-
7/27/2019 With+Severe+Obesity,+Diabetes
1/10
case records of themassachusetts general hospital
The
new england journal of
medicine
n engl j med 351;7
www.nejm.org august 12, 2004
696
Founded by
Richard C. CabotNancy Lee Harris, m.d.,
Editor
Jo-Anne O. Shepard, m.d.
,Associate Editor
Stacey M. Ellender,Assistant Editor
Sally H. Ebeling,Assistant Editor
Christine C. Peters,Assistant Editor
Case 25-2004: A 49-Year-Old Womanwith Severe Obesity,
Diabetes,
and Hypertension
Janey S. Pratt, M.D., Susan Cummings, M.S., R.D., Deborah A.
Vineberg, Psy.D.,
Fiona Graeme-Cook, M.D., and Lee M. Kaplan, M.D., Ph.D.
From the Weight Center (J.S.P., S.C.,D.A.V., L.M.K.), and the
Departments ofSurgery (J.S.P.), Psychiatry (D.A.V.), Pa-thology
(F.G.-C.), and Medicine (Gastro-intestinal Unit) (L.M.K.),
MassachusettsGeneral Hospital; and the Departments ofSurgery
(J.S.P.), Psychiatry (D.A.V.), Pa-thology (F.G.-C.), and Medicine
(L.M.K.),Harvard Medical School.
N Engl J Med 2004;351:696-705.
Copyright 2004 Massachusetts Medical Society.
A 49-year-old woman was evaluated at this hospital for the
management of obesity. She
had been overweight since childhood; at the age of 10 years she
weighed 45.4 kg, at theage of 18 she weighed 88.5 kg, and
throughout most of her adult life she weighed be-tween 108.9 and
129.3 kg. She was able to lose weight on more than 10 occasions
with
diet and exercise but always regained it within two to three
years. Dexfenfluramine wasprescribed for weight loss when she was
40 years old, and she lost 11.3 kg but gained
22.6 kg after she stopped taking the drug.Ten years earlier,
diabetes mellitus had been diagnosed; it was controlled with
met-
formin hydrochloride and glyburide. Twice within the 12 years
before the evaluation,the woman had noted intermittent, sharp pain
radiating down her left leg. Plain radio-graphs showed that there
was narrowing of the disk spaces between the second and
third and the third and fourth lumbar vertebrae and first-degree
spondylolisthesis ofthe fifth lumbar vertebra. Despite several
courses of physical therapy and the intermit-
tent use of ibuprofen, intermittent pain persisted.An episode of
exertional chest pain had occurred five years before the
evaluation; ra-
dionuclide scanning of the heart revealed a large anterior
defect suggestive of ischemia.Coronary-artery angiography
demonstrated 50 percent occlusion of one coronary ar-tery. Aspirin
and pravastatin were prescribed.
Three years earlier, treatment with insulin had been started
because of inadequatecontrol of blood glucose. At the same time,
hypertension was diagnosed (blood pres-
sure, 164/114 mm Hg), and treatment with lisinopril was started.
An ophthalmologist
diagnosed diabetic retinopathy. Two years earlier, the patient
had reported the sensa-tion of burning on the soles of her feet
that awakened her at night. Gabapentin was pre-scribed. She had
experienced episodes of depression intermittently for 11 years;
theyhad been treated first with bupropion and for the past 3 years
with fluoxetine.
The patient (gravida 2, para 2) had delivered both her children
by cesarean sectionand worked as a registered nurse for a health
care agency. A tonsillectomy had been per-
formed when she was 14 years old. She was allergic to
penicillin. She had been divorced
pres en t at i on of cas e
Downloaded from www.nejm.org on June 24, 2007 . Copyright 2004
Massachusetts Medical Society. All rights reserved.
-
7/27/2019 With+Severe+Obesity,+Diabetes
2/10
-
7/27/2019 With+Severe+Obesity,+Diabetes
3/10
n engl j med 351;7
www.nejm.org august 12
, 2004
The
new england journal of
medicine
698
tidisciplinary, long-term approach. Members of
this patients multidisciplinary clinical team willdiscuss
aspects of her assessment and care.
medical evaluation
Dr. Lee M. Kaplan:
The medical evaluation of this pa-
tient with obesity was focused on identification ofthe causes
and complications of the excess weight
and on treatment to reverse them or prevent their
progression. Therapeutic decisions in a case such as
this one are guided by the degree of obesity and theseverity of
the medical and psychological compli-
cations. For the majority of persons with obesity, aspecific
cause cannot be identified.
