Embed Size (px)
Citation preview
Who should get long term anticoagulation for PE/DVT
Financial Disclaimer: against the drug companies
● My financial interests are only as a purchaser of insurance and a taxpayer
○ Concern about prices
● Physician and caring person
○ Concern about impoverishing the needy
○ Concerned about truth and advertising
Goals of the talk
○ A framework for deciding on which patients might need prolonged anticoagulation
○ what are the guidelines for prolonged anticoagulation
○ what are the problems in applying those guidelines
○ methods for increasing the Predictive Value of the decision

Framework
Balancing Risk
Anticoagulate • Bleeding
Don’t anticoagulate • Pulmonary
embolism
Principle: Risk vs Risk
● Risk of failure to anticoagulate
○ Massive pulmonary embolism ○ Other thrombotic complication
○ Risk of anticoagulation
○ Bleeding ○ Treatment complication
Risk Decay
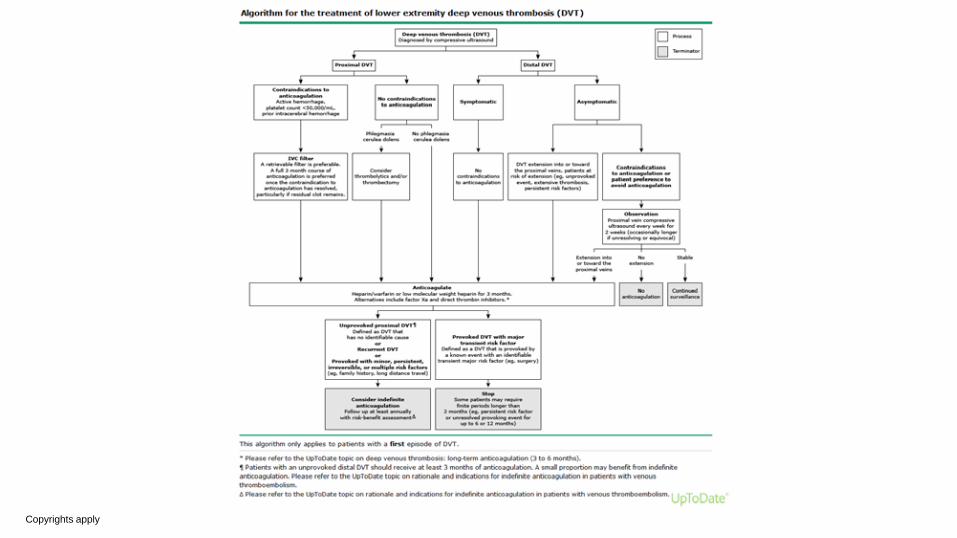
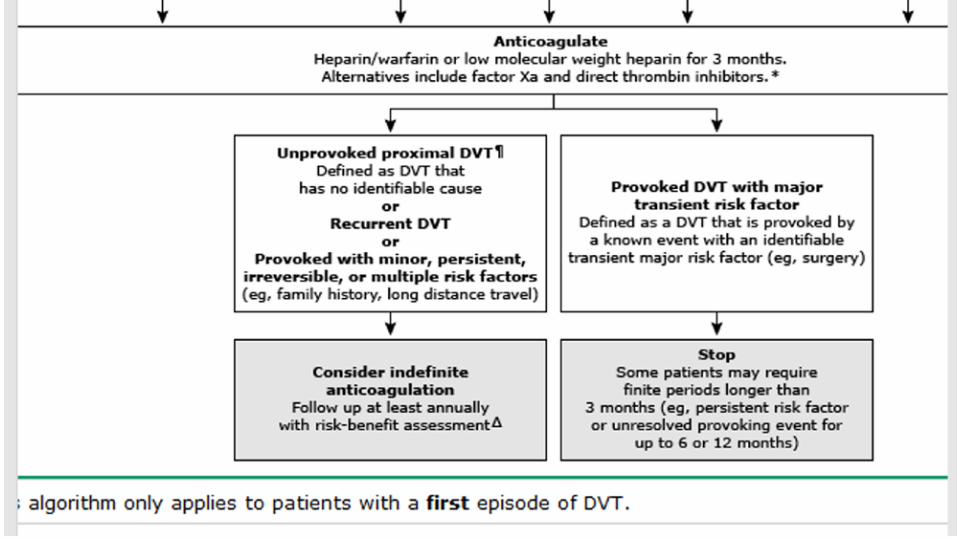
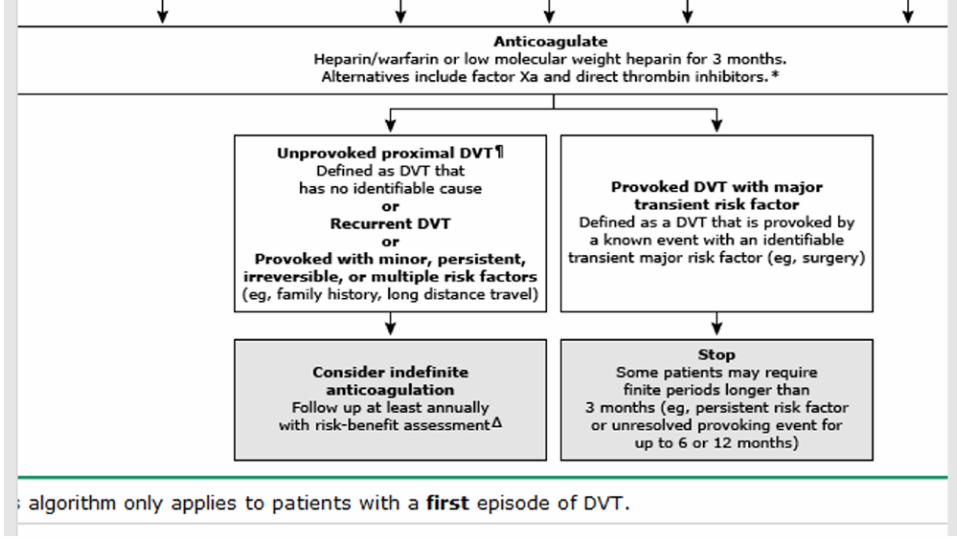
Most patients with acute venous thromboembolism (VTE) require anticoagulation for a minimum of three months
○ Risk decay curve
with some patients requiring longer finite periods of 6 to 12 months.
