-
7/25/2019 Wound Care Module
1/29
WOUND CARE MODULE
-
7/25/2019 Wound Care Module
2/29
2
1Introduct ion
........................................................................................................................................................4
1.1 What is Wound
Care?......................................................................................................................................4
1.2 What is a wound and what are the different types of
wounds?.......................................................................4
1.3 Common types of
wounds...............................................................................................................................4
2General overview of wounds
............................................................................................................................5
2.1 Complex and chronic
wounds..........................................................................................................................52.1.1Acute
wounds..........................................................................................................................................52.1.2Chronic
wounds
......................................................................................................................................5
3Healing
................................................................................................................................................................6
3.1 How does the body heal?
................................................................................................................................6
3.2 Phases of
Healing............................................................................................................................................63.2.1The
inflammatory phase
.........................................................................................................................63.2.2The
proliferative
phase............................................................................................................................63.2.3The
maturation phase
.............................................................................................................................7
3.3 Moist wound
management...............................................................................................................................7
3.4 Control Factors Affecting
Healing....................................................................................................................83.4.1Intrinsic
factors
........................................................................................................................................8
3.4.1.1 Health
status..............................................................................................................................83.4.1.2
Immune function
........................................................................................................................83.4.1.3
Diabetes.....................................................................................................................................83.4.1.4
Age
factors.................................................................................................................................83.4.1.5
Body build
..................................................................................................................................83.4.1.6
Nutritional status
........................................................................................................................8
3.4.2Extrinsic
factors.......................................................................................................................................93.4.2.1
Mechanical stress
......................................................................................................................9
3.4.2.2
Debris.........................................................................................................................................9
3.4.2.3
Temperature
..............................................................................................................................9
3.4.2.4 Desiccation
................................................................................................................................93.4.2.5
Maceration
.................................................................................................................................93.4.2.6
Infection
.....................................................................................................................................93.4.2.7
Chemical stress
.........................................................................................................................93.4.2.8
Other factors
............................................................................................................................10
3.4.2.8.1 Systemic medications
.........................................................................................................103.4.2.8.2
Lifestyle...............................................................................................................................103.4.2.8.2.1
Alcohol
............................................................................................................................103.4.2.8.2.2
Smoking..........................................................................................................................10
4Wounds
.............................................................................................................................................................11
4.1
Chronic Wounds
............................................................................................................................................11
4.1.1Leg
ulcers..............................................................................................................................................114.1.2Venous
ulcers
.......................................................................................................................................11
4.1.2.1 General features of venous
ulcers...........................................................................................114.1.3Ischaemia,
or arterial
ulcers..................................................................................................................11
4.1.3.1 General features of arterial ulcers
...........................................................................................114.1.4Venous/Arterial
(Mixed Ulcers)
.............................................................................................................124.1.5Other
causes of ulcers
..........................................................................................................................124.1.6The
Diabetic
..........................................................................................................................................12
4.1.6.1 How does diabetes affect wound healing?
..............................................................................124.1.6.2
Risk factors in
diabetes............................................................................................................13
4.1.6.2.1 Peripheral Vascular Disease
..............................................................................................134.1.6.2.2
Peripheral
Neuropathy........................................................................................................13
4.1.6.2.3
Callus
Formation.................................................................................................................13
4.1.6.2.4 Limited Joint Mobility
..........................................................................................................134.1.6.2.5
Bony Deformity
...................................................................................................................13
4.1.7Pressure
Ulcers.....................................................................................................................................13
-
7/25/2019 Wound Care Module
3/29
3
4.1.7.1 Pressure
...................................................................................................................................134.1.7.2
Friction
.....................................................................................................................................144.1.7.3
Shearing
forces........................................................................................................................14
5Wound Dressings and
Bandages...................................................................................................................15
5.1 Wound pharmaceuticals / Wound healing product classification
..................................................................15
5.2 Passive
dressings..........................................................................................................................................155.2.1A
modern inert dressing
........................................................................................................................155.2.2The
non-absorbent passive dressings
..................................................................................................15
5.3 Interactive
dressings......................................................................................................................................165.3.1Non-Absorbing
dressings......................................................................................................................16
5.3.1.1 Film Dressings (for wounds with no to low exudate)
...............................................................165.3.2Absorbing
dressings
............................................................................................................................17
5.3.2.1 Hydrocolloid dressings (for wounds with low to moderate
exudate) .......................................175.3.2.2 Foam
dressings (for wounds with medium to high exudate)
...................................................185.3.2.3
Alginate dressings (for wounds with medium to high exudate)
...............................................195.3.2.4 Hydrofibre
dressings................................................................................................................205.3.2.5
Hydroactive dressings (for wounds with medium to high exudate)
.........................................205.3.2.6 Hydrogels ( For
dry or sloughy wounds )
.................................................................................21
5.3.3Miscellaneous
dressings.......................................................................................................................22
5.3.3.1 Cadexomer Iodine Dressings (e.g. Iodosorb)
......................................................................225.3.3.2
Silver
........................................................................................................................................22
5.4 General rules for the topical use of
antiseptics..............................................................................................22
5.5 Hypertonic
Saline...........................................................................................................................................23
5.6 New burn
dressings.......................................................................................................................................23
5.7 Keloid and Hypertrophic Scar Management
..................................................................................................24
5.8
Bandages.......................................................................................................................................................245.8.1Retention
Bandages..............................................................................................................................245.8.2Support
Bandages..................................................................................................................................245.8.3Compression
Bandages........................................................................................................................24
5.8.3.1 High stretch compression bandages
.......................................................................................255.8.3.2
Short stretch
bandages............................................................................................................255.8.3.3
The hazards of compression
bandages...................................................................................25
5.8.4Zinc paste
bandages.............................................................................................................................26
6General rules
....................................................................................................................................................27
6.1 Acute wounds
................................................................................................................................................27
6.2 Chronic
wounds.............................................................................................................................................27
6.3 Protocol for wound management of skin tears
..............................................................................................27
6.4 Difficult wounds (i.e. animal or insects
bites).................................................................................................27
6.5 Post operative wounds
..................................................................................................................................28
6.6
Burns..............................................................................................................................................................28
7References........................................................................................................................................................29
ACKNOWLEDGEMENT
The development and production of the wound resources by Geoff
Sussman, Director Wound Research Wound
Foundation of Australia is acknowledged.
-
7/25/2019 Wound Care Module
4/29
1 Introduction
4
1.1
1.2
1.3
What is Wound Care?
Wound care is the provision of the appropriate environment for
healing by both direct and indirectmethods together with the
prevention of skin breakdown1. In other words wound care means
morethan just putting a dressing onto a wound. It means looking
into patients general health, lifestyle andfactors that might slow
healing down.
What is a wound and what are the different types of wounds?
A wound is a physical injury to the body consisting of a
laceration or breaking of the skin or mucousmembrane, or an opening
made in the skin or a membrane of the body incidental to a
surgicaloperation or procedure.
Wounds may be acute or chronic trauma resulting from an injury
where, because of a number offactors, the injury does not heal.
Acute wounds may be a planned or unplanned event, and
healingtypically proceeds in an orderly and timely fashion.
Examples of acute wounds include a cut, graze orburn. Examples of
chronic wounds include leg ulcers, pressure wounds and diabetic
wounds.
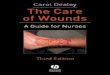
Common types of wounds
BLACK NECROTIC WOUNDYELLOW NECROTIC WOUNDWITH HIGH EXUDATE
YELLOW NECROTIC WOUNDWITH LOW EXUDATE
CAVITY WOUND WITH HIGHEXUDATE
EXUDATING WOUND WITH
SLOUGH AND CLINICAL SIGNS
OF INFECTION
SUPERFICIAL WOUND WITH
CLINICAL SIGNS OF INFECTION
SUPERFICIAL GRANULATING
WOUND WITH HIGH EXUDATE
SUPERFICIAL GRANULATING
WOUND WITH LOW EXUDATE
MALODOROUS WOUNDS
CAVITY WOUND WITH LOW
EXUDATE
EPITHELIALISING WOUNDS SKIN TEARS
-
7/25/2019 Wound Care Module
5/29
5
2.1
2 General overview of wounds
Complex and chronic wounds
A large proportion of wounds seen in clinical practice are
chronic in nature. The epidemiologicalstudies indicate that one
percent of the population has a chronic wound, and of that group
sometwenty percent have had the wound for more than two years. More
studies indicate that the level of
chronic wounds in older patients is considerably higher than
that percentage
2
.Chronic wounds may be classified into the following groups:
Leg ulcers
Pressure wounds
Post-operative wounds
Neoplasia (Cancer)
Chronic infected wounds
Diabetic wounds
The difficulty in the management of any chronic wound is that
there is always an underlyingphysiological cause of the wound which
must be treated, but many patients have multi-factorialissues and
co-morbidities. For best results the basic cause of the problem
must be addressed, andany negative factors altered.
