecurity Management Team: Provides input on the performance appraisal of senior security officers employed in a country by the United Nations system where they have personnel operating, as appropriate;Chief Security Advisers/Security Advisers: Report to the DO and concerned representatives of organizations all instances of non-compliance with security policies, practices and procedures
Yes. UNSMS Security Policy Manual. Chapter II, Section B, Framework of AccountabilityfortheUnitedNationsSecurityManagementSystem,IV/Annex.Continuous information: Framework of Accountability (UNSMS Security Policy Framework, Chapter, B: Framework of Accountability for the United Nations Security Management System, Annex, p. 10): Designated Official: “Keep the members of the SMT, as well as the senior officials of each organization at the duty stations (as applicable) fully apprised of all security-related information and measures being taken in the country”Security Management Team: 1. Collectively provides advice and support to the DO; 2. Meets on a regular basis to review the prevailing situation and ensures that security is being managed effectively at all locations throughout the country where personnel employed by the United Nations system are present; 3. Ensures that there are functioning and effective security and contingency plans which are maintained and implemented for all locations throughout the country where personnel employed by the United Nations system and their recognized dependants are present; Wardens: Regularly inform personnel regarding security arrangements and the residual security risks; Ensures that recognized dependents left at the duty station by internationally recruited staff who are serving elsewhere are accorded the same provision for security as dependents of international staff serving at the duty station; and 5. Visit every family living in his/her area to ensure that they are aware of the security arrangements.
OCHA Policy Instruction on Security (Ref. 2013/2)Security Focal Point: Ensuring that all personnel employed by OCHA are aware of security and safety related training requirements and have access to relevant training resources; h. Facilitating the provision of security training and briefings to all personnel and their dependents; i. Disseminating information and education regarding security matters; j. The development and implementation of a comprehensive data-base containing relevant security information, analysis and documents from UNDSS and OCHA;
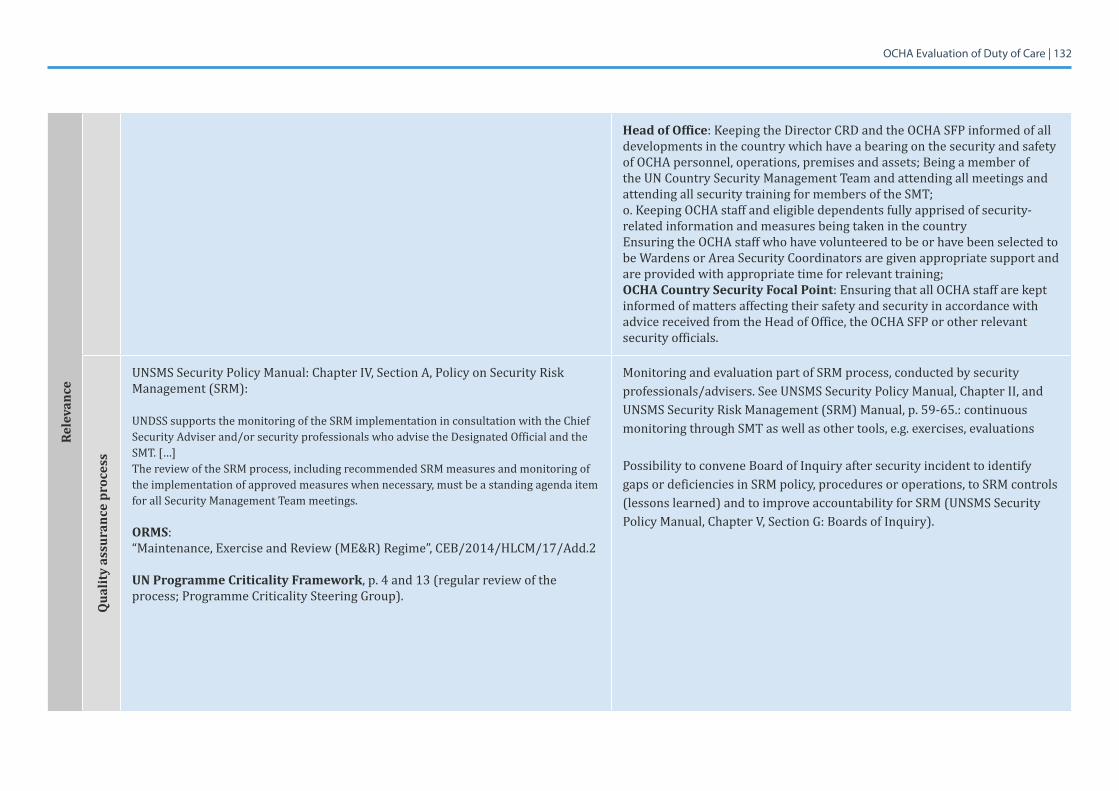
OCHA Evaluation of Duty of Care | 132Re
leva
nce
Head of Office: Keeping the Director CRD and the OCHA SFP informed of all developments in the country which have a bearing on the security and safety of OCHA personnel, operations, premises and assets; Being a member of the UN Country Security Management Team and attending all meetings and attending all security training for members of the SMT;o. Keeping OCHA staff and eligible dependents fully apprised of security-related information and measures being taken in the countryEnsuring the OCHA staff who have volunteered to be or have been selected to beWardensorAreaSecurityCoordinatorsaregivenappropriatesupportandare provided with appropriate time for relevant training;OCHA Country Security Focal Point: Ensuring that all OCHA staff are kept informed of matters affecting their safety and security in accordance with advice received from the Head of Office, the OCHA SFP or other relevant security officials.
Qua
lity
assu
ranc
e pr
oces
s
UNSMSSecurityPolicyManual:ChapterIV,SectionA,PolicyonSecurityRiskManagement (SRM):
UNDSS supports the monitoring of the SRM implementation in consultation with the Chief Security Adviser and/or security professionals who advise the Designated Official and the SMT. […]The review of the SRM process, including recommended SRM measures and monitoring of the implementation of approved measures when necessary, must be a standing agenda item for all Security Management Team meetings.
ORMS: “Maintenance, Exercise and Review (ME&R) Regime”, CEB/2014/HLCM/17/Add.2
UN Programme Criticality Framework, p. 4 and 13 (regular review of the process; Programme Criticality Steering Group).
Monitoring and evaluation part of SRM process, conducted by security professionals/advisers. See UNSMS Security Policy Manual, Chapter II, and UNSMS Security Risk Management (SRM) Manual, p. 59-65.: continuous monitoring through SMT as well as other tools, e.g. exercises, evaluations
Possibility to convene Board of Inquiry after security incident to identify gaps or deficiencies in SRM policy, procedures or operations, to SRM controls (lessons learned) and to improve accountability for SRM (UNSMS Security PolicyManual,ChapterV,SectionG:BoardsofInquiry).
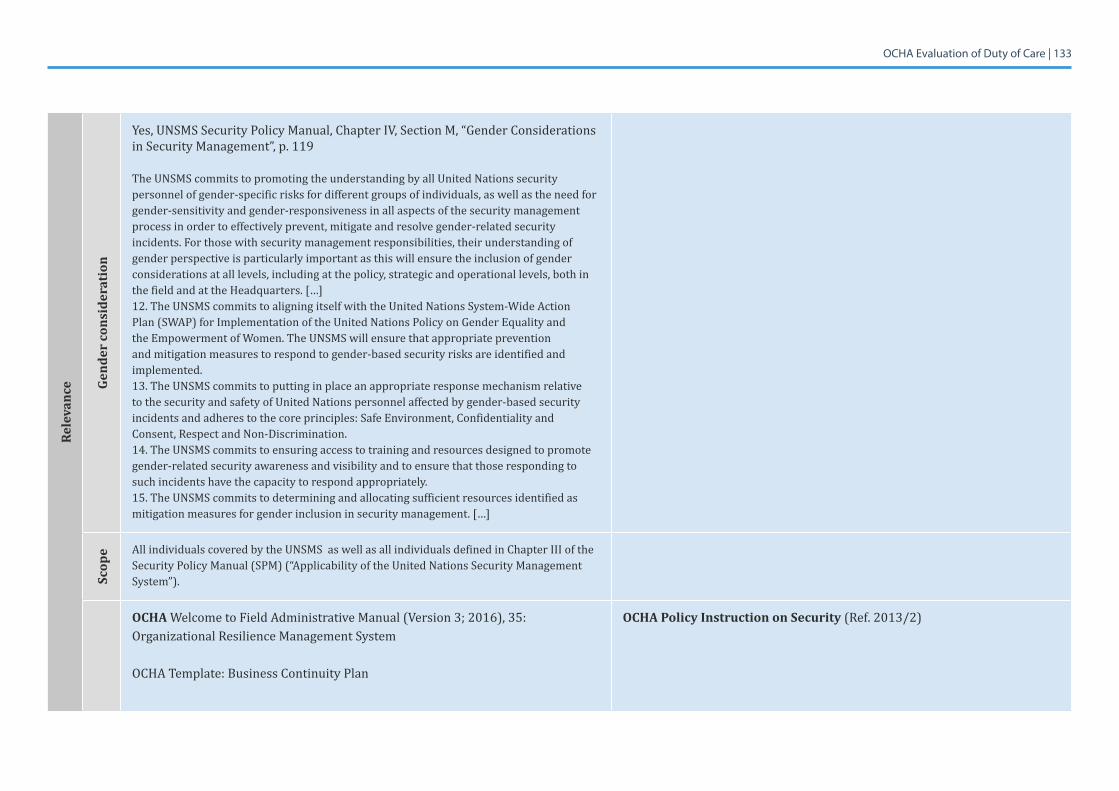
OCHA Evaluation of Duty of Care | 133Re
leva
nce Ge
nder
con
side
rati
on
Yes,UNSMSSecurityPolicyManual,ChapterIV,SectionM,“GenderConsiderationsin Security Management”, p. 119
The UNSMS commits to promoting the understanding by all United Nations security personnel of gender-specific risks for different groups of individuals, as well as the need for gender-sensitivity and gender-responsiveness in all aspects of the security management process in order to effectively prevent, mitigate and resolve gender-related security incidents. For those with security management responsibilities, their understanding of gender perspective is particularly important as this will ensure the inclusion of gender considerations at all levels, including at the policy, strategic and operational levels, both in the field and at the Headquarters. […]12.TheUNSMScommitstoaligningitselfwiththeUnitedNationsSystem-WideActionPlan(SWAP)forImplementationoftheUnitedNationsPolicyonGenderEqualityandtheEmpowermentofWomen.TheUNSMSwillensurethatappropriatepreventionand mitigation measures to respond to gender-based security risks are identified and implemented. 13. The UNSMS commits to putting in place an appropriate response mechanism relative to the security and safety of United Nations personnel affected by gender-based security incidents and adheres to the core principles: Safe Environment, Confidentiality and Consent, Respect and Non-Discrimination. 14. The UNSMS commits to ensuring access to training and resources designed to promote gender-related security awareness and visibility and to ensure that those responding to such incidents have the capacity to respond appropriately. 15. The UNSMS commits to determining and allocating sufficient resources identified as mitigation measures for gender inclusion in security management. […]
Scop
e All individuals covered by the UNSMS as well as all individuals defined in Chapter III of the Security Policy Manual (SPM) (“Applicability of the United Nations Security Management System”).
OCHA WelcometoFieldAdministrativeManual(Version3;2016),35:Organizational Resilience Management System
OCHA Template: Business Continuity Plan
OCHA Policy Instruction on Security (Ref. 2013/2)
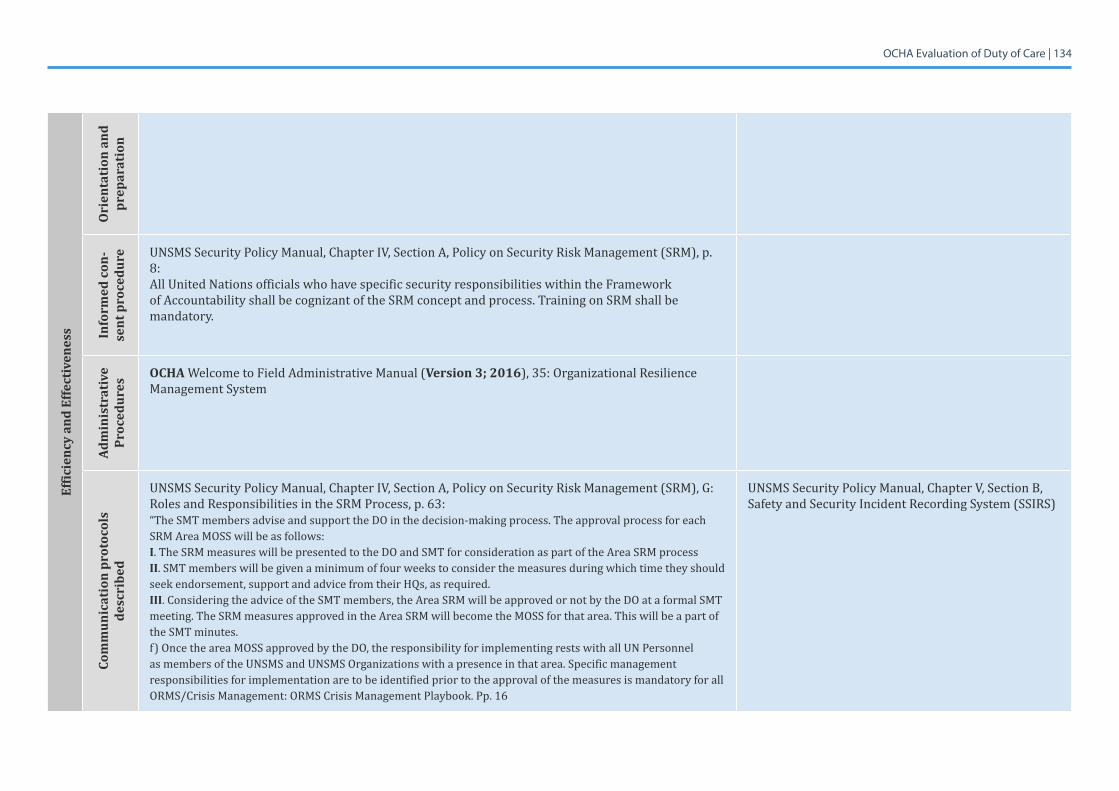
OCHA Evaluation of Duty of Care | 134Ef
ficie
ncy
and
Effe
ctiv
enes
s
Ori
enta
tion
and
pr
epar
atio
n In
form
ed c
on-
sent
pro
cedu
re UNSMSSecurityPolicyManual,ChapterIV,SectionA,PolicyonSecurityRiskManagement(SRM),p.8:All United Nations officials who have specific security responsibilities within the Framework of Accountability shall be cognizant of the SRM concept and process. Training on SRM shall be mandatory.
Adm
inis
trat
ive
Proc
edur
es
OCHAWelcometoFieldAdministrativeManual(Version 3; 2016), 35: Organizational Resilience Management System
Com
mun
icat
ion
prot
ocol
s de
scri
bed
UNSMSSecurityPolicyManual,ChapterIV,SectionA,PolicyonSecurityRiskManagement(SRM),G:Roles and Responsibilities in the SRM Process, p. 63:“The SMT members advise and support the DO in the decision-making process. The approval process for each SRM Area MOSS will be as follows: I. The SRM measures will be presented to the DO and SMT for consideration as part of the Area SRM process II. SMT members will be given a minimum of four weeks to consider the measures during which time they should seek endorsement, support and advice from their HQs, as required. III. Considering the advice of the SMT members, the Area SRM will be approved or not by the DO at a formal SMT meeting. The SRM measures approved in the Area SRM will become the MOSS for that area. This will be a part of the SMT minutes. f) Once the area MOSS approved by the DO, the responsibility for implementing rests with all UN Personnel as members of the UNSMS and UNSMS Organizations with a presence in that area. Specific management responsibilities for implementation are to be identified prior to the approval of the measures is mandatory for all ORMS/Crisis Management: ORMS Crisis Management Playbook. Pp. 16
UNSMSSecurityPolicyManual,ChapterV,SectionB,Safety and Security Incident Recording System (SSIRS)
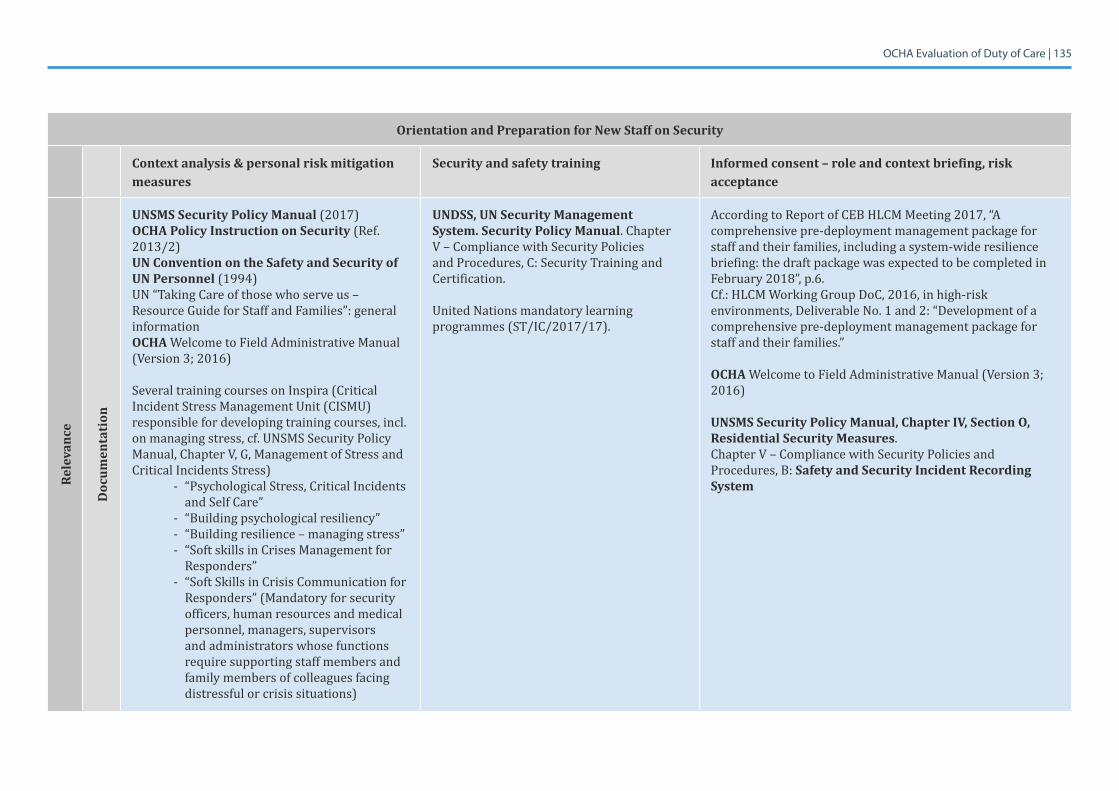
OCHA Evaluation of Duty of Care | 135
Orientation and Preparation for New Staff on Security
Context analysis & personal risk mitigation measures
Security and safety training Informed consent – role and context briefing, risk acceptance
Rele
vanc
e
Doc
umen
tati
on
UNSMS Security Policy Manual (2017)OCHA Policy Instruction on Security (Ref. 2013/2)UN Convention on the Safety and Security of UN Personnel (1994)UN “Taking Care of those who serve us – Resource Guide for Staff and Families”: general informationOCHAWelcometoFieldAdministrativeManual(Version3;2016)
Several training courses on Inspira (Critical Incident Stress Management Unit (CISMU) responsible for developing training courses, incl. on managing stress, cf. UNSMS Security Policy Manual,ChapterV,G,ManagementofStressandCritical Incidents Stress)
- “Psychological Stress, Critical Incidents and Self Care”
- “Building psychological resiliency”- “Building resilience – managing stress”- “Soft skills in Crises Management for
Responders” - “Soft Skills in Crisis Communication for
Responders” (Mandatory for security officers, human resources and medical personnel, managers, supervisors and administrators whose functions require supporting staff members and family members of colleagues facing distressful or crisis situations)
UNDSS, UN Security Management System. Security Policy Manual. Chapter V–CompliancewithSecurityPoliciesand Procedures, C: Security Training and Certification.
United Nations mandatory learning programmes (ST/IC/2017/17).
According to Report of CEB HLCM Meeting 2017, “A comprehensive pre-deployment management package for staff and their families, including a system-wide resilience briefing: the draft package was expected to be completed in February2018”,p.6.Cf.:HLCMWorkingGroupDoC,2016,inhigh-riskenvironments, Deliverable No. 1 and 2: “Development of a comprehensive pre-deployment management package for staff and their families.”
OCHAWelcometoFieldAdministrativeManual(Version3;2016)
UNSMS Security Policy Manual, Chapter IV, Section O, Residential Security Measures.ChapterV–CompliancewithSecurityPoliciesandProcedures, B: Safety and Security Incident Recording System
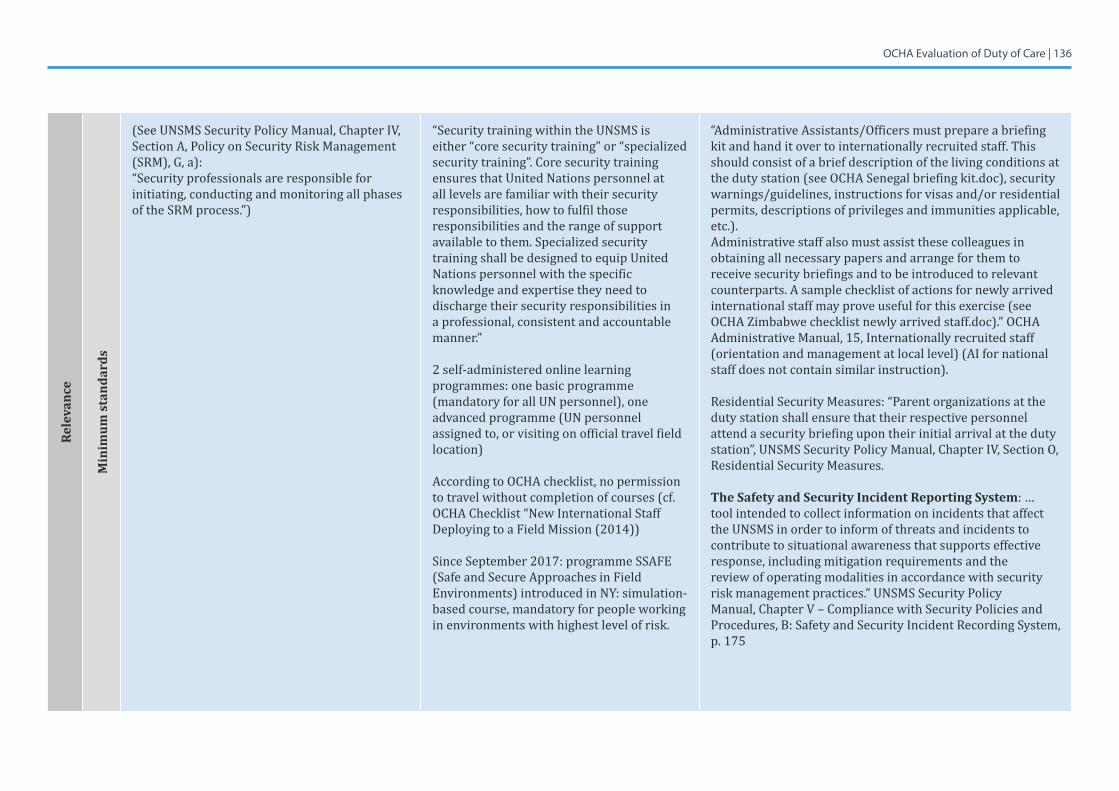
OCHA Evaluation of Duty of Care | 136Re
leva
nce
Min
imum
sta
ndar
ds
(SeeUNSMSSecurityPolicyManual,ChapterIV,Section A, Policy on Security Risk Management (SRM), G, a):“Security professionals are responsible for initiating, conducting and monitoring all phases of the SRM process.”)
“Security training within the UNSMS is either “core security training” or “specialized security training”. Core security training ensures that United Nations personnel at all levels are familiar with their security responsibilities, how to fulfil those responsibilities and the range of support available to them. Specialized security training shall be designed to equip United Nations personnel with the specific knowledge and expertise they need to discharge their security responsibilities in a professional, consistent and accountable manner.”
2 self-administered online learning programmes: one basic programme (mandatory for all UN personnel), one advanced programme (UN personnel assigned to, or visiting on official travel field location)
According to OCHA checklist, no permission to travel without completion of courses (cf. OCHA Checklist “New International Staff Deploying to a Field Mission (2014))
Since September 2017: programme SSAFE (Safe and Secure Approaches in Field Environments) introduced in NY: simulation-based course, mandatory for people working in environments with highest level of risk.
“Administrative Assistants/Officers must prepare a briefing kit and hand it over to internationally recruited staff. This should consist of a brief description of the living conditions at the duty station (see OCHA Senegal briefing kit.doc), security warnings/guidelines, instructions for visas and/or residential permits, descriptions of privileges and immunities applicable, etc.). Administrative staff also must assist these colleagues in obtaining all necessary papers and arrange for them to receive security briefings and to be introduced to relevant counterparts. A sample checklist of actions for newly arrived international staff may prove useful for this exercise (see OCHA Zimbabwe checklist newly arrived staff.doc).” OCHA Administrative Manual, 15, Internationally recruited staff (orientation and management at local level) (AI for national staff does not contain similar instruction).
Residential Security Measures: “Parent organizations at the duty station shall ensure that their respective personnel attend a security briefing upon their initial arrival at the duty station”,UNSMSSecurityPolicyManual,ChapterIV,SectionO,Residential Security Measures.
