Embed Size (px)
Citation preview
1
Produced by: The Joint Wound Management Formulary Group in collaboration with:
NHS CalderdaleCalderdale and Huddersfield NHS Foundation TrustNHS KirkleesLocala Community PartnershipsThe Mid Yorkshire Hospitals NHS TrustSpectrum Community HealthNHS Wakefield DistrictSouth West Yorkshire Partnership NHS Foundation Trust
First Edition March 2008Originally approved by SWY Area Prescribing Committee: 28th March 2008.
Second Edition: April 2010
Third Version: July 2012Review Date - July 2015
This document is available on local organisations intranet sites and on the APCwebsite athttp://www.formulary.cht.nhs.uk/Guidelines/APC/Wound_Management_Guidelines.htm
Wound ManagementFormulary
Page 1
Contributors:
Organisation Designation NameNHS Calderdale Senior Pharmacist Helen Foster
Calderdale and Huddersfield NHSFoundation Trust
Tissue Viability SpecialistNurse (TVN)
Helen FearnleyLinda Firth
Principal Pharmacist -Medicines Information -Calderdale Royal Hospital
John Yorke
Clinical Lead Podiatrist inCommunity Diabetes andWound Care
Jane Findlater
District Nurse Caroline Bradbury
Locala Community Partnerships,and also representing NHS-Kirklees
Head of MedicinesManagement Lucianne Ricketts
District Nurses Bev GreenbankDora Collick
The Mid Yorkshire Hospitals NHS Trust
Tissue Viability SpecialistNurse (TVN) - PinderfieldsHospital
Lyn Wilson
Tissue Viability SpecialistNurse (TVN) - DewsburyDistrict Hospital
Tracy Conroy
Vascular Nurse Specialist -Pinderfields Hospital Leanne Cook
Tissue Viability SpecialistNurses (TVN)
Claire BrownJoanne Newbold
Principal Pharmacist -Medicines Information -Pinderfields Hospital
Anne Fonseca
NHS Wakefield DistrictMedicines ManagementSpecialist PharmacyTechnician
Kim Mooring
Page 2
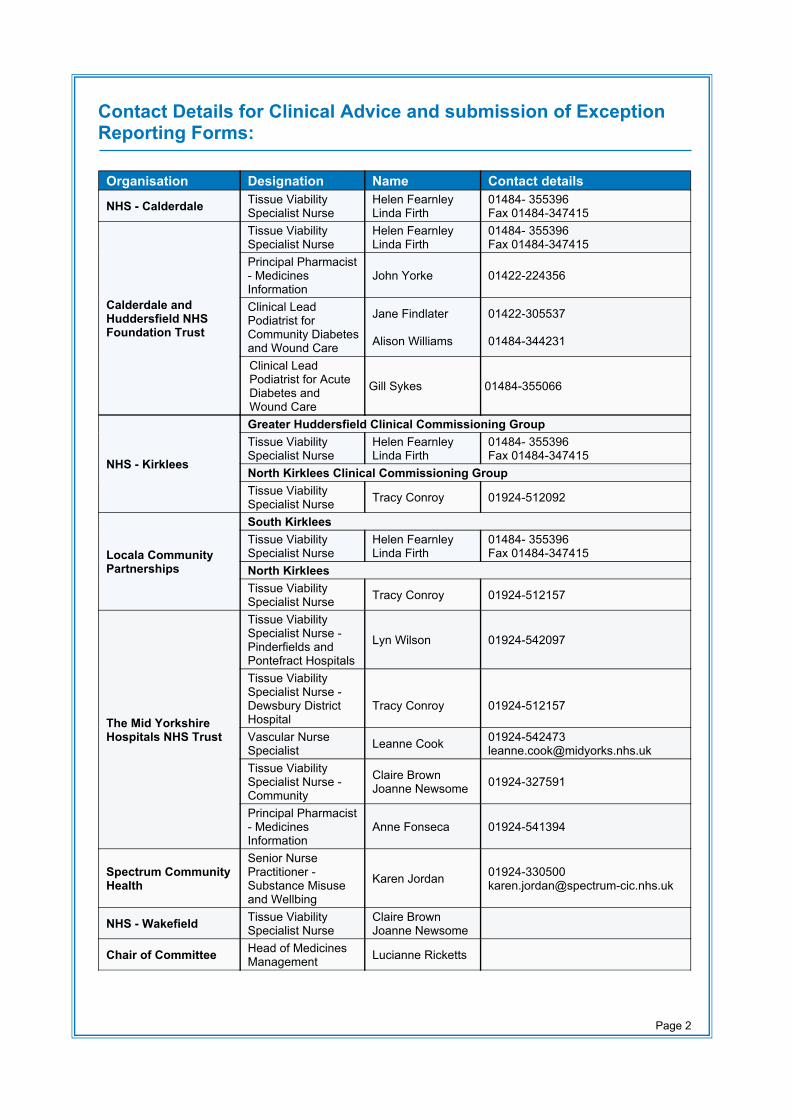
Organisation Designation Name Contact details
NHS - Calderdale Tissue ViabilitySpecialist Nurse
Helen FearnleyLinda Firth
01484- 355396Fax 01484-347415
Calderdale andHuddersfield NHSFoundation Trust
Tissue ViabilitySpecialist Nurse
Helen FearnleyLinda Firth
01484- 355396Fax 01484-347415
Principal Pharmacist- MedicinesInformation
John Yorke 01422-224356
Clinical LeadPodiatrist forCommunity Diabetesand Wound Care
Jane Findlater
Alison Williams
01422-305537
01484-344231
Clinical LeadPodiatrist for AcuteDiabetes andWound Care
Gill Sykes 01484-355066
NHS - Kirklees
Greater Huddersfield Clinical Commissioning GroupTissue ViabilitySpecialist Nurse
Helen FearnleyLinda Firth
01484- 355396Fax 01484-347415
North Kirklees Clinical Commissioning GroupTissue ViabilitySpecialist Nurse Tracy Conroy 01924-512092
Locala CommunityPartnerships
South KirkleesTissue ViabilitySpecialist Nurse
Helen FearnleyLinda Firth
01484- 355396Fax 01484-347415
North KirkleesTissue ViabilitySpecialist Nurse Tracy Conroy 01924-512157
The Mid YorkshireHospitals NHS Trust
Tissue ViabilitySpecialist Nurse -Pinderfields andPontefract Hospitals
Lyn Wilson 01924-542097
Tissue ViabilitySpecialist Nurse -Dewsbury DistrictHospital
Tracy Conroy 01924-512157
Vascular NurseSpecialist Leanne Cook 01924-542473
[email protected] ViabilitySpecialist Nurse -Community
Claire BrownJoanne Newsome 01924-327591
Principal Pharmacist- MedicinesInformation
Anne Fonseca 01924-541394
Spectrum CommunityHealth
Senior NursePractitioner -Substance Misuseand Wellbing
Karen Jordan [email protected]
NHS - Wakefield Tissue ViabilitySpecialist Nurse
Claire BrownJoanne Newsome
Chair of Committee Head of MedicinesManagement Lucianne Ricketts
Contact Details for Clinical Advice and submission of ExceptionReporting Forms:
Page 3
Contents
1. Introduction...................................................................................................................5 1.1 Notes for using the formulary
2. Wound healing process................................................................................................6 2.1 Haemostatic stage (0 - 3 days) 2.2 Proliferation stage (3 – 24 days 2.3 Maturation stage (24 days – 1 year) 2.4 Growth factors and their influence on wound healing
3. Wound types and categorisation..................................................................................8 3.1 Open and closed wounds
4. Assessment..................................................................................................................8 4.1 Wound assessment 4.2 Skin assessment
5. Factors delaying wound healing.................................................................................12
6. Wound colonisation / clinical .....................................................................................13 6.1 Wound colonisation 6.2 Wound infection
7. Wound cleansing........................................................................................................14
8. Nutrition and hydration...............................................................................................15
9. Pain assessment........................................................................................................16
10. Choosing the ideal dressing.......................................................................................16
11. Guidelines for good practice in the management of wounds.....................................18
12. Dressing selection (Poster)........................................................................................19
13. Information and practice guidelines for the products included in the formulary.........20 13.1 Alginates (e.g. Sorbsan) and hydrofibres (e.g. Aquacel) 13.2 Foams dressings (e.g. Allevyn) 13.3 Silicone dressings (eg Mepitel, Mepilex and Mepilex Border) 13.4 Hydrocolloids (e.g. Granuflex and DuoDERM) 13.5 Hydrogels (e.g. Aquaform) 13.6 Non/low adherent dressings and wound contact materials
Page 4
13.7 Film dressings (e.g. Tegaderm) 13.8 Skin protectors (e.g. Cavilon) 13.9 Antimicrobials
14. Specialised dressings.................................................................................................24 14.1 Honey (e.g. Activon) 14.2 Larvae therapy 14.3 Protease modulating matrix (e.g. Promogran) 14.4 Capillary dressing (e.g. Vacutex) 14.5 Vacuum assisted closure (VAC) 14.6 Deodorising dressings (e.g. Carboflex)
15 Challenging wounds...................................................................................................27 15.1 Overgranulation 15.2 Fungating wounds 15.3 Burns 15.4 Ischaemic/vascular wounds
16 References.................................................................................................................29
17 Glossary of Terms......................................................................................................30
18 Appendix ...................................................................................................................32 1. Non Formulary Exception Reporting Form 2. Wound Formulary Dressing List 3. Local Wound Assessment Tool (downloadable from your own local intranet site) 4. Wound Dressing Request Form 5. Evaluation of Wound Care Products Form
Page 5
1. IntroductionWelcome to the wound management formulary. We hope you find it a helpful resource inyour everyday practice.
