Embed Size (px)
Citation preview

......... I 'M...... . . . -
HERMAPHRODITISMA Critical Survey
By HUGH JOLLY, M.D., M.R.C.P., D.C.H.Consultant Paediatrician, Plymouth Clinical Area
Wo-ff ,/i,./,Pcradft$dectt
Wrolff LO,^ uct
Lsb(oastrhhp ~v
-.I ,~o5:
Iws l
U-e^latiit
FIG. I.-The undifferentiated stage of urogenital development.
The problem of hermaphroditism is one whichhas always attracted attention so that much hasbeen written on the subject. One of the finestworks appeared in 1937, with the publication ofYoung's monograph1 and this has become a classic.In recent years, Lawson Wilkins and his co-workers at Johns Hopkins have, more than anyoneelse, furthered our knowledge of the subject andmuch of the information in the present article isderived from their writings2-15 and from personalcommunication with Dr. Wilkins. Liberal usealso is made of the present author's publica-tions16-18 on the subject as well as more recentpersonal experience.EmbryologyThe occurrence of hermaprhoditism is due to
the complicated method by which the male andfemale genital tracts and external genitalia arederived, and particularly to the fact that thisdevelopment is common to both in early embryoniclife (Fig. I).The GonadsUp to the sixth week, therefore, the gonads are
identical in both sexes and the embryo potentiallybisexual. Changes in the gonad take placeearliest if the embryo is to become male when, atthe seventh week, the elements of the testes appear,being derived from the medulla of the gland.If the foetus is to become female no distinctivefeatures appear until the tenth week when thegerminal epithelium, consisting of epithelialnests and primordial follicles containing ova, is
Protected by copyright.
on March 16, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.32.374.589 on 1 D
ecember 1956. D
ownloaded from

590 POSTGRADUATE MEDICAL JOURNAL December 1956
':~ ~:::"':'"FgE~'.·~,~ggpp,~i?-~'-..?'ii,? .~'~ '·'· ii.~.'·. C' ~
'.... ...........
·:iSpL EE,& ·
PA kP~:-
:.F:~'"'....~.*ii:: i
1111~l i iN~ eriF.¢ei-· ·;;·2||W
'?''!.,,.'.:.'jS:.' i:...p
.:::'.
s
Charli :B
1.·-'..::? ..:.ii!~
.....:.. .::..:i::-:;~'-.iij.. i.~::::..,:::
.....
"I. KIDNEY
?,?!::AL LO0Pf~A N T t
RC!:
ILI
:: :::::::::::::::::: :::.. ....
'~:~'::-
Ard
~~....i
::::::::::::::::::::::::::: ...~'
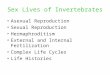
PLATE I.-P.M. specimen showing congenital adrenal hyperplasia. The hyperplasticadrenal glands are seen to be larger than the kidneys. The infantile uterustubes and ovaries are well shown.
derived from the cortex of the gland. It isapparent therefore, that the testis develops fromthe medulla and the ovary from the cortex of thegonad, but even this adult differentiation is notcomplete since the normal testis contains' female '(cortical) components and the ovary contains' male' (medullary) components. In this light itis understandable that on very rare occasions thefoetal gonad may develop into an ovo-testis, being
part ovary and part testis or that one gonadbecomes an ovary and the other a testis.
The Genital DuctsIn the undifferentiated stage (Fig. I) two pairs
of genital ducts lead from the gonad to theurogenital sinus-the male or Wolffian ducts andthe female or Mullerian ducts. These ductsare not ambisexual and remnants of the pair
Protected by copyright.
on March 16, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.32.374.589 on 1 D
ecember 1956. D
ownloaded from

December 1956 JOLLY: Hermaphroditism 591
belonging to the opposite sex are to be found inadult life. The Wolffian ducts become theepididymis, vas deferens and seminal vesicles inthe male, whereas, in the female, their remnantsexist as the epo6pheron, paro6pheron and Gartner'sducts. The Mullerian ducts become the Fallopiantubes, uterus and vagina, the latter two structuresbeing formed by fusion of the two ducts. Theirremnants in the male are the appendix testis,utricle and verumontanum.The Urogenital Sinus
In the undifferentiated stage the bladder andboth sets of genital ducts open into the urogenitalsinus. In the male the urogenital sinus becomesthe lower part of the prostatic urethra and penileurethra. In the female this sinus becomes theshallow vestibule which contains the orifices ofthe urethra and vagina. This is separated fromthe vagina by the hymen whose inner surface islined by vaginal epithelium derived from theMullerian duct and outer surface from urogenitalsinus epithelium.External GenitaliaThe genital tubercle enlarges in both sexes to
form the phallus and as it does so a median grooveappears on its caudal surface. The raised marginsof this groove are the urethral folds. In the malethe phallus lengthens to become the penis and as itdoes so the urethral folds fuse round the urogenitalsinus from behind forwards in such a way as tocarry the penile urethra, which has formed fromthe urogenital sinus, to the tip of the penis. Thetwo labioscrotal folds which have appeared oneach side of the base of the phallus become fusedin the male to form the scrotum.
In the female the phallus becomes the clitoris,while the genital and labioscrotal folds do not fusebut become the labia minora and majorarespectively.ClassificationTwo distinct groups of hermaphrodites should
first be separated on the basis of aetiology, the onebeing due to an adrenal disorder and the other not.Thus we have:
(I) Female pseudohermaphroditism due tocongenital adrenal hyperplasia.
