Embed Size (px)
DESCRIPTION
Phase 3 Trial of Everolimus in Previously Treated Patients With Advanced Gastric Cancer: GRANITE-1 . Eric Van Cutsem*, - PowerPoint PPT Presentation
Citation preview

Phase 3 Trial of Everolimus in Previously Treated Patients With
Advanced Gastric Cancer: GRANITE-1
Eric Van Cutsem*, K. H. Yeh, Y. J. Bang, L. Shen, J. A. Ajani, Y. X.
Bai, H. C. Chung, H. M. Pan, K. Chin, K. Muro, Y. H. Kim, H. Smith, C. Constantini, S. Rizvi, T.
Sahmoud, A. Ohtsu
On behalf of the GRANITE-1 Investigators* University Hospital Leuven/Belgium
Presented at the 2012 Gastrointestinal Cancers Symposium. 1

Background
• Gastric cancer is aggressive and difficult to treat1
• 5-year survival rate for advanced, metastatic disease is <5%2,3
• After failure of first-line chemotherapy, available treatment options provide minimal benefit and are associated with considerable toxicity1,4,5
2
1Catalano V et al. Crit Rev Hematol Oncol. 2009;71:127-34; 2American Cancer Society. Cancer Facts & Figures 2011; 3Matsuda T et al. Jpn J Clin Oncol. 2011;41:40-51; 4Wagner AD et al. Cochrane Database Syst Rev. 2010;CD004064; 5Field K et al. Drugs. 2008;68:299-317.

PI3K/Akt/mTOR Pathway in Gastric Cancer
• The PI3K/Akt/mTOR pathway, a key regulator of cell proliferation, growth, survival, metabolism, and angiogenesis, is dysregulated in 50%-60% of gastric cancers1-3
• Everolimus, an oral mTOR inhibitor, showed efficacy in preclinical models of gastric cancer1,4-6
3
mTOR, mammalian target of rapamycin; PI3K, phosphatidylinositol 3-kinase.
1Xu DZ et al. BMC Cancer. 2010;10:536; 2Lang SA et al. Cancer. 2007;120:1803-10; 3Yu G et al. Clin Cancer Res. 2009;15:1821-29; 4Taguchi F et al. Invest New Drugs. 2011;29:1198-205; 5Cejka D et al. Anticancer Res. 2008;28:3901-08; 6Jaeger-Lansky A et al. Cancer Biol Ther. 2010;9:919-27; 7Doi T et al. J Clin Oncol. 2010;28:1904-1910.
• In a phase 2 study of 53 patients with previously treated advanced gastric cancer, everolimus showed promising efficacy and acceptable tolerability7

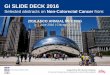
Phase 3 GRANITE-1 Study Design
4
Everolimus 10 mg PO daily
+ BSC*(n = 439)
Placebo PO daily+
BSC(n = 217)
SCR
EEN
Treatment until disease progression
or intolerable
toxicity
• Stratification by region: Asia vs rest of world• Stratification by number of lines of previous
systemic chemotherapy (1 vs 2)
Safety follow-up: EOT + 28 d
Survival follow-up: every 3 mo
RA
ND
OM
IZE
(N =
656
)
BSC, best supportive care; EOT, end of treatment; PO, orally.ClinicalTrials.gov identifier: NCT00879333.
2
1

Eligibility Criteria
5
• >2 previous systemic therapies for advanced disease
• Anticancer therapy within 3 weeks* or major surgery within 2 weeks of randomization
• Chronic treatment with steroids or immunosuppressive agents
• Enteral feeding• CNS metastases• Any severe/uncontrolled medical
condition
• Age ≥18 years• Confirmed gastric adenocarcinoma
– GEJ adenocarcinomas permitted if the majority involved the stomach
• Documented progression after 1 or 2 lines of previous systemic chemotherapy
• ECOG performance status ≤2• Adequate bone marrow, renal, and
hepatic function
Key Inclusion Criteria Key Exclusion Criteria
*Fluoropyrimidine monotherapy was permitted up to 2 weeks before randomization.CNS, central nervous system; ECOG, Eastern Cooperative Oncology Group; GEJ, gastroesophageal junction.

