5th Annual Advocacy Project:
ImmuneWiseSection on Medical Students, Residents,
and Fellowship Trainees2009-2010


Case Presentation

Case Presentation
• 4 year old female is on the illness clinic schedule
• Her mom reports 2 days of fever and decreased energy level

Case Presentation
• Review of Systems– Temp to 102°F– Mild headache– Eye redness– Mild congestion– Non-productive cough– No GI complaints– No rash
• PMHx– Healthy– Due for 4-5 year old
immunizations
• SHx– Lives with parents– No known sick
contacts– Recent travel to
Disney World (about 10 days ago)

Case Presentation - Exam
• General: Cooperative, NAD but appears ill• HEENT: PERRL, bilateral conjunctival erythema
and watery eyes, nares patent, MMM without lesions, neck supple, no lymphadenopathy
• Chest: CTA bilaterally, no wheeze/rales/rhonchi; RRR, no murmur/rub/gallop
• Abd: Active BS, soft, non-tender, no HSM• Skin: No rash or lesions noted
Case Presentation
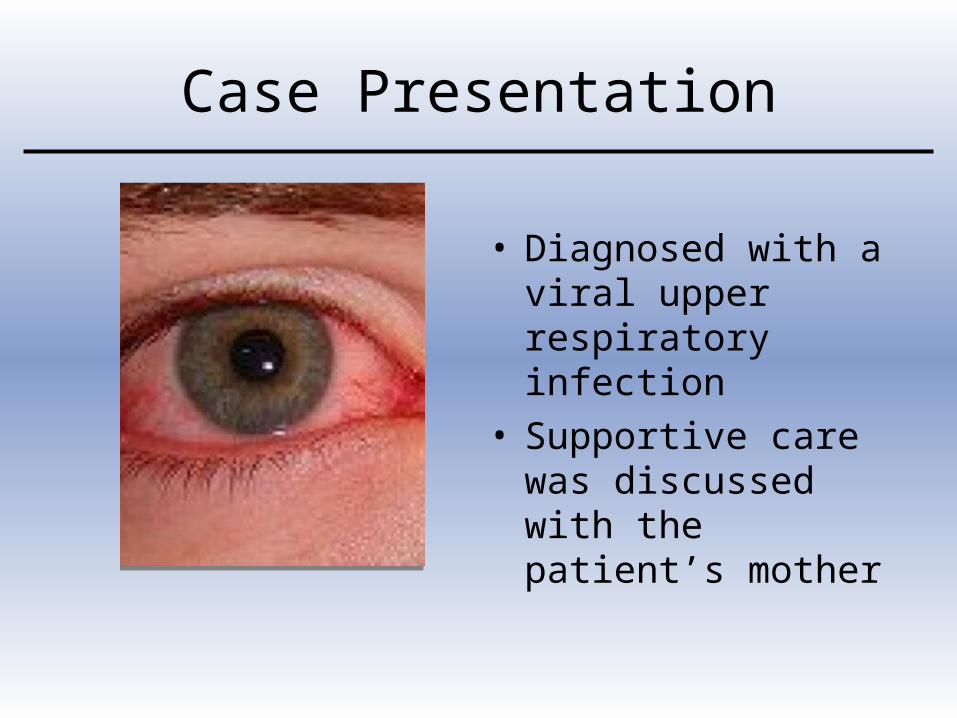
• Diagnosed with a viral upper respiratory infection
• Supportive care was discussed with the patient’s mother
Case Presentation
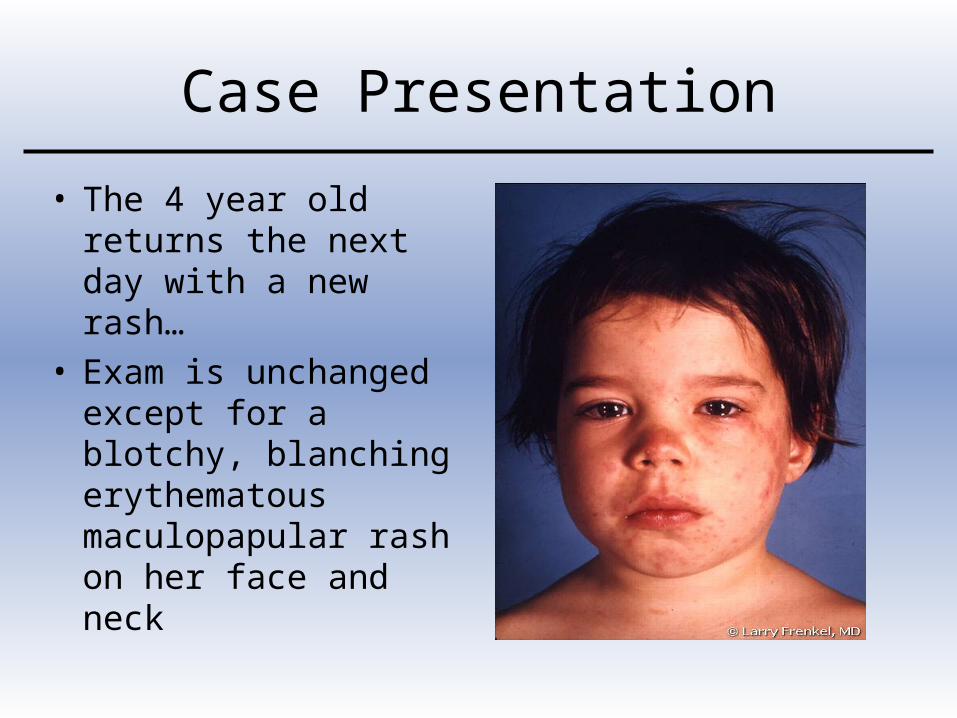
• The 4 year old returns the next day with a new rash…
• Exam is unchanged except for a blotchy, blanching erythematous maculopapular rash on her face and neck
Differential Diagnosis
- Discussion

