Embed Size (px)
Citation preview

Sot. Sci. Med. Vol. 19. No. 4, pp. 359-372, 1984 Printed in Great Britain
0277-9536/X4 %3.00 + 0.00 Pergamon Press Ltd
WORKING CONDITIONS AND HEALTH: SOCIAL EPIDEMIOLOGY, PATTERNS OF STRESS
AND CHANGE*
WILFRIED KARMAUS
Department of Medical Sociology. University-Hospital Eppendorf, Martinistr. 52, D-2000 Hamburg 20, West Germany
Abstract-This paper does not attempt to review stress research but to highlight contrary positions. Arguments about central questions such as exposure vs disposition, social factors vs the constitutional make-up has lead to refinements in methodology. However, investigations seldom do justice to these ideals discussed. It should be a conditio sine qua non when estimating the effects of dispositional factors to consider exposure which could change dispositions or interact with them. Also it becomes obvious that when investigating working life a limited view of risks factors only must faile because job latitudes and support are of salient importance. Concerning changes in working life our methodological flights of fancy are confronted with the limited horizon and world of a mole.
The topics ‘working conditions and health risks’ and ‘stress’ have one thing in common-their extreme contraversiality. Not only as far as effects of work on health are concerned but also with regard to the results of stress research there exist controversial positions (either founded or not). This paper will not attempt to pour oil onto troubled waters or to strike the scientific balance of accepted issues, but will try to throw light on contrary opinions. The discourse begins with social epidemiology (social hygiene), which, so to speak as the mother of the wayward children, ‘work and health risks’ and ‘stress research’, was the root of the evil. Different explanatory ap- proaches will be investigated on the basis of central questions such as:
Is exposure to health risks or dispositions (predis- position, susceptibility) of the individual the cause of disease?
When can a social state of affairs be termed health risks with scientific certainty?
What is the relationship between science and prac- tical change of pathogenic conditions?
These basic considerations, often neglected in every-day empirical research, lead to the connection of working conditions being established only slowly and on the basis of controversial positions or me- thodical bias. Also the term ‘health’ in this paper does not limit itself to the absence of defined occupational diseases, but refers to the wide range of occupational complaints.
1. THE ROOT OF EVIL: SOCIAL EPIDEMIOLOGY
A basic question of aetiological research is the relationship between disposition and exposure. What influences can affect the initiation/genesis of an ill- ness? Are they:
on the one hand specQ‘ic dispositions as. for exam-
*Originally prepared as a Background Paper for Section T. Eighth International Corzference on rhe Social Sciences and Medicine. Stirling, Scotland. 22-26 August 1983.
ple, immunity deficiency, innate hypercholesterinemia or an unspeciJic (innate or acquired) weakness, vul- nerability; or
on the other hand environmental agents, which have a specific ejfkt, as for example tubercular bacilli, asbestos or working and living conditions, which have an unspecific effect, as for example social class or stress?
Within the framework of interaction between exposure and disposition it is, according to Mosse and Tugenreich writing as early as 1913, the task of social hygiene “to show to what degree the complex of social factors is relevant to the origin and devel- opment of illness; and further, which factors in this complex are in each case of provement importance” [I]. They proceed froni the assumption that “the state of health of each person is the result of the effect of the environment and the reaction of the body. This reaction is determined by a sum of factors which are normally described as constitution. This constitution is not innate,. . . , but it is, however, the result of innate and acquired characteristics” [2]. Even then, about 100 years ago, there existed a controversy about the significance of working and living condi- tions as well as acquired disposition on the one hand, and of specific infections agents or of genetic disposi- tion on the 0the.F. The increased mortality of individ- ual groups within the population (e.g. the Jews) was regarded as natural selection caused by disposition and bacteria were seen as an adequate cause of diseases.
However, the scientific question of when a social state of affairs can conclusively be considered causal/causative health risk was of secondary im- portance during an era of political disputes about health. “The serious cholera epidemic in England in 1831/32 had directed public attention to the deplor- able sanitary conditions, and at once there arose from the general public, from among the representatives of the nation, in the daily press and in parliament a unanimous call for a thorough examination of the conditions which made it possible for particular places to have suffered so severely” [3]. Although not
359
360 WILFRIED KARMAUS
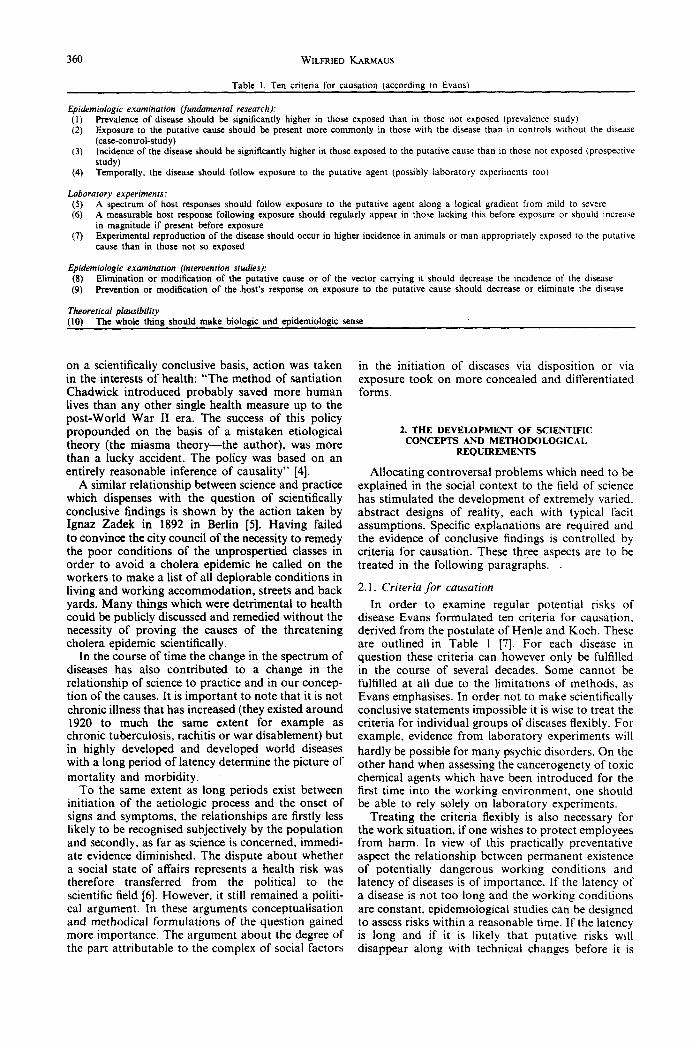
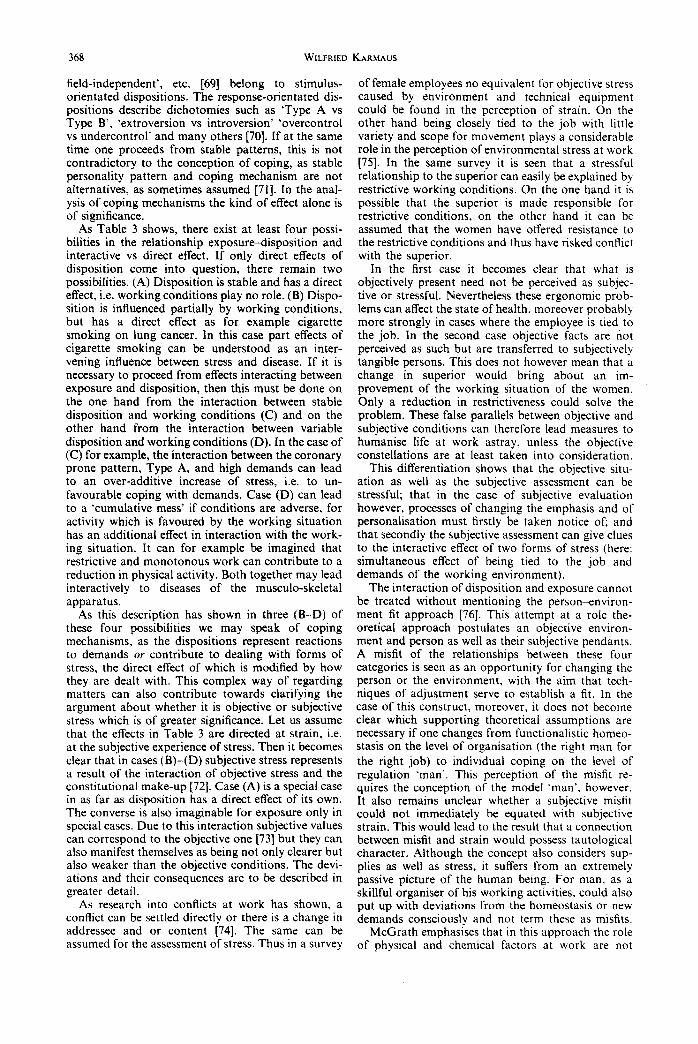
Table I. Ten criteria for causation (according to Evans)
Epidemiologic examination (fundamental research): (1) Prevalence of disease should be significantly higher in those exposed than in those not exposed (prevalence study) (2) Exposure to the putative came should be present more commonly in those with the disease than in controls without the disease
(case-control-study) (3) Incidence of the disease should be significantly higher in those exposed to the putative cause than in those not exposed (prospective
study) (4) Temporally, the disease should follow exposure to the putative agent (possibly laboratory experiments too)
Laboratory experiments: (5) A spectrum of host responses should follow exposure to the putative agent along a logical gradient from mild to severe (6) A measurable host response following exposure should regularly appear in those lacking this before exposure or should increase
in magnitude if present before exposure (7) Experimental reproduction of the disease should occur in higher incidence in animals or man appropriately exposed to the putative
cattse than in those not so exposed
Epidemiologic examination (intervention studies): (8) Elimination or modification of the putative cattse of of the vector carrying it should decrease the incidence of the disease (9) Prevention or modification of the .host’s response on exposure to the putative cause should decrease or eliminate the disease
Theoretical plausibility (10) The whole thing should make biologic and epidemiologic sense
on a scientifically conclusive basis, action was taken in the interests of health: “The method of santiation Chadwick introduced probably saved more human lives than any other single health measure up to the post-World War II era. The success of this policy propounded on the basis of a mistaken etiological theory (the miasma theory-the author), was more than a lucky accident. The policy was based on an entirely reasonable inference of causality” [4].