The Safety and Security Incident Reporting System: … tool intended to collect information on incidents that affect the UNSMS in order to inform of threats and incidents to contribute to situational awareness that supports effective response, including mitigation requirements and the review of operating modalities in accordance with security risk management practices.” UNSMS Security Policy Manual,ChapterV–CompliancewithSecurityPoliciesandProcedures, B: Safety and Security Incident Recording System, p. 175
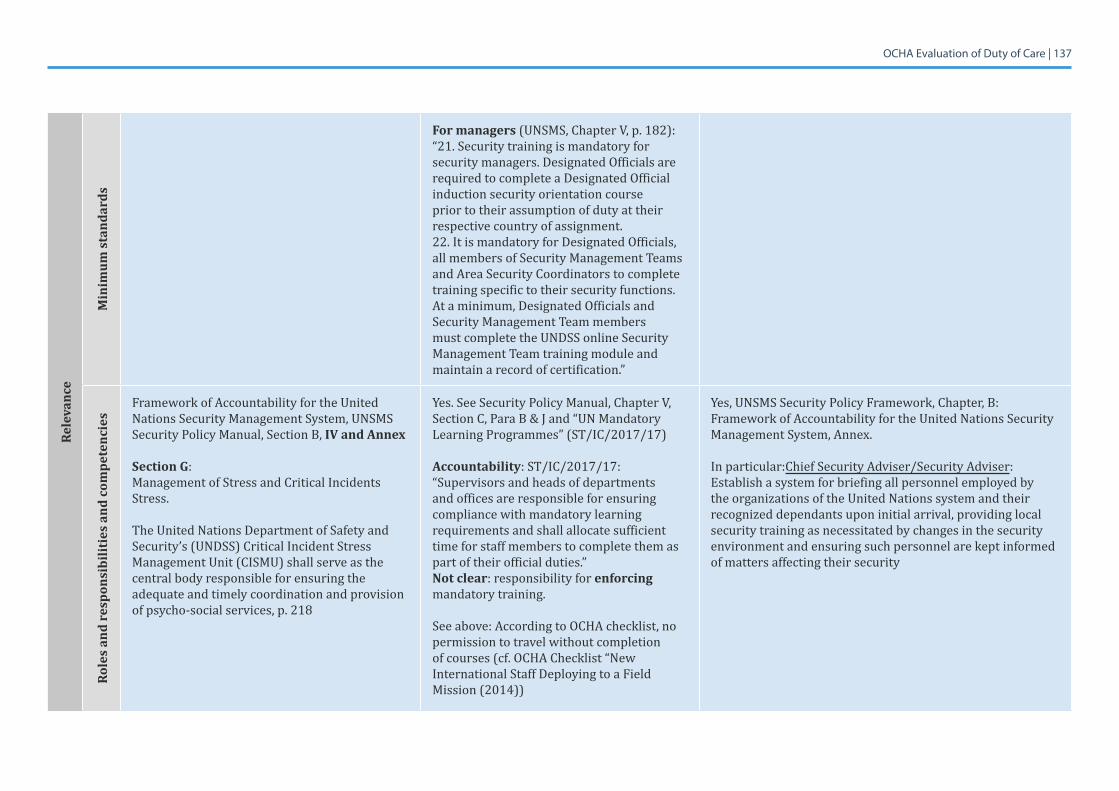
OCHA Evaluation of Duty of Care | 137Re
leva
nce
Min
imum
sta
ndar
ds
For managers (UNSMS,ChapterV,p.182):“21. Security training is mandatory for security managers. Designated Officials are required to complete a Designated Official induction security orientation course prior to their assumption of duty at their respective country of assignment. 22. It is mandatory for Designated Officials, all members of Security Management Teams and Area Security Coordinators to complete training specific to their security functions. At a minimum, Designated Officials and Security Management Team members must complete the UNDSS online Security Management Team training module and maintain a record of certification.”
Role
s an
d re
spon
sibi
litie
s an
d co
mpe
tenc
ies
Framework of Accountability for the United Nations Security Management System, UNSMS Security Policy Manual, Section B, IV and Annex
Section G: Management of Stress and Critical Incidents Stress.
The United Nations Department of Safety and Security’s (UNDSS) Critical Incident Stress Management Unit (CISMU) shall serve as the central body responsible for ensuring the adequate and timely coordination and provision ofpsycho-socialservices,p.218
Yes.SeeSecurityPolicyManual,ChapterV,Section C, Para B & J and “UN Mandatory Learning Programmes” (ST/IC/2017/17)
Accountability: ST/IC/2017/17: “Supervisors and heads of departments and offices are responsible for ensuring compliance with mandatory learning requirements and shall allocate sufficient time for staff members to complete them as part of their official duties.”Not clear: responsibility for enforcing mandatory training.
See above: According to OCHA checklist, no permission to travel without completion of courses (cf. OCHA Checklist “New International Staff Deploying to a Field Mission (2014))
Yes, UNSMS Security Policy Framework, Chapter, B: Framework of Accountability for the United Nations Security Management System, Annex.
In particular:Chief Security Adviser/Security Adviser: Establish a system for briefing all personnel employed by the organizations of the United Nations system and their recognized dependants upon initial arrival, providing local security training as necessitated by changes in the security environment and ensuring such personnel are kept informed of matters affecting their security
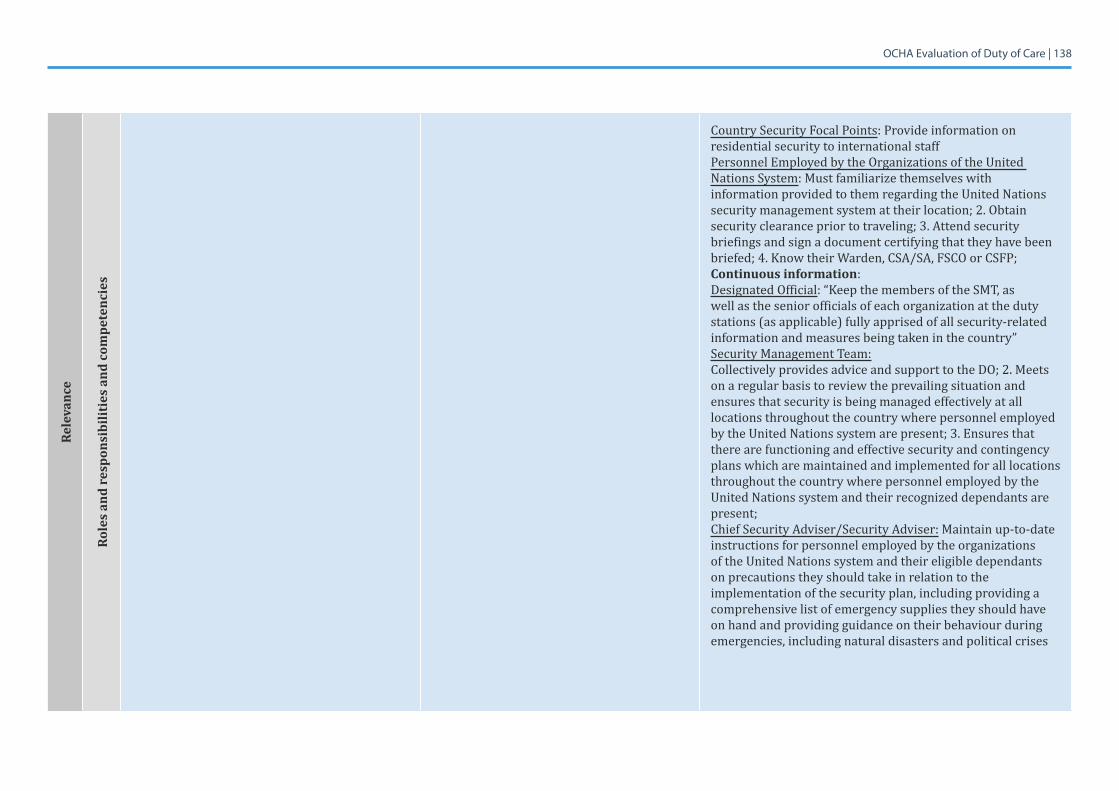
OCHA Evaluation of Duty of Care | 138Re
leva
nce
Role
s an
d re
spon
sibi
litie
s an
d co
mpe
tenc
ies
Country Security Focal Points: Provide information on residential security to international staff Personnel Employed by the Organizations of the United Nations System: Must familiarize themselves with information provided to them regarding the United Nations security management system at their location; 2. Obtain security clearance prior to traveling; 3. Attend security briefings and sign a document certifying that they have been briefed;4.KnowtheirWarden,CSA/SA,FSCOorCSFP;Continuous information:Designated Official: “Keep the members of the SMT, as well as the senior officials of each organization at the duty stations (as applicable) fully apprised of all security-related information and measures being taken in the country”Security Management Team: Collectively provides advice and support to the DO; 2. Meets on a regular basis to review the prevailing situation and ensures that security is being managed effectively at all locations throughout the country where personnel employed by the United Nations system are present; 3. Ensures that there are functioning and effective security and contingency plans which are maintained and implemented for all locations throughout the country where personnel employed by the United Nations system and their recognized dependants are present; Chief Security Adviser/Security Adviser: Maintain up-to-date instructions for personnel employed by the organizations of the United Nations system and their eligible dependants on precautions they should take in relation to the implementation of the security plan, including providing a comprehensive list of emergency supplies they should have on hand and providing guidance on their behaviour during emergencies, including natural disasters and political crises
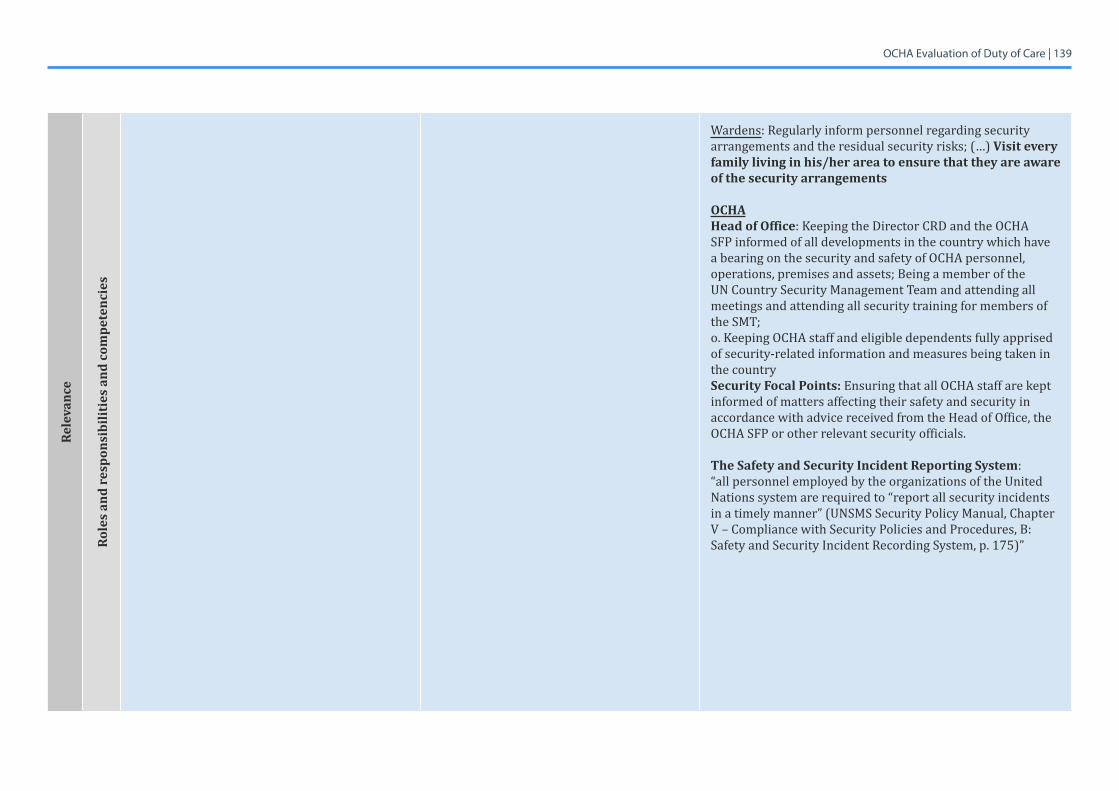
OCHA Evaluation of Duty of Care | 139Re
leva
nce
Role
s an
d re
spon
sibi
litie
s an
d co
mpe
tenc
ies
Wardens: Regularly inform personnel regarding security arrangements and the residual security risks; (…) Visit every family living in his/her area to ensure that they are aware of the security arrangements
OCHAHead of Office: Keeping the Director CRD and the OCHA SFP informed of all developments in the country which have a bearing on the security and safety of OCHA personnel, operations, premises and assets; Being a member of the UN Country Security Management Team and attending all meetings and attending all security training for members of the SMT;o. Keeping OCHA staff and eligible dependents fully apprised of security-related information and measures being taken in the countrySecurity Focal Points: Ensuring that all OCHA staff are kept informed of matters affecting their safety and security in accordance with advice received from the Head of Office, the OCHA SFP or other relevant security officials.
The Safety and Security Incident Reporting System: “all personnel employed by the organizations of the United Nations system are required to “report all security incidents in a timely manner” (UNSMS Security Policy Manual, Chapter V–CompliancewithSecurityPoliciesandProcedures,B:Safety and Security Incident Recording System, p. 175)”
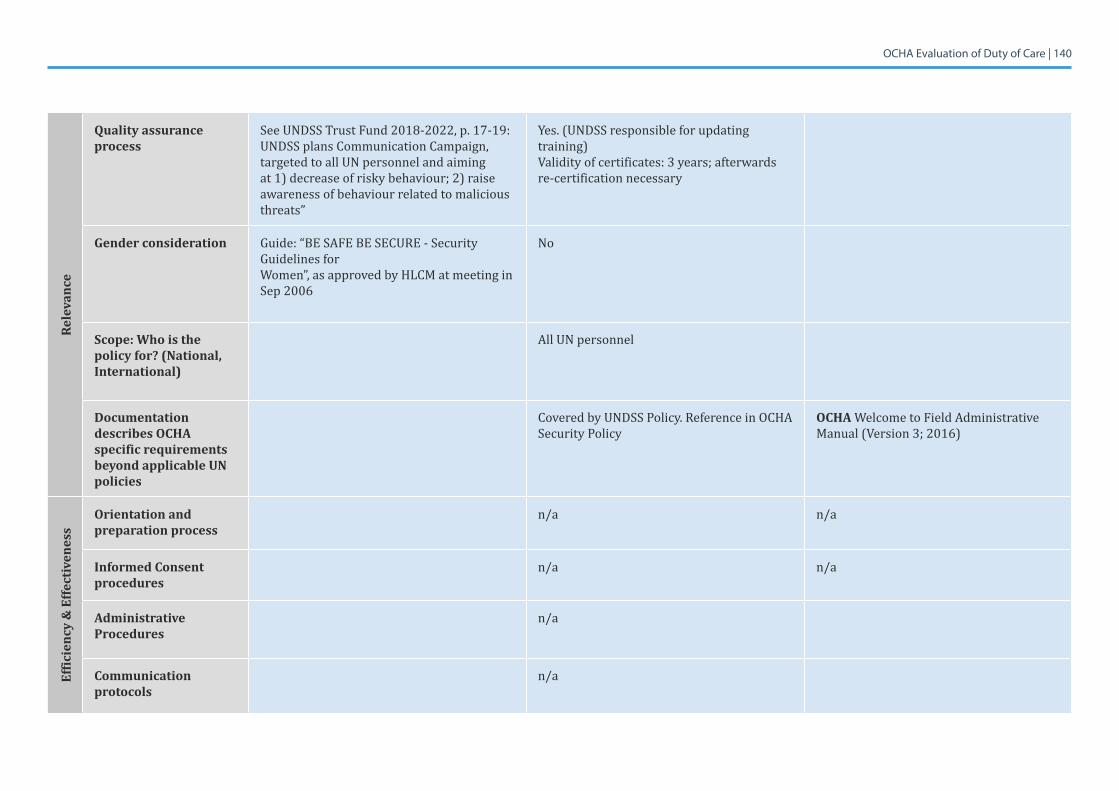
OCHA Evaluation of Duty of Care | 140Re
leva
nce
Quality assurance process
SeeUNDSSTrustFund2018-2022,p.17-19:UNDSS plans Communication Campaign, targeted to all UN personnel and aiming at 1) decrease of risky behaviour; 2) raise awareness of behaviour related to malicious threats”
Yes. (UNDSS responsible for updating training)Validityofcertificates:3years;afterwardsre-certification necessary
Gender consideration Guide: “BE SAFE BE SECURE - Security Guidelines forWomen”,asapprovedbyHLCMatmeetinginSep 2006
No
Scope: Who is the policy for? (National, International)
All UN personnel
Documentation describes OCHA specific requirements beyond applicable UN policies
Covered by UNDSS Policy. Reference in OCHA Security Policy
OCHAWelcometoFieldAdministrativeManual(Version3;2016)
Effic
ienc
y &
Effe
ctiv
enes
s
Orientation and preparation process
n/a n/a
Informed Consent procedures
n/a n/a
Administrative Procedures
n/a
Communication protocols
n/a
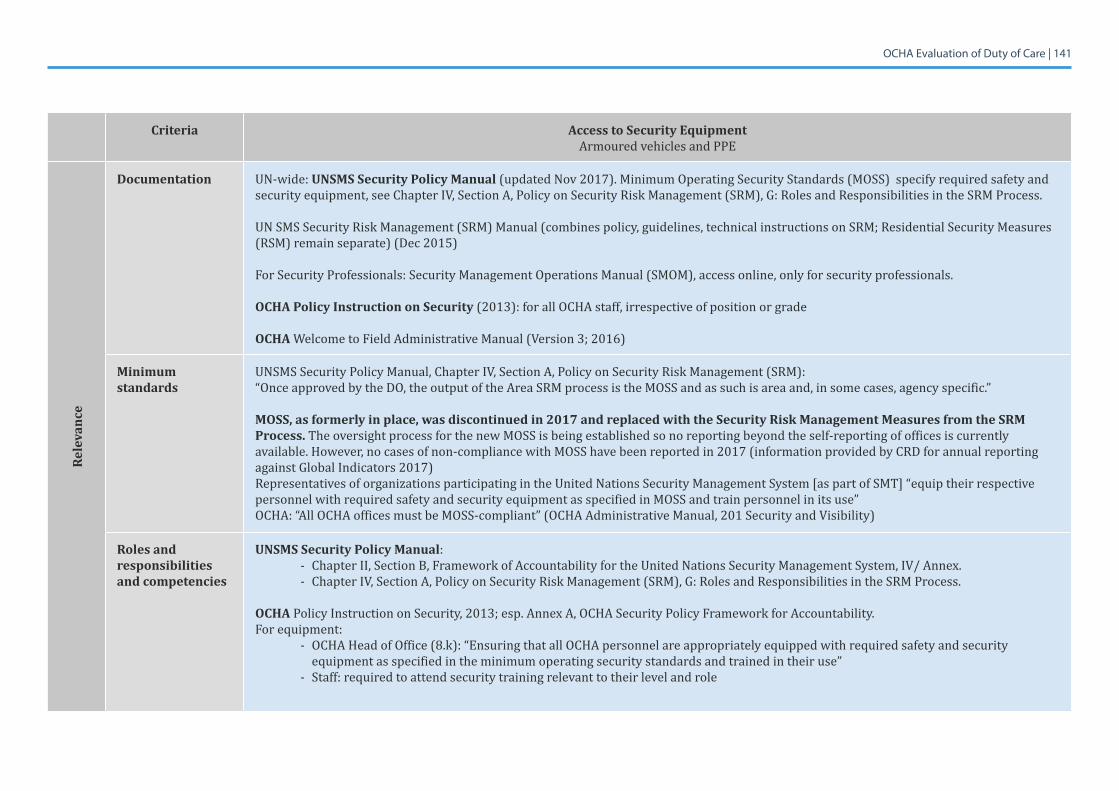
OCHA Evaluation of Duty of Care | 141
Criteria Access to Security EquipmentArmoured vehicles and PPE
Rele
vanc
e
Documentation UN-wide: UNSMS Security Policy Manual (updated Nov 2017). Minimum Operating Security Standards (MOSS) specify required safety and securityequipment,seeChapterIV,SectionA,PolicyonSecurityRiskManagement(SRM),G:RolesandResponsibilitiesintheSRMProcess.
UN SMS Security Risk Management (SRM) Manual (combines policy, guidelines, technical instructions on SRM; Residential Security Measures (RSM) remain separate) (Dec 2015)
For Security Professionals: Security Management Operations Manual (SMOM), access online, only for security professionals.
OCHA Policy Instruction on Security (2013): for all OCHA staff, irrespective of position or grade
OCHAWelcometoFieldAdministrativeManual(Version3;2016)
Minimum standards
UNSMSSecurityPolicyManual,ChapterIV,SectionA,PolicyonSecurityRiskManagement(SRM):“Once approved by the DO, the output of the Area SRM process is the MOSS and as such is area and, in some cases, agency specific.”
MOSS, as formerly in place, was discontinued in 2017 and replaced with the Security Risk Management Measures from the SRM Process. The oversight process for the new MOSS is being established so no reporting beyond the self-reporting of offices is currently available. However, no cases of non-compliance with MOSS have been reported in 2017 (information provided by CRD for annual reporting against Global Indicators 2017)Representatives of organizations participating in the United Nations Security Management System [as part of SMT] “equip their respective personnel with required safety and security equipment as specified in MOSS and train personnel in its use”OCHA:“AllOCHAofficesmustbeMOSS-compliant”(OCHAAdministrativeManual,201SecurityandVisibility)
Roles and responsibilities and competencies
UNSMS Security Policy Manual:- ChapterII,SectionB,FrameworkofAccountabilityfortheUnitedNationsSecurityManagementSystem,IV/Annex.- ChapterIV,SectionA,PolicyonSecurityRiskManagement(SRM),G:RolesandResponsibilitiesintheSRMProcess.
OCHA Policy Instruction on Security, 2013; esp. Annex A, OCHA Security Policy Framework for Accountability.For equipment:
- OCHAHeadofOffice(8.k):“EnsuringthatallOCHApersonnelareappropriatelyequippedwithrequiredsafetyandsecurityequipment as specified in the minimum operating security standards and trained in their use”
- Staff: required to attend security training relevant to their level and role
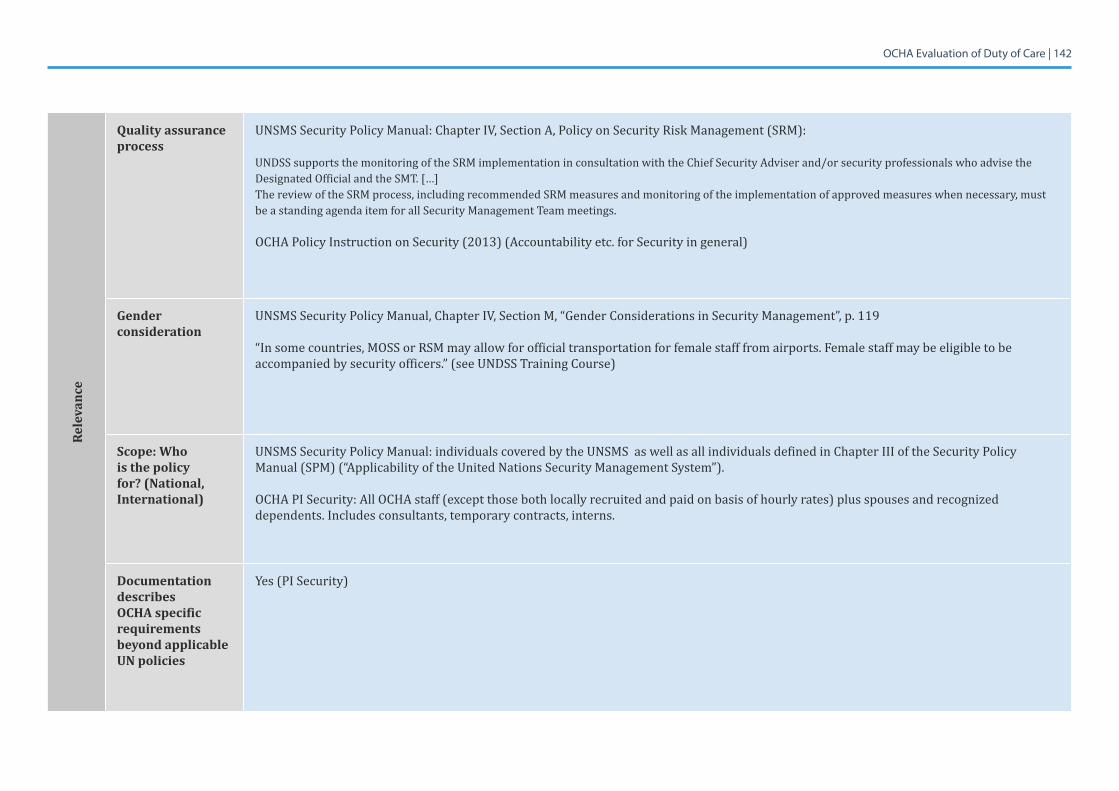
OCHA Evaluation of Duty of Care | 142
Rele
vanc
e
Quality assurance process
UNSMSSecurityPolicyManual:ChapterIV,SectionA,PolicyonSecurityRiskManagement(SRM):
UNDSS supports the monitoring of the SRM implementation in consultation with the Chief Security Adviser and/or security professionals who advise the Designated Official and the SMT. […]The review of the SRM process, including recommended SRM measures and monitoring of the implementation of approved measures when necessary, must be a standing agenda item for all Security Management Team meetings.
OCHA Policy Instruction on Security (2013) (Accountability etc. for Security in general)
Gender consideration
UNSMSSecurityPolicyManual,ChapterIV,SectionM,“GenderConsiderationsinSecurityManagement”,p.119
“In some countries, MOSS or RSM may allow for official transportation for female staff from airports. Female staff may be eligible to be accompanied by security officers.” (see UNDSS Training Course)
Scope: Who is the policy for? (National, International)
UNSMS Security Policy Manual: individuals covered by the UNSMS as well as all individuals defined in Chapter III of the Security Policy Manual (SPM) (“Applicability of the United Nations Security Management System”).
OCHA PI Security: All OCHA staff (except those both locally recruited and paid on basis of hourly rates) plus spouses and recognized dependents. Includes consultants, temporary contracts, interns.
