Embed Size (px)
Citation preview

ASC X12N UDISAC MayJune 2015
Revised 3/2011 Page 1 of 15
X12N UDI SACMay-June 2015
Refer to Scheduled Meetings Table for Call in Information
Group LeadershipChair Name Company Term End
DatePhone Email
Laurie Burckhardt WPS 608-223-5851 [email protected]
Gloria Davis(Claims)
QSI/NextGenHealthcareInformationSystem
404-467-1500 [email protected]
Secretary Name Company Term EndDate
Phone Email
Cindy Monarch BCBS of Michigan [email protected]
Quorum Requirement StatementThis group enforces quorum requirements for group voting items.
This group does not enforce quorum requirements for group voting items. X
Key Discussion Item – Attendance = 34Discussion – CR 1308 BRTS
Continued review of Risks and Challenges document;o Further discussion of Item 4 –
Moving discussion of this item to next week as Laurie has not had the opportunity to confirm if payers andresearchers have access to the all payers database;
Discussion will also include information she received from X12 Supply Chain representative;o Discussion of Items 6, 7, and 8
Stanley Nachimson expressed his concern with these items being included when we do not know what thecost or what the solution will be;
Scheduled MeetingsType of Meeting Date Location/Call in Contact AgendaCurrent Meeting 05/04/2015 712-432-0393
Access Code:218856#
LaurieBurckhardtor GloriaDavis
CR1308 BRTS
Next StandingMeeting
May 31 – June 4,2015
San Antonio, TX Co-Chairs Voting ItemsBRTS
Interim Meeting Mondays, 1:00 pmto 2:30 pm EST
712-432-0393Access Code:219956#
LaurieBurckhardtor GloriaDavis
CR 1308 BRTS

ASC X12N UDISAC MayJune 2015
Revised 3/2011 Page 2 of 15
Key Discussion Item – Attendance = 34Discussion – CR 1308 BRTS
Discussed combining Items 6 and 7 as they both speak to technology; Participants agreed technology and costs should be looked at independently; George noted he spoke with a large hospital and who indicated they are very happy with the process
they have implemented for UDI; Noted that UDI can be carried from EHR to the billing system via an HL7 transaction; Gloria was to draft revisions to Item 7 but agrees it can be combined with item 6; Drafted “Technology challenges for system integrations to link supply chain/inventory systems to
revenue cycle systems as well as the ability to pull information from the clinical record to the billingsystem.”“Adding UDI to administrative transactions could require significant system changes for providers,health plans, clearinghouses, and billing vendors with costs incurred. In order to achieve the fullbenefits of UDI for implantable devices, willing partners should be aware that the UDI must beadopted in all systems that capture data across the lifecycle of a device. These include manufacturersystems, clinical inventory systems, electronic health records, payer systems and others. “
Discussed referencing HL7 and that there could be a need to harmonize the transfer of UDI betweensystems that use different standards; added “Providers will need to consider how data is movedbetween various systems whether via HL7 or X12 transaction.”;
Noted HL7, as of July, does have a place to report the entire UDI; Laurie reminded participants that the Risks and Challenges will be a section in the BRTS, this is not
something that will be included in a Technical Report 3 (TR3) document; possibly this document couldbe something used for education;
Noted the Technical work group may read this section of the BRTS but it will not be incorporated aspart of their solution development;
Discussed when another entity may use the UDI (e.g. X12M Supply Chain – when purchasing a UDI);o Item 7 (formerly item 9) –Costs to implement UDI in revenue cycle systems;
Revised to read “Costs to implement UDI.”o Item 8 – (formerly item 10) – Risks to normal claims processing if errors with UDI on claim
Inclusion of this was questioned and discussed as it references a possible technical solution;
Discussed needing to test prior to implementing by systems not necessarily by standards organization;
Noted claims are edited for a variety of reasons, the introduction of capturing the UDI may or may notimpact payment but could possibly delay payment if payer needed the UDI (between willing tradingpartners);
Laurie moved a portion of information from item 8 to item 6; there was agreement the detail betterreferences information for HL7 collaboration;
Kevin from Geisinger noted the need to reference risk mitigation which the participants discussed;
Revised item detail to read “Whenever new information is being exchanged and validated, considerationneeds to be taken into account when Health plans validate data reported on the claim need to considervalidating the format of the UDI. Any failure of claim edits due to UDI may reject or pend the claim whichmay result in additional work by the health plan and provider and possible delays in the health care revenuecycle.”
o Item 9 (formerly item 11) – Lack of current proof of concept of connecting UDI provider organization’s supplychain/inventory management system, EHR system, and revenue cycle systems
Noted this is covered in the technology discussion via Item 6); participants agreed to remove this item;o New Item 9 (formerly item 12) – Lack of standard UDI due to three issuers and lack of uniformity of what portion
of UDI to transmit;
Participants discussed this being covered as part of the business requirements;

ASC X12N UDISAC MayJune 2015
Revised 3/2011 Page 3 of 15
Key Discussion Item – Attendance = 34Discussion – CR 1308 BRTS
Participants discussed issue/risk being the coexistence of this data for three different issuers;
Noted Medicare has a procedure code for kits applicable for some devices;
Revised to read “Co-existence of three different groups named as issuers of UDIs, GS1, HIBCC, and ICCBBA insuch case provider may split a package and implant portions of 2 different issuers. Provider may need toconsider the ability to send both and document what he did.”
Reference issue with leads; Claudia volunteered to go back and get some additional information; we willcontinue discussion next week;
o Item 10 (formerly item 13) – Not all medical devices are reported on the claim;
Discussed this being a data limitation and its application as a risk/challenge;
Claudia Birkenshaw Garabelli volunteered to do some outreach to locate examples of when packages from 2different vendors are combined and used for a patient;
Revised to read, “When doing data analytics not every patient who may have had an implantable device willbe reported. Analysis can only be done on those when UDI is reported.”
o Laurie noted BRTS name change from CR1308_TGB_WG2_BRTS to CR1308_N_UDI SAC_BRTS.
Next meeting is Monday, May 13th, from 1:00 to 2:30 EST.o Review and approve April 27th and May 4th meeting minutes;o Continue discussion of Risks and Challenges document: review results of Laurie’s Action Items and update Item 4
accordingly; review Claudia’s findings and continue discussion of Item 10.Decisions
None
Action Items:No. Description Owner Assigned Due Date1. Research all payer database topic and
present information to UDI SAC.Laurie Burckhardt 04/20/2015 05/11/2015
2. Contact Supply Chain (X12M)representative to confirm crosswalkactivities.
Laurie Burckhardt 04/20/2015 05/11/2015
3. Locate examples of when packages from2 different vendors are combined andused for a patient.
Claudia BirkenshawGarabelli
04/27/2015 05/11/2015
Scheduled MeetingsType of Meeting Date Location/Call in Contact AgendaCurrent Meeting 05/11/2015 712-432-0393
Access Code:218856#
LaurieBurckhardtor GloriaDavis
CR1308 BRTS
Next StandingMeeting
May 31 – June 4,2015
San Antonio, TX Co-Chairs Voting ItemsBRTS
Interim Meeting Mondays, 1:00 pmto 2:30 pm EST
712-432-0393Access Code:219956#
LaurieBurckhardtor GloriaDavis
CR 1308 BRTS