It must be understood that some patients may never heal due to
the basic pathophysiology of thedisease process and our inability
to alter some or all of the major factors influencing the
non-healingof the wound. However, even in the most extreme cases,
good wound care can be a great help inminimising the worst effects
of such chronic wounds.
2.1.1 Acute wounds
Acute wounds may show some of the following characteristics:
higher risk of infection due to debris contaminating the
wound
inflammation occurs
may heal by primary intention
may require antiseptic use
2.1.2 Chronic wounds
Chronic wounds may show the following characteristics:
lower risk of infection
symptom of underlying condition
heal by secondary intention
may be sloughy and moist, or dry and scabby.
-
7/25/2019 Wound Care Module
6/29
6
3.1
3.2
3 Healing
How does the body heal?
There are three phases of wound healing
inflammatory (destructive)
proliferative (regenerative)
maturation (reparative)
During all of these phases there are a number of cells that are
essential to the process of the healingincluding platelets,
neutrophils, macrophages and fibroblasts.
Some of the cells which you may think are only present for one
particular phase of the healingprocess are there from the very
beginning of the wound, through to the ultimate healing of the
wound.
The critical thing is that the phases of healing are a
continuum. Each phase continues in a steadyprocess merging with the
next phase. In fact, one wound may be in more than one phase at
onetime.
Phases of Healing
3.2.1 The inf lammatory phase
The inflammatory phase is normally the shortest, and is manifest
at the beginning of the wound itselfwhere a wound is either
surgically created, caused by trauma or some other reason. There
will bebleeding, and a clot will develop to induce haemostasis
(clotting). The tissue around the wound mayoften be red, hot, sore
and swollen. This does not indicate infection, it is merely the
inflammatoryprocess itself and, consequently, it is not always
necessary to apply topical antiseptics or topicalantibiotics. Wound
exudate is often copious during the inflammatory phase. It is not a
passivecomponent of the healing process, but serves to nourish the
tissues and to flush out necrotic tissueand foreign debris from the
wound. The inflammatory phase uses the exudate as a support
mediumfor enzymes, antibodies and the various cells necessary for
wound cleansing. Exudate also contains
a number of growth factors produced by the body which are
critical in the promotion of healing. If theinflammatory phase is
impaired, wound healing may be slowed or halted. The continued
presence offoreign material, necrotic tissue, excessive
antimicrobial use or other continued disruption of thewound can
result in prolonged inflammation thereby preventing the onset of
proliferation andmaturation. In turn, this may lead to fibrosed
tissue. Some of the factors that will affect theinflammatory phase
include continued tissue destruction due to pressure not being
relieved, drynessand desiccation, poor blood supply, clinical
infection, or thermal shock during the inflammatoryphase. The most
important cells are the platelets whose task is not only
haemostasis, but also theproduction of a growth factor which is
important in stimulating the healing process.
During this phase the destruction of non-viable tissue and
bacteria occurs. Neutrophils are involvedin phagocytosis (killing)
of bacteria as well as aiding in the extra-cellular release of
protease - an
enzyme used by the body for the destruction of necrotic tissue.
The macrophages that are involved inphagocytosis of micro-organisms
and necrotic tissue also release a growth factor important in
thehealing cascade.
3.2.2 The proli ferative phase
During this phase the new vascular bed is formed by
angio-genesis. Capillary buds are formed whichlink up with the
existing capillary network and allow oxygenated blood to provide a
lush bed ofcapillary vessels. During the proliferative phase
collagen is deposited by the fibroblasts. Collagen isthe essential
framework for the connective tissue which will eventually fill the
wound. Fibroblasts alsosynthesise proteoglycans, or ground
substance. It is collagen and ground substance which form
thescaffolding for wound repair. Collagen is laid down in a wound
over a period of weeks, after which
time no new collagen is produced. The fibroblasts produce
enzymes which help break down thecollagen.
The collagen then realigns itself by cross-linking, resulting in
tensile strength in the wound. There area number of elements
essential for collagen production and deposition including vitamin
C, oxygen,
-
7/25/2019 Wound Care Module
7/29
7
3.3
iron and zinc. A deficiency in these nutrients could lead to the
development of a weakly bondedmatrix, and ultimately to dehiscence
of the wound.
During the proliferative phase, wound contraction occurs. This
is an action of the myofibroblasts,contractile cells which pull the
wound margins together. Contraction and granulation are
theprocesses by which the wound becomes smaller. During the latter
stage of the proliferative phase,epithelialisation occurs. This
involves the growth of the epidermal cells over the surface of
thegranulation tissue, a process which is completed most
efficiently in a moist, clean environment.
3.2.3 The maturation phase
The maturation phase is the final stage of healing. During this
stage the fibroblasts decrease innumber, vascularisation decreases,
and the tensile strength of the wound increases. Maturation isthe
most misunderstood phase of healing. It is assumed that a wound is
healing once the epitheliumhas closed the surface of the wound.
Tensile strength of the wound may in fact take quite aconsiderable
time to develop, and in some patients it can take up to twelve
months. It is oftenincorrect to view a re-ephithelialised wound and
think that the wound is totally healed beneath thesurface. The lack
of tensile strength in a wound will increase the risk of breakdown
that may berelated to tension of the tissue below the surface.
Moist wound management
Knowledge and understanding of wounds, tissue and healing have
grown rapidly over the past 40years, resulting in a major change in
the method of wound management. There has been a growingawareness
that traditional wound-care products do little to aid healing, and
in many cases actuallydelay it.
Traditional theory has always been that wounds should be kept
clean and dry so that a scab mayform over the wound, the wounds
should be exposed to the air and sunlight as much as possible,and
where tissue loss is present, the wound should be packed to prevent
surface closure before thecavity is filled, and then the wound
should be covered with a dry dressing.
The clear disadvantages of these principles are that the scab,
which is made up of the dehydratedexudate and dying dermis, is a
physical barrier to healing, which is then delayed because the
epidermal cells cannot move through the scab formed. This may
ultimately lead to a poor cosmeticresult, even scarring. Exposure
to the air reduces the surface temperature of the wound
causingperipheral vasoconstriction affecting the flow of blood to
the wound which further delays healing. Thisreduced blood flow will
also effect the supply of oxygen, nutrition and other factors to
the wound. Airexposure will also cause the wound to desiccate and
form a scab.
Where a wound is packed with dry gauze, the quality of healing
is impaired due to adhesion of thematerial to the surface of the
wound, causing it to dry out. Equally, covering the wound with a
drydressing that adheres to the wound may traumatize the wound
surface on removal. Wounds coveredby an occlusive dressing do not
form a scab, so epidermal cells are able to move rapidly over
thesurface of the dermis through the exudate which collects at the
wound/dressing interface. Theapplication of a totally occlusive or
semi-permeable dressing to the wound can also prevent
secondary damage as a result of dehydration.Dr George D Winter,
in his work Formation of the scab and the rate of epithelialization
of superficialwounds in the skin of young domestic pigs'(Nature,
1962)3was able to demonstrate scientifically thedifference between
wounds of a similar nature when healing was open to the air, and
when healingwas under occlusive dressing. Winter's work was to
inflict artificial wounds on young domestic pigs,with fifty percent
of the wounds occluded and fifty percent of the wounds open to the
air. They werereviewed on a regular basis, and samples taken of
both types of wounds which were then examinedmicroscopically. The
experiment showed that the wounds healing under moist conditions
healed fiftypercent faster than the wounds healing under dry
conditions, open to the air. Winters work has sinceformed the basis
of the principles of modern moist wound management. Many subsequent
studieshave confirmed the theory that wounds heal faster in a moist
environment compared to a dry
environment.Moist wound healing also simplifies cleaning by
assisting with the autolytic debridement of wounds. Itfacilitates
wound cleansing, since the wound exudate is part of the healing
cascade, and also
-
7/25/2019 Wound Care Module
8/29
8
3.4
protects granulation and encourages epithelialization. Exudate
has now been shown to carry anumber of growth factors essential to
the healing of wounds.