Copyrights apply
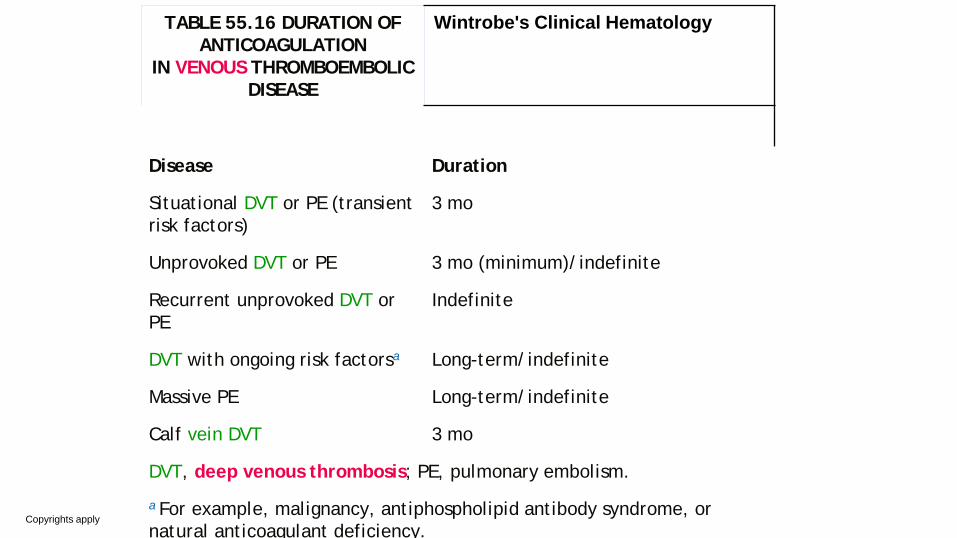
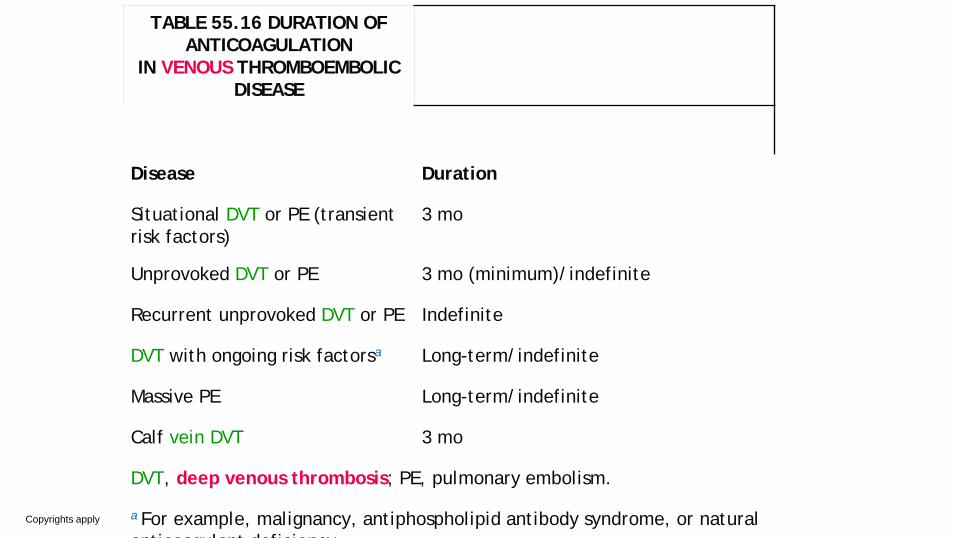
TABLE 55.16 DURATION OF ANTICOAGULATION
IN VENOUS THROMBOEMBOLIC DISEASE
Wintrobe's Clinical Hematology
Disease Duration
Situational DVT or PE (transient risk factors)
3 mo
Unprovoked DVT or PE 3 mo (minimum)/indefinite
Recurrent unprovoked DVT or PE
Indefinite
DVT with ongoing risk factorsa Long-term/indefinite
Massive PE Long-term/indefinite
Calf vein DVT 3 mo
DVT, deep venous thrombosis; PE, pulmonary embolism.
a For example, malignancy, antiphospholipid antibody syndrome, or natural anticoagulant deficiency.