(II) Intersex.In this latter group there is no endocrine dys-
function and the aetiology is unknown, althoughgenetic factors play a part. It includes the remain-ing varieties of pseudohermaphroditism and alltrue hermaphrodites.
In female pseudohermaphroditism with adrenalhyperplasia there is progressive virilization frombirth, whereas in intersexes no further changestake place until puberty which occurs at the usual
age. The problems of homosexuality and trans-vestism will not be discussed in this paper sincethey are psychological problems only.
(I) Female Pseudohermaphroditism with AdrenalHyperplasia
This is the commonest of all types of her-maphrodites and Money quoted by Wilkins et al.(I955)11 in a recent survey of published casesbetweren I895 and I95o has shown that thecondition occurs as frequently as all the types ofintersex.The hyperplasia of the adrenal cortex (Plate I)
commences in early foetal life and produces amassive masculinizing stimulus from the out-pouring of androgens. This action begins in thefourth month by which time the gonads havealready differentiated to form ovaries but theMullerian ducts have only developed as far as theformation of Fallopian tubes and uterus. Thefurther development of the genital ducts now takesplace along male lines as a result of the androgenicstimulus, so that the urogenital sinus persists asin Fig. 2, type A, instead of giving way to a separateurethra and vagina. This figure shows thecommonest anatomical arrangement in thesepatients, there being one external orifice only sothat the vagina appears to open into the floor of theurethra. The phallus steadily enlarges instead ofremaining small as a normal clitoris and the labio-scrotal folds fuse to some extent and thereby givethe impression of a scrotum rather than labiamajora. The ovaries however do not descend sothat the ' scrotum' is always empty.
Other varieties of this condition may occur,the next most common being shown as type B inFig. 2. Here the urogenital sinus opens externallythrough a funnel-like orifice which is larger thanthe previous type so that the urethra appears toopen into the roof of the vagina. Three othermuch rarer types have occurred. In type C, thereis no communication between vagina and urethra;in type D the urethra has been carried forwardby fusion of the urethral folds so that its orificeis at the tip of the clitoris. In type E the vaginaand urethra have differentiated to become separateas in the normal female, and one can only presumethat in this case the androgenic stimulus did notcommence until after the fifth month of foetal life.At birth then, the child, who is of average
rather than large size, will be normal apart from alarge clitoris, and in most cases will have a singleexternal orifice serving both urethra and vagina.A varying degree of fusion of the labioscrotalfolds will be present and the uterus can usuallybe felt on rectal examination. After birth theandrogenic stimulus continues so that the childgrows more rapidly than normal and the epiphysial
Protected by copyright.
on March 16, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.32.374.589 on 1 D
ecember 1956. D
ownloaded from

592 POSTGRADUATE MEDICAL JOURNAL December 1956
A-S
C' £FIG. 2.-Varieties of female pseudohermaphroditism with adrenal hyperplasia.
:·
....:... :.. .... .;.... ;.... ..
..........
i~ili~iiiiii.. .. ... ........ ....·: ··:::i '' ·I
................... ..... ii..:i ::::
...............
::,.i;:.... ...:I:
.......
.. ....
..k
PLATE 2.--Female pseudohermaphrodite with adrenal hyperplasia. These photographs were taken when the childwas first seen at the age of five years and before cortisone therapy was commenced. The thickened and enlargedphallus can be appreciated, together with the growth of pubic hair and the single external orifice.
Protected by copyright.
on March 16, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.32.374.589 on 1 D
ecember 1956. D
ownloaded from

December I956 JOLLY: Hermaphroditism 593
bone age is advanced. The phallus continues toincrease in size, being much thicker than a normalclitoris, but not so long as a penis. It is bounddownwards in a curve-a condition known aschordee. Grossl9 states that the enlarged clitoriscan be differentiated from the penis by the twosmall folds which run down on either side of itsmidline to join the labia minora. In the penisthere is a single frenulum on the ventral surface.Erections of the enlarged phallus become increas-ingly frequent and may be painful. The voicedeepens as a result of the same changes in the vocalcords that occur in the normal male at puberty.Pubic hair appears between the age of two to fiveyears and is followed by axillary and facial hairwith acne of the face a common accompaniment.Muscular development becomes marked althoughthe bodily contours remain predominantly femi-nine (see Plate 2 and Jollyl8 photos of cases 56 to6o). A few patients have hypertension.No breast development or menstruation occurs
at the time of an expected puberty but by this ageepiphysial fusion has occurred to such an extentthat further growth is impossible. Therefore,after an initial spurt of growth in early childhood,putting the child head and shoulders above those ofher own age, she ends up much shorter than theaverage.
Diagnosis. This must be made as soon aspossible after birth since early treatment isessential. However, at this early age the conditioncan easily be confused with some varieties ofintersex which may have the same anatomicalconfiguration. Further evidence is thereforerequired in order to prove the presence of adrenalhyperplasia and thereby confirm the diagnosis.This proof is given by the rise in urinary excretionof I7 ketosteroids from the normal of less than0.5 mg. in 24 hours at birth to a level of 2 to 5 mg.within the first few weeks of life. The levelcontinues to rise as the child grows and byadolescence may reach levels of 25 to 8o mg.In the early weeks of life the I7 ketosteroids maygive ambiguous results but in these cases thefinding of an increased excretion of pregnanetriolin the urine is diagnostic of congenital adrenalhyperplamia (Bongiovanni and Clayton20).Laparotomy has frequently been used in the
past for confirmation of the diagnosis but is un-necessary and dangerous, since adrenal failure maybe precipitated by the operation. Perirenal in-sufflation to outline the enlarged adrenals has beenrecommended by some writers, but this also is adangerous practice, and in any case the rise in 17ketosteroids is a much better guide to the state ofthe glands.