ASC X12N UDISAC MayJune 2015
Revised 3/2011 Page 4 of 15
Key Discussion Item – Attendance = 44Discussion – CR 1308 BRTS
Review and approve April 27th and May 4th meeting minutes;o Noted both are posted to CD;o Gloria Davis motion to approve; Nancy Caro seconded the motion; there were no comments; minutes
unanimously approved;
Continued review of Risks and Challenges document;o Item 4 “Ability for physicians and other health care providers to access health plans’ data on medical devices”
and discussion of Laurie’s action items;
Laurie relayed that payers do have access to the all payer database; data submitted is voluntary;
Participants discussed the application of this as a risk/challenge; several participants noted this to be moreof a concern not necessarily a risk or challenge;
Approach taken is based on the usage and this being between a willing payer and trading partner; all payerdatabase is more local, there isn’t a true central database;
Noted that this will help to facilitate aggregates at a higher level for data analyses; seems to be more of abenefit than a risk;
George Arges noted the issue is not the UDI, it is the approach (the need to gather information frommultiple payers);
George and Claudia noted they had concerns regarding removing this as a risk/challenge; however,participants agreed to remove item 4;
o Claudia is still gathering information; we will review this during the June 8th interim meeting;
Question asked if this is limited to implants; Claudia confirmed she is focusing on implants;
Participants discussed if there would a single UDI for a combination product such as an abdominal meshtreated with antibacterial drug; Benai agreed this would be considered a combination product and the mainproduct would be identified in the UDI; expects there would be a UDI for non-coated and another UDI forthe coated mesh;
Briefly discussed reporting a partial package; noted if an implant is sold as a group it should be reported as agroup; could not (should not) separate pieces within a package;
We will discuss this further during the interim June 8th meeting; Laurie invited other participants to obtainany additional information that will help the group discuss this topic;
o Laurie reviewed item 5, 6, 7 and 8;
There was no additional feedback from participants on these items;
Noted Item 8 is the item Claudia is doing further information gatheringo Item 10 – Lack of standard definition of “high risk” medical devices for reporting.
Noted the statement of “…lack of standard definition” doesn’t make sense; participants further discussedhigh risk devices and device lists;
Noted this adds administrative burden for everyone;
Noted that X12 will not be maintaining a standard list;
Stanley Nachimson commented this duplicates that not everyone is going to be reporting the same device;Heather McComas disagreed and sees this as a different flavor of item 4; item 10 addresses theadministrative risk;
Discussed FDA Class III definition and noted it does not contain/reference “high risk”; Class III are life savingor life sustaining devices; however, it is known that there are some Class III devices that can be consideredhigh risk;
Noted we have been discussing implantable devices, not necessarily high risk devices; there are Class IIIdevices that are implantable; BRTS addresses implantable devices not high risk devices;
Revised to read: “Health plans may request a different list of implantable devices to be reported whichresults in providers maintaining various lists of UDIs to be sent. While the FDA provides definitions of device

ASC X12N UDISAC MayJune 2015
Revised 3/2011 Page 5 of 15
Key Discussion Item – Attendance = 44Discussion – CR 1308 BRTS
Classes (I, II, III etc) there is no single list of implantable devices required by a health plan. Those who arewilling trading partners may want to limit the eset of devices linked to UDI to include those high risk and/orimplantable devices where the granular device information would provide enough value to justify theinvestment in resources and system and contract changes. It is assumed that both providers and payers willdiscuss the required system changes with vendors prior to entering into their agreements to exchange UDI.”
Nancy did confirm that the term “high risk device” is used in other UDI papers/documents; Laurie noted thatit appears that implantable and high risk can be used interchangeably; George noted this may be based onthe context of the document;
There was no additional feedback on the revision;o Item 11 – Health plan “formulary of devices” vs. providers purchasing agreements.
Reviewed additional verbiage provided by Terrie Reed;
Discussed losses with purchasing; some participants felt this was not germane to the UDI; this is somethingthat occurs today;
Revised paragraph to read: “Many providers work under purchasing agreements and with group purchasingorganizations to obtain the medical devices it uses. If health plans develop formularies of devices, thedevices that it “allows” may conflict with the providers preferred device impacting provider’sreimbursement. It is assumed that, if formularies are developed as a result of the voluntary exchange ofUDI, then there will be communication between the willing trading partners so that there may be impact toprovider reimbursement. ”
o Item 12 – UDI is not needed to adjudicate the claim;
Nancy noted this was put as a risk because there wasn’t anything in the BRTS that payers were going to usethe UDI to pay claims but noted that this has been added to the BRTS;
Stanley noted the use of a UDI formulary; however, feels this is not a relevant argument/risk; the point ismoot;
Some participants felt this is not any different than the NDC; a payer may not be able to properly adjudicatea claim without it (UDI could tie back to contractual fee schedule agreement);
Discussed trading partner agreement versus TR3 requirements;
Laurie commented if not required to be on the claim, this item would not be needed;
Will continue discussion of item 12 in person at the Standing Meeting, Monday, June 1st;
Reminder that the May 18th and May 25th meetings have been cancelled;
Next meeting will be in person at the ASC X12 Standing meeting, the afternoon of Monday, June 1st, from 1:00 pmto 4:00 pm; next conference call is on Monday, June 8th;
Decisions
None
Action Items:No. Description Owner Assigned Due Date1. Research all payer database topic and
present information to UDI SAC.Laurie Burckhardt 04/20/2015 Complete
2. Contact Supply Chain (X12M)representative to confirm crosswalkactivities.
Laurie Burckhardt 04/20/2015 Complete
3. Locate examples of when packages from2 different vendors are combined andused for a patient.
Claudia BirkenshawGarabelli
04/27/2015 06/08/2015