Study Endpoints• Primary: OS• Secondary
– PFS– ORR*– AEs as assessed by NCI CTCAE, version 3.0– Time to definitive deterioration of ECOG PS– Time to definitive 5% deterioration in the global health
status/quality of life scale of the EORTC QLQ-C30 questionnaire
• Exploratory– Correlation between biomarkers and clinical endpoints
6
*ORR: overall response rate according to RECIST, version 1.0.AE, adverse event NCI CTCAE, National Cancer Institute Common Terminology Criteria for Adverse Events; RECIST, Response Evaluation Criteria In Solid Tumors.

Statistical Considerations
• Between-group OS comparison performed using stratified log-rank test at overall one-sided 2.5% level, stratified by protocol stratification factors
• Single interim analysis planned after 60% of required deaths observed– At time of interim analysis (cut-off date of Jan 31, 2011), IDMC
recommended continuing study without any changes• Sample size calculation
– Considering randomization scheme and planned interim analysis, estimated that 526 deaths would give study 90% power to detect a 26% difference in the risk of death, corresponding to prolongation in OS from 4.0 months with placebo to 5.4 months with everolimus
– Assuming uniform patient accrual over 2 years, 6 months of follow-up, and 5% loss to follow-up, determined that 633 patients needed to be enrolled
• Hierarchical testing strategy– Formal statistical significance for PFS could be declared only if between-
group difference in OS statistically significant
7

Patient Disposition
8
Patients randomly assigned (N = 656)
Everolimus + BSC (n = 439) Placebo + BSC (n = 217)
Ongoing (n = 11; 2.5%)Discontinued treatment (n = 428; 97.5%)
– Disease progression (n = 292; 66.5%)– AEs (n = 94; 21.4%)– Abnormal laboratory values (n = 1; 0.2%)– Withdrew consent (n = 20; 4.6%)– Administrative problems (n = 2; 0.5%)– Death NOS (n = 16; 3.6%)– Lost to follow-up (n = 2; 0.5%)– Protocol deviation (n = 1; 0.2%)
Ongoing (n = 0; 0%)Discontinued treatment (n = 217; 100%)
– Disease progression (n = 169; 77.9%)– AEs (n = 34; 15.7%)– Abnormal laboratory values (n = 0; 0%)– Withdrew consent (n = 7; 3.2%)– Administrative problems (n = 0; 0%)– Death NOS (n = 5; 2.3%)– Lost to follow-up (n = 1; 0.5%) – Protocol deviation (n = 1; 0.5%)
Full analysis set (n = 439)Safety set (n = 437)
Full analysis set (n = 217)Safety set (n = 215)
NOS, not otherwise specified.

GRANITE-1: Participating Countries
9

Baseline Demographics and Disease Characteristics (FAS)
10
Everolimus + BSC (n = 439)
Placebo + BSC (n = 217)
Age, yrs, median (range) 62.0 (20.0-86.0) 62.0 (26.0-88.0)Age <65 yrs 260 (59.2) 129 (59.4)Male, n (%) 322 (73.3) 161 (74.2)Race, n (%)
Caucasian 166 (37.8) 75 (34.6)Asian 251 (57.2) 126 (58.1)Other 22 (5.0) 16 (7.4)
Region, n (%)Asia 243 (55.4) 120 (55.3)Rest of world 196 (44.6) 97 (44.7)
ECOG performance status, n (%)0 144 (32.8) 70 (32.3)1 269 (61.3) 120 (55.3)2 25 (5.7) 27 (12.4)
FAS, full analysis set.

Baseline Disease Characteristics (FAS)
11
Everolimus + BSC (n = 439)
Placebo + BSC (n = 217)
Anatomical site, n (%)Proximal 162 (36.9) 94 (43.3)Distal 276 (62.9) 123 (56.7)
GEJ involvement, n (%) 118 (26.9) 69 (31.8)Lauren classification, n (%)
Adenocarcinoma, diffuse 93 (21.2) 37 (17.1)Adenocarcinoma, intestinal 82 (18.7) 50 (23.0)Adenocarcinoma, mixed 29 (6.6) 18 (8.3)Adenocarcinoma, NOS 105 (23.9) 45 (20.7)Other 129 (29.4) 67 (30.9)
Previous gastrectomy, n (%)Partial 126 (28.7) 60 (27.6)Total 97 (22.1) 46 (21.2)
Previous lines of chemotherapy, n (%)1 210 (47.8) 103 (47.5)2 229 (52.2) 114 (52.5)