Urethroscopy is the only further investigationwhich should be performed if further confirmation
of the diagnosis is required. The urethrQscope ispassed into the capacious urogenital sinus untilthe vaginal opening is visible in the floor of thesinus as a slit-like aperture surrounded by folds.This opening is usually large enough toallow thepassage of the urethroscope into the vagina untilthe cervix can be seen as a smaller slit and intowhich an ureteric catheter can usually be inserted.If necessary, a radio-opaque dye can be injectedand watched under the X-ray screen as it passesalong the Fallopian tube and out into the peritonealcavity through the fimbriated opening (Plate 3).
If the child is not seen until a few years afterbirth the diagnosis is very much easier on accountof the progressive virilization which will have takenplace. This is shown by an acceleration of growthand epiphysial development as well as by thepresence of sexual hair, the muscular developmentand the deepened voice.The condition of' premature pubarche ' (Silver-
man et al.5) may cause some confusion with thesepatients and should be mentioned. It is a con-stitutional variation of adolescence whereby chil-
YI(:·"
MiitL' "::.'I:
··::·
······::;:
PLATE 3.-Female pseudohermaphrodite. Anterior sal-pingogram. The urethroscope lies in the vaginawith its tip at the cervix, while the ureteric cathetercan be seen in the left Fallopian tube. Dye hasfilled the uterus and passed up both Fallopian tubes,finally spilling over into the peritoneal cavity, whereit forms shadows which are less well defined.(Reproduced with permission from the Proceedingsof the Royal Society of Medicine.)
Protected by copyright.
on March 16, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.32.374.589 on 1 D
ecember 1956. D
ownloaded from

594 POSTGRADUATE MEDICAL JOURNAL December 1956
dren of both sexes, though more particularly girls,develop a premature growth of pubic hair. Noother signs of precocity are present, except thatskeletal maturation, and I7 ketosteroid excretionmay be slightly increased, and a normal pubertywill occur at the usual age. Silverman et al.suggest that the condition is due either to an unduesensitivity of the hair follicles to androgen secretionor to an early elaboration of adrenal androgensbefore the gonadotropic mechanism of the pituitaryhas been activated.An adrenal tumour may also lead to diagnostic
difficulties from its virilizing effect, but the con-dition occurs after birth and the anatomical de-velopment of the genitalia will be normal. Thereis a similar rise in the 17 ketosteroids, but theadministration of cortisone produces no fall intheir excretion as compared with the dramatic fallin cases with adrenal hyperplasia.
Heredity. Carter2' states that some, and perhapsall instances of congenital adrenal hyperplasia areinherited as an autosomal recessive condition andGrumbachl4 has found that if one patient of thesaltl4osing type has occurred, all other affectedchildren born into that family will have the salt-losing complication as well. There are certainlymany reports (Jolly,l8 p. 74) which illustrate theimportance of genetic factors. If congenitaladrenal hyperplasia affects a male, the conditionof macrogenitosomia praecox results. Con-sequently, if two members of opposite sex in afamily are affected, the girl is a female pseudo-hermaphrodite and the boy has macrogenitosomiapraecox. These facts of heredity should be givento the parent of any child with congenital adrenalhyperplasia.
Prognosis. Cortisone therapy has entirely alteredthe future for these patients, but it is only fair tosay that the prognosis as to life before the days ofcortisone was not as bad as was often alleged. Thepresent author (Jolly,l8 p. 76) refers to instances ofelderly patients who have never received cortisoneand there must be many others unrecorded. Atthe same time, the risk of adrenal insufficiencyduring infancy is considerable and in Gross'recent survey'9 there were 27 female pseudo-hermaphrodites and one male with adrenal hyper-plasia, of whom ' 50 per cent.' showed this com-plication. This is an unusually high proportionand Wilkinsl3 refers to I5 cases of the salt-losingtype out of a total of 67. Adrenal insufficiency inthese patients has been explained on the groundsof the hyperplasia of the zona reticulata, which isthe principal feature of the enlarged adrenal glands.This hyperplasia takes place at the expense of thezona glomerulosa and zona fasciculata, which al'ebelieved to be responsible for electrolyte control.Recent experimental work with ACTH has shown
that the explanation is not as simple as this andWilkins3 (p. 54) has suggested that the conditionmay be due to the secretion of types of glyco-genetic hormones (such as I7 hydroxycorticoster-one) which increase the excretion of salt.