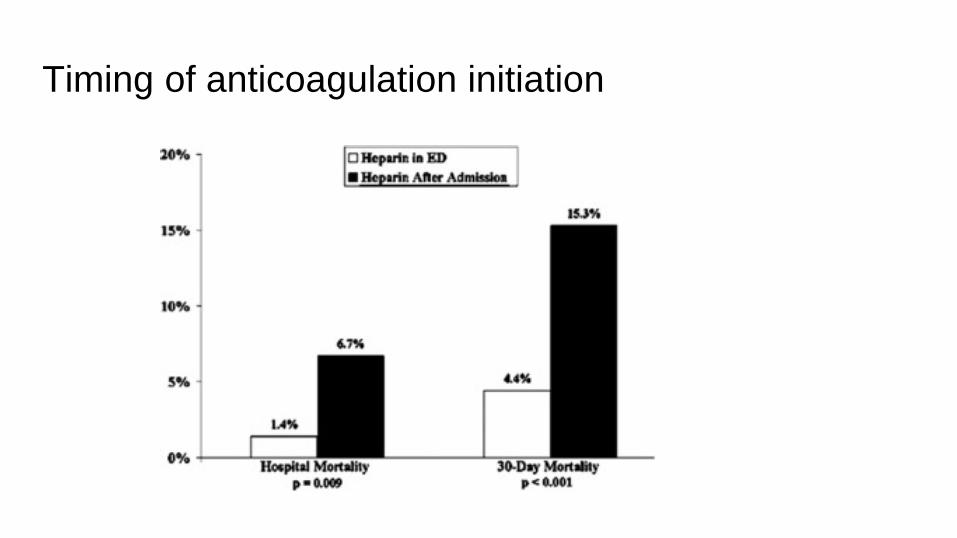
Timing of anticoagulation initiation
Copyrights apply
PATIENTS LIKELY TO BENEFIT
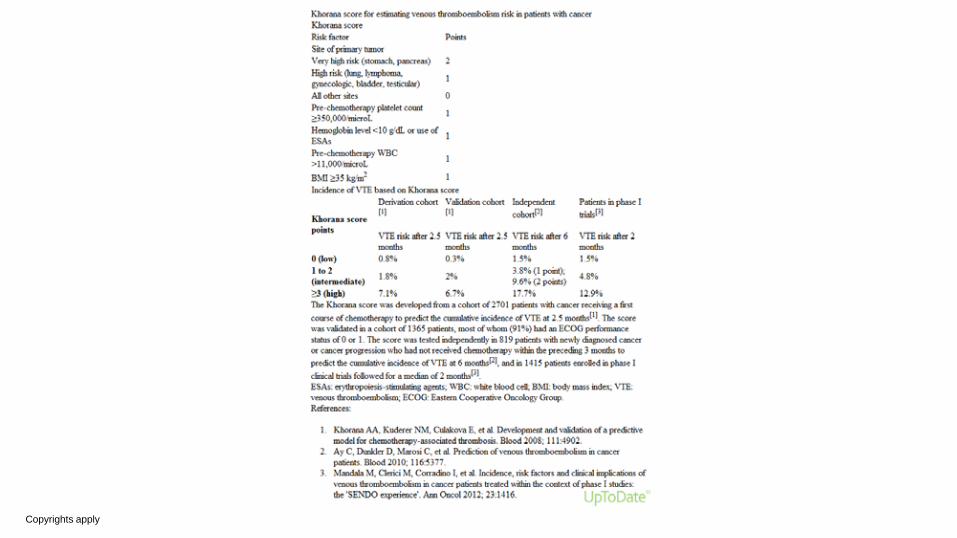
● Unprovoked proximal DVT ● Symptomatic PE ● Recurrence with anticoagulation ● Recurrence without anticoagulation ● Recurrent unprovoked VTE ● Active cancer
○ Khorana score
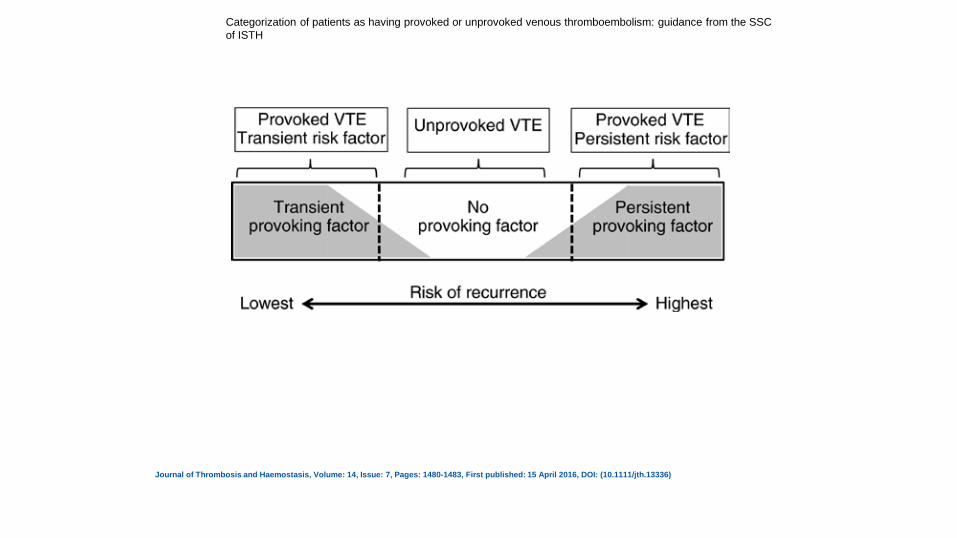
Categorization of patients as having provoked or unprovoked venous thromboembolism: guidance from the SSC of ISTH
Journal of Thrombosis and Haemostasis, Volume: 14, Issue: 7, Pages: 1480-1483, First published: 15 April 2016, DOI: (10.1111/jth.13336)
Copyrights apply
Copyrights apply
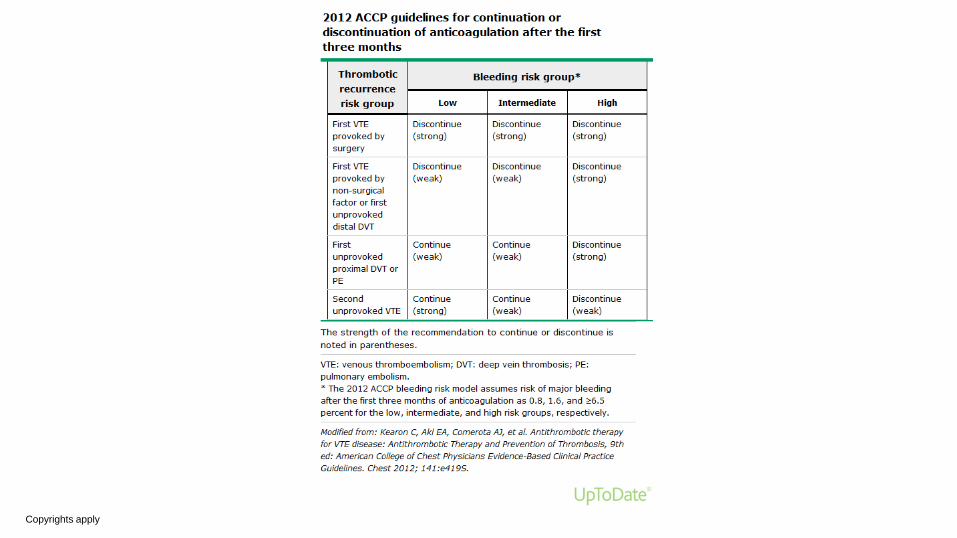
guidelines
Recent Guideline ASH: Guidelines for management of venous thromboembolism – Optimal
management of anticoagulation therapy (2018)
American College of Chest Physicians (CHEST): Guideline and expert panel
report on antithrombotic therapy for VTE disease (2016)
ISTH: Guidance for the categorization of patients as having provoked or
unprovoked venous thromboembolism (2016)
Copyrights apply
Copyrights apply