ASC X12N UDISAC MayJune 2015
Revised 3/2011 Page 6 of 15
Key Discussion Item – Attendance = 61Discussion
Laurie reviewed the June 1st standing meeting minutes with participants;o Referenced Margaret W’s review of Class I and Class II;o There was some discussion regarding NDC for supplies being replaced by a UDI;
Discussed concern regarding payer receiving NDC and it then it changes to a UDI; clarified that only newsupplies would be assigned a UDI;
Stanley N noted NDC codes are a HIPAA defined code set for drugs and pharmaceuticals; HCPCS are thenamed code set for supplies codes;
Behnaz M clarified that NDC codes are not being replaced, HRIN (health related item number) codes (NDClike codes) are to be removed from packages as of a certain date;
o Approval of the standing meeting minutes will occur at the next meeting, Monday, June 15th;
Continued review of CR 1308 BRTS document;o Section 2.1 – Business Requirements
B8 – noted
Participants agreed the comment affiliated with Requirements has been addressed and can be removed;
Discussed Stanley N’s comment regarding providers; Discussed that the exchange of UDI would typically involve institutional/facility not necessarily
individual provider or clinician; noted surgical suites can occur in office (e.g. breast implant); Participants agreed to leave “provider” as a generic reference;
Discussed hospital claims typically reporting on claims at the line level; services are summarized at theheader level; line level summarized at the revenue code level;
Updated B6 with the FDA GUDID url;o Section 2.2 - Business Assumptions
BA1 discussion:o Gloria D noted the assumption is not addressing supplies;o Discussed the need to include verbiage around the UDI being included on professional claimso Steve R noted there are no CRs regarding UDI in X12M;o Revised to read, “This change request is only addressing devices that are implantable. It is not
addressing all medical devices or supplies that may be assigned a UDI.”
BA2 – no additional feedback or discussion;
BA3 discussion:o Laurie B. noted that the Product Identifier are not part of the GUDID; Indicates the production
identifiers should be reported when indicated by the GUDID;o Participants discussed that the device identifier can be used for validation purposes of production
identifiers;
Scheduled MeetingsType of Meeting Date Location/Call in Contact AgendaCurrent Meeting 06/08/2015 712-432-0393
Access Code:218856#
LaurieBurckhardt orGloria Davis
CR1308 BRTS
Next StandingMeeting
Sept 27 – Oct 1,2015
Charlotte, NC Co-Chairs Voting ItemsBRTS
Interim Meeting Mondays, 1:00 pmto 2:30 pm EST
712-432-0393Access Code:219956#
LaurieBurckhardt orGloria Davis
CR 1308 BRTS