2
Even when en-docrine disorders such as hypothyroidism or
Cush-
ings disease are present, they are rarely the causeof the
obesity. In an increasing number of patients,
the onset or exacerbation of obesity correlates withthe use of
medications that cause weight gain as a
side effect. When I first saw this patient, she wastaking
insulin, which is commonly associated withweight gain, and
fluoxetine, which causes weight
gain in a minority of patients. However, she hadbeen severely
overweight since late childhood, be-
fore those medications were administered.The common disorders
associated with obesity
can be divided into five major categories: metabolic,structural,
degenerative, neoplastic, and psycholog-
ical (Table 2).
2
Several of them (obstructive sleep ap-nea, thromboembolism, and
degenerative arthritis)result from both structural and metabolic
dysfunc-
tion. The relationship of each complication to thebody-mass
index varies widely, with the risk of dia-
betes and other metabolic complications increas-ing at a
body-mass index as low as 23 to 25 and therisk of anatomical
complications increasing most
strikingly in persons with severe obesity. Among themany
complications of obesity, obstructive sleep
apnea, fatty-liver disease, gastroesophageal refluxdisease,
fungal skin infections, and nutrient defi-
ciencies are the most commonly undiagnosed or un-
dertreated complications in patients presenting forcare at a
specialized obesity center.
2
This patient
had diabetes, hypertension, and hyperlipidemia. Aspart of the
initial evaluation, a sleep study was con-
ducted, which showed that she had sleep apnea. Al-though it was
not among the symptoms she initial-
ly described, she later reported that she had snoredand had had
difficulty sleeping for many years.
People with obesity have an elevated risk of all
the diseases for which patients are most commonlyscreened:
hypertension, hyperlipidemia, diabetes
mellitus, and cervical, breast, prostate, and colorec-tal
cancers. Ironically, however, several studies have
shown that they are less likely to undergo screen-ing for these
disorders than are people of normalweight.
1,2
In this patient, screening was complete
and up to date. The strongest medical contraindica-tions for
weight-reduction surgery are severe lung
disease, unstable cardiovascular disease, uncon-trolled clotting
disorders, portal hypertension with
Table 2. Complications of Obesity.
MetabolicType 2 diabetes mellitusHypertensionHigh cholesterol
levelPlatelet dysfunctionThromboembolic diseaseFatty liver disease
(nonalcoholic steatohepatitis)GallstonesPancreatitisReproductive
dysfunctionCentral hypoventilation syndromeAsthmaNutritional
deficiencies
StructuralObstructive sleep apneaGastroesophageal reflux
diseaseAsthma associated with gastroesophageal reflux diseaseVenous
insufficiencyVenous thrombosisPseudotumor cerebriSkin infections
and ulcersStress incontinenceInjuries
DegenerativeAxial arthritisVertebral disk diseaseAtherosclerotic
cardiovascular diseaseComplications of diabetesLeft-ventricular
hypertrophyRight-sided heart failureCirrhosis associated with
nonalcoholic steatohepatitisAlzheimers disease
NeoplasticEndometrialBreastOvarianCervicalProstateColorectalEsophageal
adenocarcinoma (secondary to gastroesophageal reflux
disease)
GallbladderPancreaticRenal cell
PsychologicalDepressionAnxiety and panicBinge eatingReactive
bulimia
Downloaded from www.nejm.org on June 24, 2007 . Copyright 2004
Massachusetts Medical Society. All rights reserved.
-
7/27/2019 With+Severe+Obesity,+Diabetes
4/10
n engl j med 351;7
www.nejm.org august 12, 2004
case records of the massachusetts general hospital
699
gastric varices, pregnancy, and ongoing substance
abuse. This patient had none of these disorders.
nutritional evaluation
Susan Cummings:
This patients comprehensive nutri-tion evaluation included the
assessment of anthro-
pometric data and social, nutritional, and behavior-al factors.
Our objectives were to assess her risk for
complications of obesity, to identify factors con-tributing to
her obesity, if possible, and to provide
baseline data to assess the outcomes of treatment.The
measurements of height, weight, and waist
circumference provide an indication of a patients
risk for complications of obesity (Table 3).
1,2
Calcu-lations based on the patients height, weight, and
age are used to estimate energy expenditure (Table4).
3
This patients weight put her at extremely high
risk for complications. Her energy needs were esti-mated to be
2500 kcal per day to maintain her cur-
rent weight, but her reported intake was approxi-mately 3000
kcal a day 500 kcal more than hernet energy needs.
The patients weight history and that of her fam-ily may give
some indication of a genetic predispo-
sition. In this patient, the weight history revealedthat the
onset of obesity was in late childhood andthat her highest weight
as an adult was 129.3 kg, the
weight at the time of her presentation to us. Herlowest adult
weight was 79.4 kg, immediately after
dieting. Her dieting history included four commer-cial programs
and many self-directed diets. She had
lost as much as 38.5 kg at one time through dieting,
but like many people she always regained moreweight than she had
lost from each diet, and she
had gained more than 45.4 kg overall during
adulthood. Her family history revealed obesity inboth parents
and three brothers.