Copyrights apply
Copyrights apply
TABLE 55.16 DURATION OF ANTICOAGULATION
IN VENOUS THROMBOEMBOLIC DISEASE
Disease Duration
Situational DVT or PE (transient risk factors)
3 mo
Unprovoked DVT or PE 3 mo (minimum)/indefinite
Recurrent unprovoked DVT or PE Indefinite
DVT with ongoing risk factorsa Long-term/indefinite
Massive PE Long-term/indefinite
Calf vein DVT 3 mo
DVT, deep venous thrombosis; PE, pulmonary embolism.
a For example, malignancy, antiphospholipid antibody syndrome, or natural anticoagulant deficiency
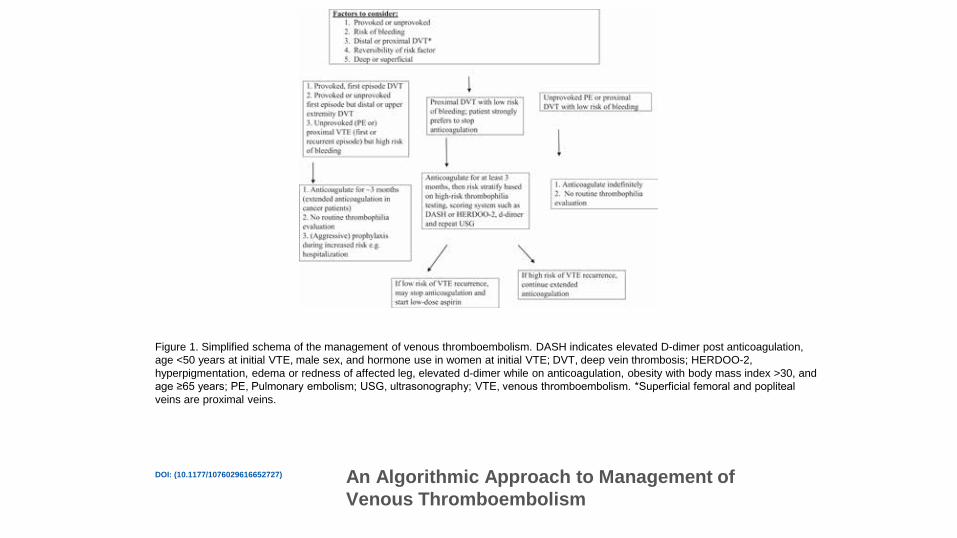
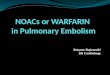
Figure 1. Simplified schema of the management of venous thromboembolism. DASH indicates elevated D-dimer post anticoagulation, age <50 years at initial VTE, male sex, and hormone use in women at initial VTE; DVT, deep vein thrombosis; HERDOO-2, hyperpigmentation, edema or redness of affected leg, elevated d-dimer while on anticoagulation, obesity with body mass index >30, and age ≥65 years; PE, Pulmonary embolism; USG, ultrasonography; VTE, venous thromboembolism. *Superficial femoral and popliteal veins are proximal veins.
