Embed Size (px)
Citation preview

What’s New with MAC, RAC, Medicaid and the OIG?
Audit findings, Updates, and Operational Ideas
Instructor: Day Egusquiza, Pres
AR Systems, Inc
RAC 2012 1
AR Systems, Inc Training Library Presents

To ensure billed services are reflected in the documentation in the record
To ensure billed services are in the medically correct setting for the pt’s condition
To ensure billed service reflect the ‘rules’ regarding billing for the specific service
To ensure documentation can support all billed services according to the payer rules.
Goal of the Audit Culture
2RAC 2012

Common issues:◦Dept staff not understanding the charge
capture must match physician order and documentation.
◦Lack of ongoing coder education◦Lack of ongoing dept head ed◦Lack of physician understanding◦Creating a culture of audit – time to be
pro-active
RAC 2012 3
Outline of Audit Findings

Commitment to Reduce the Error President Obama recently announced the
government’s commitment to reduce the error rate by 50% (using a baseline of 12.4%) by 2012 (2008 3.6% $10.3 Billion )
– 9.5% for November 2010 Report – 8.5% for November 2011 Report – 6.2% for November 2012 Report Thru MAC, CERT, ZPIC, RAC, MIC, OIG, HEAT
auditing… Funding PPACA by eliminating fraud, waste and
abuse…
National Error RateSummer 2010 - 12.4%; 2011-10.5%-8.5%
4RAC 2012

Entity Type of claims
How selected
Volume of claims
Purpose of review
QIO Inpt hospital All claims where hospital submits an adj claim for a higher DRG.Expedited coverage review requested by bene
Very small To prevent improper payment thru upcoding.To resolve disputes between bene and hospital
CERT All Randomly Small To measure improper payments
MAC All Targeted Depends on # of claims with improper payments
To prevent future improper payments
RAC All Targeted Depends on the # of claims with improper payments
To detect and correct past improper payments
PSCZPIC All Targeted Depends on the # of potential fraud claims
To identify potential fraud
OIG All Targeted Depends on the # of potential fraud claims
To identify FraudRAC 2012 5
CMS Claim’s Review EntitiesRoles of Various Medicare Improper Payment ReviewsTimothy Hill, CFO , Dir of Office on Financial Mgt9-9-08 presentation

Updates Impacting the Auditing of Claims
6RAC 2012

Jan 2012 RAC updates –Building on 2011 – 3 goals
(www/cms/gov/apps/media/
Demonstration Pre-PaymentReview –focused 7 states with high fraud
and error prone providers: FL, CA, TX, MI, NY, LA, Ill
4 states with high volume of short stay hospital stays: PA, OH, NC. MO
Does not replace Pre for MACs
Should allow for more timely rebills of corrected claims while catching potential patterns early.REACTIVATED: Go live June 2012
Prior authorization of certain medical equipment.
(www/cms/gov/apps/media/Press/factsheet.asp?counter
Part A to Part B Rebilling 380 hospitals /pilot can
sign up to volunteer All hospitals to resubmit
claims for 90% of the allowable Part B payment when RAC, CERT, MAC finds that a Medicare pt met Part B, not Part A.
NO APPEAL RIGHTS if join this demonstration project.
Can opt out at any time.RAC 2012 7

Limitations on prepayment won’t exceed current post payment ADR limits.
Medical records provided on appeal will be remanded to the RAC for review
Claims will be off limits from future post payment reviews
ADR letter will advise where to send: RAC or MAC.
30 days to reply
June 1 – 312/Syncope Aug 1 – 069/Transcient
Ischemia; 377/GI hemorrhage w/MCC
Sept 1 – 378/GI Hemorrhage w CC; 379/GI Hemorrhage w/o CC/MCC
Oct 1 – 637/diabetes w/MCC; 638/diabetes w/CC; 639/diabetes w/o CC/MCC
RAC @cms.hhs.gov//go.cms.gov/cert-demos
Pre-Payment Expanded InfoDec 2011 – Prepayment CMS calls
RAC 2012 8

