Embed Size (px)
Citation preview
Why a CrisisWhy a CrisisResidential Unit?Residential Unit?
Significantly lower cost than hospitalizationSignificantly lower cost than hospitalizationLess restrictive environmentLess restrictive environmentHighly skilled clinicians focus on group/psychosocial rehabilitation skillsHighly skilled clinicians focus on group/psychosocial rehabilitation skillsOutcomes are at least equivalent to (and probably better than) psychiatricOutcomes are at least equivalent to (and probably better than) psychiatrichospitalizationhospitalizationReduces number of voluntary hospitalizations so that involuntaryReduces number of voluntary hospitalizations so that involuntaryhospitalizations can take precedencehospitalizations can take precedence
Literature ReviewLiterature Review
Before opening the CRU, a review of relevant literature wasBefore opening the CRU, a review of relevant literature wasundertaken. It became apparent that little research had been doneundertaken. It became apparent that little research had been doneon the use of CRUs (or similar programs) as alternatives toon the use of CRUs (or similar programs) as alternatives tohospitalization.hospitalization.
W.H. Sledge, et al, produced the seminal and most widely quotedW.H. Sledge, et al, produced the seminal and most widely quotedresearch on the use of residential alternatives to hospitalization.research on the use of residential alternatives to hospitalization.Sledge, WH, Tebes J, Rakfeldt J, Davidson, I, Lyons, L Druss B.,Sledge, WH, Tebes J, Rakfeldt J, Davidson, I, Lyons, L Druss B.,Day hospital/crisis respite care versus inpatient care, 1&2: clinicalDay hospital/crisis respite care versus inpatient care, 1&2: clinicaloutcomes & service utilization and costs. Am J Psychiatry, 1996;outcomes & service utilization and costs. Am J Psychiatry, 1996;153: 1065153: 1065--1083.1083.
Sledge, et al concluded that alternative programs had not beenSledge, et al concluded that alternative programs had not been“widely implemented” because of the existence of an “incentive“widely implemented” because of the existence of an “incentivestructure that discourages their use” and because it is assumed thatstructure that discourages their use” and because it is assumed thatpsychiatric hospitalization is the “most effective method ofpsychiatric hospitalization is the “most effective method oftreatment for those acutely ill psychiatric patients.” p. 1075. Thistreatment for those acutely ill psychiatric patients.” p. 1075. Thisconclusion was still applicable at the inception of the CRU in 2004.conclusion was still applicable at the inception of the CRU in 2004.
Literature Review contd.Literature Review contd.
Sledge and other research projects have concluded that, in many cases,Sledge and other research projects have concluded that, in many cases,residential programs are a cost effective and viable alternative toresidential programs are a cost effective and viable alternative tohospitalization. E.g., Goodwin, R. & Lyons, JS, An emergency housinghospitalization. E.g., Goodwin, R. & Lyons, JS, An emergency housingprogram as an alternative to inpatient treatment for persons with severeprogram as an alternative to inpatient treatment for persons with severemental illness. Psychiatric Services, 2001; 52: 92mental illness. Psychiatric Services, 2001; 52: 92 –– 95; Hawthorne, WB,95; Hawthorne, WB,Green, EE, Gilmer, T, Garcia, P, Hough, R, Lee, M, Hammond, L, Lohr, JB:Green, EE, Gilmer, T, Garcia, P, Hough, R, Lee, M, Hammond, L, Lohr, JB:A randomized trial of shortA randomized trial of short--term acute residential treatment for veterans.term acute residential treatment for veterans.Psychiatric Services, 2005; 56: 1379Psychiatric Services, 2005; 56: 1379 –– 1386.1386.
The Sledge alternative to psychiatric hospitalization for individuals with SMIThe Sledge alternative to psychiatric hospitalization for individuals with SMIin crisis was a combined day hospital and crisis residence that resembled thein crisis was a combined day hospital and crisis residence that resembled theCRU in many respects but the CRU combines both the day hospital conceptCRU in many respects but the CRU combines both the day hospital conceptand a residence under one roof.and a residence under one roof.
The CRU differs from all models that were reviewed in two respects: 1) theThe CRU differs from all models that were reviewed in two respects: 1) thelevel of training of its clinical staff (all LPHAs except 1 QMHP RN); and 2)level of training of its clinical staff (all LPHAs except 1 QMHP RN); and 2)theCRU’s alumni organization (described later in this presentation).theCRU’s alumni organization (described later in this presentation).
Literature Review, contd.Literature Review, contd.
The preparatory research supported the conclusion thatThe preparatory research supported the conclusion thatpsychiatric crises requiring acute care with hospitalizationpsychiatric crises requiring acute care with hospitalizationaccount for the largest expenditures in community care. Fenton,account for the largest expenditures in community care. Fenton,W.S., Hoch, JS, Herrell, JM, Mosher, L & Dixon, L., Cost andW.S., Hoch, JS, Herrell, JM, Mosher, L & Dixon, L., Cost andcostcost--effectiveness of hospital vs. residential crisis care foreffectiveness of hospital vs. residential crisis care forpatients who have serious mental illness. Arch Gen Psychiatry,patients who have serious mental illness. Arch Gen Psychiatry,202; 59; 357202; 59; 357--364.364.
In designing the CRU, Sledge’s conclusion that selection ofIn designing the CRU, Sledge’s conclusion that selection ofpersonnel is critical to the “effectiveness” aspect of a costpersonnel is critical to the “effectiveness” aspect of a cost--effective program was a critical factor.effective program was a critical factor.
What we did not prepare as effectively for was to meet the needsWhat we did not prepare as effectively for was to meet the needsof individuals who are unable to participate in psychosocialof individuals who are unable to participate in psychosocialrehabilitation in any form and/or the necessity of extremerehabilitation in any form and/or the necessity of extremeflexibility in meeting the needs to clients with psychotic disordersflexibility in meeting the needs to clients with psychotic disorders
What is a CRUWhat is a CRU
A residential alternative to hospitalization forA residential alternative to hospitalization forindividuals experiencing an acute psychiatricindividuals experiencing an acute psychiatricepisodeepisode
Stabilization, evaluation, medication,Stabilization, evaluation, medication,psychosocial rehabilitation and linkage to otherpsychosocial rehabilitation and linkage to otherservices providedservices provided
Structure and Staffing of CRUStructure and Staffing of CRU
1818--bed, CARF certified, residential unitbed, CARF certified, residential unit
Open, unlockedOpen, unlocked
VoluntaryVoluntary
Clients not restricted to property during nonClients not restricted to property during non--groupgrouptimestimes
6 or more groups per day6 or more groups per day
Individual therapy and case management 3 or moreIndividual therapy and case management 3 or moretimes per weektimes per week
Structure & Staffing, contd.Structure & Staffing, contd.
Relying heavily on the conclusions of Sledge, etRelying heavily on the conclusions of Sledge, etal, that the quality of staff education and trainingal, that the quality of staff education and trainingmay be predictive of outcomes, the CRU wasmay be predictive of outcomes, the CRU wasdesigned to provide intensive psychosocialdesigned to provide intensive psychosocialservices by highly trained LPHAs. One of theservices by highly trained LPHAs. One of themain goals in opening the CRU was to end ormain goals in opening the CRU was to end oreven reduce the cycle of repeatedly accessingeven reduce the cycle of repeatedly accessingexpensive ERs, hospitals and jails.expensive ERs, hospitals and jails.
Structure & Staffing contd.Structure & Staffing contd.
Staffing is as follows: MD 15 hours per weekStaffing is as follows: MD 15 hours per weekwith backup from CRU/MCOT Medicalwith backup from CRU/MCOT MedicalDirector; 3 FTE LPHAs; 1 relief LPHA (50Director; 3 FTE LPHAs; 1 relief LPHA (50 ––75%); 1 Administrator/clinician (50%); 1 FTE75%); 1 Administrator/clinician (50%); 1 FTERN; 2 FTE psychiatric specialists per shift; 1RN; 2 FTE psychiatric specialists per shift; 1partpart--time LPHA (10 hours on weekends)time LPHA (10 hours on weekends)
Population ServedPopulation Served
The vast majority of CRU clients are homelessThe vast majority of CRU clients are homeless
Have a history of SMI (although not alwaysHave a history of SMI (although not alwaystarget population diagnoses)target population diagnoses)
Have coHave co--occurring disordersoccurring disorders
Have a history of multiple hospitalizationsHave a history of multiple hospitalizationsand/or incarcerations or bothand/or incarcerations or both
Clinical FocusClinical Focus
Bringing attention to skills that enable clients toBringing attention to skills that enable clients toavoid future psychiatric crisesavoid future psychiatric crises
Based on a cognitive behavioral therapy modelBased on a cognitive behavioral therapy modelbecause it is evidencebecause it is evidence--basedbased
ProblemProblem--solving and communication skillssolving and communication skillsemphasized, as well as management of coemphasized, as well as management of co--occurring disordersoccurring disorders
Education/Skills TrainingEducation/Skills TrainingPhilosophyPhilosophy
Objectives include teaching clients to use supportObjectives include teaching clients to use supportgroups as sounding board and problemgroups as sounding board and problem--solving toolsolving tool
Teach emotional regulation skills that can be practicedTeach emotional regulation skills that can be practicedindependently and without the intervention of a mentalindependently and without the intervention of a mentalhealth professionalhealth professional
Teach and model effective communication skills so thatTeach and model effective communication skills so thatmisunderstandings can be avoided and clients have amisunderstandings can be avoided and clients have abetter chance of getting their needs metbetter chance of getting their needs met
Education/Skills Training contd.Education/Skills Training contd.