DOI: (10.1177/1076029616652727) An Algorithmic Approach to Management of Venous Thromboembolism
DASH score ● D dimer
○ 1 month after stopping anticoagulation
● Age
○ Less than 50
● Sex
○ Male
● Hormone
○ Estrogen
Copyrights apply
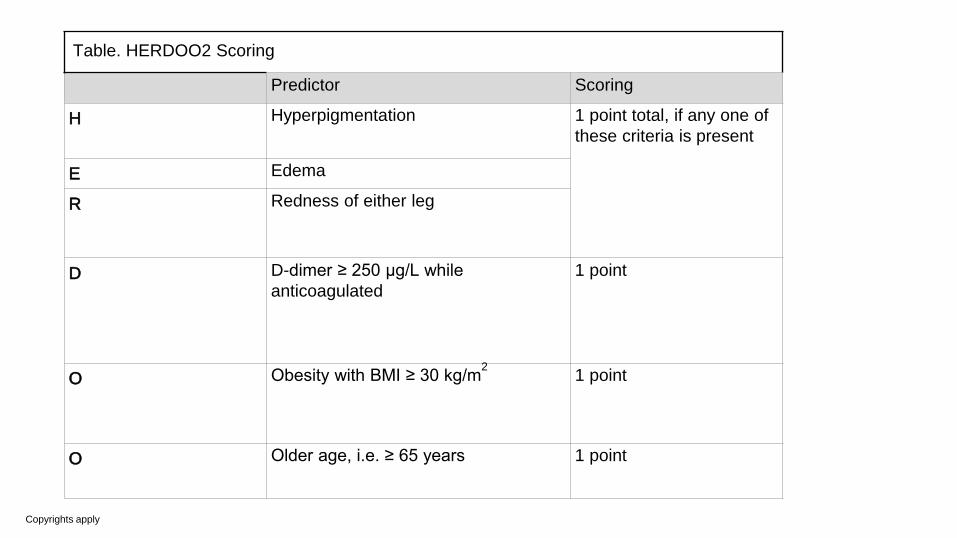
Table. HERDOO2 Scoring
Predictor Scoring
H Hyperpigmentation 1 point total, if any one of these criteria is present
E Edema
R Redness of either leg
D D-dimer ≥ 250 μg/L while anticoagulated
1 point
O Obesity with BMI ≥ 30 kg/m2 1 point
O Older age, i.e. ≥ 65 years 1 point
problems in applying the guidelines
Things that are not clear ● What constitutes provoked?
○ Airline flight
○ Cast immobilization
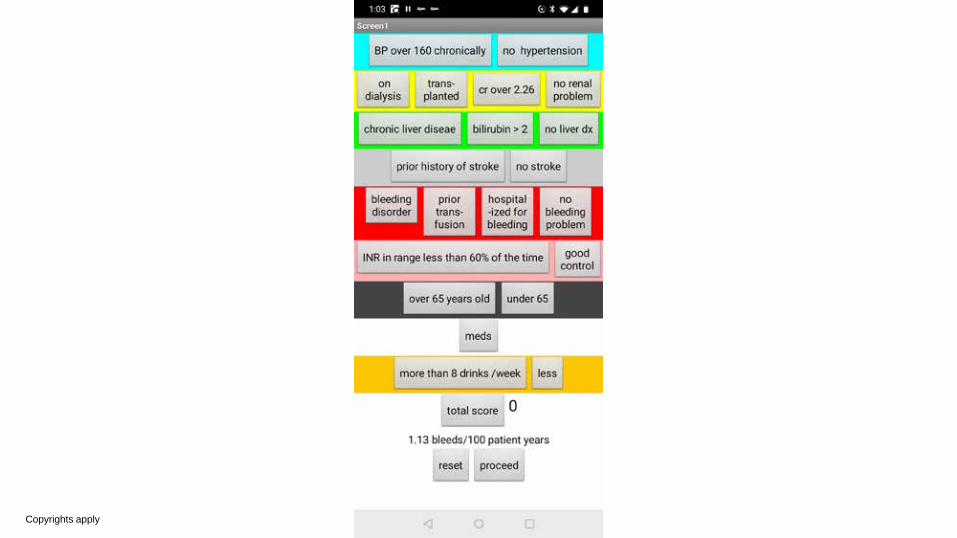
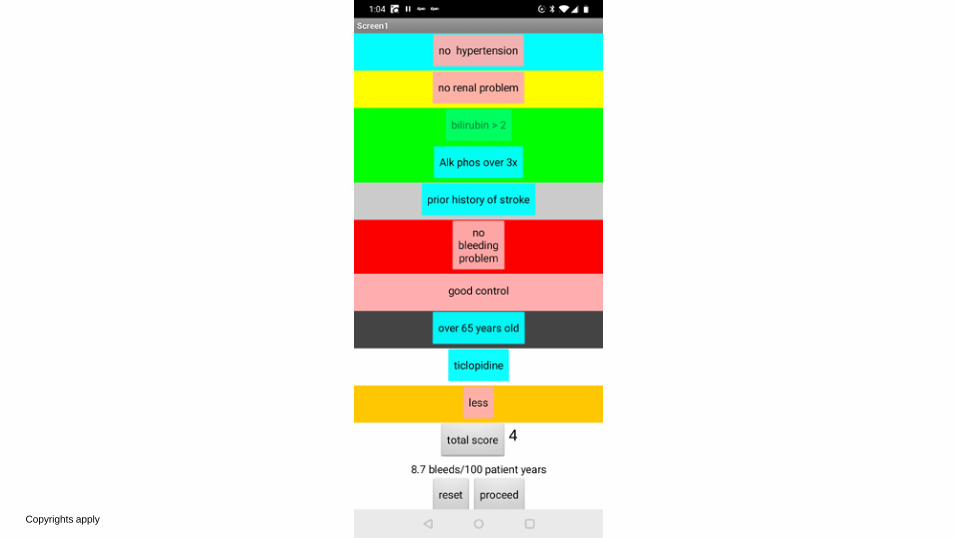