Documentation describes OCHA specific requirements beyond applicable UN policies
Yes (PI Security)
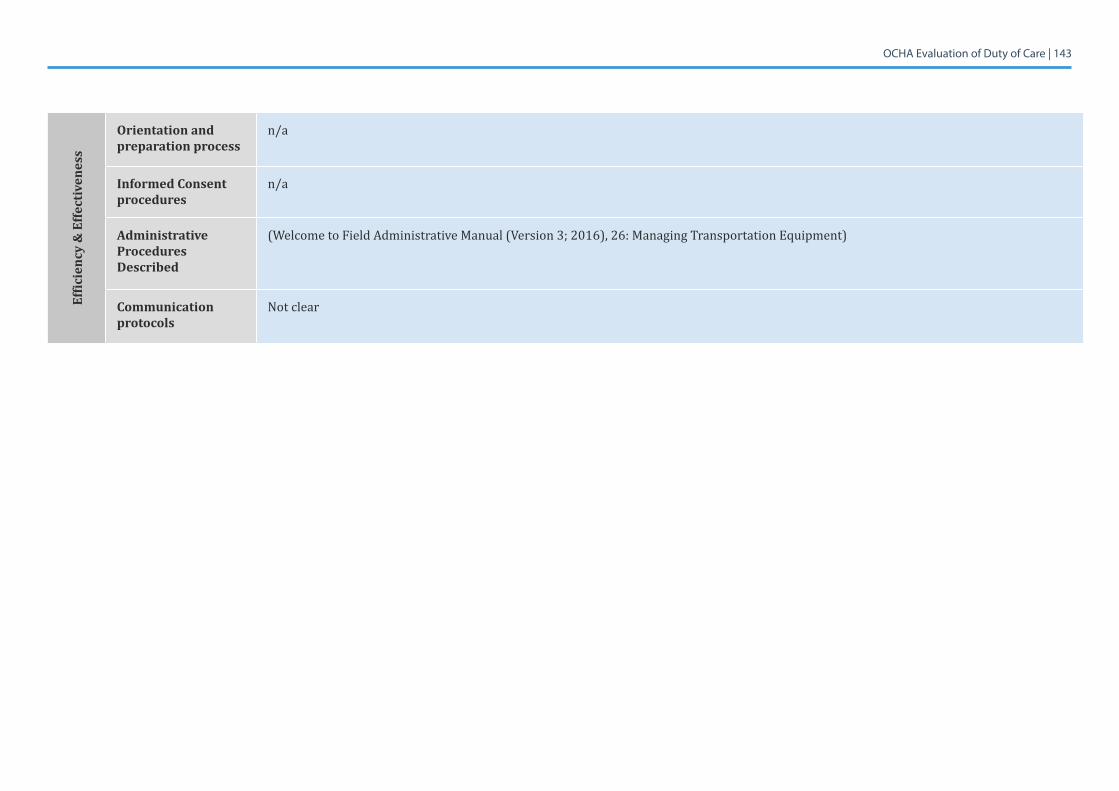
OCHA Evaluation of Duty of Care | 143
Effic
ienc
y &
Effe
ctiv
enes
s
Orientation and preparation process
n/a
Informed Consent procedures
n/a
Administrative Procedures Described
(WelcometoFieldAdministrativeManual(Version3;2016),26:ManagingTransportationEquipment)
Communication protocols
Not clear
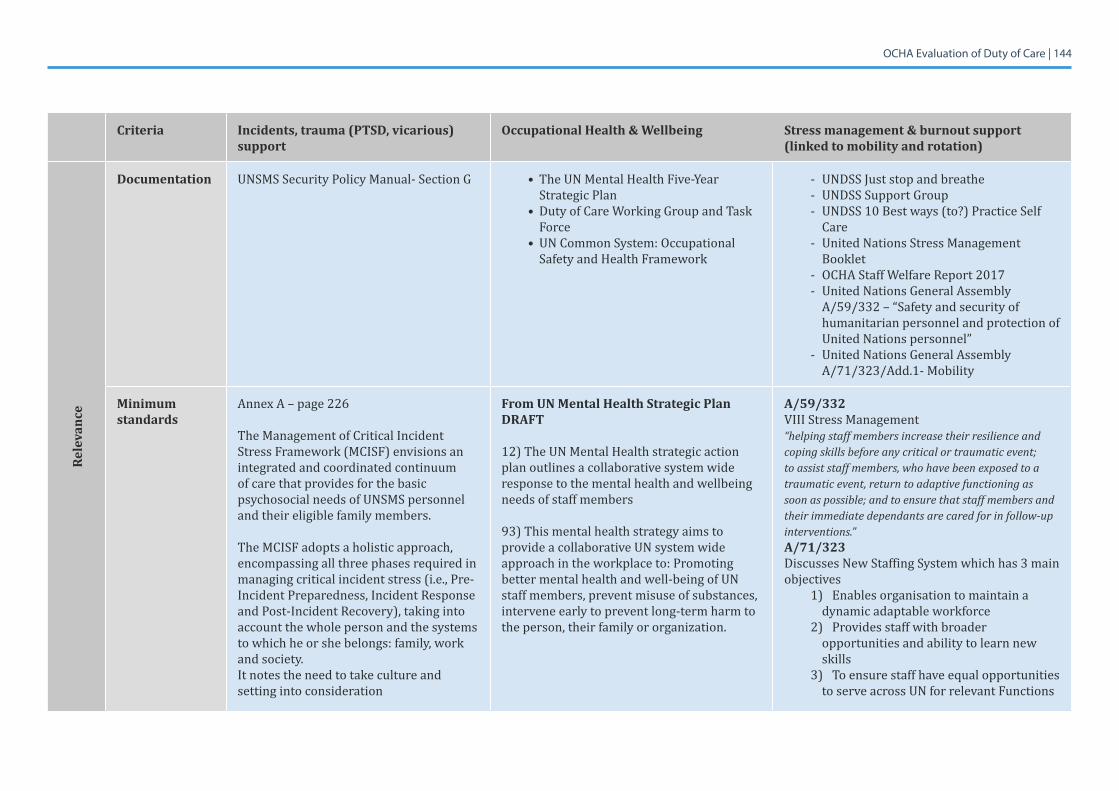
OCHA Evaluation of Duty of Care | 144
Criteria Incidents, trauma (PTSD, vicarious) support
Occupational Health & Wellbeing Stress management & burnout support (linked to mobility and rotation)
Rele
vanc
e
Documentation UNSMS Security Policy Manual- Section G • The UN Mental Health Five-Year Strategic Plan
• DutyofCareWorkingGroupandTaskForce
• UN Common System: Occupational Safety and Health Framework
- UNDSS Just stop and breathe- UNDSS Support Group- UNDSS 10 Best ways (to?) Practice Self
Care- United Nations Stress Management
Booklet - OCHAStaffWelfareReport2017- United Nations General Assembly
A/59/332 – “Safety and security of humanitarian personnel and protection of United Nations personnel”
- United Nations General Assembly A/71/323/Add.1- Mobility
Minimum standards
Annex A – page 226
The Management of Critical Incident Stress Framework (MCISF) envisions an integrated and coordinated continuum of care that provides for the basic psychosocial needs of UNSMS personnel and their eligible family members.
The MCISF adopts a holistic approach, encompassing all three phases required in managing critical incident stress (i.e., Pre-Incident Preparedness, Incident Response and Post-Incident Recovery), taking into account the whole person and the systems to which he or she belongs: family, work and society. It notes the need to take culture and setting into consideration
From UN Mental Health Strategic Plan DRAFT
12) The UN Mental Health strategic action plan outlines a collaborative system wide response to the mental health and wellbeing needs of staff members
93) This mental health strategy aims to provide a collaborative UN system wide approach in the workplace to: Promoting better mental health and well-being of UN staff members, prevent misuse of substances, intervene early to prevent long-term harm to the person, their family or organization.
A/59/332VIIIStressManagement“helping staff members increase their resilience and coping skills before any critical or traumatic event; to assist staff members, who have been exposed to a traumatic event, return to adaptive functioning as soon as possible; and to ensure that staff members and their immediate dependants are cared for in follow-up interventions.”A/71/323Discusses New Staffing System which has 3 main objectives
1) Enables organisation to maintain a dynamic adaptable workforce
2) Provides staff with broader opportunities and ability to learn new skills
3) To ensure staff have equal opportunities to serve across UN for relevant Functions
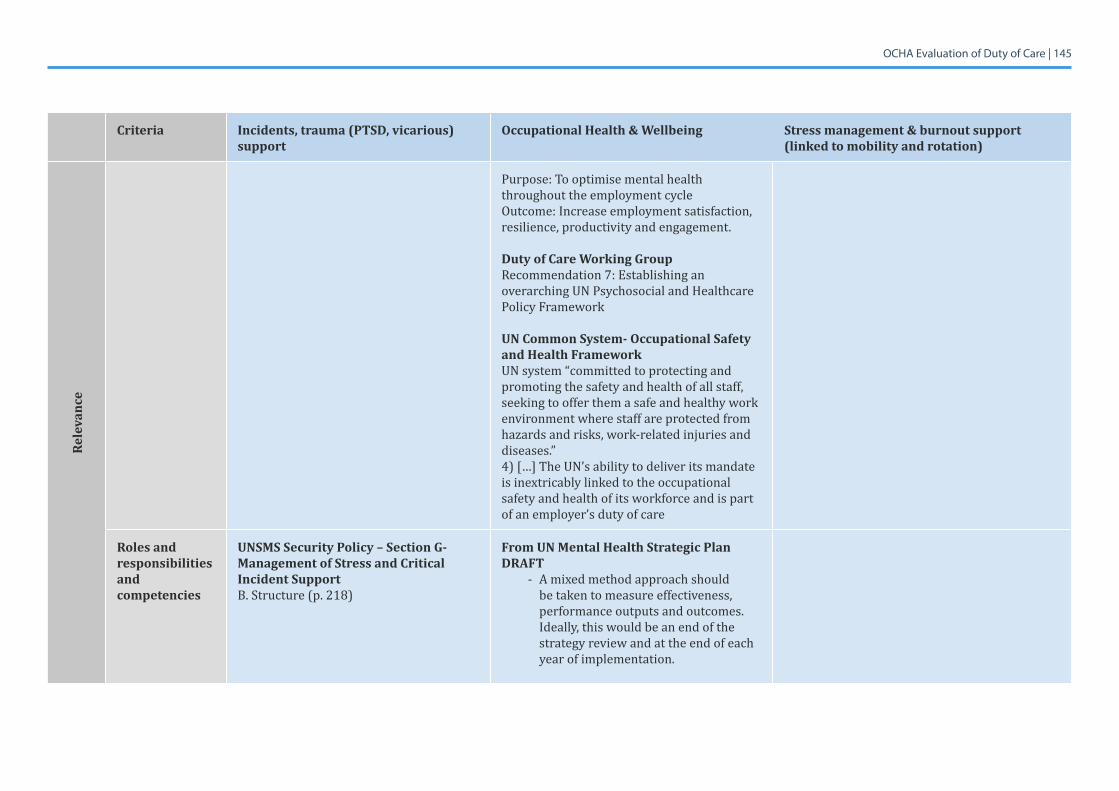
OCHA Evaluation of Duty of Care | 145
Criteria Incidents, trauma (PTSD, vicarious) support
Occupational Health & Wellbeing Stress management & burnout support (linked to mobility and rotation)
Rele
vanc
e
Purpose: To optimise mental health throughout the employment cycleOutcome: Increase employment satisfaction, resilience, productivity and engagement.
Duty of Care Working GroupRecommendation 7: Establishing an overarching UN Psychosocial and Healthcare Policy Framework
UN Common System- Occupational Safety and Health FrameworkUN system “committed to protecting and promoting the safety and health of all staff, seeking to offer them a safe and healthy work environment where staff are protected from hazards and risks, work-related injuries and diseases.”4) […] The UN’s ability to deliver its mandate is inextricably linked to the occupational safety and health of its workforce and is part of an employer’s duty of care
Roles and responsibilities and competencies
UNSMS Security Policy – Section G- Management of Stress and Critical Incident SupportB.Structure(p.218)
From UN Mental Health Strategic Plan DRAFT
- A mixed method approach should be taken to measure effectiveness, performance outputs and outcomes. Ideally, this would be an end of the strategy review and at the end of each year of implementation.
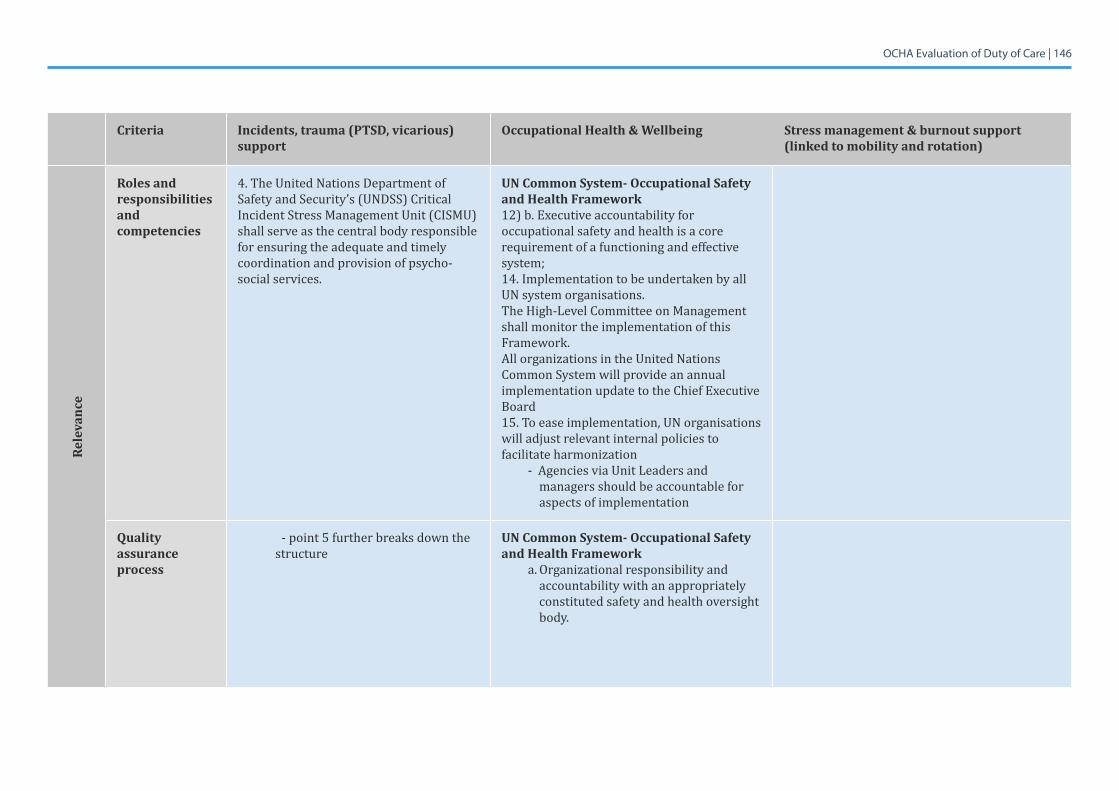
OCHA Evaluation of Duty of Care | 146
Criteria Incidents, trauma (PTSD, vicarious) support
Occupational Health & Wellbeing Stress management & burnout support (linked to mobility and rotation)
Rele
vanc
e
Roles and responsibilities and competencies
4. The United Nations Department of Safety and Security’s (UNDSS) Critical Incident Stress Management Unit (CISMU) shall serve as the central body responsible for ensuring the adequate and timely coordination and provision of psycho-social services.
UN Common System- Occupational Safety and Health Framework12) b. Executive accountability for occupational safety and health is a core requirement of a functioning and effective system; 14. Implementation to be undertaken by all UN system organisations.The High-Level Committee on Management shall monitor the implementation of this Framework.All organizations in the United Nations Common System will provide an annual implementation update to the Chief Executive Board 15. To ease implementation, UN organisations will adjust relevant internal policies to facilitate harmonization
- Agencies via Unit Leaders and managers should be accountable for aspects of implementation
Quality assurance process
- point 5 further breaks down the structure
UN Common System- Occupational Safety and Health Framework
a. Organizational responsibility and accountability with an appropriately constituted safety and health oversight body.
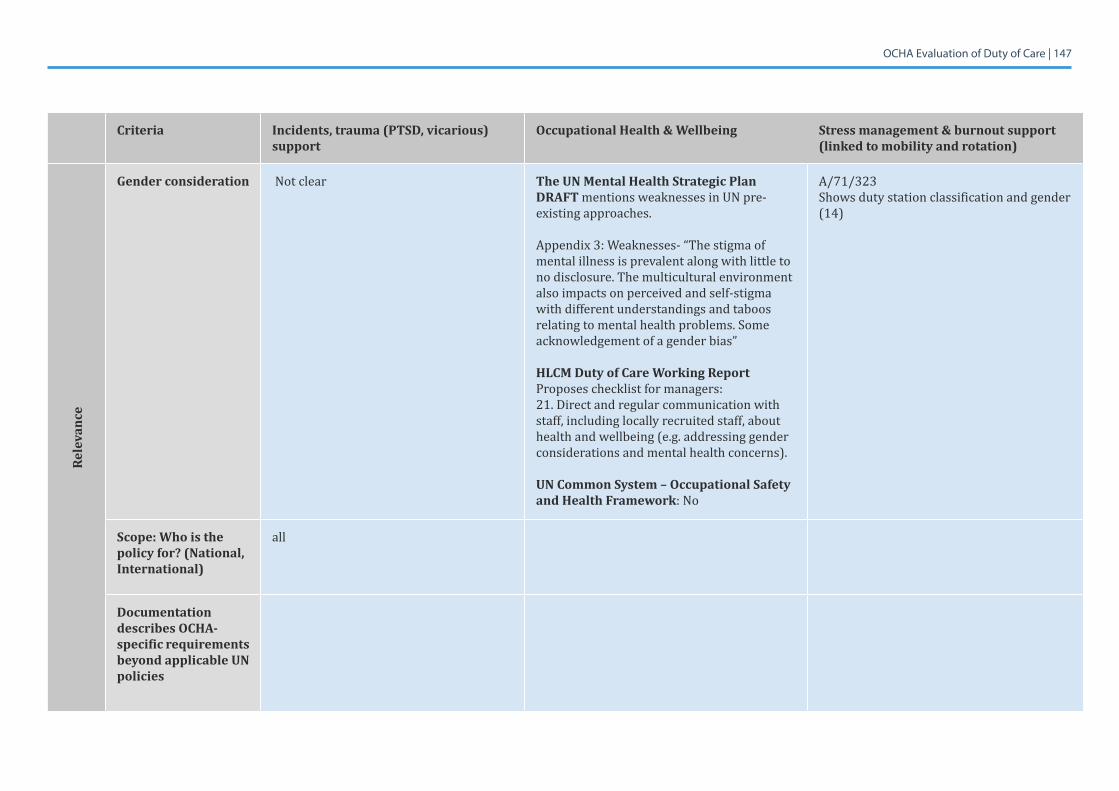
OCHA Evaluation of Duty of Care | 147
Criteria Incidents, trauma (PTSD, vicarious) support
Occupational Health & Wellbeing Stress management & burnout support (linked to mobility and rotation)
Rele
vanc
e
Gender consideration Not clear The UN Mental Health Strategic Plan DRAFT mentions weaknesses in UN pre-existing approaches.
Appendix3:Weaknesses-“Thestigmaofmental illness is prevalent along with little to no disclosure. The multicultural environment also impacts on perceived and self-stigma with different understandings and taboos relating to mental health problems. Some acknowledgement of a gender bias”
HLCM Duty of Care Working Report Proposes checklist for managers:21. Direct and regular communication with staff, including locally recruited staff, about health and wellbeing (e.g. addressing gender considerations and mental health concerns).
UN Common System – Occupational Safety and Health Framework: No
A/71/323Shows duty station classification and gender (14)
Scope: Who is the policy for? (National, International)
all
Documentation describes OCHA-specific requirements beyond applicable UN policies
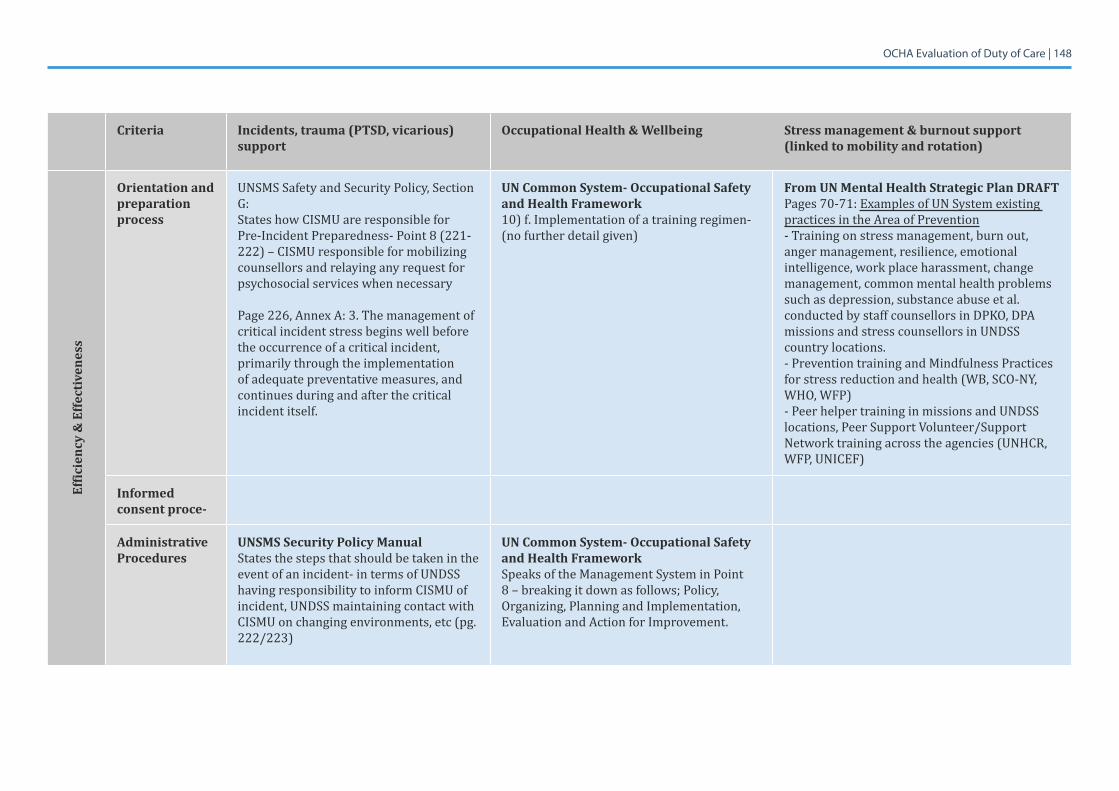
OCHA Evaluation of Duty of Care | 148
Criteria Incidents, trauma (PTSD, vicarious) support
Occupational Health & Wellbeing Stress management & burnout support (linked to mobility and rotation)
Effic
ienc
y &
Effe
ctiv
enes
s
Orientation and preparation process
UNSMS Safety and Security Policy, Section G:States how CISMU are responsible for Pre-IncidentPreparedness-Point8(221-222) – CISMU responsible for mobilizing counsellors and relaying any request for psychosocial services when necessary
Page 226, Annex A: 3. The management of critical incident stress begins well before the occurrence of a critical incident, primarily through the implementation of adequate preventative measures, and continues during and after the critical incident itself.
UN Common System- Occupational Safety and Health Framework10) f. Implementation of a training regimen- (no further detail given)
From UN Mental Health Strategic Plan DRAFTPages 70-71: Examples of UN System existing practices in the Area of Prevention- Training on stress management, burn out, anger management, resilience, emotional intelligence, work place harassment, change management, common mental health problems such as depression, substance abuse et al. conducted by staff counsellors in DPKO, DPA missions and stress counsellors in UNDSS country locations.- Prevention training and Mindfulness Practices forstressreductionandhealth(WB,SCO-NY,WHO,WFP)- Peer helper training in missions and UNDSS locations,PeerSupportVolunteer/SupportNetwork training across the agencies (UNHCR, WFP,UNICEF)
Informed consent proce-
Administrative Procedures
UNSMS Security Policy ManualStates the steps that should be taken in the event of an incident- in terms of UNDSS having responsibility to inform CISMU of incident, UNDSS maintaining contact with CISMU on changing environments, etc (pg. 222/223)
UN Common System- Occupational Safety and Health FrameworkSpeaks of the Management System in Point 8–breakingitdownasfollows;Policy,Organizing, Planning and Implementation, Evaluation and Action for Improvement.
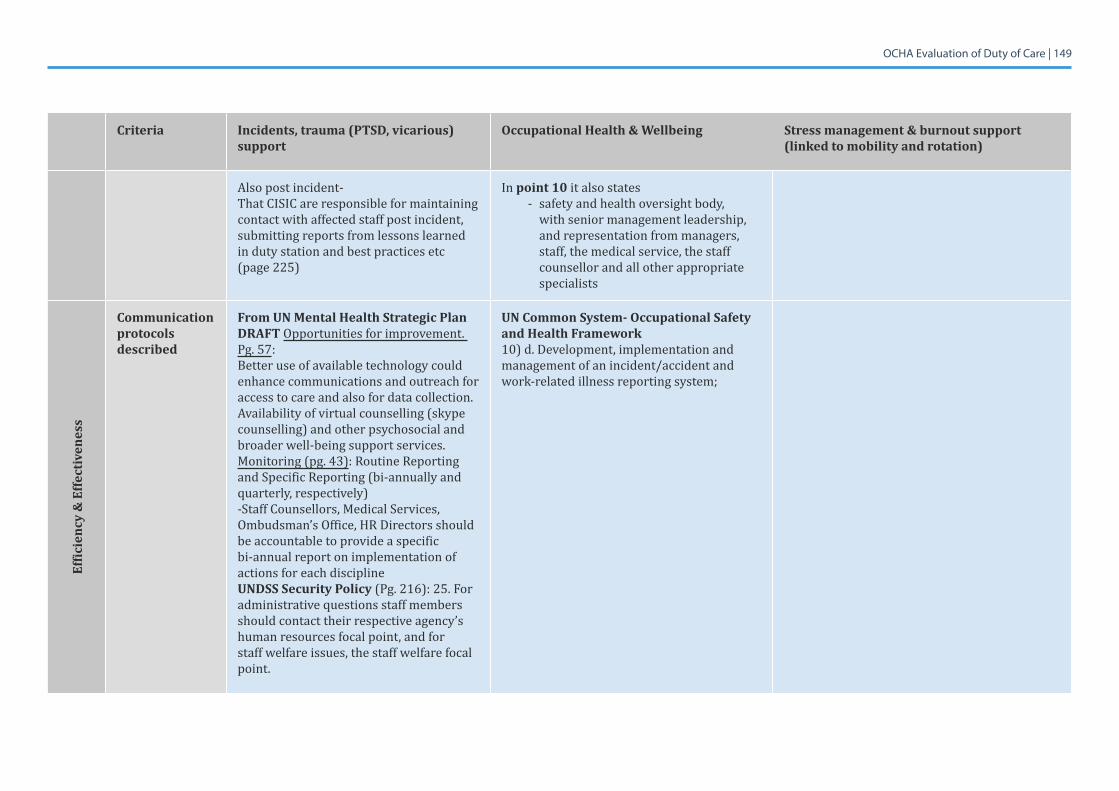
OCHA Evaluation of Duty of Care | 149
Criteria Incidents, trauma (PTSD, vicarious) support
Occupational Health & Wellbeing Stress management & burnout support (linked to mobility and rotation)
Also post incident- That CISIC are responsible for maintaining contact with affected staff post incident, submitting reports from lessons learned in duty station and best practices etc (page 225)
In point 10 it also states - safety and health oversight body,
with senior management leadership, and representation from managers, staff, the medical service, the staff counsellor and all other appropriate specialists
Effic
ienc
y &
Effe
ctiv
enes
s
Communication protocols described
From UN Mental Health Strategic Plan DRAFT Opportunities for improvement. Pg. 57:Better use of available technology could enhance communications and outreach for access to care and also for data collection. Availability of virtual counselling (skype counselling) and other psychosocial and broader well-being support services.Monitoring (pg. 43): Routine Reporting and Specific Reporting (bi-annually and quarterly, respectively) -Staff Counsellors, Medical Services, Ombudsman’s Office, HR Directors should be accountable to provide a specific bi-annual report on implementation of actions for each discipline UNDSS Security Policy (Pg. 216): 25. For administrative questions staff members should contact their respective agency’s human resources focal point, and for staff welfare issues, the staff welfare focal point.