The Joint Wound Management Formulary is available for all practitioners prescribingand/or applying wound care products throughout the acute and primary care trusts. Thereare some variations between acute and primary care provision of products dependentupon appropriateness and availability. The formulary has been devised by a panel ofpractitioners, who have specialist knowledge and expertise in wound management. It aimsto provide a clinically effective, appropriate and cost effective choice of products tomanage the vast majority of wounds and will be evaluated and updated on a two yearlybasis.
All the dressings in this formulary are for general use, with the exception of thoseindicated for specialist prescribing. All new products need to be approved by, theJoint Wound Management Formulary Group, before being added to the formulary.
Treatment for patients should be based on the best evidence of what does and does notwork and what provides the best value for money.
It must be emphasised that an holistic wound assessment must take place prior tochoosing a dressing.
1.1 Notes for using the formulary● The formulary should not be used in isolation and should not replace sound clinical
judgment.● Practitioners with specialist wound care knowledge in each Trust should be referred
to if necessary.● Specialist products listed should only be used following discussion with/assessment
by designated wound care specialists.● It is expected that the vast majority of wound care products will be selected from
this formulary. Should a product be required which is not listed, the rationale for thismust be supplied in writing on the exception reporting form attached. This will aid inthe updating process of the formulary. See appendix 1.
● Antimicrobial dressings should only be used on wounds which are clinically infectedor critically colonised (where the level of bacterial load is hindering healing).Antimicrobial dressings should only be used for a two week period then reviewed.Refer to 6.0 for further information.
● When prescribing dressings practitioners should ensure there are sufficientdressings to last up to the next review date and not necessarily to the nearest packsize.
Page 6
2. The Wound Healing Process
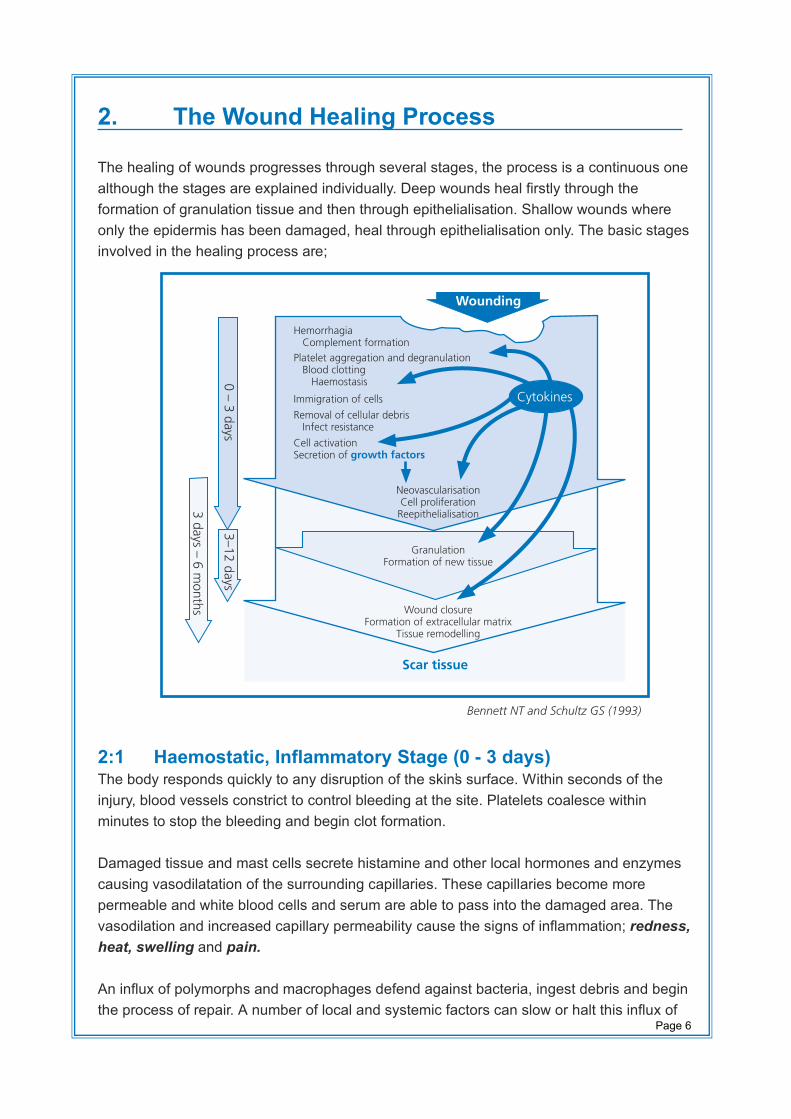
The healing of wounds progresses through several stages, the process is a continuous onealthough the stages are explained individually. Deep wounds heal firstly through theformation of granulation tissue and then through epithelialisation. Shallow wounds whereonly the epidermis has been damaged, heal through epithelialisation only. The basic stagesinvolved in the healing process are;
2:1 Haemostatic, Inflammatory Stage (0 - 3 days)The body responds quickly to any disruption of the skin’s surface. Within seconds of theinjury, blood vessels constrict to control bleeding at the site. Platelets coalesce withinminutes to stop the bleeding and begin clot formation.
Damaged tissue and mast cells secrete histamine and other local hormones and enzymescausing vasodilatation of the surrounding capillaries. These capillaries become morepermeable and white blood cells and serum are able to pass into the damaged area. Thevasodilation and increased capillary permeability cause the signs of inflammation; redness,heat, swelling and pain.
An influx of polymorphs and macrophages defend against bacteria, ingest debris and beginthe process of repair. A number of local and systemic factors can slow or halt this influx of
Wounding
HemorrhagiaComplement formation
Immigration of cells
Removal of cellular debrisInfect resistance
Cell activationSecretion of growth factors
NeovascularisationCell proliferation
Reepithelialisation
GranulationFormation of new tissue
Wound closureFormation of extracellular matrix
Tissue remodelling
Platelet aggregation and degranulationBlood clotting
Haemostasis
Scar tissue
Cytokines
0 – 3 days
3–12 days
3 days – 6 m
onths
Bennett NT and Schultz GS (1993)
Page 7
white blood cells. For example, high doses of corticosteroids such as prednisolone canstop or slow this inflammatory response and subsequent wound healing.
Dead tissue and bacteria are removed in this stage to make way for new growth. Cells inhealthy tissues are held together by proteoglycan – fibronectin cement. Where cells die dueto injury, the body acts to dissolve this intercellular cement. Liquefaction of connectivetissues in order to eliminate necrotic matter is called auto-debridement. Macrophagesmigrate into the wound and play a vital role in this stage by engulfing bacteria, any foreignbodies and necrotic tissue. With neutrophils, the macrophages attract fibroblasts andinfluence the growth of new blood vessels into the wound by chemotactic activity and therelease of growth factors
2.2 Proliferation Stage 3-24 daysThere is extensive growth of epithelial cells under the scab that bridges the wound. Withthe developing new blood vessels multiplication of the fibroblasts occurs. Fibroblasts beginto produce collagen, a process that depends on zinc, oxygen and ascorbic acid. This maybe deficient in some disease states such as diabetes. Collagen strands are deposited in ahaphazard way and form a fibrous network that supports the new capillary loops. Thetissue formed is called granulation tissue. It has a moist translucent red appearance. Signsof inflammation disappear now and the fibroblasts contract pulling the wound edgestogether.
Wound contraction is an important part of wound healing as it means that the body doesnot have to make as much granulation tissue to fill in the wound cavity. The tensile strengthof the wound is increased during this stage of the healing process and this processcontinues into the next phase, the maturation stage.
2.3 Maturation Stage 24 days – 1 yearDuring the maturation phase, fibroblasts leave the wound and collagen is remodelled into amore organized matrix. This changes the appearance from red granulation tissue to a pinkearly epithelialisation. Finally a white relatively avascular tissue develops, and theepidermis is restored to normal thickness. Tensile strength increases for up to one yearfollowing the injury. While healed wounds never regain the full strength of uninjured skin,they can regain up to 70% - 80% of its original strength.
2.4 Growth factors and their Influence on wound healingIt is thought that growth factors produced by various cells involved in wound healing act tocommunicate with each other as to ‘what to do next’. Examples of growth factors include:● Platelet derived growth factor● Fibroblast growth factor● Angiogenesis promoting growth factor● Epidermal growth factor
Page 8
● Transforming growth factor Alpha and Beta● Vascular endothelial growth factor
Each of these has different roles and for instance epidermal growth factor promotesepithelial growth.
Page 9
3. Wound types and categorisationWounds are categorised by Harding (1992) into acute and chronic wounds.● Acute wounds comprise of surgical, traumatic and thermal injuries, where it is expected
that the healing process should be uneventful and scarring and long term damageminimised.
● Chronic wounds fail to complete the healing process and have an impact on the healthstatus and lifestyle. Chronic wounds include malignant fungating wounds, pressureulcers, leg ulcers and diabetic foot ulcers. These wounds are the result of systemicdisease processes that often require specialist intervention, investigation and treatmentof the underlying cause in conjunction with the care of an open wound.
3.1 Open and closed woundsSutures, clips or wound adhesives bring the opposing edges of a wound together andcreate the moist, warm, clean environment necessary for healing. In this situation,dressings are of secondary importance.
However, on open wounds such as abrasions, burns or pressure ulcers, sutures cannot beused. In such open wounds, the choice of dressing is of critical importance as it canprovide the right environment to prevent complications and optimise healing.