The nutrition evaluation included a 24-hour re-call of total
food intake and the frequency of foodintake, as well as inquiry
into hunger, satiety (how
frequently she experienced hunger and what madeher feel
satiated), and behaviors such as binge eat-
ing, grazing (eating not related to hunger), night-time eating,
eating in restaurants, and alcohol con-
sumption. This information helped to determinethe patients usual
food intake and provided an in-dication of the environmental
influences on her eat-
ing patterns. Most of her calories were consumedat meals with
large portions of calorically dense
foods. She ate three meals a day but occasionallyskipped lunch
and had a planned snack in the mid-
afternoon. She often ate in fast-food restaurants.The assessment
of physical activity included in-
formation about the activities of daily living, physi-cal
limitations, and structured exercise. This patientwas sedentary and
did not engage in a structured
program of exercise because of her chronic backpain. The
patients expectations concerning ideal
weight were also addressed, as were her self-efficacy(confidence
in the ability to make the necessary be-havioral changes),
motivation, readiness for weight
loss, and potential barriers to treatment. This pa-tients
primary motivation to lose weight was to im-
prove her overall health and well-being.
psychological evaluation
Dr. Deborah A. Vineberg:
Psychological assessment ofpatients with obesity was once
thought to be impor-
* The risk of disease is calculated for type 2 diabetes,
hypertension, and cardiovascular disease. The information is
fromthe National Institutes of Health.
1
NA denotes not applicable.
An increased waist circumference can denote increased disease
risk even in persons of normal weight.
Table 3. Assessing Obesity: Body-Mass Index, Waist
Circumference, and Risk of Disease.*
Category Body-Mass Index Obesity ClassDisease Risk Relative to
Normal Weight
and Waist Circumference
Men, 102 cm,or Women, 89 cm
Men, >102 cm,or Women, >89 cm
Underweight 40 III Extremely high Extremely high
Downloaded from www.nejm.org on June 24, 2007 . Copyright 2004
Massachusetts Medical Society. All rights reserved.
-
7/27/2019 With+Severe+Obesity,+Diabetes
5/10
n engl j med 351;7
www.nejm.org august 12
, 2004
The
new england journal of
medicine
700
tant in identifying the cause of the obesity, whichwas believed
to be related to a lack of self-control or
to a psychological addiction to food. The currentunderstanding
is that the most important reasons
for this evaluation are to diagnose and treat psycho-logical
disorders that result from the obesity, com-
pound the existing weight problem, or interfere
with effective treatment. Pretreatment evaluation ofthis patient
included screening for psychiatric dis-
orders that could interfere with the management ofobesity. Axis
I disorders in the Diagnostic and Statisti-cal Manual of Mental
Disorders
, fourth edition (psychi-atric disorders that are clinical in
nature,
4
such as
depression or anxiety) and eating disorders (suchas binge eating
or bulimia) can complicate medicalmanagement unless they are
treated adequately.
This patient reported poor self-esteem and a pro-found sense of
inferiority that she attributed to be-
ing overweight. She reported that stressful events,including the
births of her children and her divorce,
had exacerbated her weight problem. At the time ofher evaluation
she identified her job, single parent-hood, and her declining
health as stressful factors
in her life. At the initial evaluation her Beck Depres-sion
Inventory
5
score was 19, which corresponds
to mild-to-moderate depression. Obesity is strong-ly associated
with depression. Persons over 50 years
of age who are obese are twice as likely to become
depressed within five years as those who are notobese,
6
but when followed for five years, those
who are depressed are not at increased risk of be-coming obese.
Thus, obesity is a risk factor for de-pression, but the converse is
not true.
Psychological complications associated withgastric bypass are
similar to those associated with
other major surgical procedures; transient postop-erative
depression is the most frequent complica-
tion. Exacerbation of preexisting psychiatric anxietyor
depression is rare, and more than 90 percent ofcases of depression
and 50 percent of cases of anx-
iety disorders improve.
7
Depression before weight-loss surgery does not worsen
outcomes
8
; in fact,
one study found that patients with higher Beck De-pression
Inventory scores lost more weight after
surgery than those with lower scores.
9
This patient described neither binge eating nor
inappropriate behaviors such as self-induced vom-iting or the
use of laxatives or diuretics. She demon-strated good insight into
the psychological function
of her weight, which she characterized as providingher with a
sense of safety and a form of protection.
She admitted to being fearful of substantial weightchange, and
she worried about her potential forself-sabotaging behavior. She
was provided addi-
tional sessions with a psychologist to address
theseconcerns.
The presence of an Axis II disorder (a personalitydisorder or
mental retardation) can lead to difficul-
ties in management or can be a contraindication to
surgery and should be addressed before surgery isundertaken.