UN Common System- Occupational Safety and Health Framework10) d. Development, implementation and management of an incident/accident and work-related illness reporting system;
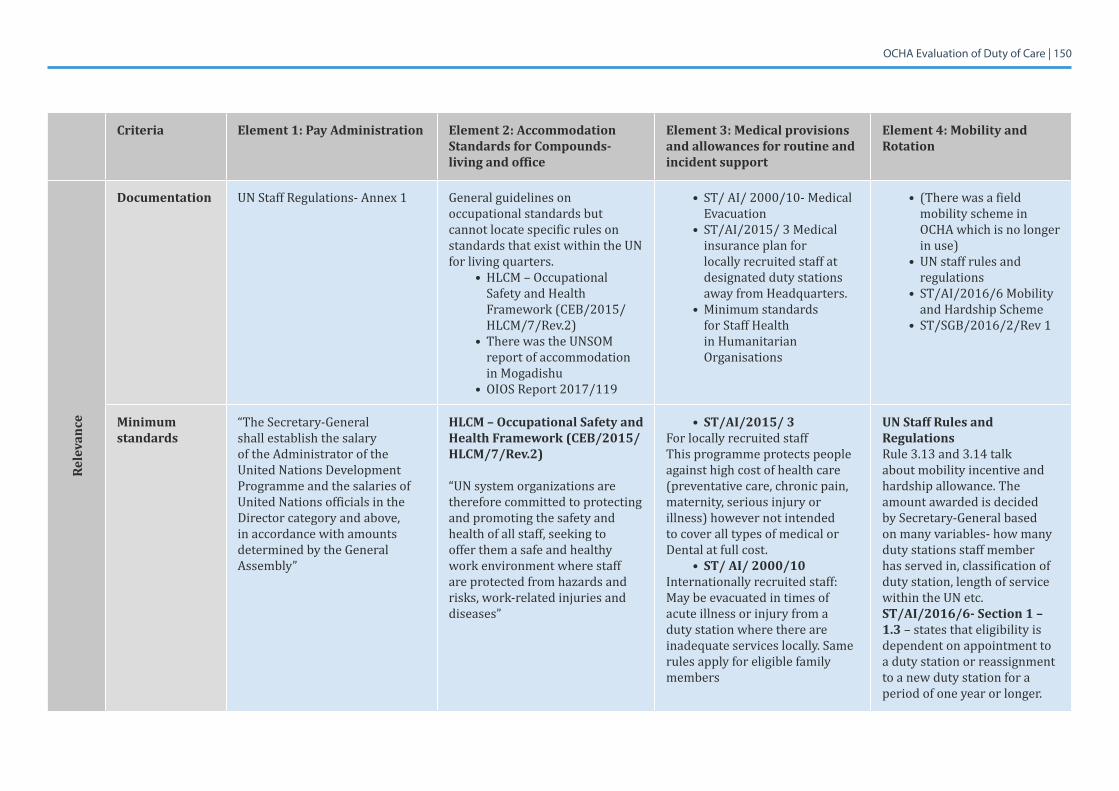
OCHA Evaluation of Duty of Care | 150
Criteria Element 1: Pay Administration Element 2: Accommodation Standards for Compounds- living and office
Element 3: Medical provisions and allowances for routine and incident support
Element 4: Mobility and Rotation
Rele
vanc
e
Documentation UN Staff Regulations- Annex 1 General guidelines on occupational standards but cannot locate specific rules on standards that exist within the UN for living quarters.
• HLCM – Occupational Safety and Health Framework (CEB/2015/HLCM/7/Rev.2)
• There was the UNSOM report of accommodation in Mogadishu
• OIOS Report 2017/119
• ST/ AI/ 2000/10- Medical Evacuation
• ST/AI/2015/ 3 Medical insurance plan for locally recruited staff at designated duty stations away from Headquarters.
• Minimum standards for Staff Health in Humanitarian Organisations
• (There was a field mobility scheme in OCHA which is no longer in use)
• UN staff rules and regulations
• ST/AI/2016/6 Mobility and Hardship Scheme
• ST/SGB/2016/2/Rev 1
Minimum standards
“The Secretary-General shall establish the salary of the Administrator of the United Nations Development Programme and the salaries of United Nations officials in the Director category and above, in accordance with amounts determined by the General Assembly”
HLCM – Occupational Safety and Health Framework (CEB/2015/HLCM/7/Rev.2)
“UN system organizations are therefore committed to protecting and promoting the safety and health of all staff, seeking to offer them a safe and healthy work environment where staff are protected from hazards and risks, work-related injuries and diseases”
• ST/AI/2015/ 3For locally recruited staffThis programme protects people against high cost of health care (preventative care, chronic pain, maternity, serious injury or illness) however not intended to cover all types of medical or Dental at full cost.
• ST/ AI/ 2000/10 Internationally recruited staff: May be evacuated in times of acute illness or injury from a duty station where there are inadequate services locally. Same rules apply for eligible family members
UN Staff Rules and RegulationsRule 3.13 and 3.14 talk about mobility incentive and hardship allowance. The amount awarded is decided by Secretary-General based on many variables- how many duty stations staff member has served in, classification of duty station, length of service within the UN etc. ST/AI/2016/6- Section 1 – 1.3 – states that eligibility is dependent on appointment to a duty station or reassignment to a new duty station for a period of one year or longer.
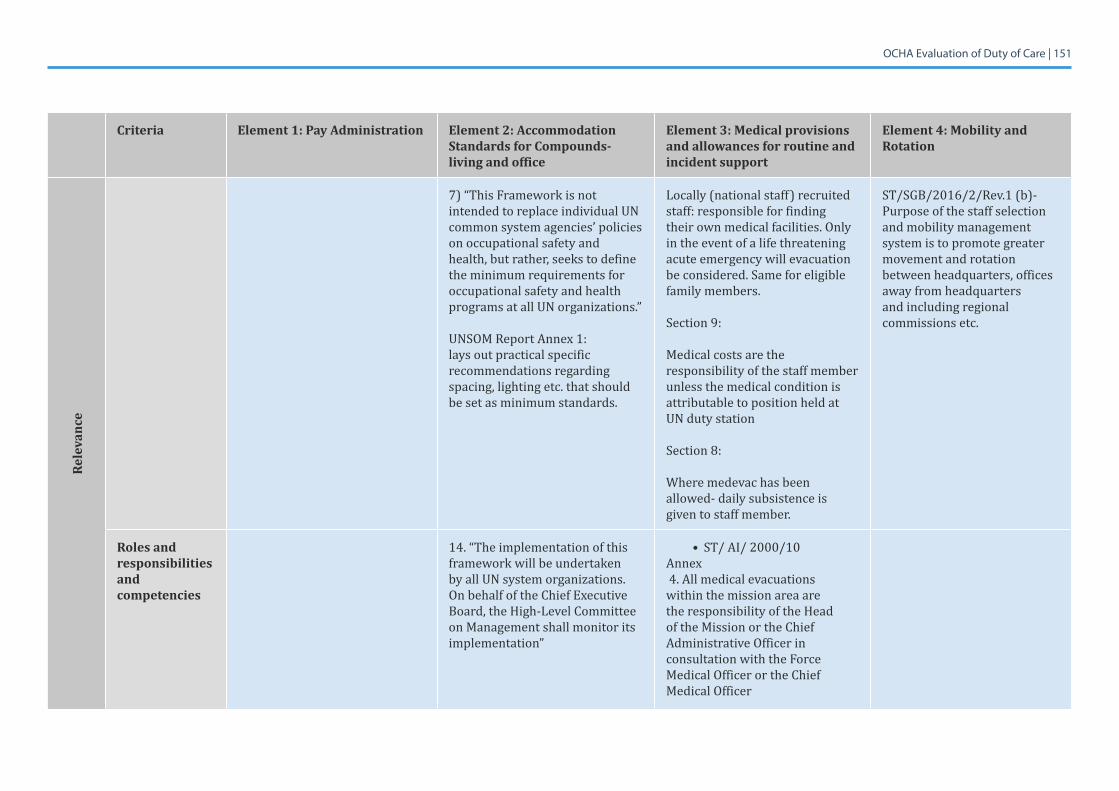
OCHA Evaluation of Duty of Care | 151
Criteria Element 1: Pay Administration Element 2: Accommodation Standards for Compounds- living and office
Element 3: Medical provisions and allowances for routine and incident support
Element 4: Mobility and Rotation
Rele
vanc
e
7) “This Framework is not intended to replace individual UN common system agencies’ policies on occupational safety and health, but rather, seeks to define the minimum requirements for occupational safety and health programs at all UN organizations.”
UNSOM Report Annex 1: lays out practical specific recommendations regarding spacing, lighting etc. that should be set as minimum standards.
Locally (national staff) recruited staff: responsible for finding their own medical facilities. Only in the event of a life threatening acute emergency will evacuation be considered. Same for eligible family members.
Section 9:
Medical costs are the responsibility of the staff member unless the medical condition is attributable to position held at UN duty station
Section8:
Wheremedevachasbeenallowed- daily subsistence is given to staff member.
ST/SGB/2016/2/Rev.1 (b)- Purpose of the staff selection and mobility management system is to promote greater movement and rotation between headquarters, offices away from headquarters and including regional commissions etc.
Roles and responsibilities and competencies
14. “The implementation of this framework will be undertaken by all UN system organizations. On behalf of the Chief Executive Board, the High-Level Committee on Management shall monitor its implementation”
• ST/ AI/ 2000/10 Annex 4. All medical evacuations within the mission area are the responsibility of the Head of the Mission or the Chief Administrative Officer in consultation with the Force Medical Officer or the Chief Medical Officer
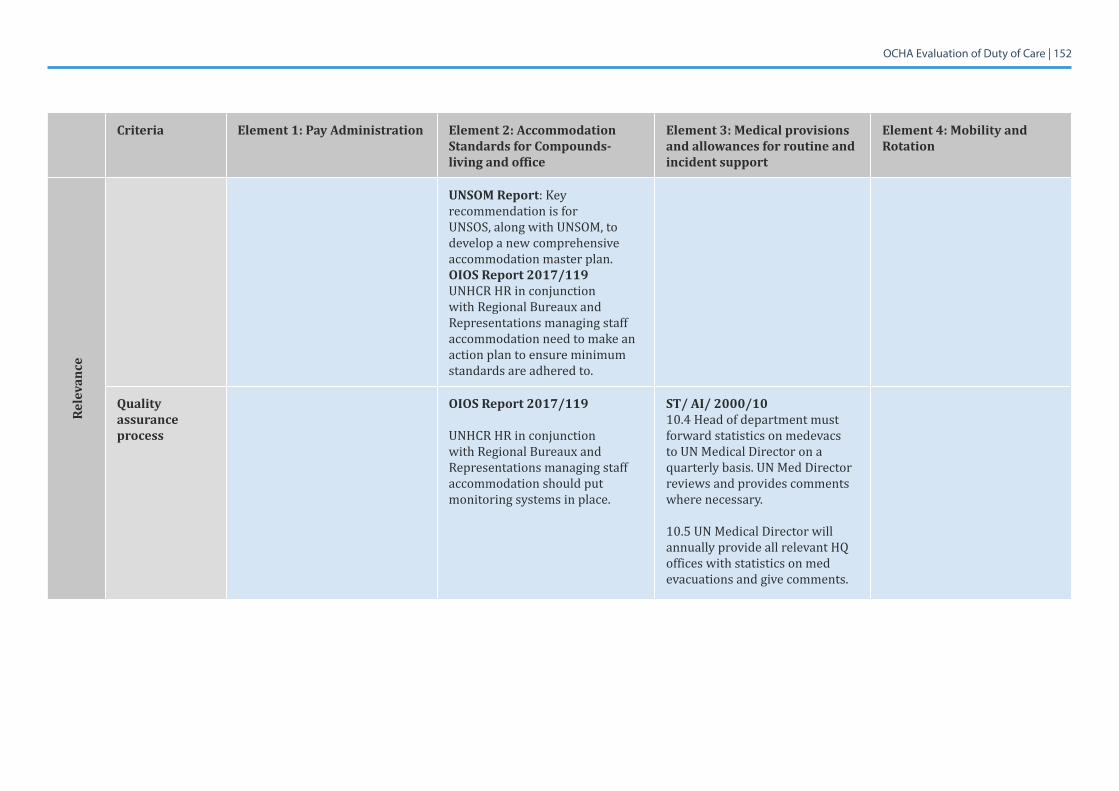
OCHA Evaluation of Duty of Care | 152
Criteria Element 1: Pay Administration Element 2: Accommodation Standards for Compounds- living and office
Element 3: Medical provisions and allowances for routine and incident support
Element 4: Mobility and Rotation
Rele
vanc
e
UNSOM Report: Key recommendation is for UNSOS, along with UNSOM, to develop a new comprehensive accommodation master plan. OIOS Report 2017/119UNHCR HR in conjunction with Regional Bureaux and Representations managing staff accommodation need to make an action plan to ensure minimum standards are adhered to.
Quality assurance process
OIOS Report 2017/119
UNHCR HR in conjunction with Regional Bureaux and Representations managing staff accommodation should put monitoring systems in place.
ST/ AI/ 2000/10 10.4 Head of department must forward statistics on medevacs to UN Medical Director on a quarterly basis. UN Med Director reviews and provides comments where necessary.
10.5 UN Medical Director will annually provide all relevant HQ offices with statistics on med evacuations and give comments.
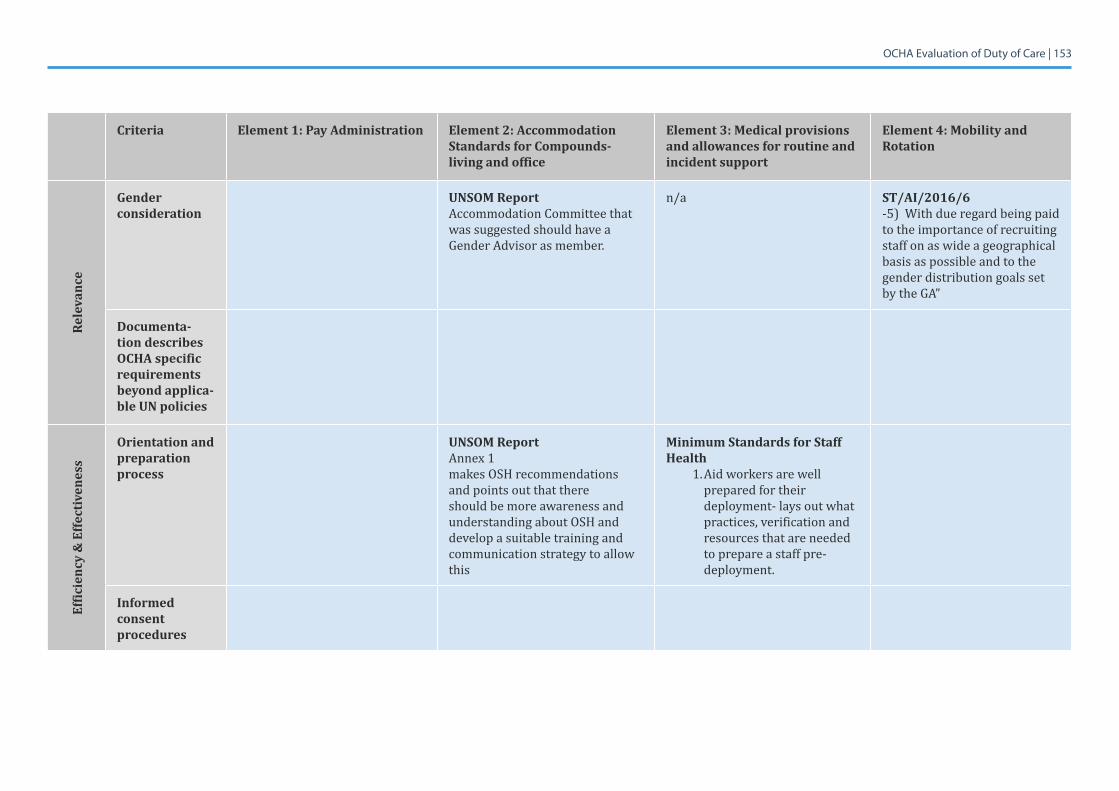
OCHA Evaluation of Duty of Care | 153
Criteria Element 1: Pay Administration Element 2: Accommodation Standards for Compounds- living and office
Element 3: Medical provisions and allowances for routine and incident support
Element 4: Mobility and Rotation
Rele
vanc
e
Gender consideration
UNSOM ReportAccommodation Committee that was suggested should have a Gender Advisor as member.
n/a ST/AI/2016/6 -5)Withdueregardbeingpaidto the importance of recruiting staff on as wide a geographical basis as possible and to the gender distribution goals set by the GA”
Documenta-tion describes OCHA specific requirements beyond applica-ble UN policies
Effic
ienc
y &
Effe
ctiv
enes
s
Orientation and preparation process
UNSOM ReportAnnex 1makes OSH recommendations and points out that there should be more awareness and understanding about OSH and develop a suitable training and communication strategy to allow this
Minimum Standards for Staff Health
1. Aid workers are well prepared for their deployment- lays out what practices, verification and resources that are needed to prepare a staff pre-deployment.
Informed consent procedures
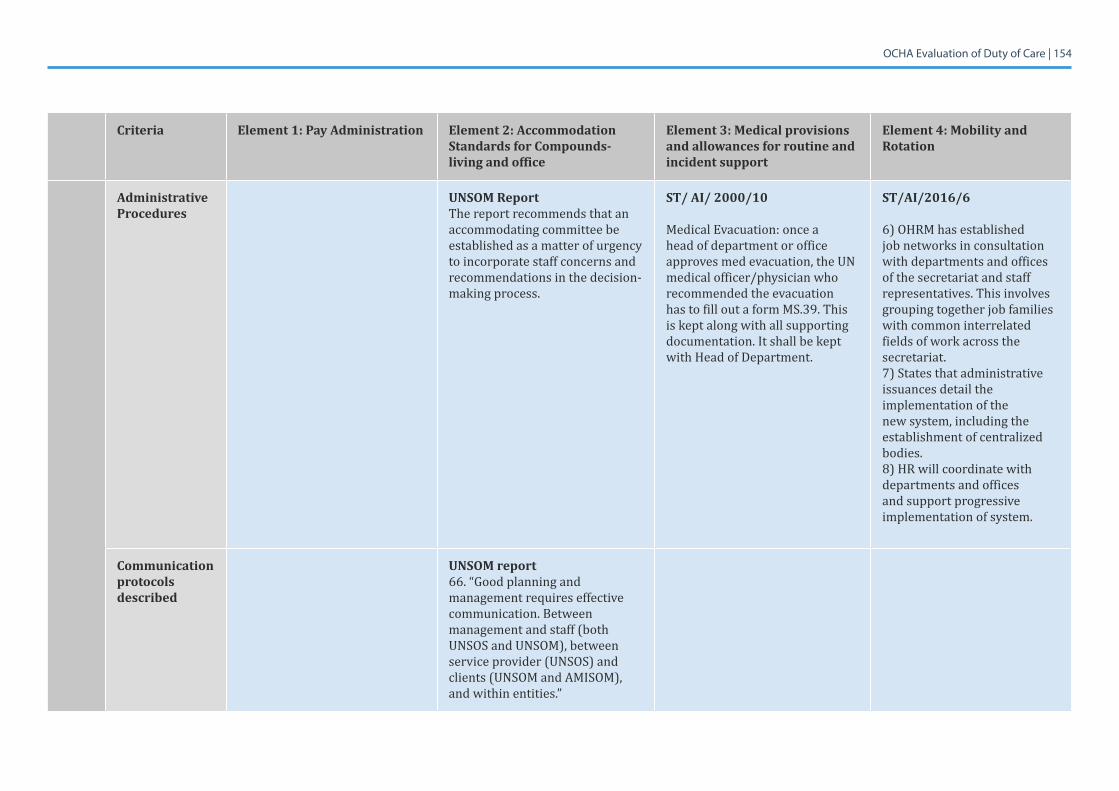
OCHA Evaluation of Duty of Care | 154
Criteria Element 1: Pay Administration Element 2: Accommodation Standards for Compounds- living and office
Element 3: Medical provisions and allowances for routine and incident support
Element 4: Mobility and Rotation
Administrative Procedures
UNSOM ReportThe report recommends that an accommodating committee be established as a matter of urgency to incorporate staff concerns and recommendations in the decision-making process.
ST/ AI/ 2000/10
Medical Evacuation: once a head of department or office approves med evacuation, the UN medical officer/physician who recommended the evacuation has to fill out a form MS.39. This is kept along with all supporting documentation. It shall be kept with Head of Department.
ST/AI/2016/6
6) OHRM has established job networks in consultation with departments and offices of the secretariat and staff representatives. This involves grouping together job families with common interrelated fields of work across the secretariat.7) States that administrative issuances detail the implementation of the new system, including the establishment of centralized bodies.8)HRwillcoordinatewithdepartments and offices and support progressive implementation of system.
Communication protocols described
UNSOM report66. “Good planning and management requires effective communication. Between management and staff (both UNSOS and UNSOM), between service provider (UNSOS) and clients (UNSOM and AMISOM), and within entities.”
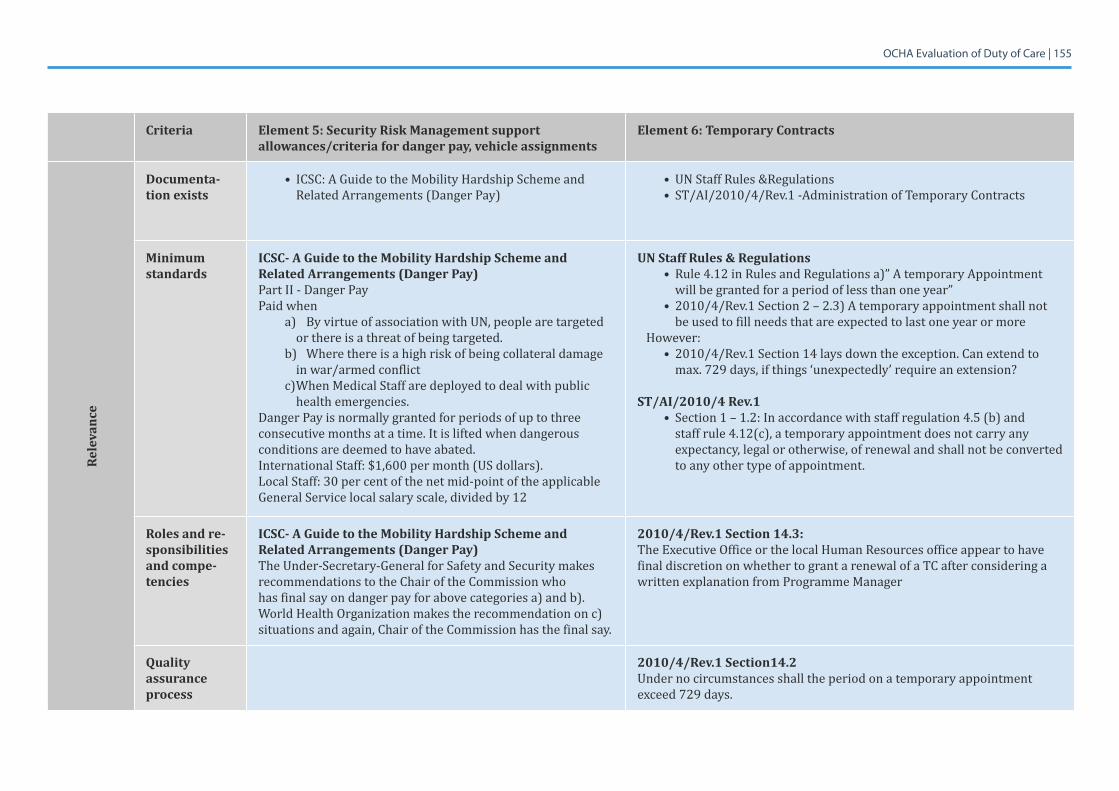
OCHA Evaluation of Duty of Care | 155
Criteria Element 5: Security Risk Management support allowances/criteria for danger pay, vehicle assignments
Element 6: Temporary Contracts
Rele
vanc
e
Documenta-tion exists
• ICSC: A Guide to the Mobility Hardship Scheme and Related Arrangements (Danger Pay)
• UN Staff Rules &Regulations• ST/AI/2010/4/Rev.1 -Administration of Temporary Contracts
Minimum standards
ICSC- A Guide to the Mobility Hardship Scheme and Related Arrangements (Danger Pay)Part II - Danger PayPaid when
a) By virtue of association with UN, people are targeted or there is a threat of being targeted.
b) Wherethereisahighriskofbeingcollateraldamagein war/armed conflict
c)WhenMedicalStaffaredeployedtodealwithpublichealth emergencies.