Control Factors Affecting Healing
Most wounds heal readily whereas others are slow or remain
unhealed for a considerable length oftime. There are a number of
factors which affect the healing of a wound, and these factors are
both
intrinsic and extrinsic.
3.4.1 Intrinsic factors
health status
immune function
diabetes
age factors
body build
nutritional status.
3.4.1.1 Health status
Good circulation, both arterial and venous, is essential for
good wound healing. Anaemia, regardlessof type, reduces the
capacity of the blood to provide oxygen to the tissues, since
haemoglobintransports oxygen to the cells.
3.4.1.2 Immune function
Normal immune system function is required for the inflammatory
phase of healing. A reduction inimmune function slows the cleansing
of the wound bed and reduces the ability of the body to
fightinvading pathogens (This is likely to be due to a reduction of
the number and activity of the whiteblood cells).
3.4.1.3 Diabetes
Diabetes is one of the major problems for chronic wounds.
Diabetics have a delayed capillaryresponse to injury, reduced
cellular function at the injury site, and defects in collagen
synthesis andwound strength. Hyperglycaemia (caused by reduced
insulin availability and increased insulinresistance) appears to be
a major predisposing factor in delaying healing in diabetic
patients andincreasing the rate of infection.
3.4.1.4 Age factors
As we age our skin and tissues change. We lose the sensory
cells, as well as the secretory cellswhich are so essential for the
maintenance of skin moisture and flexibility. We lose the
vasculaturewithin the skin, and hair follicles. The skin becomes
thinner, dryer, and far more prone to destruction-
whether by physical or by chemical means.
3.4.1.5 Body build
Because of the adipose tissue being poorly vascularised, an
obese patient will have a great deal oftrouble healing due to the
inability to deliver oxygen and nutrients to the wound site.
Underweightindividuals may also experience difficulties in the
healing process.
3.4.1.6 Nutritional status
Nutrition is one of the most important factors in the healing of
wounds. Proteins, carbohydrates, fats,vitamins, trace elements and
fluids all play a vital role in wound repair. Research has shown
thatamino acids (eg. Arginine), when given as a supplement, will
improve the rate of wound healing.
-
7/25/2019 Wound Care Module
9/29
9
3.4.2 Extrinsic factors
mechanical stress
debris
temperature
desiccation / maceration
infection
chemical stress
other factors.
3.4.2.1 Mechanical stress
When a patient is immobile and pressure is exerted locally,
especially over a bony prominence, formore than two hours, at a
pressure exceeding 30 mm of mercury, localised microvascular
ischaemiawill occur. This will ultimately lead to tissue
destruction both at the surface and deeper into thewound-leading
eventually to a pressure ulcer. Equally, shearing forces and
friction occur when thetissue below the skin is forced to move
while the skin itself is restrained by contact to a surface,
such
as the bed sheet. This is particularly evident in the patients
heels.3.4.2.2 Debris
Debris-whether slough, eschar, scab, wound dressing residue,
gauze fibres or sutures- will impedewound healing. Their presence
will prolong the inflammatory phase, as well as predisposing
thewound to infection. Debris should be removed, either surgically
or by the use of hydrogels, proteolyticenzymes or
hydrocolloids.
3.4.2.3 Temperature
The optimum temperature for the growth of human cells is 37
degrees centigrade. It is thereforeessential to maintain the wound
environment at body temperature. A drop in body temperature
willlead to peripheral vasoconstriction- affecting the flow of
blood through the wound- and it will markedly
reduce the activity of growth factors and proteases. Increased
body temperature can lead tochanges at the wound site increasing
the risk of cellular breakdown and limiting the healing
process.
3.4.2.4 Desiccation
If a wound dries, healing is either delayed, or will cease.
Exposed, dry wounds are more inflamed,painful, itchy, and have more
scab material during the early stages of wound healing.
3.4.2.5 Maceration
Maceration may be due to incontinence, perspiration or excessive
exudation. Maceration will causethe destruction of tissue and slow
the healing process. It is essential to maintain the
moistenvironment without excessive exudation.
3.4.2.6 InfectionAll wounds will have some level of bacterial
colonisation, however, this does not mean that thewound is
infected. The presence of erythema, discharge, fever, pain with
elevated white blood cellcount, and sometimes odour, is evidence
that the wound is infected. If clinical signs of infection
arepresent, the use of systemic antibiotics is mandatory. If there
are no clinical signs of infection there islittle reason to use
either systemic or topical antibiotics. An exception to this may be
the use of veryspecific topical antibiotics in very specific cases
to reduce the level of bacteria in wounds ofcompromised patients
(eg. the use of topical metronidazole in anaerobic colonised
wounds).
3.4.2.7 Chemical stress
Iodine, peroxide, chlorhexidine, alcohols, hypochlorites and
acetic acid are commonly used
antiseptics and cleansing agents. Use of these agents is often
responsible for delayed healing, sincethey are non-selective in
their activity and will kill healthy cells as well as bacteria. It
is preferable toavoid the prolonged use of these products on a
granulating wound. Even their use in infected woundsis somewhat
dubious, as research has shown that although they may reduce the
surface load of
-
7/25/2019 Wound Care Module
10/29
10
bacteria in an infected wound, they do not penetrate below the
surface and therefore have no realeffect on the infection in the
tissue itself4. They may be of use in dilute forms when applied to
somechronic wounds and left in place for no more than five minutes
and then washed off.
3.4.2.8 Other factors
3.4.2.8.1 Systemic medications
The effects of systemic medications on the healing wound vary
greatly. We commonly see medicines
prescribed for a condition which is unrelated to the wound, but
may have side effects which couldeither inhibit or stimulate
healing. Medications can therefore be divided into two groups;
thestimulatory drugs and the inhibitory drugs. The stimulatory
drugs affect the inflammatory response,epithelialisation,
fibroblast activity, fibrinolysis, and cell stimulation, whereas
the inhibitorymedications affect tensile strength, cell activity,
capillary proliferation, and fibroplasia.
3.4.2.8.2 Lifestyle
3.4.2.8.2.1 Alcohol
Excessive and/or chronic alcohol intake can lead to health
problems affecting wound healing.Alcohol-induced digestive problems
may lead to malnutrition and anaemia. Liver damage can result
in chronic disturbances due to a reduction in platelet levels,
and subsequent circulatory damage thatmay reduce the blood flow
that is required for wound healing.
3.4.2.8.2.2 Smoking
The adverse effects of smoking and the potentiation of cancer in
various parts of the body have beenunderstood for many years.
However, it is clear that the toxic constituents of smoking such
asnicotine, carbon monoxide and cyanide have a dramatic and
inhibiting effect on healing. Nicotine willdiminish red blood
cells, fibroblasts and macrophages, and increase platelet
adhesiveness. This willproduce cutaneous vasoconstriction. Carbon
monoxide has an affinity for haemoglobin 200 timesgreater than that
of oxygen. This will have a major effect on the oxygen-carrying
capacity of the bloodand may potentially lead to ischaemia.
Hydrogen cyanide inhibits the enzyme-systems necessary for
oxygen transport at the cellular level, as well as oxidative
metabolism. Smoking can therefore be amajor cause of the
non-healing of wounds.
-
7/25/2019 Wound Care Module
11/29
11
4.1
4 Wounds
Chronic Wounds
4.1.1 Leg ulcers
Leg ulcers have a number of different causes, including venous
insufficiency, arterial disease,
diabetes mellitus, vascular complication of auto-immune disease
(such as rheumatoid arthritis),malignant disease and trauma.
4.1.2 Venous ulcers
Venous ulcers result from the breakdown of the venous
circulation of the leg, and are an associationof the inability of
the leg to force the passage of blood through the various
connecting veins via thebicuspid valves by muscular contraction.
Deep veins are supported by thick connective tissue andtheir
surrounding muscle masses. Superficial veins dilate easily under
sustained back pressure.Communicating veins connect the two
systems. Valves, usually bicuspid, are found in all threesystems
and they may become damaged, thickened or may degenerate with age.
Thrombosis cancause their destruction.