Highlights◦ Allows /outlines Semi Automated Reviews◦ RAC decisions beyond 60 days = no payment to
the RAC but can request an extension.◦ Discussion period continues but no timelines for
replies from the RAC. Should be in writing and responded to within 30 days of receipt. If appeal is filed, discussion period ends.
◦ Posting of new issues still a problem with HDI and Connolly. But no new guidelines for the RACs
◦ Timely period between results letter and demand letter . (Estimated at 2 weeks)
(CMS’s website, posted 9-1-11)
Updated Statement of Work 9-11
RAC 2012 9

Effective March 15, 2012, calculation for record count has increased.
“The limit is equal to 2% (use to be 1%) of all claims submitted for the previous calendar year divided by 8. EX) billed 156,253 claims, 2% = 3125 /8 = 390 every 45 days”
“RAC can request up to 35 records per 45 days for providers whose calculated limit is 34 or less”
“Maximum # of records per 45 is 400” (was 300) “Providers with over $100,000,000 in MS-DRG payments
who had the 500 requests cap will now have a 600 record cap”
Hospital feedback on 3-16: GA “went up 118%; Al doubled, Texas up by 100 records each 45 days, NC up by 87 records, IN 300-400 between our 3 hospitals.”
New 45 day record countwww.cms.gov/recovery-audit-program/downloads/providers_adrlimit-Update_03-12.pdf
RAC 2012 10

Semi-automated reviews are a two-part review that is now being used in the Recovery Audit Program. The first part is the identification of a billing aberrancy through an automated review using claims data. This aberrancy has a high index of suspicion to be an improper payment. The second part includes a Notification Letter that is sent to the provider explaining the potential billing error that was identified.
Still no limit on requests; in addition to complex record requests.
Updated SOW –Semi
RAC 2012 11

Region Overpaymts($ in millions)
Underpaymt
Total 3rd Q Corrections(Based on actual collections
FY to DateCorrectionsData thru June 30, 2011)
Region ADCS
$40.4 $5.0 $45.4 $98.2
Region BCGI
$33.9 $9.8 $43.7 $118.5
Region CConnolly
$46.9 $7.4 $54.3 $133.3
Region DHDI
$112.2 $33.7 $145.9 $242.5
TOTALS $233.4 $55.9 $289.3 $592.5
CMS Quarterly Newsletter, June 2011
RAC 2012 12

Region A: Renal and Urinary Tract Disorders (Not medically appropriate for inpt status)
Region B: Extensive Operating room procedures unrelated to principal dx (DRG validation – primary and 2nd dx errors)
Region C: Durable Medical Equipment/Prosthetics/DMEPOS (Automated review – no separate payment when inpt.)
Region D: Minor surgery and other treatment billed as an inpt (Not medically appropriate for an inpt status.)
HDI purchased by NY based HMS Holdings $400M. 11-11
Top Issues per Region, CMS, 3Q 2011
RAC 2012 13

Region Overpaymts($ in millions)
Underpaymt
Total 3rd Q Corrections(Based on actual collections
FY to DateCorrectionsData Oct 2010-Sept 30, 2011)
Region A/DCS
$ 43.3 $ 5.8 $ 49.1 $146.3
Region B/CGI
$ 60.4 $ 3.2 $ 63.6 $170.3
Region C/Connolly
$ 65.2 $ 60.7 $125.9 $260.9
Region D/HDI
$108.2 $ 6.9 $115.1 $361.8
Nationwide Totals
$277.1 $ 76.6 $353.7 $939.4
CMS Quarterly Newsletter – *Based on collected amts thru Sept 30, 2011
RAC 2012 14