A similar relationship between science and practice which dispenses with the question of scientifically conclusive findings is shown by the action taken by Ignaz Zadek in 1892 in Berlin [S]. Having failed to convince the city council of the necessity to remedy the poor conditions of the unprospertied classes in order to avoid a cholera epidemic he called on the workers to make a list of all deplorable conditions in living and working accommodation, streets and back yards. Many things which were detrimental to health could be publicly discussed and remedied without the necessity of proving the causes of the threatening cholera epidemic scientifically.
In the course of time the change in the spectrum of diseases has also contributed to a change in the relationship of science to practice and in our concep- tion of the causes. It is important to note that it is not chronic illness that has increased (they existed around 1920 to much the same extent for example as chronic tuberculosis, rachitis or war disablement) but in highly developed and developed world diseases with a long period of latency determine the picture of mortality and morbidity.
To the same extent as long periods exist between initiation of the aetiologic process and the onset of signs and symptoms, the relationships are firstly less likely to be recognised subjectively by the population and secondly, as far as science is concerned, immedi- ate evidence diminished. The dispute about whether a social state of affairs represents a health risk was therefore transferred from the political to the scientific field [6]. However, it still remained a politi- cal argument. In these arguments conceptualisation and methodical formulations of the question gained more importance. The argument about the degree of the part attributable to the complex of social factors
in the initiation of diseases via disposition or via exposure took on more concealed and differentiated forms.
2. THE DEVELOPMENT OF SCIENTIFIC CONCEPTS AND METHODOLOGICAL
REQUIREMENTS
Allocating controversal problems which need to be explained in the social context to the field of science has stimulated the development of extremely varied. abstract designs of reality, each with typical facit assumptions. Specific explanations are required and the evidence of conclusive findings is controlled by criteria for causation. These three aspects are to be treated in the following paragraphs.
2.1. Criteria for causation
In order to examine regular potential risks of disease Evans formulated ten criteria for causation, derived from the postulate of Henle and Koch. These are outlined in Table 1 [7]. For each disease in question these criteria can however only be fulfilled in the course of several decades. Some cannot be fulfilled at all due to the limitations of methods, as Evans emphasises. In order not to make scientifically conclusive statements impossible it is wise to treat the criteria for individual groups of diseases flexibly. For example, evidence from laboratory experiments will hardly be possible for many psychic disorders. On the other hand when assessing the cancerogenety of toxic chemical agents which have been introduced for the first time into the working environment, one should be able to rely solely on laboratory experiments.
Treating the criteria flexibly is also necessary for the work situation, if one wishes to protect employees from harm. In view of this practically preventative aspect the relationship between permanent existence of potentially dangerous working conditions and latency of diseases is of importance. If the latency of a disease is not too long and the working conditions are constant, epidemiological studies can be designed to assess risks within a reasonable time. If the latency is long and if it is likely that putative risks will disappear along with technical changes before it is
Working conditions and health 361
possible to determine the connections scientifically, laboratory experiments are more suitable for ascer- taining health risks at an early date.
It is incumbent on researchers into social epi- demiological stress when proving causality to explain criteria one to four, and if these are fulfilled to conduct intervention studies (criteria 8 and 9). The conclusive evidence of risks having a specific effect in adequately elaborate models of mere science does not necessarily lead to the development and use of prac- tical methods of prevention of risks [8]. This will be dealt with in more detail at the end of this paper.
2.2. The desire to speclyy relationships
A large part of research is determined by the hope of coming across more and more specific connections by means of perseverance and good designs. The desire to attain specifity can be regarded as having four aspects:
(a) Specificity of variables (b) Specificity of the model (c) Specificity by transferring temporarily the ana-
lytical study of pathogenesis to a point nearer to the outcome
(d) Specificity of patterns of stress.
Specificity of variables
McQueen, Siegrist and Thoits stress that a most telling weakness of research into the role of social factors including social support in disease is oversimplification of social variables [9]. This is also the case for descriptions of occupations and com- parison of occupations regarding prevalence and incidence of certain diseases. The variation of ‘stress- ful’ situations within one occupational group is very often greater than the variation of stress factors between different occupations. Therefore inconsistant findings with regard to occupations are not a suitable reason for rejecting diseases caused by working con- ditions.
Specificity may however not only be limited to a means of getting away from global indices. These, as the example of results of the concept of social class. shows, can, in spite of-or indeed because of-their global character, give a good picture of a part of reality. Specificity also means the division of different causative aspects of apparently specific, but in reality multi-dimensional terms. Karasek demonstrates this using the example of the characteristic ‘re- sponsability’. which mixes aspects of the compulsion to make decisions on the one hand with job decision latitudes on the other [IO]. Compulsion can involve problems and represent a health risk. Latitudes, however, can have a protective effect and thus protect from disease. as the employee can regulate on his own authority the degree of other forms of stress. The term ‘responsability’ is therefore too unspecific and has various effects according to the type of work- e.g. a repair mechanic in production or a top manager.
This unsatisfactory specificity of conventional con- cepts can contribute to substantial misinterpretations and inconsistent results [l 11. Also other con- ventionally accepted concepts in stress research, as
for example ‘death of the spouse’ in the ‘life-event- model’ cannot represent a risk per se. It would be necessary to consider stress or loss of support which have a specific effect, and not a meaningless word. Otherwise, because of methodical weakness, it is very easy to come to the conclusion that “situations are not objectively ‘stressful’. . . thus bereavement or divorce may be subjectively defined as extremely disturbing, but only by some, under certain circum- stances, as a relief or as a positive challenge” [12].
A methodological disaster can be observed in nor- mative pigeon-holing (as for example active vs pas- sive) in the case of concretely ascertained behaviour patterns or of situations before the statistical analysis step. Not until the relationships between concrete coping styles and the disease being investigated have been interpreted, is the researcher at liberty to assess the results in a way subjectly comprehensible to others and, then, in some circumstances, to assess them in a more complex manner.
The specificity of the model is a further condition necessary not only to discover specific relationships but also to avoid inconsistent results and consistent misinterpretations. Many studies-particularly in occupational medicine--consider only one or a group of homogenous factors, ignoring the control of other influences. The requirement to design studies so that a wide range of possible contributing factors can be assessed simultaneously is however not yet sufficient. Moreover it is necessary to understand the demands, latitudes, personal dispositions including the conditions of the living and working situation of the persons examined, so that not only many, but also the relevant characteristics are considered in ‘wide range’.
As far as the working situation is concerned it is important to remember in particular the interaction of stress and job latitudes (scope for action and movement at work, etc.). Thus it is seen that stress factors, which previously were regarded as having no effects, can take on substantial significance if job latitudes are specifically taken into account. This happens because part of the protective effect of job latitudes is statistically transferred to the stress fac- tors via positive correlations between both [13]. In order to evaluate the forms of stress properly it is always necessary to consider latitudes at work as well, as in any case work consists not only of stress but also of certain freedoms.
A further attempt to attain specificity of relation- ships takes place when one transfers the analytical study during the latency of the disease to a point temporally near the onset of symptoms or the out- come. There is no doubt that relationships become all the more specific the closer and nearer the connection between risk and disease: the first prodromes of disease are the best predictors. The success of moving the analytical study forward on the’temporal axis from the initiation of the aetiologic process in the direction of the onset of symptoms and outcomes does however have serious consequences. Firstly, predictors which show specific relationships because of their temporal proximity to the disease are often banal in the aetiologica explanation and permit hardly any preventive measures being taken against the development of the disease. Secondly, it is poss-

362 WILFRED KARMAUS
ible that, according to the stage at which analytical studies are made in the process of development. different cause and effect mechanisms are discovered. Thus, for example, in the first phases of the career of female legal drug (ab)use, factors of the work situ- ation such as pressure of time among others or self medication play a role. In later phases of this career visits to the doctor and prescriptions are of greater importance [14]. Therefore, if the time alone is for- mally considered and not the special features pre- vailing, a different interpretation of predictors can result at various ages. This circumstance is however not to be equated with the fact that the explanatory approaches are contradictory.
Thus, it is wise in the case of a protracted process of development of the disease, to establish not only explanatory models for the precursors of the disease (e.g. level of cholesterol, deviations in blood pressure) as dependent variables, but also to set up explanatory models for the disease as dependent variables as well as precursors and other influences as independent variables. For in fact one can seldom expect that at the end of the process a specific relationship can still be established for the real causes which brought about the process of disease.
A fourth possibility to attain specificity takes pat- terns of stress into consideration. When different stressors or protective factors of a defined disease are indentified, it is of interest to discover the group of predictors (e.g. by cluster analysis) which are typi- cally common to the working situation. The basis of this consideration is that atomised effect mechanisms alone are hardly of significance, but the whole is important as an interaction of factors having hetero- genous effects. Gathering factors which are typically common to the working situation is not to be under- stood as an attempt to discover different patho- genetically relevant patterns, but to demonstrate the simultaneous incidence of risks and protective factors in various groups of employees in various phases in the development of organisation and mechanisation at work. By using this information, risk situations and groups enduring a great deal of stress can be identified. In this way too the loss of information which arises when specifiying singular relationships (e.g. in the comparison of unspecific descriptions of social classes) can be partially regained. As here in the specification of multiple patterns of inputs it is possi- ble to proceed in a similar way in the case of patterns of multiple outcomes [ 151.
After this outline of methodological requirements for social epidemiologic investigations which examine the significance of social factors in the initiation of disease, the next section will deal with the spectrum of explanatory approaches. This leads on to the third part which discusses the problems of the various approaches taken in stress research.
