A decentralized model of care for drug-resistant tuberculosis in a high HIV
prevalence setting
Cheryl McDermid, Helen Cox, Simiso Sokhela, Gilles van Cutsem, Busisiwe Beko, Andiswa Vazi, Johnny Daniels, Virginia Azevedo, Eric
Goemaere
Background
In 2008:• 390,000 – 510,000 incident MDR-TB cases worldwide• Only 29,243 MDR-TB cases reported=7% of estimated• <3% of cases receive appropriate treatment
WHO, 2010
Global M/XDR-TB response plan 2007-8 1.6 million MDR-TB patients treated by 2015
DR-TB treatment outcomes
• Treatment success 62% among 4,959 MDR-TB patients in a systematic review
• Only 39 (0.8%) were HIV-infected(Johnston et al, PLoS One,
2009)
No data on DR-TB outcomes for HIV positive patients
Key challenges• Scaling up treatment• Improving diagnosis & case-detection • Models of care (hospital, community)• Cost of treatment• Optimal treatment regimens• HIV and DR-TB integrated care• Length and difficulty of current treatment
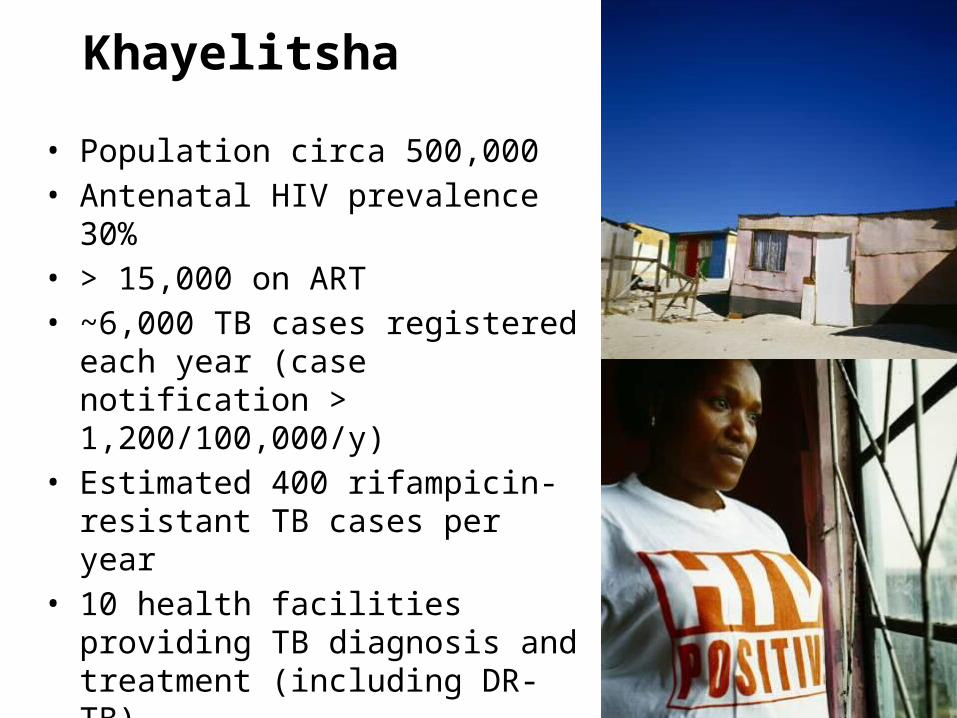
Khayelitsha
• Population circa 500,000• Antenatal HIV prevalence 30%• > 15,000 on ART • ~6,000 TB cases registered each year
(case notification > 1,200/100,000/y)• Estimated 400 rifampicin-resistant TB
cases per year • 10 health facilities providing TB
diagnosis and treatment (including DR-TB)
Review of DR-TB in Khayelitsha - 2007
Many areas identified needing support:– Long wait for treatment (bed capacity at TB hospital
unable to meet demand)– High defaulter rate (>30%)– Limited knowledge and understanding of DR-TB by
HCW at primary care level– No DR-TB register at the clinics (no reliable data on