ASC X12N UDISAC MayJune 2015
Revised 3/2011 Page 7 of 15
Key Discussion Item – Attendance = 61Discussion
o Revised to read “The GUDID provides valid device identifiers and indicates what productionidentifiers will be transmitted (for example, lot number, serial number, expiration date).”
BA4 discussion:o Stanley questioned why we are assuming this will be in the hospital’s EHR; the participants noted
EHR is an example; discussed other system where it could be captured/stored;o Revised to read, “The provider has the ability to capture, store (e.g. EHR, supply system, revenue
cycle), to link to appropriate patient record and share the UDI with willing trading partners.”
BA5 discussion:o Reviewed Use Cases 1.4.1.8 and 1.4.1.9o Laurie B noted that all payer database, people may apply to have access to the data;o Joe D commented that the use cases assume that qualified researchers have access to the claims
data; noted claims because tradingo Revised to read, “Use cases (1.4.1.8 and 1.4.1.9) above assumes qualified researchers have access to
the exchanged data.”
Created BA6 to address UDI for supplies;o “A separate change request may be submitted requesting UDI for supplies to be added to the claim
transaction.”o Several participants noted that adding supplies will increase the scope tremendously; all agreed this
BRTS is only focusing on implantable devices;
No other business assumptions were identified;o Laurie reviewed the BRTS with participants and there were no other comments/notes remaining for discussion;
Gloria reviewed revised Risks and Challenges documento Noted that last week review at the Standing Meeting resulted in accepting all changes;o Gloria asked participants if the format of Item 8, 9, and 10 need to align with the format of other items;
participants agreed and this resulted in adding descriptions for each as follows:
Item 8 – Multiple Issuers of UDI.
Item 9 – Not all implanted devices are reported.
Item 10 – Health plans may request different list of implantable device to be reported which results inproviders maintaining various lists of UDIs.
o Gloria noted item 12 is still open; pending additional information from AMA (Nancy); will be discussed at nextweek’s meeting;
o Noted this document will become Section 1.3 of the BRTS;
Next meeting is Monday, June 15th
o Review and approve June 1st standing meeting minutes;o Review rework of B7 and B8 (Laurie and Gloria to complete this week);o Review examples identified by Claudia (action item 3);o Review additional information for item 12 in the Risks and Challenges document.
Decisions
None
Action Items:No. Description Owner Assigned Due Date1. Research all payer database topic and
present information to UDI SAC.Laurie Burckhardt 04/20/2015 Complete
ASC X12N UDISAC MayJune 2015
Revised 3/2011 Page 8 of 15
Action Items:No. Description Owner Assigned Due Date2. Contact Supply Chain (X12M)
representative to confirm crosswalkactivities.
Laurie Burckhardt 04/20/2015 Complete
3. Locate examples of when packagesfrom 2 different vendors are combinedand used for a patient.
Claudia BirkenshawGarabelli
04/27/2015 06/15/2015
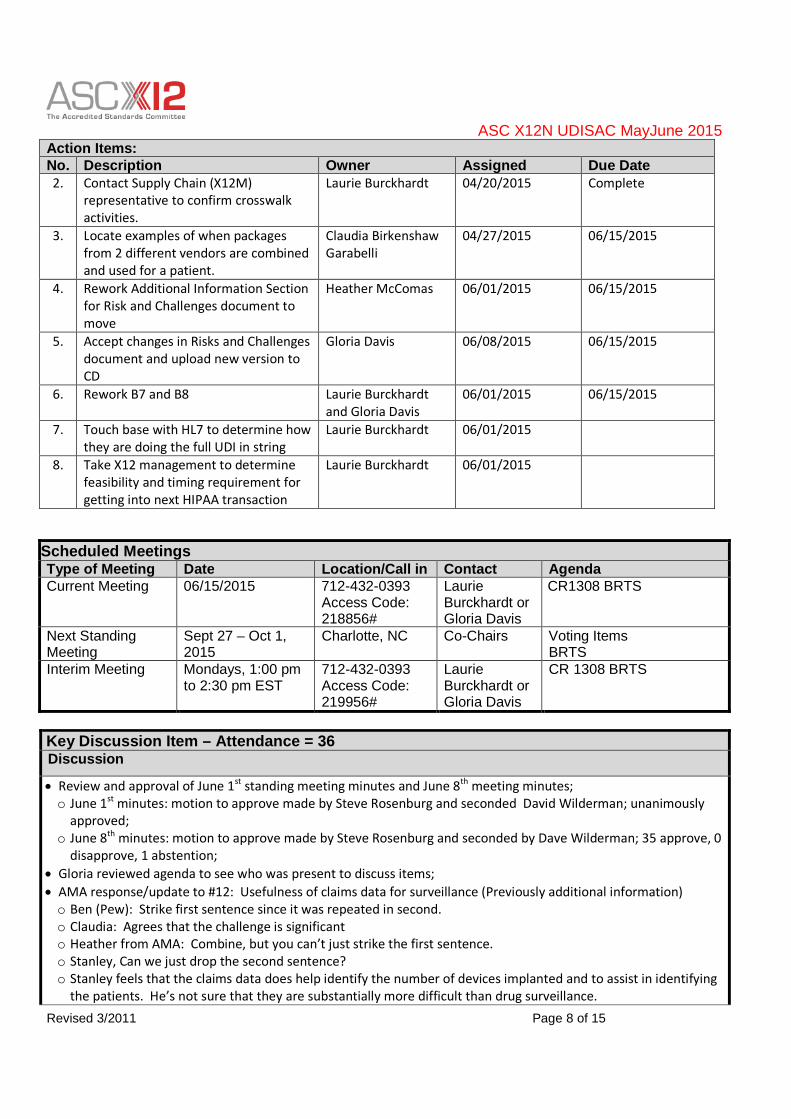
4. Rework Additional Information Sectionfor Risk and Challenges document tomove
Heather McComas 06/01/2015 06/15/2015
5. Accept changes in Risks and Challengesdocument and upload new version toCD
Gloria Davis 06/08/2015 06/15/2015
6. Rework B7 and B8 Laurie Burckhardtand Gloria Davis
06/01/2015 06/15/2015
7. Touch base with HL7 to determine howthey are doing the full UDI in string
Laurie Burckhardt 06/01/2015
8. Take X12 management to determinefeasibility and timing requirement forgetting into next HIPAA transaction
Laurie Burckhardt 06/01/2015
Key Discussion Item – Attendance = 36Discussion
Review and approval of June 1st standing meeting minutes and June 8th meeting minutes;o June 1st minutes: motion to approve made by Steve Rosenburg and seconded David Wilderman; unanimously
approved;o June 8th minutes: motion to approve made by Steve Rosenburg and seconded by Dave Wilderman; 35 approve, 0
disapprove, 1 abstention;
Gloria reviewed agenda to see who was present to discuss items;
AMA response/update to #12: Usefulness of claims data for surveillance (Previously additional information)o Ben (Pew): Strike first sentence since it was repeated in second.o Claudia: Agrees that the challenge is significanto Heather from AMA: Combine, but you can’t just strike the first sentence.o Stanley, Can we just drop the second sentence?o Stanley feels that the claims data does help identify the number of devices implanted and to assist in identifying
the patients. He’s not sure that they are substantially more difficult than drug surveillance.
Scheduled MeetingsType of Meeting Date Location/Call in Contact AgendaCurrent Meeting 06/15/2015 712-432-0393
Access Code:218856#
LaurieBurckhardt orGloria Davis
CR1308 BRTS
Next StandingMeeting
Sept 27 – Oct 1,2015
Charlotte, NC Co-Chairs Voting ItemsBRTS
Interim Meeting Mondays, 1:00 pmto 2:30 pm EST
712-432-0393Access Code:219956#
LaurieBurckhardt orGloria Davis
CR 1308 BRTS
ASC X12N UDISAC MayJune 2015
Revised 3/2011 Page 9 of 15
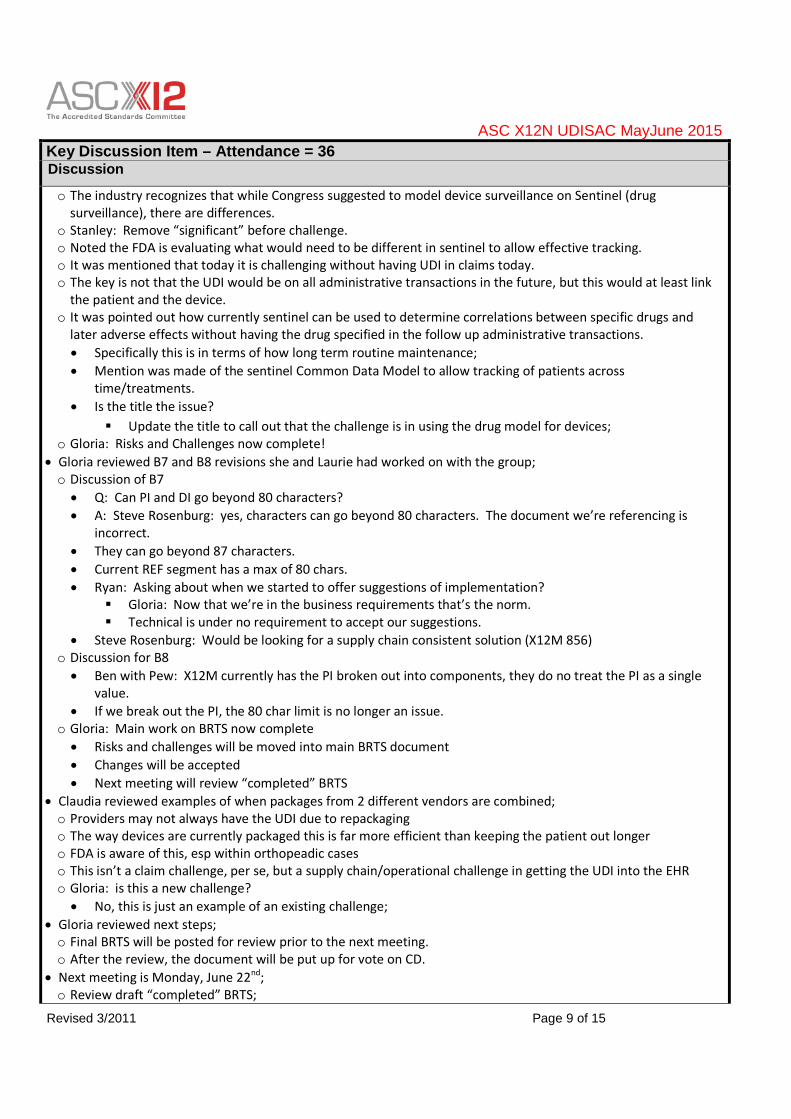
Key Discussion Item – Attendance = 36Discussion
o The industry recognizes that while Congress suggested to model device surveillance on Sentinel (drugsurveillance), there are differences.
o Stanley: Remove “significant” before challenge.o Noted the FDA is evaluating what would need to be different in sentinel to allow effective tracking.o It was mentioned that today it is challenging without having UDI in claims today.o The key is not that the UDI would be on all administrative transactions in the future, but this would at least link
the patient and the device.o It was pointed out how currently sentinel can be used to determine correlations between specific drugs and
later adverse effects without having the drug specified in the follow up administrative transactions.
Specifically this is in terms of how long term routine maintenance;
Mention was made of the sentinel Common Data Model to allow tracking of patients acrosstime/treatments.
Is the title the issue?
Update the title to call out that the challenge is in using the drug model for devices;o Gloria: Risks and Challenges now complete!
Gloria reviewed B7 and B8 revisions she and Laurie had worked on with the group;o Discussion of B7
Q: Can PI and DI go beyond 80 characters?
A: Steve Rosenburg: yes, characters can go beyond 80 characters. The document we’re referencing isincorrect.
They can go beyond 87 characters.
Current REF segment has a max of 80 chars.
Ryan: Asking about when we started to offer suggestions of implementation? Gloria: Now that we’re in the business requirements that’s the norm. Technical is under no requirement to accept our suggestions.
Steve Rosenburg: Would be looking for a supply chain consistent solution (X12M 856)o Discussion for B8
Ben with Pew: X12M currently has the PI broken out into components, they do no treat the PI as a singlevalue.
If we break out the PI, the 80 char limit is no longer an issue.o Gloria: Main work on BRTS now complete
Risks and challenges will be moved into main BRTS document
Changes will be accepted
Next meeting will review “completed” BRTS
Claudia reviewed examples of when packages from 2 different vendors are combined;o Providers may not always have the UDI due to repackagingo The way devices are currently packaged this is far more efficient than keeping the patient out longero FDA is aware of this, esp within orthopeadic caseso This isn’t a claim challenge, per se, but a supply chain/operational challenge in getting the UDI into the EHRo Gloria: is this a new challenge?
No, this is just an example of an existing challenge;
Gloria reviewed next steps;o Final BRTS will be posted for review prior to the next meeting.o After the review, the document will be put up for vote on CD.
Next meeting is Monday, June 22nd;o Review draft “completed” BRTS;