Teach methods for changing interpretations ofTeach methods for changing interpretations ofevents to change feelings and destructiveevents to change feelings and destructivebehaviorsbehaviors
Recognition of symptoms and symptomRecognition of symptoms and symptommanagement techniquesmanagement techniques
Emphasis on mindfulness practice as a way ofEmphasis on mindfulness practice as a way offocusing on the present and managing angerfocusing on the present and managing anger
Teach other anger management and stressTeach other anger management and stress--reducing techniquesreducing techniques
Benefits of CRU vs. InpatientHospitalization
Psychiatric hospitalizations – high incidence of physical aggression CRU – low incidence of aggression. In 6 years, one incident involving
physical aggression toward a resident. In the same occurrence, the clienthit a staff member. CRU Operational Guidelines do not permit use ofrestraint.
Indigent care hospitals are frequently without beds and alternatives tohospitalization facilitate better use of hospitals
Fairly rapid turnover in CRU creates much higher bed availability Use of Peer Navigators to assist in educating consumers about the
community mental health system and linking them to community supports.Current research supports use of peers.
Hospital environments do not always support dignity, safety and privacyand are not always flexible enough to meet and respect cultural needs anddifferences or allow for individualized treatment plans. In addition, clientsreport that they do not usually like hospitals. CRU has potential to bemore humane
CRU vs. hospitalization, contd.
Possible reduction in stigma when receiving servicesin a residential facility rather than a psychiatrichospital.
Avoid “institutionalized” patients or identificationwith the “patient” role
CRUs produce quicker results Greater focus on self-actualization and
empowerment in treatment and discharge planning Social problems leading to relapse are more easily
identified and addressed CRUs focus more directly on co-occurring disorders Alumni program can be used for relapse prevention
Lagniappe