DR-TB numbers, defaulter rates and outcomes)– Inconsistent DR-TB screening, monitoring and
contact tracing– Infection control non-existent
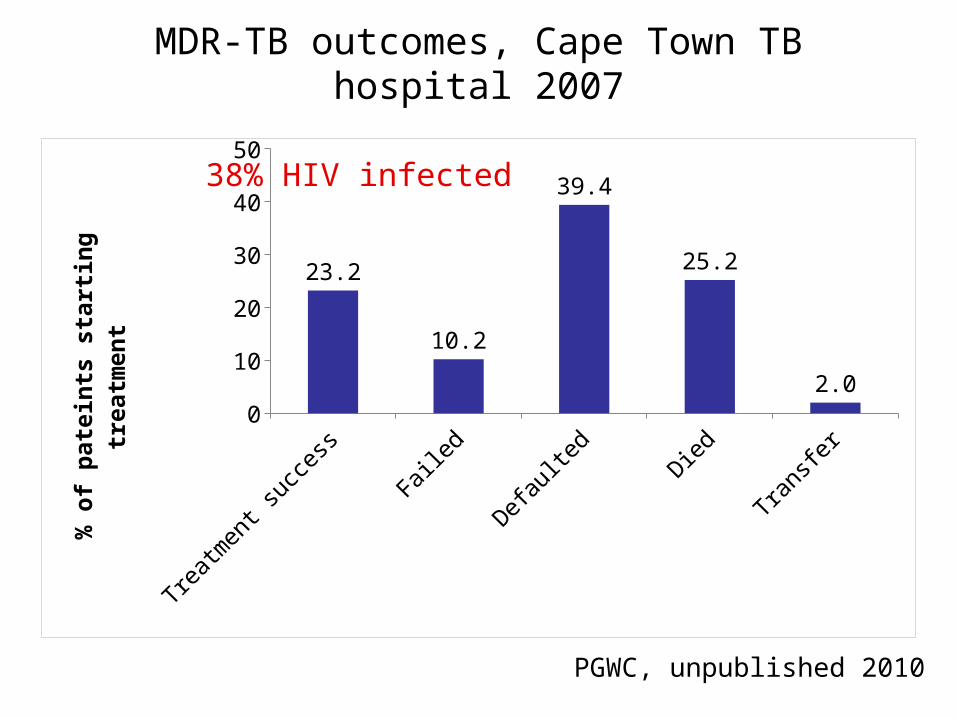
MDR-TB outcomes, Cape Town TB hospital 2007
Treatment success
Failed Defaulted Died Transfer0
10
20
30
40
50
23.2
10.2
39.4
25.2
2.0% o
f p
ate
ints
sta
rtin
g
treatm
en
t
38% HIV infected
PGWC, unpublished 2010
Aims
1. Improve case detection of DR-TB2. Improve treatment outcomes3. Decrease DR-TB transmission4. Develop a model of care applicable to
other settings
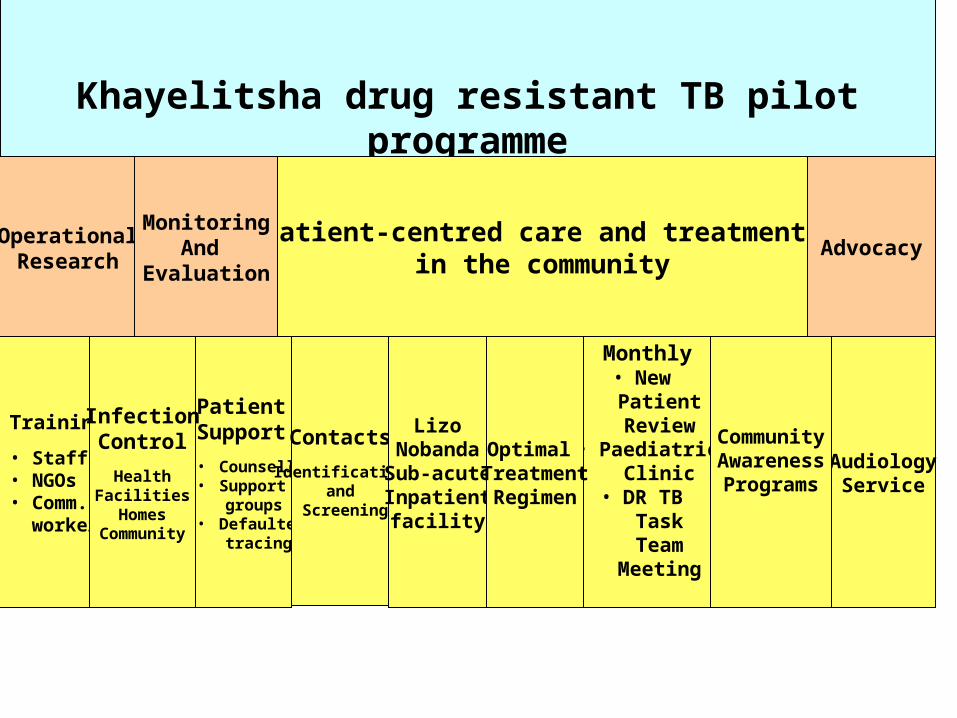
Khayelitsha drug resistant TB pilot programme
AdvocacyPatient-centred care and treatment
in the communityOperationalResearch
MonitoringAnd
Evaluation
PatientSupport