Region A: Renal & Urinary Tract Disorders (medically necessary/incorrect setting)
Region B: Surgical Cardiovascular Procedures (medically necessary)
Region C: Acute inpt admission neurological disorders (medically necessary)
Region D: Minor surgeries and other treatment billed as an inpt (medically necessary ) *When pts with known dx enter a hospital for a specific minor surgical procedure and is expected to keep them les than 24 hrs, they are considered outpt regardless of the hour they present to the hospital, whether a bed was used or whether they remain after midnight.
Top Issues per Region/9-2011
RAC 2012 15

After many confusing/delayed RAC recovery and demand letters, CMS has made the following change.
“Effective Jan 3, 2012, CMS is transferring the responsibility for issuing demand letters to providers from its Recovery Auditors to its claims processing contractors. This change was made to avoid any delays in demand letter issuance. As a result, when a Recovery Auditor finds that improper payments have been made to you, they will submit claim adjustments to your Medicare contractor. Your Medicare contractor will then establish receivables and issue automated demand letters for any RAC identified overpayment. The Medicare contactor will follow the same process as is used to recover other overpayments. The Medicare contractor will then be responsible for fielding any administrative concerns you may have with timelines, appeals, etc.”
Messy: Letter to MAC/FI’s contact, not the RAC contact. Yell !
Details as to the reason/pt identifier are missing. Not required.
Change with Demand letters-HUGE CR 7436, MM Matters7436
RAC 2012 16

• Focusing on curbing fraud, waste and abuse in the Medicare program.
• Time period for filing Medicare FFS claims in Section 6404 of the PPACA amended the timely filing requirements to reduce the maximum time period for submission of all Medicare FFS claims to one calendar year after the date of service.
• Under the new law, claims for services furnished on or after Jan 1, 2010 must be filed within 1 calendar year after date of service. In addition, mandates that claims for services furnished before Jan 1, 2010 must be filed no later than Dec 31, 2010.
• The following rules apply to claims with dates of service prior to Jan 1, 2010: claims with dates of service before Oct 1, 2009 must follow the pre-PPACA timely filing rules. Claims with dates of service Oct 1-Dec 31, 2009 must be submitted by Dec 31, 2010.
• Impact on denied claims with rebill potential with the RAC and MIC?• MESSAGE: GET IT RIGHT THE FIRST TIME.
RAC 2012 17
Patient Protection and Affordable Care Act, March 23, 2010

Requires report and repayment of overpayments.
“Overpayment’ = funds a person receives or retains to which person is not entitled after reconciliation.
Providers and suppliers must: Report and return overpayments to HHS, the state or contractor by the later of:◦ 60 days after the date the overpayment was identified or◦ The date the corresponding cost report is due.Provide a written explanation of the reason for overpayment
(PPACA 6402)Retaining overpayments after the deadline for reporting is
subject to False Claims Act and Civil Monetary Penalties law.
More Pt Protection and Affordable Act (PPACA)“Most of the healthcare reform can be paid for by finding savings within the existing health care system, a system that is currently full of waste and abuse.” Pres. Obama
18RAC 2012

SE1024 “RAC: High Risk Vulnerabilities- No documentation or insufficient documentation submitted” (July 2010)
Two areas of high risk were identified from the demonstration project:
No reply to request/timely submission (1 additional attempt must be made prior to denial)
Incomplete or insufficient documentation to support billable services
RAC 2012 19
CMS series w/ MedLearnwww.cms.gov/RAC

SE1024/July No documentation or insufficient documentation submitted
SE1027/Sept Medical necessity vulnerabilities for inpt hospitals
SE1028/Sept DRG coding vulnerabilities for inpt hospitals SE1036/Dec Physician RAC vulnerabilities SE1037 /Jan 11 Guidance on Hospital Inpt Admission
(referencing CMS guidelines, does not mandate Interqual/Milliman, RAC judgment allowed)
SE1104/Mar 11 Correct Coding POS/Physicians Special Edition #SE1121/June 11 RAC DRG
Vulnerabilities –coding w/o D/C summary SE1210/Mar 12 RAC with MN of Renal & Urinary Tract Disorders
Additional CMS/MedLearn Training
20RAC 2012