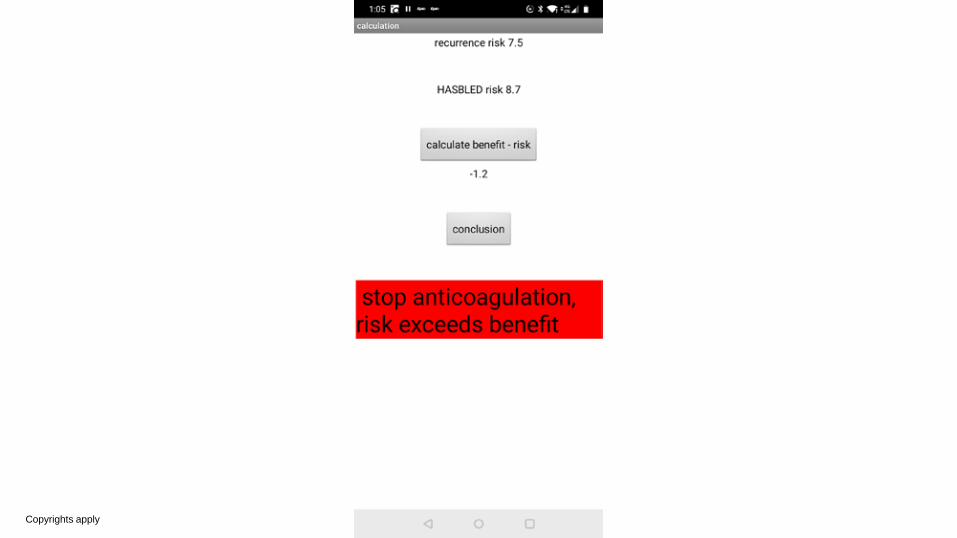
● How to calculate the balance of risks
○ Apps
● Which anticoagulant
○ Heparinoids
○ NOACs
Copyrights apply
Airline flight: UpToDate
Provoked VTE with transient risk factor
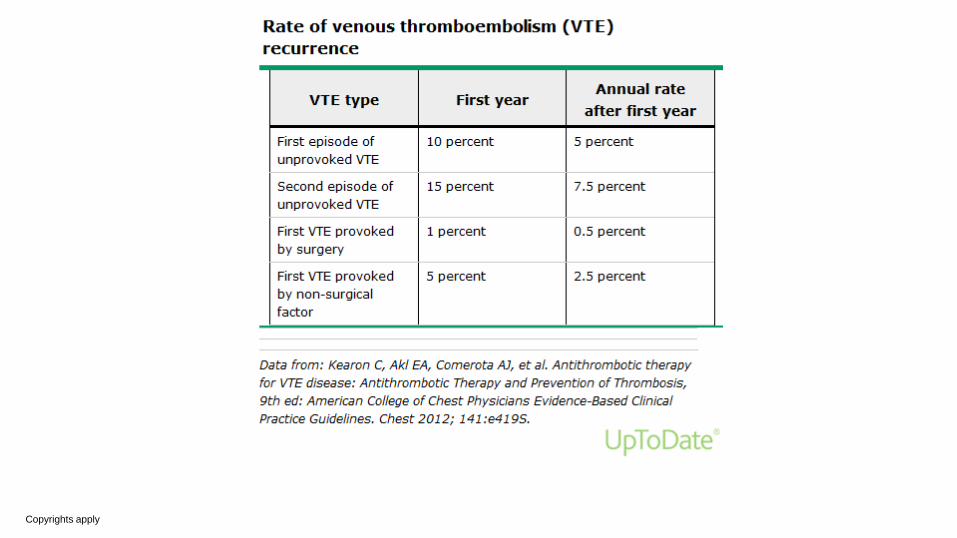
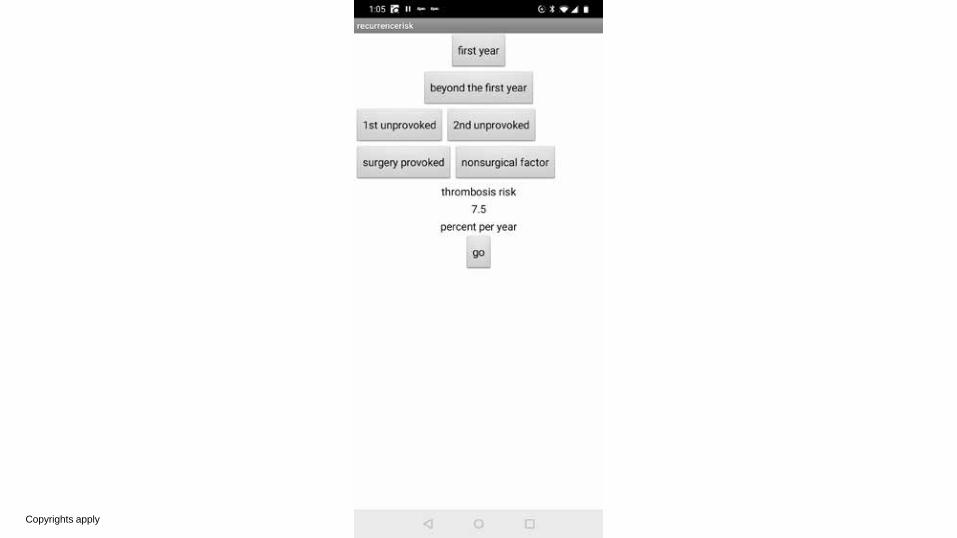
VTE provoked by a nonsurgical trigger (eg, oral contraceptive pill, long flight, pregnancy), the risk of VTE recurrence is estimated to 5 percent at one year and 15 percent at five years (approximately 2.5 percent per year after the first year)
Airline Flight Risk Recent publications report the risk of venous thromboembolism (VTE) is increased 1.5 to 3 fold (Timp 2015), by approximately two fold (Cannegieter 2006; WRIGHT project 2007), or four fold (Kuipers 2007), following long-haul travel.