Without incurring significant additionalcost, and to further the goal of reducingepisodes of ER visits, hospitalizations anduse of jail services, the CRU hasdeveloped an ad hoc alumni programwhich provides an additional safeguardagainst reoccurring crises
The CRU staff members provide servicesto alumni on an informal basis and alumnican receive brief individual therapy asthey transition out of the CRU and intothe community or if the need arises afterthey are living in the community
Lagniappe contd.
Alumni are allowed to use the CRUfacilities and have meals at the CRU thebudget permits and providing they adhereto Alumni Rules
Alumni are invited to participate in allholiday activities with CRU residents
The alumni program is an attempt toprovide a home/family of choice settingfor individuals who long ago burnedfamily (and other) bridges
Alumni
The alumni program has formalmeetings on at least a quarterlybasis
Efforts are being made to provide agroup therapy/aftercare trackspecific to alumni needs
Many alumni report anecdotally thatthey would have returned toemergency rooms and jails had itnot been for having access to theCRU
Readmission
The original design of the CRU didnot permit readmission. As theprogram became operational, itbecame apparent that, at times,readmission presents a viablealternative to hospitalization whichis more cost effective and lesstraumatic.
Readmission, contd.
Readmissions to the CRU aredecided on a case by case basis bythe staff, reviewed by the MedicalDirector, and limited to a maximumof 5 days.
In several difficult cases,readmission on a date chosen bythe client has been used as anincentive to keep clients out of ERsand hospitals
Crisis Residential UnitCrisis Residential UnitProgram OutcomesProgram Outcomes
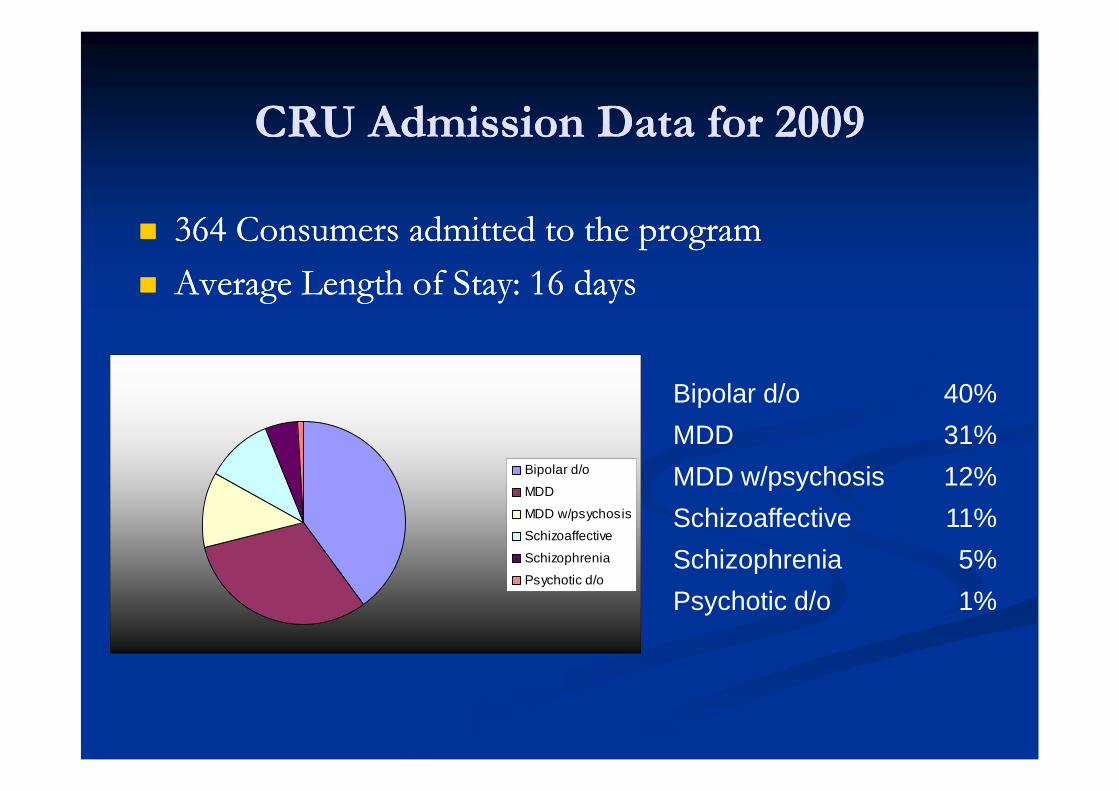
CRU Admission Data for 2009CRU Admission Data for 2009
364 Consumers admitted to the program364 Consumers admitted to the program
Average Length of Stay: 16 daysAverage Length of Stay: 16 days
Bipolar d/o
MDD
MDD w/psychosis
Schizoaffective
Schizophrenia
Psychotic d/o
Bipolar d/o 40%
MDD 31%
MDD w/psychosis 12%
Schizoaffective 11%
Schizophrenia 5%