This patient did not have an Axis II dis-
order, and she had no family history of psychiatricdisorders.
Thus, she did not have psychiatric con-
traindications to surgery.We also discussed her personal support
system,
since the involvement of family or friends in medicaland
surgical treatment of obesity can improve theoutcome.
10
She reported that both her family and
her friends were supportive of her efforts to loseweight.
weight-loss surgery
Dr. Pratt:
A clinical-team meeting of the obesity-medicine specialist,
nutritionist, and psychologistconcluded that this patient was a
suitable candidate
for bariatric, or weight-loss, surgery. The term bar-iatric
comes from the Greek word baros, meaning
weight, and refers to the treatment of weight dis-orders. Many
different surgical procedures have
* The resting metabolic rate is derived from the HarrisBenedict
formula.
3
Table 4. Estimating Energy Expenditure.
Resting Metabolic Rate (RMR)
*
For men:66.5+(13.75weight in kg)+ (5.003 height in
cm)(6.775agein years)
For women:
655.1+ (9.563 weight in kg)+ (1.850 height in cm) (4.676 age in
years)
Activity Factors
Sedentary little or no exercise
Daily calorie expenditure = RMR1.2
Lightly active (light exercise or sports 13 days/wk)
Daily calorie expenditure = RMR1.375
Moderately active (moderate exercise or sports 35 days/wk)
Daily calorie expenditure = RMR1.55
Very active (hard exercise or sports 67 days/wk)
Daily calorie expenditure = RMR1.725
Extra active (very hard daily exercise or sports and physical
job or twice-a-daytraining)
Daily calorie expenditure = RMR1.9
Downloaded from www.nejm.org on June 24, 2007 . Copyright 2004
Massachusetts Medical Society. All rights reserved.
-
7/27/2019 With+Severe+Obesity,+Diabetes
6/10
n engl j med 351;7
www.nejm.org august 12, 2004
case records of the massachusetts general hospital
701
been tried during the past 50 years, but there are
three major categories in current use: restrictive op-erations
(gastroplasties with the use of adjustable
gastric bands), malabsorptive operations (biliopan-creatic
diversions), and gastric bypasses. Each canbe performed either
laparoscopically or in an open
fashion. The standard types of gastric bypass do notcarry the
risk of clinically significant protein mal-
nutrition that is associated with biliopancreatic-diversion
procedures.
Weight-loss surgery provides the best long-termresults for
patients with moderate (class II) or severe(class III) obesity who
have not responded to more
conservative approaches.
11,12
It is generally reservedfor patients with a body-mass index
greater than 40
or for those with a body-mass index greater than 35whose obesity
is complicated by one or more major
diseases. This patient met the criteria for this ap-proach,
since she had a body-mass index of 52 and
several major complications and was unable tomaintain weight
loss by other means.
The overall morbidity and mortality associated
with gastric bypass surgery are approximately 10percent and less
than 1 percent, respectively.
13,14
Early postoperative complications of laparoscopicgastric bypass
surgery include wound infections (in-cidence, 3 percent),
anastomotic leak (2 percent),
bowel obstruction (2 percent), gastrointestinal hem-orrhage (2
percent), and pulmonary embolus (less
than 0.5 percent). Late complications include bow-el obstruction
(3 percent) and stomal stenosis (5 per-
cent)
13
; both of these problems are more common
after laparoscopic procedures than after open pro-cedures.
Although reported in less than 1 percent of
cases,
7
anastomotic ulcers have been one of themost common late
postoperative complications in
my experience. In patients who have gastric bypasssurgery, there
is often improvement or resolution
of coexisting diseases such as diabetes,
15
hyperten-sion, hyperlipidemia, and sleep apnea,
12
as well asimproved quality of life.
7,14
For this patient, my col-
leagues and I believed that the risks of continuedobesity
outweighed those of bariatric surgery and
its potential complications.Laparoscopic Roux-en-
Y
gastric bypass was rec-
ommended, because this procedure is associatedwith the best
long-term outcomes.
14,16
This opera-tion includes a restrictive procedure and a
short-
limb gastroduodenal bypass (Fig. 1). It does not re-sult in
protein-calorie malabsorption, but it appears
to induce neurohumoral effects that result in de-creased hunger,
accelerated postprandial satiety,
and diminished emotion-based or reward-based
eating.
2
The physiological and molecular mecha-nisms of these effects
remain poorly understood.
In the current case, preparation for surgery in-volved the full
multidisciplinary team. The preoper-ative nutrition program
included an individual ses-
sion of nutrition counseling with a dietitian and agroup
education session to familiarize the patient
with the postoperative diet protocol. The diet to befollowed
after gastric bypass surgery is advanced in
a staged approach (Table 5). Psychological counsel-ing was
instituted to assist the patient in making
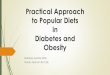
Figure 1. Roux-en-Y Gastric Bypass Surgery.