4.1.2.1 General features of venous ulcers
They are most often found in the lower 1/3 of leg (in the gaiter
area) are usually irregular in shape,may not be painful, and oedema
is often present. The skin is often stained around the ulcer area
dueto haemosiderin deposition. Part of the underlying cause is past
fractures or trauma with a possiblesilent deep vein thrombosis
(DVT). Skin changes such as eczema and atrophy blanche
(whitestippled scars on the skin) are often present, and ankle
flare, distended small veins on the medialaspect of the foot are
seen and there is a history of varicose veins. The main feature is
a lack ofvenous return caused by a malfunction of the valve system
either in the deep or the peripheralsystem. There is often a
history of obesity, past DVT, and/or poor mobility resulting in
venous stasis.Venous leg ulcers are usually painless, irregular in
shape, and may have copious exudate.
The treatment for Venous Incompetence includes surgery in some
cases, however, the main stay oftreatment is the application of
compression therapy- toe to knee 30-40mmHg at ankle. It is,
however,essential to exclude arterial involvement. Exercise should
be encouraged and occupational factorssuch as long periods of
standing which leads to venous stasis, should be avoided.
4.1.3 Ischaemia, or arterial ulcers
The death of skin automatically follows occlusion of its
arterial blood supply unless this occlusion isgradual enough to
allow a collateral blood supply to be established. Atheroma
(thickening) is themost common cause of arterial ulcers of an
ischaemic nature. The loss of arterial circulation may bedue to
extramural strangulation. Scar tissue or other factors may cause
strangulation of thearterioles, or fibrosis resulting from
longstanding, chronic oedema. Chronic infection may also
obstruct arterial flow. Arterial ulcers can result from mural
and intramural changes to the vesselwalls:
Mural changes: Atherosclerosis, or plaque formation reduces the
blood flow until thrombosis,embolism or infection cause complete
closure.
Intramural changes: Occlusion of small vessels by changes in
blood viscosity, plateletadhesiveness or fibrinogenesis,
(especially in small painful ulcers of the feet and ankles).
4.1.3.1 General features of arterial ulcers
Arterial ulcers are very painful, especially at night. This is
as marked in small ulcers as in largerulcers. Their edges are
sharply defined, and the ulcer is 'punched out'. The base is often
coveredwith slough, which may deepen to bare the tendons. There is
often a history of intermittent
claudication (pain on exercise), dependent foot (dusky foot)
white on elevation, a history of peripheralvascular disease, lower
Ankle Brachial Index (ABI), weak/absent pulses, and sluggish/poor
capillaryrefill.
-
7/25/2019 Wound Care Module
12/29
12
The ulcer site is usually below the ankles to toes. The skin is
often shiny and friable. Uncontrolleddiabetes and smoking are
significant factors causing arterial insufficiency. Healing is
often slow andmay depend on the control of the underlying
cause.
Some examples of arterial ulcers are
traumatic ulcers on the shin and ankles
ulcers following fractures
ulcers caused by ill-fitting callipers or braces
post-burn ulcers
those caused by intra-lesional injections (in an area with an
already impoverished blood supply).
Treatment of arterial ulcer may involve a surgical intervention
- angioplasty, stenting, bypass, graftingand ultimately amputation.
Pain control is an important aspect of the management of arterial
ulcers.
4.1.4 Venous/Arterial (Mixed Ulcers)
It is important to note that between 10 percent and 15 percent
of leg ulcers are of mixed aetiology.These ulcers are often hard to
heal due to associated oedema, cellulitis, thrombophlebitis,
diabetes
or underlying vascular disease, rheumatoid diseases especially
in bed-ridden patients, and generalconditions of the skin in
elderly patients which are often associated with
malnourishment.
4.1.5 Other causes of ulcers
In addition to the more common forms of ulceration, there are a
number of less familiar causes.Vasculitic ulcers may develop as a
result of other medical conditions, such as those that effect
theimmune system (eg. rheumatoid arthritis, lupus and
polyarthritis).
Infections of the skin can produce ulcers especially if
necrotising bacteria are involved. Otherpotential causes of ulcers
are:
Haematological problems such as thalassemia or leukaemia.
Polycythaemia and skin conditions like pyoderma gangrenosum and
epidermolysis bullosa.
Some ulcers may be as a result of neoplasia (cancer) which may
develop into non-healingulcers. The most common of these are
squamous cell and basal cell carcinomas.
Ulcers may also form in patients with lymphoedema, caused by a
reduction in the function of thelymph vessels to drain
extracellular fluid. The resultant oedema will place the patient at
risk ofulcer development as a result of minor trauma and by the
hyperkerototic nature of the skin.
4.1.6 The Diabetic
The prevalence of diabetes in Australia is on the rise with
estimates of 3 to 4 percent of the
population currently having diabetes
5
. The trend is of concern as the number of people diagnosedwith
diabetes, as of 2006, is 1925 people every week6.
This constitutes a very large number of people in this country
and many health professionals will beconfronted by patients with
the problem of diabetic foot ulcers. Many diabetics may have a
small andminor skin breakdown which they may not consider important
however, due to their disease, theseminor wounds have the potential
of becoming serious.
4.1.6.1 How does diabetes affect wound healing?
Patients with diabetes are prone to have:
Impaired inflammatory response
Association of atherosclerosis (small vessel disease)
Damaged nerves which diminish pain sensation and nerve
response
Up to a five fold risk of infection.
-
7/25/2019 Wound Care Module
13/29
13
4.1.6.2 Risk factors in diabetes
4.1.6.2.1 Peripheral Vascular Disease
A major consequence of diabetes is the damage to both
macro-vascular and micro-vascular systems.The resultant reduction
in perfusion will contribute to the development of ulcers and also
to a delay inwound healing.
4.1.6.2.2 Peripheral Neuropathy
The lack of feeling or diabetic peripheral sensory neuropathy is
the major risk factor for footulceration. The fact that the
diabetic patient is unable to detect even minor injuries or
discomfort inthe feet will often place the patient at risk of
developing a small wound. Due to the lack of sensation,the patient
is unaware of the tissue damage and the wound will progress and
only be noticed when itis larger in size. The other indicator may
be the presence of odour which may indicate an infectedwound. In
addition to sensory neuropathies there may be autonomic and motor
neuropathies present.
4.1.6.2.3 Callus Formation
The development of excess callus will elevate plantar dynamic
pressure and when combined withperipheral neuropathy, may lead to
ulcer development.
4.1.6.2.4 Limi ted Joint Mobil ity
This will increase foot pressures and therefore increase the
risk of ulcer development.
4.1.6.2.5 Bony Deformity
Deformities of the ankle, feet, bunions and toes will all
increase the risk of ulcers forming.
4.1.7 Pressure Ulcers
Pressure ulcers are the most preventable of all of the chronic
wounds. Pressure wounds may be assimple as the blister most of us
may have experienced over the years from footwear, to the
extensivepressure sores experienced by patients suffering from
mobility decreasing conditions.
It has been estimated that between six to twelve percent of all
patients treated in hospital develop apressure wound, but sadly,
this number increases to about 30 percent in the elderly7.
A pressure wound develops when the capillary blood flow to the
skin and tissue over a bonyprominence is decreased for a sufficient
period of time.
The capillary pressure in the arterial blood system is some 32mm
of mercury. It therefore requires apressure of only about 30mm of
mercury to restrict the arterial blood flow. The consequence of
thisrestricted blood supply is a reduction in oxygen supply and
nutrition to the tissue, accompanied bythe problem of waste
products not being removed from the site.
The result of this is hypoxia, tissue acidosis, increased
capillary permeability- which allowsintravascular fluid to escape
causing oedema, and cell death.
The main causes of pressure wounds are
pressure
friction
shear
4.1.7.1 Pressure
Direct pressure on tissue over a bony prominence in excess of
30mm of mercury will cause
ischaemia in the surrounding tissue. This will occur not only
from a patient being in bed, but also on atrolley or sitting in a
chair. The extent of tissue damage will depend on the intensity of
the pressure,and the length of time the pressure remains
unrelieved. The tissue can tolerate pressure for short
-
7/25/2019 Wound Care Module
14/29
14
periods of time; however, even low pressure over a long period
of time will have some detrimentaleffect.
4.1.7.2 Friction
Friction occurs when the top layers of skin are worn away by
continued rubbing against an externalsurface. This can manifest
itself in a simple blister or tissue oedema, or an open pressure
wound.This can be caused by ill-fitting footwear, or even bed
linen.