CMS refers hospitals to Medicare Program Integrity Manual and reiterates that CMS requires contractor staff to use a screening tool as part of their medical review process of inpt hospital claims. While there are several commercially available screening tools…such as Milliman, Interqual and other PROPRIETARY systems… CMS does not endorse any particular brand.
CMS repeats that contractors are not required to automatically pay a claim even if screening indicates the admission was appropriate and conversely,
contractors are not automatically to deny claims that do not meet screening tool guidelines
“In all cases, in addition to the screening instruments, the reviewer shall apply his/her own clinical judgment to make a medical review determination based on the documentation in the record.”
The guidance restates that the Medicare Benefit Policy Manual, Chpt 1, instructions that a physician is responsible for deciding whether the pt should be admitted as inpt.
RAC 2012 21
CMS reiterates guidance on inpt admission determinations SE 1037, 2-3-11

Determining correct status Clarifying order of the status
◦ Examples of weak orders: Admit to Dr Joe, Admit to tele, Transfer to the floor, admit to 23:59, admit to medical service, admit to FIT. None clearly define : Admit to inpt status and why –add (intent of the order)
Directing the clinical team as to the intensity of services that need provided when the pt ‘hits the bed’ as well as thru the course of treatment.
42 CFR 482.12 (c) (2) “Patients are admitting to the hospital only on a recommendation of a licensed practitioner permitted by the state to admit pts to the hospital. “
Medicare State Operations Manual “In no case may a non-physician make a final determination that a pt’s stay is not medically necessary or appropriate.” Case Mgt protocol can ‘recommend’ to the providers but only takes effect when the provider has authenticated it.
RAC 2012 22
Only physician’s can ….

Many facilities are using outside physician advisors or are growing their own advisors – many times the UR physician.
Ensure that any 2nd opinion by a non-treating provider is ‘validated’ and used for directing care by the attending/admitting. Otherwise it is just another non-treating opinion. Additionally, look for educational opportunities thru patterns --dx, documentation, doctor.
Double check with the QIO for their opinion during audit.
23
If a non-attending/admitting…
RAC 2012

2-11 CMS announced a revised threshold for hospitals with $100 million in Medicare payments. The cap was raised to 500 per 45 day period, up from the 300 cap. AHA expressed concern over the 87 hospitals that will be impacted by this change. (New #, 3-12, 600)
PIP hospitals will begin to have records requested 2nd Q 2012.. Many PIP hospitals are large hospitals who could easily have their first record request be 500 records.
RAC 2012 24
ADR plus PIP hospitals

All RACs have begun doing (4-11) Using the automated review/data mining to
identify billing abnormalities with a high potential for improper payment.
This is followed by a request for records/complex to audit to determine if an error did occur in charge capture or claim’s submission.
EX) Tx hospital: Cataract removal can occur once per eye for the same date of service. 66984/removal with insertion of lens AND 67010-59 removal with mechanical vitrectomy) created the edit. 59 overrode edits = 2 payments.
Semi –Automated Claims Review
RAC 2012 25

More Semi Automated Examples Connolly, 5-11 Remicade billed
w/chemo drug adm CPT codes
Letter says: “Data analysis showed an aberrant billing pattern inconsistent with a policy. “
Unknown limit, not subject to complex limits
Connolly, 5-11 Letter for at least 100
claims. Infliximab –is a
monoclonal antibody agent. Drugs “may’ be administered using the chemo therapy CPTs.
Reply with records within 45 days, same penalities
RAC 2012 26

As of 2-14-11, modified changes Limits based on physician or non PP’s billing Tax
ID # as well as the first three positions of the ZIP code where that physician/non PP is physically located.
EX: Group ABC has TIN 12345 and two physical locations in ZIP code 4567 and 4568. This group qualifies as a single entry for additional documentation requests/ADR.
Ex: Group XYZ has TIN 12345 and two physical locations in ZIP 4556 and 5566. This group would qualify as two unique entities for ADR
RAC 2012 27
Physician/Non PP Additional Documentation Limits