Explanatory approaches
Because of the different methods of conceptualising environments, agent and host in various explanatory approaches, the opportunity of ordering these according to the criteria ‘specific vs unspecific’ and ‘exposure vs disposition’ presents itself. The emphasis on specific exposure introduced the development of the concept of contagion or concept qf’specific agents.
The assumption is that an external factor can disturb the inner function or structure of an individual. an organ or a cell. Explanations of infectious diseases, the risk factor model and approaches to occupational medicine belong to this type of model.
Nevertheless, the concept of specificity for infec- tious diseases has a lot of limitations. The establish- ment of a causal relationship of a given virus with a given syndrome became possible only under special circumstances; and a number of common illness existed in which several agents could produce the same clinical picture [16].
The characteristics of the risk factor model exist on the one hand in the lack of differentiation between exogenous and endogenous factors and on the other hand in the equation of social facts with events within the scope of physical objects in natural science. In this way cigarette smoking and cholesterol level are treated as being on the same plane [17]. These weaknesses are caused by the lack of concep- tualisation of the environment, for if a coronary artery alone is observed, everything which has an effect on it is exterior, irrespective of whether it is caused by circumstances, by behaviour or is genetically determined.
The distinctive feature of explanations in occupational medicine is found in the reductionistic conception of causes of occupational diseases. This conception recognises no auxiliary effects, no ade- quate effects but only adequate main effects. To clarify this differentiation it must be noted that the ‘Auxifliations-Theorie’ assumes that factors, which alone are themselves not causative but have a patho- genic effect when interacting with others, are also valid as causes. The ‘Adiiquanz-Theorie’ emphasises that only those factors which are also the cause of disease in their own right can be considered to be main or secondary causes [18]. However, only those factors which are adequate and major causes can lead to an occupational disease [19]. Other developments are determined by fate. This conception limits all scientific analysis of occupational risks. Furthermore, at least in West Germany, tradition in the held of occupational medicine has led to the emphasis in analysis being placed on the material dimensions in the field of work and not on psychological or or- ganisational aspects.
In analogy to the emphasis on specific exposure in the above described approaches, the assumption of a specific disposition in the case of infections diseases led to the development of the concept of immunity and of host resistance. Genetic models of diseases are another variant of a specific disposition effect. The concept of specific agents and the concepts of immu- nity and host resistance were combined in ecological models. Yet specific agent and human host do not however act alone; they are complemented by specific (and unspecific) auxiliary effects of the environment [201.
Concepts of unspecific exposure and unspecific disposition must in principle be differentiated from these models of specific effects. It is necessary to mention the following concepts here: that of social class on the level of social explanations and that of stress on the level of individual explanation.
The concept of social class is rather unspecific
Working conditions and health 363
when global inequalities are described, the concrete causes of which remain open. They may be obtained via unspecific exposure conditions such as economic reality, occupation, living conditions, family struc- ture or indirectly via unspecific disposition conditions such as nutritional state, level of professional edu- cation, etc. In the case of the concept of social class it is paradoxical to note that although extremely different definitions of social classes are applied, the scientific validity of which is doubted, empirical results are surprisingly consistent [21]. It must there- fore be assumed that, in spite of their over- simphcation, they grasp an aspect of reality in some way or another.
The stress approach also proceeds from the prem- ise of unspecifity of esposure and disposition. This thesis is postulated because in the original conception the same stimuli can have varied reactions as results, but also the same reactions occur in the case of various stimuli [22]. As far as the agent is concerned, there is an analytical difference between two com- ponents: the specific, characteristic effect and an unspecific stressor effect. The specific component causes, for example, hypacusis in the case of noise, the unspecific component (= stressor) results in a stereotype physiological or behavioural reaction to noise.
retically possess wide integrative scope. In contrast to the risk factor model, the inner structure of which tends to be empiric and atheoretical, specific con- cepts to include the social and material environment as well as more specific effect mechanisms are elabo- rated in the stress approach [25]. The integration of medical risk factors in the stress approach therefore appears to be more effective than the converse method. The concept can therefore contribute to answering the question of what significance can be attributed to the complex of social causes in the initiation and development of disease. The various further developments of the stress approach are to be examined in the next section of this paper in respect to their significance and strength of evidence as far as the working situation is concerned.
3. WORKING CONDITIONS AND THE CONCEF’T OF STRESS
In previous decades a series of concepts were
A one-to-one relationship exists for hypacusis, as the noise is, as it were, the only cause. The phys- iological or behavioural reaction could also occur because of other causes (fire, etc.). Type and extent of the reaction are unspecifically influenced by the existing homeostatic equilibrium on the dispositional side. As an aetiologic concept the stress concept requires additional specific explanations, which, either acquired or genetically determined, establish the locus of the disease (e.g. heart or stomach) as locus minoris resistentiae.
developed to examine the relationship between envi- ronmental conditions and disease and to explain illness. Most of these models have their origin in the stress approach. The aim of this paper is not to continue with fruitless discussions about what stress is. The stress model is regarded here as a heuristic device for clarifying and integrating existent research and suggesting critical areas for further research [26].
Apart from the simple example of noise, it is problematical in empiric studies to divide specific and unspecific parts. When developing the stress concept futher with regard to transactional and the interactional aspects, the corresponding attempt is also made to expose specific effect mechanisms [23].
Almost all the various stress models had, until the time of their zenith, a charismatic significance for social epidemiological research. Each of them empha- sises single aspects of the working situation. Only a few have managed to integrate different views in such a way that their results remain stable, even when other aspects are controlled. Only a few have man- aged to identify occupational risks which are suitable for initiating attempts to humanise working condi- tions by (a) combining strength and frequency of influence and (b) by making practical suggestions.
This sketch of various aetiological approaches is to show that the argument about the significance of a social cause of disease is basically already settled by the choice of research approaches. Social factors are excluded to a great extent in the concept of specific agents, in the concept of immunity and host resistance, and in the concept of risk factors. It is only through the back door that social epidemiologic approaches regain significance (and that only second- ary), for example when it is a question of social dependence of the defensive condition (e.g. Immu- nocompetence) or of risk factors being derived from the second context [24]. Entirely on the pre-scientific level the dispute in the field of explanation of occupational diseases seems to be settled. In this respect the choice of the particular research approach and thus of the later result is already determined by tacit ideologic assumption.
So far no satisfactory explanation and system- isation of the different research approaches have been found which is recognised by the scientific commu- nity. Therefore all attempts at ordering give the impression of being arbitrary, just as the following attempt seems to be. It is orientated on each of the examined dimensions and their conception in various approaches. The first step is to order the central dimensions, as for example demands, social support, personality patterns, coping etc., in the areas ‘dispo- sition’ and ‘exposure’ according to their origins, and in the groups ‘risks’ or ‘protectors’ according to their success (Table 2). The second step is then to observe the interaction of exposure and disposition.
Contrary to the global survey of aetiological expla- natory models, their subject area and conception of causes, in Section 2.3, the attempt will be made in the following to describe the conception of the subject area and the degree of specificity of the models more concretely and with regard to the role played by working conditions.
3.1. Research area ‘exposure’
Consistent results can only be expected if contro- Conditions of environment, whether they are pro- versial approaches can be taken into consideration in tective or harmful, can have an effect on state of a methodologically appropriate way. Not only the health and also on the individual disposition via concept of risk factors but also the stress concept theo- physical or psychological mechanisms. McGrath has
364 WILFRIED KARMAUS
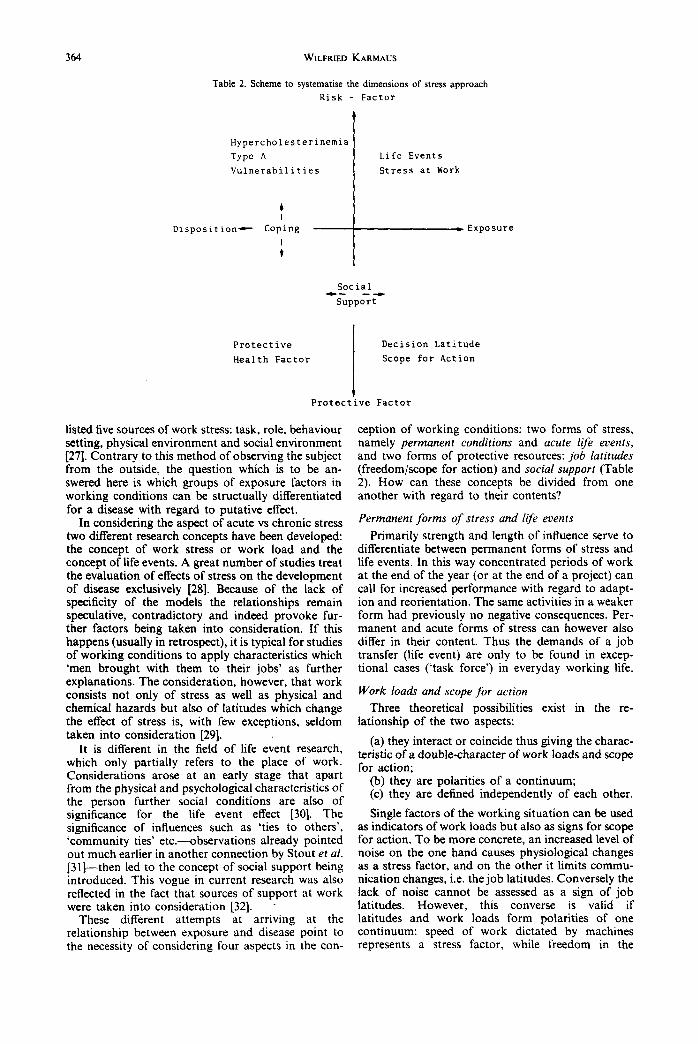
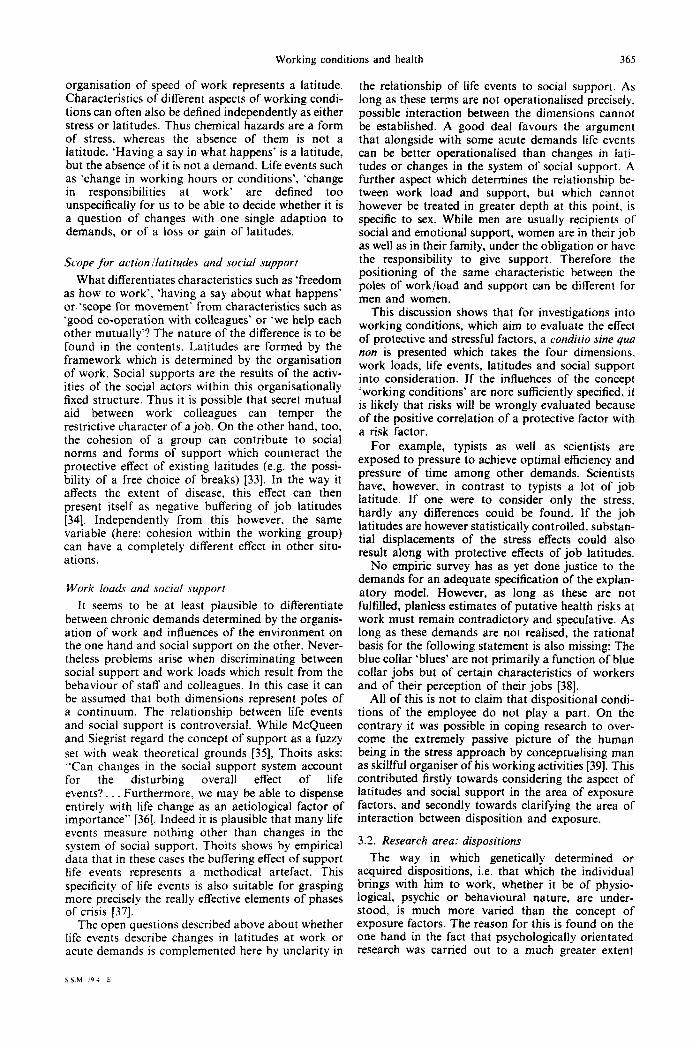
Table 2. Scheme to systematise the dimensions of stress approach
Risk - Factor
Hypercholesterinemia I Typo A Life Events
Vulnerabilities Stress at Work
Disposition- Coping
i -I---- Exposure
Social Ir- --
Support
Protective Decision Latitude
Health Factor Scope for Action
t Protective Factor
listed five sources of work stress: task, role, behaviour setting, physical environment and social environment [27]. Contrary to this method of observing the subject from the outside, the question which is to be an- swered here is which groups of exposure factors in working conditions can be structually differentiated for a disease with regard to putative effect.