Kuipers and colleagues also reported that the "absolute risk of a symptomatic event within 4 weeks of flights longer than 4 h is 1/4600 flights" and "the risk of severe pulmonary embolism (PE) occurring immediately after air travel increases with duration of travel, up to 4.8 per million in flights longer than 12 h" (Kuipers 2007).
Low molecular weight heparin for prevention of venous thromboembolism in patients with lower-limb immobilization.
● Moderate-quality evidence showed LMWH reduced DVT when immobilization of the lower limb was required
○ when compared with no prophylaxis or placebo.
● Low-quality evidence showed no clear differences in PE between the LMWH and control groups,
● less symptomatic VTE in the LMWH groups. ● The quality of the evidence was downgraded due to risk of bias and
imprecision.
Predictive Value
How to decide ● Sum of all risks ● Physiologic understanding ● Aversions
○ Risk
○ cost
How is the decision made ● Kahneman system I
○ Risk aversion ○ Ineffables
● System II ○ Quantitative analysis
Copyrights apply
Copyrights apply
Copyrights apply
Copyrights apply
Copyrights apply
Goals of the talk
○ A framework for deciding on which patients might need prolonged anticoagulation
○ what are the guidelines for prolonged anticoagulation
○ what are the problems in applying those guidelines
○ methods for increasing the Predictive Value of the decision
Low molecular weight heparin for prevention of venous thromboembolism in patients with lower-limb immobilization.
rationale for extending anticoagulation indefinitely
● based upon long-term epidemiologic studies of recurrence risk after cessation of a conventional course of anticoagulation
● as well as randomized trials and meta-analyses that suggest that anticoagulation for prolonged periods successfully reduces the rate of VTE recurrence
Airline flight: UpToDate PATIENTS UNLIKELY TO BENEFIT
We and others agree that indefinite anticoagulation is unlikely to benefit the populations described below, provided that
persistent risk factors, which would elevate the risk of recurrence, are absent [3-5]. (See 'Assess additional risk factors'
below.)
Provoked VTE with transient risk factor — For most patients who have a provoked VTE with transient medical or surgical
risk factors, we recommend anticoagulation for three to six months rather than periods of longer or shorter duration. For
those with a VTE provoked by a transient surgical risk factor, the risk of VTE recurrence is estimated to be 1 percent at one
year and 3 percent at five years (approximately 0.5 percent per year after the first year) [3-5,7,8]. For those with a VTE
provoked by a nonsurgical trigger (eg, oral contraceptive pill, long flight, pregnancy), the risk of VTE recurrence is
estimated to 5 percent at one year and 15 percent at five years (approximately 2.5 percent per year after the first year) [3-
5,7,8].
issues
● How to decide
○ Sum of all risks
○ Physiologic understanding
○ Aversions
■ Risk
■ cost
● Things that are not clear
● Which anticoagulant
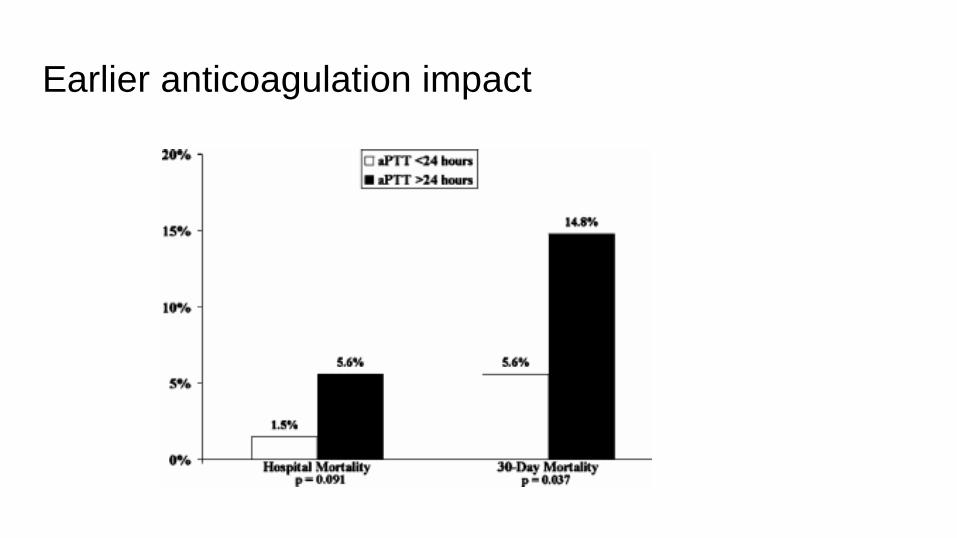
Earlier anticoagulation impact
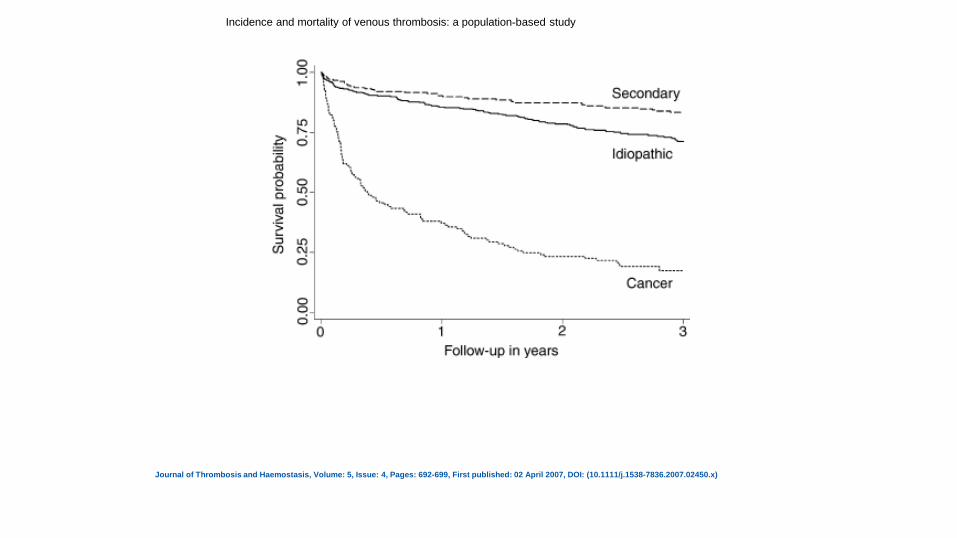
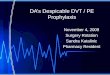
Incidence and mortality of venous thrombosis: a population-based study
Journal of Thrombosis and Haemostasis, Volume: 5, Issue: 4, Pages: 692-699, First published: 02 April 2007, DOI: (10.1111/j.1538-7836.2007.02450.x)
rationale for extending anticoagulation indefinitely
● long-term epidemiologic studies ● of recurrence risk ● after cessation of a conventional course of anticoagulation
● randomized trials and meta-analyses ● suggest that anticoagulation for prolonged periods ● reduces the rate of VTE recurrence
DASH score Application
● previously diagnosed with VTE ● completed a 3-6 month course of anticoagulation ● DASH Scores ≤1 are associated with 3.1% annual recurrence
○ may be low enough to consider discontinuing anticoagulation.