ADR limits will be based on the # of individual rendering physician/non-PP reported under each TIN/ZIP combination in the previous calendar year. Reserves the right to exceed the cap if indicated.
RAC 2012 28
More on Physician ADR
Group/Office Size Maximum # of requests per /each 45 days
50 or more 50 records
25-49 40 records
6-24 25 records
Less than 5 10 records

Place of Service – outpt hospital vs office (SE1104 Med Learn; 11 vs 22 or 23)
Separate E&M leveling within the surgical/CPT bundle period
New vs Established Level of service conflicts with the hospital – doc /inpt;
hospital/OBS Based on CERT audit results/ West coast, the following was
targeted for audit: (2011)◦ 99214◦ 99223 (Initial day)◦ 99233 (Subsequent hospital visit)◦ Cert audits can trigger requests for records if provider history
shows an abnormal volume/risk for targeted CPT codes Office E&M leveling is not a focus of the RAC audits..yet
RAC 2012 29
Physician Focus Areas

…can be the same material as the RACs. Ex. Az hospital had a ST MUE error. They
received automated demand letters from HDI; however, they also received ‘first notice’ from WPS on the same issue. Per WPS, the site has 30 days from receipt of the WPS letter without interest to repay or be recouped on the 41st day with interest.
No published items; no limits on requests, same appeal rights. Letters SOMETIMES explain..
WPS – Prepayment 310, 313, 192, 690 NHIC – Prepayment auditing of Chest pain,
syncope and collapse, CHF.
MACs are auditing … w/CMS moving from 15 to 11 MACS
30RAC 2012

Noridian/J3 has announced Probe audits for AZ, MT, ND, SD, UT, WY
Probe for 1 day stays, 2 day stays, 3 day stays and high dollar (w/o definition of $)
Noridian was awarded JF MAC on 8-22-11 Includes ID, ND, Alaska, WA, Ore, SD, MT, WY, UT and AZ. Look for more wide spread auditing. Using CERT data for more probes
NGS – Mobile CMS audits/NY & Prepayment (2012) No letters with reasons.
More MAC audits
RAC 2012 31

Highmark (Now Novitas Solutions)◦ Probe for DRG 470/Major Joint Replacement or
reattachment of lower extremity w/MCC. Need to document 6 months of failed conservative therapy!!
◦ Probe for DRG 244 Permanent Cardiac Pacemaker implant w/o CC or MCC.
◦ NEW: 313, 392, 292 (2012)◦ Msg from provider: Have been having 100% prepayment
audit payment for DRG 313/chest pain for almost 2 years now. The site indicates they are being successful around 90% of time at the 3rd level appeal/ALJ but it is taking about 18 months. There does not appear to be a change with the pre-payment review even with the overturn rate. (per PA facility history 9-11)
And more MAC auditing
RAC 2012 32

Trailblazer/TX highlights◦ Developed LCD 41-96SAB for Hydration (96360-
61)◦ Reviewing DRG appeals and determining patient
status was incorrect. Denied entire inpt stay. ◦ Issued 5 DRGs that will be on prepayment review:
243, 246, 247, 460, 470 (Ex: Stents, pacemaker)◦ 2011- Lost MAC bid. Highmark awarded. 1/12 –
Highmark ‘s Medicare Division , MAC J12, was sold to BC/BC of FL (BCBSF) with their subsidiary, First Coast who is a MAC J9.
And more MAC
RAC 2012 33

Trailblazer: to increase consistency in Medicare reimbursement, effective 11-11, Trailblazer will begin cross-claim review of these services. The related Part B service (E&M, procedures) reported to Medicare will be evaluated for reimbursement on a post payment basis. Overpayments will be requested for services related to the inpt stay that are found to be in error.
First Coast & HighMark/Novitas– similar
MACs are beefing up prepayment auditing –with physician impact
RAC 2012 34