This operation includes a restrictive procedure, creating a
small proximal gas-
tric pouch, followed by the creation of a jejunojejunostomy in a
Y configura-
tion to allow an end of the jejunum to be brought up and
anastomosed to thisproximal pouch.
Gastric pouch
Gastrojejunostomy
Jejunojejunostomy
Loop of jejunum
Retrocolic, retrogastricetrocolic, retrogastricpassage of
loopassage of loopRetrocolic, retrogastricpassage of loop
Downloaded from www.nejm.org on June 24, 2007 . Copyright 2004
Massachusetts Medical Society. All rights reserved.
-
7/27/2019 With+Severe+Obesity,+Diabetes
7/10
n engl j med 351;7
www.nejm.org august 12
, 2004
The
new england journal of
medicine
702
the behavioral changes that would be required after
surgery. The preoperative medical evaluation includ-
ed a thorough assessment of the operative risks andthe need for
perioperative management of coexist-
ing diseases, with discussion among the obesity-medicine
physician, anesthesiologist, and surgeon
to optimize her care.The operation took about three hours. The
sur-
gical team first gained access by placing two 12-mmports and
three 5-mm ports through the abdominalwall in the upper abdomen one
for a camera, one
for the liver retractor, one for stapling devices, andthe other
two for graspers to manipulate the stom-
ach and intestines. The stomach was first dividedby staplers
across the cardia, creating a 30-ml prox-
imal gastric pouch (Video Clip 1 in the Supplemen-tary Appendix,
available with the full text of thisarticle at www.nejm.org). We
then created a 100-cm
Roux limb by dividing the intestines, stapling a
je-junojejunostomy (Video Clip 2 in the Supplementary
Appendix), and passing the limb behind the colonand stomach
(Video Clip 3 in the Supplementary Ap-
pendix). Finally, this limb was stitched to the pouch
in a double-layer anastomosis 1.5 cm in diameter(Video Clip 4 in
the Supplementary Appendix). Be-
cause the liver appeared fatty, a wedge-biopsy spec-imen of the
liver was obtained. Postoperatively, anamidotrizoic acid
(Gastrografin) swallow examina-
tion confirmed that the gastrojejunal anastomosiswas intact and
without leak. The patient was dis-
charged on the third hospital day while following astage 1 diet
(Table 5).
Dr. Fiona Graeme-Cook:
The specimen obtained byliver biopsy revealed hepatocellular
steatosis with a
very few foci of ballooning degeneration; the portaltracts
showed slight proliferation of the bile ductules
with minimal chronic inflammatory infiltrate (Fig.2A).
Glycogenated hepatocellular nuclei were scat-
tered. These findings are consistent with the pres-ence of
nonalcoholic fatty liver disease, without ev-idence of
steatohepatitis, fibrosis, or cirrhosis.
In the presence of insulin resistance, high levelsof circulating
insulin lead to high levels of free fatty
acids within the liver, increasing the synthesis
oftriglycerides. Although the mechanism is not com-pletely
understood, hepatocytes accumulate fat,
manifested as hepatocellular steatosis. This is themost common
finding in the liver in patients with
severe obesity, present in more than 75 percent ofcases. The
additional feature of glycogenated nuclei
is also a marker for insulin resistance and hypergly-
cemia. Steatohepatitis may complicate steatosis,possibly as a
result of excessiveb
-oxidation of fatty
acids by hepatocellular mitochondria. The resultantoxidative
stress is thought to lead to peroxidation of
lipids, resulting in hepatocyte necrosis, an influx
ofmononuclear inflammatory cells, and eventually, fi-
brosis and cirrhosis (Fig. 2B).
17,18
Dr. Kaplan:
During the early postoperative period,
the patients most prominent symptom was consti-pation, which was
probably a result of mild dehy-
dration. The mobilization of stored fat by lipolysisconsumes
prodigious amounts of water, and fluidrequirements are high during
the first several
months after surgery. During the first few weeks, pa-tients are
closely monitored for dehydration, which
may be manifested as constipation, lethargy, orlight-headedness.
The use of diuretics or other an-
pat h olog i cal di s cus s i on
di s cus s i on of out com e
Table 5. Protocol for Diet after Gastric Bypass Surgery.