4.1.7.3 Shearing forcesShear is when the skin remains in place,
usually unable to move against the surface it is in contactwith,
while the underlying bone and tissue are forced to move. This force
will contribute to thedestruction of microvasculature in a manner
similar to direct pressure. This type of pressure injury isseen in
patients left sitting up in bed or on a chair, while gravity causes
the patient to slide down withthe skin adhering to the bed linen or
the surface of the chair.
-
7/25/2019 Wound Care Module
15/29
15
5.1
5.2
5 Wound Dressings and Bandages
Wound pharmaceuticals / Wound healing product classification
The history of the development and use of dressings has seen an
evolution through many centuriesfrom inert and passive products
such as gauze, lint and fibre products to a dazzling range of
modernmoist wound dressings.
The range of dressings increases every year and is often a
source of confusion when attempting todifferentiate between both
similar and different dressings. The simplest way of classifying
dressingsis by their functionality.
Wound products can be divided into two broad groups:
Passive products
Interactive products
Within these two groups, the passive dressings can be
sub-classified into absorbing and non-absorbing dressings whereas
the interactive dressings can be sub-classified as absorbing,
non-absorbing and moisture donating. The interactive group has six
different dressing types.
Turner8has defined the following as the properties of the ideal
wound dressing:
Remove excessive exudate from the wound without allowing the
wound to dry out therebymaintaining a moist environment
Allow gaseous exchange so that oxygen, water vapour and CO2may
pass in and out of thedressing
Be thermally insulating so as to maintain the wound core
temperature at approximately 37degrees C
Be impermeable to micro-organisms in order to minimise
contamination of the wound fromoutside the wound itself
Be free from either particulate or toxic contamination
Be non-traumatic and not adhere to the wound, so that at
dressing change it will not damagegranulating tissue.
Passive dressings
For many years the products used were of the 'passive' or the
'plug and conceal' concept andincluded gauze, lint, non-stick
dressings, and tulle dressings. Passive dressings fulfil very few
of theproperties of an ideal dressing and have very limited (if
any) use as a primary dressing, however,some are useful as
secondary dressings.
In addition to gauze, lint and cotton dressings, other simple
modified absorbent pads covered with a
perforated plastic film to prevent adhering to a wound (such
products include Melolin, Cutilin andTelfa) are used both as
primary and secondary dressings. They are used in minor and
lowexudating wounds.
5.2.1 A modern inert dressing
Exudry and Mesorb are examples of products with a highly
absorbent pad and a non-stick, non-shear surface. They can be used
as a secondary dressing over moderate to highly exudating woundsand
over hydrocolloid paste, cadexomer iodine, alginate and other
primary dressings.
5.2.2 The non-absorbent passive dressings
The non-absorbent passive dressings such as paraffin gauze
(tulle) dressings, are among theearliest modern dressings. Many
variations have been developed over the years by changing
theloading of paraffin in the base. In general, these dressings
produce a waterproof paraffin cover over
-
7/25/2019 Wound Care Module
16/29
16
5.3
the wound which may lead to maceration in that water vapour and
exudation may not pass throughand so become trapped within the
wound. These products:
are permeable to bacteria
are known to adhere to the wound causing trauma on removal
require a secondary dressing.
Their use is limited to simple, clean, superficial wounds and
minor burns. They are also used as a
primary dressing over skin grafts. There are modern alternative
dressings composed of syntheticfibres tightly meshed and
impregnated with materials that allow moisture to pass through and
thusminimise any maceration of the wound and tissues. Examples
include Adaptic, Cuticerin andAtrauman.
Interactive dressings
These dressings help to control the micro-environment by
combining with the exudate to form eithera hydrophilic gel, or by
means of semipermeable membranes, controlling the flow of exudate
from thewound into the dressing. They may also stimulate activity
in the healing cascade and speed up thehealing process.
There are six classes of interactive dressings which are
classified according to their functionality.
5.3.1 Non-Absorbing dressings
5.3.1.1 Film Dressings (for wounds with no to low exudate)
These dressings consist of a thin, poly-urethane membrane coated
with a layer of acrylic adhesiveand:
are waterproof
are gas/vapour permeable
are flexible
protect from shear, friction, chemicals and microbes
are transparent
spread tension forces.
They are particularly useful in superficial, clean wounds and in
the prevention of breakdown and pre-ulcers in pressure wounds. They
are also used as a post operative dressing over sutures and
toreduce sub-tissue tension over a closed sutured wound after
removal of the sutures or clips. Filmdressings should not be used
for infected wounds.
BRAND MANUFACTURER TYPE
Opsite Smith & Nephew Plain film, Island Film
Flexigrid
Flexi Fix {continuous rolls}
IV 3000 {high MVTR*}
Post-op {island dressing}
Tegaderm 3 M Plain film
HP* {high MVTR}with absorbent pad
island dressing
-
7/25/2019 Wound Care Module
17/29
17
Biofilm Johnson & Johnson Plain film
Polyskin II
Aqua Protect
Hydrofilm
Tyco
Beiersdorf
Hartmann
Plain film
MR* {high MVTR}
Plain film
Island Film
Plain film
*MVTR = Moisture Vapour Transmission Rate ie. the level of
passage of water vapour or exudatethrough the surface of the
dressing.
*HP = Holding Power
*MR = Moisture Responsive
5.3.2 Absorbing dressings
5.3.2.1 Hydrocolloid dressings (for wounds with low to moderate
exudate)
Hydrocolloids are a combination of polymers held in a fine
suspension, and often containpolysaccharides, proteins and
adhesives. When placed on a wound the polymers combine with
theexudate and form a soft, moist gel-like mass. They also
encourage autolysis to aid in the removal ofslough from a
wound.
They:
are flexible and waterproof
provide a physical barrier
form a gel with exudate
aid in debriding
need no secondary dressing
are available in a thin form (transparent).
The early forms of hydrocolloids are occlusive, so as to make
them impermeable to gases and watervapour. They do, however, act as
a barrier to external bacteria and are waterproof enabling
thepatient to shower. The thin, transparent hydrocolloids have a
polyurethane film backing, are non-occlusive, thereby allowing the
passage of water vapour and gases.
Hydrocolloids should be applied over the wound with at least 3-4
cm extra product greater than thesize of the wound. The skin should
be dry and free from creams, ointments or oil to ensure
goodadhesion. The dressing should be placed 1/3 above the wound and
2/3 below the wound, as this willprolong the wear time of the
dressing. The dressing can remain in place for up to 7 days with
removal
dependent on the level of exudate and when strikethrough has
occurred (i.e. the exudate hasmigrated to the edge of the
dressing).
Hydrocolloid products are used in low to moderately exudating
wounds- including ulcers, donor sites(after haemostasis) and
granulating wounds. They may also be used in conjunction with a
paste orpowder form. The paste or powder is used in a deeper ulcer
or cavity. These convert to the samehydrophilic gel and are covered
with the normal hydrocolloid wafer.
BRAND MANUFACTURER TYPE
Comfeel Ulcer Dressing
Comfeel Paste
Comfeel Powder
Coloplast Multiple Sizes
Tube
Pack
-
7/25/2019 Wound Care Module
18/29
18
Comfeel PlusTransparent
Multiple Sizes
DuoDerm CGF
DuoDerm Border
DuoDerm ExtraThin
DuoDerm Paste
ConvaTec Multiple Sizes
Multiple Shapes and Sizes
Multiple Shapes and Sizes
Tube
Replicare Smith & Nephew Multiple Sizes
Ultec Tyco Multiple Shapes and Sizes
Hydrocoll
Hydrocoll Thin
Hartmann Multile Sizes
Multiple Sizes
Tegasorb
Tegasorb Thin
3M Multiple Shapes and Sizes
Multiple Shapes and Sizes
5.3.2.2 Foam dressings (for wounds with medium to high
exudate)
These products are soft, open-celled hydrophobic/ hydrophilic
non-adherent dressings that may besingle or multiple layered and
meet many of the properties of an ideal dressing.
They:
allow the passage of exudate through the non-adherent surface to
be absorbed in the mainbody of the product
are absorbent
maintain a moist environment
are thermally insulating
are cushioning
are non-adherent
are non-residual.
Foams are mainly used in moderately to heavily exudating wounds-
including ulcers, donor sites andminor burns, and they act as a
secondary dressing, particularly as a covering with the use
ofamorphous hydrogels. In addition to standard and waterproof foams
there is also a charcoal-impregnated version, Lyofoam C, as well as
shaped cavity devices which may be inserted into
cavity wounds or gaping surgical wounds.