Palmetto, Pre Payment Auditing Began early 2012 DRGs focus:
◦ 871 Septicemia/Sepsis◦ 641 Misc disorders of nutrition◦ 690 Kidney / UTI◦ 470 Joint replacement
Site: CA site. Prior to Feb, 2012 – never had a pre-payment audit request. Had 12 in 1st request.
More MAC auditing
RAC 2012 35

Cahaba – Pre-Auditing of the below DRGs. (2-12) 069 (Transient Ischemia) 191 (Chronic Obstructive Pulmonary Disease w CC) 195 (Simple Pneumonia & Pleurisy w/o CC/MCC) 247 (Percutaneous Cardiovascular Procedure w Drug-Eluting Stent w/o
MCC) 287 (Circulatory Disorders Except AMI, w Cardiac Cath w/o MCC) 313 (Chest Pain) 392 (Esophagitis, Gastroenteritis & Misc Digestive Disorders /o MCC) 552 (Medical Back Problems w/o MCC) 641 (Nutritional & Misc Metabolic Disorders w/o MCC) 945 (Rehabilitation w CC/MCC) 470 (Joint replacement)
And more MAC – AL hospital
RAC 2012 36

DRG Description 2009 Error Rate
2010 Error Rate
313 Chest pain 55.16% 76.71%
552 Medical back pain w/o MCC
70.92% 71.25%
392 Gastro & misc disorders w/o MCC
49.08% 41.93%
641 Nutrition misc metabolic disorder w/o MCC
49.27% 48.43%
227 Cardiac defib w/o cath lab w/o MCC
20.65% 45.43%
The Florida ExperienceMAC /FSCO Focused Probe, 2009 & 2010Preliminary results , FHA, RAC summit 9-10Common w/all: No Physician order for inpt Update: 2011/moved to pre-payment for 313, 5523-12: 6 new prepayment DRGs -153, 328,357,455,473,517
37RAC 2012

“Louisville, KY based Norton Healthcare agreed to pay the federal govt $782,842 in March to settle allegations that it overbilled Medicare for wound care, infusion and cancer radiation services by adding a separate E&M charge that should have been included in the basic rate. The alleged overbilling, which occurred between Jan 2005-Feb 2010 involved outpt care. The settlement is twice the amt Norton allegedly overbilled.”
ISSUE: Transmittal A-00-40, A-01-80 indicate that there is inherent nursing in all CPT codes. Therefore, the facility must ‘earn an E&M when done with a procedure.’ Unlikely events, other medical conditions being treated, new pt=examples.
False Claims and Kickback Lawsuits Involving Hospitals and Health Systems” –Becker’s Hospital Review, 7-11
RAC 2012 38

OIG’s 2011-12 Work Plan – Risk Areas for Hospitals Outpt claims pd greater than
charges. (APC methodology) Inpt claims pd greater than
chgs Inpt $ greater $150.000 Outpt $ greater $25,000 One day stays at acute
care Major complications /comorb Payments for septicemia
servs Payments for inpt same
day discharges and readmissions
Outpt claims billed during the DRG payment window
Payments for hemophilia Payments for outpt surgeries
w/units greater than 1 Inpt and outpt claims
/manufacturer credits for replacement of devices
Post –acute transfers to SNF/HHA/another acute care inpt facility
SNF/HHA consolidated billing-separate outpt services
Outpt claims with 59 modifier Inpt claims pd greater than
chgs
39

2-1-11 CMS Bulletin RAC for Medicaid postponed
9-14-11 CMS issued new RAC for Medicaid final rules
Patterned after Medicare RAC – 3 yr look back, prohibits auditing done by another group, set limits on medical record requests, notify of overpayment in 60 days and coordinate.
www.ofr.gov/ORFUpload/OFRdata/2011-23695 PI.pdf
2-16-11 CMS proposes Medicaid payment reductions for provider-preventable conditions
Follow Medicare’s hospital acquired conditions
Allow for additional conditions for reduction, state specific
RAC 2012 40
Quick Updates - Medicaid