Psychotic d/o 1%
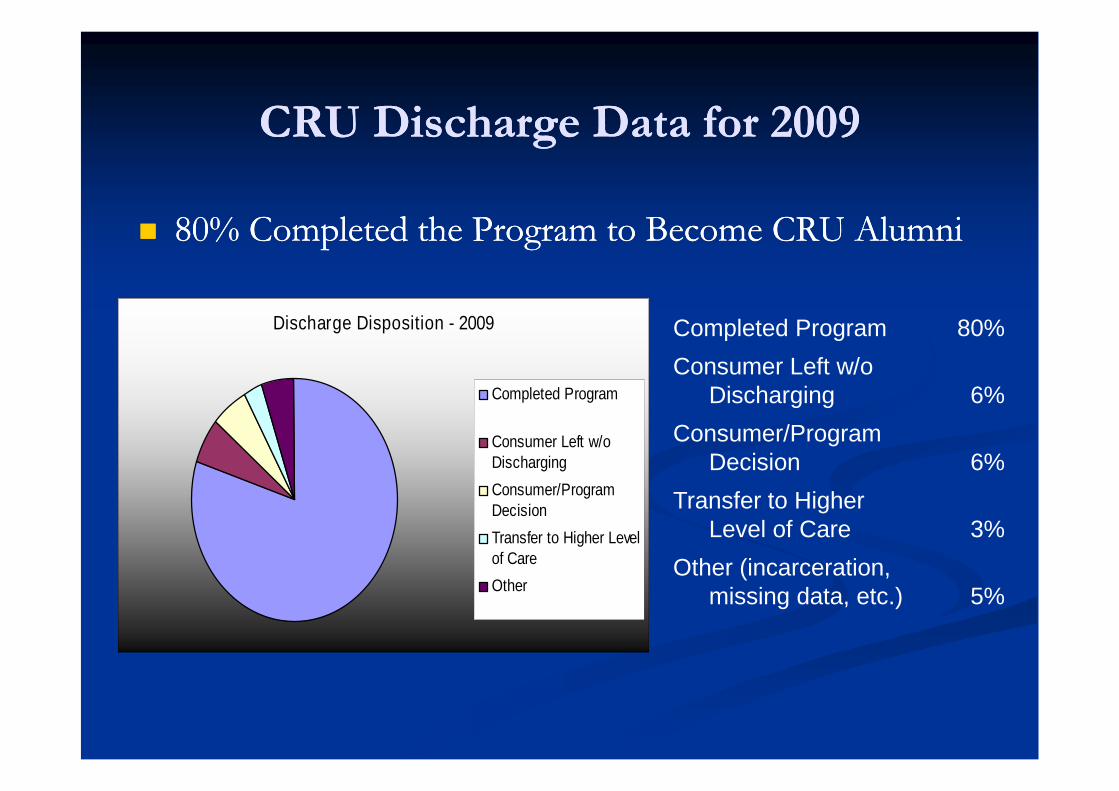
CRU Discharge Data for 2009CRU Discharge Data for 2009
80% Completed the Program to Become CRU Alumni80% Completed the Program to Become CRU Alumni
Discharge Disposition - 2009
Completed Program
Consumer Left w/oDischarging
Consumer/ProgramDecision
Transfer to Higher Levelof Care
Other
Completed Program 80%
Consumer Left w/oDischarging 6%
Consumer/ProgramDecision 6%
Transfer to HigherLevel of Care 3%
Other (incarceration,missing data, etc.) 5%
CRU: Program EffectivenessCRU: Program Effectiveness
Admission & Discharge AssessmentsAdmission & Discharge Assessments
Relapse OccurrencesRelapse Occurrences
Alumni ParticipationAlumni Participation
Effectiveness measured by three indicators:Effectiveness measured by three indicators:
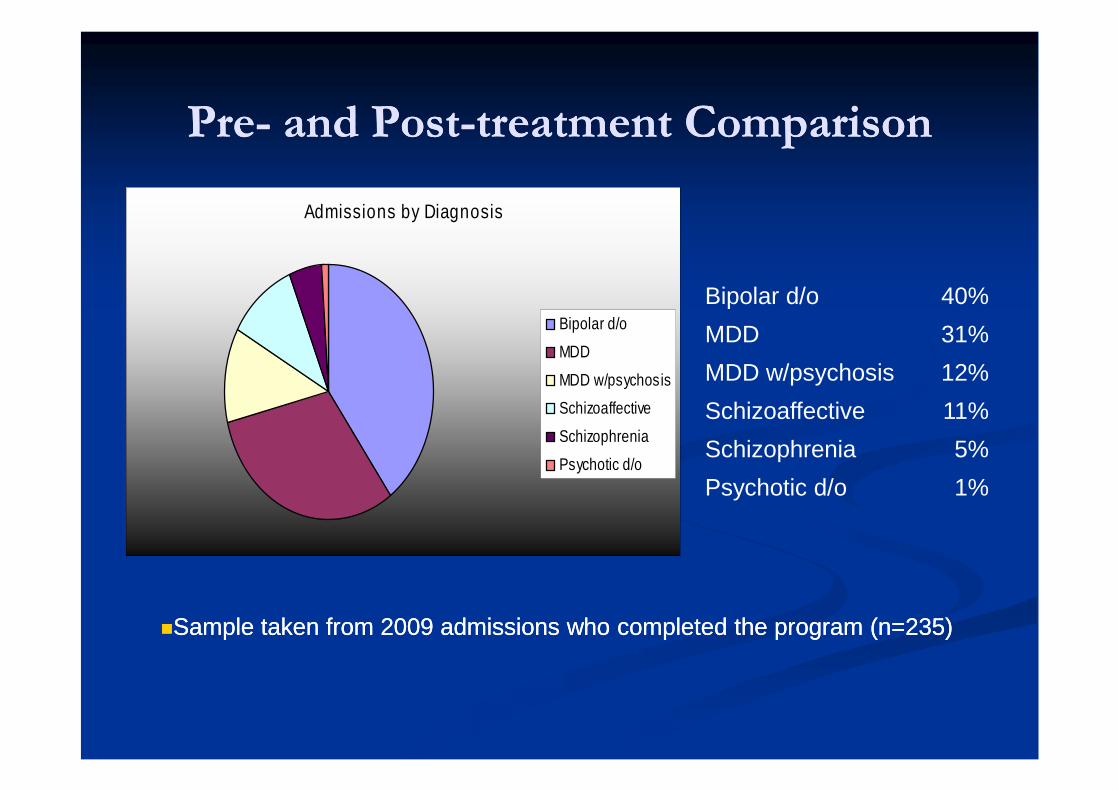
PrePre-- and Postand Post--treatment Comparisontreatment Comparison
Admissions by Diagnosis
Bipolar d/o
MDD
MDD w/psychosis
Schizoaffective
Schizophrenia
Psychotic d/o
Bipolar d/o 40%
MDD 31%
MDD w/psychosis 12%
Schizoaffective 11%
Schizophrenia 5%
Psychotic d/o 1%
Sample taken from 2009 admissions who completed the program (n=235)Sample taken from 2009 admissions who completed the program (n=235)
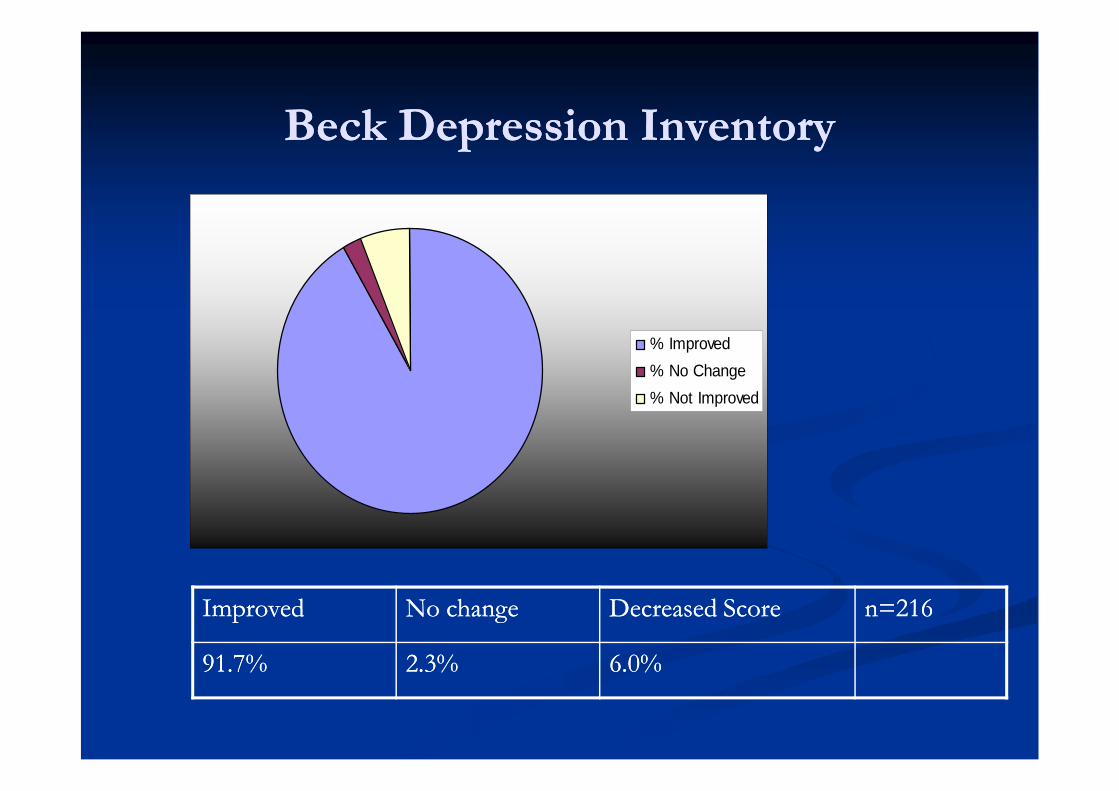
Beck Depression InventoryBeck Depression Inventory
% Improved
% No Change
% Not Improved
ImprovedImproved No changeNo change Decreased ScoreDecreased Score n=216n=216
91.7%91.7% 2.3%2.3% 6.0%6.0%
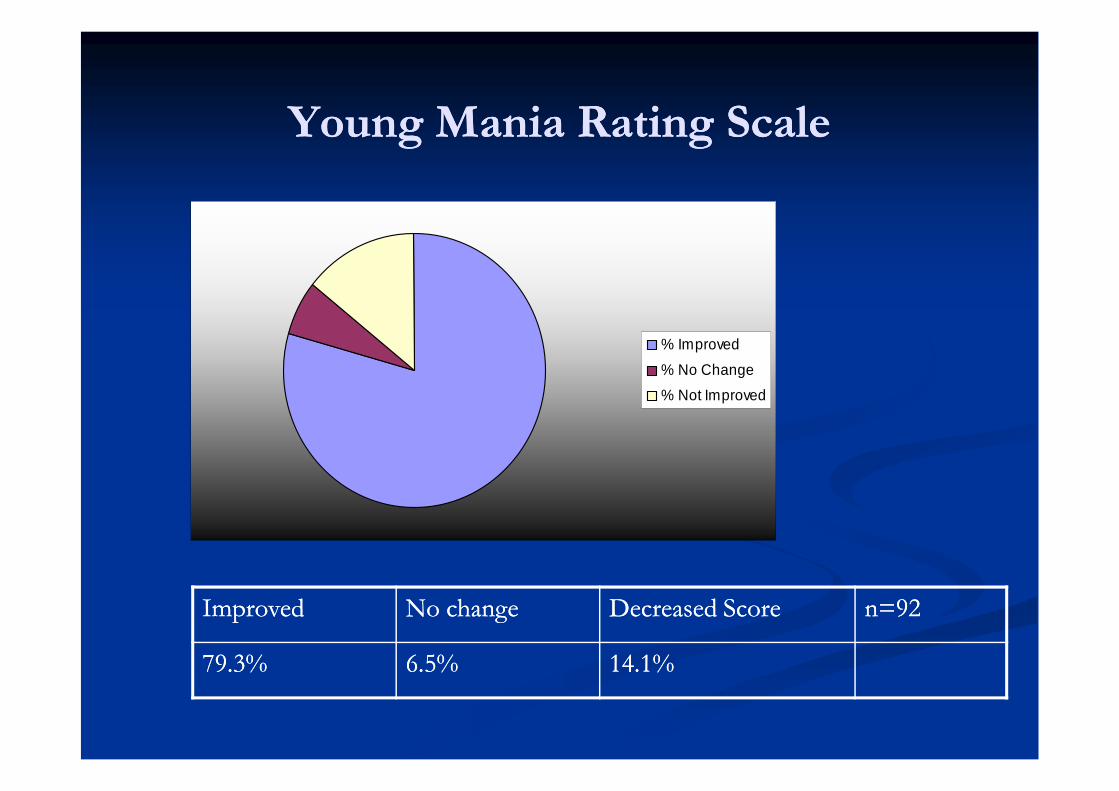
Young Mania Rating ScaleYoung Mania Rating Scale
% Improved
% No Change
% Not Improved
ImprovedImproved No changeNo change Decreased ScoreDecreased Score n=92n=92
79.3%79.3% 6.5%6.5% 14.1%14.1%
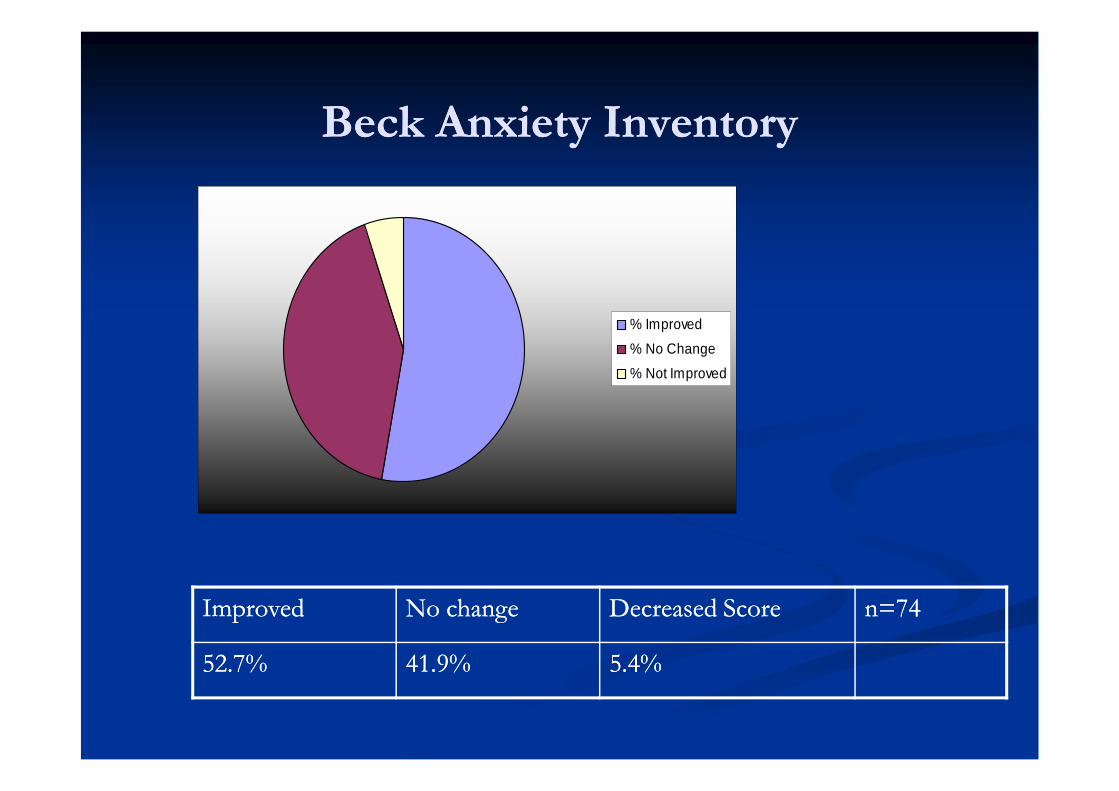
Beck Anxiety InventoryBeck Anxiety Inventory
% Improved
% No Change
% Not Improved
ImprovedImproved No changeNo change Decreased ScoreDecreased Score n=74n=74
52.7%52.7% 41.9%41.9% 5.4%5.4%
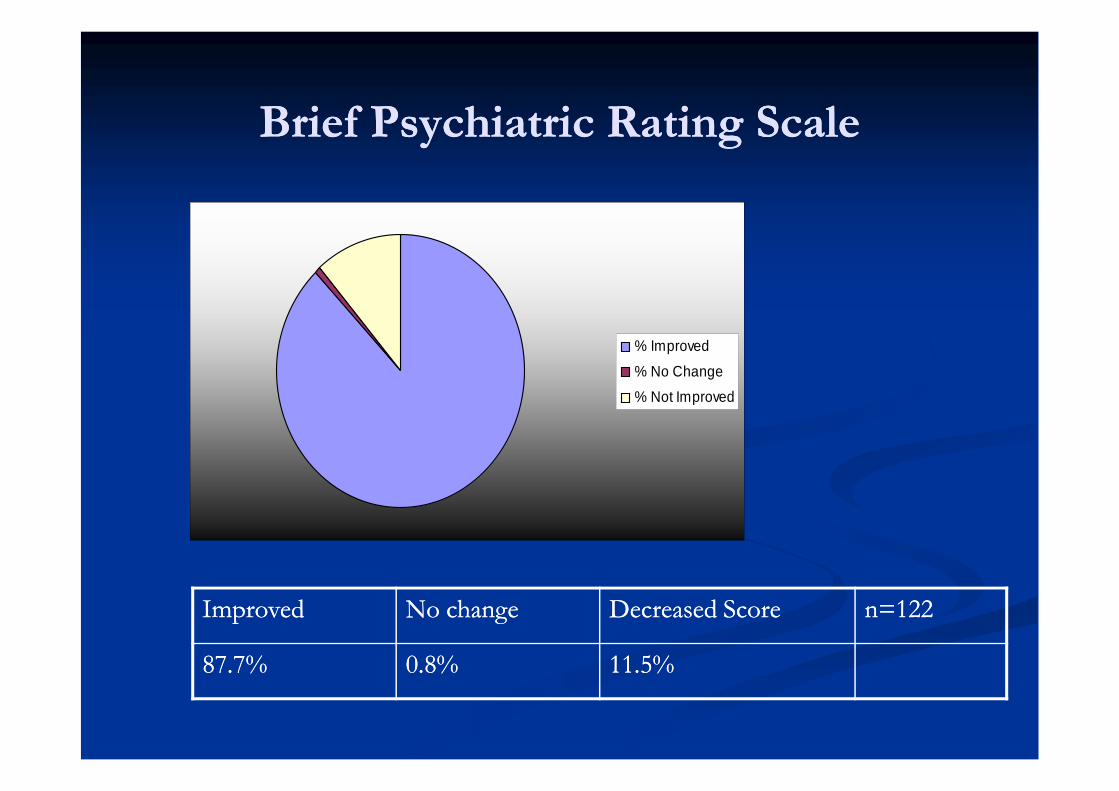
Brief Psychiatric Rating ScaleBrief Psychiatric Rating Scale
% Improved
% No Change
% Not Improved
ImprovedImproved No changeNo change Decreased ScoreDecreased Score n=122n=122