Treatment. All patients should be given cortisoneprovided the. condition is diagnosed during thefirst year or two. The exception to this rule is thechild who in error has already been brought up as aboy and may be better left unchanged in sex andtherefore untreated with cortisone. This problemis discussed more fully in the later section on thepsychological aspect of hermaphroditism. Underno circumstances should partial adrenalectomy, apopular operation in the past, be performed. Theoperation carries a considerable risk and its effectsare only temporary.The aim of cortisone therapy is to reduce the
level of I7 ketosteroids as rapidly as possible andthen, by trial and error, to find the smallest main-tenance dose to keep them at this low level. Inolder children it may not be possible to reduce thelevel below 4 to 6 mg., but in small infants itshould be possible to reach 0.5 mg. Cortisone maybe given intramuscularly or by mouth, but Wilkinsprefers the intramuscular route since its action ismore predictable, it lasts longer and smaller dosesare required than when given by mouth. More-over, it may be possible to maintain suppression of17 ketosteroid excretion by an injection of cortisonegiven every fourth day only. It is important thatonly the smallest amount of cortisone required formaximum suppression of ketosteroids is given,since an excess of cortisone suppresses growth.During periods of infection there may be a tem-porary release from cortisone suppression, sincethe adrenals are still capable of responding tostress, but no immediate change in cortisonedosage is required and this should only be made ifthe rise in the 17 ketosteroids persists.
Cortisone therapy should be started as early inlife as possible in order to prevent the secondarystructural changes in the body from taking place.Furthermore, if cortisone is not started until thebone age has reached io years or more, a rapidand premature adolescence takes place, breastdevelopment and menstruation occurring within afew weeks. In these cases it appears that thepituitary-gonadal mechanism has already reacheda stage which on release with cortisone precipitatesan immediate adolescence.
Cortisone started shortly after birth will allownormal growth and normal female development totake place. Wilkins et al.15 refer to two instanceswhere pregnancy has occurred. If sexual hair hasalready appeared, the further rapid skeletal growthcan be prevented. Similarly acne, and hyper-tension if present, disappear, as do the frequent
Protected by copyright.
on March 16, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.32.374.589 on 1 D
ecember 1956. D
ownloaded from

December 1956 JOLLY: Hermaphroditism 595
... .. ..s ..
.|
-..vIA........
.. .....
11-. .. .. ..
li~ll-;1
i.
i''iii':::'ii'~i'ill'lifl~"i~lp...........e~:i·:"':i'.i::iilfi~~dgpll~s18IBsrsE~%8glfa~f~DZ~le~Y-~ii~~l~?.........ii:iii:'"':'.i'(itlleaaresI~llaes~nsrap~lre.III-s...........~"::
dventst!.!:
t~8ftl~if~~rr·B~o~tf~l~t%,~.. .....t~!
:...
PLATE 4.-True hermaphrodite. This boy had well-developed breasts, as seen in the left-handphoto taken at the age of 5 years. The genitalia, photographed at 12 years, showed a penis witha hypospadic urethral meatus at its base. An ovotestis was found in the right side of the scrotumand a left ovary in the correct position. Uterus, vagina and Fallopian tubes were present.(This patient was under the care of Mr. Denis Browne and his case has been recorded byWilliams (1952), Brit. med. J., i, 1264.)
and sometimes painful erections of the clitoriswhich occur in many of the children. If the voicehas already become deep the cortisone cannot alterit, as permanent structural changes have takenplace in the vocal cords.
It is still too early for the assessment of thelong-term results of cortisone therapy, but presentfindings (Wilkins9) indicate that the suppressionof adrenal activity persists to some extent after thewithdrawal of the drug. This possibly indicatesthat the adrenal disorder may be permanentlyaltered so that no relapse will occur when cortisoneis withdrawn, comparable to the treatment ofhyperthyroidism with thiouracil.Some of the patients, particularly infants, may
show electrolyte disturbances from adrenal in-sufficiency and the patient may first present withthese symptoms. This adrenal lack manifestsitself as a failure to thrive, persistent severe vomit-ing, diarrhoea and attacks of acute circulatoryfailure. The child becomes dehydrated and thereis a fall in serum sodium and carbon dioxide levelswith a rise in potassium.
Wilkins recommends the following line of treat-
ment for the cases of congenital adrenal hyper-plasia of the salt-losing type:
i. When first seen the child should be givenlarge doses of sodium chloride (3 to 6 g. daily) inorder to correct the dehydration and salt lack.
2. When the immediate emergency is over corti-sone should be given and its dose adjusted whilecontinuing with the large doses of sodium chloride.
3. When the dose of cortisone has been adjusteddesoxycorticosterone (DOCA) should be given andthe dose of DOCA and salt worked out in order toobtain normal electrolyte levels.
4. The calculated dose of DOCA should begiven by implantation.The advantage of giving DOCA is that it reduces
the amount of salt required, so that the large dosesof salt can be kept for emergencies.With early treatment the removal of the enlarged
clitoris is seldom necessary and even in thosediagnosed later the organ should not be removedunless the large size is causing distress, in whichcase early amputation is desirable. Hampson22 hasshown that amputation of the clitoris in childhooddoes not prove detrimental to subsequent sexual
Protected by copyright.
on March 16, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.32.374.589 on 1 D
ecember 1956. D
ownloaded from

596 POSTGRADUATE MEDICAL JOURNAL December I956
responsiveness, as stated by some authors, and ifthe parents have been in doubt about the child'scorrect sex the removal of the enlarged clitoris willassist their adjustment. A vaginoplasty should becarried out in order to provide an adequate orificefor the vagina and Gross19 recommends that thisshould be undertaken when the child is in her'teens.
(II) IntersexThe varieties of this condition have been sum-
marized by Wilkins in the following table (repro-duced with permission from Pediatrics, i6, 288,1955), where findings are compared with those incases of female pseudohermaphroditism associatedwith adrenal hyperplasia.