• Counselling• Support groups• Defaulter tracing
Contacts
Identificationand
Screening
Monthly• New Patient Review
• Paediatric Clinic
• DR TB Task Team
Meeting
AudiologyService
Training
• Staff• NGOs• Comm. workers
CommunityAwarenessPrograms
LizoNobanda
Sub-acuteInpatientfacility
Optimal TreatmentRegimen
InfectionControl
HealthFacilitiesHomes
Community
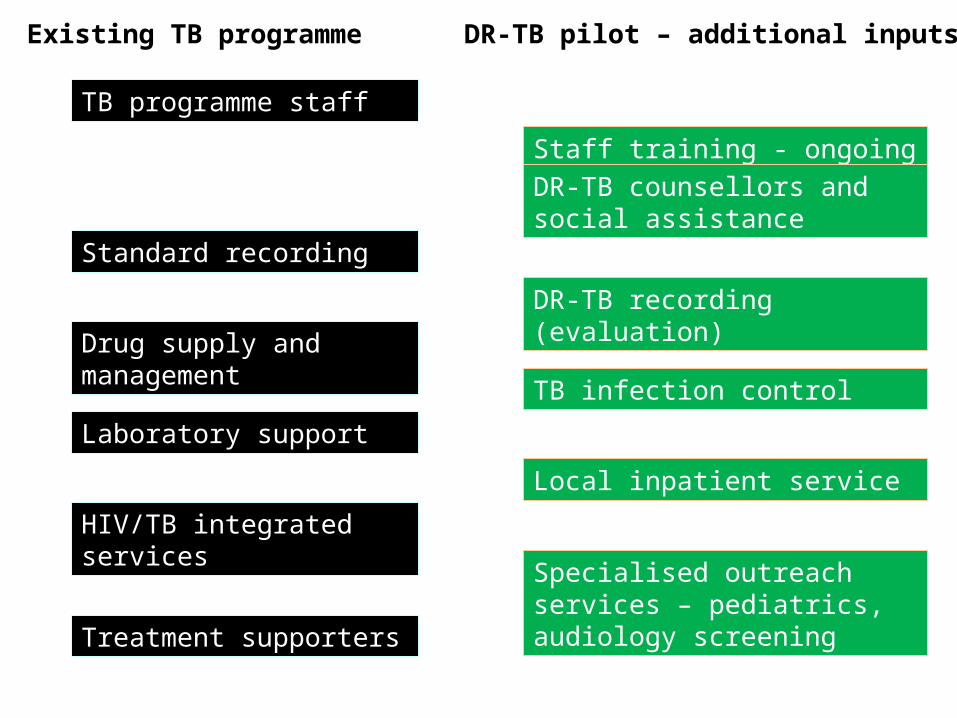
TB programme staff
Standard recording
Drug supply and management
Laboratory support
HIV/TB integrated services
Treatment supporters
Staff training - ongoing support
DR-TB recording (evaluation)
TB infection control
DR-TB counsellors and social assistance
Local inpatient service
Specialised outreach services – pediatrics, audiology screening
Existing TB programme DR-TB pilot – additional inputs