1) Medicaid integrity contractors – CMS has established a 5 year look back period with 30 days to reply to requests for record (10-1-10)
2) RAC for Medicaid – Final rule out Sept 14, 2011. To have in place by Jan 1, 2012. Target: $2.1B, with $900M to the states
3) State Medicaid – state fraud units are auditing and coordinating all data for audits.
Concern – avoid duplication! 3 unique groups. Track and watch each one separately.
NOTE: Medicare RACs are also becoming Medicaid RACs. (HDI-Ks)
Medicaid is auditing
41RAC 2012

OB – protocols Physicians/extended must order/direct pt
care, pt specific. Protocols are excellent clinical pathways,
but the physician must order the protocol. EX) Pt is 26 weeks. Nursing implements
protocol for under 27 weeks. Doesn’t call the provider until results from first items on the protocol. Not billable. Must contact the provider to initiate protocol , then follow protocol. Billable.
Medicaid Hot Exposure Area
RAC 2012 42

CERT audits have continued to identify weakness in the use of Protocols.
EX) Lab urine test ordered but culture done as 2nd test due to protocol. (Noridian/Nov 2009)
EX) Without contrast but 2nd one done with contrast based on protocols.
Ensure the order is either updated or the initial order clearly states ‘with protocol as necessary.”
YEAH – how about including the protocols that are referenced in the record when submitting for audit?
Protocols- Challenges with Fixes
43RAC 2012

N432 = means 2 different things on the RAs.◦ Pending recoupment, should coincide with the Demand
letter◦ Actual recoupment, 41 days after the demand letter
which should include interest from the 31-41st days◦ Remark codes from transmittal 659 clarify
N469 = CERT and MAC denials (Per MAC/NGS training on 3-11) Also used when postponing recoupment/Transmittal 141.
MAC accepted the payment (within 30 days) and did the recoupment on the 41st day too! (GA)
Transmittal 659/CR 68709 PLB reason code (FB ) forward balance. Demand letter is also sent at this time. PLB reason code (WO) overpayment recovery.
http://cms.gov/transmittals/downloads/R6590TN.pdf
Remittance/Payment Anguish
44RAC 2012

Transmittal 47, Interpretive Guidelines for Hospitals June 5, 2009 www.cms.hhs.gov/transmittals/downloads/R47SOMA.pdf
“All entries in the medical record must be complete. Defined by: sufficient info to identify the pt; support the dx/condition; justify the care, treatment, and services; document the course and results of care, treatment and services and promote continuity of care among providers.
“All entries must be dated, timed and authenticated, in written or electronic format, by the person responsible for providing or evaluating the service provided.”
“All entries must be legible. Orders, progress notes, nursing notes, or other entries ….. (Also CMS covers in SE1024 MedLearn release)
45
Powerful transmittal
RAC 2012

Provide a legible full signature (a readable first name and last name)
Provide a legible first initial and last name
Write an illegible signature over a typed or printed name.
Write an illegible signature on letterhead with information indicating the identity of the signer. (EX: a prescription has an illegible signature but the letterhead of the prescription lists three physician names.
Circle the name of the physician who wrote the prescription.
Use an illegible signature accompanied by a signature log or attestation statement.
Write initials over a typed or printed name.
Write initials not over a typed or printed name, but accompanied by a signature log or attestation statement.
Neglect to sign a portion of a handwritten note, but other entries on the same page in the same handwriting are signed.
SEND the LOG WITH AUDIT MATERIAL.
RAC 2012 46
More on Signature Transmittal 3278 ways CMS can meet requirements (3/10)

Heart Failure (MS DRG 291, 292, 293)Physician documentation must include the ‘type ‘ of CHF in order to capture this diagnosis as either being a CC or a MCC condition.
Excisional Debridement (MS DRG 463, 464, 465)
Medical record documentation must support the code assignment of 86.22 and must meet the definition of ‘excisional debridement.” …involves the surgical removal or cutting away as opposed to mechanical removal, i.e. brushing, scrubbing and/or washing.
DRG High at Risk
47RAC 2012