I. True Hermaphrodites. In these rare patientsthe gonads differentiate so that both testicular andovarian tissue is present in the same individual.The commonest finding is that one or both gonadsare ovotestes, the other being an ovary or testis ifonly one ovotestis is present. Less commonly,one gonad is a testis and the other an ovary. Theovotestis may descend as a normal testis, but anovary seldom reaches the inguinal canal. Manydifferent arrangements of the external genitaliahave been reported (Plate 4).To make the diagnosis both gonads must be
biopsied and one cannot predict the type ofsecondary sexual development which will takealace at puberty. No case of true hermaphroditismpchieving parenthood in either sex has beenreported.
2. Male Pseudohermaphroditism. In these patientsthe gonads are morphologically testes and are sitedin the abdomen or in the labioscrotal folds. Ifthey are in the abdomen they lie either in the siteof the ovaries or in the inguinal canal. The tubulesare immature, being composed of undifferentiatedgerminal cells, but after puberty Sertoli cells maypredominate and numerous Leydig cells are oftenfound in large clumps.There are two principal types of male pseudo-
hermaphroditism, one in which the externalgenitalia are male or ambiguous, and the other inwhich they are female. Familial factors play apart so that more than one case may occur in thesame family (Plate 5).A. Male or Ambiguous External Genitalia. A
varying degree of phallic development and labio-scrotal fusion exists, while uterus and tubes maybe present and fully developed. In other cases theuterus is incompletely developed and one or bothtubes absent. Paradoxically, if the genital ductsare predominantly female, the child is likely todevelop male secondary characteristics at puberty,whereas those in which the ducts are predominantly
male may develop along either line. Femininedevelopment, when it occurs, is' due to the secre-tion ef oestro-ens by the testes.
B. Female External Genitalia. The externalgenitalia of these patients are entirely feminine ex-cept that in some the clitoris may be slightly en-larged. The urethra and vagina are usually separ-ate and the latter often ends blindly owing toabsence of the uterus. At puberty developmentis always along female lines with normal breastformation but no menstruation. Sexual hair insome is entirely absent.
3. Female Pseudohermaphrodites (without adrenalhyperplasia). This is the rarest type of intersexand Wilkins et al.1l state that only iz authenticatedcases have been recorded. The genital tract isidentical with that found in female pseudoherma-phrodites with adrenal hyperplasia but thepatients differ in showing no virilization. Normalsecondary sexual development occurs at pubertywith menstruation taking place through theurethral meatus. The ovaries mature and showevidence of ovulation with formation of corporalutea.
Diagnosis of Intersex. The first step in thediagnosis is to exclude female pseudoherma-phroditism due to adrenal hyperplasia. Thisis done on the basis of the progressive virilizationalready discussed.The next step is urethroscopy and dye studies
as already described, in order to determine thetype and extent of the internal genitalia. Thisshould be followed by laparotomy to examine theinternal genitalia and make biopsies of bothgonads. As an additional diagnostic aid thechromosomal sex should be determined by meansof Barr's technique of skin biopsy (Moore et al.23;Barr24) which is based on the smaller size of theY chromosome. Females have an XX chro-mosome combination and the mass of sexchromatin formed by the fusion is sufficientlylarge to be visible. It forms a planoconvex massjust under one micron in diameter and usuallylies against the inner surface of the nuclear mem-brane but is occasionally free in the nucleoplasmor adjacent to the nucleolus. Males have an XYcombination which is too small to be distinguishedfrom the general particulate chromatin.
Barr's results have so far shown that all malepseudohermaphrodites and female pseudoher-maphrodites with adrenal hyperplasia tested,have given correct results. True hermaphroditesand female pseudohermaphrodites without adrenalhyperplasia may have either male or female typenuclei. It will be apparent that those givingcorrect results involve by far the largest group ofthose with ambisexual development.
It had been hoped that this work would demon-
Protected by copyright.
on March 16, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.32.374.589 on 1 D
ecember 1956. D
ownloaded from

December i956 JOLLY: Hermaphroditism 597
-,~;: I·: i.ii .. ..... ...
......: .i
....i::·:: :; ::. ..: .,:iliii%·i~ii
1:.; imiii i!:i 3.........
liii~l~l'ii ·... ..... ....::
... .... ~. .···
liliiilir~iii~iiii~i............:i
E:::··:::::;·:;··:i·i.
.*
..........;:':il~ifii~iil~ii-.:i:i-"': ..·;
...... .::iii~ii;:.iii~i::
.:::: ii :'
..
PLATE 5.-Two male pseudohermaphrodite brothers, aged ten months and three years respectively.The gonads, which proved to be testes, were found in the site of the ovaries and surrounded bystructures resembling Fallopian tubes, including fimbriated ends. No uterus or vagina was seen.
strate the ' dominant' sex-in equivocal cases butthis has not proved to be so. For example, malepseudohermaphrodites with strongly femininecharacteristics both anatomically and psycho-logically still show a male chromatin pattern.It is for this reason that Barr, both in his earlierand later writings25, 26 has emphasized that thechromatin pattern should not unduly influenceclinicians in their decisions as to which sex a childshould be brought up. The test is a valuablediagnostic aid but the decision as to the sex ofupbringing must be decided on all the available
data and particularly the psychological factors.It is for this reason that Barr pleads for the use ofthe terms ' chromatin positive' or 'chromatinnegative' rather than female or male nuclei,pointing out that much unnecessary distress mightbe caused to a patient were he or she to learn thatthe cell nuclei were of a different sex from that inwhich he or she had been brought up.