In considering the aspect of acute vs chronic stress two different research concepts have been developed: the concept of work stress or work load and the concept of life events. A great number of studies treat the evaluation of effects of stress on the development of disease exclusively [28]. Because of the lack of specificity of the models the relationships remain speculative, contradictory and indeed provoke fur- ther factors being taken into consideration. If this happens (usually in retrospect), it is typical for studies of working conditions to apply characteristics which ‘men brought with them to their jobs’ as further explanations. The consideration, however, that work consists not only of stress as well as physical and chemical hazards but also of latitudes which change the effect of stress is, with few exceptions, seldom taken into consideration [29].
It is different in the field of life event research, which only partially refers to the place of work. Considerations arose at an early stage that apart from the physical and psychological characteristics of the person further social conditions are also of significance for the life event effect [30]. The significance of influences such as ‘ties to others’, ‘community ties’ etc.-observations already pointed out much earlier in another connection by Stout et al. [31]-then led to the concept of social support being introduced. This vogue in current research was also reflected in the fact that sources of support at work were taken into consideration [32]. .
These different attempts at arriving at the relationship between exposure and disease point to the necessity of considering four aspects in the con-
ception of working conditions: two forms of stress, namely permanent conditions and acute life events, and two forms of protective resources: job latitudes (freedom/scope for action) and social support (Table 2). How can these concepts be divided from one another with regard to their contents?
Permanent forms of stress and life events
Primarily strength and length of influence serve to differentiate between permanent forms of stress and life events. In this way concentrated periods of work at the end of the year (or at the end of a project) can call for increased performance with regard to adapt- ion and reorientation. The same activities in a weaker form had previously no negative consequences. Per- manent and acute forms of stress can however also differ in their content. Thus the demands of a job transfer (life event) are only to be found in excep- tional cases (‘task force’) in everyday working life.
Work loads and scope for action
Three theoretical possibilities exist in the re- lationship of the two aspects:
(a) they interact or coincide thus giving the charac- teristic of a double-character of work loads and scope for action;
(b) they are polarities of a continuum; (c) they are defined independently of each other.
Single factors of the working situation can be used as indicators of work loads but also as signs for scope for action. To be more concrete, an increased level of noise on the one hand causes physiological changes as a stress factor, and on the other it limits commu- nication changes, i.e. the job latitudes. Conversely the lack of noise cannot be assessed as a sign of job latitudes. However, this converse is valid if latitudes and work loads form polarities of one continuum: speed of work dictated by machines represents a stress factor, while freedom in the
Working conditions and health 365
organisation of speed of work represents a latitude. Characteristics of different aspects of working condi- tions can often also be defined independently as either stress or latitudes. Thus chemical hazards are a form of stress, whereas the absence of them is not a latitude. ‘Having a say in what happens’ is a latitude, but the absence of it is not a demand. Life events such as ‘change in working hours or conditions’, ‘change in responsibilities at work’ are defined too unspecifically for us to be able to decide whether it is a question of changes with one single adaption to demands, or of a loss or gain of latitudes.
Scope &or action /latitudes and social support
What differentiates characteristics such as ‘freedom as how to work’, ‘having a say about what happens’ or-‘scope for movement’ from characteristics such as ‘good co-operation with colleagues’ or ‘we help each other mutually’? The nature of the difference is to be found in the contents. Latitudes are formed by the framework which is determined by the organisation of work. Social supports are the results of the activ- ities of the social actors within this organisationally fixed structure. Thus it is possible that secret mutual aid between work colleagues can temper the restrictive character of a job. On the other hand, too, the cohesion of a group can contribute to social norms and forms of support which counteract the protective effect of existing latitudes (e.g. the possi- bility of a free choice of breaks) 1331. In the way it affects the extent of disease, this effect can then present itself as negative buffering of job latitudes [34]. Independently from this however, the same variable (here: cohesion within the working group) can have a completely different effect in other situ- ations.
Work loads and social support
It seems to be at least plausible to differentiate between chronic demands determined by the organis- ation of work and influences of the environment on the one hand and social support on the other. Never- theless problems arise when discriminating between social support and work loads which result from the behaviour of staff and colleagues. In this case it can be assumed that both dimensions represent poles of a continuum. The relationship between life events and social support is controversial. While McQueen and Siegrist regard the concept of support as a fuzzy set with weak theoretical grounds [35], Thoits asks: “Can changes in the social support system account for the disturbing overall effect of life events?. . . Furthermore, we may be able to dispense entirely with life change as an aetiological factor of importance” [36]. Indeed it is plausible that many life events measure nothing other than changes in the system of social support. Thoits shows by empirical data that in these cases the buffering effect of support life events represents a methodical artefact. ‘This specificity of life events is also suitable for grasping more precisely the really effective elements of phases of crisis [37].
The open questions described above about whether life events describe changes in latitudes at work or acute demands is complemented here by unclarity in
the relationship of life events to social support. As long as these terms are not operationalised precisely, possible interaction between the dimensions cannot be established. A good deal favours the argument that alongside with some acute demands life events can be better operationalised than changes in lati- tudes or changes in the system of social support. A further aspect which determines the relationship be- tween work load and support, but which cannot however be treated in greater depth at this point, is specific to sex. While men are usually recipients of social and emotional support, women are in their job as well as in their family, under the obligation or have the responsibility to give support. Therefore the positioning of the same characteristic between the poles of work/load and support can be different for men and women.
This discussion shows that for investigations into working conditions, which aim to evaluate the effect of protective and stressful factors, a conditio sine qua non is presented which takes the four dimensions, work loads, life events, latitudes and social support into consideration. If the influehces of the concept ‘working conditions’ are nore sufficiently specified, it is likely that risks will be wrongly evaluated because of the positive correlation of a protective factor with a risk factor.
For example, typists as well as scientists are exposed to pressure to achieve optimal efficiency and pressure of time among other demands. Scientists have, however, in contrast to typists a lot of job latitude. If one were to consider only the stress, hardly any differences could be found. If the job latitudes are however statistically controlled, substan- tial displacements of the stress effects could also result along with protective effects of job latitudes.
No empiric survey has as yet done justice to the demands for an adequate specification of the explan- atory model. However, as long as these are not fulfilled, planless estimates of putative health risks at work must remain contradictory and speculative. As long as these demands are not realised, the rational basis for the following statement is also missing: The blue collar ‘blues’ are not primarily a function of blue collar jobs but of certain characteristics of workers and of their perception of their jobs [38].
All of this is not to claim that dispositional condi- tions of the employee do not play a part. On the contrary it was possible in coping research to over- come the extremely passive picture of the human being in the stress approach by conceptualising man as skillful organiser of his working activities [39]. This contributed firstly towards considering the aspect of latitudes and social support in the area of exposure factors, and secondly towards clarifying the area of interaction between disposition and exposure.
3.2. Research area: dispositions
The way in which genetically determined or acquired dispositions, i.e. that which the individual brings with him to work, whether it be of physio- logical, psychic or behavioural nature, are under- stood, is much more varied than the concept of exposure factors. The reason for this is found on the one hand in the fact that psychologically orientated research was carried out to a much greater extent
366 WILFRIED KARMAUS
than job research. On the other hand the conceptions are more complex, as exterior conditions of culture, of training and working and living conditions also precipitate in individual dispositions. This section will deal with differentiation of the direction of effect, i.e. protection or harm. The theme of the next section will be the interaction of exposure and disposition taking the following aspects into consideration: stable vs variable disposition and direct vs interactive effects.