Page 10
4. AssessmentWounds will heal themselves given the right conditions. It is crucial to combine a thoroughassessment of the patient with the wound assessment. Identification, improvement andminimisation of any factors known to impede healing will benefit the patients progress. Itmay not be possible to alleviate all factors that are detrimental to wound healing, howeverthese should be considered in the management and expected outcomes.
Assessment should include information from different sources. It should bring togethergeneral and specific information on the patient, the skin and the wound itself, only in thisway can an accurate diagnosis be made, risk factors evaluated and effective treatmentcommenced (Vowden and Vowden 1998).
Patient assessment can be thought of on four levels (Morison,1992)● General patient factors that could delay healing● Immediate causes of the wound and any underlying pathophysiology● Local conditions at the wound site● Potential consequences of the wound for the individual
Assessment should identify the following:Chronic diseases, which prolong or delay healing● Circulatory disorders, e.g. Anaemia, peripheral vascular disease and arteriosclerosis.● Respiratory disorders e.g. Chronic pulmonary disease, bronchitis and pneumonia● Malabsorption disorders e.g. Crohn’s disease, ulcerative colitis● Metabolic disorders e.g. Diabetes, renal & hepatic failure.● Disorders of mobility & sensation e.g. Hemiplegia, paraplegia and neuropathy.● Immune deficiency disorders e.g. Rheumatoid arthritis, HIV/AIDS, malignancyLocal factors which prolong or delay healing● Impaired blood supply● Oxygen deficit● Temperature fluctuations● Dehydration● Wound location
● Age of wound● Mechanical stress (pressure,
shear and friction)● Extent of tissue loss● Local infection
● Type of tissue involvement● Foreign bodies● Necrotic tissue● Skin maceration
Other factors that affect healing● Nutritional state● Dehydration● Body build● Systemic infection
● Stress● Immuno-suppressive agents● Drug therapy● Lack of sleep/rest
● Aging● Inappropriate wound care● Factitious injury● Pain
Psychological factors which affect healing● Motivation● Concordance
● Attitudes of patients & carer● Knowledge & understanding
● Body image
Lifestyle factors that may affect healing● Lifestyle e.g.. patterns of
working● Care environment
● Financial status● Major life stress
● Cultural or religious belief● Substance misuse
Page 11
4.1 Wound assessmentThe aim of any wound assessment is, to describe the wound appearance and allowaccurate classification of pressure ulcers. Measurement of wounds forms an important partof documentation and can be achieved by using tracing maps, disposable rulers orphotography. (Refer to local guidelines for photography.)Assessment of the wound should include a detailed evaluation of:● Wound classification● Wound appearance● Wound exudate, levels and type● Any signs of clinical infection● Condition of wound margin● Condition of surrounding skinAlthough wound exudate should not be assessed alone it must be recognised as animportant aspect of the healing process and gives distinct clues as to the condition of thewound. Wound exudate is not just an inert fluid – understanding its components will help toimprove patient care. An unexpected change in exudate characteristics may indicate achange in wound status or associated disease process and should prompt re evaluation.All the above information should be recorded on a wound assessment chart.
It is essential that a date be set for reassessment of the wound and that any changesin treatment following reassessment should be recorded.
The information gathered from the assessment should form the initial plan of carewhich should include:1) Factors such as the general appearance of the skin, wound pain or allergies.
2) Factors that will delay healing such as general health, nutritional status, underlyingdisease, medication or incontinence.
3) The cause of the wound so that further problems can be prevented, such as immobilityresulting in pressure ulcers or diabetes giving rise to a neuropathic ulcer.
4) Functional and psychological factors that will result from the wound or its treatment thatmay delay healing.
5) The requirements needed on discharge for the patient and/or carer.
6) All factors that could influence wound healing should be addressed. This may includereferral to other members of the multi disciplinary team such as Tissue Viability Nurses,Dieticians, Physiotherapists, Podiatrists, General Practitioners, Vascular Consultant orDermatologist.
Page 12
4.2 Skin assessmentWhen selecting wound management products, assessment of the surrounding skin must beundertaken to determine the potential impact the specific product may have on managingthe wound characteristics, in addition consideration of allergies must be given. Caring forthe surrounding skin may include use of topical treatments.
Definitions of topical skin applications
Emollients: also known as moisturisers. These are grease-based substances which whenapplied to the skin either trap water in or allow water to be pulled from the dermis to theepidermis. Emollients can be used as wash products in the form of soap substitutes andbath oils. Once washing is complete, emollients can be applied to the skin in the form oflotions, creams or ointments to seal water into the skin (Penzer and Burr, 2005).For example; Diprobase, Zerobase, Doublebase, Oilatum emollient.
Lotions: these are the lightest and least greasy emollients. They are less effective as theycontain less oil.For example; Dermol lotion
Creams: these have a higher oil content than lotions, allowing the oil to sink into the skin.They are good for daytime use.For example; Diprobase, Zerobase, Doublebase
Ointments: these have the highest oil content and are very greasy. They can leave theskin looking shiny and clothes greasy. However if the skin is very dry, ointments should beused and may be best applied at night.For example; Emulsifying ointment, Diprobase ointment.
NB:Some cream based products may contain preservatives that patients can becomesensitive to. Please refer to latest edition of BNF for more information on individualproducts.
NB:Please refer to National Patient Safety Agency (NPSA) website regarding use offlammable productsi.e. Yellow soft paraffin.
Page 13
5. Factors delaying wound healing
Many factors have been recognised that reduce or delay healing, the following areidentified as some of the main causes for delay in wound healing.● Poor circulation
Delayed healing and tissue breakdown is frequently associated with poor circulation. Thismay be due to local pressure, vascular disease or diabetes.
● Poor nutrition/malnutritionNutrition has a significant impact on wound healing. Lack of protein will result ininsufficient building blocks for cell regeneration. Deficiency of vitamin C which is essentialfor collagen synthesis, will delay healing.Zinc deficiency will cause slowing down of epithelialisation and collagen synthesis.
● Drug therapyAnti inflammatory drugs suppress initial inflammatory process. Systemic and topicalcorticosteroids can suppress both multiplication of fibroblasts and the immune system.
● Immune responseAllergy to topical applications, e.g. iodine may delay healing. Irritants and allergensinclude lanolin (wool alcohols), topical antibiotics, emulsifiers such as cetyl alcohol,rubber, parabens group of preservatives, colophony, fragrance mix or balsam of Peru.
● AgeCell replication is slower (senescence) and the skin’s resistance to injury decreases withincreasing age.
● ObesityAdipose tissue has poor vascularity. No known mechanism is responsible for increasedinfection and wound breakdown in obese surgical patients, but these patients are at highrisk of postoperative wound problems.
● PsychologicalIncreases in hormone levels, particularly glucocorticoids (occurring in stress and anxietyfor example) may suppress the inflammatory phase and affect healing in both acute andchronic wounds. Reducing stress has been demonstrated to reduce postoperative woundinfection.
● InfectionLocal or systemic infection inhibits healing. Resistance to infection is related tophysiological ability and the patient’s physical health. Bacterial toxins are potent inhibitorsof healing. Some have more devastating effects than others.
● MoistureExposure to excessive exudate can be associated with other clinical issues in chronicwounds. It may result from increased bacterial burden related to local wound infection.Poorly managed urinary and faecal incontinence can have a devastating effect on theskin integrity and represents a significant threat to the peri-anal skin. In severe cases, theskin can also be so badly damaged that a moisture lesion develops. These are painfuland require prompt treatment to prevent them growing in size.
Page 14
● TemperatureThe optimum temperature for cellular activity and division is 37ºC. Frequent dressingchanges, application of cold solution and leaving the wound exposed can decrease thelocal temperature.
● ChemicalInappropriate use of chemicals, for example, dyes or antiseptics, can damage the woundand retard healing. This practice should be discouraged.
● MechanicalUnnecessarily disturbing the wound bed can damage the developing granulation tissue.Inappropriate dressings can also damage the granulation tissue. Mechanical cleansing ofthe wound is not required.
● MalignancyMalignancy can inhibit healing as can a range of anti-neoplastic therapies
● Drug TherapySome medication has the potential to cause ulceration e.g. Nicorandil.
● Sensory NeuropathySensory loss as a result of diabetic peripheral neuropathy is a major factor contributing tofoot ulceration, 15% of diabetic neuropathy sufferers develop foot ulcers (Bild et al(1989)cited in Baker et al (2005). Sensory neuropathy can have other causes and the foot is atrisk due to the loss of protective sensations. Damage to the tissues happens and thepatient less likely to limit function due to the lack of pain from the wound, they are morelikely to underestimate the seriousness of the wound.NB pain in a foot that normally has no sensation can be a sign of infection and should benoted and investigated.
● Local factorsPoor surgical technique such as over use of diathermy or poor choice of suturing materialare among factors that will delay healing of a surgical wound (Leaper and Gottruo 1998)Poor assessment or some wound care practices may predispose to delayed or nonhealing.Inappropriate choice of wound dressing, the use of fibre shedding materials like cottonwool or gauze swabs, tight bandaging can all lead to deterioration in the wound.
● General factorsPoor assessment of the cause of the wound can lead to inappropriate treatment and thiswill lead to poor healing. Any deterioration in the patients overall health adversely affectshealing.