Research is continuing to discover other sitesin the body from which material can be obtainedfor the sexing of nuclei and in particular to obviatethe need for a biopsy. Davidson and Smith27 have
Protected by copyright.
on March 16, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.32.374.589 on 1 D
ecember 1956. D
ownloaded from

598 POSTGRADUATE MEDICAL JOURNAL December I956
used the polymorph nuclei in blood films whileMoore and Barr28 have recently described amethod based on scrapings of oral mucosa whichthey state are easier to interpret than skin biopsies.
Differential Diagnosis. Two conditions-GonadalDysgenesis and Klinefelter's Syndrome--whichmay enter into the diagnostic problems of intersexremain to be mentioned.
Gonadal Dysgenesis. This condition was pre-viously called ' ovarian agenesis' but recent work(Polani et al.29; Wilkins et al.30) has shown that thenuclei are most often male. Grumbach et al.10have therefore suggested the title of ' GonadalDysgenesis.' (Dysgenesis rather than agenesissince varying amounts of rudimentary mesonephricelements are present in the genital ridge.) Thesepatients with gonadal dysgenesis and male typenuclei must be regarded as the most extreme formof male pseudohermaphrodite-in other words,genetic males who are completely feminized.The patients have a normal female appearance
but are stunted in growth. Secondary sexcharacters fail to develop at puberty except thatsexual hair develops. Laparotomy shows thepresence of an infantile uterus and tubes with a thinstrip of tissue in the site of the ovary. This tissuecontains no germ cells but is composed of cellsresembling ovarian stroma although this is not infact sex-specific. The diagnosis is confirmed bythe finding of a high level of follicle stimulatinghormone (FSH). Associated anomalies, parti-cularly webbed neck, cubitus valgus and coarcta-tion of the aorta may be present.
Klinefelter's Syndro.me. This condition, whichaffects males, was described by Klinefelter et al.31in I942. The patients have small testes, azospermiaand an increased urinary excretion of FSH.Secondary sexual characteristics may be fairly welldeveloped but the testes are of preadolescent sizeand the configuration of the body may be feminine.Gynaecomastia is a common accompaniment andit is particularly for this reason that diagnosticdifficulties may arise as in the true hermaphroditerecorded by Williams32.
The Psychological Aspect of HermaphroditesIn deciding the correct sex of upbringing the
psychological aspect is probably of more im-portance than all the other methods used for thedetermination of sex, namely, the gonadal, hor-monal and chromosomal sex as well as the typeof internal and external genitalia. This statementis based on my own experience (Jolly,18 page 8o),and is supported by the recent careful and veryimportant studies of Money, Hampson and Hamp-son.22, 33, 34 These workers have carried out ex-tensive studies on many hermaphrodites of differenttypes and emphasize the importance of the' gender
role.' This term is used to signify all thosethings that a person does or says to disclose him-self or herself as having the status of boy or man,girl or woman respectively. It includes, but is notrestricted to, sexuality in the erotic sense. Theirresearch has shown that the gender role andorientation as a male or female closely conforms tothe sex to which the patient has been assignedand reared and that it is largely independent ofgonadal, hormonal or chromosomal sex or the stateof the genitalia.As part of their work 22 patients, who had lived
with a contradictory genital appearance for periodsof five to 47 years, were studied. In all but onecase these patients had come to terms with theiranomaly and had a sexual orientation consistentwith their assigned sex and opposite to theirexternal appearance. The conclusion was reachedthat the psychological aspect of sex is undiffer-entiated at birth and becomes differentiated as theresult of the experience of growing up. Thegender role is well established by the age of two anda half years and remains so indelibly printed thatnot even gross discrepancies between it and theexternal appearance of the patient will displace it.
Ellis35 in a different type of study reached similarconclusions. Eighty-four cases from the medicalliterature were studied and it was shown that thegreat majority assumed a sexual role whichaccorded with the sex of upbringing rather thanwith the internal or external genital characteristics.From the practical point of view, this work
indicates that any change in the child's sex mustbe made before the age of three years, since thegender role is by then established. After this agechanges of sex should only be made at the requestof the patient and after the most careful considera-tion. In these cases the decision would only bemade after puberty.
In the management of all hermaphrodites it isimperative that the common feeling of the childthat he or she is half boy and half girl should beremoved. This can be dealt with by an explanationthat he or she is a boy or girl and that it is only thegenital development which is incomplete.Selection of Sex of Rearing in Cases Seen inInfancyI. Congenital Female Pseudohermaphroditism withAdrenal HyperplasiaThese patients should always be brought up as
girls and given cortisone unless seen later in child-hood and already brought up as boys, when nochange should be made and no cortisone given.2. IntersexMale Pseudohermaphrodites and True Hermaphro-
dites. In these cases the best guide is the state ofthe external genitalia, and particularly the size of
Protected by copyright.
