Embed Size (px)
Citation preview

Year 2 MBChB
Clinical Skills
Examination of the hands & nails
Written by: Clinical Skills Lecturer Team
Reviewed by: Dr Stuart N Cohen, Specialty Lead for Dermatology

2
Learning objectives
• To understand the basic principles of inspection of the hands and nails.
• To demonstrate an understanding of linking hand and nail signs to a differential diagnosis.
Theory and background
Information from examination of the patient should always be interpreted in conjunction with the history. Apparent
indicators of disease may turn out to be congenital or secondary to trauma. It is important to know whether changes are
acute or chronic, and whether they are stable or evolving. Inspection is a key component of physical examination. In the
hands and nails, many different findings can occur, which can indicate a wide array of diagnoses. Some are primary skin or
nail conditions, whilst others are secondary to underlying disease processes.
Please be aware that this study guide is not exhaustive. It is designed to give you an overview of some findings that you may
encounter whilst performing an examination of a patient’s hands and nails. Further reading may be needed to help you to
understand why certain disease processes may cause different signs on the hands and nails to develop.
Indications
Inspecting the hands and nails can be a key component of clinical examinations, for example:
o Respiratory exam
o Gastrointestinal exam
o Thyroid exam
o Cardiovascular exam
o Neurological exams
o Musculoskeletal exams
o Dermatological exams
Procedure
Patient safety
On first meeting a patient, introduce yourself, and confirm that you have the correct patient by name and date of
birth; if available please check this with the wristband and written documentation, confirming the patients NHS /
hospital number or first line of address.
Check the patient’s allergy status, being aware of the equipment you will be using in your examination. Ensure
that the procedure is explained to the patient in terms that they understand, gain informed consent and ensure
that you are supervised, with a chaperone available as appropriate. Don personal protective equipment as
required, especially if you are likely to come into contact with bodily fluids.
Be aware of hand hygiene and preventing the spread of disease, WHO (2018) http://www.who.int/infection-
prevention/tools/hand-hygiene/en/

3
Inspection of the hands
Observe for:
Movement
Please be aware that some patients will be unable to move how you wish them to, due to frailty or underlying
medical conditions. Ensure that you allow for this during your examination and do not cause the patient distress
or discomfort.
Ask the patient to raise their hands out in front of them with their palms facing the floor. You may see:
o Tremor (this may be due to a number of reasons, such as alcohol withdrawal, parkinsonism, thyrotoxicosis
or medication)
Then ask the patient to hold out their arms with their wrists extended to check for:
o Metabolic flap (this may be due to a neurological cause or increased CO2 retention)
o Asterixis – coarse flapping tremor (occurs with hepatic encephalopathy)
Skin texture
Make sure that you are assessing the dorsal and palmar aspect of the hands (front and back), and ensure you are
comparing both sides to each other. Don’t forget to ask the patient if anything you note is new or old for them; if

4
they have any scars ask them what caused them. This may aid you in your diagnosis. When examining the hands
you may find:
o A rash such as dermatitis
o Scarring
o Swelling / thickening
o Callouses (a thickening or hardened part of the skin)
o Loss of muscle bulk (wasting)
o Changes in colour
o Clammy palms
Skin colour
o Peripheral cyanosis (this could be due to lack of oxygen, or they could be cold or have poor circulation)
o Pale skin creases (if the skin creases are as pale as the surrounding palms, this may be an indicator of
anaemia)
o Palmar erythema (this may be normal for the patient; specific causes include pregnancy, chronic liver
disease or thyrotoxicosis)
o Tobacco staining of the fingers from smoking
Hand and Nail changes
Fig.1
Dupuytren’s contracture – This is a thickening of the
palmar fascia, (the band or sheet of connective tissue,
primarily collagen, beneath the skin that attaches,
stabilises, encloses and separates muscle and other
internal structures), causing fixed flexed deformity and
usually affects the little and ring fingers. Usually starts as
small hard nodules on the palmar surface under the
skin. This is often familial but may be caused by
alcoholism or other factors.
http://meded.ucsd.edu/clinicalimg/browse.htm
Charlie Goldberg M.D.
Fig.2
Peripheral cyanosis – Distal bluish discolouration which
can be associated with hypoperfusion, environmental
factors i.e. cold temperature or the patient may have a
cardiorespiratory condition causing hypoxia.
By James Heilman, MD - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=17978808

