Centre forHealth Communication
Design Responses to Changing Clinical Practices

Centre forHealth Communication
Why a Re-think?
• Changing clinical practices and treatment patterns
• Multidisciplinary approach to care, clinical pathways
• Technology – clinical and support
• Staff shortages – optimum utilisation
• Patient expectations – well informed, competition
• Financial imperatives – Health $$$$ under pressure

Centre forHealth Communication
Hospital Space Allocation
1950s Now

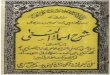
Centre forHealth Communication
Ambulatory
23%
D&T
24% Inpatients
18%
Research
4%Education
2%
Administration
10%
Back of House
4%
Cricitical Care
5%
FOH/Family
10%
350 Beds[250 multi day + 100 day]

Centre forHealth Communication
Conceptual Functional Models
• Zonal Model– Horizontal– Vertical
• Institutional Model- Number of ‘mini’ hospitals
• Separation of Ambulatory Procedures

Centre forHealth Communication
Zonal Model - HorizontalAMBULATORY
D&T
WARDS
Norfolk & Norwich Hospital, UK
AMBULATORY
D&T
WARDS

Centre forHealth Communication
Zonal Model - VerticalINPATIENTS
PROCEDURES / INTENSIVE CARE
D &T/AMBULATORY
Royal North Shore Hospital
Sydney
INPATIENTS
PROCEDURES
D&T / AMBULATORY

Centre forHealth Communication
Institutional Model
GASTRO
RESPIRATORY
ORTHO
NEUROSCIENCES
CANCER
WOMEN’S & KIDS
VASCULAR
CARDIAC
HOT FLOOR
MENTAL HEALTH
GERIATRIC
RPA Hospital, Sydney

Centre forHealth Communication

Centre forHealth Communication
CSSD PaLMS plant
PlantAdminExecutive – RNSH, NSCCAHSMedical ServicesDivision of MedicineDivision of Surgery and AnaethesiaAllied Health
Plant
Inpatient units
Inpatient units
Diagnostic +Treatment
Clinical offices
Clinical officesClinical offices
Clinical offices
Administration

Centre forHealth Communication
Implications for Facility Planning
1. D&T Block with Inpatient Units 2. Horizontal ‘mini hospitals’

Centre forHealth Communication
Areas addressed today
• Inpatient Units
• Emergency Department
• Interventional Suite
• Workplace

Centre forHealth Communication
Inpatient Units
• Large number of beds on one floor – flexibility; resource sharing
• Greater numbers of 1-bed rooms
• Larger rooms• Acuity Adaptable - patient centred care - treatment and clinical
procedures at bedside - Family and carers - infection control
• Decentralised staff stations, taking advantage of communication systems
• Modules of 7 - 10 beds

Centre forHealth Communication
Inpatient Units - decentralised staff stationsSt Vincent’s Public and Private Hospitals Redevelopment, Sydney

Centre forHealth Communication
Typical Inpatient ArrangementTrondheim University Hospital, Norway

Centre forHealth Communication

Centre forHealth Communication
Bed Utilization
85 beds in single rooms=
100 beds in multi-bed rooms
Anecdotal evidence from America, quoted by BDPGroupe6 of UK/France

Centre forHealth Communication
Emergency Department
• Process Re-think Lean Thinking principles
• Patient processing Triaged according to - primary care, short stay or admitted
• Patient waiting Minimal – more numbers of walk-through triage stations; waiting in care area
• Short Stay unit 30-bed unit ; stays of upto 2 days?
• Imaging Dedicated, decentralised

Centre forHealth Communication

Centre forHealth Communication
Interventional Suite
• Process Re-think Induction Rooms - why?Pre-op Holding - increase; patient prep
• Future Technology Real time Imagery – MRI in OR
• More Equipment Larger ORs; Control Rooms
• Barn Theatres Zurich; Liverpool UK; Oswestry UK - orthopaedic surgery,……
Recommended











![Blazhevich - 70 Etudes for Tuba [1of2]](https://img.pdfslide.us/doc/110x75/544dfcc7b1af9f23638b4a1b/blazhevich-70-etudes-for-tuba-1of2.jpg)