on March 16, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.32.374.589 on 1 D
ecember 1956. D
ownloaded from

December 1956 JOLLY: Hermaphroditism 599
TYPES OF AMBISEXUAL DEVELOPMENT
SecondaryLabial Sex
Gonads Phallus Fusion Genital Ducts Develop-ment
I. Congenital adrenal hyperplasia:Female pseudohermaphrodites .. Ovaries Large + + +- - O Female Male
precocious
II. Intersexes:I. True hermaphrodites .. .. Mixed Variable Variable Mixed Male or
female
Predominantly2. Male pseudohermaphrodites: female Usually
(male vestiges) maleLarge to
A. External genitalia simulating medium + +-+ + Predominantlymale or ambiguous .. male Male or
Testes (female female(Abdominal vestiges)or inguinal)
PredominantlyB. External genitalia simulating female uterus Usually
female .. .. .. Small O usually absent female(male vestiges)
Large (may.3. Female pseudohermaphrodites .. Ovaries have penile + + + Female Female
urethra)
the phallus or the presence of a serviceable vagina.If the phallus is of a reasonable size the childshould be brought up as a boy, but if it is small,and female external genitalia are present, the childshould be brought up as a girl, particularly sincemale pseudohermaphrodites of this type mostoften become more feminine at puberty.The question of orchidectomy in these patients
is debatable. With true hermaphrodites the idealis to remove the gonad and the internal organswhich do not conform to the assigned sex. If malepseudohermaphrodites are to be brought up asgirls, removal of the testes has been recommendedon the grounds of an increased risk of futuremalignant change. On the other hand, this willremove the source of the oestrogens which can beexpected in those with female external genitaliaand necessitate later oestrogen therapy. However,this is not too serious and in all cases the correcthormone should be given at puberty as required, inorder to enhance the secondary sexual characteristics.
Female Pseudohermaphroditism without AdrenalHyperplasia. These patients should be brought upas girls, since they will later menstruate. A vagino-plasty and possibly amputation of the clitoris willbe required.SummaryA survey of present-day views on hermaphro-
ditism is presented and the different types de-
scribed in the light of embryological knowledge.Particular attention is paid to the psychologicalaspect, since the sex in which a hermaphrodite isreared is more important than any other feature indetermining the ' gender role,' that is, the sexwhich he or she feels they are. This gender roleis firmly established by the age of two and a halfyears and only very rarely should any change insex be made after this age.With the development of newer methods for the
detection of sex, such as the examination of cellnuclei, one must beware lest patients are therebyforced to take up a sex contrary to their own desiresand inclinations. In general (apart from cases offemale pseudohermaphroditism), it is the externalgenitalia which determine the sex in which thepatient can lead the happiest life.
AcknowledgmentsI would like to thank Mr. Denis Browne and
Mr. D. Innes Williams for permission to reproducephotographs of their patient (Plate 4). I am alsograteful to Mr. Derek Martin and the PhotographicDepartment of the Hospital for Sick Children,Great Ormond Street, London, and to the samedepartment of the South Devon and East CornwallHospital, Plymouth, for the illustrations.
REFERENCESI. YOUNG, H. H. (I937), ' Genital Abnormalities, Hermaphro-
ditism and Related Adrenal Diseases,' Williams and Wilkins,Baltimore.
Continued on page 607.
Protected by copyright.
on March 16, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.32.374.589 on 1 D
ecember 1956. D
ownloaded from

December I956 FAWCETT AND DHILLON: Leukaemoid Re-action in Bronchogenic Carcinoma 607
TABLE I1956 Feb. 27 March 5 March 8 March 12 March 15 March 17
R.B.C.s (n./c.mm.) .. .. .. 4.2 - 3.0 3.3
Hb. (g. IOO ml.) .. .. .. 3.5 12.3 93 10.1 10.7
W.B.C.s (n./c.mm.) .. .. .. 370,000700,000 100,000 I10,000 I110,000
N. polvmorphs () .. .. .. 87 8i 90 87 90 91
Eosinophils(%) .. .....
Band cells (%) .. .. .. .. 9 5 3 I 4 5
N. myelocytes (%) .. .. .. I I
Iymphocytes(%) .. .... 4 7 3 7 3 3
Monocytes (%) .. .. .. .. 5 4 4 2
Platelet (thousands per c.mm.) (Lemport) 220 200 200
same histological picture as the primary bronchialcarcinoma.
DiscussionHinshaw et al.2 have reported a case of severe
leukaemoid reaction associated with bronchogeniccarcinoma; the leucocyte count reached I44,000and majority of the cells were mature granulocytes.Several observers have reported leukaemoid bloodpicture in association with malignancy.3 4 5 Inour patient the diagnosis of leukaemia could not beexcluded until the histological examination of theorgans at autopsy. Hill et al.6 have discussed theproblem of leukaemoid reactions and have madeseveral useful suggestions in arriving at the correctdiagnosis during life.
This case also illustrates the value of angio-cardiography in assessing operability of the car-cinoma lung.
SummaryA case of carcinoma lung with severe leukaemoid
reaction is reported. The absence of leukaemicinfiltration in kidney, liver and spleen differentiatedthe condition from true leukaemia.
AcknowledgmentsWe are indebted to Dr. Blackburn, the con-
sultant haematologist, for his help and criticism inpreparing this paper.
REFERENCESI. KRUMBHAAR, E. B. (1926), ' Leukaemoid Blood Picture in
Various Clinical Conditions,' Amer. J. Med. Sc., 172, 519.2. HINSHAW, D. B., and HOXIE, H. J. (I949), ' Leukaemoid
Reactions in Cardinoma,' Calif. Med., 71, 300-301.3. DOWNEY, H., MAJOR, S. G., and NOBLE, J. F. (1934),
'Leukaemoid Blood Pictures of the Myeloid Type,' FoliaHaematol., 8, 383.