BRAND TYPE MANUFACTURER
Allevyn Sheet
Allevyn Island
Allevyn Adhesive
Allevyn Cavity
Multiple layer
Multiple layer waterproof
Multiple layer waterproof andadhesive
Dual layer cavity insert
Smith & Nephew
Cavicare Conforming Foam Smith & Nephew
Curafoam Single layer Kendall
-
7/25/2019 Wound Care Module
19/29
19
Hydrasorb Single layer Kendall
Lyofoam
LyofoamAdhesive
Lyofoam Extra
Lyofoam C
Permafoam
Mepilex
Mepilex Thin
Dual layer
Dual layer waterproof
Multiple layer
Dual layer combination with
charcoal
Multiple layer
Multiple layer
Thin Multiple layer
Aaxis Pacific
Aaxis Pacific
Aaxis Pacific
Aaxis Pacific
Hartmann
Molnlycke
Molnlycke
5.3.2.3 Alginate dressings (for wounds with medium to high
exudate)
Alginates are the calcium or sodium/calcium salts of alginic
acid, composed of manuronic andguluronic acids obtained from
seaweed. When applied to a wound, the sodium salts present in
the
wound exchange with the calcium in the alginate to form sodium
alginate which is a hydrophilic gel.This gel has the ability to
absorb exudate into itself while maintaining a moist environment at
theinterface between the dressing and the tissue.
Alginate dressings:
are highly absorbent
form a gel with exudate
create a moist interface
are easily removed
are haemostatic.
Alginates are used on donor sites, bleeding sites, exudating leg
ulcers and cavities. They are notconsidered to be of value in low
exudating wounds or dry wounds with eschar.
They come in a number of different forms, including sheets,
packing rope and in combination withcharcoal for exudating
malodorous wounds.
Sheet alginates should be cut to the shape of the wound, placed
on the wound and covered with asuitable secondary dressing (eg.
foam and non-stick dressings). They should then be held in
placewith a cohesive or tubular bandage. If the wound is highly
exudating then an outer absorbent padmay be added. In the case of a
moist cavity wound, the rope or packing ribbon is gently placed
intothe cavity taking care not to pack the material tightly into
the space. In general, alginates should bechanged when they have
fully converted to a gel, this will vary from 1 to 3 days depending
on the
level of exudate in the wound. When used on a donor site, the
material is placed over the area afterskin harvesting and covered
with a film or a foam dressing, which can remain in place for up to
7days.
BRAND TYPE MANUFACTURER
Algoderm
Kaltostat
Carboflex(withcharcoal)
Surface sheet {firm gel}
Cavity Rope {firm gel}
Surface sheet{firm gel}
Cavity rope {firm gel}
Surface sheet
Johnson & Johnson
Convatec
Comfeel Alginate Cavity Rope {soft gel} Coloplast
-
7/25/2019 Wound Care Module
20/29
20
Comfeel Seasorbsoft
Surface sheet {firm gel}
Curasorb Surface sheet {firm gel}
Cavity rope {firm gel}
Tyco
Sorbsan Surface sheet {soft gel}
Cavity rope {soft gel}
Unomedical
Tegagen HI
Algisite M
Surface sheet {firm gel}
Surface sheet {firm gel}
Cavity rope {firm gel}
3-M
Smith & Nephew
5.3.2.4 Hydrofibre dressings
Hydrofibre dressings have some of the properties of alginates in
that they are a fibre rope or dressingthat forms a firm gel in
contact with fluid.
They:
are composed of a synthetic fibrous mat
form a firm gel in contact with exudate
are highly absorbent
have no lateral wickingprotects peri-skin
An example of this product is Aquacel.
5.3.2.5 Hydroactive dressings (for wounds with medium to high
exudate)
These multi-layered highly absorbent polymer dressings with a
surface adhesive and a waterproofouter layer are similar to
hydrocolloids, however, instead of forming a gel in contact with
exudate, thefluid is trapped within the product itself, to maintain
a moist environment.
Hydroactive dressings are:
highly absorbent polymer dressings
waterproof
expandable
non-residual
semi-permeable.
Hydroactive dressings are indicated for use in highly exudating
surface and cavity wounds includingleg ulcers, pressure wounds and
minor burns. They are particularly useful over joints such as
elbows,knees, fingers and toes due to their ability to expand and
contract without causing constriction.Hydroactive dressings are not
indicated for dry or lightly exudating wounds.
BRAND TYPE MANUFACTURER
Cutinova Hydro
Allevyn Thin
AllevynCompression
Allevyn plus Cavity
Surface sheet thick
Surface sheet thin
Surface sheet non-adhesive
Cavity dressing
Smith & Nephew
-
7/25/2019 Wound Care Module
21/29
21
Tielle Surface sheet Johnson & Johnson
Biatane Surface sheet
Cavity dressing
Coloplast
PolyMem Surface sheet Ferris
5.3.2.6 Hydrogels ( For dry or sloughy wounds )
Hydrogels are a group of complex organic polymers having a high
water content ranging between 30to 90 percent. This broad class of
polymers swells extensively in water, but does not dissolve
inwater. They have the properties of both rehydrating dry tissue,
and absorbing certain amounts of fluidinto themselves. They are
provided as either amorphous gels or sheet gels. These products are
usedto help re-hydrate sloughy wounds and necrotic tissue to aid in
the autolytic debridement of wounds.They are also used in the
management of burns, including sunburn, scalds and other
partialthickness burns. Amorphous hydrogels have also been used in
the management of chicken pox and
shingles, applied to the eruptions three to four times a day.
They provide a moist environment andrelieve the discomfort of the
lesion, and also reduce the probability of scarring.
Hydrogels are also available in sheet form consisting of a
cross-linked polymer and water held in abacking. These products are
particularly useful in the management of burns, and also to aid
theremoval of necrotic tissue in pressure wounds.
BRAND TYPE MANUFACTURER
DuoDERM Gel Amorphous non-preserved Convatec
Safgel Amorphous preserved Convatec
Intrasite gel Amorphous non-preserved Smith & Nephew
Intrasite gelconformable
Impregnated amorphous Smith & Nephew
Solosite Amorphous preserved Smith & Nephew
Curafil gel Amorphous preserved Tyco
Curafil Impregnatedgauze
Curagel
Impregnated amorphous Sheet Gel Tyco
Purilon gel Amorphous non-preserved Coloplast
Solugel
Nu-gel
AquaClear
Amorphous both preserved and nonpreserved
Sheet Gel
Sheet Gel adhesive and non-adhesive
Johnson &Johnson
Johnson &Johnson
Hartmann
-
7/25/2019 Wound Care Module
22/29
22
5.3.3 Miscellaneous dressings
There is a small number of specialised dressings for use in
particular wound types.
5.3.3.1 Cadexomer Iodine Dressings (e.g. Iodosorb)
This is a non-toxic iodophor that combines iodine with a
polysaccharide polymer. When applied to thewound, the exudate
combines with the polymer and is absorbed at the same time as the
iodine isreleased- over a period of 72 hours at a low strength.
Cadexomer Iodine was developed in the 1980s and consists of
cadexomer polysaccharide polymerand iodine 0.9%. The iodine is
cross-linked into the structure of the polymer. Upon contact with
awound, this dressing:
is absorbent forms a gel with exudate
releases iodine as gel forms
pulses iodine at 0.1% (not cytotoxic)
is used for sloughy/ infected wounds, diabetic wounds, chronic,
slow healing wounds
may stimulate growth factors.
5.3.3.2 SilverSilver has been used for many years, and has
proven antimicrobial activity. It is broad spectrum andinactivates
almost all known bacteria, including methicillin-resistant
staphylococcus aureus (MRSA)and vancomycin-resistant enterococci
(VRE). No cases of bacterial resistance have beendocumented9,10.
Silver has been used in the treatment of burns as a silver
sulfadiazine cream, andthis cream has also been applied to some
wounds. The difficulty in applying a cream to a mucoussurface is
that it will cause the development of mucilaginous slough. The
development of a range ofmodern silver dressings overcomes this
difficulty by delivering varying levels of silver directly from
thedressing. The base dressings include hydrocolloids, alginates,
tulles, hydroactives, foams, gels andpolyethylene mats. The amount
of silver and the method of action vary greatly between
thesedressings. Some release silver into the wound and some
maintain the silver within the dressing and
kill bacteria as they are absorbed into the dressing.