Stage 1
12 days after surgeryConsume no-calorie, noncarbonated,
decaffeinated, clear beverages
Stage 2
12 wk after surgery
Consume 600 ml (minimum) of stage 1 liquids plus 600 ml
(minimum)full liquids (skim or 1% milk with Instant Breakfast with
no sugar added,blended low-fat yogurt, diet pudding made with skim
or 1% milk, tomatosoup made with milk, soy-protein powder mixed
with milk), and no con-centrated sweets
Stage 3
324 wk after surgery (a transitional phase, with advancement to
a solid-fooddiet as tolerated)
Soft, moist foodsBegin with cooked, moist, protein-rich foods
(eggs, fish, poultry) diced
smallAdd cooked vegetables; avoid raw vegetables until 1 mo
after surgeryAdd whole-grain starch to diet gradually
Guidelines:Do not drink fluids with mealsTake very small bites,
chew very well, stop when comfortably full
Plan 3 meals a day, no more than 5 hours apart, with protein at
eachmealGradually add vegetables, fruit, and starch; take 23 bites
of protein
before eating vegetables, starch
Stage 4
(24 wk after surgery, or as tolerated)Solid-food diet
Avoid carbonated beveragesPlan all meals and snacksAvoid eating
when not hungry, eating high-calorie soft foods, and
drinking beverages with meals
Downloaded from www.nejm.org on June 24, 2007 . Copyright 2004
Massachusetts Medical Society. All rights reserved.
-
7/27/2019 With+Severe+Obesity,+Diabetes
8/10
n engl j med 351;7
www.nejm.org august 12, 2004
case records of the massachusetts general hospital
703
tihypertensive agents often must be reduced orstopped altogether
in the immediate postoperative
period. This patients blood pressure remained nor-mal, and the
lisinopril was discontinued without ad-
verse effect. Her blood sugar levels became normalwithin two
days after surgery, despite the discontin-uation of insulin and
metformin. This rapid im-
provement in insulin sensitivity within several daysafter
surgery is typical, and many patients require
little or no therapy for their diabetes during thistime. To
avert potentially life-threatening hypogly-
cemic episodes, her blood glucose levels were mon-itored
frequently and insulin and sulfonylureas wereavoided.
Ten days after surgery, she had lost 9.1 kg. Threemonths after
the operation, she was eating three
meals and two snacks daily and had lost 27.2 kg.Six months after
surgery, she had lost 37.2 kg and
was eating most foods without having symptoms.
Participation in postoperative programs of nutritioneducation
and cognitive behavioral therapy appears
to minimize both short-term complications relat-ed to
nutritional issues and subsequent weightgain.
10,11
Beginning six months after surgery, the
patient participated in a monthly program for sur-gical support
and education, which provides ongo-
ing support and counseling. Her weight decreasedby 54.4 kg, to
70.3 kg, during the first 12 months
after surgery. Excess skin with ptosis in the lower ab-domen was
treated with abdominoplasty 15 monthsafter the weight-loss surgery.
She later regained ap-
proximately 4.5 kg, and her weight then stabilizedat 74.8 kg for
the next year.
nutritional outcome
Two years after surgery, the patients body-mass in-dex was 30,
down from 52, and her energy expen-
diture was estimated to be about 1800 kcal per day,down from
2500 kcal per day. She ate three meals aday and did not routinely
eat snacks. She experi-
enced satiety with half-normal portions of food, andher hunger
returned about five hours after each
meal. She tolerated all types of food, although sheavoided
concentrated carbohydrates at the begin-ning of each meal as a way
of preventing the dump-
ing syndrome (i.e., rapid gastric emptying). She didnot have any
change in her food preferences. She
walked 4.8 km a day and reported enjoying exercisefor the first
time.
medical outcome
Two years after surgery, the patients diabetes im-
proved but did not completely resolve. She no long-er required
insulin, and her metformin dose de-
creased from 850 mg taken three times daily to 500mg taken twice
daily. Her levels of hemoglobin A
1
c
and urinary microalbumin fell (Table 1). Her dia-betic
retinopathy did not progress. Her sleep apnea,hypertension, and
folliculitis resolved. Her lumbar
back pain and sciatica improved substantially. Herhyperlipidemia
remained well controlled with the
use of a lower dose of atorvastatin than she was tak-ing before
the surgery, and there was no progres-
sion of her coronary artery disease.A deficiency of
micronutrients is common after
gastric bypass surgery. We regularly assessed the
patients levels of iron, calcium, vitamin B
12
, vita-min D, and vitamin K. Iron deficiency developed ap-
proximately 10 months after surgery (Table 1). Itwas treated
successfully with oral ferrous bisglyci-
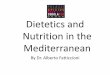
Figure 2. Liver-Biopsy Specimen (Hematoxylin
and Eosin).
Hepatocellular steatosis with small-droplet and large-
droplet fat is apparent, with glycogenated nuclei (Panel A,
arrows). Panel B shows a liver-biopsy specimen from an-other
patient with nonalcoholic steatohepatitis, with ste-
atosis, ballooning degeneration, and portal and lobular
mononuclear infiltrates.
A
B
Downloaded from www.nejm.org on June 24, 2007 . Copyright 2004
Massachusetts Medical Society. All rights reserved.