4. MEYER, L. M., and ROTTER, S. D. (x942), 'LeukaemoidReaction in Malignancy,' Amer. Clin. Path., X2, 218.
5. KLEEMAN, C. R. (I95I),' Lymphocytic Leukaemoid ReactionAssociated with Primary Carcinoma of the Breast,' Amer. J.Med., 10, 522.
6. HILL, J: M., and DUNCAN, C. N. (I94I), 'LeukaemoidReactions,' Amer. J. Med. Sc., 20o, 847-857.
Continued from page 599 .-Hugh Jolly, M.D., M.R.C.P., D.C.H.2. WILKINS, L. (I949), Pediatrics, 3, 533.3. WILKINS, L. (1950), 'The Diagnosis and Treatment of
Endocrine Disorders in Childhood and Adolescence,' Thomas,Springfield.
4. WILKINS, L., LEWIS, R. A., KLEIN, R., GARDNER,L. I., CRIGLER, J. F., ROSEMBERG, E., and MIGEON,C. J. (195 ), J. clin. Endocr., x, i.
5. SILVERMAN, S. H., MIGEON, C., ROSEMBERG, E., andWILKINS, L. (I952), Pediatrics, 10, 426.
6. WILKINS, L., GARDNER, L. I., CRIGLER, J. F., SILVER-MAN, S. H., and MIGEON, C. J. (1952), J. clin. Endocr.& Metab., 12, 257.
7. WILKINS, L., CRIGLER, J. F., SILVERMAN, S. H.,GARDNER, L. I., and MIGEON, C. J. (1952), Ibid.,12, 1015.
8. CRIGLER, J. F., SILVERMAN, S. H., and WILKINS, L.(1952), Pediatrics, o1, 397.
9. WILKINS, L. (1952), J. Pediatrics, 41, 86c.Io. GRUMBACH, M. M., VAN WYK, J. J., and WILKINS, L.
(I955), J. clin. Endocr. & Metab., 15, i i6i.11. WILKINS, L., GRUMBACH, M. M., VAN WYK, J. J.,
SHEPHARD, T. H., and PAPADATOS, C. (1955),Pediatrics, I6, 287.
I2. SILVERMAN, S. H., MIGEON, C., ROSEMBERG, E., andWILKINS, L. (I952), Ibid., 1o, 426.
13. WILKINS, L. (1955), Report of 13th M. and R. PediatricResearch Conference.
14. GRUMBACH, M. M., Ibid.15. WILKINS, L., BONGIOVANNI, A. M., CLAYTON, G. W.,
GRUMBACH, M. M., and VAN WYK, J. (1955), Ciba
Foundation Colloquia on Endocrinology, Vol. VIII, Churchill,London.
I6. JOLLY, H. R. (1950), Arch. Dis. Childh., 25, 207.I7. JOLLY, H. R. (I95I), Proc. Roy. Soc. Med., 44, 459.I8. JOLLY, H. R. (I955), ' Sexual Precocity,' Thomas, Springfield.I9. GROSS, R. E. (I955), Pediatrics, I6, 303.20. BONGIOVANNI, A. M., and CLAYTON, G. W. (1954),
Bull. Johns Hopkins Hosp., 94, I8o.21. CARTER, C. O. (1955), in ' Paediatrics for the Practitioner',
edited bv Gaisford and Lightwood, Butterworth, London.22. HAMPSON, J. G. (I955), Bull. Johns Hopkins Hosp., 96, 265.23. MOORE, K. L., GRAHAM, M. A., and BARR, M. L. (1953),
Surg. Gynec. Obstet., 96, 64I.24. EARR, M. L. (1954), Ibid., 99, i84.25. BARR, M. L. (I954), Lancet, i, 779.26. BARR, M. L. (1956), Ibid., i, 47.27. DAVIDSON, W. M., and SMITH, D. R. (I954), Brit. med. J.,
i, 1379.28. MOORE, K. L., and BARR, M. L. (1955), Lancet, ii, 57.29. POLANI, P. E., HUNTER, W. F., and LENNOX, B. (I954),
Ibid., 2, I20.30. WILKINS, L., GRUMBACH, M. M., and VAN WYK, J. J.
(I 954), J. clin. Endocr. & Metab., I4, 1270.3I. KLINEFELTER, H. F., REIFENSTEIN, E. C., and
ALBRIGHT, F. (I942), J. clin. Endocr., 2, 615.32. WILLIAMS, D. I. (I952), Brit. med. J., i, 1264.33. MONEY, J. (1955), Bull. Johns Hopkins Hosp., 96, 253.34. MONEY, J., HAMPSON, J. G., and HAMPSON, J. L.
(I955), Ibid.,97, r81.35. ELLIS, A. (I945), Psyc.'t.sownatic Medicine, 7, IO8.
Protected by copyright.
on March 16, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.32.374.589 on 1 D
ecember 1956. D
ownloaded from
![N. 0. STATE V5. VIRGINIA January 3], I956 William Neal ... · L. L. RAY, Assistant to the Chancellorfor J. G. VANN, Business Manager Public Relations and Development CAREY H. BOSTlAN,](https://img.pdfslide.us/doc/110x75/5ac1cf2c7f8b9a213f8d85c4/n-0-state-v5-virginia-january-3-i956-william-neal-l-ray-assistant-to.jpg)