● PainAll wounds have the potential to cause pain, and the nature of the pain varies with thetype of wound. Many factors may exacerbate pain, including infection and dressingchange. Inadequately managed pain can lead to adverse physical and psychologicalpatient outcomes. Continuous, unrelieved pain activates the pituitary-adrenal axis, whichcan suppress the immune system and result in post-surgical infection and poor woundhealing
Page 15
Continuous, unrelieved pain also affects the psychological state of the patient and familymembers. Common psychological responses to pain include anxiety and depression.The inability to escape from pain may create a sense of helplessness and evenhopelessness, which may predispose the patient to a more chronic depression (Wells etal 2008)
● Other Smoking
Page 16
6. Wound colonisation / clinical infection
Increased bacterial load on the wound bed is a common factor that can delay wound healing.An understanding of microbiology concepts, normal wound healing process and the ability toidentify factors which are delaying wound healing is crucial for any practitioner involved inwound care.
All chronic wounds that are healing by secondary intention will be contaminated with a varietyof bacteria, but this level of bacteria will NOT affect wound healing, therefore DOES NOTrequire routine use of antimicrobial dressing. Although wounds may become colonised bya diverse range of bacteria, infection is not an inevitable consequence. Only wounds that arecritically colonised or infected require topical antimicrobial dressings and the effect of thesedressings need to be regularly reviewed to ensure treatment is effective and discontinued assoon as bacterial load is under control. Clinical wound infection occurs when there is apresence of multiplying bacteria which results in a host response. Identification of woundinfection should be viewed as a clinical skill which is supported by laboratory finding whennecessary, but should not rely on pure laboratory science. Signs and symptoms of clinicalwound infection include Erythema, heat, swelling, pain, abscess formation, pyrexia, and raisedwhite cell count (with no other source of infection).
Wound swabbing should only be undertaken when signs of clinical infection are present.Routine wound swabbing should not be undertaken. All wounds contain microorganisms yetthe majority are not clinically infected, wound swabs will often show evidence of bacteria(contamination), positive wound swab results need to be taken in context of clinical symptomsand DO NOT routinely need to be treated with either topical antimicrobials or systemicantibiotics. To reiterate reports of growth of organism on a laboratory result is not an indicationfor antimicrobial/antibiotic therapy.
Topical antimicrobial dressings contain agents to provide sustained antimicrobial effects;these include ones containing Honey, Silver, Iodine and PolyhexamethyleneBiguanide(PHMB). The aim of these dressings is to reduce the bacterial load therefore promptinghealing. However it is important to note that there is a lack of robust evidence that antimicrobialdressings are effective in preventing or treating infection and widespread use may result inbacterial resistance and toxicity. The need for an antimicrobial dressing should be based onholistic assessment of the patient and the wound. It is imperative to select a woundmanagement product which is appropriate for the tissue type, the level of exudate and patientcomfort. Other options of reducing bacterial load should be considered including wounddebridement which may eliminate the need for topical antimicrobials.
If antimicrobial dressings are utilised they require regular review and once consistent signsof healing are observed antimicrobial therapies should be stopped. If there is no evidenceof wound improvement after 2 weeks of treatment with an antimicrobial dressing, it isrecommended that an alternative topical antiseptic or antimicrobial agent is used. If the

Page 17
wound begins to show further signs of infection, the use of a systemic antibiotic should beconsidered, (Wounds UK, 2010).
It should be noted that infection of Diabetic foot Ulceration often requires aggressivetreatment including antimicrobial therapy in combination with antibiotic therapy and willrequire review by a member of the Diabetic foot team (NICE, 2011), as often effectivemanagement requires surgical incision, aggressive debridement and drainage with orwithout re vascularisation, (American Diabetes Association, 2003).
Page 18
7. Wound cleansingThe aim of cleansing is to create the optimal local conditions for a wound to heal byremoving exudate, debris such as dressing residue, slough and necrotic tissue. (Morison1989)
Wound cleansing should only be considered following a thorough assessment of thewound. If the disturbance to the wound bed is not justified, then the wound is probably bestleft alone.(Cutting 1990)
The most common solutions, which are currently used, are sodium chloride 0.9% or tapwater. The use of antiseptics are no longer recommended, as they are not effective and arepotentially harmful (Miler 1994)
Practice Guidelines● Irrigation is the preferred method of wound cleansing● Irrigation solutions should be applied at approximately 37ºC to prevent a drop in the
wound bed temperature● Chronic wounds such as venous leg ulcers can be cleansed using tap water and an
emollient● Do not use cotton wool balls/gauze as they shed fibres prolonging the inflammatory
phase, delaying healing. (Surgical Materials Testing Laboratory 1992)
Page 19
8. Nutrition and hydrationGood nutrition facilitates the wound healing process but malnutrition will delay, inhibit andcomplicate wound healing. Many nutrients have a role to play in wound healing, working inisolation or in combination with others.
Whilst a large percentage of patients admitted to hospital are already malnourished, it mustalso be recognised that many have a good nutritional status which deteriorates onceadmitted due to the consequence of their illness.
In a malnourished patient the phases of healing are the same. However, wound healingtakes a large amount of metabolic energy due to an increased number of inflammatorycells, and the fibroblastic formation of collagen and matrix remodelling. In the patient withprotein energy malnutrition the healing process can take 5 – 10 times longer.
Nutrition is a crucial aspect of a holistic approach to the healing of wounds. (Todorovic2002).Nutritional status should always be assessed in patients with wounds; if patients have adecreased nutritional status then this can be addressed.
NICE Clinical Guideline 32 - Nutritional Support in Adults offers best practice adviceon the care of adults who are malnourished or at risk of malnutrition and how toidentify them. The malnutrition universal screening tool (MUST) is recommended -www.bapen.org.uk/pdfs/must/must_page1.pdf.
It is therefore important to encourage patients to have a wide and varied food intake toprovide a balanced diet to maintain body cell mass and promote wound healing.
Carbohydrates provide the energy for the inflammatory response to occur
Protein deficiency results in impairment of the proliferative and remodelling stage of woundhealing. Impaired collagen synthesis, reduced wound strength and increase in infection dueto a compromised immune system has been reported. (Collins 2001)
Fats have a key role in the structure and function of cell membranes and are directlyinvolved in cholesterol metabolism, the formation of inflammatory mediators, and clottingcomponents. Following injury there is an increased requirement for polyunsaturated fattyacids, during the inflammatory phase of healing. Recent studies suggest that omega-3 fishoils are beneficial as they have an anti-inflammatory response and could influence woundhealing. (Mclaren 1992)
Vitamins: Many vitamins are involved in wound healing, the main one being vitamin C. Thisis vital for collagen synthesis, as it is an essential co-factor in the hydroxylation of proline.
Page 20
Deficiency of vitamin A and Vitamin B complex will also have adverse effects on woundhealing.
Zinc, Copper and Iron are the main minerals in wound healing. Zinc deficiency inhibitswound repair by reducing the rate of epithelialisation and cellular proliferation. It is also anessential co-factor in many enzyme systems, as is copper, which plays an important role incollagen and elastin synthesis. Iron deficiency needs to be avoided, as an inadequateblood flow to the wound site will inhibit the healing process.Other supplements of vitamins and minerals, however, should be avoided as this can bedetrimental to the patient, affecting absorption and metabolic interactions and, ultimately,impair nutritional status.
Hydration. In addition to nutrition, fluid balance is important. Dehydration can result indiminished healing ability since water is a major component of healthy cells. A large woundmay exude significant volumes of fluid that can result in electrolyte imbalance as well asdehydration. A heavily exudating wound may also delay healing by macerating surroundingskin.
Page 21
9. Pain assessmentUnresolved pain negatively affects wound healing and has an impact on quality of life. Painat wound dressing-related procedures can be managed by a combination of accurateassessment, suitable dressing choices, skilled wound management and individualisedanalgesic regimens. For therapeutic as well as humanitarian reasons it is vital thatclinicians know how to assess, evaluate and manage pain.
Having a basic understanding of pain physiology will help anyone involved in a wounddressing-related procedure to understand the patient’s pain experience. It is fundamental toappreciate that pain from wounds is multidimensional, and the patient’s psychosocialenvironment will influence and impact on the physiological experience of pain.
Practical applications● Assume all wounds are painful● Over time wounds may become more painful● Accept that the skin surrounding the wound can become sensitive and painful● Accept that for some patients the lightest touch or simply air moving across the wound
can be intensely painful● Know when to refer for specialist assessment
Ref - Principles of best practice: Minimising pain at wound dressing-related procedures.A consensus document. London: MEP Ltd. 2004
Page 22
10. Choosing the ideal dressingThere are two different categories of dressings:1) Primary – This is in contact with the wound.2) Secondary – This is not in contact with the wound but it covers the primary dressing.
When choosing a secondary dressing ensure its compatibility with the primary woundcontact layer.
There are many hundreds of wound products available, all having slightly differentproperties. The ideal wound management choice is dependant on the type, depth andcolour of the wound in conjunction with the stage of healing and what the main objective oftreatment is: e.g. debridement or protection. Dressing choice should also be influenced bythe level and type of exudate.
The ideal dressing is considered to be, one that ensures optimal healing and addressesthe following:● Maintain high humidityEpidermal cells require a moist (not wet) surface to permit them to migrate across thewound surface. A dry wound forces the cells to burrow deeper until they meet a moist level,delaying healing. This is based on the initial work of George Winter (1962). Studies haveshown that the moist environment enhances natural autolytic processes by breaking downnecrotic tissue.
● Removes excess wound exudateExudate, micro organisms, toxins and dead cells are removed to relieve maceration, tissueoedema and to reduce pain and swelling. The dressing choice will allow control of theexudate, either by absorbing it into the dressing or by passing it onto a hydrophylicabsorbent secondary dressing (Cherry and Harding 1997).
● Permit thermal insulationA constant temperature of 37º C is essential to maintain biological processes (mitosis andenzymatic activity).