Apart from some exceptions all physiological dis- positions are conceived as risks 1401. All pathogenic factors for coronary heart diseases, cancer and degen- erative rheumatic diseases belong to this group. These influences have been investigated within the frame- work of risk factor medical research, mostly without exposure control factors being present [41].
Psychological constitutions are described not only as risks (Type A [42], vulnerabilities, hopelessness [43]) but also as protectors (resistence sources 1441, hardiness [45]). In order to measure personal disposi- tions a large number of characterisations and tests have been elaborated. Mechanic points out that in the development of research the theoretical basis for conducting tests is usually not plausible, or it was forgotten. Nevertheless many of these tests continued to be employed as a standardised measure [46] if they were simply enough.
On the level of behaviour at least two different conceptions can be differentiated. In the first ap- proach ‘health-protective-behaviour’ or ‘preventive- health-behaviour’ [47], the putative direction of influence is determined according to the moral atti- tude of the researcher. This does not mean to say that the health behaviour investigated is also attributed with the predicted effect [48]. This investigation of subjective behaviour has a great deal of similarity to research into medical risk factors. It is not necessary to have for this a conception of every-day activities to cope with life but-as criticised by von Ferber-it is a question of an utilitarian group of behaviour patterns, orientated on the utilitarianism of the med- ical utopia ‘health’ [49]. Questions are considered as relevant which refer to the areas of cigarette smoking, physical activity, alcohol consumption, sleeping pat- terns, wearing of car seat belt, taking vitamins, etc.
In the second approach, the coping concept, no protective or harmful effect is postulated a priori. Dealing with and the course of transactional pro- cessing of stress is theoreticised [50]. While the term ‘coping’ was originally limited in laboratory research to non-routine behaviour which indicates a creative and reflective adaption under difficult conditions [51], the term in empirical research has been extended to all processes of dealing with stress 1521. The terms ‘problem solving’, ‘adaption’, ‘defense’, ‘mastery’ and ‘adjustment’ are not clearly defined and are used differently by many authors [53]. In each case they thematicise different possibilities of coping with stress.
The main difference of the coping approach towards the previously described dispositional factors is to be found in the way an extremely passive picture of the human being is overcome [54]. Man is not only seen as a passive bearer of characteristics, who, when bombarded by stress factors, is variously susceptible to illness according to his constitution, but he is also
regarded as a being who can change himself and his environment to reduce stress or to create new chal- lenges for himself. On the basis of the conception of an active role, abilities, skills. values and needs, can also be integrated into this approach [55] which have in the past played only a marginal role [56]. These aspects are of salient significance for the way coping styles express themselves, either as change or adapt- ion.
The boom in research into coping has however made the borders to health behaviour indistinct. There is an inflatory use of the term ‘coping’. In order to bring out the differences it is necessary to return to basis consideration. Coping should not represent any arbitrary further factor in its own right as far as the initiation of disease is concerned, but-thus the assumption-the relationship between exposure to stress and strain or disease is contingent on the state of coping. This means that coping (c) represents either an intervening variable between exposure (e ) and disease (d) (e--t c -+ d) or, however, coping enters into interaction with stress and thereby mod- erates the relationship of exposure to disease (e x c -+ d) [57]. The result of these assumptions is that for coping research a conditio sine qua non is to consider simultaneously each of the sources of stress which must be coped with [58].
In the design of the assessment the coping approach has until now hardly done justice to the conceptional requirement of analysing the concrete every-day patterns of dealing with stress [59]. The aim of most analysis is to identify single effective coping variables. This results in single form of behaviour, which are very likely to follow one after the other or to be interlocked, being placed arbitrarily in alterna- tive positions. For example, ‘self-reliance’ vs ‘advice- seeking’ belong to these [60]. In order to be able to identify these patterns of coping, which as patterns have, under certain circumstances, a quite different effect from atomised variables of behaviour, it would be necessary to carry out structure analysis or cluster analysis. It is then of interest to compare the ‘patterns of stress, latitudes and support’ with ‘patterns of coping’ and ‘multiple outcomes’.
Dispositional factors as a whole are given credit for the fact that their correlation to strain. symptoms or outcomes is usually more obvious than those of the objective environment. However, only with care should this advantage be interpreted as indicating that dispositional factors in the initiation of disease play a relatively large part. Before this happens, two possible methodological artefacts are to be consid- ered: (1) as described in Section 2.2. more specific and stronger relationships can then become visible if one conducts the analytical survey at a point approaching the onset of syndromes. This trick is however often limited to subjectively measurable factors-as for example predisposition. (2) Unfortunately, the for- mulation of stress as subjective in nature as well as the self-report of a lot of predispositions (with the exception of physiological risks) has led to a self- serving trap which trivialised a good deal of research on stress: the measurement of the independent vari- able and the measurement of the dependent variable (strain, symptoms) are sometimes so close oper- ationally that they appear to be simply two similar
Working conditions and health 367
measures of a single concept [61]. (The same objec- tion is also valid for subjective surveys of exposure.) Kasl sees ways out of this triviality trap firstly by objective measuring, whereby objective means that income and outcome data are not supplied by the self-same respondent; secondly by operationalising two conceptually distinct variables as differently and as independently as possible [62].
Focusing alone on dispositional concepts without simultaneously considering situational conditions, which, in the case of the coping concept it is certainly imperative to do, represents a tacit assumption in favour of analagous results. Also a focus exclusively on intra-psychic phenomena tends to over-look the role of behaviour coping responses.
Independent of the fact whether dispositions as for example the classical risk factors explain a good part of the variance, it is a methodical weakness not to consider the exposures. For these could also have a substantial influence on the extent of predispositions or would have an effect only when interacting with the constitutional make-up. The question in how far personal peculiarities constitute intervening variables of the working situation or in how far they interact with them will be dealt with in the next section.
3.3. The interaction of exposure and disposition
Long existing controversies centre around the par- ticular significance given to exposure and disposition factors, for example (1) is the situation objectively stressful or just a subjective assessment characterised by individual peculiarities? (2) Should dispositional factors be analysed as stable personality patterns or as coping mechanism? (3) In how far are dispositional factors a reaction to working conditions?
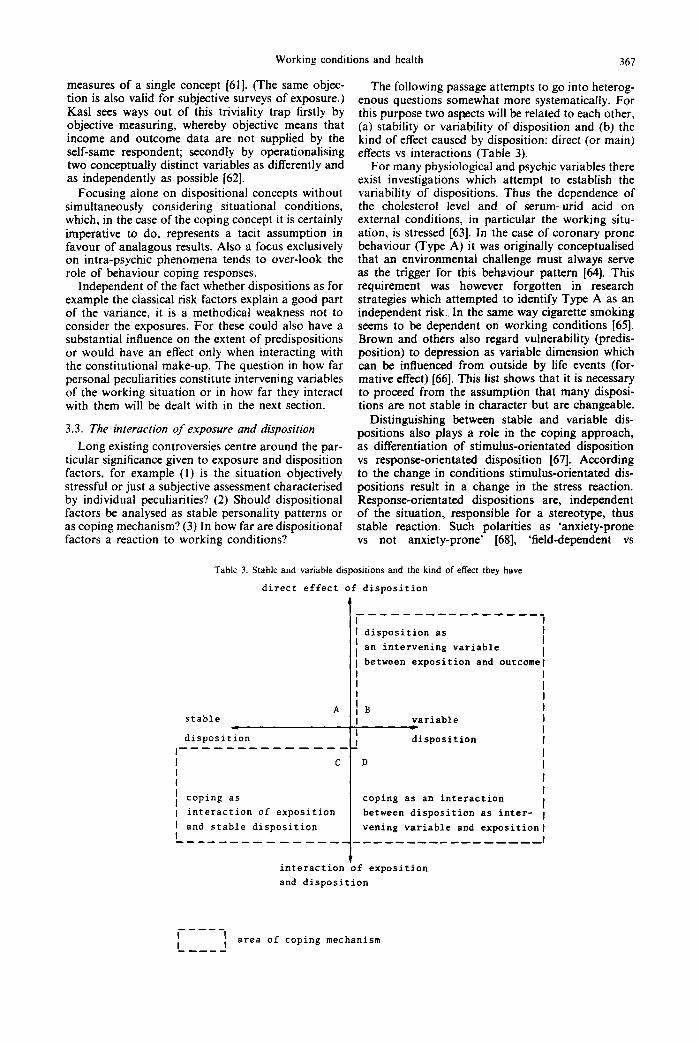
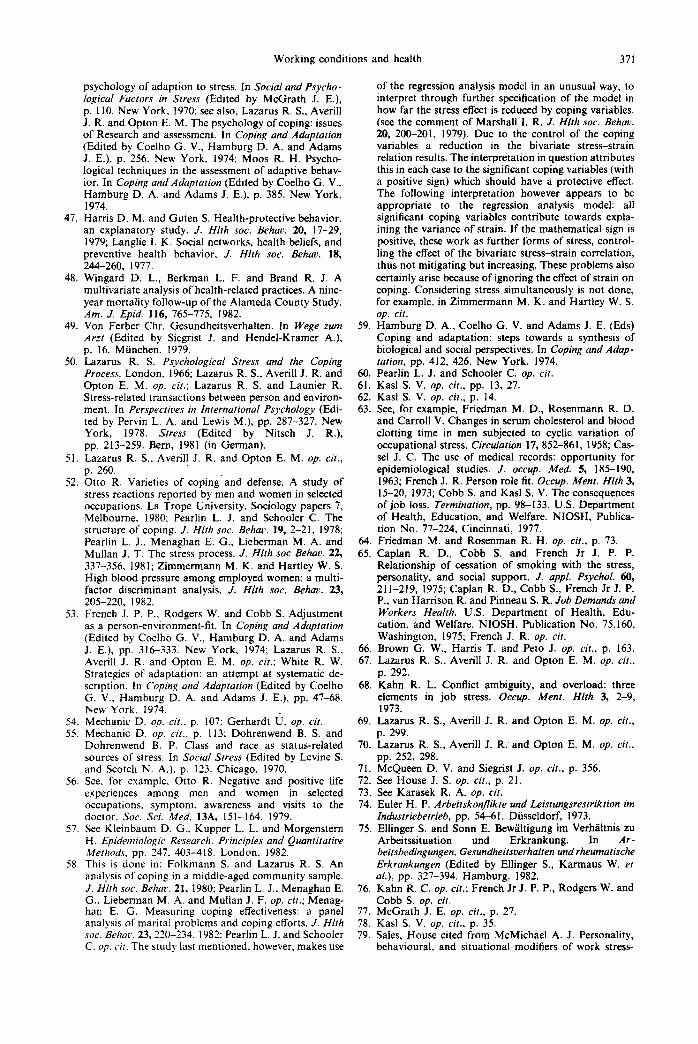
The following passage attempts to go into heterog- enous questions somewhat more systematically. For this purpose two aspects will be related to each other, (a) stability or variability of disposition and (b) the kind of effect caused by disposition: direct (or main) effects vs interactions (Table 3).