Danger Pay is normally granted for periods of up to three consecutive months at a time. It is lifted when dangerous conditions are deemed to have abated.International Staff: $1,600 per month (US dollars). Local Staff: 30 per cent of the net mid-point of the applicable General Service local salary scale, divided by 12
UN Staff Rules & Regulations• Rule 4.12 in Rules and Regulations a)” A temporary Appointment
will be granted for a period of less than one year”• 2010/4/Rev.1 Section 2 – 2.3) A temporary appointment shall not
be used to fill needs that are expected to last one year or more However:
• 2010/4/Rev.1 Section 14 lays down the exception. Can extend to max. 729 days, if things ‘unexpectedly’ require an extension?
ST/AI/2010/4 Rev.1• Section 1 – 1.2: In accordance with staff regulation 4.5 (b) and
staff rule 4.12(c), a temporary appointment does not carry any expectancy, legal or otherwise, of renewal and shall not be converted to any other type of appointment.
Roles and re-sponsibilities and compe-tencies
ICSC- A Guide to the Mobility Hardship Scheme and Related Arrangements (Danger Pay)The Under-Secretary-General for Safety and Security makes recommendations to the Chair of the Commission who has final say on danger pay for above categories a) and b). WorldHealthOrganizationmakestherecommendationonc)situations and again, Chair of the Commission has the final say.
2010/4/Rev.1 Section 14.3: The Executive Office or the local Human Resources office appear to have final discretion on whether to grant a renewal of a TC after considering a written explanation from Programme Manager
Quality assurance process
2010/4/Rev.1 Section14.2Under no circumstances shall the period on a temporary appointment exceed 729 days.
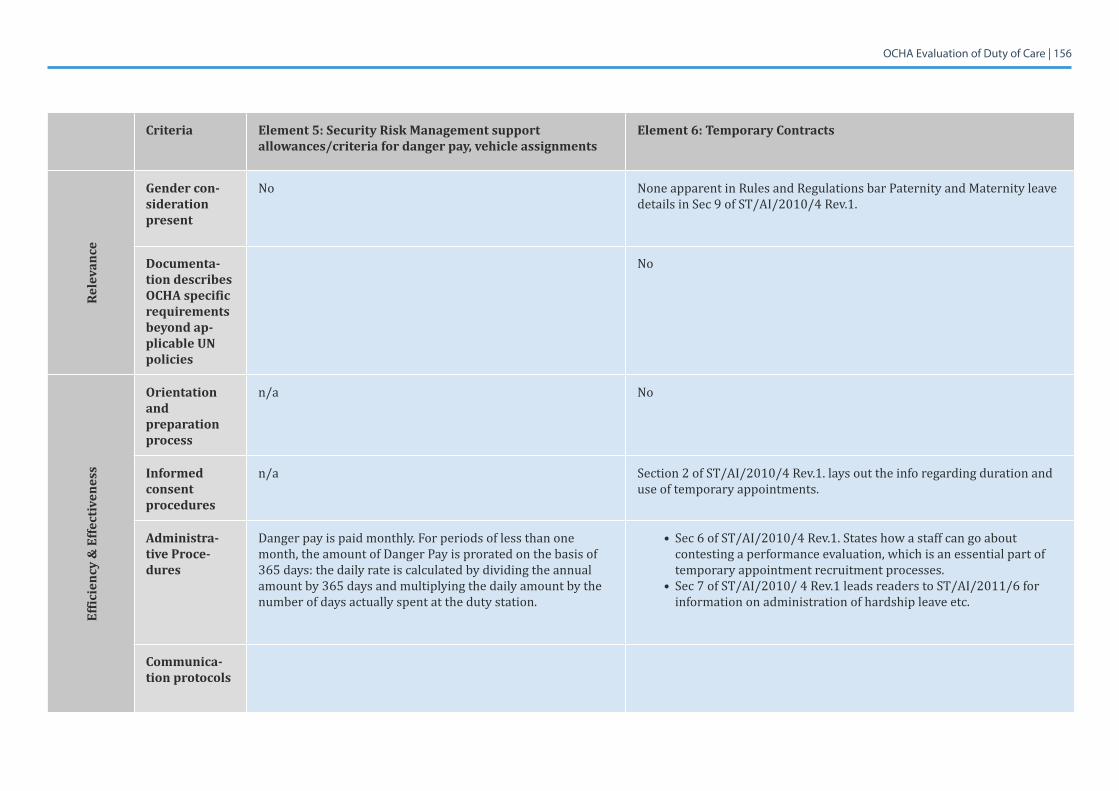
OCHA Evaluation of Duty of Care | 156
Criteria Element 5: Security Risk Management support allowances/criteria for danger pay, vehicle assignments
Element 6: Temporary Contracts
Rele
vanc
e
Gender con-sideration present
No None apparent in Rules and Regulations bar Paternity and Maternity leave details in Sec 9 of ST/AI/2010/4 Rev.1.
Documenta-tion describes OCHA specific requirements beyond ap-plicable UN policies
No
Effic
ienc
y &
Effe
ctiv
enes
s
Orientation and preparation process
n/a No
Informed consent procedures
n/a Section 2 of ST/AI/2010/4 Rev.1. lays out the info regarding duration and use of temporary appointments.
Administra-tive Proce-dures
Danger pay is paid monthly. For periods of less than one month, the amount of Danger Pay is prorated on the basis of 365 days: the daily rate is calculated by dividing the annual amount by 365 days and multiplying the daily amount by the number of days actually spent at the duty station.
• Sec 6 of ST/AI/2010/4 Rev.1. States how a staff can go about contesting a performance evaluation, which is an essential part of temporary appointment recruitment processes.
• Sec 7 of ST/AI/2010/ 4 Rev.1 leads readers to ST/AI/2011/6 for information on administration of hardship leave etc.
Communica-tion protocols
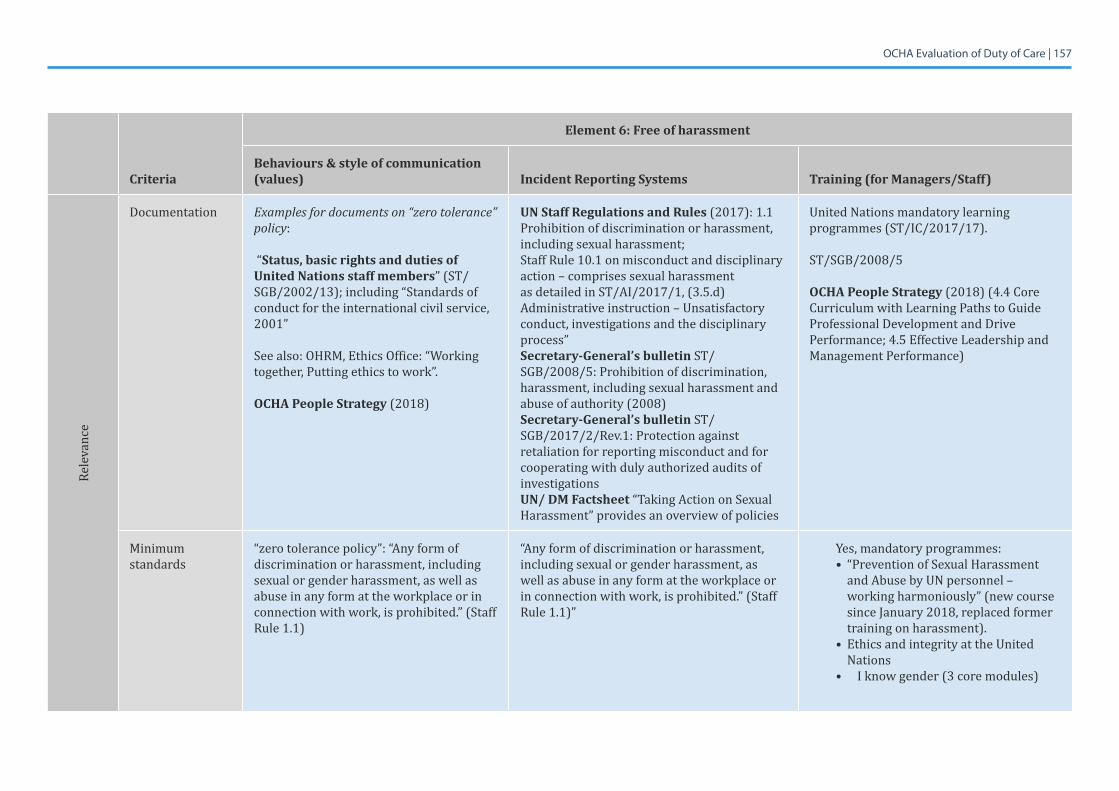
OCHA Evaluation of Duty of Care | 157
Criteria
Element 6: Free of harassment
Behaviours & style of communication (values) Incident Reporting Systems Training (for Managers/Staff)
Rele
vanc
e
Documentation Examples for documents on “zero tolerance” policy:
“Status, basic rights and duties of United Nations staff members” (ST/SGB/2002/13); including “Standards of conduct for the international civil service, 2001”
Seealso:OHRM,EthicsOffice:“Workingtogether, Putting ethics to work”.
OCHA People Strategy(2018)
UN Staff Regulations and Rules (2017): 1.1 Prohibition of discrimination or harassment, including sexual harassment; Staff Rule 10.1 on misconduct and disciplinary action – comprises sexual harassment as detailed in ST/AI/2017/1, (3.5.d) Administrative instruction – Unsatisfactory conduct, investigations and the disciplinary process”Secretary-General’s bulletin ST/SGB/2008/5:Prohibitionofdiscrimination,harassment, including sexual harassment and abuseofauthority(2008)Secretary-General’s bulletin ST/SGB/2017/2/Rev.1: Protection against retaliation for reporting misconduct and for cooperating with duly authorized audits of investigationsUN/ DM Factsheet “Taking Action on Sexual Harassment” provides an overview of policies
United Nations mandatory learning programmes (ST/IC/2017/17).
ST/SGB/2008/5
OCHA People Strategy(2018)(4.4CoreCurriculum with Learning Paths to Guide Professional Development and Drive Performance; 4.5 Effective Leadership and Management Performance)
Minimum standards
“zero tolerance policy”: “Any form of discrimination or harassment, including sexual or gender harassment, as well as abuse in any form at the workplace or in connection with work, is prohibited.” (Staff Rule 1.1)
“Any form of discrimination or harassment, including sexual or gender harassment, as well as abuse in any form at the workplace or in connection with work, is prohibited.” (Staff Rule 1.1)”
Yes, mandatory programmes:• “Prevention of Sexual Harassment
and Abuse by UN personnel – working harmoniously” (new course sinceJanuary2018,replacedformertraining on harassment).
• Ethics and integrity at the United Nations
• I know gender (3 core modules)
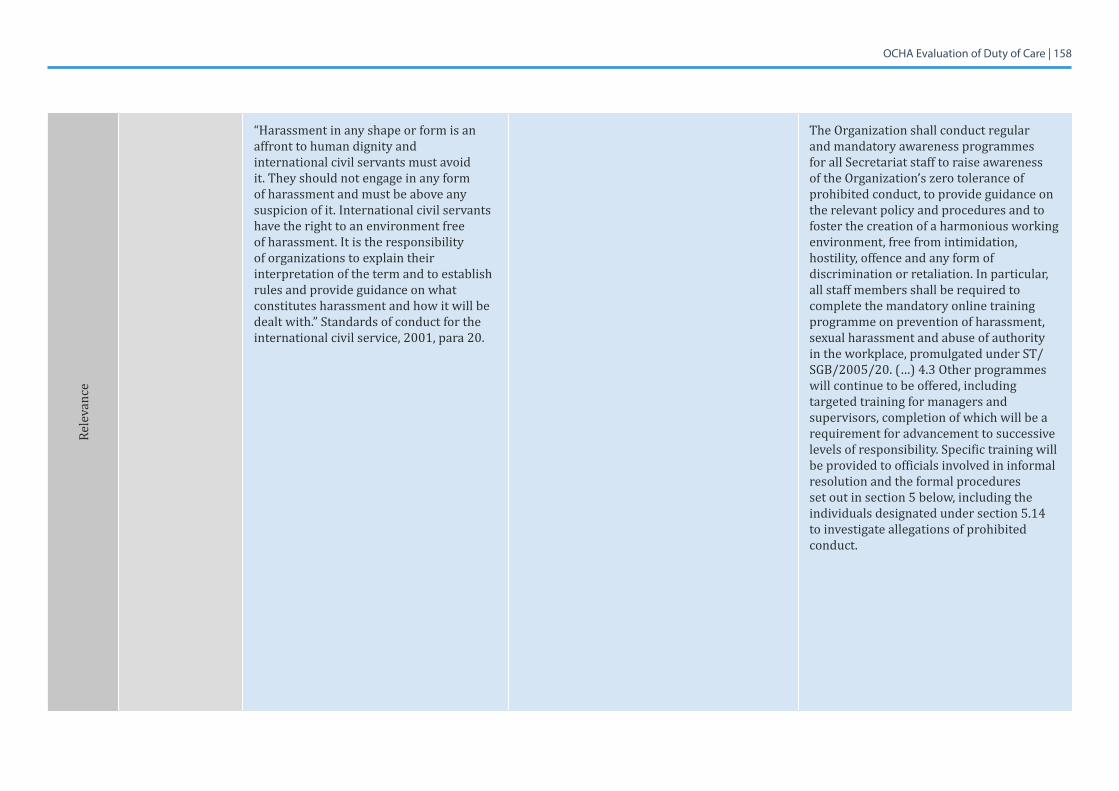
OCHA Evaluation of Duty of Care | 158
Rele
vanc
e
“Harassment in any shape or form is an affront to human dignity andinternational civil servants must avoid it. They should not engage in any form of harassment and must be above any suspicion of it. International civil servants have the right to an environment free of harassment. It is the responsibility of organizations to explain their interpretation of the term and to establish rules and provide guidance on what constitutes harassment and how it will be dealt with.” Standards of conduct for the international civil service, 2001, para 20.
The Organization shall conduct regular and mandatory awareness programmes for all Secretariat staff to raise awareness of the Organization’s zero tolerance of prohibited conduct, to provide guidance on the relevant policy and procedures and to foster the creation of a harmonious working environment, free from intimidation, hostility, offence and any form of discrimination or retaliation. In particular, all staff members shall be required to complete the mandatory online training programme on prevention of harassment, sexual harassment and abuse of authority in the workplace, promulgated under ST/SGB/2005/20. (…) 4.3 Other programmes will continue to be offered, including targeted training for managers and supervisors, completion of which will be a requirement for advancement to successive levels of responsibility. Specific training will be provided to officials involved in informal resolution and the formal procedures set out in section 5 below, including the individuals designated under section 5.14 to investigate allegations of prohibited conduct.
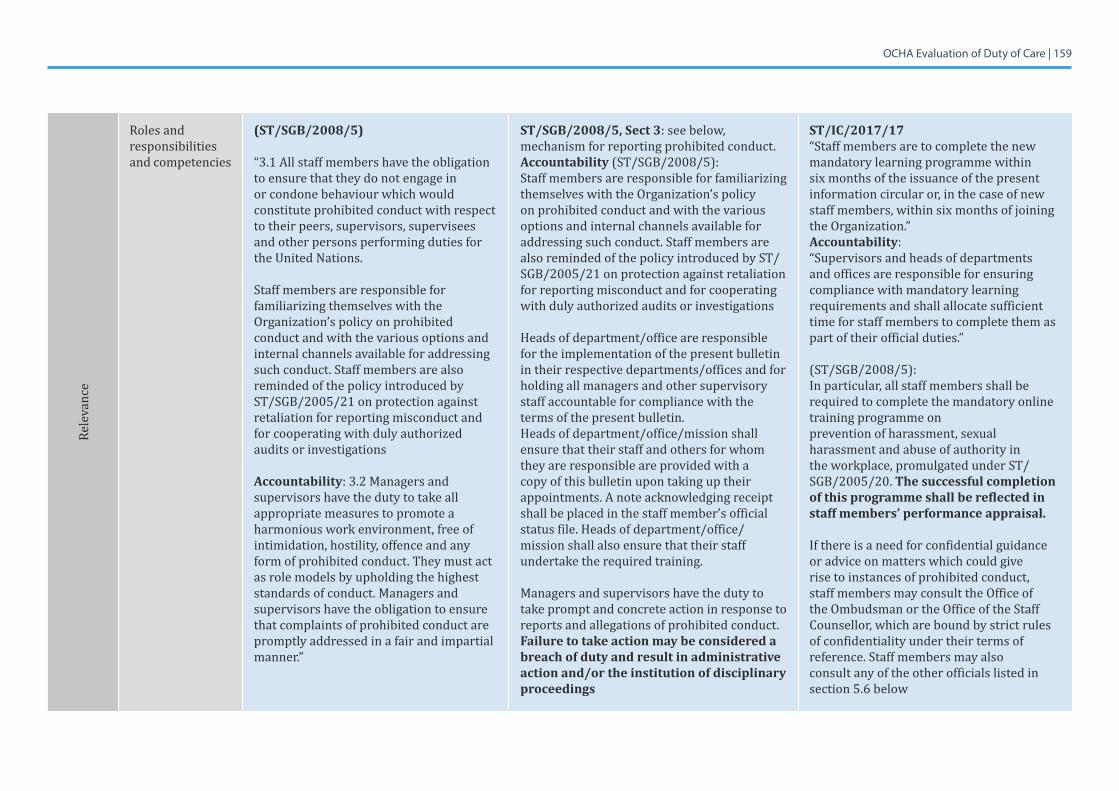
OCHA Evaluation of Duty of Care | 159
Rele
vanc
e
Roles and responsibilities and competencies
(ST/SGB/2008/5)
“3.1 All staff members have the obligation to ensure that they do not engage in or condone behaviour which would constitute prohibited conduct with respect to their peers, supervisors, supervisees and other persons performing duties for the United Nations.
Staff members are responsible for familiarizing themselves with the Organization’s policy on prohibited conduct and with the various options and internal channels available for addressing such conduct. Staff members are also reminded of the policy introduced by ST/SGB/2005/21 on protection against retaliation for reporting misconduct and for cooperating with duly authorized audits or investigations
Accountability: 3.2 Managers and supervisors have the duty to take all appropriate measures to promote a harmonious work environment, free of intimidation, hostility, offence and any form of prohibited conduct. They must act as role models by upholding the highest standards of conduct. Managers and supervisors have the obligation to ensure that complaints of prohibited conduct are promptly addressed in a fair and impartial manner.”
ST/SGB/2008/5, Sect 3: see below, mechanism for reporting prohibited conduct.Accountability(ST/SGB/2008/5):Staff members are responsible for familiarizing themselves with the Organization’s policy on prohibited conduct and with the various options and internal channels available for addressing such conduct. Staff members are also reminded of the policy introduced by ST/SGB/2005/21 on protection against retaliation for reporting misconduct and for cooperating with duly authorized audits or investigations
Heads of department/office are responsible for the implementation of the present bulletin in their respective departments/offices and for holding all managers and other supervisory staff accountable for compliance with the terms of the present bulletin.Heads of department/office/mission shall ensure that their staff and others for whom they are responsible are provided with a copy of this bulletin upon taking up their appointments. A note acknowledging receipt shall be placed in the staff member’s official status file. Heads of department/office/mission shall also ensure that their staff undertake the required training.
Managers and supervisors have the duty to take prompt and concrete action in response to reports and allegations of prohibited conduct. Failure to take action may be considered a breach of duty and result in administrative action and/or the institution of disciplinary proceedings
ST/IC/2017/17“Staff members are to complete the new mandatory learning programme within six months of the issuance of the present information circular or, in the case of new staff members, within six months of joining the Organization.” Accountability: “Supervisors and heads of departments and offices are responsible for ensuring compliance with mandatory learning requirements and shall allocate sufficient time for staff members to complete them as part of their official duties.”
(ST/SGB/2008/5):In particular, all staff members shall be required to complete the mandatory online training programme onprevention of harassment, sexual harassment and abuse of authority in the workplace, promulgated under ST/SGB/2005/20. The successful completion of this programme shall be reflected in staff members’ performance appraisal.
If there is a need for confidential guidance or advice on matters which could give rise to instances of prohibited conduct, staff members may consult the Office of the Ombudsman or the Office of the Staff Counsellor, which are bound by strict rules of confidentiality under their terms of reference. Staff members may alsoconsult any of the other officials listed in section 5.6 below
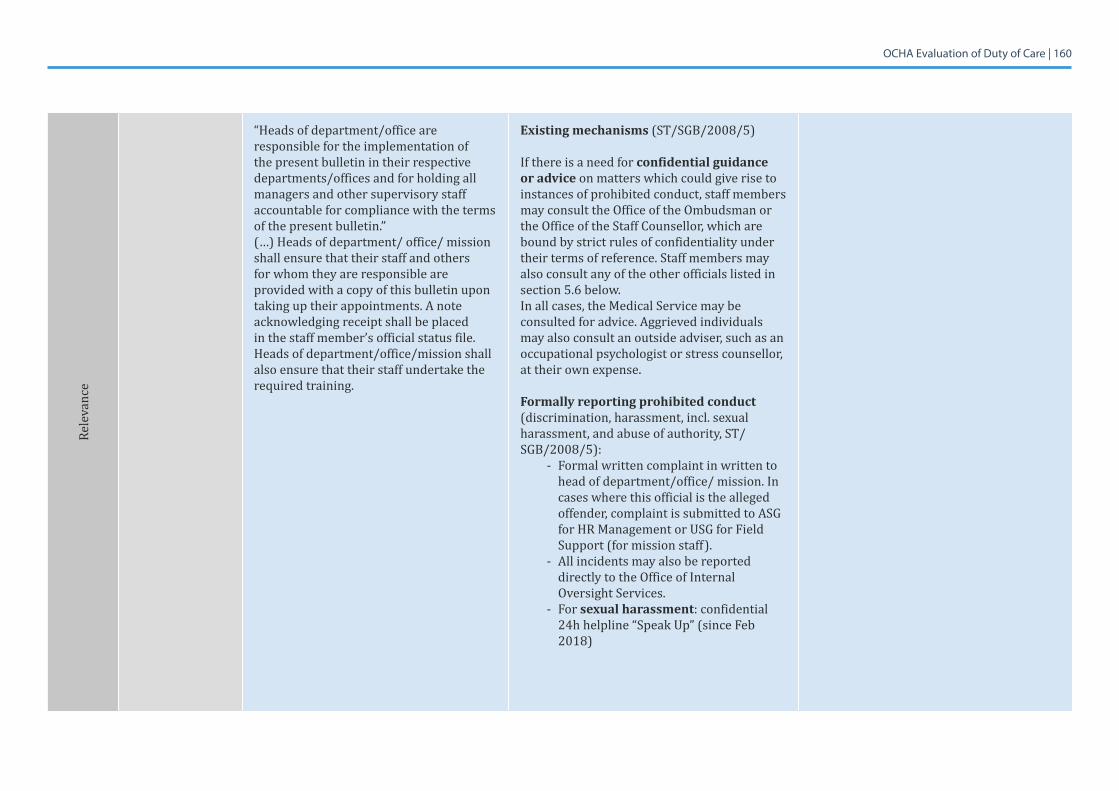
OCHA Evaluation of Duty of Care | 160
Rele
vanc
e
“Heads of department/office are responsible for the implementation of the present bulletin in their respective departments/offices and for holding all managers and other supervisory staff accountable for compliance with the terms of the present bulletin.”(…) Heads of department/ office/ mission shall ensure that their staff and others for whom they are responsible are provided with a copy of this bulletin upon taking up their appointments. A note acknowledging receipt shall be placed in the staff member’s official status file. Heads of department/office/mission shall also ensure that their staff undertake the required training.
Existing mechanisms(ST/SGB/2008/5)
If there is a need for confidential guidance or advice on matters which could give rise to instances of prohibited conduct, staff members may consult the Office of the Ombudsman or the Office of the Staff Counsellor, which are bound by strict rules of confidentiality under their terms of reference. Staff members may also consult any of the other officials listed in section 5.6 below. In all cases, the Medical Service may be consulted for advice. Aggrieved individuals may also consult an outside adviser, such as an occupational psychologist or stress counsellor, at their own expense.
Formally reporting prohibited conduct (discrimination, harassment, incl. sexual harassment, and abuse of authority, ST/SGB/2008/5):
- Formal written complaint in written to head of department/office/ mission. In cases where this official is the alleged offender, complaint is submitted to ASG for HR Management or USG for Field Support (for mission staff).
- All incidents may also be reported directly to the Office of Internal Oversight Services.
- For sexual harassment: confidential 24h helpline “Speak Up” (since Feb 2018)
OCHA Evaluation of Duty of Care | 161
7.8 Annex 8: Online Survey Results
Trends
Rele
vanc
e
Investigation of sexual harassment:On 26 February, the SG announced that OIOS Investigations Division will take responsibility for investigating all complaints of sexual harassment to centralize response capacity. A streamlined, fast-tracked procedure to receive, process and address allegations of sexual harassment is implemented and a specialized team with additional investigators created.
Should the report indicate that the allegations of prohibited conduct were unfounded and based on malicious intent, the Assistant Secretary-General for Human Resources Management shall decide whether disciplinary or other appropriate action should be initiated against the person who made the complaint or report.
Once the investigation has been completed and a decision taken on the outcome, appropriate measures shall be taken by the head of department/office/mission to keep the situation under review.
OCHA Evaluation of Duty of Care | 162
Rele
vanc
e
Quality assurance process
ST/SGB/2008/5:Section6,Monitoring:Head of Department/Office: annual reports to ASG O(?)HRM, incl. preventive and corrective measures taken etc.; copies of all complaints to OHRM for monitoring; annual report DM to SG containing statistics.Also: monitoring during investigation (protection retaliation, see ST/SGB/2017/2/Rev.1), Post-investigation review to ensure implementation, monitor status of all parties concerned.
Once the investigation has been completed and a decision taken on the outcome, appropriate measures shall be taken by the head of department/office/mission to keep the situation under review.
Course assessment/Inspira “control mechanism”
Gender consider-ation present
Yes Yes
Scope:Whois the policy for? (National, International)
All staff, incl. consultants Staff Rules refer to UN Secretariat Staff. As per SGB/2008/5complaintscanbemadebya)anystaff member, b) any other person who may have been subject to harassment by UN staff member c) third party with direct knowledge of the situation
All staff, plus consultants
Documentation describes OCHA specific require-ments beyond applicable UN policies
OCHA People Strategy OCHA covered by UN Secretariat provisions OCHA induction training? Management training?