● ImpermeabilityA dressing should prevent bacteria gaining access to the wound surface. A soaked orleaking dressing provides a pathway for bacteria in either direction. Some dressings arewaterproof allowing showering whilst in position.
● Gaseous exchangeAt different phases of wound healing both hypoxia and normal amounts of oxygen arerequired. A more rapid restoration of the microcirculation occurs in an anaerobicenvironment. High levels of oxygen are necessary for the development of fibroblasts andcollagen.
Page 23
● Non fibre shedding / non toxicFibres shed into the wound can cause irritation and can become a focal point for infection.Granulating tissue can grow into the open mesh, attaching the dressing to the wound.Local irritation or sensitivity can occur with some products.
● Non adhesive, comfortable and conformingThe dressing must be non adhesive to the wound bed and protect the wound andsurrounding skin from further trauma. (Dealey 2004). Patient concordance is best achievedwith a comfortable, conforming, flexible dressing causing minimal pain when changed anddoes not take excessive time to redress.
● Care of ischaemic woundsThe toes and sometimes the foot can be affected by so called “dry gangrene” in chronicarterial insufficiency. The tissues are black, shrivelled and dry. Whilst it is traditionallycalled gangrene there is in fact no infective process. The tissues are undergoingspontaneous breakdown and drying. It is a form of mummification. It is important that suchareas, unlike other wounds, are kept dry. Introducing moisture carries the risk of infection.Ideally the area should be left exposed to the air. A non adherent dressing to separate toesis useful. If a dressing is required it should be light, dry and allowing the circulation of air.
Page 24
11. Guidelines for good practice in themanagement of wounds
● Always employ an holistic approach to wound care: e.g. investigate any underlyingproblems
● Wounds should not be routinely cleansed, but if they require cleansing irrigation shouldbe used
● Good hand hygiene must be practiced at all times● Nutrition assessment must be completed and acted upon● It is essential that a date be set for reassessment of the wound and that any changes in
treatment following reassessment should be recorded● Wounds should not be left exposed or wrapped in a dressing towel. The action of
dehydration and reduction in wound temperature is detrimental to wound healing● A multidisciplinary approach must be taken in wound care● A clear explanation of the action of certain types of dressings must be explained to the
patient● Avoid layering dressings, most products are designed as a primary dressing, use of
more products only reduces the effectiveness of the product.● All dressings should be disposed of according to local waste disposal guideline● All dressings must be prescribed● For any wound not progressing as anticipated consider referral to the Tissue
Viability Team by using the appropriate referral process.
Page 25
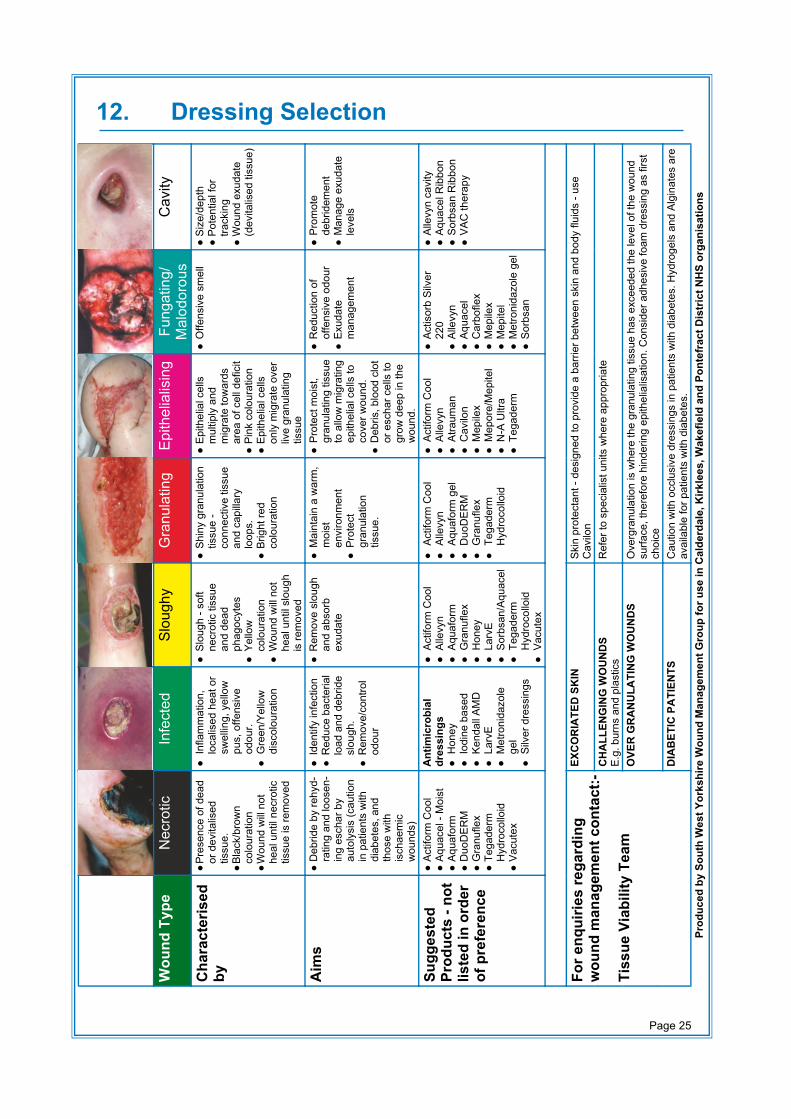
12. Dressing Selection
Wou
nd T
ype
Nec
rotic
Infe
cted
Slou
ghy
Gra
nula
ting
Epith
elia
lisin
gFu
ngat
ing/
Mal
odor
ous
Cav
ity
Cha
ract
eris
edby
●Pr
esen
ce o
f dea
dor
dev
italis
edtis
sue.
●Bl
ack/
brow
nco
lour
atio
n●
Wou
nd w
ill no
the
al u
ntil
necr
otic
tissu
e is
rem
oved
●In
flam
mat
ion,
loca
lised
hea
t or
swel
ling,
yel
low
pus,
offe
nsiv
eod
our.
●G
reen
/Yel
low
disc
olou
ratio
n
●Sl
ough
- so
ftne
crot
ic ti
ssue
and
dead
phag
ocyt
es●
Yello
wco
lour
atio
n●
Wou
nd w
ill no
the
al u
ntil
slou
ghis
rem
oved
●Sh
iny
gran
ulat
ion
tissu
e -
conn
ectiv
e tis
sue
and
capi
llary
loop
s.●
Brig
ht re
dco
lour
atio
n
●Ep
ithel
ial c
ells
mul
tiply
and
mig
rate
tow
ards
area
of c
ell d
efic
it●
Pink
col
oura
tion
●Ep
ithel
ial c
ells
only
mig
rate
ove
rliv
e gr
anul
atin
gtis
sue
●O
ffens
ive
smel
l●
Size
/dep
th●
Pote
ntia
l for
track
ing
●W
ound
exu
date
(dev
italis
ed ti
ssue
)
Aim
s●
Deb
ride
by re
hyd-
ratin
g an
d lo
osen
-in
g es
char
by
auto
lysi
s (c
autio
nin
pat
ient
s w
ithdi
abet
es, a
ndth
ose
with
isch
aem
icw
ound
s)
●Id
entif
y in
fect
ion
●R
educ
e ba
cter
ial
load
and
deb
ride
slou
gh.
●R
emov
e/co
ntro
lod
our
●R
emov
e sl
ough
and
abso
rbex
udat
e
●M
aint
ain
a w
arm
,m
oist
envi
ronm
ent
●Pr
otec
tgr
anul
atio
ntis
sue.
●Pr
otec
t moi
st,
gran
ulat
ing
tissu
eto
allo
w m
igra
ting
epith
elia
l cel
ls to
cove
r wou
nd.
●D
ebris
, blo
od c
lot
or e
scha
r cel
ls to
grow
dee
p in
the
wou
nd.
●R
educ
tion
ofof
fens
ive
odou
r●
Exud
ate
man
agem
ent
●Pr
omot
ede
brid
emen
t●
Man
age
exud
ate
leve
ls
Sugg
este
dPr
oduc
ts -
not
liste
d in
ord
erof
pre
fere
nce
●Ac
tifor
m C
ool
●Aq
uace
l - M
oist
●Aq
uafo
rm●
Duo
DER
M●
Gra
nufle
x●
Tega
derm
Hyd
roco
lloid
●Va
cute
x
Ant
imic
robi
aldr
essi
ngs
●H
oney
●Io
dine
bas
ed●
Kend
all A
MD
●La
rvE
●M
etro
nida
zole
gel
●Si
lver
dre
ssin
gs
●Ac
tifor
m C
ool
●Al
levy
n●
Aqua
form
●G
ranu
flex
●H
oney
●La
rvE
●So
rbsa
n/Aq
uace
l●
Tega
derm
Hyd
roco
lloid
●Va
cute
x
●Ac
tifor
m C
ool
●Al
levy
n●
Aqua
form
gel
●D
uoD
ERM
●G
ranu
flex
●Te
gade
rmH
ydro
collo
id
●Ac
tifor
m C
ool
●Al
levy
n●
Atra
uman
●C
avilo
n●
Mep
ilex
●M
epor
e/M
epite
l●
N-A
Ultr
a●
Tega
derm
●Ac
tisor
b Si
lver
220
●Al
levy
n●
Aqua
cel
●C
arbo
flex
●M
epile
x●
Mep
itel
●M
etro
nida
zole
gel
●So
rbsa
n
●Al
levy
n ca
vity
●Aq
uace
l Rib
bon
●So
rbsa
n R
ibbo
n●
VAC
ther
apy
For e
nqui
ries
rega
rdin
gw
ound
man
agem
ent c
onta
ct:-
Tiss
ue V
iabi
lity
Team
EXC
OR
IATE
D S
KIN
Skin
pro
tect
ant -
des
igne
d to
pro
vide
a b
arrie
r bet
wee
n sk
in a
nd b
ody
fluid
s - u
seC
avilo
nC
HA
LLEN
GIN
G W
OU
ND
SE.
g. b
urns
and
pla
stic
sR
efer
to s
peci
alis
t uni
ts w
here
app
ropr
iate
OVE
R G
RA
NU
LATI
NG
WO
UN
DS
Ove
rgra
nula
tion
is w
here
the
gran
ulat
ing
tissu
e ha
s ex
ceed
ed th
e le
vel o
f the
wou
ndsu
rface
, the
refo
re h
inde
ring
epith
elia
lisat
ion.