-
7/27/2019 With+Severe+Obesity,+Diabetes
9/10
n engl j med 351;7
www.nejm.org august 12
, 2004
The
new england journal of
medicine
704
nate and polysaccharide iron supplementation. Be-
fore surgery, she had been found to have a vitaminB
12
deficiency, which occurs in a small number of
patients with obesity who have followed many dietprograms.
Intranasal vitamin B
12
supplementationwas begun before the operation and was
continued
afterward, and two years later she had normal levelsof vitamin
B
12
(Table 1). Secondary hyperparathy-
roidism from malabsorption of calcium and vita-min D occurs in
more than 60 percent of patients
after gastric bypass. Metabolic bone disease is com-mon and must
be screened for and treated. This pa-tient took prophylactic
supplementation with an
oral calcium preparation (1000 mg of elemental cal-cium per
day), and her levels of calcium, vitamin D,
and parathyroid hormone have remained normal.
psychological outcome
Six weeks after the operation, the patient recognized
feelings of loss related to being unable to overin-dulge in
food. She commented, You fixed my stom-ach, but I need to fix my
head, alluding to the need
to focus on psychological triggers for eating thatcould no
longer be satisfied by food. Twelve weeks
after surgery, she reported feeling great. She wasexcited about
her increased energy, and the BeckDepression Inventory score fell
to 3, within the
range of minimal depressive symptoms, and it re-mained at that
level thereafter. She stopped taking
fluoxetine.Two and a half years after the gastric bypass
sur-
gery, both her self-confidence and her self-esteem
have increased. She is more assertive in her relation-ships,
with positive results.
Dr. Pratt:
This case illustrates the importance ofa multidisciplinary team
that includes an obesity-
medicine specialist, a nutritionist, a psychologist,and a
surgeon to ensure optimal medical and psy-
chological results from weight-loss surgery.
1,10,19
Although this patient was able to initiate exercise onher own,
it is important to include a physical thera-
pist or trainer when needed. Although her obesitywas not cured,
since her body-mass index remained
elevated (at 30), the team viewed this case as havinga
successful outcome.
Dr. A. Benedict Cosimi (Surgery): How would youassess whether
the patients psychological issues
were solved or complicated by the surgery? This pa-
tient considered her weight a protective shield. Howdid she feel
when this shield disappeared?
Dr. Vineberg:
Instead of using the weight as a pro-tection, she worked to
establish appropriate bound-aries with people in her life, so that
she could main-
tain appropriate emotional distance that did notdepend on the
physical or emotional distance
caused by her size.
Dr. Kaplan:
It is not clear whether the protection
that she felt the excess weight provided was a pri-mary or a
secondary event. If you are shunned in so-ciety because of obesity,
you may then use the weight
as an excuse not to interact with people.
Dr. Carlos Fernndez-del Castillo (Surgery): The ad-
justable gastric band has been approved by the Foodand Drug
Administration for use in the United
States. I anticipate that its application is an easieroperation
than bypass. Why was it not used here?
Dr. Pratt:
The early experience with the adjust-able gastric band in the
United States showed a highrate of reoperation,
20
and definitive studies of long-
term outcomes are not yet available. To achieve anoptimal
outcome, the band has to be adjusted every
two to six months by the addition or removal of sa-line. This
dependence on frequent follow-up visitssuggests that success with
this procedure may be
more dependent on voluntary behavior than thesuccess observed
after gastric bypass.
Dr. Jay Vacanti (Pediatric Surgery): Can you com-ment on the use
of surgery in the management of
pediatric obesity?
Dr. Pratt:
Obesity in adolescents is being treatedsurgically in several
centers around the country, in-
cluding the Weight Center.
21
Although the pediat-ric program here focuses primarily on
behavioral
and medical approaches, gastric bypass surgery hasbeen used to
treat a few teenagers with severe obe-
sity and obesity with medical complications, suchas type 2
diabetes mellitus or obstructive sleep ap-nea, who have not been
responsive to other inter-
ventions. Recent studies have shown that resolu-tion of diabetes
is most likely in patients who have
had it for less than five years, so waiting to performsurgery in
children with type 2 diabetes may be more
dangerous in the long term than performing thesurgery.
22
Downloaded from www.nejm.org on June 24, 2007 . Copyright 2004
Massachusetts Medical Society. All rights reserved.
-
7/27/2019 With+Severe+Obesity,+Diabetes
10/10
n engl j med 351;7
www.nejm.org august 12, 2004
case records of the massachusetts general hospital
705
references
1.
Clinical guidelines on the identification,evaluation, and
treatment of overweight andobesity in adults: the evidence report.
ObesRes 1998;6:Suppl 2:51S-209S. [Erratum,Obes Res 1998;6:464.]
2.