Early results…
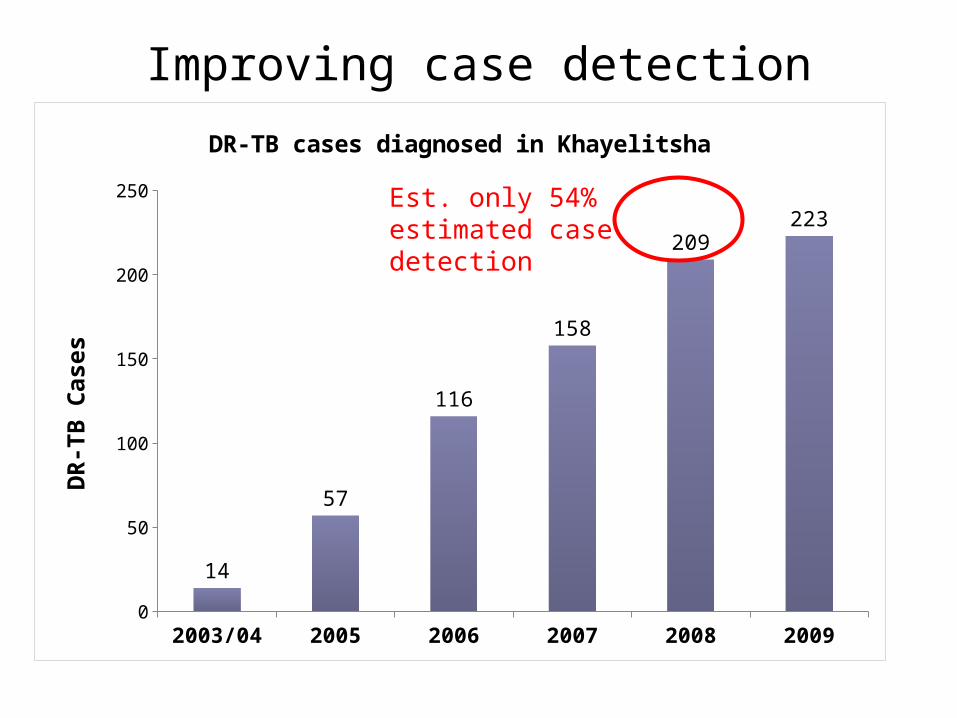
Improving case detection
2003/04 2005 2006 2007 2008 20090
50
100
150
200
250
14
57
116
158
209223
DR-TB cases diagnosed in Khayelitsha
DR-
TB C
ases
Est. only 54% estimated case detection
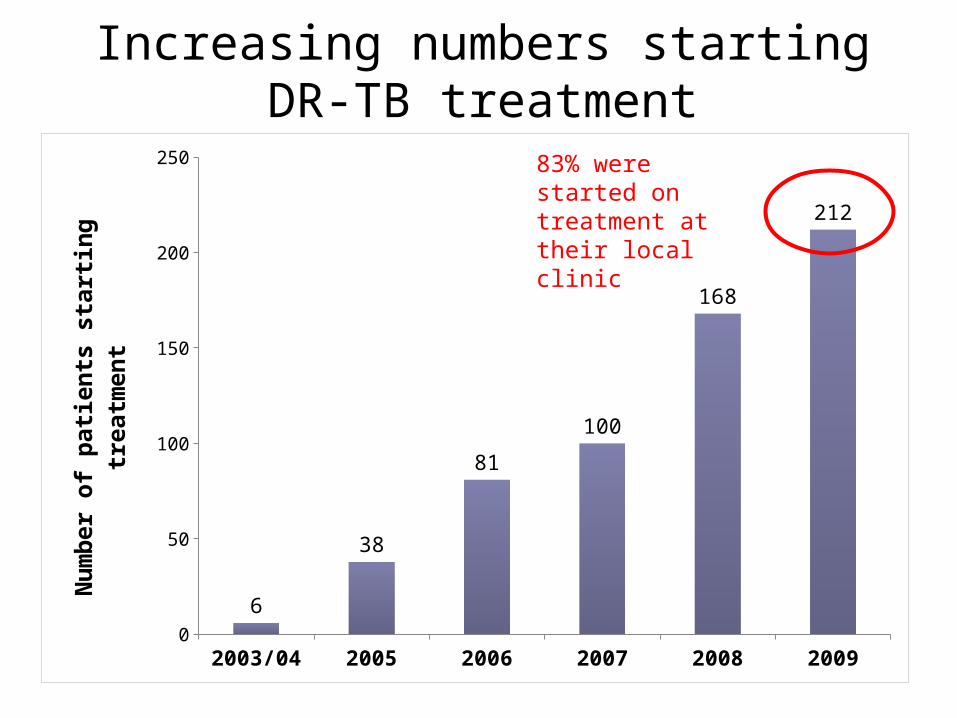
Increasing numbers starting DR-TB treatment
2003/04 2005 2006 2007 2008 20090
50
100
150
200
250
6
38
81
100
168
212
Num
ber o
f pati
ents
sta
rting
trea
tmen
t
83% were started on treatment at their local clinic
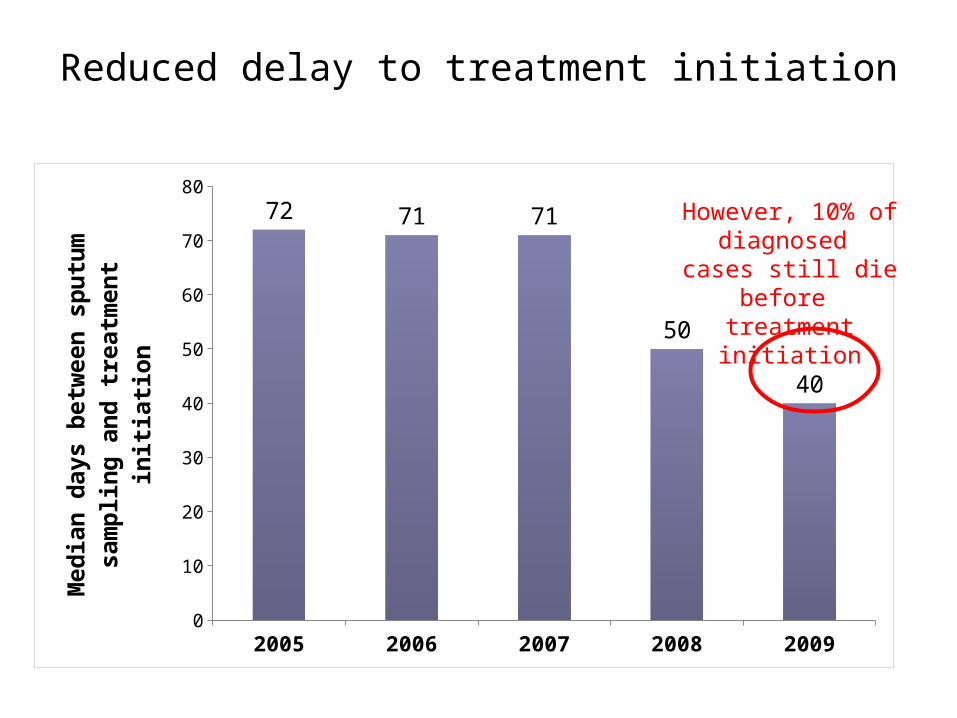
Reduced delay to treatment initiation
2005 2006 2007 2008 20090
10
20
30
40
50
60
70
80
72 71 71
50
40
Med
ian
days
bet
wee
n sp
utum
sa
mpl
ing
and
trea
tmen
t ini
tiatio
n
However, 10% of diagnosed
cases still die before treatment initiation