Con
side
r adh
esiv
e fo
am d
ress
ing
as fi
rst
choi
ceD
IAB
ETIC
PA
TIEN
TSC
autio
n w
ith o
cclu
sive
dre
ssin
gs in
pat
ient
s w
ith d
iabe
tes.
Hyd
roge
ls a
nd A
lgin
ates
are
avai
labl
e fo
r pat
ient
s w
ith d
iabe
tes.
Prod
uced
by
Sout
h W
est Y
orks
hire
Wou
nd M
anag
emen
t Gro
up fo
r use
in C
alde
rdal
e, K
irkle
es, W
akef
ield
and
Pon
tefr
act D
istr
ict N
HS
orga
nisa
tions
Page 26
13. Information and practice guidelines for theproducts included in the formulary
13.1 Alginates (e.g. Sorbsan) and hydrofibre (e.g. Aquacel)Alginates are dressings derived from alginic acid extracted from seaweed. The gellingcharacteristics of alginate dressings vary according to the product used. Some productsonly gel to a limited extent to form a partially gelled sheet that can be lifted off, others forman amorphous gel that can be rinsed off with water. A secondary dressing is needed. Theyare highly absorbent and are suitable for moderately or heavily exuding wounds, but not foreschars or for dry wounds.
Aquacel dressings are hydrofibre dressings which combine:● The healing benefits of hydrocolloids● A fluid handling capacity exceeding that of the alginates● Reduce microbial transmission by retaining bacteria and minimising airborne dispersal
during dressing changes● A pain free removal● Aquacel can be applied moist to a dry wound with eschar
Guidelines for use● Useful for debriding● Aquacel can be moist when applied to a dry wound● Highly absorbent, suitable for use on medium to high exudate● Cover with a secondary dressing● Can be used on clinically infected wounds but the patient will require systemic antibiotics
and daily dressing changes● May be left in place for a maximum of seven days● If filling cavities do not pack the dressing tightly● Alginates are considered to have some haemostatic properties
13.2 Foam dressings (e.g. Allevyn)Most foam dressings are made out of polyurethane foam or silicone foam. They are lowadherent and are suitable for light to moderately exuding wounds. Used as a primarydressing on clean granulating wounds or as a secondary dressing on sloughy wet wounds.
Guidelines for use● Available with or without adhesive borders● They can be cut/ shaped to aid application (except Allevyn Cavity). This should be con-
sidered before selecting a ‘shaped dressing’ as it may be more cost-effective e.g. asquare Allevyn adhesive can be cut/ shaped to aid application to a heel wound.
● A variety of shapes are available. Consider the full range of shapes and sizes prior to se-lection e.g. Allevyn heel can be applied to elbow wounds
Page 27
● Allow at least 2cm overlap around the wound edges● Can be left in place up to 7 days depending upon exudate levels.● Do not secure with an occlusive dressing as this may lead to tissue maceration● Can be used on clinically infected wounds; however the patient may require systemic
antibiotics and daily dressing changes (Morgan, 2000).● May be useful on overgranulation tissue● Not recommended for dry wounds● Can be used under compression bandages/ hosiery● Foam dressings should be used as a wound care product and not a pressure relieving
product. Other devices are more suitable for this purpose e.g. Dermal pads.● Allevyn cavity is a conformable, absorbent, non-adhesive dressing comprised of perforat-
ed, low-adherent outer layer with a core of foam chips – suitable for cavity wounds.
13.3 Silicone dressings (eg Mepitel, Mepilex and Mepilex Border)
13.3a MepitelMepitel is a porous,transparent and flexible wound contact layer with adherent properties. Itconsists of a flexible polyamide net coated with a soft silicone layer. Mepitel is notabsorbent, but contains apertures or pores approximately 1mm in diameter that allows thepassage of exudate into a secondary dressing. The secondary dressing must be changedas required by the conditions of the wound and the amount of exudate in order to preventmaceration.
Indications● Typical use is in the management of wounds where adherence of a dressing to the
underlying tissue presents a particular clinical problem.● Typical applications include skin tears or abrasions, surgical excisions, second-degree
burns, blistering conditions such as Epidermolysis bullosa,lacerations, partial and fullthickness grafts, and skin damage following radiotherapy or steroid therapy.
Guidelines for use.● If clinically indicated the wound should be cleansed and the surrounding skin thoroughly
dried● Choose a size of Mepitel that covers the wound and the surrounding skin by 2cm. It can
be cut to size if needed before removing the protective outer films. If more than one pieceis required, the dressings may be partially overlapped, ensuring that the pores are notblocked.
● Moistening gloves with sterile water or saline will help to stop the dressing from stickingto the fingers and thus facilitate application.
● Smooth the dressing in place ensuring a good seal with the surrounding skin.● Where clinically indicated, topical steroids or antimicrobial agents can be applied either
over or under the Mepitel● Apply a secondary absorbent dressing pad and a suitable fixation device or bandage.
Page 28
Frequency of change.● Mepitel can be left in place for extended periods, up to 7-14 days in some instances. The
outer absorbent layer should be changed as frequently as required.● Warning; If Mepitel is used on burns treated with meshed grafts or after facial resurfacing
imprints can occur if excess pressure is placed upon the dressing. As with all types ofdressings, wounds should be regularly monitored for signs of infection or deterioration.
Contra-indications● The manufacturers have identified no absolute contra-indications to the use of Mepitel.
13.3b Mepilex and Mepilex BorderMepilex and Mepilex Border are absorbent, atraumatic dressings made from polyurethanefoam. The outer surface has a vapour-permeable membrane which acts as a barrier toliquid and microorganisms. The wound contact surface is coated with a soft layer ofsilicone that does not stick to the surface of the wound or cause trauma to delicate newtissue on removal.
Indications● Mepilex and Mepilex Border are suitable for many types of exuding wounds including leg
and pressure ulcers, and traumatic wounds resulting in skin loss. The dressing absorbsexudate and maintains a moist wound-healing environment whilst minimising the risk ofmaceration.
Guidelines for use● Available with or without adhesive border● Allow at least 2cm overlap around the wound edges● The non-bordered dressing may be held in place with a bandage or other suitable
retention aid● If clinically indicated, the wound should be cleaned and the surrounding skin thoroughly
dried before application of the dressing.
Frequency of change● The interval between changes is determined by the degree of exudate produced. The
dressing may be left undisturbed for several days on clean lightly exuding wounds orclean non-infected wounds.
Contra-indications● Highly exuding wounds
13.4 Hydrocolloids (e.g. Granuflex and DuoDERM)Hydrocolloids act by autolysis, rehydrating the wound thereby promoting debridement. Thedressing can be used throughout the entire wound healing process and can provide localpain relief by keeping the nerve endings moist. (Morgan 2000)
Page 29
Some hydrocolloids, including Granuflex and DuoDERM, contain gelatin of porcine origin(of purified pharmaceutical quality), however, the manufacturers have a document writtenby a Muslim cleric advising on their use in members of the Muslim faith. The Comfeel rangeof dressings do not contain gelatin, the only hydrocolloid in these products is sodiumcarboxymethylcellulose.
Guidelines for use● Hydrocolloids absorb low to medium levels of exudate● Hydrocolloids form a yellow gel as the exudate is absorbed; this may be malodourous
and should not be confused with clinical wound infection● The dressing is waterproof enabling the patient to shower● Care should be taken when applying to fragile skin● Use with caution on diabetic foot ulcers, which require regular evaluation● The dressing is more flexible and gives better adhesion if warmed in the hands prior to
use● Apply with a minimum of 2 cm beyond the wound edges to aid good adhesion● Secondary dressings are not required● Leave dressing on the wound for 3 – 7 days● Lightly dust with un-perfumed talcum powder to reduce rucking of the edges of the
dressing● In some cases overgranulation may occur, this may resolve spontaneously when the
dressing is no longer used
Contra indications● Highly exuding wounds – consider alginates● Not suitable for clinically infected wounds● In the presence of an anaerobic infection, occlusive dressings should not be used
13.5 Hydrogels (e.g. Aquaform or Actiform Cool)Hydrogel dressings are available as an amorphous gel or in the form of a sheet. Asecondary dressing is usually required. These dressings are usually used to donate liquidto dry sloughy/ necrotic wounds and facilitate autolytic debridement. They may also havethe ability to absorb limited amounts of exudate.