Exposure to Study Treatment (Safety Set)
12
Everolimus + BSC (n = 437)
Placebo + BSC (n = 215)
Duration, wks, median (range) 7.1 (0.1-79.6) 6.4 (0.4-90.9)
Duration, wks, mean (SD) 11.5 (12.09) 8.5 (8.76)
Duration of exposure, wks, n (%)
<4 84 (19.2) 49 (22.8)
4 to <8 163 (37.3) 101 (47.0)
8 to <12 55 (12.6) 23 (10.7)
12 to <16 46 (10.5) 20 (9.3)
16 to <20 26 (5.9) 7 (3.3)
20 to <24 12 (2.7) 3 (1.4)
24 to <28 9 (2.1) 5 (2.3)
28 to <32 7 (1.6) 2 (0.9)
≥32 35 (8.0) 5 (2.3)

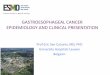
Overall Survival (FAS)
13
Prob
abili
ty o
f ove
rall
surv
ival
(%) 100
80
60
40
20
00 2 4 6 8 10 12
Time (months)14
Censoring TimesEverolimus + BSC (n/N = 352/439)Placebo + BSC (n/N = 180/217)
Kaplan-Meier medians Everolimus + BSC: 5.39 months Placebo + BSC: 4.34 months
Hazard ratio: 0.90 (95% CI, 0.75-1.08)Log-rank P value = 0.1244
No. of patients still at riskTime (months)EverolimusPlacebo
16 18 20 22 24
0 2 4 6 8 10 12 14 16 18 20 22 24
217 172 117 82 60 35 28 16 12 8 4 1 0439 355 253 195 139 87 52 30 13 6 3 1 0

Overall Survival by Stratification Factors (FAS)
14ROW, rest of world.
Priorchemotherapy
Region
Cross-class.of strata
Hazard Ratio(95% CI)
0.80.6Everolimus
10 mg/dPlacebo
In favor of
1.0 1.2 1.4
All (N = 656) 0.90 (0.75-1.08)
2 (n = 343) 0.90 (0.70-1.15)
Asia (n = 363) 0.96 (0.75-1.23)
ROW (n = 293) 0.85 (0.65-1.10)
1 prior chemo & ROW (n = 167) 0.91 (0.64-1.31)
2 prior chemo & ROW (n = 126) 0.74 (0.50-1.09)
1 (n = 313) 0.94 (0.73-1.23)
0.98 (0.71-1.35)2 prior chemo & Asia (n = 217)
0.94 (0.63-1.39)1 prior chemo & Asia (n = 146)

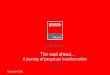
Progression-Free Survival (FAS)
15
Prob
abili
ty o
fpr
ogre
ssio
n-fr
ee s
urvi
val (
%)
100
80
60
40
20
00 2 4 6 7 9 10
Time (months)12
Censoring TimesEverolimus + BSC (n/N = 386/439)Placebo + BSC (n/N = 206/217)
Kaplan-Meier medians Everolimus + BSC: 1.68 months Placebo + BSC: 1.41 months
Hazard ratio: 0.66 (95% CI, 0.56-0.78)Log-rank P value < 0.0001
No. of patients still at riskTime (months)EverolimusPlacebo
14 15 17 21
0 2 4 5 7 9 11 12 14 16 17 20 21
217 55 23 17 7 3 2 2 2 2 2 1 0439 179
1
168367 92
3
28117 60
6
844 37 20
8
627 10
10
213 6 3 2
15
23
13
25 1
19
20
18
21 0 0
18 2019161311851 3

Tumor Response (Patients With Measurable Disease)
16DCR, disease control rate.
Everolimus + BSC (n = 379)
Placebo + BSC (n = 191)
Best overall response, n (%)CR 1 (0.3) 0PR 16 (4.2) 4 (2.1)SD 147 (38.8) 38 (19.9)PD 157 (41.4) 119 (62.3)Unknown 58 (15.3) 30 (15.7)
ORR (CR + PR), n (%) 17 (4.5) 4 (2.1)DCR (CR + PR + SD), n (%) 164 (43.3) 42 (22.0)