For many physiological and psychic variables there exist investigations which attempt to establish the variability of dispositions. Thus the dependence of the cholesterol level and of serum-urid acid on external conditions, in particular the working situ- ation, is stressed [63]. In the case of coronary prone behaviour (Type A) it was originally conceptualised that an environmental challenge must always serve as the trigger for this behaviour pattern [64]. This requirement was however forgotten in research strategies which attempted to identify Type A as an independent risk.. In the same way cigarette smoking seems to be dependent on working conditions [65]. Brown and others also regard vulnerability (predis- position) to depression as variable dimension which can be influenced from outside by life events (for- mative effect) 1661. This list shows that it is necessary to proceed from the assumption that many disposi- tions are not stable in character but are changeable.
Distinguishing between stable and variable dis- positions also plays a role in the coping approach, as differentiation of stimulus-orientated disposition vs response-orientated disposition [67]. According to the change in conditions stimulus-orientated dis- positions result in a change in the stress reaction. Response-orientated dispositions are, independent of the situation, responsible for a stereotype, thus stable reaction. Such polarities as ‘anxiety-prone vs not anxiety-prone’ [68], ‘field-dependent vs
Table 3. Stable and variable dispositions and the kind of effect they have
direct effect of disposition
I, --_-_-----_-----_
I i disposition as I an intervening variable
i I between exposition and outcome1
I
A I stable
I B I variable I c
disposition I disposition I ---------------
C D I I
i coping as coping as an interaction
1 interaction of exposition I
between disposition as inter- 1 1 and stable disposition vening variable and exposition1 I --_----------- _________________ I I
interaction of exposition
and disposition
--w-m
I I I
area of coping mechanism a----
368 WILFRIED KARMAUS
field-independent’, etc. [69] belong to stimulus- orientated dispositions. The response-orientated dis- positions describe dichotomies such as ‘Type A vs Type B’, ‘extroversion vs introversion’ ‘overcontrol vs undercontrol’ and many others [70]. If at the same time one proceeds from stable patterns, this is not contradictory to the conception of coping, as stable personality pattern and coping mechanism are not alternatives, as sometimes assumed [71]. In the anal- ysis of coping mechanisms the kind of effect alone is of significance.
As Table 3 shows, there exist at least four possi- bilities in the relationship exposure-disposition and interactive vs direct effect. If only direct effects of disposition come into question, there remain two possibilities. (A) Disposition is stable and has a direct effect, i.e. working conditions play no role. (B) Dispo- sition is influenced partially by working conditions, but has a direct effect as for example cigarette smoking on lung cancer. In this case part effects of cigarette smoking can be understood as an inter- vening influence between stress and disease. If it is necessary to proceed from effects interacting between exposure and disposition, then this must be done on the one hand from the interaction between stable disposition and working conditions (C) and on the other hand from the interaction between variable disposition and working conditions (D). In the case of (C) for example, the interaction between the coronary prone pattern, Type A, and high demands can lead to an over-additive increase of stress, i.e. to un- favourable coping with demands. Case (D) can lead to a ‘cumulative mess’ if conditions are adverse, for activity which is favoured by the working situation has an additional effect in interaction with the work- ing situation. It can for example be imagined that restrictive and monotonous work can contribute to a reduction in physical activity. Both together may lead interactively to diseases of the musculo-skeletal apparatus.
As this description has shown in three (B-D) of these four possibilities we may speak of coping mechanisms, as the dispositions represent reactions to demands or contribute to dealing with forms of stress, the direct effect of which is modified by how they are dealt with. This complex way of regarding matters can also contribute towards clarifying the argument about whether it is objective or subjective stress which is of greater significance. Let us assume that the effects in Table 3 are directed at strain, i.e. at the subjective experience of stress. Then it becomes clear that in cases (B)-(D) subjective stress represents a result of the interaction of objective stress and the constitutional make-up [72]. Case (A) is a special case in as far as disposition has a direct effect of its own. The converse is also imaginable for exposure only in special cases. Due to this interaction subjective values can correspond to the objective one [73] but they can also manifest themselves as being not only clearer but also weaker than the objective conditions. The devi- ations and their consequences are to be described in greater detail.
As research into conflicts at work has shown, a conflict can be settled directly or there is a change in addressee and or content [74]. The same can be assumed for the assessment of stress. Thus in a survey
of female employees no equivalent for objective stress caused by environment and technical equipment could be found in the perception of strain. On the other hand being closely tied to the job with little variety and scope for movement plays a considerable role in the perception of environmental stress at work [75]. In the same survey it is seen that a stressful relationship to the superior can easily be explained by restrictive working conditions. On the one hand it is possible that the superior is made responsible for restrictive conditions, on the other hand it can be assumed that the women have offered resistance to the restrictive conditions and thus have risked contlict with the superior.
In the first case it becomes clear that what is objectively present need not be perceived as subjec- tive or stressful. Nevertheless these ergonomic prob- lems can affect the state of health, moreover probably more strongly in cases where the employee is tied to the job. In the second case objective facts are tiot perceived as such but are transferred to subjectively tangible persons. This does not however mean that a change in superior would bring about an im- provement of the working situation of the women. Only a reduction in restrictiveness could solve the problem. These false parallels between objective and subjective conditions can therefore lead measures to humanise life at work astray, unless the objective constellations are at least taken into consideration.
This differentiation shows that the objective situ- ation as well as the subjective assessment can be stressful; that in the case of subjective evaluation however, processes of changing the emphasis and of personalisation must firstly be taken notice of; and that secondly the subjective assessment can give clues to the interactive effect of two forms of stress (here: simultaneous effect of being tied to the job and demands of the working environment).
The interaction of disposition and exposure cannot be treated without mentioning the person-environ- ment-fit approach [76]. This attempt at a role the- oretical approach postulates an objective environ- ment and person as well as their subjective pendants. A misfit of the relationships between these four categories is seen as an opportunity for changing the person or the environment, with the aim that tech- niques of adjustment serve to establish a fit. In the case of this construct, moreover, it does not become clear which supporting theoretical assumptions are necessary if one changes from functionalistic homeo- stasis on the level of organisation (the right man for the right job) to individual coping on the level of regulation ‘man’. This perception of the misfit re- quires the conception of the model ‘man’. however. It also remains unclear whether a subjective misfit could not immediately be equated with subjective strain. This would lead to the result that a connection between misfit and strain would possess tautological character. Although the concept also considers sup- plies as well as stress, it suffers from an extremely passive picture of the human being. For man, as a skillful organiser of his working activities, could also put up with deviations from the homeostasis or new demands consciously and not term these as misfits.
McCrath emphasises that in this approach the role of physical and chemical factors at work are not
Working conditions and health 369
taken into consideration [77]. Kasl doubts whether the misfit measures represent better predictors than exposure measures [78]. Investigations within the framework of this approach have however produced a number of interesting results, whereby the narrow- ness of this concept was abandoned in favour of the wideness of the stress approach.
In the interaction of exposure and disposition this presentation has until now mainly concentrated on the effects of exposure and on joint influences. Finally it is necessary to deal with dispositional character- istics which can have an effect on exposure. In this case it is not as necessary to remember that employees make their jobs more tolerable as that they look for or leave certain jobs. Thus it is assumed that a Type A person possesses personality traits that, due to desire for social achievement, cause self-selection into jobs that entail greater exposure to stressors [79]. Apart from this drift into particular occupations negative self-selection also occurs. Thus employees leave their jobs because of their impaired state of health. This healthy-worker effect [8] can occur through premature death, premature retirement a change to less stressful jobs or higher positions. Both drift effects distort the relationships between ex- posure, disposition and disease. The first tends to lead to over-evaluations of the role of working conditions, the second drift direction to under-evaluation.
4. THE RELATIONSHIP BETWEEN SCIENCE AND PRACTICAL TRANSFORMATION OF
THE WORKING SITUATION
If one looks at the immense number of in- vestigations and the sum of results which at least do not contradict common sense, the question arises: How can the stress approach, which was developed under laboratory conditions, be so successful when used on reality? According to Holzkamp [81] labora- tory investigations are characterised in that initial conditions are divided up and isolated to such an extent that only the variables defined in the promi- nent hypothesis but not other elements connected to this process produce the effect. Designs of this kind cause a reduction of conditions in total, a fragmen- tation qf reality and a destabilisation in the orientated laboratory emlironment. In accordance with these postulates Young sees investigations in the stress approach limited by decomposability, fragmenting and obscuring of social processes [82). But also the converse interpretation is plausible: the stress concept is applicable in the analysis to the social reality of industrialised countries only because this reality has been formed by fragmentation, reduction of condi- tions in total and destabilisation in the stimulus- orientated working situation because of economic considerations in such a way that it shows a similarity to laboratory conditions [82].
Apart from the question discussed in this analysis:
(I) Which singular factors in the working situation are detrimental to health?