● DASH Scores ≥2 are at high risk for recurrent VTE
○ may require long-term anticoagulation.
● https://www.mdcalc.com/dash-prediction-score-recurrent-vte#use-cases
Copyrights apply
UNPROVOKED VTE
No provoking risk factor (transient or persistent)

Copyrights apply
Total follow-up# Periods of follow-up after VT
0–0.49 years
0.50–2.99 years
≥ 3 years
Total population
92 804 1 1 1 1
Idiopathic† 373 2.57 (2.17–3.04)
4.36 (3.12–6.08)
1.83 (1.44–2.32)
1.24 (0.87–1.75)
Secondary‡ 236 1.97 (1.52–2.57)
4.85 (3.07–7.66)
1.05 (0.68–1.63)
1.09 (0.68–1.75)
Cancer¶ 131 12.73 (10.59–15.29)
33.78 (26.41–43.21)
7.29 (5.25–10.13)
2.48 (1.24–4.95)
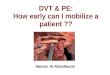
Categorization of patients as having provoked or unprovoked venous thromboembolism: guidance from the SSC of ISTH
VTE PROVOKED BY A TRANSIENT RISK FACTOR*
Major transient risk factor during the 3 months before diagnosis ofVTE
A risk factor is considered ‘major’ if it has been shown to beassociated with:
(1)half the risk of recurrent VTE after stopping anticoagulant ther-apy (compared with if there was no transient risk factor), whenthe risk factor occurred up to 3 months before the VTE†;or
(2)a greater than10-fold increase in the risk of having a first VTE.
Examples:
•Surgery with general anesthesia for greater than 30 min.
•Confined to bed in hospital (only ‘bathroom privileges’) for atleast 3 days with an acute illness.
•Cesarean section
Minor (yet important) transient risk factor during the 2 months before diagnosis of VTE A risk factor is considered ‘minor’ if it has been shown to be associated with:
(1)half the risk of recurrent VTE after stopping anticoagulant therapy (compared with if there was no transient risk factor), when the risk factor occurred up to 2 months before the VTE †;or
(2)a 3 to 10-fold increase in the risk of having a first VTE.
Examples:•Surgery with general anesthesia for less than 30 min.
•Admission to hospital for less than 3 days with an acute illness.
•Estrogen therapy.
•Pregnancy or puerperium.
•Confined to bed out of hospital for at least 3 days with an acuteillness.
•Leg injury associated with reduced mobility for at least 3 days
VTE PROVOKED BY A PERSISTENT RISK FACTOR
Active cancer
Cancer is considered active if any of the following apply:(1)has not received potentially curative treatment; or
(2)there is evidence that treatment has not been curative (e.g. recurrent or progressive disease)‡;or
(3)treatment is ongoing.
On-going non-malignant condition associated with at least a 2-fold riskof recurrent VTE after stopping anticoagulant therapy
Example:Inflammatory bowel disease.
Cochrane Systematic Review - Intervention Version published: 14 September 2016
Compression stockings for preventing deep vein thrombosis in airline passengers
Eleven randomised trials (n = 2906) were included in this review
Sixteen of 1804 people developed superficial vein thrombosis
There were no symptomless DVTs
No deaths, pulmonary emboli or symptomatic DVTs were reported.
Copyrights apply
• D-dimer abnormal • Measured ~1 month after stopping anticoagulation
• Age ≤50 years
• Male patient
• Hormone use at VTE onset (if female)
DASH score
HERDOO2
● Women ≥18 years old with unprovoked VTE. ● Patients diagnosed 5–7 months before enrollment. ● On heparin or low molecular weight heparin (LMWH) for ≥5 days and oral
anticoagulation for 5–7 months after the event. ● Without recurrent VTE during the treatment period. ● Noncompressible segment on compression ultrasound of popliteal (or more
proximal) leg vein, high-probability V/Q scan, or segmental (or larger) artery filling defect on spiral CT.
● Exclusion criteria: ● Leg fracture. ● Lower-extremity plaster cast. ● Immobilization for >3 days.
Gl thti <3 th bf id t