Silver Product Type Trade name Manufacturer
High Density Polyethylenedressings
Acticoat Smith & Nephew
Foam Dressing Avance Aaxis Pacific
Alginate Dressing Acticoat Absorbent Smith & Nephew
Hydrocolloid Dressing Contreet H Coloplast
Hydroactive Dressing Contreet Coloplast
Hydrofibre Dressing Aquacel Ag Convatec
Tulle Dressing AtraumanAg Hartmann
5.4 General rules for the topical use of antiseptics
The role of topical antiseptics in chronic wounds is not as
clear as in the case of acute wounds.There is a group of patients
with long standing, non-healing leg ulcers. There are some
clinicians
who believe that one of the reasons for non-healing of these
wounds is the presence of largenumbers of colonised bacteria,
especially in those patients who may be malnourished, diabetic
orimmuno-compromised. In some of these patients, the use of a short
course of dilute topical
-
7/25/2019 Wound Care Module
23/29
23
antiseptics may help reduce the surface flora and speed the
process of wound healing. The decisionshould be made for the
individual patient, taking into account all of the benefits and
risks.
WOUND TYPE MANAGEMENT
CUT/LACERATION
Clean the area with water or saline. If there is any
contamination, use asurfactant antiseptic (eg. Savlon or Povidone
Iodine scrub) to remove
any foreign material that may be a focus for infection. Apply
anantiseptic around the area and cover with a simple dressing (eg.
a filmdressing).
GRAZE Due to the presence in most grazes of dirt, gravel and
other material,scrub the area with a surfactant antiseptic eg.
Savlon or PovidoneIodine scrub.
Apply an antiseptic around the wound and cover with either a
filmdressing or an island film dressing.
BURN Most minor burns do not require the use of a topical
antiseptic. Their
use will depend on the depth of the burn and if there is damaged
andnecrotic tissue present. If there is, then the use of SSD cream
isconsidered appropriate in the early management. If the burn is
minorand there is little tissue damage (eg. minor blisters) then
apply anamorphous or sheet hydrogel.
CHRONICWOUNDS
eg. Leg Ulcersand Pressure
Ulcers
If the level of colonised bacteria is high, the short term use
of PovidoneIodine Solution is the most effective antiseptic to use.
Therecommendation is to use a low strength (eg. 1%) solution and to
applyfor 3 to 5 minutes and then wash the product off. Within this
time theproduct will have significantly reduced the numbers of
surface bacteria.
The other option is the use of Iodosorb being non-toxic.
5.5
5.6
Hypertonic Saline
Hypergranulation is generally treated with topical silver
nitrate or copper sulphate. An alternative andless toxic method is
the application of a hypertonic saline dressing. These are applied
to thehypergranulation and covered with a simple secondary dressing
and a compression bandage. Thedressing is changed daily. Examples
of this dressing are Mesalt and Curasalt.
New burn dressings
Once the burn has settled down and any necrotic tissue removed
by autolysis, an additional modalitymay be used. The use of
retention tape dressings, for example Fixomull and Hypafix,
applieddirectly over a minor burn is also a possibility. Such a
protocol was introduced by the Burns Unit atRoyal Perth Hospital
and is now in general use.
The tape, once applied, remains in place for seven days at a
time. It is removed by dissolving theadhesive in a fixed oil or
citrus oil, allowing the tape to be easily removed without damaging
the newepithelium. These retention tapes are permeable, allow
exudate to flow through their surface, areflexible and although not
waterproof may be washed after the first 48 hours of application
and theywill dry and remain in place.
It is also important to cover the dressing with a cohesive
bandage to apply some compression to the
skin.
-
7/25/2019 Wound Care Module
24/29
24
5.7
5.8
Keloid and Hypertrophic Scar Management
A topical method for treatment of keloid and hypertrophic scars
is the use of a silicone dressing. Thedressing is applied to the
scar initially for 4 hours and then progressively increasing the
contact to 24hours. The scar may gradually reduce in depth and
colour. This will however, be a slow processrequiring application
for six months or more. Examples of this type of dressing are Cica
Care andMepiform.
Bandages
The use of material to bind a wound is as ancient as medicine
itself. Techniques and material havechanged little over the
centuries, but in the past fifteen years there has been an
explosion in the typeof bandages available.
When choosing and applying a bandage it is important to
differentiate between the traditional and theritual on one hand,
and what is best and most cost effective for the patient on the
other.
The bandage may be needed for keeping a dressing in place,
supporting an injured joint or assistingvenous return.
5.8.1 Retention Bandages
The role of retention bandages is effectively to hold a dressing
in place. They are of particular usewhere a patient has very fine
and very fragile skin that is easily damaged if the dressing was
held inplace with any type of adhesive tape or other adhesive
product. For many years, cotton crepebandages have been used to
hold dressings in place for this purpose. However, today there are
anumber of more effective and appropriate bandages that may be used
to hold a dressing in place.
The first is the lightweight conforming cohesive bandage. This
type of bandage is a lightweight crepecoated with a thin latex. As
a result of this coating the bandage sticks to itself but not to
skin, hair orclothing. You only require a very small length to hold
the dressing in place, compared with using acomplete roll of a
standard crepe bandage. This type of bandage comes in widths that
areappropriate for fingers and toes and also for limbs and larger
sizes for the head. The other mainadvantage is that the same amount
is not required to hold the dressing in place compared with
using
a standard crepe bandage. This makes this type of bandage less
bulky and very cost effective.Examples of this type of bandage are
Handigauze Cohesive, Easy Fix Cohesive and Hospifix.
The other type of product is the elasticised tubular bandage
available in a light weight form that maybe cut to the required
size and placed over the dressing, again holding it in place. An
example is TubiFast.
5.8.2 Support Bandages
Support Bandages are of a heavier construction and are made from
both natural and synthetic fibres.They achieve their stretch by the
use of high twist yarns and the heavier construction. The main
roleof strong support bandages is the support of joints in strains
and also in the management of muscular
injuries. Strong support bandages can be used singularly or in
combination to restrict movement, tohelp reduce some of the oedema
and act as a mechanism of support following soft tissue injury.
Theexamples of this type of bandage are the heavy duty crepe
bandage such as Elastocrepe andHandycrepe, and the heavier weight
cohesive bandage (eg. Coban, Coplus, Handygrip).Also, single layers
of the heavier weight tubular bandage may also be used for this
purpose (eg. TubiGrip, Handyplast Tubular or Tensogrip).
5.8.3 Compression Bandages
The action of these bandages is to provide pressure firm enough
to compress the pathologicallydistended veins, thus enabling the
valves to remain tightly against the wall of the vessel,
increasingvelocity of the venous blood stream and normalising the
returned flow of blood to the heart.
Accumulated fluid and waste products are removed from the
affected tissue by the accelerated rateof flow resulting from
application of a pressure bandage.
-
7/25/2019 Wound Care Module
25/29
25
Effective therapeutic compression starts with a sub-bandage
pressure of 18 mm of mercury at theankle. Anything giving a lower
value may be appropriate for support, but is not
consideredappropriate in the treatment of venous leg ulcers.
The primary aim of compression is to reduce pressure in the
superficial veins in order to encouragevenous return to the heart.
This is performed by increasing the velocity of flow in the deep
veins anddiscouraging oedema by reducing the pressure difference
between the capillaries and the tissues.The most effective method
is to apply graduated compression from the toes to the knee. The
highest
pressure should be exerted at the ankle, gradually falling to 50
percent at the knee. Anti-embolicstockings should only be used for
the prevention of deep vein thrombosis in hospitalised
patients.They provide a pressure of between 12mm and 18mm of
mercury.
Compression bandages are divided into two types: high stretch
compression and shortstretch.
5.8.3.1 High stretch compression bandages
These bandages have an extension from 130 percent to 200
percent, high elasticity, medium to highresting pressure, and
medium to high working pressure. They exert their effects
superficially, workingin combination with the muscles. They are
indicated for venous oedema and the management ofvenous ulcers and
may be left in place for 24 hours. Examples include Tensopress,
Setopress,Surepress and Eloflex.
5.8.3.2 Short stretch bandages
These have an extension of 30 percent to 90 percent, low
elasticity, low to slight resting pressure, buthigh to very high
working pressure. They exert their main effects deep within the
limb and areindicated for venous oedema and lymphoedema. These may
be left in place for 24 hours. Examplesof this type of bandage are
Comprilan, Lastolan and Tensolan.