5
Fig.3
Raynaud’s phenomenon – This is digital ischaemia which is
induced by cold or emotional stress. It has three phases,
pallor, cyanosis and redness. It may be primary and idiopathic
(Raynaud’s disease), or secondary (Raynaud’s syndrome) due
to factors such as malignancy, connective tissue syndromes
(e.g. systemic lupus erythematosus [SLE]), atherosclerosis (a
build-up of plaque inside the arteries) or it may be drug
related.
Kindly anonymously donated to the Clinical Skills Team
Fig.4
Palmar erythema – Redness of the palmar skin.
This may be normal for the patient or can be due
to excess oestrogen associated with reduced
hepatic breakdown of hormones. It is also
common in pregnancy or when malabsorption of
hormones is reduced in the presence of liver
damage.
Gastrointestinal system Rochford, Andrew, Hutchison's Clinical Methods, 14, 241-271 Copyright © 2018 © 2018 Elsevier Ltd. All rights reserved
Fig.5
Clubbing – This is where there is a loss of the angle
between the nail bed and the fingernail. The exact
cause of fingernail clubbing is unknown. Whilst it
may be seen in healthy individuals as a congenital
variant, associated chronic conditions include: lung
cancer, chronic lung disease, cyanotic heart
disease, cirrhosis of the liver and inflammatory
bowel disease.
General aspects of examination Dover, Anna R, Macleod's Clinical Examination, 3, 19-36
Copyright © 2018 © 2018 Elsevier Ltd. All rights reserved.

6
Fig.6
Koilonychia – A rare finding of spoon-shaped nails,
which may be a normal variant or caused by chronic
iron deficiency anaemia and occasionally other
factors.
General patient examination and differential diagnosis Drake, William M., Hutchison's Clinical Methods, 2, 15-29 Copyright © 2018 © 2018 Elsevier Ltd. All rights reserved
Fig.7
Lindsay’s nails (half-and-half nails) - Distal red or brown band on
the nails. The proximal nails may be white or pink. This mostly
occurs in the setting of chronic renal failure. Again, this is an
occasional finding but a useful clue if noted on examination.
http://health.allrefer.com/pictures-images/half-and-half-nails.html
Fig.8
Leukonychia - Whitening of the nails, which can
appear as linear or be transverse. True leukonychia
stays white when pressure is applied to the nail bed.
This may be a clinical sign of hypoalbuminemia (low
albumin), which can be seen in nephrotic syndrome (a
form of kidney disease), liver failure and protein
malabsorption.
General patient examination and differential diagnosis Drake, William M., Hutchison's Clinical Methods, 2, 15-29 Copyright © 2018 © 2018 Elsevier Ltd. All rights reserved

7
Fig.9
Beau’s lines - These are deep, grooved lines that run
from side to side on the fingernails or toenails. They
may look like indentations or ridges in the nail plate.
They can be due to cessation of nail growth due to
recent severe illness or chemotherapy but may also
be due to trauma to the nail.
Skin, Hair, and Nails Ball, Jane W., DrPH, RN, CPNP, Seidel's Guide to Physical Examination, Chapter 9, 131-183
Copyright © 2019 Copyright © 2019 by Elsevier, Inc. All rights reserved.
Fig.10
Splinter haemorrhages - Asymmetrical,
splinter-like lesions; the most common cause is
trauma to the individual nail bed. Clinical causes
may include infective endocarditis or vasculitis.
Caused when blood leaks or swells from small
vessels that run up and down the nail bed.
Fig. 11
Janeway’s lesions – Non-tender, haemorrhagic macules of a
few millimetres in diameter. They can be found on the palms
and soles. They are rare but may be indicative of infective
endocarditis, SLE or gonococcaemia (gonorrhoea).
Osler’s nodes - Painful, red, raised lesions found
typically on the fingers and or toes; pain will usually
precede the development of an Osler’s node. The cause
is still subject to debate. They are associated with a
number of conditions, but especially infective
endocarditis.
Blood Vessels Klatt, Edward C., MD, Robbins and Cotran Atlas of Pathology, Chapter 1, 1-26.e3
Copyright © 2015 Copyright © 2015, 2010, 2006 by Saunders, an imprint of Elsevier Inc
Both Janeway’s lesions and Osler’s nodes are very similar in appearance and may be found in conjunction.