ASC X12N UDISAC MayJune 2015
Revised 3/2011 Page 10 of 15
Key Discussion Item – Attendance = 36Discussion
Decisions
None
Action Items:No. Description Owner Assigned Due Date1. Research all payer database topic and
present information to UDI SAC.Laurie Burckhardt 04/20/2015 Complete
2. Contact Supply Chain (X12M)representative to confirm crosswalkactivities.
Laurie Burckhardt 04/20/2015 Complete
3. Locate examples of when packagesfrom 2 different vendors are combinedand used for a patient.
Claudia BirkenshawGarabelli
04/27/2015 Complete
4. Rework Additional Information Sectionfor Risk and Challenges document tomove
Heather McComas 06/01/2015 Complete
5. Accept changes in Risks and Challengesdocument and upload new version toCD
Gloria Davis 06/08/2015 Complete
6. Rework B7 and B8 Laurie Burckhardtand Gloria Davis
06/01/2015 Complete
7. Touch base with HL7 to determine howthey are doing the full UDI in string
Laurie Burckhardt 06/01/2015
8. Take to X12 management to determinefeasibility and timing requirement forgetting into next HIPAA transaction
Laurie Burckhardt 06/01/2015
Key Discussion Item – Attendance = 36Discussion
Reviewed 6/15/2015 meeting minuteso Gloria made a motion to accept meeting minutes; seconded by Margaret Weiker; 34 approved, 0 disapproved, 2
abstentions (Joe Drozda and Nancy Sanchez Caro).
Scheduled MeetingsType of Meeting Date Location/Call in Contact AgendaCurrent Meeting 06/22/2015 712-432-0393
Access Code:218856#
LaurieBurckhardt orGloria Davis
CR1308 BRTS
Next StandingMeeting
Sept 27 – Oct 1,2015
Charlotte, NC Co-Chairs Voting ItemsBRTS
Interim Meeting Mondays, 1:00 pmto 2:30 pm EST
712-432-0393Access Code:219956#
LaurieBurckhardt orGloria Davis
CR 1308 BRTS

ASC X12N UDISAC MayJune 2015
Revised 3/2011 Page 11 of 15
Key Discussion Item – Attendance = 36Discussion
Reviewed outstanding Action items:o Item 7: Laurie will follow-up;o Item 8: Will be brought to X12N Management meeting on Thursday, 6/25/2015;
Nancy Spector requested to review bullet 3 and Section 2, Requirements B1, to reflect high-risk implantabledevices;o Section 1.2 Additional Information Bullet 3 changed to read “This CR is only intended to support the
transmission of UDIs of high-risk implantable devices from hospitals to health plans where trading partners havemutually agreed to exchange UDI.”
o Business Requirement B1 changed wording to read “Provide the ability to report a unique device identifier forimplanted devices which reflects the initial implant procedure.”;
Reviewed BRTS Section 1.2 Additional Information and discussiono Reviewed and changed first paragraph to: As there is no current standard method to communicate UDI within
an X12N transaction, following are some of the business reasons why willing trading partners would want toexchange UDI between providers and health plans:
o Changed wording on bullet #2 - This CR is intended to allow interested trading partners (primarily hospitals andpayers, since no standard mechanism exists today) to exchange UDI as part of administrative transactionsbetween willing trading partners.
o Action Item: Laurie to reach out to TGC on potential necessity to define willing trading partner;
Gloria and Laurie reviewed the BRTS (final) with all changes accepted and realized that we did not review Section1.4.2 Expected Criteria/Outcome previously on any UDI SAC calls;o Stanley asked if all Use Cases need a corresponding Criteria/Outcome;
Laurie stated/Gloria confirmed that it is not necessary to have a corresponding Criteria/Outcome to eachUse Case;
o Reviewed each Criteria/Outcome and determined that all are addressed either in the Section 1.4 Future, 1.4.1Use Cases or in Section 2 Business requirements;
SAC agreed to remove the items in Expected Criteria/Outcome;o Brian Reitz asked in 1.4.2.1 for change in sentence one to change “will” to “may”
Discussion followed on reviewing Section 1.4 Future and 1.4.1 Use Cases and wording used to be consistent
Action Item: Laurie to review both sections and make sure that the wording of ’may’, ‘could’ ‘would’‘should’ be consistent throughout the BRTS and post new BRTS for WG to review
Reviewed 1.4 Future;o Heading paragraph changed to include Providers and health plans;o Bullet 1 and 2 are combined and new #3 to address Cost calculations and all following renumbered;
Discussed Brian Reitz’s question regarding voting and next steps;o Vote will occur in X12N UDI SAC and if SAC approves then BRTS is moved to Change Request CD Workspace;o TGB/WG2 and WG10 (as active changers) will vote on the business requirements in their CD workspace;o The WG2 and WG10 reports the vote and any comments for changes on the BRTS in Change Requests CD;o The requested changes, if any, will be brought back to UDI SAC to review the requested changes;o If any dispute with the B WGs and UDI SAC then X12N management will handle;o Once all changes are made and approved by UDI SAC by vote then the BRTS goes to TGC/WG3 to create the
technical solution;o TGC/WG3 assigns a Technical Change Request Delegate (TCRD) who creates the technical solution;o Technical Solution voted and approved in TGC/WG3;o Technical Solution is brought back to UDI SAC to vote to approve technical solution;o Once approved by UDI SAC, TGB/WG2 and WG10 (as active changers) will vote on the technical solutions;o WG2 and WG10 reports the vote and any comments for changes on the BRTS in Change Requests CD;