Application methods include the simple spiral method which is
performed by applying the bandagewith a figure eight at the ankle,
and continuing up the limb in a spiral application covering 50% of
thepreviously bandaged area. The application is generally
undertaken with the high stretch type ofbandage.
A continuous figure eight method of application is performed by
overlapping as the bandage is woundup the leg so that it is applied
in one direction and then in the opposite direction, producing a
Vshape in the bandage. This method is used particularly with the
low stretch compression bandages.
A development in bandaging has been the introduction of the
Charing Cross 4 layer system. Thiscombines an orthopaedic wool,
crepe, elastic and cohesive bandage in multiple layers. This
achieves40 mm of mercury at the ankle, graduating to 17 mm of
mercury at the knee. A number of publishedstudies have shown good
healing rates in 12 weeks with this particular system 11. The
commercialbrands of this type of bandage system are Profore,
Profore Lite, Pro-guide and Veno-4.
If it has been clearly demonstrated by Doppler and/or Duplex
scanning that a true venous pathologyexists, compression bandaging
is then used in combination with management of the wound
byappropriate dressings, using either a high or low stretch
compression bandage.
Where there is some indication of minimal arterial involvement,
compression is provided by the useof a straight tubular bandage.
Where more significant arterial disease is present, no compression
isapplied over the dressing.
5.8.3.3 The hazards of compression bandages
Care must be exercised when applying compression bandages to
ensure that there is adequatearterial blood flow. The application
of compression can cause skin necrosis, trauma, ulceration, oreven
amputation (which may result from damage caused by lack of arterial
blood in the area).
An alternate method of applying graduated pressure to the leg is
through the use of compressionstockings. Stockings may be used as
part of the treatment of venous leg ulcers, as an ongoingmanagement
modality of venous disease, and/or for the prevention of venous
stasis.
The use of compression stockings both as a preventive measure
and anti-embolic stocking tominimise the risks of venous stasis is
common. The difficulty is that there is considerable confusion
-
7/25/2019 Wound Care Module
26/29
26
as to the appropriate type of stocking to use and the level of
compression necessary for besttreatment.
Anti-embolic stockings may also be used alone or in conjunction
with systemic medication (eg. LowMolecular Weight Heparin) for the
prevention of Deep Vein Thrombosis in patients undergoingsurgery.
The stockings are worn by non-ambulatory patients in hospital pre
and post surgery to helpprevent DVTs.
It should be noted that anti-embolic stockings are not suitable
for the treatment or management of
venous disease.
Compression stockings have a major role to play in the
prevention of venous stasis, should also beworn when travelling
long distances to minimise oedema and thrombosis development.
5.8.4 Zinc paste bandages
Zinc has been used in medicine for hundreds of years, even
though very little published data of itspharmacology is available.
Zinc is an important trace element in many functions of the body.
Inwound healing it is essential for cell proliferation and tissue
regeneration, and is also involved incollagen synthesis and
epithelialisation.
There are a number of commercial zinc paste bandages available
on the Australian market. These
include: Zincaband and Steripaste of Seton, Viscopaste and
ZipZoc of Smith and Nephew,Flexidress of Convatec, and Gelocast of
BSN Medical.
The bandage can be applied to the limb, as a patch over the
wound or as a full length bandage. Awater-based zinc paste bandage
with no preservatives is beneficial in the management of
chronicvenous leg ulcers, particularly where venous eczema is
present and when used in conjunction withappropriate compression
bandaging.
-
7/25/2019 Wound Care Module
27/29
27
6.1
6 General rules
Acute wounds
Assess and identify
Clean and decontaminate
Stop the bleeding (alginates/ pressure)
Wound closure (closure strips/ film dressings)
Dressing film, island film or island dressing
Bandage (simple cohesive).
6.2
6.3
6.4
Chronic wounds
Confirm underlying cause ie. venous / arterial etc
Dressing dependent on wound type and the level of exudate
If true venous-pathology exists, graduated compression should be
used.
Protocol for wound management of skin tears
Clean the wound with water or saline. If there is contamination,
use a surfactant wash product(eg. QV Wash) to help remove any
debris.
If bleeding, apply gentle pressure with a piece of gauze padding
(ensure that the gauze doesnot stick as this may result in further
tearing), if unsuccessful then apply a haemostatic alginatedressing
(eg. Kaltostat) to aid in haemostasis.
If there is major separation of the skin edges, apply an elastic
sterile strip, preferably 3-4mm inwidth to several parts of the
skin tear to hold the skin flap in place.
Apply a low strength povidone iodine solution to the wound,
leave in place for 3 minutes andthen wash off.
Apply a small amount of an amorphous hydrogel (eg. IntraSite
Gel) to the wound.
Cover with a foam dressing (eg. Lyofoam, Allevyn, Mepilex).
Hold in place with a light weight cohesive bandage.
This system is left in place for 4 to 5 days at which time the
dressing is removed, the wound cleanedand the system replaced.
After the next 4 5 days the dressing is removed and replaced with
apatch of non-preserved zinc paste bandage (eg. Gelocast,
Steripaste, ZipZoc). This is thencovered with foam and held in
place with a lightweight cohesive bandage (eg. Handygauze
cohesive
) and left in place for seven days. Upon removal the wound
should be healed. If not, then repeatthe zinc paste patch dressing
system for a further seven days.
Difficult wounds (i.e. animal or insects bites)
Assess and identify
Plan treatment
Clean
Dress as appropriate
NB. May need systemic antibiotics, infection may be due to
atypical micro-organisms.
-
7/25/2019 Wound Care Module
28/29
28
6.5
6.6 Burns
Post operative wounds
Assess
Dress over sutures with a film or thin hydrocolloid.
If exudating use an island dressing.
For an open cavity wound, use alginates and/or foam. Use film
dressings over the incision once sutures are removed.
For sunburn, apply cold water then amorphous hydrogels.
For simple burns and scalds of partial thickness, apply cold
running water for 10-15 minutesthen hydrogels (either sheet or
amorphous), or retention tape (eg. Fixomull or Hypafix).
The final aspect of wound care is a plan for management. Once
the wound is healed, it is important
to investigate and examine the intrinsic and extrinsic factors.
Once identified, try to alterenvironmental aspects such as
nutrition, exercise, use of compression stockings, and
environmentalissues such as standing for long periods of time
leading to venous stasis. These actions may wellprevent
redevelopment of the wound or the development of new ones.
-
7/25/2019 Wound Care Module
29/29
7 References
1. Sussman G, Wound Management: How to treat. Australian Doctor
30 November 2001:S1-S8
2. Nelzen O, Bergqvist D, Lindhagen A. The prevalence of chronic
lower-limb ulceration has beenunder estimated: results of a
validated population questionnaire. British Journal of Surgery
1996;83:255-258
3. Winter, G. Formation of the scab and the rate of
epithelization of superficial wounds in the skin ofthe young
domestic pig. Nature 1962;193: 293-4
4. Drosou, A. Antiseptics on wounds an area of controversy.
Wounds 2003 15(5):149-166
5. Australian Institute of Health and Welfare 2002. Diabetes:
Australian facts 2002. AIHW Cat. No.CVD 20 (Diabetes Series No.3).
Canberra: AIHW.
6. Diabetes Australia press release 16th May 2006)
7. Bennett G, Leigh IH. Pressure ulcers: prevalence, aetiology
and treatment modalities: a review,American Journal of Surgery
1994,167(1a):25S-30S (correct)
8. Turner, T D. Products and their Development in Wound
Management, Plastic Surgery Journal1979 75-84
9. Thomas S, McCubbin P. A comparison of the antimicrobial
effects of four silver-containingdressings on three organisms.
Journal of Wound Care.2003 Mar;12(3):101-7
10. Lansdown ABG. Silver 1: its antibacterial properties and
mechanism of action, Journal of WoundCare 2002,11(4):125-130
11. Moffatt CJ, Dickson D. The Charing Cross High Compression
Four Layer Bandage System,Journal of Wound Care (1993) 2(2):
91-94.
http://../worddoc_wc_md/javascript:AL_get(this,%20'jour',%20'J%20Wound%20Care.');http://../worddoc_wc_md/javascript:AL_get(this,%20'jour',%20'J%20Wound%20Care.');