8
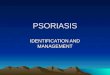
Fig.12
Pitting – Small depressions in the nail plate. They are most
commonly seen in psoriasis, but are also a feature of other
skin conditions such as eczema, alopecia areata and lichen
planus. They are caused by defective development of the
layers of the superficial nail plate.
http://www.dermatlas.org/derm/result.cfm?Diagnosis=-946037564
Fig.13
Oncholyosis – This is where the free edge of the
nail separates from the underlying nail bed. It can
be caused by psoriasis, fungal infections or
thyrotoxicosis.
Fig.14
Onychomycosis – This is infection of the nail plate
with dermatophyte fungus. It can cause white,
yellowish, brown or sometimes dark discoloration
of the nail, as well as onycholysis. Toe-nails often
become markedly thickened.
Fungal Diseases Bolognia, Jean L., MD, Dermatology Essentials, 64, 613-633 Copyright © 2014 © 2014, Elsevier Inc. All rights reserved

9
Fig.15
Contact dermatitis – this is divided into allergic contact
dermatitis (ACD), in which the eruption is due to type IV
(delayed) hypersensitivity, and irritant contact dermatitis
(ICD), where environmental insults – such as repeated
exposure to water or irritant chemicals – exceed the
skin’s barrier defences. Both present with dryness,
erythema and scaling. Vesiculation (blistering) may occur
in ACD and itching can be severe; fissures are more likely
to be seen in ICD (or palmar psoriasis), where soreness is
often more marked. ICD can exacerbate any other form
of hand dermatitis.
Eczema – Basic principles and irritant contact dermatitis Gawkrodger, David J., DSc MD FRCP FRCPE, Dermatology: An Illustrated Colour Text, 17, 34-35.e1
Copyright © 2017 © 2017 Elsevier Ltd. All rights reserved
Fig.16
Atopic dermatitis (atopic eczema) – Commonly familial and
more prevalent in children, usually presents as itchy, dry,
cracked sore or red skin especially on flexor aspects of the
skin (back of elbows and knees). It can be widespread and
frequently affects the hands. There is often an irritant
component, from wet-work or frequent handwashing, and
exposure to soaps or detergents.
Image kindly donated to the clinical skills department
Fig.17
Psoriasis – A chronic, immune-mediated inflammatory
skin disorder. It is a common papulosquamous condition
characterised by well-demarcated, erythematous
plaques with overlying thick, silvery scale. Psoriasis
occurs at all ages and is characterised by chronic and
relapsing episodes. There are varying subtypes. It is most
commonly found on the extensor aspects of the elbows
and knees, scalp, periumbilical region, lumbosacral
region and intergluteal cleft. There is also a
palmoplantar variant (i.e. affecting the palms and soles)
which can occur in isolation or alongside more
widespread psoriasis.