ASC X12N UDISAC MayJune 2015
Revised 3/2011 Page 12 of 15
Key Discussion Item – Attendance = 36Discussion
o The requested changes, if any, will be brought back to UDI SAC to review the requested changes;o If any dispute with the TGB WGs and UDI SAC then X12N management will handle;o Once all changes are made and approved by UDI SAC, then the requested changes are brought back to
TGC/WG3 TCRD to determine changes;o The BRTS will be considered final; future version will be determined by X12N;
Gloria reviewed next steps;o Final BRTS will be posted for review prior to the next meeting.o After the review, the document will be put up for vote on CD.
Next meeting is Monday, June 29th;o Review BRTS comments posted by SAC members.
Decisions
None
Action Items:No. Description Owner Assigned Due Date1. Research all payer database topic and
present information to UDI SAC.Laurie Burckhardt 04/20/2015 Complete
2. Contact Supply Chain (X12M)representative to confirm crosswalkactivities.
Laurie Burckhardt 04/20/2015 Complete
3. Locate examples of when packagesfrom 2 different vendors are combinedand used for a patient.
Claudia BirkenshawGarabelli
04/27/2015 Complete
4. Rework Additional Information Sectionfor Risk and Challenges document tomove
Heather McComas 06/01/2015 Complete
5. Accept changes in Risks and Challengesdocument and upload new version toCD
Gloria Davis 06/08/2015 Complete
6. Rework B7 and B8 Laurie Burckhardtand Gloria Davis
06/01/2015 Complete
7. Touch base with HL7 to determine howthey are doing the full UDI in string
Laurie Burckhardt 06/01/2015 06/29/2015
8. Take to X12 management to determinefeasibility and timing requirement forgetting into next HIPAA transaction
Laurie Burckhardt 06/01/2015 06/29/2015
9. Reach out to TGC on potentialnecessity to define willing tradingpartner.
Laurie Burckhardt 06/22/2015
10. Review Section 1.4 Future and 1.4.1Use Cases to make sure the wording of’may’, ‘could’ ‘would’ ‘should’ isconsistent throughout the BRTS.
Laurie Burckhardt 06/22/2015
11. Post revised BRTS to CD so WGparticipants can review and comment.
Laurie Burckhardt &all UDI SACparticipants
06/22/2015
ASC X12N UDISAC MayJune 2015
Revised 3/2011 Page 13 of 15
Key Discussion Item – Attendance = 40Discussion
Reviewed 6/29/2015 meeting minuteso Gloria made a motion to accept meeting minutes; seconded by Nancy Caro; minutes unanimously approved.
Reviewed outstanding Action items:o Action item 7: Laurie indicates she will have further information in the next couple of weeks; revised due date to
7/13/2015.
Discussion occurred regarding the ability of the work group to move ahead on voting without having thisinformation;
Laurie B. noted that this it more of a technical requirement discussion, it will not impact the businessrequirements; HL7 and ASC X12 are both going to be reporting the full string of data (staying in sync).
o Action items 8 through 11 have all been completed and applicable information has been posted to CD.
Reviewed BRTS Section 1.4 Future;o Laurie B. reviewed the business reasons with participants;o Discussed the use of ‘total cost’ in the business reasons;
Joe D. noted this being viewed as the bill charges being communicated not necessarily the cost of the UDI;
Laurie suggested that in the future we may need to create a TR2 (Technical type report 2, not an officialdocument, it provides some guidelines for the industry) or possibly working with WEDI to provideclarification to the industry;
o Nancy S. noted for reason #5 the word “ensure” indicates guarantee, better stated as “support” (also applicablefor section 4.1.4.5 of the BRTS); participants agreed to replace “ensure” with “support;
o Fred R. noted for reason #4, questioned the use of the term “price” and participants further discussed;participants agreed to change “price” to “unit amount”;
o George A. felt the use of “enforce” in business reason #6 was incorrect; participants discussed and agreed tochange “enforce” to “administer”;
Reviewed BRTS Section 1.4.1 Use Caseso Laurie noted she did make revisions for consistency;o 1.4.1.1:
Nancy S. requested change to the last sentence to reflect “based on usage” and Gloria D. noted it shouldstate contracts with providers not provider networks; revised to read “The health plan can use theinformation in their payment modeling to predict expenditures for next year or modify contracts withproviders that are based on usage.”
o 1.4.1.2: participants had no comments/feedback;o 1.4.1.3:
Participants discussed identification of duplicate services;
Scheduled MeetingsType of Meeting Date Location/Call in Contact AgendaCurrent Meeting 06/29/2015 712-432-0393
Access Code:218856#
LaurieBurckhardt orGloria Davis
CR1308 BRTS
Next StandingMeeting
Sept 27 – Oct 1,2015
Charlotte, NC Co-Chairs Voting ItemsBRTS
Interim Meeting Mondays, 1:00 pmto 2:30 pm EST
712-432-0393Access Code:219956#
LaurieBurckhardt orGloria Davis
CR 1308 BRTS

