Embed Size (px)
Citation preview

What’sYourDiagnosis???
RenéeFahrenholz,Classof2012
Signalment‐“Emma”,a9yearold,Female,Spayed,DomesticShortHairedFeline
PresentingComplaint‐Weightloss,vomitedthemorningofhervisit,pendulousabdomen,andpalemucusmembranes
History‐Emmawasvomitingoccasionallyathome.HerownernoticedthatEmmawasn’therusualselfforthepastcoupleofdays;shelayaroundallnightinsteadofroamingthehouselikenormal.Accordingtoherowner,Emmahadnoturinatedordefecatedduringthistime.ItwasalsonotedthatEmmawaslosingweightoverthelast3months.
PhysicalExam‐UponpresentationtoKSUhervitalswereasfollows;Temperature=102.4F,HeartRate=160b/min,RespiratoryRate=28b/min,BCS=2/5,Weight=3.48kgs,MucusMembranes=pale.Emma’sabdomenwassoftandpendulous.Alarge,palpablemasswasfeltinherrightabdomen.Peripherallymphnodeswerenormalinsizeandshape.Dehydrationwasnoted.Emma’sheartauscultatednormally.
DDx‐Renomegaly:Hydronephrosis,RenalInfection/Abcessation,Neoplasiasuchaslymphoma.
DiagnosticsandTreatmentsbyVisit:
3/07/12:CompleteBloodCount,Chemistry,Urinalysis,AbdominalRadiographs,AbdominalUltrasound,FeLV/FIVTest

AcompletebloodcountwasperformedandresultsindicatedahighWBCcount.Therewasanacuteinflammatoryleukogram.ThechemistryresultsshowedelevatedlevelsofBUNandCreatinine.TheUSGwas1.037andtheurinalysisresultswerepositiveforprotein.Therewereoccasionalstruvitecrystals.TheFeLV/FIVtestwasnegative.
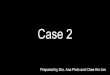
Radiographs‐AVDand2RightLateralAbdominalViewsweretaken.
Figure 1‐ VD Abdomen

Theleftkidneyisnormalinsizeandshape.Thereisamassintherightcraniodorsalabdomen.Thereiscaudalandleftdisplacementofthesmallintestine.Differentialsforrightmass:renomegaly,hydronephrosis,perirenalcyst,neoplasia,granuloma,orabscess.Onthelateralview,therearetwosmall,welldefinedmineralopacitieslocatedcaudaltotherightkidney.Oneopacityissuperimposedwith
Figure 3‐ Right Lateral Abdomen compression with wooden spatula
Figure 2‐ Right Lateral Abdomen

theregionoftherightkidneyontheventrodorsalview.Botharesuperimposedwiththeleftrenalsilhouette.Oneopacitymoveswithcompression.
Suspectrightureterolithandleftnephrolith.
Atthecompletionofthisvisit,EmmawasprescribedClavamoxforpossibleinfectionandsenthomewithsubcutaneousfluids
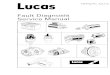
Ultrasound‐Anabdominalultrasoundwasperformedon3/7/12.
Figure 4‐ Left Kidney with hyperechoic foci
Figure 5‐ Right Kidney with irregular margins and bordered by fluid

3/7/12:Therightkidneyismarkedlyenlargedandhasirregularmargins.Theinternalarchitectureoftherightkidneyisdistorted.Therenalpelvisandcollectingsystemaredilatedwithechogenicmaterial.Thereareseveralvariablysizedhyperechoicfocipresentintherightkidney.Theproximalureterisdilatedandtorturous.Theleftkidneywasofnormalsizeandcontainedmultiplesmallhyperechoicfoci.
3/08/12:UltrasoundGuidedFineNeedleAspirates,CytologyandAerobicCultureofaspirates
Cytologyrevealedneutrophilicinflammationanddegenerateneutrophils.AerobicCulturedidnothavegrowthpresent.Theculturewasnegative.
3/13/12:ProfileRenalChemistryBloodwork,AbdominalUltrasound
RenalProfile:AzotemiaandincreasedPhosphorus
ContinueClavamoxandSubcutaneousFluids
RecommendHill’sK/DDietandconsultswithInternalMedicineandSurgeryServices
Ultrasound‐3/13/12
OwnerreportedthatEmmawasdoingbetterathome.