OCHA Evaluation of Duty of Care | 163
Effic
ienc
y &
Effe
ctiv
enes
s
Describes orientation and preparation process
ST/SGB/2008/5:The Secretary-General shall include in the annual circular informing staff of his practice in disciplinary matters information on cases where discrimination, harassment, including sexual harassment, and abuse of authority have been found. The information circular shall also inform staff of the most common examples of prohibited conduct and their consequences, including any disciplinary or legal action taken, with due regard to the privacy of the staff members concerned.
UN/ DM Factsheet “Taking Action on Sexual Harassment” provides an overview of policies
Informed consent procedures
Oath of Office Oath of Office
Administrative procedures
ST/AI/2017/1, (3.5.d: Administrative instruction – Unsatisfactory conduct, investigations and the disciplinary process)
ST/AI/2017/1, (3.5.d: Administrative instruction – Unsatisfactory conduct, investigations and the disciplinary process)
Communication protocols
ST/SGB/2008/5 ST/SGB/2008/5
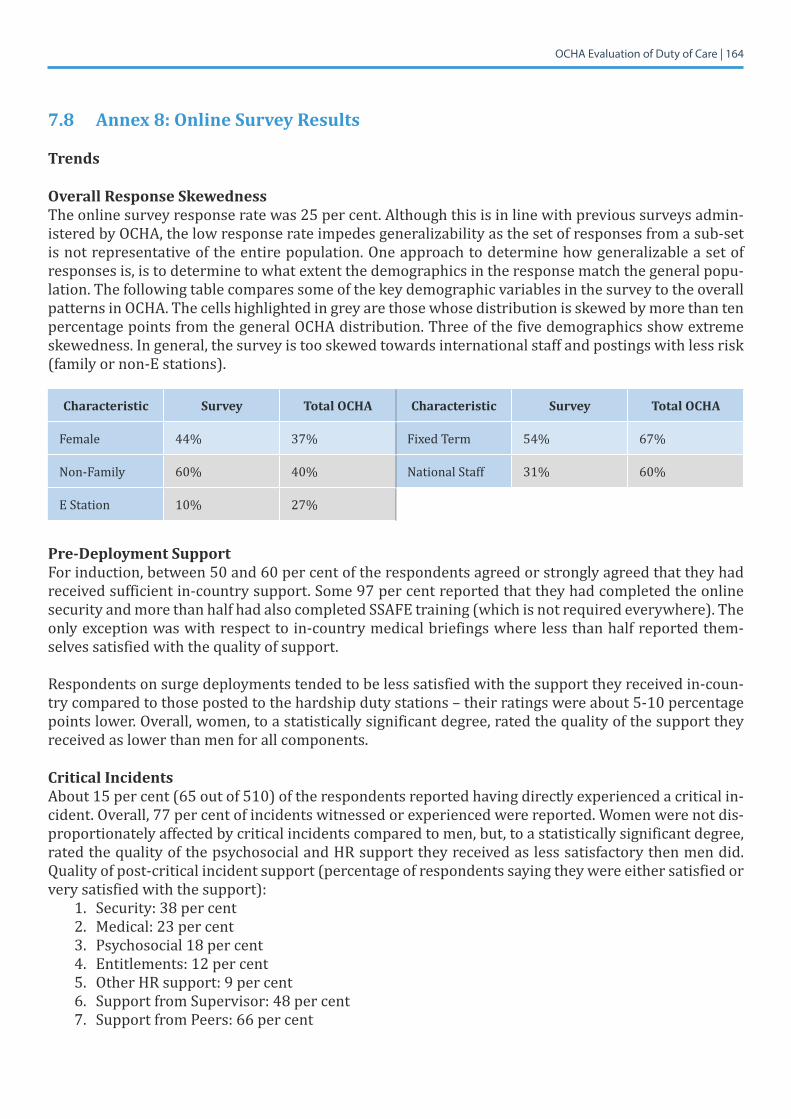
OCHA Evaluation of Duty of Care | 164
7.8 Annex 8: Online Survey Results
Trends
Overall Response SkewednessThe online survey response rate was 25 per cent. Although this is in line with previous surveys admin-istered by OCHA, the low response rate impedes generalizability as the set of responses from a sub-set is not representative of the entire population. One approach to determine how generalizable a set of responses is, is to determine to what extent the demographics in the response match the general popu-lation. The following table compares some of the key demographic variables in the survey to the overall patterns in OCHA. The cells highlighted in grey are those whose distribution is skewed by more than ten percentage points from the general OCHA distribution. Three of the five demographics show extreme skewedness. In general, the survey is too skewed towards international staff and postings with less risk (family or non-E stations).
Characteristic Survey Total OCHA Characteristic Survey Total OCHA
Female 44% 37% Fixed Term 54% 67%
Non-Family 60% 40% National Staff 31% 60%
E Station 10% 27%
Pre-Deployment SupportFor induction, between 50 and 60 per cent of the respondents agreed or strongly agreed that they had received sufficient in-country support. Some 97 per cent reported that they had completed the online security and more than half had also completed SSAFE training (which is not required everywhere). The only exception was with respect to in-country medical briefings where less than half reported them-selves satisfied with the quality of support.
Respondents on surge deployments tended to be less satisfied with the support they received in-coun-try compared to those posted to the hardship duty stations – their ratings were about 5-10 percentage points lower. Overall, women, to a statistically significant degree, rated the quality of the support they received as lower than men for all components.
Critical IncidentsAbout 15 per cent (65 out of 510) of the respondents reported having directly experienced a critical in-cident.Overall,77percentofincidentswitnessedorexperiencedwerereported.Womenwerenotdis-proportionately affected by critical incidents compared to men, but, to a statistically significant degree, rated the quality of the psychosocial and HR support they received as less satisfactory then men did. Quality of post-critical incident support (percentage of respondents saying they were either satisfied or very satisfied with the support):
1. Security:38percent2. Medical: 23 per cent3. Psychosocial18percent4. Entitlements: 12 per cent5. Other HR support: 9 per cent6. SupportfromSupervisor:48percent7. Support from Peers: 66 per cent
OCHA Evaluation of Duty of Care | 165
The highest-rated satisfaction came from support from their peers followed by their supervisors’ sup-port. HR support after a critical incident was rated extremely low with only about 9-12 per cent rating the quality of the support satisfactory or very satisfactory.
General OCHA SupportWithregardtogeneralsupport(notrelatedtocriticalincidents),respondentsratedsecuritythehigh-est in terms of quality of support and HR support the lowest. Quality of OCHA support (percentage of respondents saying they were either satisfied or very satisfied with the support):
1. Security: 65 per cent2. Medical: 57 per cent3. Psychosocial: 32 per cent4. Housing: 36 per cent5. Workingspace:55percent6. Entitlements: 34 per cent
There was a statistically significant difference in ratings between those in family compared to non-fami-ly duty stations. Personnel in non-family duty stations tended to rate medical, security, and psychosocial supportlower.Womenagainhadastatisticallysignificantdifferencewithmorenegativeratingscom-pared to men on the perceived quality of psychosocial support, working office, and entitlements and benefits.
Work EnvironmentPercentage of respondents saying they were either positive or very positive concerning the environ-ment:
1. Respectful: 66 per cent2. Harassment Free: 62 per cent3. Discrimination Free: 52 per cent4. Stressed: 45 per cent5. Staff all can Advance: 27 per cent6. WomenOpportunities:41percent
7. WitnessedHarassment:35percent8. ReportedIncidents:41percent9. Satisfied with Measures: 12 per cent
10.Knowwheretoreport:89percent(26percentdidnotanswerthequestion)11.WouldbeProtectedifdidreport:27percent
Interestingly, a large majority of respondents (60%+) rated their work environment as being respectful or harassment-free, and only 45 per cent rated themselves as stressed. More negatively, less than half felt that women had equal opportunities for advancement and very few felt that staff of all nationalities had equal opportunities for advancement.
Of some concern, more than a third of the respondents reported experiencing or witnessing harassment in the workplace, less than half reported the incidents and only 12 per cent reported themselves satis-fied with the actions taken. Primary reasons for not reporting incidents were that the respondents felt there was a lack of evidence, did not feel that any action would be taken or were not sure of the proce-dures.
OCHA Evaluation of Duty of Care | 166
Worryingly,whilealargemajoritystatedthattheyknewthereportingmechanisms,only27percentsaid that they felt that they would be protected from retaliation if they reported an incident.
Type of duty station did not affect the responses in terms of work environment. However, women were consistently more negative than men on their assessment of the workplace, opportunities for advance-ment, experiencing harassment or being protected if reporting an incident. There was no difference between men and women on feeling stressed.
Heads and Deputy Heads of Offices and Factors Affecting Duty of CareHeads and Deputy Heads of Offices comprised about 7 per cent of the responses. However, in their as-sessment the factors that impeded good duty of care in OCHA were (per cent who said it was a signifi-cant or very significant factor):
1. Policiesunclear:82percent2. Roles, responsibilities unclear: 76 per cent3. Insufficient training on DOC management: 94 per cent4. InsufficientbudgetforDOC:85percent5. Administrativeprocessesnotsupportive:85percent6. Procurementprocesses:80percent
Essentially, all elements listed were considered factors that were limiting OCHA’s duty of care.
Frequency Distributions - Narrative
Demographics (questions 21-17)Almost half of all respondents are male, 44 per cent female, and the remainder did not answer. Some 22 per cent have worked at OCHA for over 10 years, 42 per cent between 4 and 10 years, and 31 per centunder3years.Whilethemajority(54percent)haveafixed-termcontract,17percentworkona permanent or continuous basis, and one in ten is on a temporary appointment. The representation is highest at the P4 (21 per cent) and P3 (21 per cent) grades, followed by the General Service (10 per cent). Some 37 per cent of respondents are based in a country office (main office), a quarter works in headquarters, and 19 per cent are based in sub-offices. The majority of participants work at a family duty station (66 per cent), compared to a quarter who work at a non-family duty station, out of whom almost one-fourth are based in Africa and 17 per cent in the Middle East.
Security Risk Management in High-Risk Environments (1-8)Some 59 per cent of those who took the survey are either based in or have travelled to a non-family duty station over the last three years. Almost all of them (97 per cent) have completed the online security trainings (Basic and Advanced Security in the Field) before their assignment, and 49 per cent have com-pleted additional security trainings, such as SSAFE or in-person briefings. The majority (63 per cent) of those who are based in or have travelled to non-family duty stations agree that they have been suffi-ciently informed of the safety, security and health risks of the location, while almost a quarter disagree. Some 35 per cent agree that they have been sufficiently informed of support services and entitlements available to them, compared to 46 per cent who disagree. Among respondents, 56 per cent believe they received sufficient administrative support and 60 per cent in-country safety, security and other rele-vantbriefingsuponarrival,comparedto28percentand27percentwhodisagreerespectively.Athirdagrees that they received sufficient in-country medical and other relevant briefings upon arrival, com-pared to 45 per cent who disagree. The majority (66 per cent) believes they received necessary security equipment, compared to 24 per cent who disagree.
OCHA Evaluation of Duty of Care | 167
Less than half (47 per cent) of all respondents have been exposed – directly or indirectly – to an incident where there was a potential for death or severe injury while on OCHA duty, and most incidents (77 per cent)werereported.Outofthosewhoexperiencedsuchincidents,38percentfoundthesecurity-relat-ed support to be good or very good, compared to 29 per cent who found it poor or very poor. About 23 per cent received good or very good for medical support compared to 25 per cent who rated such sup-port as poor or very poor. 19 per cent received good or very good for psychosocial support compared to 48percentwhoratedsuchsupportaspoororverypoor.Entitlementsandbenefitswereseenasgoodby1in8(12percent)andpoorbyalmostathird(30percent),whereasotherHRsupportwasratedas good by 9 per cent and poor by every second respondent (49 per cent). In contrast, general support fromsupervisorswasratedasgoodby48percent,andsupportbypeersby66percent.
Whenaskedaboutthingsthatstaffrequiredbutdidnotreceive,themostcommonaspectsincludedinformation regarding entitlements and services, security and medical briefings prior to deployment, administrative support especially upon induction, e.g. regarding accommodation, more efficient and responsive administration, and provision of adequate security equipment, such as vests and satellite phones.
Health and Welfare (9 -12)The majority (62 per cent) of respondents can access adequate medical care in case of illness or injury, however, 23 per cent had difficulties and 12 per cent were not able to get access at all. Half of all re-spondents know how to access counselling, psychological or psychosocial support if needed compared to 21 per cent who do not. Security-related support was rated as good or very good by 64 per cent, compared to 11 per cent for poor and very poor. Medical support was rated as good or very good by 57 per cent compared to 16 per cent for poor and very poor. Psychosocial support was rated 32 per cent as good or very good compared to 26 per cent who found it poor or very poor. Housing accommodation was rated as good by 36 per cent and poor by 20 per cent. Office space was rated good by 46 per cent as poor by 17 per cent. Every 1 in 3 (34 per cent) rated entitlements and benefits as good compared to a fifth who rated them as poor, and 22 per cent rated other HR support measures as good compared to 32 per cent who rated them as poor.