Guidelines for use● Can be used throughout the entire wound healing process● Remove by irrigation if necessary● Can be used on clinically infected wounds but will required systemic antibiotics and
daily dressing changes (Morgan, 2000)● Change between 1 – 3 days● For amorphous gels (e.g. Aquaform) apply a minimum of 5mm and cover with a
secondary dressing
Page 30
● Amorphous hydrogels can be introduced into narrow wounds and sinuses ifnecessary
● Dry or necrotic wounds may require an occlusive secondary dressing e.g. film● Effectiveness may be compromised if used under compression bandages● Hydrogels have been found to be useful in the management of moisture excoriation
due to incontinence when applied as a lotion after cleansing● Actiform cool is suitable for painful wounds and skin conditions. It can be used under
compression. It should be changed if it becomes discoloured or opaque.
Contraindications● Unmanageable exudate – consider an alginate or hydrofibre● Maceration of the surrounding skin – consider skin protection and review primary
dressing
13.6 Non/low Adherent Dressings and wound contact materialsThese dressings can be made from a variety of materials but the majority of them are madeup of silicone and polymide net. These dressings vary in their non adherent properties.
Silicone coated dressings are usually non-adherent, while others are mostly low adherent.
Guidelines for use● Often used as a primary dressing on granulating/lightly exuding wounds● Low adherent dressings can cause trauma if care is not taken when removing● These dressings have limited absorbency and strike-through may occur● Frequency of dressing changes varies and is required before or when strike-through
occurs● Mepitel is considered to be cost effective only if left in-situ for a minimum of 7 days but
will require a secondary dressing change as required● Apply in single sheets – do not layer
13.7 Film dressings (e.g. Tegaderm)Provide a moist wound healing environment. They are non absorbent but are vapourpermeable. Most are transparent, allowing monitoring of the skin/wound.
Guidelines for use● Suitable for non exudating wounds, as fluid may accumulate underneath causing
maceration● Can be used prophylactically to reduce risk of trauma from shearing and friction● Often used for retention of canula/drains or protection around catheters and peg sites● Use with caution on fragile skin● May be used as a secondary dressing over alginates or gels● To remove – stretch the film at the corners to release the adhesive and reduce trauma
Page 31
Contra indications● Not recommended for routine use on infected wounds
13.8 Skin Protectors (Cavilon)Designed to provide a barrier between the skin and body fluids.● Those products that do not contain alcohol are marked as non sting and are
recommended● It can be useful to protect wound edges from maceration secondary to wound exudate● May be used as a barrier against irritation from body fluids
Guidelines for use● Single patient use only● Will not alter the effectiveness of incontinence products● Cavilon barrier film is available in 1ml or 3ml applicator or a pump spray action bottle● Can be used around a stoma site to protect against skin excoriation and as a protector
against radiation tissue damage for oncology patients, or to protect fragile skin fromadhesive stripping
● When using Cavilon cream as a barrier cream re- application is recommended after threeincontinent episodes
● Cavilon barrier film is waterproof: reapplication is recommended every 24 – 72 hoursunder normal use
● Does not contain alcohol and can be used on broken skin with no detriment● Skin should be clean and dry before application● Apply a uniform coating over the whole area● Wash and clean area before reapplication● When applied to an area where there are skin folds, hold these apart for approximately
30 seconds o allow the skin to dry
13.9 Anti-microbialsMedicated dressings most frequently contain silver or iodine, which are released in anappropriate concentration over time. They assist in infection control by reducing the numberof wound pathogens and are effective in the management of both aerobic and anaerobicbacteria. Systemic antibiotics are the preferred choice of treatment for clinical infection butshould only be used when absolutely necessary and in accordance with local guidelines. Ifischaemia is present and the blood supply to the wound is compromised anti-microbials areparticularly useful.
The antimicrobial activity of silver has been known of for many years and its efficacy inpreventing secondary infections. The growing threat of antibiotic resistance, and theconcerns about safety and toxicity of topical antiseptics, appears to have spurred a surge ofinterest in silver in wound care products. Investigations into the molecular mechanisms ofdisinfection support that metal ions such as silver, may inhibit bacterial survival by reactingwith the inside or outside of bacterial cells either directly or indirectly.
Page 32
The use of antimicrobial products within the Wound Care Formulary is recommended withcare, and is restricted. All products must only be used following full assessment of thewound to ensure the product is appropriate.
Guidelines for using antiseptic products (e.g. iodine based)● Should only be used on wounds that are high risk for bacterial contamination● Effective against a broad spectrum of bacteria, including MRSA, protozoal and fungal
infections● Iodine is absorbed systemically and when using Iodoflex the amount applied must not
exceed more than 50g in a single dose or 150g in one week. A course of treatmentshould not exceed 3 months in duration
● A maximum of four layers of povidone iodine (Inadine) dressings to be applied at onetime
● Free iodine content is low but some iodine sensitivity has been reported● Iodine products are useful in the management of the patient with diabetic foot ulcers
when there is an increased risk of clinical infection and potential risk to the limb’s integrity● Remove with care, change dressing when the colour changes to white● Dressing requires changing frequently if levels of antibacterial activity are to be
maintained● Requires a secondary dressing
Contra Indications for using iodine based products● Should not be used on patients with a known iodine sensitivity, thyroid disease, pregnant
and breast feeding women, or patients on lithium (Morgan 2000)● Not recommended for children under 2 years.● Should be avoided in patients with severe renal impairment
Guidelines for using silver dressing products (e.g. Aquacel AG)● Effective against bacteria, including MRSA, protozoal and fungal infections● Most are applied directly to the wound bed, should adherence be a problem apply a non-
adherent dressing first● Some require a secondary dressing● Change between 1-7 days refer to product guidelines● Silver sulfadiazine (Flamazine) is available for limited use in certain circumstances● All silver dressings should be used with caution as the mechanism of action differs
between products● It is essential that a date be set for reassessment of the wound and that any changes in
treatment following reassessment should be recorded
Special precautions● Use with caution in pregnant or lactating women● Use with caution in patients with hepatic and renal impairment
Page 33
14. Specialised dressings
14.1 Honey (e.g. Activon)Antibacterial properties of honey and its potential in the treatment of wounds has beenextensively reviewed by Molan (1992 and 1999.) The mechanisms by which honeyinfluences the wound healing process are currently incompletely understood. (Tonks et al2001)
Molan (2005) recommend honey to treat all aspects of wound healing, stating that honeyhas:● Anti-inflammatory properties● Clearance of infection● Deodorising action● Barrier function● Provision of the optimum moist healing environment● Debriding action
For the properties of honey to be most effective within healing, honey needs to be incontact with the wound bed continuously, when the honey has absorbed into the woundbed the dressing needs to be re-applied.
It is essential that a date be set for reassessment of the wound and that any changes intreatment following reassessment should be recorded.
14.2 LarvE therapyLarvE are sterile maggots of the green bottle fly Lucillia sericata and have been found tohave a use in cleansing and deodorising wounds that are infected or have devitalisedtissue. The Larvae produce powerful proteolytic enzymes that breakdown sloughy ornecrotic wound tissue, which is ingested as a source of nutrient.
Guidelines for use● Supplied in sterile containers (LarvE) or sterile nets (Biofoam)● Suitable for a variety of wounds, pressure ulcers, leg ulcers, and diabetic foot ulcers● Can be used to prepare a wound for grafting● Ensure the correct number of pots, or correct size of Biofoam is ordered by using the
LarvE calculator● Although the maggots remain on the wound for a maximum of 5 days a daily secondary
dressing is required this should be changed daily and maggots checked for viability.● A hydrocolloid should be prescribed, as this will protect the surrounding skin. If using
Biofoam then a cream e.g. Sudocrem is used to protect the skin● Maggots are removed from the wound by irrigation, removing any remaining maggots
with forceps or simply remove the Biofoam.
Page 34
● Any hydrogel used prior to larvae therapy must be completely removed from the woundas it kills the maggots by suffocation
● Should only be used by practitioners who have received training in the use of maggots● Refer to local policy for more details re use of maggots
Contra indications● Caution should be used if wounds have a tendency to bleed● Caution should be used for patients currently on anticoagulants, e.g. warfarin● Caution should be used if wounds have a sinus or fistula● LarvE should never be used on wounds that lie in close proximity to large blood vessels● Increased levels of pain have been reported when used on ischaemic feet
14.3 Protease modulating matrix (e.g. Promogran)Promogran matrix is made from a freeze dried mixture of 45% ORC (oxidised regeneratedcellulose) and 55% bovine collagen. Promogran is able to re-balance and modulate thepathological wound environment in all chronic wounds. Excess proteases are inactivated,whilst endogenous growth factors are protected simultaneously. On absorption ofPromogran into the wound the proteases remain inactivated and growth factors arereleased active back into the wound. Thus Promogran creates a favourable healingenvironment.
Guidelines for use● Lightly apply to wound bed, to fit shape of wound● Promogran absorbs into the wound● The wound should be clinically free from infection● Irrigate to cleanse wound if needed● The wound may appear sloughy if Promogran has not fully absorbed into the wound bed.● Change daily or alternate days● Will need a secondary dressing● May increase wound exudateNB: Contains collagen of bovine origin.
14.4 Capillary dressing (e.g. Vacutex)VACUTEX is a 3 mm layered ‘sandwich’ dressing. The layers of the dressing ‘pull’interstitial fluid from the wound and place it within the central layer until saturation when itmoves to the third outer layer. VACUTEX can be used on infected or heavily exudatingwounds such as venous ulcers, pressure ulcers, burns, fungating wounds, stoma sites,cavity wounds and non-healing wounds. It is available in a range of sizes and can betailored to suit each wound requirement individually.
Guidelines for use● Can be used on wet or dry wounds● Can be layered to absorb exudate
Page 35
● When used on dry wounds needs occluding with a film dressing● Must be cut to sizeContra indications● Do not use on bleeding wounds● Caution should be used for patients currently on anticoagulants, e.g. warfarin
14.5 Topical Negative Pressure (e.g. Vacuum assisted closure.VAC)
This device assists in wound closure by applying localised, topical negative pressure todraw the edges of the wound to the centre.