Best Percentage Change From Baseline in Tumor Size
17
Bes
t % c
hang
e fr
om b
asel
ine
(mea
sura
ble
lesi
ons)
160%140%120%100%
80%60%40%20%
0%–20%–40%–60%–80%
–100%
160%140%120%100%
80%60%40%20%
0%–20%–40%–60%–80%
–100%
Everolimus 10 mg/day (n = 304) Placebo (n = 154)
º No change º No change
Everolimus + BSC (n = 304)
Placebo + BSC (n = 154)
Decrease in best percentage change from baseline, n (%) 115 (37.8) 19 (12.3)
Zero change in best percentage change from baseline, n (%) 16 (5.3) 2 (1.3)
Increase in best percentage change from baseline, n (%) 109 (35.9) 98 (63.6)
Best % change from baseline available but contradicted by overall lesion response of progressive disease, n (%) 64 (21.1) 35 (22.7)

Summary of Adverse Events and Deaths (Safety Set)
Everolimus + BSC
(n = 437)
Placebo + BSC
(n = 215)Any AE, n (%) 433 (99.1) 208 (96.7)Any grade 3/4 AE, n (%) 310 (70.9) 115 (53.5)Any serious AE, n (%) 207 (47.4) 89 (41.4)AE leading to discontinuation, n (%) 94 (21.5) 34 (15.8)AE requiring dose interruption/reduction, n (%) 242 (55.4) 46 (21.4)AE requiring additional therapy, n (%) 395 (90.4) 174 (80.9)All deaths, n (%) 352 (80.5) 179 (83.3)On-treatment deaths*, n (%) 88 (20.1) 49 (22.8)
Study indication as primary cause 79 (18.1) 45 (20.9)Other primary cause 9 (2.1) 4 (1.9)
18
*On-treatment deaths are those that occurred during study treatment and up to 28 days after treatment discontinuation.

Most Common All-Cause Adverse Events (Safety Set)
Adverse Event, n (%)
Everolimus + BSC (n = 437)
Placebo + BSC (n = 215)
All grades Grade 3/4 All grades Grade 3/4Nonhematologic
Decreased appetite 208 (47.6) 48 (11.0) 78 (36.3) 12 (5.6)Stomatitis 174 (39.8) 20 (4.6) 23 (10.7) 0Fatigue 150 (34.3) 34 (7.8) 65 (30.2) 11 (5.1)Nausea 132 (30.2) 16 (3.7) 69 (32.1) 8 (3.7)Diarrhea 115 (26.3) 15 (3.4) 33 (15.3) 2 (0.9)
HematologicAnemia 114 (26.1) 70 (16.0) 42 (19.5) 27 (12.6)Thrombocytopenia 80 (18.3) 22 (5.0) 5 (2.3) 3 (1.4)Neutropenia 47 (10.8) 17 (3.9) 6 (2.8) 1 (0.5)
Abnormal biochemistryHypokalemia 52 (11.9) 26 (5.9) 9 (4.2) 2 (0.9)Blood alkaline phosphatase increased 34 (7.8) 20 (4.6) 6 (2.8) 3 (1.4)Aspartate aminotransferase increased 34 (7.8) 14 (3.2) 8 (3.7) 2 (0.9)
19

Conclusions
• Compared with BSC, everolimus did not significantly reduce the risk of death in patients with advanced gastric cancer
• Everolimus did reduce the risk of progression or death compared with BSC
• The safety profile of everolimus was similar to that observed with everolimus in other cancers, with no new safety signals identified
• Biomarker analysis is ongoing
20

Acknowledgements
• The patients participating in this trial and the study investigators
• Independent data monitoring committee– Roberto Labianca (chair)– Ichinosuke Hyodo (member)– Ian Ford (biostatistician)
• The Novartis teams
• Steering committee members– Eric Van Cutsem (co-chair)– Atsushi Ohtsu (co-chair)– Jaffer Ajani– Yung-Jue Bang– Lin Shen– Kun-Huei Yei– Chiara Constantini– Syed Rizvi– Tarek Sahmoud– Heind Smith
21