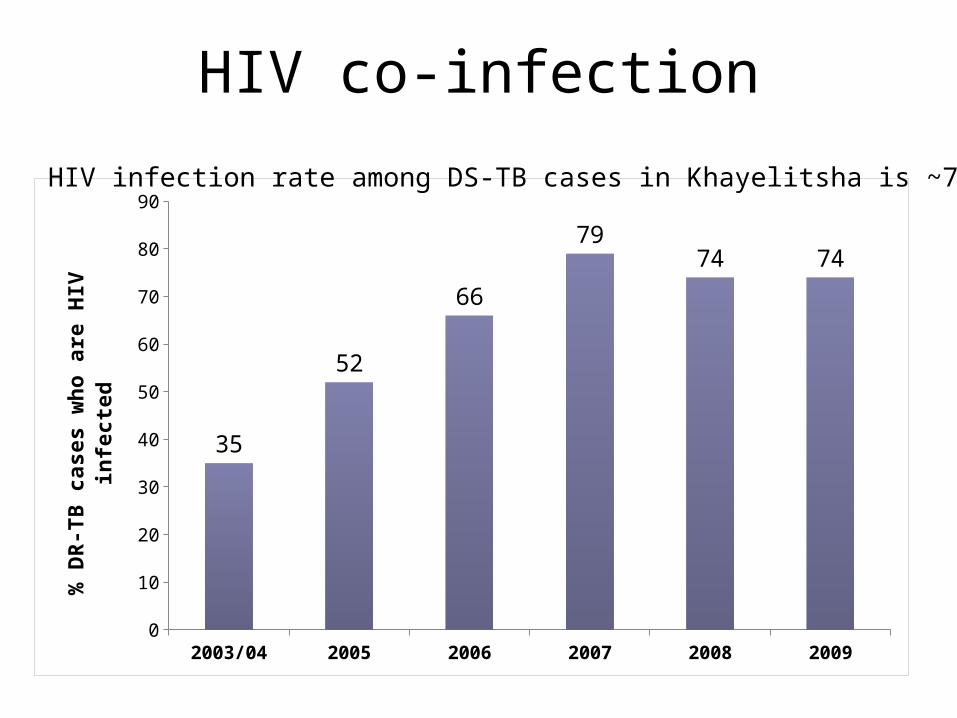
HIV co-infection
2003/04 2005 2006 2007 2008 20090
10
20
30
40
50
60
70
80
90
35
52
66
7974 74
% D
R-TB
cas
es w
ho a
re H
IV in
fect
ed
HIV infection rate among DS-TB cases in Khayelitsha is ~70%
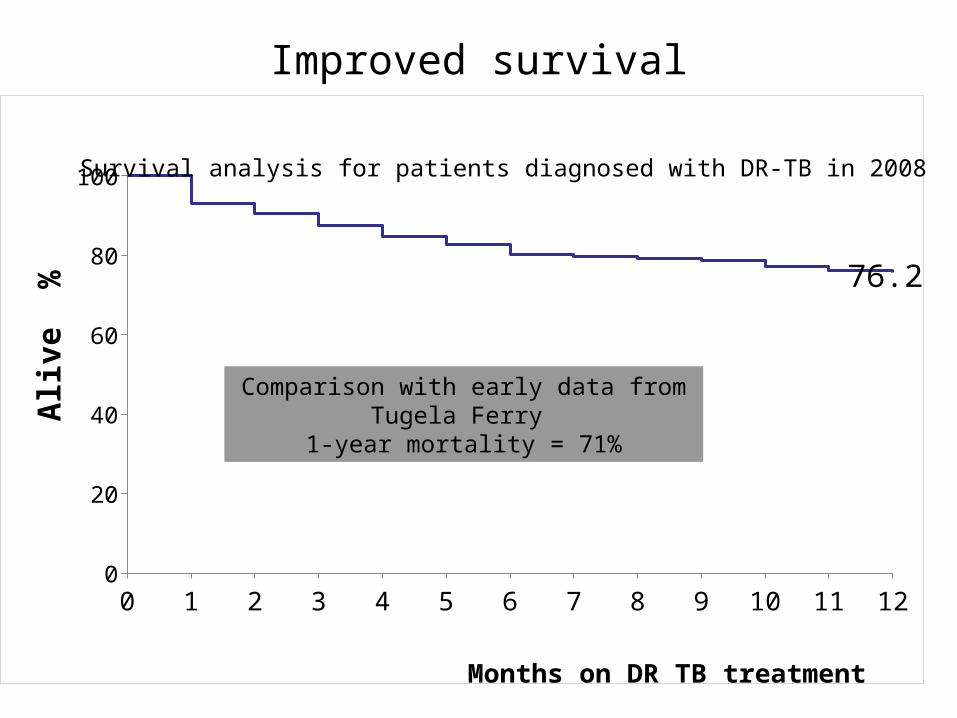
Improved survival
0 1 2 3 4 5 6 7 8 9 10 11 120
20
40
60
80
100
76.2
Months on DR TB treatment
Aliv
e %
Comparison with early data from Tugela Ferry 1-year mortality = 71%
Survival analysis for patients diagnosed with DR-TB in 2008
0
10
20
30
40
50
60
70
80
90
100
0 10 20 30 40 50 60 70 80 90 100 110 120 130 140 150
% r
em
ain
ing
ali
ve
Time (days)
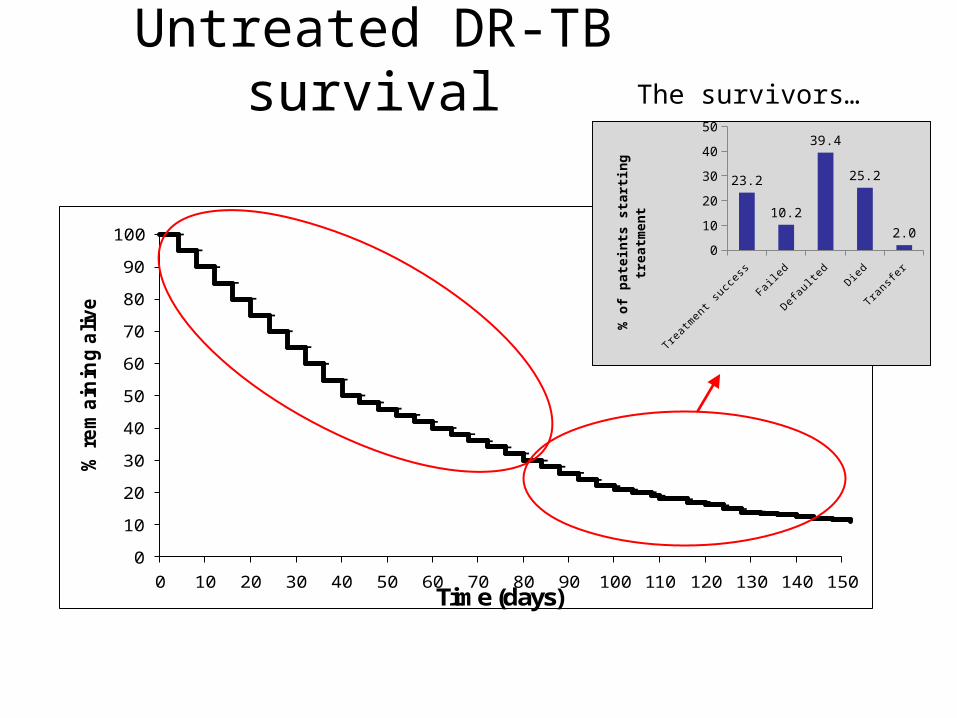
Untreated DR-TB survivalThe survivors…
Trea
tmen
t suc
cess
Faile
d
Defau
lted
Died
Tran
sfer
0
10
20
30
40