It is also of decisive importance for a change in working conditions to answer the following questions which might well be able to recapture the complexity:
(2) What are the patterns of typical constellations of health risks in the working situation?
(3) What patterns of stress, latitudes and social support and what patterns of coping are related to which multiple outcomes?
The suggestion to take up a mutual position on these questions and on essential scientific criteria in international working groups seems appropriate in order to refer the answers in the form of tasks back to the political arena. Such working group of scientists could help to solve some of the contro- versies about the importance of social causes of disease. They should however also emphasise:
(4) Which areas-e.g. woman, work and stress [84]-have not yet been adequately examined?
The fact, that many scientists have inter- nationalised partialised research under laboratory conditions as mere science is a reason for concern. They avoid stepping into the arena of conflicting class and group interests and taking up position on the questions with regard to political relevance.
In comparison to knowledge about aetiology of infectious diseases we have more theoretical know- ledge yet more practical helplessness for diseases with longer latency. Our methodological flights of fancy in mere science are, as far as practical change is con- cerned, confronted by the limited horizon and world of a mole.
Also, even if we are basically not able or willing to change anything in working life, the lack of readiness to at least point out the dangerous effects observed in stress research becomes obvious, for example in the cases of Lazarus and Launier. Of five possibilities the authors favour that form of coping in which tranquil- lisers are used to control the nervosity of the individ- ual [85]. To put it more pointedly stress research appears to have had only one social effect, namely to legitimise the use of tranquillisers and pain killers and thus to mask the necessity for social change. In this respect Lennard and Cooperstock write [86]: “A number of middle class informants found they ceased use (of tranquillisers-the author) during or after making structural changes in their lives. Are such alternatives open to all members of society? The poor? The elderly? If not, are tranquilizers to be accepted as adequate solutions to social stresses?”
The only cloud with a silver lining seems to be in Scandinavian countries. Thus Garde11 [87] describes legal requirements as possibilities for change. He further emphasises the necessity not to avoid the conflict that often exists between the health and the safety perspective and the technical efficiency of our production system. Social epidemiologic stress research will then be successful when it can prove scientifically what is already known by most working people.
I.
2.
REFERENCES
Mosse M. and Tugendreich G. Krankheir und SoSale Lage, Berlin. 1913 (Re-edited by Cromm J.). p. 4. Giittingen. 1977. Mosse M. and Tugendreich G. op. cir.. p, 19.
370 WILFRIED KARMAUS
3.
4.
Hirsch A. Uber die historische Entwicklung der iiffentlichen Gesundheitspflege. Berlin, 1889. Susser M. Causal thinking in the health sciences. Con- cepts and Strategies of Epidemiology, p. 51. New York, 1973.
28.
5. 29.
Labisch A. Selbsthilfe zwischen Auflehnung und An- passung. Arbeiter-Sanitltskommission und Arbeiter- Samariterbund. Argument-Sonderband AS 77. Alter- nat. Mediz. 11-26, 1983. Maschewsky W. Zum Stand der Belastungs- und Bean- smuchunasforschung. Soziale Welt 33, 328-345, 1982. E%ans A_ S. Causafion and disease: ;he Henle-Koch postulates revisited. Yale J. Biol. Med. 49, 192, 1976. Evans 4. S. op. cit., p. 190. McQueen D. V. and Siegrist J. Social factors in the etiology of chronic disease: an overview. Sot. Sci. Med. 16, 353-354, 1982; Thoits P. A. Conceptual, meth- odological, and theoretical problems in studying social support as a buffer against life stress. J. Hlth sot. Behau. 23, 146-148, 1982. Karasek R. A. Job demands, job decision latitude, and mental strain: implications for job redesign. Admin. Sci. Q. 24, 268, 1979. Karasek R. A. op. cit. Shuval J. T. The contribution of psychological and social phenomena to an understanding of the aetiology of disease and illness. Sot. Sci. Med. 15A, 338, 1981. Karmaus W. and Schafer K. H. Rheumatic diseases of female office-workers: the importance of medical risks. working conditions and coping as determinants of chronic complaints. Sot. Sci. Med. In press. Ellinger S., Karmaus W. and Mischo M. Frauen und Medikamente. Epidemiologie, Erkllnmgsansltze und Vorschlage zur Privention. Unpublished Paper, Ham- burg, 1984. McQueen D. V. and Celetano D. D. Social factors in the etiology of multiple outcomes: the case of blood pres- sure and alcohol consumption patterns. Sot. Sri. Med. 16, 397-418, 1982. Evans A. S. op. cit. p. 181. Karmaus W. Das Konzept der Risikofaktoren als mii- glicher Beitrag zur .&ologieforschung. Argument- Sonderband AS 37. Jahr. Krit. Mediz. 6-42. 1979. Kries J. U., according to Curtius F. Individuum und Krankheil, p. 64. Berlin, 1959. See for instance Valentin H., Lehnert G. et al. (Eds) Arbeitsmedizin, Bd. I, pp. 265-282. Stuttgart, 1979. Susser M. op. cit., pp. 26-32. Gleiss J., Seidel R. and Abholz H. Soziale Psychiatric. Zur Ungleichheil in der psychialrischen Versorgung, p. 30. Frankfurt, 1973; Townsend P. and Davidson N. (Eds) Inequalities in Health. The Black Report. DHSS, Harmondsworth. 1982: Kessler R. C. Methodoloeical issues in the study of p$ychosocial stress: measurement, design and analysis. Paper presented at the 10th World Congress of Sociology, Mexico City, 1982. Selye H. Stress. Bewiilrigung und Lebensgewinn. Miinchen, 1974. Mason J. W. A re-evaluation of the concept of “non- specifity” in stress theory. J. psychial. Res. 8, 323-333, 1971; Selye H. Confusion and controversy in the stress field. J. Hum. Stress 1, 37. 1975. Sterling P. and Eyer J. Biological basis of stress-related mortalitv. Sot. Sci. Med. 15E. 3-42. 1981: Schaefer H. Die Hierarchic der Risikofaktoren. Mensch. Mediz. Gesellsch. 1, 141-146, 1976. Henry J. P. and Stephens P. M. Stress, health, and the social environment. A Sociobiologic Approach 10 Medi- cine. New York, 1977; Sterling P. and Eyer J., op. cit. House J. S. Occupational stress and coronary heart disease: a review and theort?tical integration. J. Hlrh sot. Behav. 15, 15, 1974.
30.
10. 31.
Il. 12. 32.
13. 33.
14.
15.
16. 17.
34. 35. 36. 37. 38. 39.
40. 18.
19.
20. 21.
41.
42.
22.
23. 43.
24.
25.
26. 44. 45.
27. McGrath J. E. Stress and behaviour in organizations. in 46.
Handbook of Industrial and Organi-_ational Psycholog! (Edited by Dunette M. D.). pp. 1351-1395. Chicago. 1976. cf. Kasl S. V. Epidemiological contributions to the study of work stress. In Stress at Work (Edited by Copper C. L. and Payne R.), pp. 3-48. Chichester, 1978. KarasekR.A.op.cit.;KarasekR.A.,BakerD.,Marxer F. and Theorell T. Job decision latitude, job demands and coronary heart disease-a cross sectional and pro- spective study of Swedish men. Columbia University, 1979; Karmaus W. and Schlfer K. H. op. cit. Hinkle Jr L. E. The effect of exposure to culture change. social change, and change in interpersonal relationship on health. In S~ressjiil Life Events: Their Nature and EfSects (Edited by Dohrenwend B. S. and Dohrenwend B. P.), p. 24, 41. New York. 1974; Antonovsky A. Conceptual and methodological problems in the study of resistance resources and stressful life events. In Stressful Life Events: Their Narure and EJjects (Edited by Dohrenwend B. S. and Dohrenwend B. P.). pp. 252-254. New York. 1974. According to Liem R. and Liem J. Social class and mental illness reconsidered: the role of economic stress and social support. J. Hlth sot. Behav. 19, 150, 1978. LaRocco J. M., House J. S. and French I. R. P. Social support occupational stress, and health. J. Hlrh sot. Behav. 21, 202-218, 1980. Karmaus W., Schiifer K. H., Ellinger S. and Sonn E. Die Bedeutung sozialer Unterstiitzung fiir das Ver- hiiltnis von arbeitsbezogenen Belastungen, Hand- lungsspierlrlumen und rheumatischen Erkrankungen. In Arbeitsbedingungen. Gesundheitsverhalren und Rheu- matische Erkrankungen (Edited by Ellinger S. et al.), pp. 306-325. Hamburg, 1982. LaRocco J. M. et al. op. cit., p. 214. McQueen D. V. and Siegrist J. op. cit., p. 359. Thoits P. A. op. cir., p. 155. Ibid., pp. 8-9. Kasl S. V. op. cit., p. 27. Gerhardt U. Coping and social action: theoretical reconstruction of the life-event approach. Social. Hlrh Illness I, 197, 1979. See, for example, The Pooling Project Research Group. Relationship of blood pressure, serum cholesterol. smoking habit, relative weight and ECG abnormities to incidence of major coronary events. Final Report of the Pooling Project. J. chron. Dis. 31, 201-306. 1978; Mul- tiple risk factor intervention trial research group: multi- ple risk factor intervention trial. Risk factor changes in mortality Results. J. Am. med. Ass. 248, 1465-1477. See, for example, Abholz H., Borgers B., Karmaus W. and Korporal J. (Eds) Risikofaktorenmedizin. Konzepr und Kontroverse. Berlin, 1982. Friedmann M. and Rosenman R. H. Der A-rbp und der B-Tvo. Reinbek bei Hambura. 1975: Glass D. Behav- iour.balrerns. Stress and Coronary Disease. New York. 1977. Brown G. W., Harris T. and Peto I. Life events and psychiatric disorders. Part 2: nature of causal link. Psychol. Med. 3, 159-176, 1973; Brown G. G., Bro- lchrdin M. N. and Harris T. Social class and psychiatric disturbance among women in an urban population. Sociology 225-254, 1975; Shuval J. T. op. cit., p. 338: Disease is seen from this point view, as only one of possible responses by vulnerable persons. Seligman M. E. P. Helplessness. San Francisco, 1975; Schmale H. A. and lker M. Hopelessness as a predictor of cervical Cancer. Sot. Sci. Med. 5, 95-100. 1971. Antonovsky A. op. cir. Kobasa S. C., Maddi S. R. and Courington S. Person- ality and constitution as mediators in the stress-illness relationship. J. Hlrh sot. Behac. 22, 368-378, 1981. Mechanic D. Some problems in developing a social
Working conditions and health 371
47.