87.7%87.7% 0.8%0.8% 11.5%11.5%
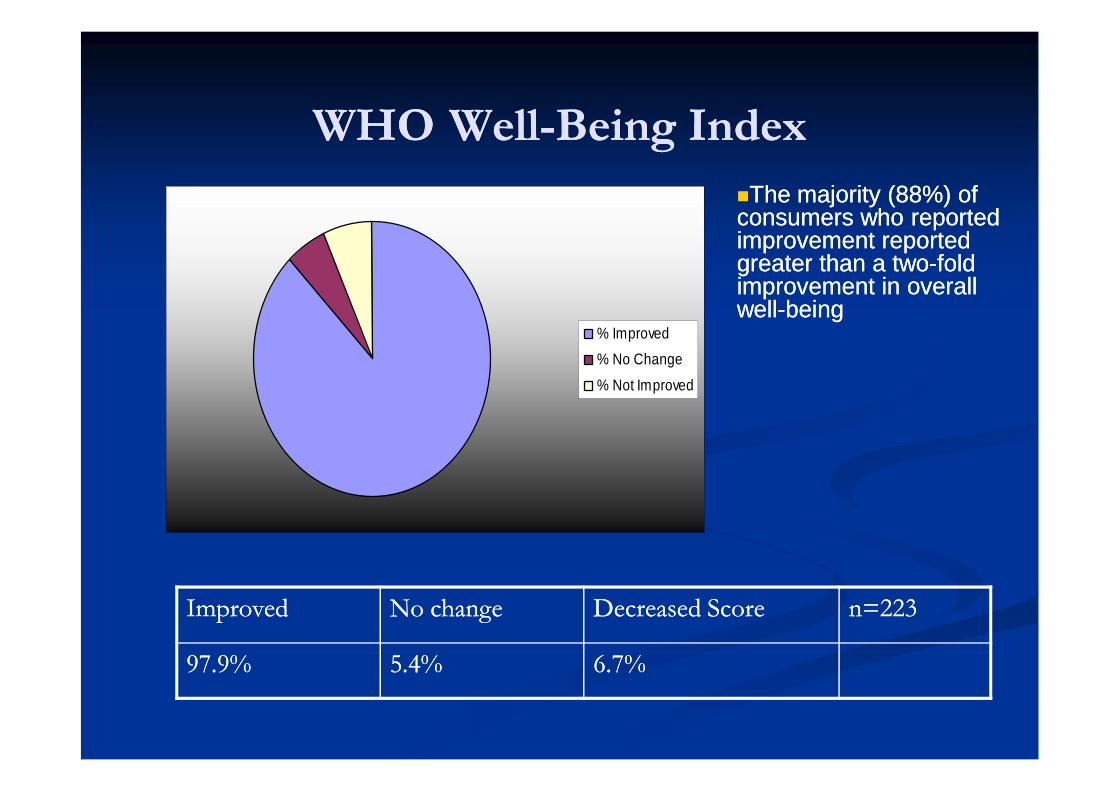
WHOWHO WellWell--Being IndexBeing Index
% Improved
% No Change
% Not Improved
ImprovedImproved No changeNo change Decreased ScoreDecreased Score n=223n=223
97.9%97.9% 5.4%5.4% 6.7%6.7%
The majority (88%) ofThe majority (88%) ofconsumers who reportedconsumers who reportedimprovement reportedimprovement reportedgreater than a twogreater than a two--foldfoldimprovement in overallimprovement in overallwellwell--beingbeing
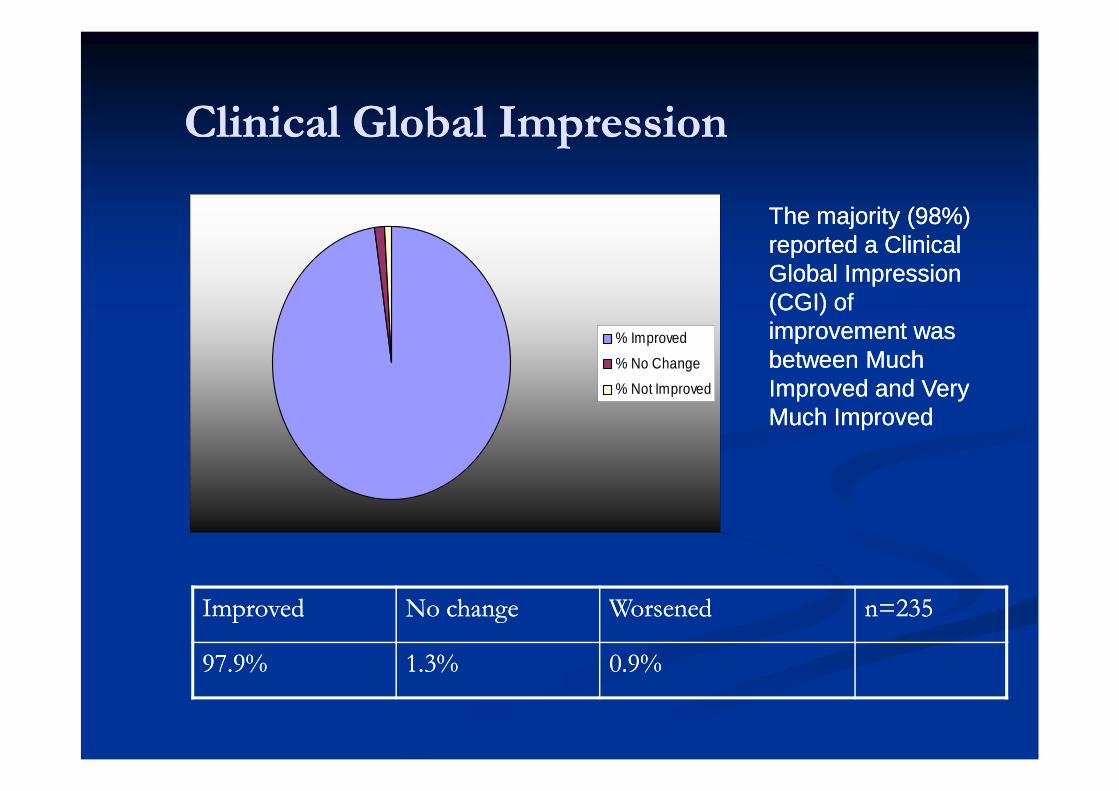
Clinical Global ImpressionClinical Global Impression
% Improved
% No Change
% Not Improved
ImprovedImproved No changeNo change WorsenedWorsened n=235n=235
97.9%97.9% 1.3%1.3% 0.9%0.9%
The majority (98%)The majority (98%)reported a Clinicalreported a ClinicalGlobal ImpressionGlobal Impression(CGI) of(CGI) ofimprovement wasimprovement wasbetween Muchbetween MuchImproved and VeryImproved and VeryMuch ImprovedMuch Improved
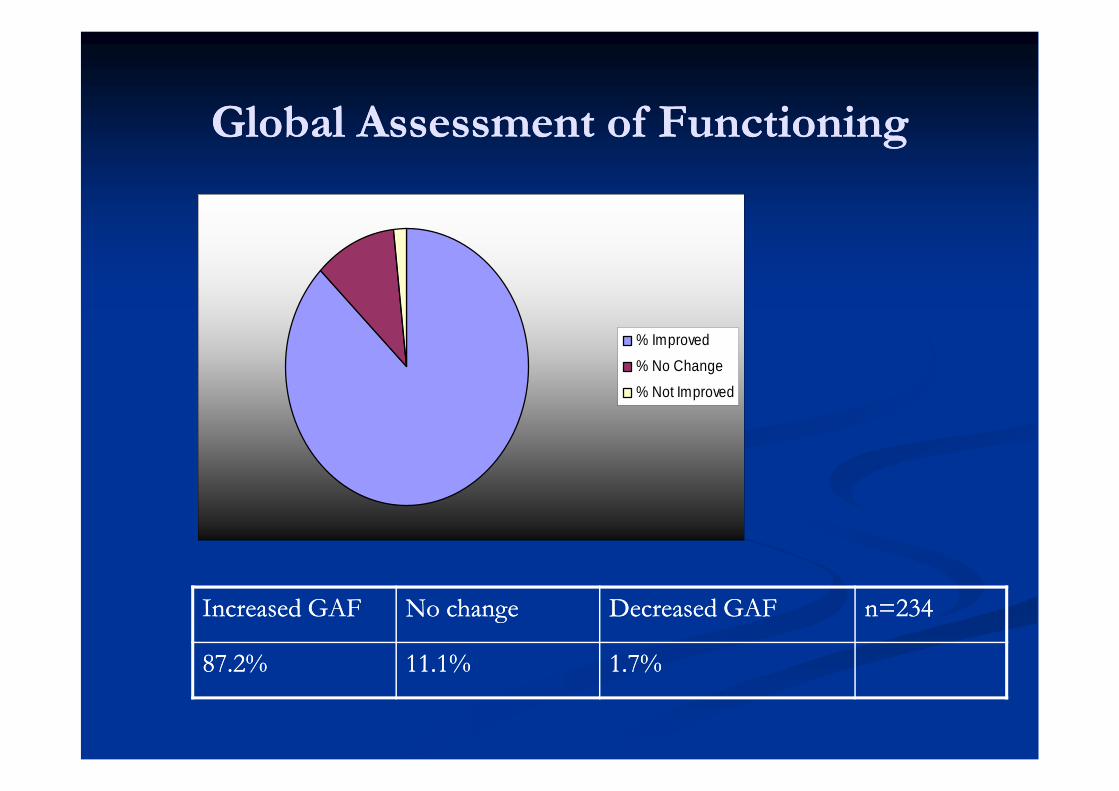
Global Assessment of FunctioningGlobal Assessment of Functioning
% Improved
% No Change
% Not Improved
Increased GAFIncreased GAF No changeNo change Decreased GAFDecreased GAF n=234n=234
87.2%87.2% 11.1%11.1% 1.7%1.7%
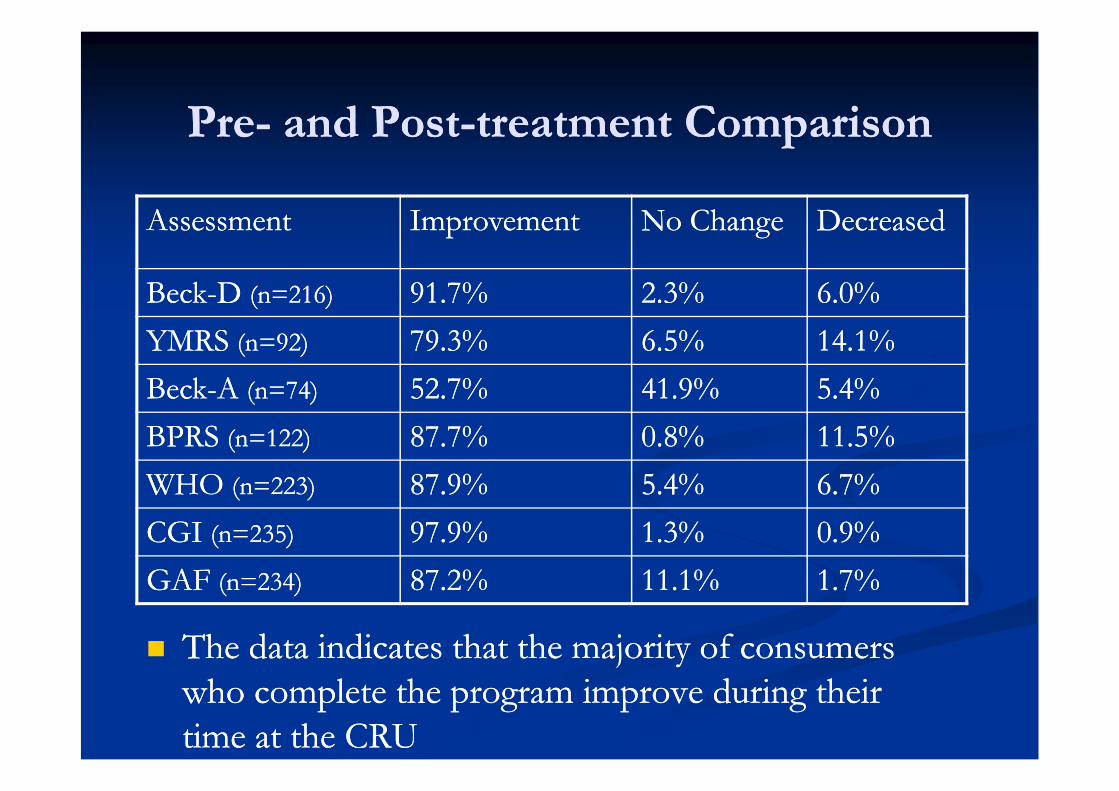
PrePre-- and Postand Post--treatment Comparisontreatment Comparison
The data indicates that the majority of consumersThe data indicates that the majority of consumerswho complete the program improve during theirwho complete the program improve during theirtime at the CRUtime at the CRU
AssessmentAssessment ImprovementImprovement No ChangeNo Change DecreasedDecreased
BeckBeck--DD (n=216)(n=216) 91.7%91.7% 2.3%2.3% 6.0%6.0%
YMRSYMRS (n=92)(n=92) 79.3%79.3% 6.5%6.5% 14.1%14.1%
BeckBeck--AA (n=74)(n=74) 52.7%52.7% 41.9%41.9% 5.4%5.4%
BPRSBPRS (n=122)(n=122) 87.7%87.7% 0.8%0.8% 11.5%11.5%
WHOWHO (n=223)(n=223) 87.9%87.9% 5.4%5.4% 6.7%6.7%
CGICGI (n=235)(n=235) 97.9%97.9% 1.3%1.3% 0.9%0.9%
GAFGAF (n=234)(n=234) 87.2%87.2% 11.1%11.1% 1.7%1.7%
Linkages: Where do they go afterLinkages: Where do they go aftercompleting the CRU program?completing the CRU program?