Kaplan LM. Body weight regulation andobesity. J Gastrointest
Surg 2003;7:443-51.
3.
Harris JA, Benedict FG. A biometricstudy of basal metabolism in
man. Wash-ington D.C.: Carnegie Institute of Washing-ton, 1919.
4.
Diagnostic and statistical manual ofmental disorders, 4th ed.:
DSM-IV. Wash-ington, D.C.: American Psychiatric Associa-tion,
1994.
5. Beck A, Steer R. Manual for revised BeckDepression Inventory.
San Antonio, Tex.:Psychological Corporation, 1987.6. Roberts RE,
Deleger S, Strawbridge WJ,Kaplan GA. Prospective association
be-tween obesity and depression: evidencefrom the Alameda County
Study. Int J ObesRelat Metab Disord 2003;27:514-21.7. Schauer PR,
Ikramuddin S, Gourash W,
Ramanathan R, Luketich J. Outcomes afterlaparoscopic Roux-en-Y
gastric bypass formorbid obesity. Ann Surg 2000;232:515-29.8. Dymek
MP, le Grange D, Neven K, Al-
verdy J. Quality of life and psychosocial ad-
justment in patients after Roux-en-Y gastricbypass: a brief
report. Obes Surg 2001;11:32-9.9. Averbukh Y, Heshka S, El-Shoreya
H, etal. Depression score predicts weight lossfollowing Roux-en-Y
gastric bypass. ObesSurg 2003;13:833-6.
10. Balsiger BM, Murr MM, Poggio JL, SarrMG. Bariatric surgery:
surgery for weightcontrol in patients with morbid obesity. MedClin
North Am 2000;84:477-89.11. Brolin R. Update: NIH consensus
con-ference: gastrointestinal surgery for severeobesity. Nutrition
1996;12:403-4.12. Idem. Bariatric surgery and long-termcontrol of
morbid obesity. JAMA 2002;288:2793-6.13. Podnos YD, Jimenez JC,
Wilson SE,Stevens CM, Nguyen NT. Complications af-ter laparoscopic
gastric bypass: a review of3464 cases. Arch Surg
2003;138:957-61.14. Nguyen NT, Goldman C, Rosenquist CJ,et al.
Laparoscopic versus open gastric by-pass: a randomized study of
outcomes,
quality of life, and costs. Ann Surg 2001;234:279-91.15.
MacDonald KG Jr, Long SD, SwansonMS, et al. The gastric bypass
operation re-duces the progression and mortality of non-
insulin-dependent diabetes mellitus. J Gas-trointest Surg
1997;1:213-20.16. Jones KB Jr. Bariatric surgery wheredo we go from
here? Int Surg 2004;89:51-7.17. McCullough A. Update on
nonalcoholicfatty liver disease. J Clin Gastroenterol
2002;34:255-62.
18. Neuschwander-Tetri BA, Caldwell SH.Nonalcoholic
steatohepatitis: summary ofan AASLD Single Topic Conference.
Hepa-tology 2003;37:1202-19. [Erratum, Hepa-tology 2003;38:536.]19.
Blackburn GL, Greenberg I. Multidisci-plinary approach to adult
obesity therapy.Int J Obes 1978;2:133-42.20. Ren CJ, Horgan S,
Ponce J, et al. US ex-perience with the LAP-BAND system. Am JSurg
2002;184:46S-50S.21. Sugerman HJ, Sugerman EL, DeMariaEJ, et al.
Bariatric surgery for severely obeseadolescents. J Gastrointest
Surg 2003;7:102-8.22. Schauer PR, Burguera B, Ikramuddin S,et al.
Effect of laparoscopic Roux-en-Y gas-
tric bypass on type 2 diabetes mellitus. AnnSurg
2003;238:467-85.Copyright 2004 Massachusetts Medical Society.
35-millimeter slides for the case records
Any reader of theJournal who uses the Case Records of the
Massachusetts General Hospital as a medical teaching
exercise or reference material is eligible to receive 35-mm
slides, with identifying legends, of the pertinent x-ray films,
electrocardiograms, gross specimens, and photomicrographs of
each case. The slides are 2 in. by 2 in., for use with a
standard 35-mm projector. These slides, which illustrate the
current cases in the Journal, are mailed from the Department
of Pathology to correspond to the week of publication and may be
retained by the subscriber. Each year approximately
250 slides from 40 cases are sent to each subscriber. The cost
of the subscription is $450 per year. Application forms for
the current subscription year, which began in January, may be
obtained from Lantern Slides Service, Department of
Pathology, Massachusetts General Hospital, Boston, MA 02114
(telephone 617-726-2974).
Slides from individual cases may be obtained at a cost of $35
per case.
Downloaded from www.nejm.org on June 24, 2007 . Copyright 2004
Massachusetts Medical Society. All rights reserved.