Topical negative pressure is applied to a foam or gauze dressing positioned in the woundcavity or over the flap or graft. The foam/gauze dressing helps remove fluid from the woundand stimulate the growth of healthy granulation tissue.
Topical negative pressure devices are only to be used following advice from surgeons orTissue Viability Nurses.NB: Refer to local policy/manufacturers guidelines for more details regarding the useof Topical Negative Pressure
14.6 Deodorising dressings (e.g. Carboflex)Most deodorising dressings are made up of activated charcoal. There are reasons thatwounds become malodorous and a thorough wound assessment should be undertaken todetermine the cause of the odour.
Guidelines for use● Can be used in conjunction with other dressings● Can be combined with metronidazole gel for wounds colonised with anaerobic bacteria,
however this should be for a short period only● Can be used on malignant fungating wounds● Can be used on infected wounds; however the patient requires systemic antibiotic
therapy and daily dressing change. (Morgan 2000)● Deodorising dressings should be used as a primary dressing. However they may stick to
the wound bed, therefore the use of a non-adherant dressing is advised.
Page 36
15. Challenging wounds
15.1 Over-granulating woundsOvergranulation is excessive granulation tissue, which stands proud of the rest of the skin.It poses a problem as it prevents epithelial cells from migrating across the wound surface.Suggested treatment in order of preference:1. Foam dressings have been found to reduce the level of overgranulation but need to
maintain contact with the wound surface. If not self adhesive they should be securedaround the edges to prevent movement and to maintain contact without limiting thedressings evaporation qualities. They should not be occluded with a secondarydressing or tape.
2. Mild Topical Corticosteroids (1% hydrocortisone) have been used to reduceovergranulation but the evidence for this is limited. They should be applied daily for amaximum of 7 days and will require a secondary dressing. It should be noted by thepractitioner that overgranulation is unlikely to be a licensed indication, even though 1%hydrocortisone is used widely.
3. Silver nitrate sticks – are not recommended as best practice and should only beconsidered when all other options have failed to reduce the overgranulation. They havea caustic effect and destroy overgranulation tissue efficiently but they also damagehealthy tissue. Care must be taken with application. Therefore apply yellow soft paraffintype product around the wound edges to protect. Use should only be after fullconsultation with medical practitioner responsible for that aspect of the patient’s care.
NB: Please refer to National Patient Safety Agency (NPSA) website regarding use offlammable products i.e. Yellow soft paraffin.
15.2 Fungating wounds:Fungating wounds occur when a cancerous mass invades the epithelium thus ulceratingthrough to the body surface (Dealey 2000). The common symptoms of a fungating woundare malodour, copious exudate, pain, and bleeding. If surgical intervention is notappropriate or healing is an unlikely outcome, the treatment objective is palliative and thecare should focus on symptom control. The objective of the dressing is not to promote ahealing environment but to promote comfort and manage the symptoms efficiently.Metronidazole gel has antibiotic properties and is useful in the palliative treatment ofmalodorous, malignant wounds.
15.3 BurnsBurns are traumatic wounds caused by excessive heat or cold, which damages the tissueto varying degrees. When considering the management of burns, the extent of the injurymust be defined as the treatment varies drastically. The treatment of minor burns isdependant on the condition of the wound bed and should be managed as any other wound.
Page 37
Burns are susceptible to infection and often antimicrobials are used prophylactically.(Dealey 2000)
NB: Staff in Mid Yorkshire Hospitals Trust should refer to burn management pathway andpolicy for more details regarding management of thermal injuries.
15.4 Ischaemic/vascular woundsThe toes and sometimes the foot can be affected by so called “dry gangrene” in chronicarterial insufficiency. The tissues are black, shrivelled and dry. Whilst it is traditionally calledgangrene there is in fact no infective process. The tissues are undergoing spontaneousbreakdown and drying. It is a form of mummification. It is important that such areas, unlikeother wounds, are kept dry. Introducing moisture carries the risk of infection. Ideally thearea should be left exposed to the air. A non adherent dressing to separate toes is useful. Ifa dressing is required it should be light, dry and allowing the circulation of air.
Page 38
16. ReferencesAmerican Diabetes Association (2003) Peripheral arterial disease in people with diabetes.Diabetes Care 26(12): 3333–4Bennett, NT and Schultz, GS Growth factors and wound healing: biochemical properties ofgrowth factors and their receptors. American Journal of Surgery 165: 728-737 (1993);Cherry, G and Harding, K (1997). Management of wound exudate. London : Churchill.Cooper, R and Lawrence, J. (1996) The Isolation & Identification of bacteria from wounds.Journal of Wound Care S: 7 335-40.Cutting, K (1990) Wound Cleansing. Surgical Nurse. 3(3) 4-8Collins, N. (2001) Protein and wound healing. Adv skin wound care 14; 6. 288-89Dealey, C. (2000) The Care of Wounds London: Blackwell ScienceDealey, C. (2004). The Care of Wounds. Oxford : Blackwell ScienceFlanagan, M. (1997) Wound Management Churchill Livingstone: New Yorkwww.bapen.org.uk/pdfs/must/must_page1.pdf.Huovinen, S. Kotilainnen, P. Jarvinen, H. (1994) Comparison of Ciprofloxacin orTrimethoprim Therapy for Venous Leg Ulcers. Journal of American Academy ofDermatology 31: 279-81Miler, M (1994) Wound Cleansing/A Matter of Choice. Nursing Standard Supplement9(S2)/7Morgan, D (2000). Formulary of Wound Management Products (8th Ed) UromedCommunications Ltd.Morison, M J (1992). A colour guide to the nursing management of wounds. London : WolfePublishingMclaren, S M G (1992) Nutrition and wound healing. J Wound Care 1.3.44-55Molan, P. (2005) Honey A modern wound management product. Wounds UK LtdNICE (2011) National Institute for Health and Clinical Excellence: Diabetic Foot Problems,London UK.Penzer, R Burr, S (2005). Promoting skin health. Nursing Standard 19 (36) : 57-65Surrey, Morison M, (1987) Wound Assess, Professional Nurse, 3 (10) 315-317Todorovic, V. (2002) Food and wounds: Nutritional factors in wound healing and formation.Brit J Comm Nurs: 43 – 53Vowden, K Vowden, P (1998). Venous leg ulcers part 2 : Assessment. Professional Nurse13 (9) : 633-638Wells, Nancy. Pasero, Chris McCaffery, Margo. (2008) Improving the Quality of CareThrough Pain Assessment and Management. Patient Safety and Quality: An EvidenceBased Handbook for Nurses#Wounds UK (2010) Best Practice Statement: The use of topical antiseptic/antimicrobial agentsin wound management. Wounds UK, Aberdeen, 2010.
Page 39
17. Glossary of TermsAngiogenesis: The generation of new blood vessels in tissues
Autolysis: The body’s natural ability to debride dead tissue. Softening of dead cellsbrought about by enzymes in the cells themselves.
Collagen: The main protein constituent of white fibrous tissue
Cellulitis: A spreading infection into soft tissue.
Colonisation: Multiplication of organisms without a corresponding host reaction
Contamination: Presence of micro organism but without multiplication
Contraction: A function of the healing process in granulating tissue whereby edges ofthe wound are drawn towards each other
Debridement: The removal of devitalised tissue and foreign matter
Eczema: Originates from the Greek word ‘to boil over’. Features dry, itching, redand inflamed skin. The words eczema and dermatitis are synonymous.It affects 1 in 10 people in the United Kingdom it can be mild moderateor severe.
Epidermis The outer layer of the skin, which forms a protective covering of thebody. Comprising five layers, the epidermis constantly renews itself,with the bottom or germinative layer producing new cells and the toplayer, stratum corneum, made up of dead cells which regularly worn off.
Epithelium Is the tissue that covers the body surface, lines body cavities and formsglands
Epithelialisation The final stage of the proliferative stage of tissue healing
Erythema Redness of the skin due to hyperaemia
Eschar A scab consisting of dried serum and devitalised dermal cells
Fibroblast An immune collagen producing cell of connective tissue
Granulation: The formation of new tissue filling the defect which takes place during,the proliferation phase of healing. The name is derived from the fact thatthe buds of new tissue take on the appearance of small granules.
Granulations: Small masses of formative cells containing loops of newly formed blood-vessels which spring up over any raw surface, as the first step in theprocess of healing of wounds.
Haemostasis: The termination of bleeding by mechanical or chemical means or by thecomplex coagulation process of the body, consisting of vasoconstriction,platelet aggregation, thrombin and fibrin synthesis.
Infection: Micro-organisms are not only present but are multiplying and producingan associated host reaction. This may take various forms.
Page 40
Maceration: A softening or sogginess of the tissue owing to retention of excessivemoisture. Often showing as white wet tissue.
Necrosis: The local death of tissue. The tissue is often black /brown in colour and‘leathery ‘in texture
Oedema: The abnormal accumulation of fluid beneath the skin, or in one or morecavities in the body.
Pathogenic: Disease-producing, and is a term for example, applied to bacteria,capable of causing disease
Slough: Devitalised tissue which has a yellow/white/grey hue.
Vasoconstriction Narrowing of the blood vessels which results in the blood flow to aparticular part of the body being reduced. Cold will causevasoconstriction of the vessels under the skin, reducing heat loss andshock due to injury or blood loss





