CompletedProgram
Did NotComplete
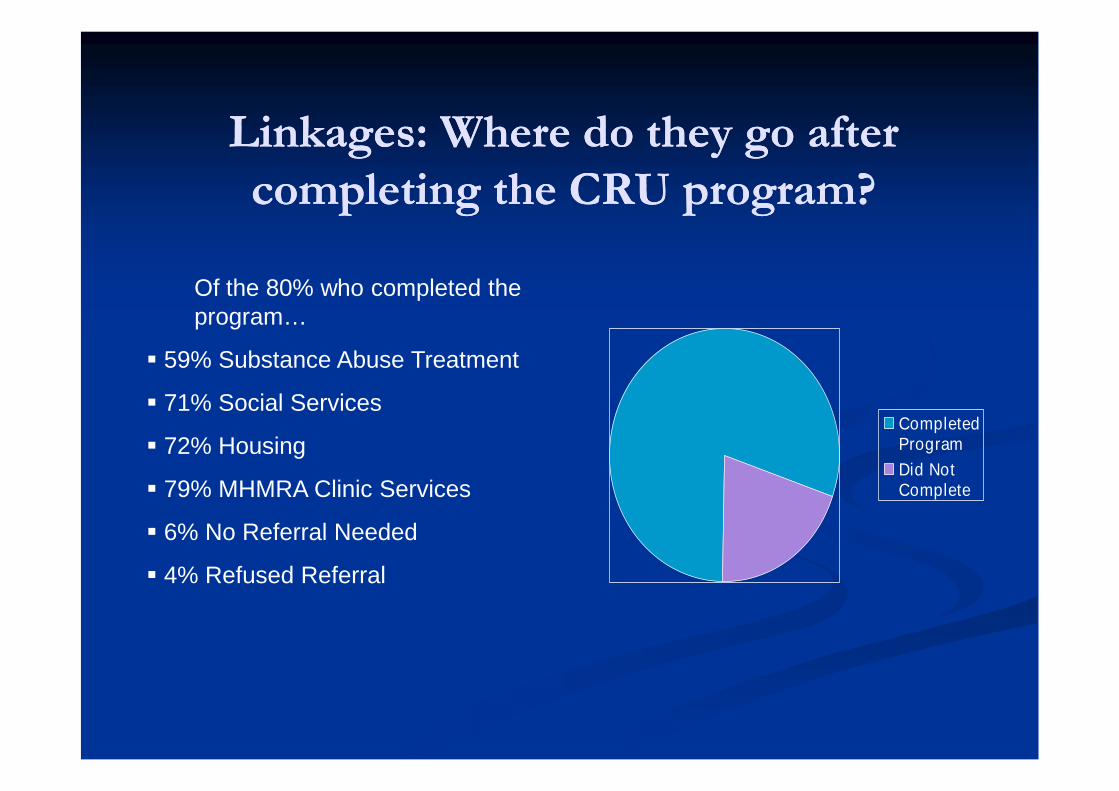
Of the 80% who completed theprogram…
59% Substance Abuse Treatment
71% Social Services
72% Housing
79% MHMRA Clinic Services
6% No Referral Needed
4% Refused Referral
PostPost--Discharge Visits to PsychiatricDischarge Visits to PsychiatricEmergency Services (PES)Emergency Services (PES)
0%
5%
10%
15%
20%
25%
1 2 3 4 5 6 7
Number of Visits to PES
Pe
rce
nt
of
CR
UC
on
su
me
rsV
isit
ing
PE
SP
os
t-D
isc
ha
rge
(alu
mn
ia
nd
no
n-a
lum
ni)
7-12 months after d/c
0-6 months after d/c
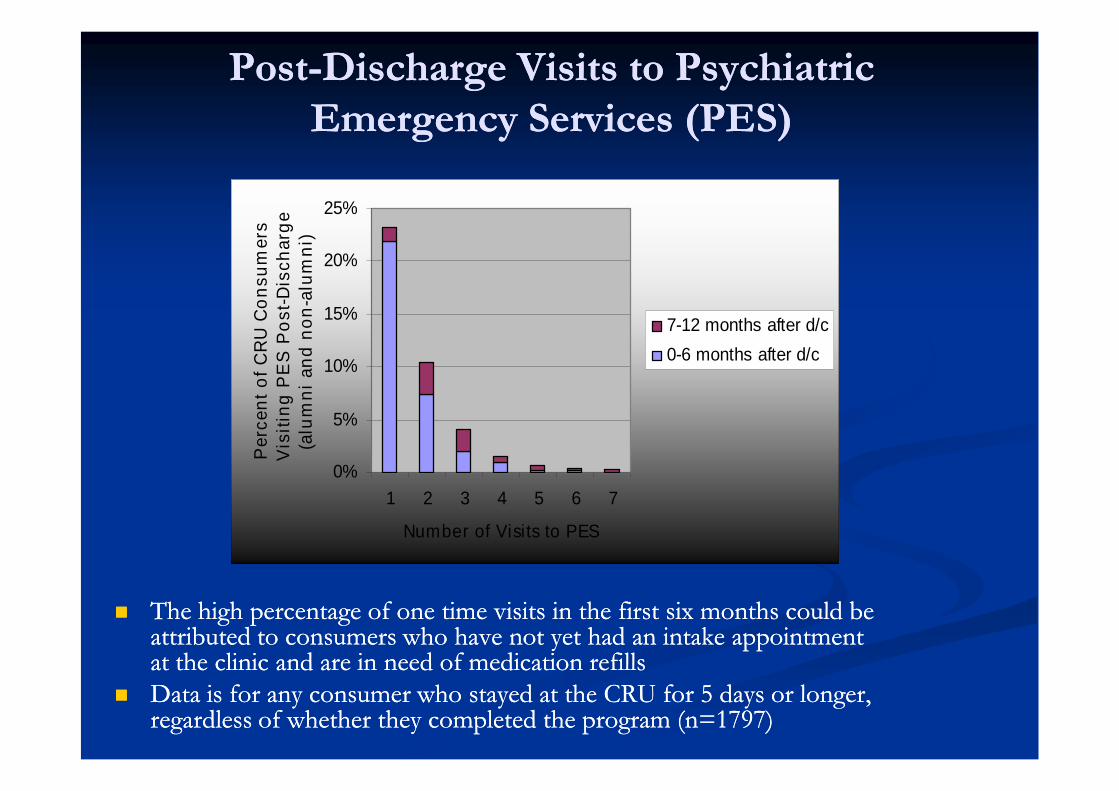
The high percentage of one time visits in the first six months could beThe high percentage of one time visits in the first six months could beattributed to consumers who have not yet had an intake appointmentattributed to consumers who have not yet had an intake appointmentat the clinic and are in need of medication refillsat the clinic and are in need of medication refills
Data is for any consumer who stayed at the CRU for 5 days or longer,Data is for any consumer who stayed at the CRU for 5 days or longer,regardless of whether they completed the program (n=1797)regardless of whether they completed the program (n=1797)
Comparison of SixComparison of Six--Month PreMonth Pre--CRU andCRU andSixSix--Month PostMonth Post--CRU Visits to PESCRU Visits to PES
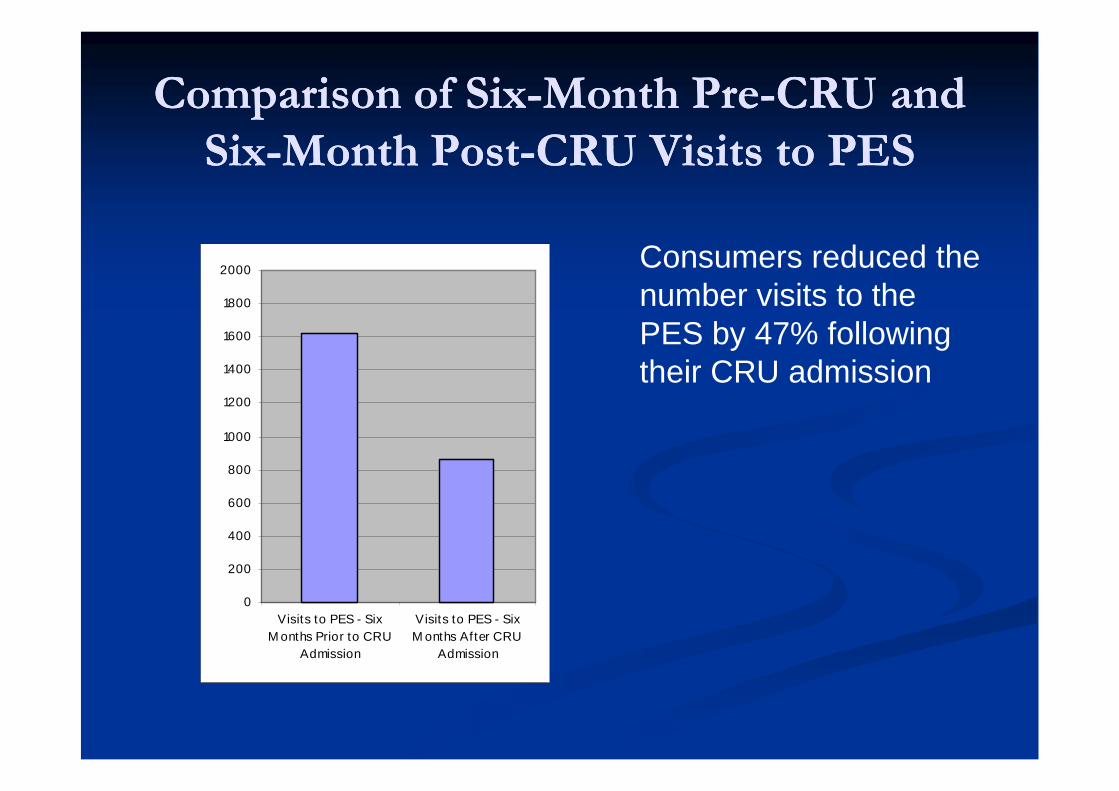
Consumers reduced thenumber visits to thePES by 47% followingtheir CRU admission
0
200
400
600
800
1000
1200
1400
1600
1800
2000
Visits to PES - Six
M onths Prior to CRU
Admission
Visits to PES - Six
M onths After CRU
Admission
Comparison of OneComparison of One--Year PreYear Pre--CRU andCRU andOneOne--Year PostYear Post--CRU visits to PESCRU visits to PES
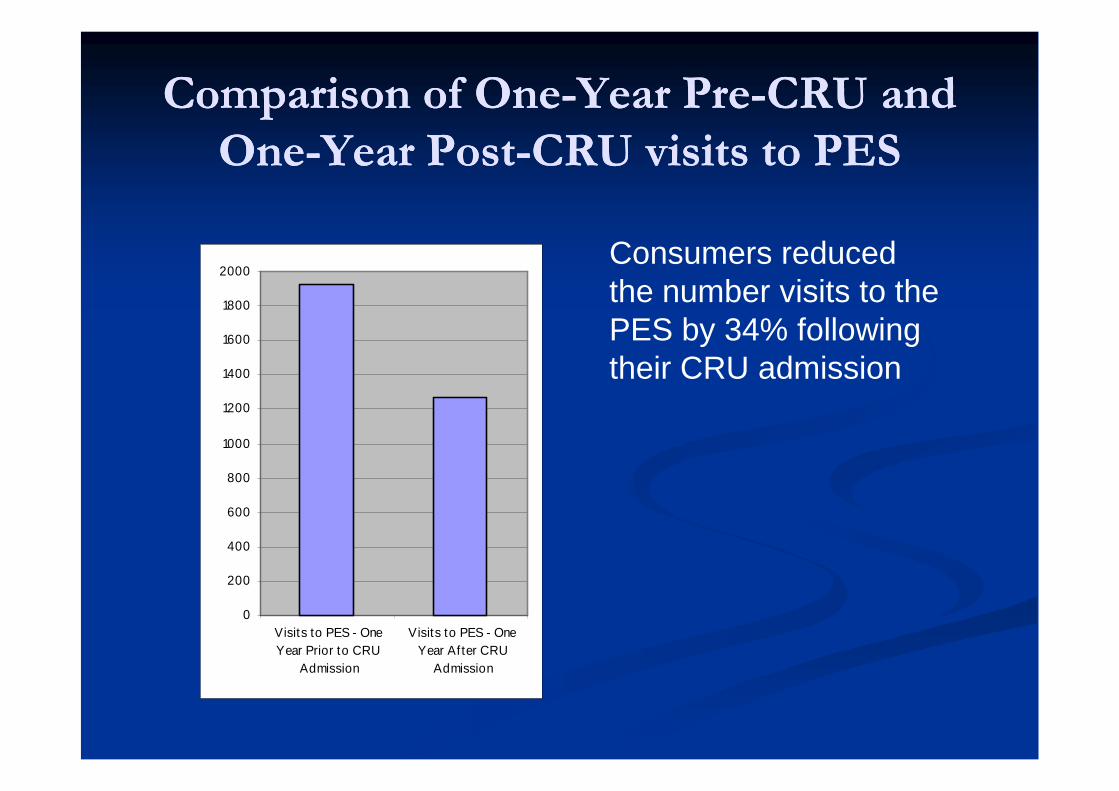
Consumers reducedthe number visits to thePES by 34% followingtheir CRU admission
0
200
400
600
800
1000
1200
1400
1600
1800
2000
Visits to PES - One
Year Prior to CRU
Admission
Visits to PES - One
Year After CRU
Admission
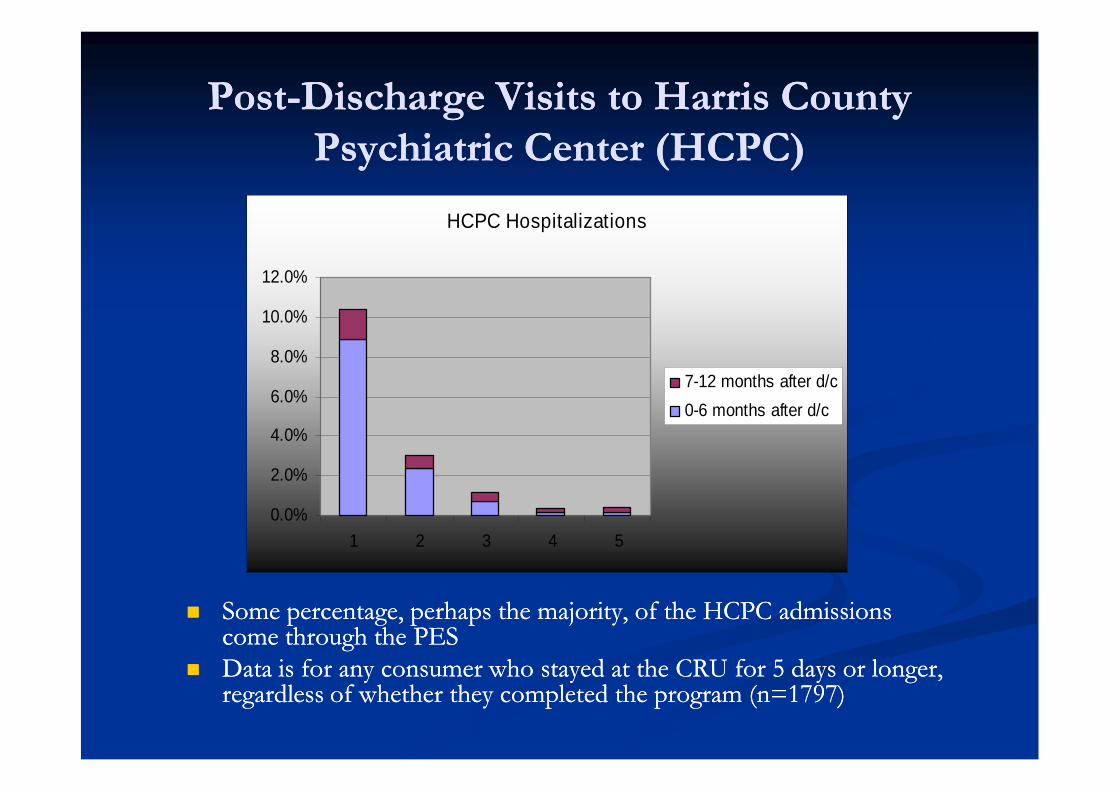
PostPost--Discharge Visits to Harris CountyDischarge Visits to Harris CountyPsychiatric Center (HCPC)Psychiatric Center (HCPC)
Some percentage, perhaps the majority, of the HCPC admissionsSome percentage, perhaps the majority, of the HCPC admissionscome through the PEScome through the PES
Data is for any consumer who stayed at the CRU for 5 days or longer,Data is for any consumer who stayed at the CRU for 5 days or longer,regardless of whether they completed the program (n=1797)regardless of whether they completed the program (n=1797)
HCPC Hospitalizations
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
1 2 3 4 5
7-12 months after d/c
0-6 months after d/c
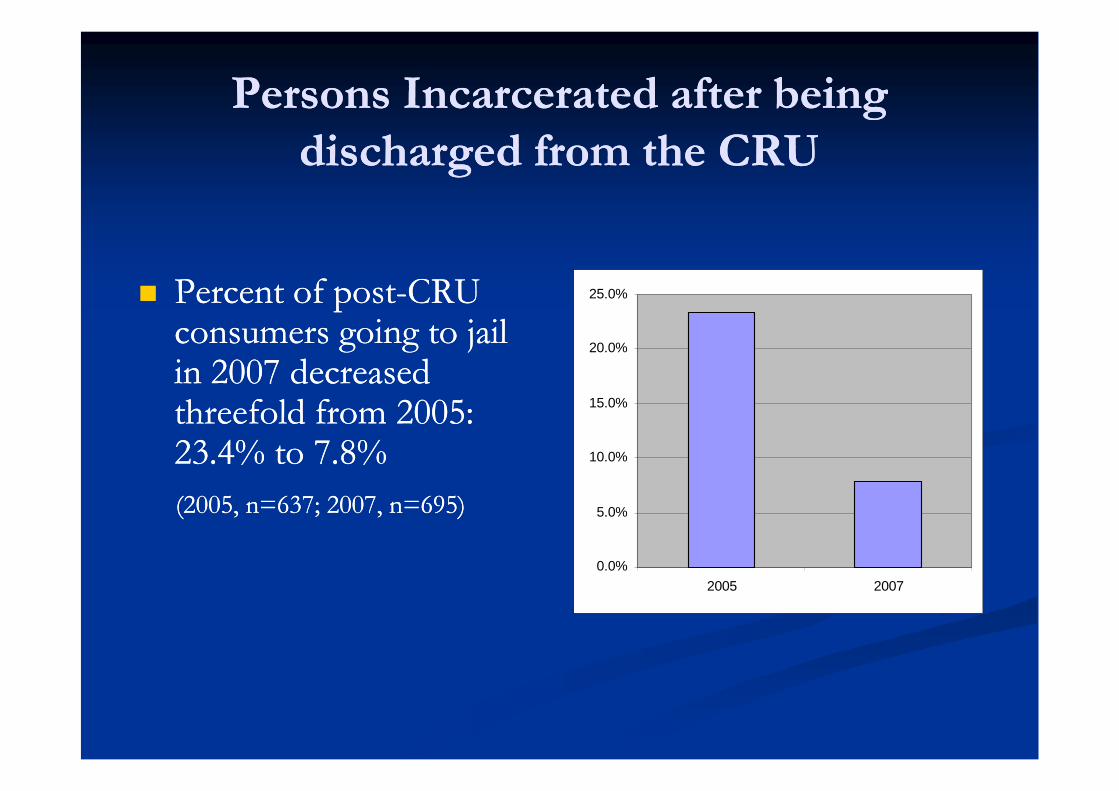
Persons Incarcerated after beingPersons Incarcerated after beingdischarged from the CRUdischarged from the CRU
Percent of postPercent of post--CRUCRUconsumers going to jailconsumers going to jailin 2007 decreasedin 2007 decreasedthreefold from 2005:threefold from 2005:23.4% to 7.8%23.4% to 7.8%
(2005, n=637; 2007, n=695)(2005, n=637; 2007, n=695)
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
2005 2007
Readmits…Readmits…
Readmits as a measure of CRU effectivenessReadmits as a measure of CRU effectiveness
Since the beginning of FY 2009 the CRU readmittedSince the beginning of FY 2009 the CRU readmitted19 consumers (3% of total admits)19 consumers (3% of total admits)
All readmissions occurred more than 90 days after initialAll readmissions occurred more than 90 days after initialCRU dischargeCRU discharge