ASC X12N UDISAC MayJune 2015
Revised 3/2011 Page 14 of 15
Key Discussion Item – Attendance = 40Discussion
Noted the last sentence needs the word “that”; last sentence revised to read “When UDI is sent to thehealth plan it can be used to reflect accurate billing and that there was no duplicate billing involved.”
Participants agreed this is applicable to provider and not hospital; revised to read, ”Provider has performedtwo cardiac stenting procedures for the same patient on the same date. When UDI is sent to the health planit can be used to reflect accurate billing and that there was not duplicable billing involved.”
o 1.4.1.4: participants had no comments/feedback;o 1.4.1.5:
Discussed that it is not always the health plan coming up with the follow-up care; revised to read, “Supportmember is following the appropriate follow up care once a device has been implanted. When the UDI is sentto the health plan, the health plan can use this as a basis to help support follow up care, such as thatordered and prescribed by the provider, in hopes to maximize outcomes as well as help answer anyquestions member may have.”
o 1.4.1.6: participants had no comments/feedback;o 1.4.1.7:
Added plan after health in the second sentence;o 1.4.1.8: participants had no comments/feedback;o 1.4.1.9: participants had no comments/feedback;o 1.4.1.10: participants had no comments/feedback;o 1.4.1.11: participants had no comments/feedback;o 1.4.1.12:
Removed “and hospitals” from the second sentence;o 1.4.1.13:
Discussed the use of “purchase” and if this is the health plan or provider purchasing;
Revised to read, “A health plan is interested in negotiating rebates from manufacturers based on thevolume of implanted devices utilized. When UDI is exchanged between the provider and health plan, thehealth plan can use the UDI (at a minimum DI) to report volumes back to the manufacturers.”
Laurie B. noted that participants had previously agreed to remove Section 1.4.2 as it is already covered in Section1.4.1;
Reviewed Section 2 Requirementso B1: participants had no comments/feedback;o B2: participants had no comments/feedback;o B3:
Stanley N. believes this is in contradiction with one of the HIPAA regulatory requirements and questioned ifwe can move forward with this noted as a requirement;
Noted provider reps requested the first statement and the second statement was developed to supporthealth plans;
Laurie B. noted this requirement is one participants have indicated we must have to move forward;
It was noted we also do not know if the solution will be applied to one of the HIPAA mandated transactions(could be a new transaction or one not mandated by HIPAA);
Discussed removing “The receiver is under no obligation to store, validate, or forward the UDI information.”o Noted this was developed as an addendum to B2;o Suggested changing it to read “Under X12N expectations, the receiver should be under no obligation to
store, validate, or forward the UDI information.”
Stanley N. also noted direct conflict with B2 as well; Laurie clarified that if B2 fails then B3 is applied;
Participants agreed B3 should be part of B2, revised to be B2.1
Question raised regarding the handling of non-implantable devices; due to time constraints Laurie noted we

ASC X12N UDISAC MayJune 2015
Revised 3/2011 Page 15 of 15
Key Discussion Item – Attendance = 40Discussion
will further discuss at next week’s meeting;
Laurie requested participants approval for her to accept BRTS revisions discussed during today’s meeting(up through Section 2 B.1). Motion to accept BRTS revisions up through Section 2 B.1 made by Joe Drozdaand seconded by Nancy Sanchez-Caro; motion unanimously approved.
Next meeting is Monday, July 6th;o Continue discussion of B2.1 and review remainder of the BRTS.
Decisions
Approval to accept revisions made to the BRTS up through Section 2 Requirement B.1.
Action Items:No. Description Owner Assigned Due Date1. Research all payer database topic and
present information to UDI SAC.Laurie Burckhardt 04/20/2015 Complete
2. Contact Supply Chain (X12M)representative to confirm crosswalkactivities.
Laurie Burckhardt 04/20/2015 Complete
3. Locate examples of when packagesfrom 2 different vendors are combinedand used for a patient.
Claudia BirkenshawGarabelli
04/27/2015 Complete
4. Rework Additional Information Sectionfor Risk and Challenges document tomove
Heather McComas 06/01/2015 Complete
5. Accept changes in Risks and Challengesdocument and upload new version toCD
Gloria Davis 06/08/2015 Complete
6. Rework B7 and B8 Laurie Burckhardtand Gloria Davis
06/01/2015 Complete
7. Touch base with HL7 to determine howthey are doing the full UDI in string
Laurie Burckhardt 06/01/2015 07/13/2015
8. Take to X12 management to determinefeasibility and timing requirement forgetting into next HIPAA transaction
Laurie Burckhardt 06/01/2015 Complete
9. Reach out to TGC on potentialnecessity to define willing tradingpartner.
Laurie Burckhardt 06/22/2015 Complete
10. Review Section 1.4 Future and 1.4.1Use Cases to make sure the wording of’may’, ‘could’ ‘would’ ‘should’ isconsistent throughout the BRTS.
Laurie Burckhardt 06/22/2015 Complete – lastMonday
11. Post revised BRTS to CD so WGparticipants can review and comment.
Laurie Burckhardt &all UDI SACparticipants
06/22/2015 Complete

TGB WG2 - UDI Topic
First Name Last Name COMPANY
Monday,
Feb 23,
2015
Monday,
May 4,
2015
Monday,
May 11,
2015
Monday,
June 8,
2015
Monday,
June 15,
2015
Monday,
June 22,
2015
Monday,
June 29,
2015
Amber Butterfield TRICARE
Anita Stover DSO
Angie Barlett CMS
Angela Franklin Pew Trusts
Anne Johnston Express Scripts
Anqi Lu Pew Trusts X X X X X X
Barry Simmons Wake Forest Baptist Medical Center
Behnaz Minaei FDA X X X X X X X
Ben Moscovitch The Pew Charitable Trusts X X X X X X X
Bertha Ambriz-Crespin Kaiser Permanente
Beth Ortega HPES
Betsy Clore Wake Forest University Health Sciences
Betty Gomez Zerox X
Bob Poiesz AMA Associatio
Brent Hall Blue Cross Blue Shield Associations
Bret Yarczower Geisinger Health System X
Brian Reitz CMS X X X X X X
Bruce Bellefuille Aetna Inc. X
Carol Germain Med Impact
Carol Benthorne Valence Health
Catherine Brock Blue Cross Blue Shield of MinnesotaX
Cheryl Walraven Aetna
Chris Cioffi Wellpoint, Inc. X
Christi Gist HCA Healthcare
Christol Green Wellpoint, Inc. X X X
Christopher J Gracon Independent Health X X X X X
Cindy Monarch BCBS Michigan X X X X X
Claudette Sikora CMS
Printed on: 07/17/2015 Page 1 of 6