Further comments with regards to additional requirements that were not available included informa-tion and guidance regarding entitlements, mobility and accommodation, access to psychological sup-port and medical resources, better security equipment, a more responsive and transparent administra-tion, equal treatment between international and local staff, and adequate office space.
Working Environment (13-16)Almost half of all respondents (46 per cent) found their work environment respectful; almost 1 in 5 (19 per cent) disagreed. Majorities agreed that their work environment is free from harassment (62 per cent)anddiscrimination(52percent),comparedto21percentand28percent,respectively,whodis-agreed. Almost one third (31 per cent) often feel stressed and overwhelmed in their current job, com-paredto30percentwhodonotfeelthatway.While28percentbelievethatstaffofallnationalitieshavethe same opportunities to advance in OCHA, over half (51 per cent) disagree, including 27 per cent who strongly disagree. In contrast, 41 per cent believes that women and men have the same opportunities to advance in OCHA, compared to 35 per cent who were of opposite opinions.
Of those who took the survey, 35 per cent have either personally experienced harassment (including but not limited to sexual harassment) at OCHA, witnessed it, or both. Of those 41 per cent reported the case, while the rest cited fears of retaliation or of being seen as a whistle-blower, as well as the lack of a clear reporting mechanism, as reasons for not reporting harassment. However, the majority (65 per cent) have not experienced nor witnessed harassment at the workplace while at OCHA. Every 6 out of
OCHA Evaluation of Duty of Care | 168
10 are not satisfied that appropriate measures were taken to address the issue, with some stating that sometimes no action was taken at all. The majority of respondents (67 per cent) would know what to do if they were to experience or witness harassment, including sexual harassment, and what to do and whomtoapproachtoreportit.Some28percentbelievetheywouldbeprotectedfromretaliationiftheywere to witness and report misconduct in OCHA, while 43 per cent do not believe this.
In addition, in the comments section some respondents mentioned discrimination between women and men, international and national staff as well as between those on short-term and fixed-term contracts, bad work-life balance, and the need to improve diversity, especially at the headquarters.
Summation (17-27)Some 7 per cent of all respondents are a Head or Deputy Head of Office, out of whom 41 per cent per-ceived unclear policies, roles and responsibilities related to duty of care (DOC) as very significant con-straints when considering OCHA’s DOC, while more than one third thought they were somewhat sig-nificant constraints. Some 56 per cent perceived insufficient provision of training and and 62 per cent perceived insufficient budget for DOC as very significant constraints, while almost 6 out of 10 (59 per cent) believed that administration processes are insufficiently supportive of DOC needs. Half of all who took the survey agree that procurement processes impede adequate DOC. Further constraints included lack of clear reporting channels in cases of harassment, a cumbersome administrative process and une-qual access to DOC between HQ and field staff.
All respondents were asked about additional observations. The main themes that emerged include the need for more information sharing, the need to improve staff welfare as well as mobility or rotation, new staff need more guidance upon induction, UNDSS capacity is overwhelmed and that short-term contracts cause instability and stress.
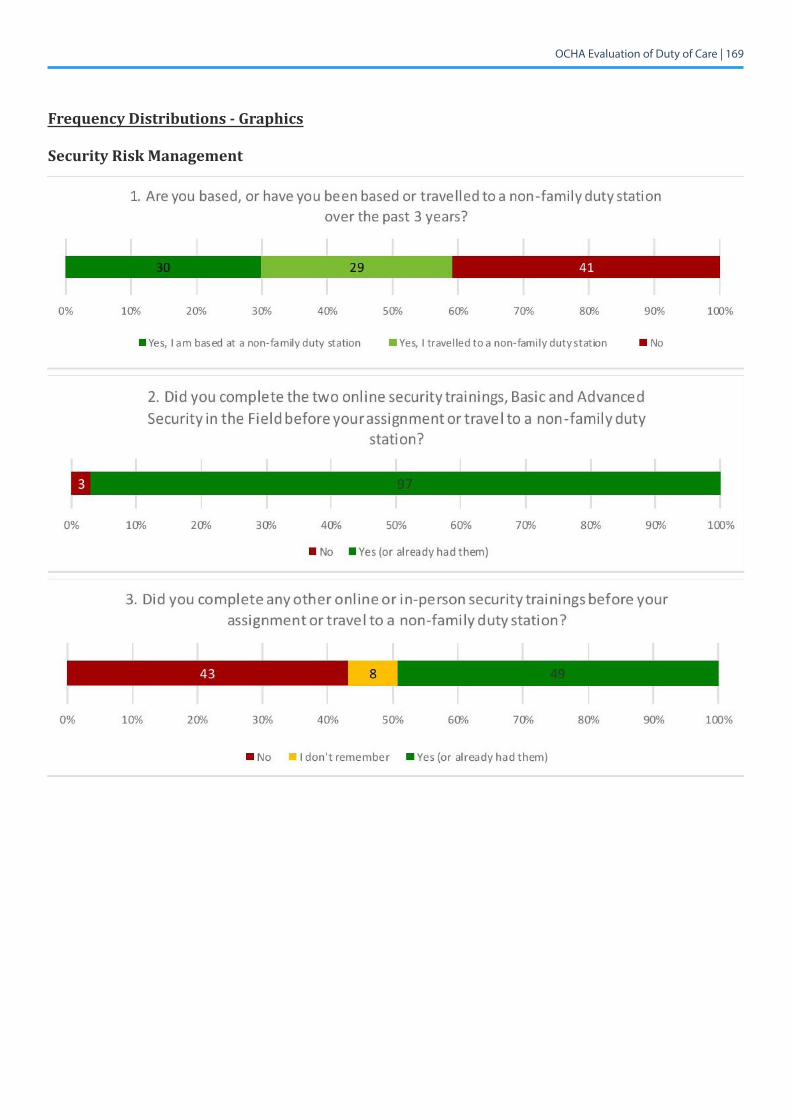
OCHA Evaluation of Duty of Care | 169
Frequency Distributions - Graphics
Security Risk Management
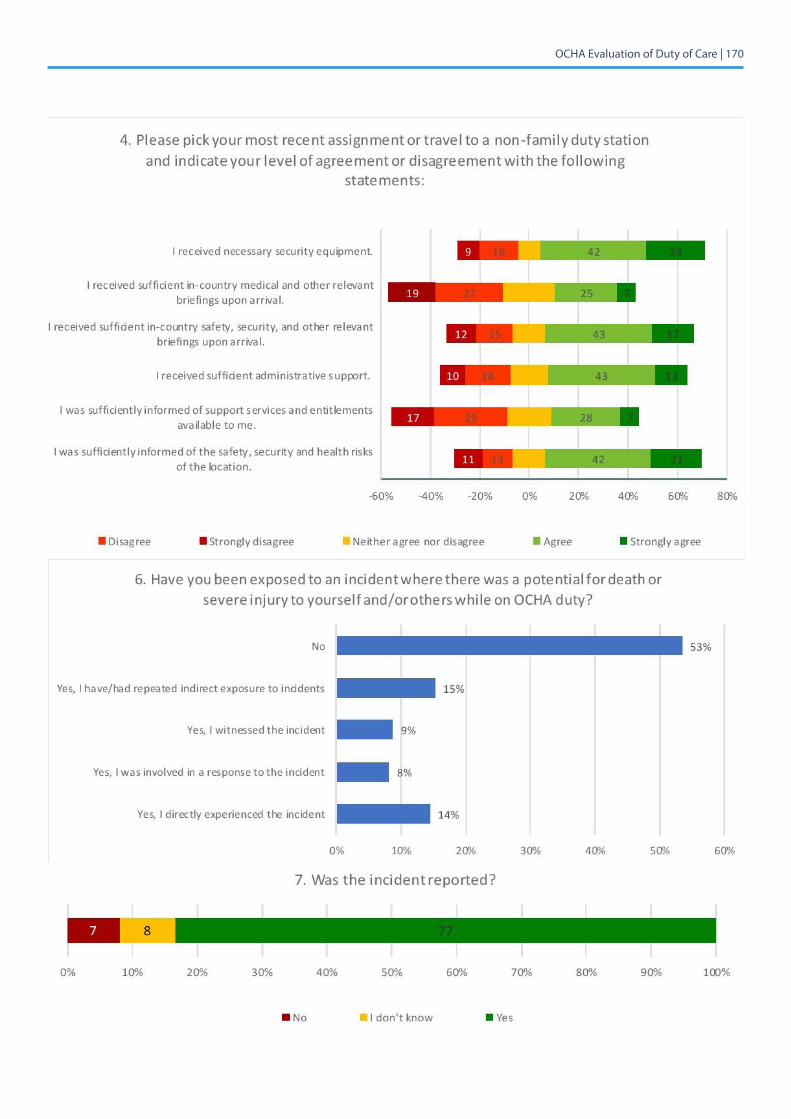
OCHA Evaluation of Duty of Care | 170
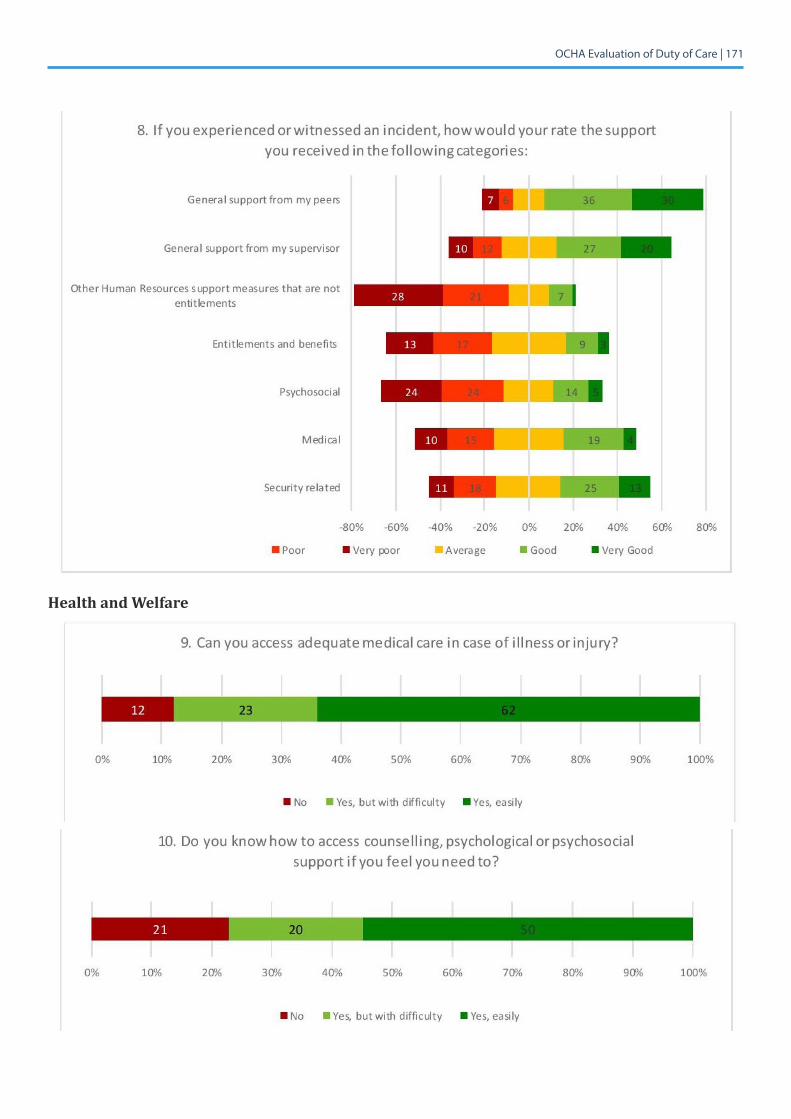
OCHA Evaluation of Duty of Care | 171
Health and Welfare
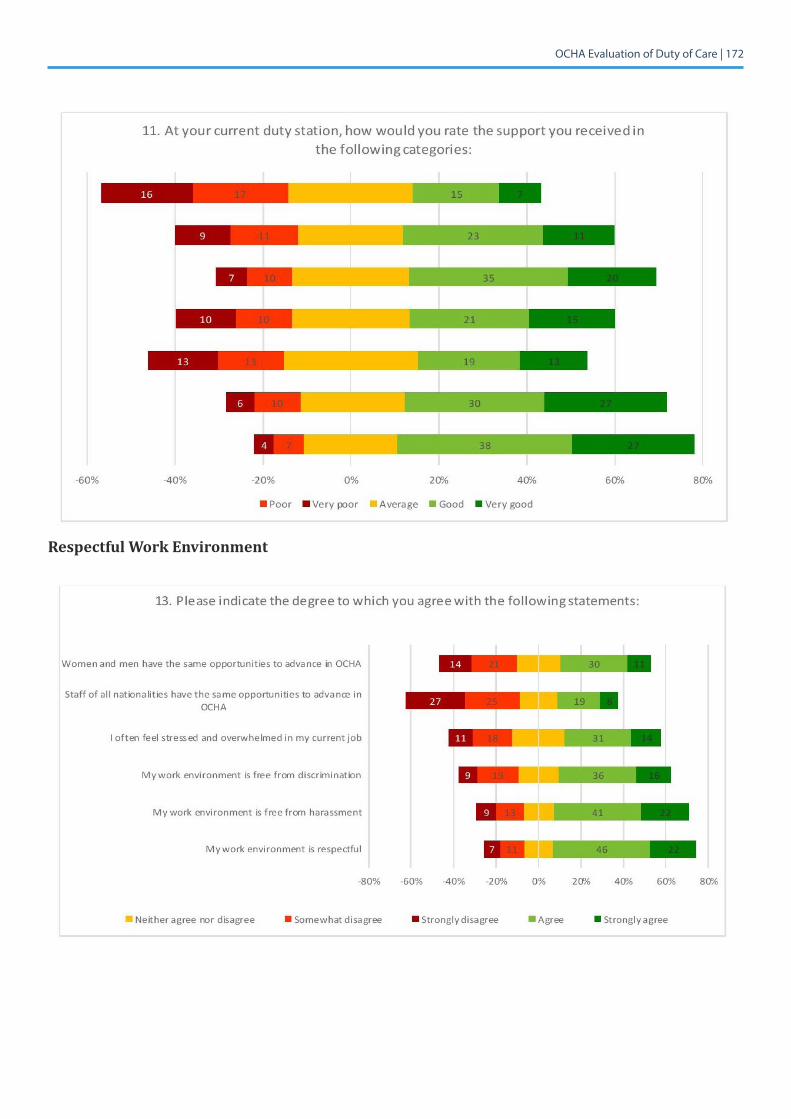
OCHA Evaluation of Duty of Care | 172
Respectful Work Environment
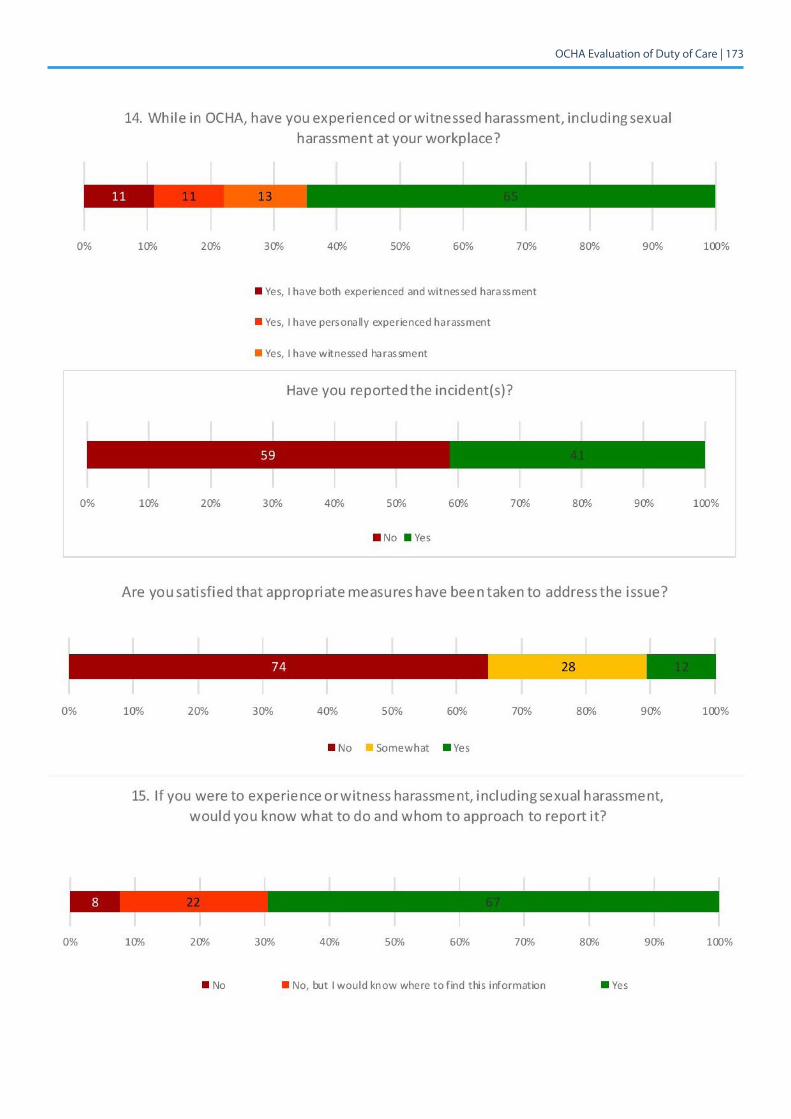
OCHA Evaluation of Duty of Care | 173
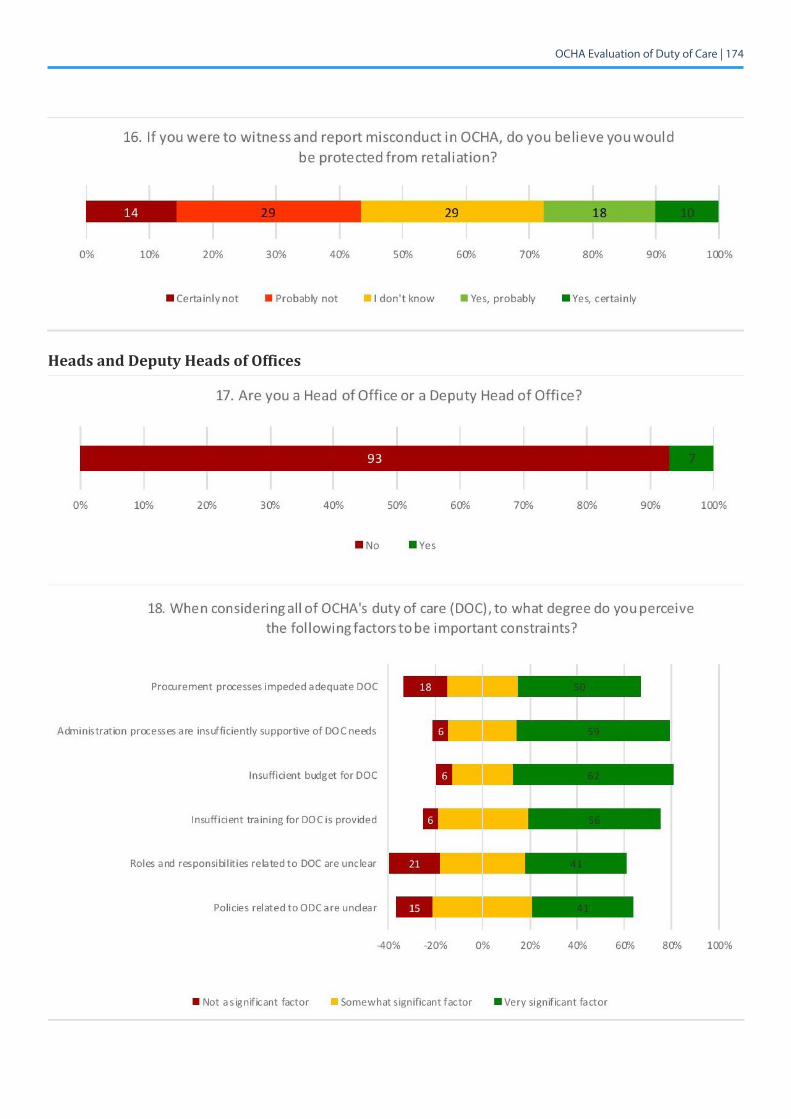
OCHA Evaluation of Duty of Care | 174
Heads and Deputy Heads of Offices
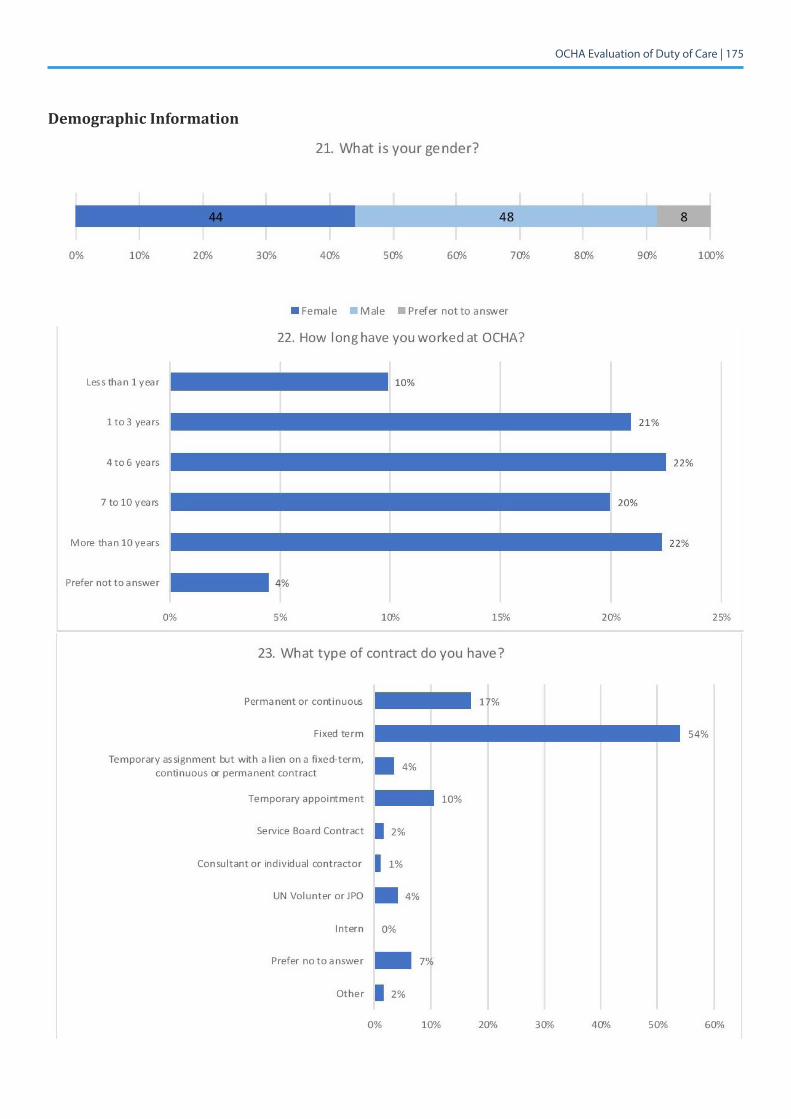
OCHA Evaluation of Duty of Care | 175
Demographic Information
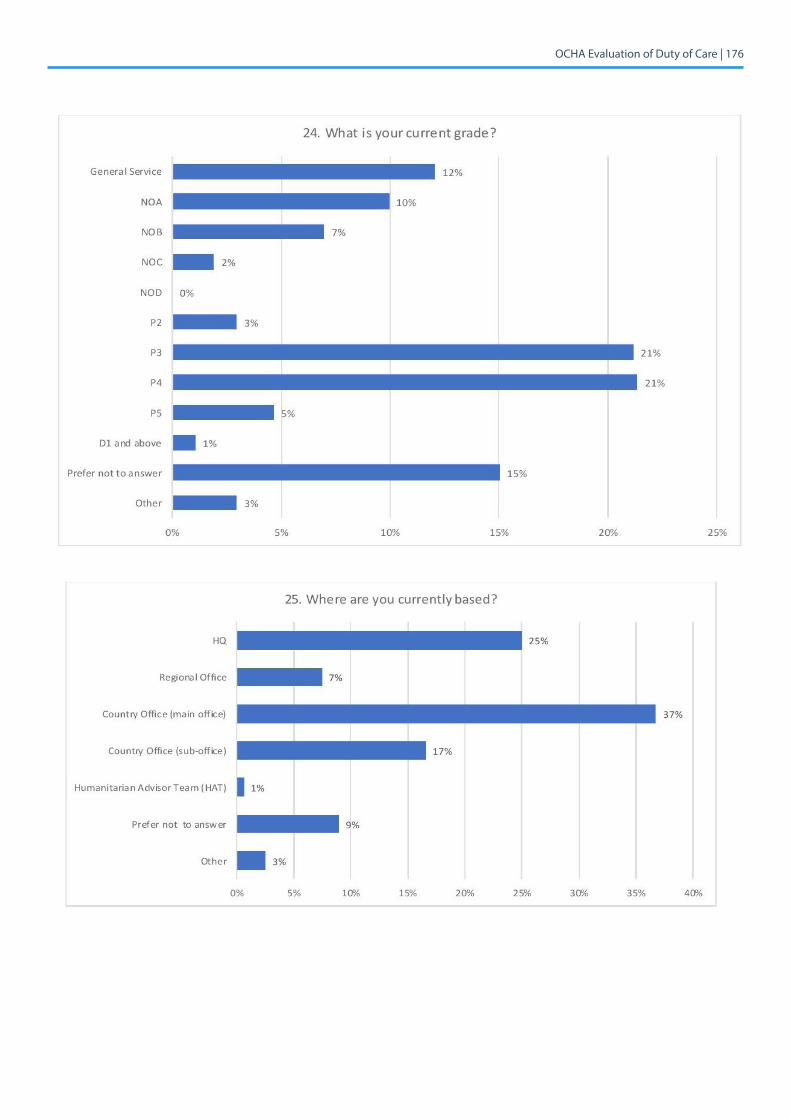
OCHA Evaluation of Duty of Care | 176
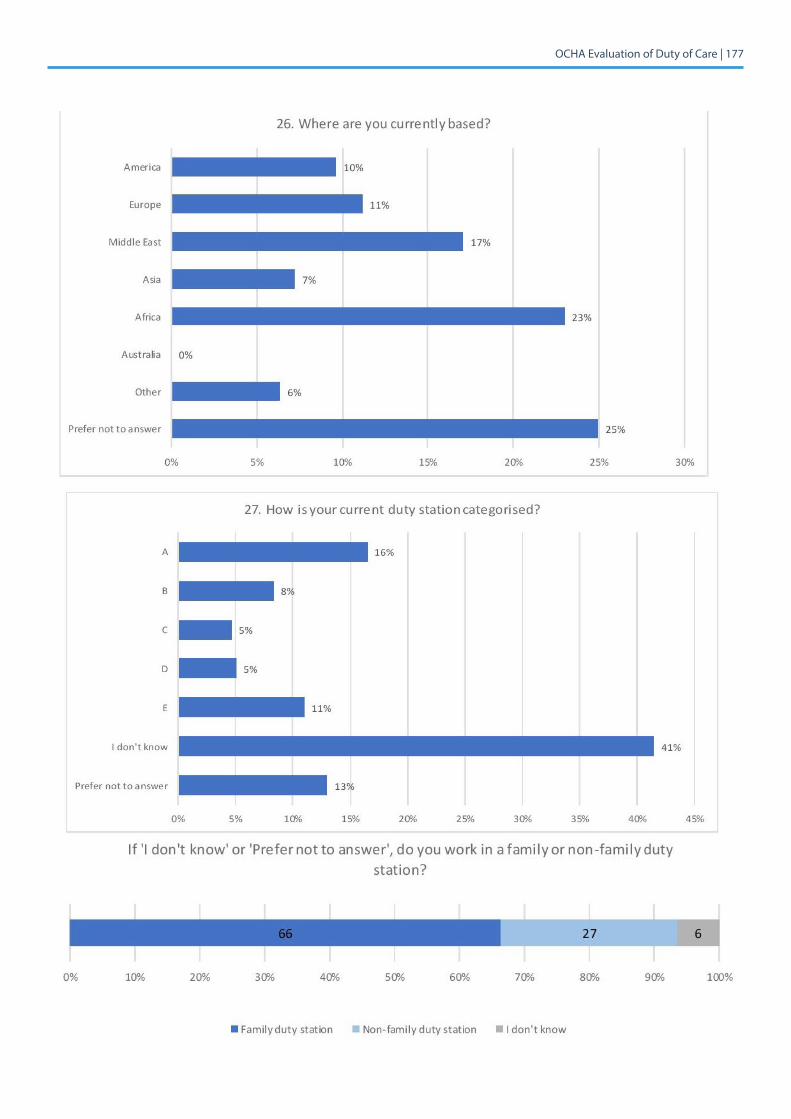
OCHA Evaluation of Duty of Care | 177
OCHA Evaluation of Duty of Care | 178
7.9 Annex 9: Other Quantitative Surveys
Surveys reviewed are the UN Staff Engagement Survey 2017 commissioned by the Department of Man-agement in the UN Secretariat,1 the UN Staff Union Survey 2017,2 and the Functional Review OCHA Satisfaction Survey 2016.3
Summary of Engagement and Functional Reviews: Across all the surveys, results showed pride in work and a strong belief in the organization’s values by the workforce. One of the major concerns voiced by staff was the lack of support of learning, skill development and career opportunities. In OCHA, a staff survey on organizational culture4 was carried out in the context of the Functional Review in 2016: 35% of respondents did not feel they received the support they need for learning and professional develop-ment.
WhileOCHAstaffinthesurveygenerallyshowedastrongbeliefintheorganization’svalues,theyatthesame time believed that adherence to these values was generally low – only 39 per cent thought that there were consequences for non-adherence. Another critical issue concerned performance manage-ment and recognition. In general, respondents believed that poor performance was tolerated and strong performance not rewarded: 51 per cent of respondents did not believe that promotion was clearly tied to performance. Respondents on average thought that the organizational culture was characterized by moderation, also in the sense that there were concerns about challenging senior leaders.
The Staff Engagement Survey of December 2017 among Secretariat staff covered work environment and several other areas defining conditions for an organization’s success.5 The response rate was 39 per cent. Regarding the organizational culture, one third of respondents indicated that they do not feel comfortable challenging the status quo and feel a lack of performance and ethical accountability. Some 64 per cent of respondents indicated feeling valued as a staff member. About 63 per cent of respondents felt they were able to maintain a healthy work/life balance, 24 per cent of the respondents experienced unacceptable levels of job stress. The incongruity between performance and success showed again in more than half of the respondents not believing that by performing consistently well they will have a successful career.
Asfordiversityandequalityamongstaff,83percentofrespondentsansweredfavourablytotheques-tion whether staff of diverse racial, cultural and religious backgrounds were respected in their depart-ments/offices/missions. There was slightly less belief that man and women are treated equally in the workplace (72%). In particular, female staff assessed gender equality significantly less favourably than men (62% versus 79%).6 Similarly, and women and men felt differently about whether their manager actively empowers women in the workplace (62% versus 77% – 71% overall).
[1] UnitedNationsandCEB[Gartner].(2018).UnitedNationsStaffEngagementSurvey:UNSecretariatSurveyResults.UN-internaldocument.Alsoseehttp://webtv.un.org/en/ga/watch/martha-helena-lopez-ohrm-on-the-staff-engagement-survey-press-conference-5-march-2018/5745358919001/?term=&page=5?lanenglish(accessed18April2018)[2] Seehttp://www.ccisua.org/2017/03/02/results-un-global-staff-satisfaction-survey-2017-now/(accessed18April2018)[3] Mannet&TheBostonConsultingGroup.(29July2016).OCHAFunctionalReview.OCHA-internaldocument.[4] Theanonymoussurveycoveredthethreeareasengagement,behavioursatworkandstafffeedback.TheresponserateamongOCHAstaffwasabout50 per cent.[5] Inadditiontotheuniversalmeasuresof“Engagement”,“Alignment”and“Agility”,areasofpriority fortheUNtoreach itsorganizationalobjectives(“Continuous Improvement”, “Gender Diversity” were also covered). As part of the analysis, results were compared to CEB’s Public Sector Norm as external benchmark.[6] Malerespondentstothesurveyingeneralexpressedmorefavourableopinionsthanfemalerespondents,theaveragedifferencebetweenthegroupsamountingto11percentagepoints.Therewasalsosignificantvariationinfavourableopinionsacrosscategoriesofstaff,withGeneralServiceandNationalOfficerstaffexpressingmorefavourableopinions,professionalstafftheleastfavourable–theaveragedifferencebetweencategoriesbeing27percentagepoints. On average non-managers’ perception was more favourable than managers’ – especially in the category of work/life balance, non-managers were 13 percentage points more favourable.
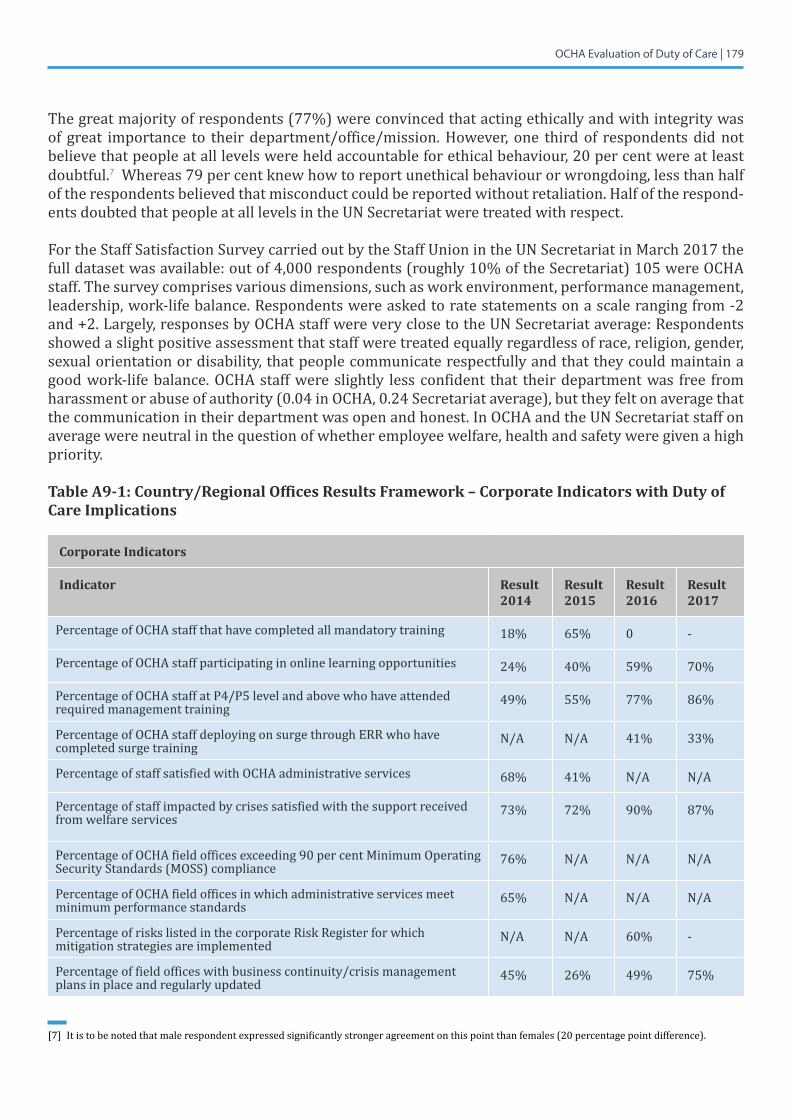
OCHA Evaluation of Duty of Care | 179
The great majority of respondents (77%) were convinced that acting ethically and with integrity was of great importance to their department/office/mission. However, one third of respondents did not believe that people at all levels were held accountable for ethical behaviour, 20 per cent were at least doubtful.7Whereas79percentknewhowtoreportunethicalbehaviourorwrongdoing,lessthanhalfof the respondents believed that misconduct could be reported without retaliation. Half of the respond-ents doubted that people at all levels in the UN Secretariat were treated with respect.
For the Staff Satisfaction Survey carried out by the Staff Union in the UN Secretariat in March 2017 the full dataset was available: out of 4,000 respondents (roughly 10% of the Secretariat) 105 were OCHA staff. The survey comprises various dimensions, such as work environment, performance management, leadership, work-life balance. Respondents were asked to rate statements on a scale ranging from -2 and +2. Largely, responses by OCHA staff were very close to the UN Secretariat average: Respondents showed a slight positive assessment that staff were treated equally regardless of race, religion, gender, sexual orientation or disability, that people communicate respectfully and that they could maintain a good work-life balance. OCHA staff were slightly less confident that their department was free from harassment or abuse of authority (0.04 in OCHA, 0.24 Secretariat average), but they felt on average that the communication in their department was open and honest. In OCHA and the UN Secretariat staff on average were neutral in the question of whether employee welfare, health and safety were given a high priority.
Table A9-1: Country/Regional Offices Results Framework – Corporate Indicators with Duty of Care Implications
Corporate Indicators
Indicator Result 2014
Result 2015
Result 2016
Result 2017
Percentage of OCHA staff that have completed all mandatory training 18% 65% 0 -
Percentage of OCHA staff participating in online learning opportunities 24% 40% 59% 70%
Percentage of OCHA staff at P4/P5 level and above who have attended required management training
49% 55% 77% 86%
Percentage of OCHA staff deploying on surge through ERR who have completed surge training
N/A N/A 41% 33%
Percentage of staff satisfied with OCHA administrative services 68% 41% N/A N/A
Percentage of staff impacted by crises satisfied with the support received from welfare services
73% 72% 90% 87%
Percentage of OCHA field offices exceeding 90 per cent Minimum Operating Security Standards (MOSS) compliance
76% N/A N/A N/A
Percentage of OCHA field offices in which administrative services meet minimum performance standards
65% N/A N/A N/A
Percentage of risks listed in the corporate Risk Register for which mitigation strategies are implemented
N/A N/A 60% -
Percentage of field offices with business continuity/crisis management plans in place and regularly updated
45% 26% 49% 75%
[7] Itistobenotedthatmalerespondentexpressedsignificantlystrongeragreementonthispointthanfemales(20percentagepointdifference).