Ten of the 19 readmissions did not successfully completeTen of the 19 readmissions did not successfully completethe program during their initial admissionthe program during their initial admission
Alumni ParticipationAlumni Participation
Example of alumni services:Example of alumni services:
During April, 2010 there were 443 entries in theDuring April, 2010 there were 443 entries in thealumni log at the CRUalumni log at the CRU
324 suppers were served to alumni324 suppers were served to alumni
235 lunches were served to alumni235 lunches were served to alumni
190 resource contacts by alumni190 resource contacts by alumni
56 group contacts by alumni56 group contacts by alumni
23 alumni counselor contacts (19 hours total)23 alumni counselor contacts (19 hours total)
Crisis Residential UnitCrisis Residential UnitProgram Outcomes SummaryProgram Outcomes Summary
Consumers improve while at the CRUConsumers improve while at the CRU
After completing the CRU program consumersAfter completing the CRU program consumersreduce the number of visits to emergencyreduce the number of visits to emergencyservicesservices
The number jail bookings of CRU consumersThe number jail bookings of CRU consumersappears to be trending downwardappears to be trending downward
Consumers with limited resources have found aConsumers with limited resources have found asupportive environmentsupportive environment
BedBed--Day Costs of CRU vs. HospitalDay Costs of CRU vs. Hospital
The CRU bedThe CRU bed--day cost is $220day cost is $220
MHMRA pays approximately $487 per bed dayMHMRA pays approximately $487 per bed dayfor Harris County Psychiatric Center (countyfor Harris County Psychiatric Center (countyhospital) and $800 or more per bed day forhospital) and $800 or more per bed day forprivate hospital bedsprivate hospital beds
ConclusionConclusion
The implementation of crisis redesign programs hasThe implementation of crisis redesign programs hasmarked the first time in which Texas CMHCs havemarked the first time in which Texas CMHCs havemade a concerted effort to create and implementmade a concerted effort to create and implementalternatives to hospitalization on a widespread basis.alternatives to hospitalization on a widespread basis.
What is clear from Sledge, subsequent research and theWhat is clear from Sledge, subsequent research and thedata produced in connection with the CRU is thatdata produced in connection with the CRU is thatresidential alternatives to hospitalization can be bothresidential alternatives to hospitalization can be bothcost effective and can produce outcomes at least ascost effective and can produce outcomes at least asgood as the outcomes from hospitalization.good as the outcomes from hospitalization.
Conclusion, contd.Conclusion, contd.
It is important to note that the strength of the CRU isIt is important to note that the strength of the CRU isdependent, in large part, on the voluntary nature of thedependent, in large part, on the voluntary nature of theprogram (although we have had “involuntary” patientsprogram (although we have had “involuntary” patientsin our care) and on the availability of hospitalizationin our care) and on the availability of hospitalizationoptions if necessary.options if necessary.
In rural areas where voluntariness and hospitalizationIn rural areas where voluntariness and hospitalizationare not readily available options, more questions areare not readily available options, more questions areraised about the safety of such a unit and the capacityraised about the safety of such a unit and the capacityto be flexible enough to meet the needs of involuntaryto be flexible enough to meet the needs of involuntarypatients.patients.