TGB WG2 - UDI Topic
First Name Last Name COMPANY
Monday,
Feb 23,
2015
Monday,
May 4,
2015
Monday,
May 11,
2015
Monday,
June 8,
2015
Monday,
June 15,
2015
Monday,
June 22,
2015
Monday,
June 29,
2015
Claudia Birkenshaw Garabelli HFMA X X X X X X
Craig Streit Brookings Institution
Crystal Ewing Zirmed
Curtis Dudley Sisters of Mercy Heatlh System
Danny Sawyer DoD Tricare
David Spring IL Medicaid
David Wilderman DHA X X X X X X
Debbie Taylor Humana
Diane Franks Health Net
Duane Collins BCBSAL
Ellen Hanneman Accenture
Elizabeth Templeton DSO
Fred Rooke CMS X X X X X X
Gale Scott Tampa General Hospital X X
Gail Kocher BCBSA
George Arges American Hospital Association X X X X X X
Gigi Medenhall HPES
Gladys Jones Group Health Cooperative X X X X X
Gladys Wheeler CMS X X X X X
Gloria DavisQSI/NextGen Healthcare Information
System X X X X X X X
Heather McComas American Medical Association X X X X X X
Ira Klein Aetna X
JP Kelley DHA
Jamie Mosteller Cerner X X
Jane Depeaux Horizon Blue Cross Blue Shield of NJX X X X X X
Jaine Weingarth Anthem
Jay Eisenstock Aetna X X
Jean Narcisi ADA
Jeff Jennings California Medicaid X X X X X X
Printed on: 07/17/2015 Page 2 of 6

TGB WG2 - UDI Topic
First Name Last Name COMPANY
Monday,
Feb 23,
2015
Monday,
May 4,
2015
Monday,
May 11,
2015
Monday,
June 8,
2015
Monday,
June 15,
2015
Monday,
June 22,
2015
Monday,
June 29,
2015
Jill Money Blue Cross Blue Shield of Mi X X X
Jim Daly BCBS SC
Jim Whicker Kaiser Permanente X X X X
Jimmy Terrapin BCBSSC
Jodie Banks Relay Health X X X X X X X
Jonathan Brian
Joe Stanton Delta Dental
John Roberts GS1 US
John Voorhees Applied Policy
Joseph Drozda Sisters of Mercy Heatlh System X X X X
Josh Rising Pew Trusts X X
Jove Graham Geisinger Health System X X
Julie Suko FDB Health
Karen Encinosa Tampa General Hospital X X X X X X
Karen Shutt Highmark, Inc. X X X X X X X
Karen Zannone Tampa General Hospital X X
Kathy Reep Florida Hospital Association X X X X
Karen Zannone Tampa General Hospital X
Katie Sullivan Cognosante, LLC X
Keith Simmons Wake Forest University X X
Kelly Butler Emdeon, LLC
Ken Edick SIEMENS
Kevin Capatch Geisinger Health System X X X X X
Kevin Haynes University of Pennsylvannia
Kimberley Ryan CVS Caremark
Latrecia Moran Medtronic X
Laura Caldwell CSC X
Lauren Choi Premier Inc.
Laurie Burckhardt WPS Insurance Corp. X X X X X X
Laurie Darst Mayo Foundation X X X
Laurie Holtsford Community Health Systems X
Printed on: 07/17/2015 Page 3 of 6

TGB WG2 - UDI Topic
First Name Last Name COMPANY
Monday,
Feb 23,
2015
Monday,
May 4,
2015
Monday,
May 11,
2015
Monday,
June 8,
2015
Monday,
June 15,
2015
Monday,
June 22,
2015
Monday,
June 29,
2015
Laurie Woodrove Labcorp
Linda Brent BCBSSC
Lisa Savicki Humana
Lynn Chapple UnitedHealth Group X X X X
Marc Leib ASA X X X X X
Margaret Weiker Weiker Group X X X X
Martha Bridwell Humana
Martin Willbanks VA
Mary Lynam Argus Health X X X X X
Mary Tyra VA
Mary Helm HP
Mary Kay McDaniel Cognosante, LLC
Mary Lynn Bushman Wellpoint, Inc.
Matthew Klischer CMS/HHS X X
Melissa Andel Applied Policy X
Merri-Lee Stine Aetna Inc. X X X
Michael Nichols PGBA X X X X
Michele Lanzetta Aetna Inc. X X X
Michelle Hunter CMS
Morasa Shaker ADA
Nancy Sanchez-Caro IM X X X X X X
Nancy Spector American Medical Association X X X X X X
Naomi Herz Pew Trusts
Pam Davis Ability
Parvan Dyn Meda Health
Patrick Cannady ADA X X X X X
Patrick Lupinetti First Databank
Paul Brown National Provider Service Center
Phil Lerner Aetna X
Pranav Shah VA
Rachel Foerster Rachel Foerster & Associates X X X X
Printed on: 07/17/2015 Page 4 of 6

TGB WG2 - UDI Topic
First Name Last Name COMPANY
Monday,
Feb 23,
2015
Monday,
May 4,
2015
Monday,
May 11,
2015
Monday,
June 8,
2015
Monday,
June 15,
2015
Monday,
June 22,
2015
Monday,
June 29,
2015
Ramzy ElGomayel Aetna X X
Richard Platt Harvard
Robert Dieterle Enablecare
Robert Wacloff HSAA
Rose Hodges Aetna Inc. X X X X X
Sam Rubenstein Montfiore
Shannon Hughes State of Illinois X X
Sharon Gruttadauria CVS X X
Sheri Kosko CMS X
Stacey Barber HP
Stanley Nachimson Nachimson Advisors, LLC X X X X X X X
Stephanie Boyland Deloitte X X X X
Steven Rosenberg GS1 X X X X
Steven Carter Accenture
Stewart Presser GNYHA X X X X X X X
Stuart Kilpinen Aetna Inc. X
Sue Thompson NCPDP X X X
Sumita Sen CMS/HHS
Susan Ulmen Cerner
Suzie Burke-Bebee HHS
Tammara Jean PaulCDC/National Center for Health
Statistics X X X X
Tanya Fryltsove Edifecs
Teresa Strickland NCPDP
Terrence Cunningham AMA X X X X X
Terrie Reed Duke Clinical Research Institute X X X X X
Timithy Morgan UnitedHealth Group
Tina Greene Mitchell
Todd Omundson American Hospital Association X X X X X X X
Tony Benson Blue Cross Blue Shield of Alabama X X X X X X
Tony Laurie Noridian Healthcare Services
Printed on: 07/17/2015 Page 5 of 6

TGB WG2 - UDI Topic
First Name Last Name COMPANY
Monday,
Feb 23,
2015
Monday,
May 4,
2015
Monday,
May 11,
2015
Monday,
June 8,
2015
Monday,
June 15,
2015
Monday,
June 22,
2015
Monday,
June 29,
2015
Wendy Slater Humana
Zachary Caudill Humana
Total Attendance: 39 34 44 61 36 36 40
Printed on: 07/17/2015 Page 6 of 6