10
http://www.danderm.dk/atlas/5-32-4.html
Fig.18
Paronychia (whitlow) – This is an infection of
the skin just next to the nail (the nail-fold). The
skin is usually red, swollen and tender; there
may be a visible collection of pus that requires
lancing. Causes include bacteria and Candida
(a type of yeast). This is more common in
patients who bite their nails or have had some
trauma to the area.
Skin disorders Henry, Michael M, MB FRCS, Clinical Surgery, 39, 703-720 Copyright © 2012 © 2012 Elsevier Ltd. All rights reserved.
Fig. 19
Acropachy – A rare and severe autoimmune
dermopathy associated with Graves’
hyperthyroidism, where there is soft tissue swelling
of the hands and feet that in turn causes clubbing of
the fingers and toes. There is also periostitis
(inflammation of the periosteum which overlies
bone), which can lead to new bone formation.
General aspects of examination Dover, Anna R, Macleod's Clinical Examination, 3, 19-36
Copyright © 2018 © 2018 Elsevier Ltd. All rights reserved Fig.20
Nicotine tar staining – Tobacco stains on a heavy cigarette smoker,
primarily on the second and third finger.
By James Heilman, MD - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=9444890
Commented [SNC1]: This is a more appropriate picture of psoriasis. D@nderm images are approved for educational use without permission. I’m afraid I’ve messed up the spacing though, here and below – hopefully you can fix it.

11
fig.21
Muscle wasting (atrophy) – Can
be due to a lower motor neurone
lesion, but may be seen in
patients with a long-standing
upper motor neurone lesion. Can
also be caused by muscular
dystrophy, motor neurone
disease and trauma. Can result
from the muscles in the area not
being used (disuse atrophy).
(Note that in the image, the
tendons in the left hand appear
more pronounced than the right
due to muscle wasting).
The neurological examination: The peripheral nervous system Talley, Nicholas J, MBBS (Hons)(NSW), MD (NSW), PhD (Syd), MMedSci (Clin Epi)(Newc.), FRACP, FAFPHM, FAHMS, FRCP (Lond. & Edin.), FACP, FACG, AGAF, FAMS, FRCPI (Hon), Talley & O'Connor's Clinical Examination, Chapter 34, 548-579 Copyright © 2018 ©2018 Elsevier Australia. 1st edition ©1988, 2nd edition ©1992, 3rd edition ©1996, 4th edition ©2001, 5th edition ©2006, 6th edition ©2010, 7th edition ©2014 Elsevier Australia
Fig.22
Rheumatoid arthritis – An autoimmune disease in which the
immune system damages the cells that line the joints. It frequently
affects the distal interphalangeal and proximal interphalangeal
joints. It causes pain, swelling and stiffness, and over time leads to
damage to the joints, cartilage and nearby bone. It can result in
deformity, and ulnar deviation of the hand.
Other Rheumatologic Diseases Bolognia, Jean L., MD, Dermatology Essentials, 37, 329-335
Copyright © 2014 © 2014, Elsevier Inc. All rights reserved.
Commented [SNC2]: I’d never heard of Lou Gehrig!
Commented [SNC3]: Stroke deleted as this is covered by upper motor neurone lesion

12
Fig.23
Osteoarthritis – This is the most common
type of joint disease, in which the protective
cartilage on the ends of the bones breaks
down causing pain, swelling and restriction
of movement. In the hands, the DIP joints are
most commonly affected. Bony growths may
occur. Many risk factors are recognised in
osteoarthritis, including age, repetitive use
of joints, previous inflammatory conditions
such as rheumatoid arthritis or gout, and
bony trauma including surgery.
Osteoarthritis Aitken, Marc Joseph, MBChB, MRCP (UK), Crash Course Rheumatology and Orthopaedics, 11, 67-71 Copyright © 2019 © 2019, Elsevier Limited. All rights reserved.
Some other signs you may see in patients with Rheumatoid / Osteoarthritis Arthritis
Rheumatoid Arthritis and Osteoarthritis
Hawkins, Tina, Clinical Pharmacy and Therapeutics, 54, 923-948 Typical ulnar deviation, swan neck and boutonnière deformities. Copyright © 2019 © 2019, Elsevier Limited. All rights reserved.