ChallengesChallenges Sledge, et al. observed that “direct personnel expense is a proxySledge, et al. observed that “direct personnel expense is a proxy
for the essential element for effective outcomes in the provisionfor the essential element for effective outcomes in the provisionof intensive psychiatric services.” p. 1081. This conclusion hasof intensive psychiatric services.” p. 1081. This conclusion hasbeen accurate as it relates to the CRU where many outcomes arebeen accurate as it relates to the CRU where many outcomes areattributable, in large part, to the quality of direct care services.attributable, in large part, to the quality of direct care services.The use of “direct care” here is not limited to quasiThe use of “direct care” here is not limited to quasi--professionalprofessionalstaff, but includes licensed QMHPs and LPHAs. One concernstaff, but includes licensed QMHPs and LPHAs. One concernthis observation raises is how changes in staffing might affect thethis observation raises is how changes in staffing might affect thequality of care provided.quality of care provided.
Challenges, contd.Challenges, contd. A serious recurrent issue is the impact of homelessness onA serious recurrent issue is the impact of homelessness on
relapses among CRU alumni. Ongoing homelessness with littlerelapses among CRU alumni. Ongoing homelessness with littlehope of relief makes this population especially vulnerable tohope of relief makes this population especially vulnerable tocrisiscrisis
The CRU still faces the challenge of adapting its treatment modelThe CRU still faces the challenge of adapting its treatment modelto the needs of seriously psychotic patients who cannot sustainto the needs of seriously psychotic patients who cannot sustainextended periods of group workextended periods of group work
The number of consumers with Axis II diagnoses appears to beThe number of consumers with Axis II diagnoses appears to betrending upward. This creates a difficult group dynamic andtrending upward. This creates a difficult group dynamic andillustrates the need to better serve this populationillustrates the need to better serve this population
An additional challenge is to begin offering more group servicesAn additional challenge is to begin offering more group servicesto alumni to decrease longto alumni to decrease long--term use of acute care hospitals.term use of acute care hospitals.
Quantifying and monitoring outcomes is one of the biggestQuantifying and monitoring outcomes is one of the biggestongoing challenges faced by the CRUongoing challenges faced by the CRU
FinisFinis
It is the journeyIt is the journey –– not the destinationnot the destination –– that hasthat hasbeen an humbling experience to all of us whobeen an humbling experience to all of us whohave been on the road since the beginning ofhave been on the road since the beginning ofthe CRU. Our patients are among the mostthe CRU. Our patients are among the mostresourceful, adaptable and resilient people thatresourceful, adaptable and resilient people thatany of us have ever had the privilege of workingany of us have ever had the privilege of workingwith. Not only have our patients gotten betterwith. Not only have our patients gotten betterin this setting, but so have we.in this setting, but so have we.





