Management
MeaslesEpidemiology
• Humans are the only natural host• Transmitted by direct contact with droplets
– may contract from airborne droplets too
• Most common in preschool and early school-aged children with a late winter peak
• Vaccine licensed in 1963• Vaccine failure rate of 5% in those with only
a single dose

MeaslesEpidemiology

Measles Epidemiology
Measles Clinical Presentation
• Incubation period of 8-12 days• Symptoms and signs include:
– Fever, malaise, cough– Conjunctivitis, coryza, +/- photophobia– Koplik spots on soft palate (often occur before
the rash and are diagnostic)– Rash, usually day 2-3 of illness
• Contagious for 1-2 days before onset of symptoms until ~4 days after rash appears

Measles Clinical Presentation
Measles Diagnosis
• Serum sample positive for measles IgM antibody on initial presentation– Sensitivity varies - low in first 72 hours of rash– If the initial test is negative, consider repeating
after the rash is present > 72 hours
• Significant rise in measles IgG in paired acute – convalescent samples
• Measles RNA in blood, throat, nasopharyngeal or urine samples (by PCR)

MeaslesComplications
• Complications include:– Otitis media– Croup or bronchopneumonia– Diarrhea
• Severe complications:– Acute encephalitis in 1/1000 cases– Death in 1-3/1000 cases
• Usually due to respiratory or neuro complications
– Subacute sclerosing panencephalitis (SSPE)• Degenerative CNS disease
Measles Treatment
• Supportive care
• Vitamin A– Give if vitamin A deficiency is endemic– Give in the U.S under certain conditions
Consult Red Book
• Ribavirin– Not FDA approved, but may help those
severely affected and immunocompromised

Measles Infection Control
• Vaccine given within 72 hrs of exposure my provide protection in susceptible individuals
• Immune globulin given within 6 days of exposure may prevent or modify measles

ImmuneWise Advocacy

ImmuneWise• 5th Annual Advocacy Project
• SOMSRFT partnered with Section for Seniors Members
• Goal: Educate providers and parents
• Goal: Improve immunization rates
• Goal: Foster advocacy interest among SOMSRFT members
Why?