13
Quincke’s sign – This occurs when there is aortic insufficiency. For example, in aortic regurgitation where blood
flows back into a dilated left ventricle it causes a decrease in diastolic pressure and a subsequent increase in
stroke volume. This manifests as a blanching and flushing of the nail beds. Follow the below link to watch a
video of how this appears.
https://www.youtube.com/watch?v=V7u3vaKEDCI
Quick guide to hands and nail assessment
Hand or Nail Changes Description Differential diagnosis
Dupuytren’s contraction Fig.1
Flexed fixed deformity Thickening of the palmar fascia,
may be hereditary or be due to
chronic liver disease
Peripheral cyanosis Fig.2
Discoloration to the peripheries May be due to cold, hypoperfusion
or cardiovascular disease
Raynaud’s phenomenon Fig.3
Discoloration to the digits and cold
to the touch
Can be idiopathic or due to a
secondary disease process
Palmar erythema Fig.4
Redness of the palms May be genetic, or due to chronic
liver disease or pregnancy
Clubbing Fig.5
Loss of the nail angle Multiple disease processes may
cause this; may also be normal for
the patient
Koilonychia Fig.6
Spoon shaped depression of the
nail plate
Iron deficiency anaemia
Lindsay’s nails Fig.7
White or brown half-and-half nails Chronic kidney disease
Leukonychia Fig.8
White spots, ridges or a complete
discoloration of the nail
Hypoalbuminemia
Beau’s Lines Fig.9
Transverse grooves Can be due to any severe systemic
illness that may affect the growth
of the nails, or trauma
Splinter haemorrhages Fig.10
Small red streaks that lie
longitudinally in the nail bed
Trauma, infective endocarditis or
vasculitis
Janeway’s lesions Fig.11
Painless blanching macules on the
palms of the thenar/hypothenar
eminences
May be caused by infective
endocarditis, systemic lupus
erythematosus (SLE) or
gonococcaemia (gonorrhoea)
Osler’s nodes Painful raised erythematous
lesions, typically found on the
pads of the fingers
May be due to infective
endocarditis and having an
immune complex disposition
Pitting Fig.12
Fine or coarse indentations in the
nail bed
Can be due to a number of
conditions such as alopecia areata,
psoriasis, eczema or lichen planus

14
Onycholysis Fig.13
Separation of the nail plate from
the underlying nail bed
Usually due to psoriasis or fungus
Onychomycosis Fig.14
Thickening and discoloration of
the nail plate
Fungal infection
Atopic eczema Fig.15
Dry, red, itchy and flaky skin Usually a familial tendency;
exacerbated by exposure to water
or irritant chemicals
Contact dermatitis Fig 16
It usually involves itchy, dry, red,
flaky skin. The skin may also
blister, ooze or flake off
Dermatitis is a common condition
that can be caused by many
different factors
Psoriasis Fig.17
Well-demarcated, erythematous,
scaly plaques
A common, chronic, immune-
mediated inflammatory skin
disorder
Paronychia Fig.18
Red, swollen and often pus-filled
area around the nail bed
Usually caused by a localised
infection
Acropachy Fig.19
Soft tissue swelling of the hands
that causes finger clubbing and
periosteal reaction of the
extremities
Associated with Graves’ disease
Nicotine tar staining Fig.20
Tobacco stains Suggests heavy smoking
Muscle wasting Fig.21
Wasting of the muscles of the
hands
May be due to a neurological
lesions, muscular dystrophy,
motor neurone disease, stroke or
trauma.
Rheumatoid arthritis Fig.22
Pain, swelling, weakness and
deformities
Caused by the body’s own immune
system attacking it
Osteoarthritis Fig.23
Pain, swelling, stiffness and bony
growths
Caused by the protective cartilage
on the ends of the bones breaking
down
Quincke’s sign A pulsating flicker in the nail beds This is due to aortic insufficiency
Further resources
The British association of Dermatologists
http://www.bad.org.uk/
British Hair and Nail society
https://bhns.org.uk/
Patient info
https://patient.info/
DermNet NZ
https://www.dermnetnz.org/