Thedilationoftherenalcollectingsystemismoresevere.Thereisincreasedhypoechoicmaterialsurroundingthekidney,whichappearstobebetterencapsulated.
Dx‐Rightkidneyhydronephrosis,rightureterolith,softtissuestructuresandeffusionnotedinretroperitonealspacemayrepresenturinoma,abscessorretroperitonitis.Leftnephrocalcinosis/nephrolith.
TxRecommendations‐AssessmentofEmma’sglomerularfiltrationrateandsurgicalremovaloftherightkidney.
Figure 7‐ Right Kidney with increased perirenal fluid
Figure 8‐ Right Kidney with increased perirenal fluid

Tx‐Ownerelectedconservativemanagement.Antibiotics:Clavamoxgivenevery12hoursuntilgonefortreatmentofinfection.PainMedication:Buprenorphinegiventransmucosallyevery6‐8hoursforpain.SubcutaneousFluids:150mlLRStobegivenathomeeachday.DiscussionHydronephrosisisaseriousconditionthatresultsindistensionoftherenalpelvisandrenalcalicieswithurineduetoanobstruction.Hydronephrosiscanleadtoatrophyoftherenalparanchyma,causingdistortionoftherenalarchitecture.Iftheobstructionisinthelowerurinarytract,hydrouretercanbeseen.Astheprocessofhydronephrosiscontinues,thekidneywilltransformintoanon‐functionalsacfilledwithfluid.Theobstructionofurineoutflowcanbecongenitalduetomalformedureterorkidney,oracquiredduetoneoplasia,ureterstricture,orureteroliths.Emma’shydronephrosisismostlikelyduetoaureteralcalculus.Thesofttissuestructuresandeffusionnotedinretroperitonealspacemayrepresentaurinoma,abscessorretroperitonitis.Furtherdiagnosticsarerequiredinordertodeterminetheirorigin.
RenalAbscesses
Renalabscessesusuallyoccurduetoascendingurinaryinfection.Insomecases,tissuebreakdownandnecrosiswilloccur,leadingtomicroabscessformation.Thesecanliquefyandcoalesceintolargeabscesses.Extra‐renalabscessusuallyresultsfromruptureofarenalabscessorinfectedhydronephrosisthroughtherenalcapsule.

Renalabscessesaremostcommonlyasequelaofsevere,acutepyelonephritis.Theyfailtorespondtoappropriateantibiotictherapy.Patientsmayalsohaveanonsetofsymptomswithabsenceoflocalizingsignssuchasflankpain,pyuriaorbacteriuria.Renalabscessescanbeidentifiedwithultrasound.Theabscesscanappearsimilartoacystwhenviewedwithultrasound,butcanalsomimicarenalneoplasm.Sometimestheabscessmaybeindistinguishablefromadjacentrenalparenchyma.Abscessescancontainavariablemixtureofanechoic,hypoechoic,andhyperechoiccomponents.
Urinomas
Aurinomaisanencapsulatedextravasationofurinethatformsthroughatearinthecollectingsystemortheproximalureterwhenureteralobstructionispresent.Causesforurinomasincludeiatrogenicorsurgicaltrauma,uretericobstruction,ureteraltumor,stones,andperiuretericfibrosis.Acuteorsubacuteoutflowobstructioncancauseurinetoleakintotheperirenalspace.Urinomashavearadiologicalappearanceofasofttissuemass.Largelesionscandisplacethekidney.Radiologicalandultrasonographicfindingsofchronicobstructionareoftenpresent.