48
49.
50.
51.
52.
53.
54. 55.
56.
57.
58.
psychology of adaption to stress. In Social and Psycho- logical Factors in Stress (Edited by McGrath .I. E.), p. 110. New York. 1970; see also, Lazarus R. S., Averill J. R. and Opton E. M. The psychology of coping: issues of Research and assessment. In Coping and Adoptorion (Edited by Coelho G. V., Hamburg D. A. and Adams J. E.), p. 256. New York, 1974; Moos R. H. Psycho- logical techniques in the assessment of adaptive behav- ior. In Coping and Adupration (Edited by Coelho G. V., Hamburg D. A. and Adams J. E.), p. 385. New York, 1974. Harris D. M. and Guten S. Health-protective behavior. an explanatory study. J. Hlth sot. Behnv. 20, 17-29, 1979; Langlie I. K. Social networks, health beliefs, and preventive health behavior, J. Hlfh sot. Behav. 18, 244-260, 1977. Wingard D. L., Berkman L. F. and Brand R. J. A multivariate analysis of health-related practices. A nine- year mortality follow-up of the Alameda County Study. Am. J. Epid.-116, 765-775. 1982. Von Ferber Chr. Gesundheitsverhalten. In Weae zum Arzr (Edited by Siegrist J. and Hendel-Kramer A.), p. 16. Miinchen. 1979. Lazarus R. S. Psychological Srress and the Coping Process. London, 1966; Lazarus R. S., Averill J. R. and Opton E. M. op. cit.: Lazarus R. S. and Launier R. Stress-related transactions between person and environ- ment. In Perspectives in International Psychology (Edi- ted by Pervin-L. A. and Lewis M.), pp..287-327. New York. 1978. Sfress (Edited bv Nitsch J. R.). pp. 213-259. Bern, 1981‘ (in German).
,_
Lazarus R. S., Averill J. R. and Opton E. M. op. cit., p. 260. Otto R. Varieties of coping’and defense. A study of stress reactions reported by men and women in selected occupations. La Trope University. Sociology papers 7, Melbourne, 1980: Pearlin L. J. and Schooler C. The structure of coping. J. Hlth sot. Behac. 19, 2-21, 1978; Pearlin L. J., Menaghan E. G., Lieberman M. A. and Mullan J. T. The stress process. J. Hhh soc Behav. 22, 337-356, 1981; Zimmermann M. K. and Hartley W. S. High blood pressure among employed women: a multi- factor discriminant analysis. J. Hhh sot. Behuv. 23, 205-220, 1982. French J. P. P., Rodgers W. and Cobb S. Adjustment as a person-environment-fit. In Coping and Adaptafion (Edited by Coelho G. V.. Hamburg D. A. and Adams J. E.), pp. 316333. New York, 1974; Lazarus R. S., Averill J. R. and Opton E. M. op. cu.; White R. W. Strategies of adaptation: an attempt at systematic de- scriotion. In Coning and Adaptation (Edited bv Coelho G. V., Hamburg D. A. and ‘Adams ‘J. E.), pp. 47-68. New York, 1974. Mechanic D. op. cif., p. 107: Gerhardt U. op. cir. Mechanic D. op. cit.. p. 113; Dohrenwend B. S. and Dohrenwend B. P. Class and race as status-related sources of stress. In Social Stress (Edited by Levine S. and Scotch N. A.), p. 123. Chicago. 1970. See. for example. Otto R. Negative and positive life experiences among men and women in selected occupations. symptom. awareness and visits to the doctor. Ser. Sri. Med. 13A, 151-164. 1979. See Kleinbaum D. G.. Kupper L. L. and Morgenstem H. Epidemiologic Research. Principles and Quantitative MetI1od.s. pp. 247. 403-418. London. 1982. This is done in: Folkmann S. and Lazarus R. S. An analysis of coping in a middle-aged community sample. J. Hlrh sot. Behac. 21, 1980; Pearlin L. J., Menaghan E. G.. Lieberman M. A. and Mullan J. F. OP. cit.: Menag- han E. G. Measuring coping effectiveness: a panel analysis of marital problems and coping efforts. J. Hlth sot. Behnr. 23,2X-234. 1982: Pearlin L. J. and Schooler C. 0~. cit. The study last mentioned. however. makes use
of the regression analysis model in an unusual way, to interpret through further specification of the model in how far the stress effect is reduced by coping variables. (see the comment of Marshall I. R. J. Hlzh sot. Behnv. 20, 200-201, 1979). Due to the control of the coping variables a reduction in the bivariate stress-strain relation results. The interpretation in question attributes this in each case to the significant coping variables (with a positive sign) which should have a protective effect. The following interpretation however appears to be appropriate to the regression analysis model: all significant coping variables contribute towards expla- ining the variance of strain. If the mathematical sign is positive, these work as further forms of stress, control- ling the effect of the bivariate stress-strain correlation, thus not mitigating but increasing. These problems also certainly arise because of ignoring the effect of strain on coping. Considering stress simultaneously is not done, for example, in Zimmermann M. K. and Hartley W. S. op. cit.
59. Hamburg D. A., Coelho G. V. and Adams J. E. (Eds) Coping and adaptation: steps towards a synthesis of biological and social perspectives. In Coping and Adup- tation. pp. 412. 426. New York, 1974.
60. PearIin’L. J. and Schooler C. op. cif. 61. Kasl S. V. op. cir., pp. 13, 27. 62. Kasl S. V. op. cir., p. 14. 63. See, for example, Friedman M. D., Rosenmann R. D.
and Carroll V. Changes in serum cholesterol and blood clotting time in men subjected to cyclic variation of occupational stress. Circulation 17, 852-86 I, 1958; Cas- se1 J. C. The use of medical records: opportunity for epidemiological studies. J. occup. Med. 5, 185-190, 1963; French J. R. Person role fit. Occup. Menr. Hlfh 3, 15-20, 1973; Cobb S. and Kasl S. V. The consequences of job loss. Termination, pp. 98-133. U.S. Department of Health, Education, and Welfare. NIOSH, Publica- tion No. 77-224, Cincinnati, 1977.
64. Friedman M. and Rosenman R. H. op. cit., p. 73. 65. Caplan R. D., Cobb S. and French Jr J. P. P.
Relationship of cessation of smoking with the stress, personality; and social support. J. appl. Psychol. 60, 211-219. 1975: Caolan R. D.. Cobb S., French Jr J. P. P., van Harrison R. and Pin&au S. R. Job Demands and Workers Health. U.S. Department of Health, Edu- cation, and Welfare. NIOSH, Publication No. 75.160, Washington, 1975; French J. R. op. cir.
66. Brown G. W., Harris T. and Peto J. op. cit., p. 163. 67. Lazarus R. S., Averill J. R. and Ooton E. M. OP. cit..
p. 292. 68. Kahn R. L. Conflict ambiguity, and overload: three
elements in job stress. Occup. Ment. Hlth 3, 2-9, 1973.
69. Lazarus R. S., Averill J. R. and Opton E. M. op. cu., p. 299.
70. Lazarus R. S., Averill J. R:and Opton E. M. op. cit., pp. 252, 298.
71. McQueen D. V. and Siegrist J. op. cit., p. 356. 72. See House J. S. op. cit., p. 21. 73. See Karasek R. A. op. cir. 74. Euler H. P. Arbeitskonzikre und Leistungsrestriktion im
Indusrriebetrieb, pp. 54-6 1. Dusseldorf, 1973. 75. Ellinger S. and Sonn E. Bewaltigung im Verhaltnis zu
76.
77. 78. 79.
ArbeTtssituation und Erkrankung. In Ar- beitsbedingungen. Gesundheitsverhalten und rheumarische Erkrunkungen (Edited by Ellinger S., Karmaus W. et al.), pp. 327-394. Hamburg, 1982. Kahn R. C. op. cit.; French Jr J. P. P., Rodgers W. and Cobb S. op. cil. McGrath J. E. op. cit., p. 27. Kasl S. V. op. cit.. p. 35. Sales, House cited from McMichael A. J. Personality, behavioural, and situational modifiers of work stress-
312 WILFRIED KARMAUS
ors. In Stress at Work (Edited by Cooper C. L. and Payne R.), p. 135. Chichester, 1978.
80. see McMichael A. J., Haynes S. G. and Tyroler H. A. Observation on the evaluation of occupational mor- tality data. J. occup. Med. 17, 128-131, 1975.
81. Holzkamp K. Kritische Psychologie. Vorbereitende Arbeiten, pp. 19-21. Frankfurt, 1972.
82. Young A. The discourse on stress and the reproduction of conventional knowledge. Sot. Sci. Med. 14B, 133-146, 1980.
83. Karmaus W. Das Stresskonzept: Medizinsoziologische
tjberlegungen zu einem Erklarungsmodell der Krank- heitsgenese. Psrchoso~ial 2, 84-103. 1979.
84. Haw M. A. Women. work and stress: a review and agenda for the future. J. Hlrh sot. Behm. 23, 132-144. 1982.
85. Lazarus R. S. and Launier R. on. cir.. D. 239 (German edition).
86. Cooperstock R. and Lennard H. L. Some social mean- ings of tranquilizer use. Social. H1117 Illness 1, 344. 1979.
87. G&dell B. Scandinavian research on stress in working life. In?. J. Hllh Serv. 12, 31-41. 1982.