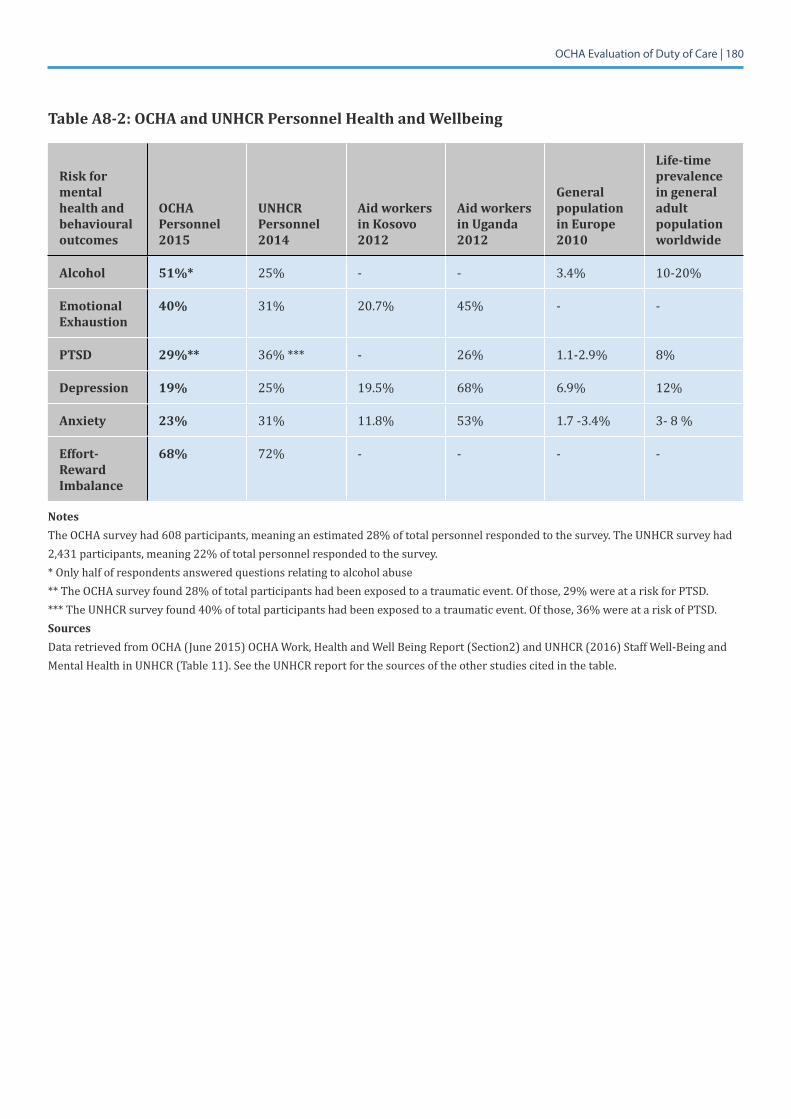
OCHA Evaluation of Duty of Care | 180
Table A8-2: OCHA and UNHCR Personnel Health and Wellbeing
Risk for mental health and behavioural outcomes
OCHA Personnel 2015
UNHCR Personnel 2014
Aid workers in Kosovo2012
Aid workers in Uganda2012
General population in Europe 2010
Life-time prevalence in general adult population worldwide
Alcohol 51%* 25% - - 3.4% 10-20%
Emotional Exhaustion
40% 31% 20.7% 45% - -
PTSD 29%** 36% *** - 26% 1.1-2.9% 8%
Depression 19% 25% 19.5% 68% 6.9% 12%
Anxiety 23% 31% 11.8% 53% 1.7 -3.4% 3-8%
Effort-Reward Imbalance
68% 72% - - - -
NotesTheOCHAsurveyhad608participants,meaninganestimated28%oftotalpersonnelrespondedtothesurvey.TheUNHCRsurveyhad2,431 participants, meaning 22% of total personnel responded to the survey.* Only half of respondents answered questions relating to alcohol abuse**TheOCHAsurveyfound28%oftotalparticipantshadbeenexposedtoatraumaticevent.Ofthose,29%wereatariskforPTSD.*** The UNHCR survey found 40% of total participants had been exposed to a traumatic event. Of those, 36% were at a risk of PTSD.SourcesDataretrievedfromOCHA(June2015)OCHAWork,HealthandWellBeingReport(Section2)andUNHCR(2016)StaffWell-BeingandMental Health in UNHCR (Table 11). See the UNHCR report for the sources of the other studies cited in the table.
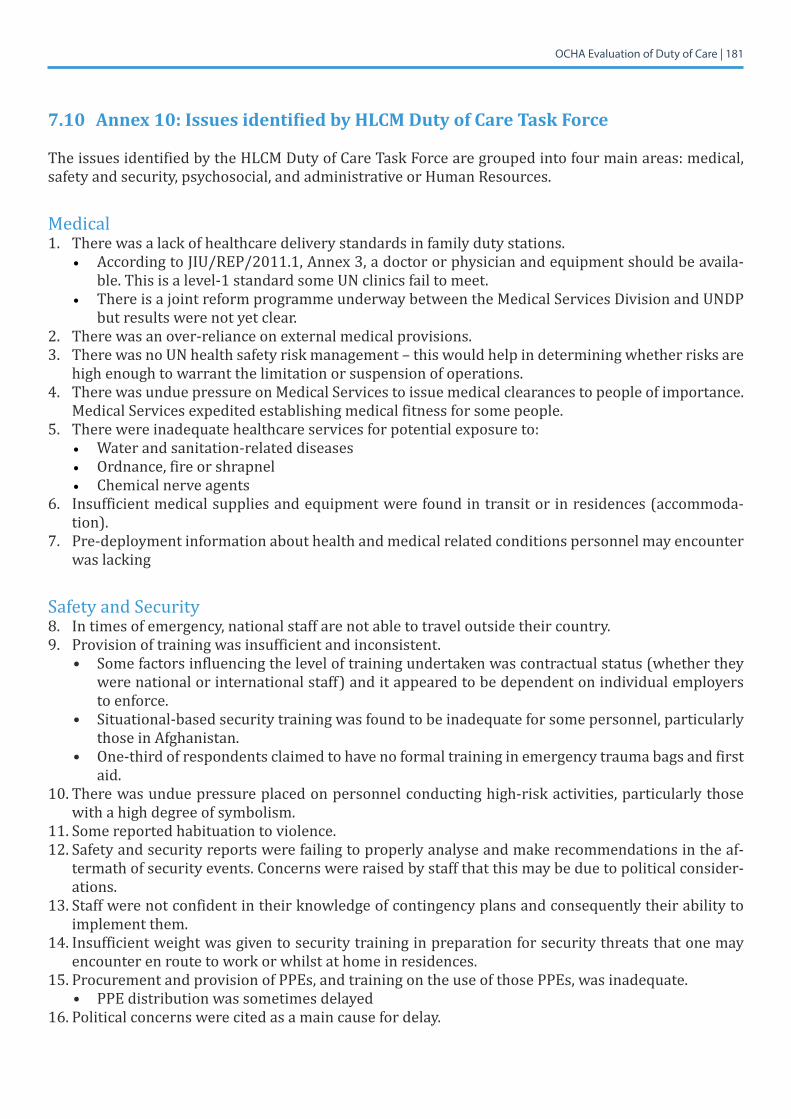
OCHA Evaluation of Duty of Care | 181
7.10 Annex10:IssuesidentifiedbyHLCMDutyofCareTaskForce
The issues identified by the HLCM Duty of Care Task Force are grouped into four main areas: medical, safety and security, psychosocial, and administrative or Human Resources.
Medical 1. There was a lack of healthcare delivery standards in family duty stations.
• According to JIU/REP/2011.1, Annex 3, a doctor or physician and equipment should be availa-ble. This is a level-1 standard some UN clinics fail to meet.
• There is a joint reform programme underway between the Medical Services Division and UNDP but results were not yet clear.
2. There was an over-reliance on external medical provisions. 3. There was no UN health safety risk management – this would help in determining whether risks are
high enough to warrant the limitation or suspension of operations. 4. There was undue pressure on Medical Services to issue medical clearances to people of importance.
Medical Services expedited establishing medical fitness for some people.5. There were inadequate healthcare services for potential exposure to:
• Waterandsanitation-relateddiseases• Ordnance, fire or shrapnel • Chemical nerve agents
6. Insufficient medical supplies and equipment were found in transit or in residences (accommoda-tion).
7. Pre-deployment information about health and medical related conditions personnel may encounter was lacking
Safety and Security 8. Intimesofemergency,nationalstaffarenotabletotraveloutsidetheircountry.9. Provision of training was insufficient and inconsistent.
• Some factors influencing the level of training undertaken was contractual status (whether they were national or international staff) and it appeared to be dependent on individual employers to enforce.
• Situational-based security training was found to be inadequate for some personnel, particularly those in Afghanistan.
• One-third of respondents claimed to have no formal training in emergency trauma bags and first aid.
10. There was undue pressure placed on personnel conducting high-risk activities, particularly those with a high degree of symbolism.
11. Some reported habituation to violence.12. Safety and security reports were failing to properly analyse and make recommendations in the af-
termath of security events. Concerns were raised by staff that this may be due to political consider-ations.
13. Staff were not confident in their knowledge of contingency plans and consequently their ability to implement them.
14. Insufficient weight was given to security training in preparation for security threats that one may encounter en route to work or whilst at home in residences.
15. Procurement and provision of PPEs, and training on the use of those PPEs, was inadequate.• PPE distribution was sometimes delayed
16. Political concerns were cited as a main cause for delay.
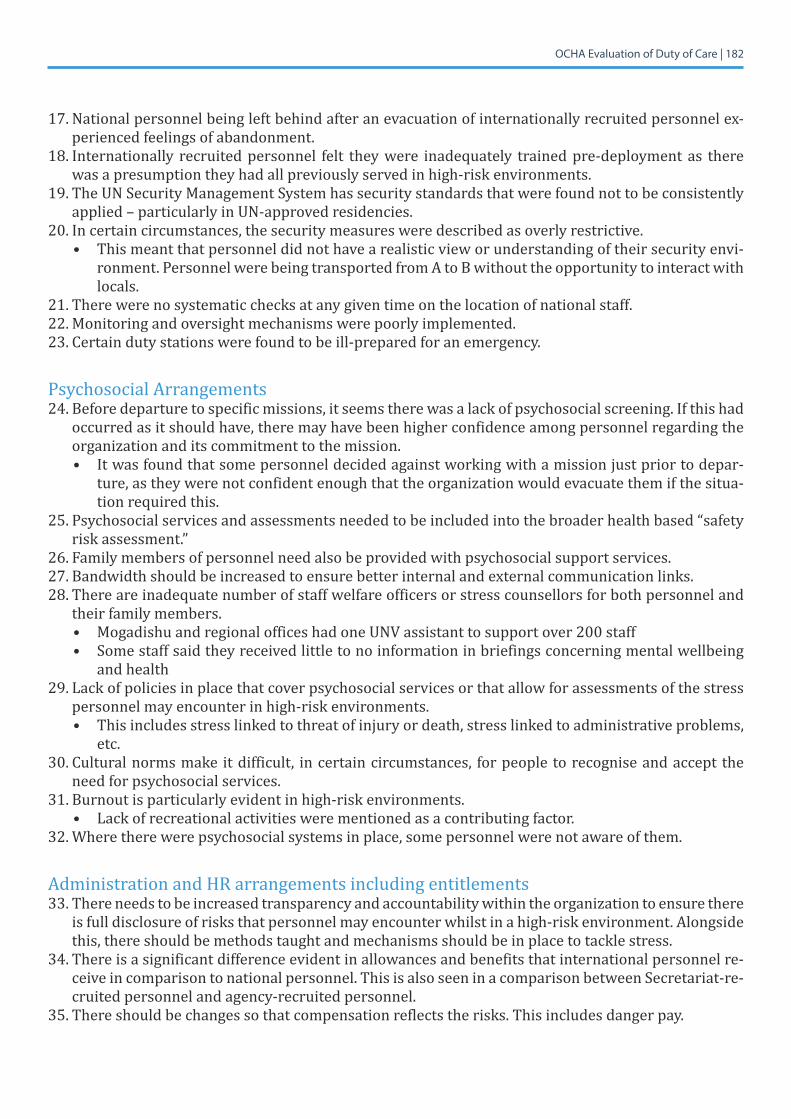
OCHA Evaluation of Duty of Care | 182
17. National personnel being left behind after an evacuation of internationally recruited personnel ex-perienced feelings of abandonment.
18.Internationally recruitedpersonnel felt theywere inadequately trainedpre-deploymentas therewas a presumption they had all previously served in high-risk environments.
19. The UN Security Management System has security standards that were found not to be consistently applied – particularly in UN-approved residencies.
20. In certain circumstances, the security measures were described as overly restrictive.• This meant that personnel did not have a realistic view or understanding of their security envi-
ronment. Personnel were being transported from A to B without the opportunity to interact with locals.
21. There were no systematic checks at any given time on the location of national staff.22. Monitoring and oversight mechanisms were poorly implemented.23. Certain duty stations were found to be ill-prepared for an emergency.
Psychosocial Arrangements 24. Before departure to specific missions, it seems there was a lack of psychosocial screening. If this had
occurred as it should have, there may have been higher confidence among personnel regarding the organization and its commitment to the mission.• It was found that some personnel decided against working with a mission just prior to depar-
ture, as they were not confident enough that the organization would evacuate them if the situa-tion required this.
25. Psychosocial services and assessments needed to be included into the broader health based “safety risk assessment.”
26. Family members of personnel need also be provided with psychosocial support services. 27. Bandwidth should be increased to ensure better internal and external communication links.28.Thereareinadequatenumberofstaffwelfareofficersorstresscounsellorsforbothpersonneland
their family members. • MogadishuandregionalofficeshadoneUNVassistanttosupportover200staff• Some staff said they received little to no information in briefings concerning mental wellbeing
and health 29. Lack of policies in place that cover psychosocial services or that allow for assessments of the stress
personnel may encounter in high-risk environments. • This includes stress linked to threat of injury or death, stress linked to administrative problems,
etc. 30. Cultural norms make it difficult, in certain circumstances, for people to recognise and accept the
need for psychosocial services. 31. Burnout is particularly evident in high-risk environments.
• Lack of recreational activities were mentioned as a contributing factor.32.Wheretherewerepsychosocialsystemsinplace,somepersonnelwerenotawareofthem.
Administration and HR arrangements including entitlements33. There needs to be increased transparency and accountability within the organization to ensure there
is full disclosure of risks that personnel may encounter whilst in a high-risk environment. Alongside this, there should be methods taught and mechanisms should be in place to tackle stress.
34. There is a significant difference evident in allowances and benefits that international personnel re-ceive in comparison to national personnel. This is also seen in a comparison between Secretariat-re-cruited personnel and agency-recruited personnel.
35. There should be changes so that compensation reflects the risks. This includes danger pay.
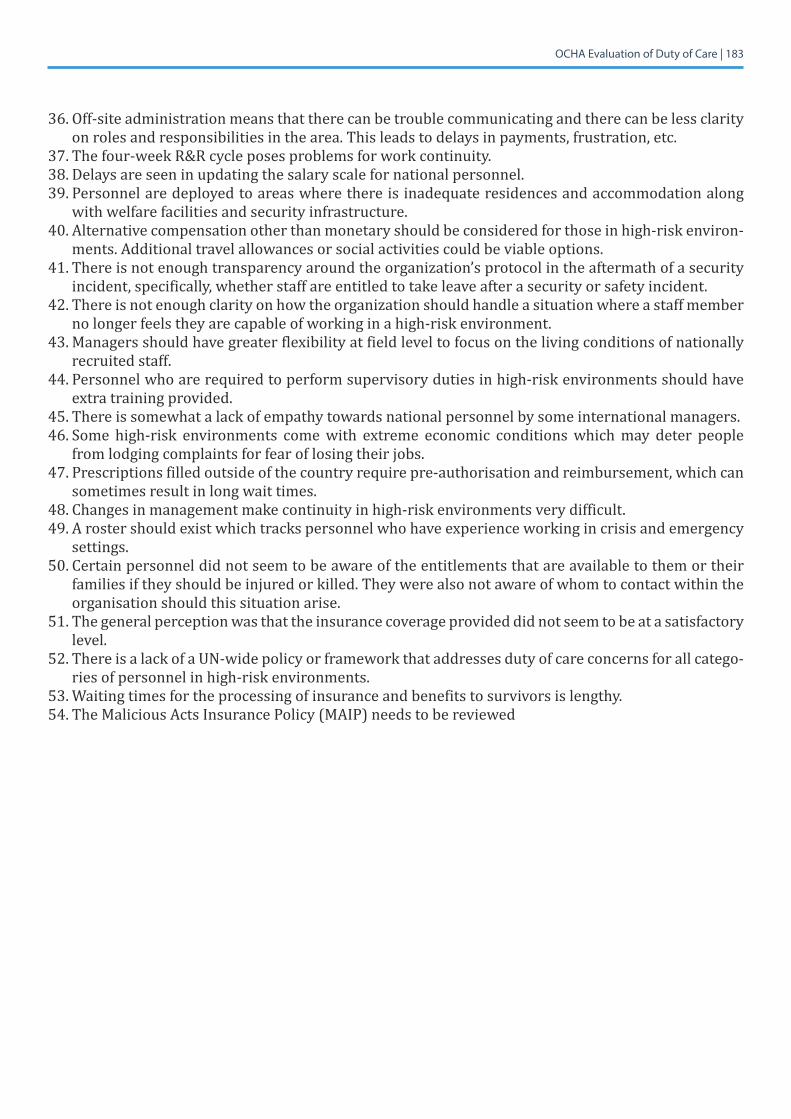
OCHA Evaluation of Duty of Care | 183
36. Off-site administration means that there can be trouble communicating and there can be less clarity on roles and responsibilities in the area. This leads to delays in payments, frustration, etc.
37. The four-week R&R cycle poses problems for work continuity.38.Delaysareseeninupdatingthesalaryscalefornationalpersonnel.39. Personnel are deployed to areas where there is inadequate residences and accommodation along
with welfare facilities and security infrastructure. 40. Alternative compensation other than monetary should be considered for those in high-risk environ-
ments. Additional travel allowances or social activities could be viable options. 41. There is not enough transparency around the organization’s protocol in the aftermath of a security
incident, specifically, whether staff are entitled to take leave after a security or safety incident. 42. There is not enough clarity on how the organization should handle a situation where a staff member
no longer feels they are capable of working in a high-risk environment. 43. Managers should have greater flexibility at field level to focus on the living conditions of nationally
recruited staff.44. Personnel who are required to perform supervisory duties in high-risk environments should have
extra training provided. 45. There is somewhat a lack of empathy towards national personnel by some international managers. 46. Some high-risk environments come with extreme economic conditions which may deter people
from lodging complaints for fear of losing their jobs.47. Prescriptions filled outside of the country require pre-authorisation and reimbursement, which can
sometimes result in long wait times. 48.Changesinmanagementmakecontinuityinhigh-riskenvironmentsverydifficult.49. A roster should exist which tracks personnel who have experience working in crisis and emergency
settings.50. Certain personnel did not seem to be aware of the entitlements that are available to them or their
families if they should be injured or killed. They were also not aware of whom to contact within the organisation should this situation arise.
51. The general perception was that the insurance coverage provided did not seem to be at a satisfactory level.
52. There is a lack of a UN-wide policy or framework that addresses duty of care concerns for all catego-ries of personnel in high-risk environments.
53.Waitingtimesfortheprocessingofinsuranceandbenefitstosurvivorsislengthy.54. The Malicious Acts Insurance Policy (MAIP) needs to be reviewed
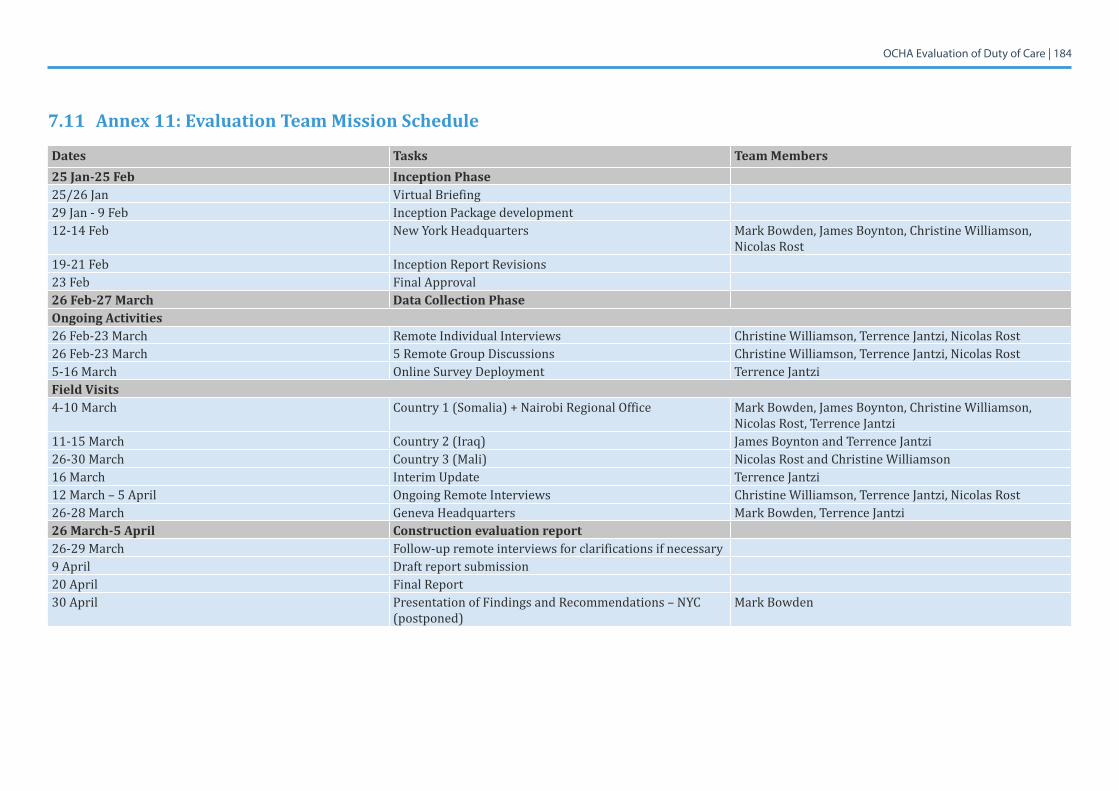
OCHA Evaluation of Duty of Care | 184
7.11 Annex 11: Evaluation Team Mission Schedule
Dates Tasks Team Members25 Jan-25 Feb Inception Phase 25/26 Jan VirtualBriefing 29 Jan - 9 Feb Inception Package development 12-14 Feb New York Headquarters MarkBowden,JamesBoynton,ChristineWilliamson,
Nicolas Rost19-21 Feb Inception Report Revisions 23 Feb Final Approval 26 Feb-27 March Data Collection Phase Ongoing Activities26 Feb-23 March Remote Individual Interviews ChristineWilliamson,TerrenceJantzi,NicolasRost26 Feb-23 March 5 Remote Group Discussions ChristineWilliamson,TerrenceJantzi,NicolasRost5-16 March Online Survey Deployment Terrence Jantzi Field Visits4-10 March Country 1 (Somalia) + Nairobi Regional Office MarkBowden,JamesBoynton,ChristineWilliamson,
Nicolas Rost, Terrence Jantzi11-15 March Country 2 (Iraq) James Boynton and Terrence Jantzi26-30 March Country 3 (Mali) NicolasRostandChristineWilliamson16 March Interim Update Terrence Jantzi12 March – 5 April Ongoing Remote Interviews ChristineWilliamson,TerrenceJantzi,NicolasRost26-28March Geneva Headquarters Mark Bowden, Terrence Jantzi 26 March-5 April Construction evaluation report 26-29 March Follow-up remote interviews for clarifications if necessary 9 April Draft report submission 20 April Final Report 30 April Presentation of Findings and Recommendations – NYC
(postponed)Mark Bowden
OCHA Evaluation of Duty of Care | 185
7.12 Annex 12: List of Acronyms
AMISOM African Union Mission to SomaliaASG Assistant Secretary-General AV ArmouredVehicleBCP Business Continuity PlansBCM Business Continuity ManagementCAR Central African RepublicCEB Chief Executives Board for CoordinationCISIC Critical Incident Stress Intervention CellCISMU Critical Incident Stress Management UnitCO Country officeDAC Development Assistance CommitteeDERC Deputy Emergency Relief CoordinatorDFS Department of Field SupportDM Department of ManagementDMS Director of Mission SupportDO Designated OfficialDOC Duty of careDPKO Department of Peacekeeping OperationsDRC Democratic Republic of the Congo EISF European Interagency Security ForumEMC Executive Management CommitteeEO Executive OfficeERC Emergency Relief CoordinatorET Evaluation TeamGA General AssemblyHC Humanitarian CoordinatorHLCM High-Level Committee on ManagementHOO Head of Office HQ HeadquartersHR Human ResourcesHRE High-Risk EnvironmentIASC Inter-Agency Standing CommitteeIASMN Inter-Agency Security Management NetworkIED Improvised Explosive DevicesIR Inception reportKII Key Informant InterviewMAIP Malicious Acts Insurance PolicyMCISF Management of Critical Incident Stress FrameworkME&R Monitoring, Evaluation and ReportingMOSS Minimum Operating Security StandardsMORSS Minimum Operating Residential Security StandardsMoU Memorandum of UnderstandingNGO Non-Governmental OrganizationsNYC New York CityOAD Operations and Advocacy DivisionOCHA Office for the Coordination of Humanitarian AffairsOCHA-CAR OCHA Central African RepublicOECD Organization for Economic Co-Operation and DevelopmentOHRM Office of Human Resources Management
OCHA Evaluation of Duty of Care | 186
OIOS Office of Internal Oversight ServicesoPt Occupied Palestinian territoryORMS Organizational Resilience Management SystemOSH Occupational Safety and HealthPCCT Programme Criticality Coordination TeamPCF Programme Criticality FrameworkPC Sec Programme Criticality SecretariatPCSG Programme Criticality Steering GroupPK PeacekeepingPPE Personal Protective EquipmentPS&M Committee People Strategy and Management CommitteePTSD Post-Traumatic Stress DisorderQA Quality AssuranceRO Regional OfficeRAC Regional Areas of CareROMENA Regional Office for the Middle East and Northern AfricaROSEA Regional Office for Southern and Eastern AfricaR&R Rest and RecuperationRSM Residential Security MeasuresSEA Sexual Exploitation and AbuseSFP Security Focal PointSGBV SexualandGender-basedViolenceSG Secretary-GeneralSGD Small Group DiscussionsSLA Service Level AgreementSMOM Security Management Operations ManualSOP Standard Operating ProcedureSPEGS Strategy, Planning, Evaluation and Guidance SectionSRM Security Risk ManagementSSAFE Safe and Secure Approaches in Field EnvironmentsSSIRS Safety and Security Incident Recording SystemTJO Temporary Job Opening TOR Terms of Reference UK United KingdomUNDP United Nations Development ProgrammeUNDSS United Nations Department of Safety & SecurityUNHCR United Nations High Commissioner for RefugeesUNOG United Nations Office in GenevaUNSMS United Nations Security Management SystemUNSOM United Nations Assistance Mission in SomaliaUNSOS United Nations Support Office in SomaliaUSG Under-Secretary-GeneralWEOG WesternEuropeanandOtherGroupWFP WorldFoodProgrammeWSAT Women’sSecurityAwarenessTraining

Recommended