50
23.2
10.2
39.4
25.2
2.0
% o
f pate
ints
sta
rtin
g
treatm
ent
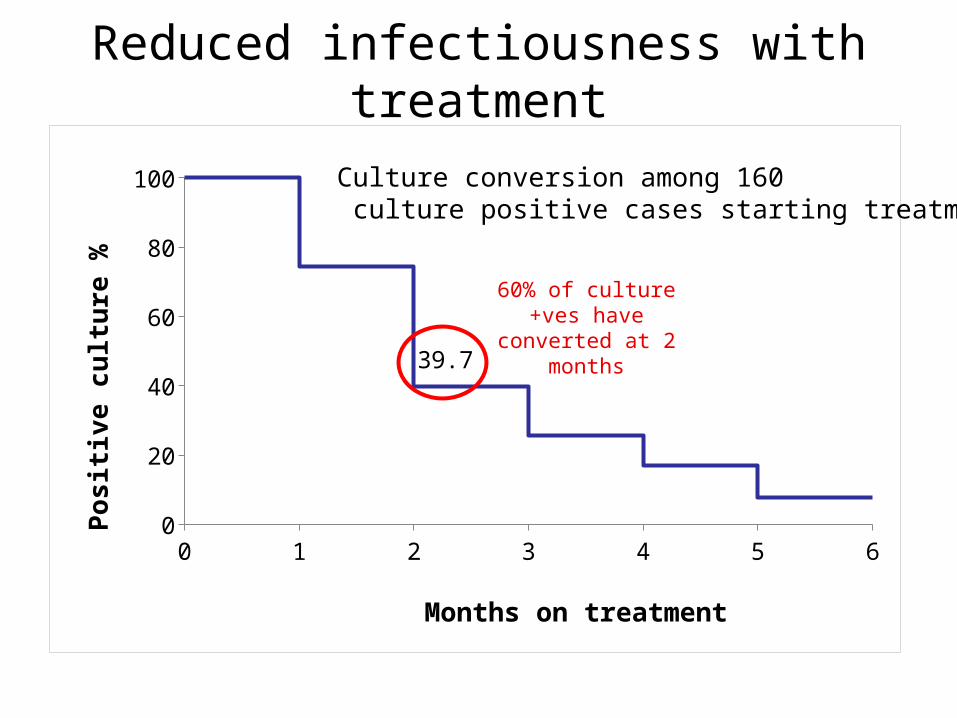
Reduced infectiousness with treatment
0 1 2 3 4 5 60
20
40
60
80
100
39.7
Months on treatment
Posi
tive
cultu
re %
Culture conversion among 160 culture positive cases starting treatment
60% of culture +ves have converted at 2
months
Challenges
• Improving case detection – need a rapid test for all TB suspects
• Reducing mortality prior to treatment initiation
• Improving support for patients during treatment – reducing default
• Overcoming stigma and fear among health care staff and in the community
• Determining the minimum inputs required in order to scale up treatment provision elsewhere
Conclusion• Decentralizing DR TB treatment to PHC led to:
– Increase in case detection and started on treatment– Reduced delay to treatment initiation– 76% survival at one year on treatment increased % HIV/DR-TB co-infected detected– Reduced transmission of DR TB as most infection
occurs before diagnosis and treatment
Acknowledgments
• City of Cape Town Health Department
• Western Cape Province• National Health
Laboratory Service• Staff in Khayelitsha
clinics• People suffering from
drug resistant TB in Khayelitsha
Recommended


![Commentson:AccuracyofRamanlidarwater ......1.Abstract In a recent publication, LeBlanc and McDermid[LeblancandMcDermid,2009] proposedahybridcalibrationtechniqueforRamanwatervaporlidarinvolving](https://img.pdfslide.us/doc/110x75/5e488c6d5ead127a2471f62f/commentsonaccuracyoframanlidarwater-1abstract-in-a-recent-publication.jpg)