Who Else?
• Within the AAP, many are concerned
Paul Offit, M.D.

What about You?
• Many levels of advocacy – Individual level– Residency program / Clinic level– State level– Federal level

Individual Level
Individual Advocacy
• Talk to the Press– Write a letter to the editor
– Make yourself available to the media
• Contact your state legislators– Write a letter or an email
– Provide them with information
• Discuss the issue with parents– Provide parents with info on Myths vs. Facts
– Answer questions about vaccine components, side effects, and alternate schedules
Myths vs. Facts

Program / Clinic Level

Program-Wide Advocacy
• Implement a quality improvement project focused on improving immunization rates
• Implement an immunization education curriculum
Quality Improvement
ACGME Program Requirement on Practice Based Learning
and Improvement states, “systematically analyze practice using quality
improvement methods, and implement changes with the
goal of practice improvement- Residents are expected to
participate in a quality improvement project.”

QI ProjectImmunization Rates
• QI projects focused on improving immunization rates can target– Particular vaccine (eg, influenza)– Target population (eg, 2-24 month olds)– Entire population served
• An example of how to
do QI for immunization
rates comes from TIDE – Teaching
Immunization Delivery and Evaluation

Designing QI – Step 1
• Assess Immunization Rates (“Plan”)
• Assessment methods:– Chart method– Active method– Consecutive method
• Record the assessment data collected• There is a sample to download

Designing QI – Step 2
• Implement Change (“Do”)– Describe and analyze key office routines
related to immunizations using an office immunization practices questionnaire
• There is a sample to download
– Based on findings… • Select an intervention likely to improve
immunization rates• Focus on the “vital few” interventions rather than
the “useful many”

Office Immunization Practices Questionnaire

Designing QI – Step 3
• Assess the Effects of Change (“Study”)– Assess the immunization rates again (after a
set period of time)– Continue to improve your effort after noting
barriers / set-backs– Celebrate successes

Community Level
Community Advocacy
• Find community supporters and leaders
• Speak to parent groups
• Post ImmuneWise posters in key locations
• Utilize national PSAs at the local level

PSA Every Child By Two
State Level

State Advocacy
Each state has their own reimbursement issues

State Advocacy
• Statewide campaigns are an opportunity to partner with AAP Chapters
• The activities available/needed vary by state, so for more information turn to:– ImmuneWise CD-ROM– AAP Committee on State
Government Affairs

National / Federal Level
national Advocacy
• National media campaigns underway– Every Child by Two – The Vaccinate
Your Baby Web site:
www.vaccinateyourbaby.org

Federal Advocacy
• Other opportunities for involvement:– Attend AAP Advocacy Institute
• March 10-12, 2010 in Chicago
– Familiarize yourself with AAP position papers– Become a Key Contact for the AAP Federal
Affairs Advocacy Network (FAAN)
You Can Make a Difference!
• Find out the special needs of your clinic or community
• Develop a project YOU have a passion for• Return the Project Outcome Report for
ImmuneWise. This will help us improve future advocacy projects!
• Let us know what you have accomplished. We want to recognize you in district newsletters and !
Brought to You By:
• SOMSRFT Executive Committee Advocacy Subcommittee– Co-Chairs
• Drs. Katie Snyder and Jennifer Williams
– Members• Drs. Shawn Batlivala, Clara Filice, Jenni Linebarger,
Christina Robinson, Sara Slovin, Josh Smith, Amy Starmer, David Tayloe
– Other Contributors/Supporters• Lucy Crain, MD, FAAP, Buz Harlor, MD, FAAP,
Michael Warren, MD, FAAP, Julie Raymond, Ian Van Dinther
Recommended

