Hybrid records present extreme challenges in identifying the skilled care/handoffs of intensity of service between the care areas.
EMRs tend to present the patient’s history in a ‘cookie cutter’ concept without pt specific issues.
Treatment/outcomes/results of ordered services are often omitted from the clinical/nursing record.
EMR Challenges
48RAC 2012

Living with
RAC
49RAC 2012

1850 reporting, 1400 had activity/2000 hospitals
RAC denied $86M, up from $42 in 3rd Q
Of the $86M, 23% were appealed, 77% was not appealed/ 75% (4Q 2011)
Of the 25% that was appealed, 85% were overturned in favor of the providers.
Medically unnecessary 57% of denials, 33% were short stays
Ave automated : $399
Ave complex : $5281 with a growing amt in medically unnecessary
Will expand the tracking of administrative burden
RAC 2012 50
AHA RAC TRAC 4th Q 2010/updated 2 Q 2011 w/4Q 2011

“Implementation of Recovery Auditing at the CMS. FY 2010 Report to Congress as required by 6411 of Affordability Act.
Accuracy rate by the RACs: Low to high: DCS/98.6 –HDI/ 99.2%
$75 M in overpayments. 82% of all activity 16 M in underpayments. 18% of all activity Reasons:
◦ Not coded correctly◦ Not meeting Medicare’s guideline for an inpt◦ Supporting documentation does not match the order.
First report to Congress –FY 2010
RAC 2012 51

CGI has started complex requests for OUTPT services. So far all outpt have been automated -most MUE problems. (Sept 2010)
Basic Radiation Dosimetry Calculation - Outpt- CPT 77300 Comparison will be made in regards to units of Dosimetry
calculations reported in the medical record versus those units of dosimetry calculation reported on the claim, to establish whether a difference inn reported units compared to those documented resulted in an overpayment for CPT 77300.
HDI has issued “minor surgery and other treatment billed as an inpt stay” Claims billed for minor surgery or other treatment are identified for medical review based on risk of inpt improper payment.” (Oct 2010)
Involve surgery scheduling/surgery director and UR to review all cases.
Outpt Complex Reviews
52RAC 2012

June, 2010 Connolly posted new issues relative to drug /J code accuracy. Tying the J code and the units/multiplier on the UB.
Paclitaxel Cetuximab Paclitaxel protein –bound particles Tenectplase Pamidronate disodium Adenosine Zoledronic acid (reclast) 1 mg
Connolly – Drug dosages /multiplier issues
53RAC 2012

54
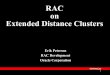
From Cmdr Casey, RN, CMS
Summary: Review & Collection Process
If no findingsSTOP
Complex Review
• Provider has 45 + 10 calendar days to respond
• Providers may request an extension
• Claim is denied if no response
• RAC has 60 calendar days from receipt of medical record to send the Review Results Letter
Automated Review
RAC makes a claim
determination
2
Day 1RAC issues Demand Letter to
Provider (includes $$$ and appeal
rights)INTEREST
BEGINS TO ACCRUE
AFTER 30 DAYS FROM
DETERMINATION
4
Day 41
Carrier/FI/MAC
recoups by offset
5
New Complex Review Issue
Posted to RAC’s
Website
6
RAC issues Medical Record
Request Letter
to provider
7
Provider submits medical records
8 RAC clinician reviews medical records;
makes a claim determination
9RAC issues Review Results
Letter to provider (does NOT include $$$ or appeal rights)
10
Carrier/ FI/MAC issues
Remittance Advice (RA)
to provider
N432: “Adjustment based on a Recovery
Audit”
3
New Automated
Review Issue
Posted to RAC’s
website
1
• Recoupment will NOT occur if:
provider has paid in full; or
provider filed an appeal BY
day 30
The Collection Process
RAC 2012 54

Charged to the provider if demand amt is not paid within 30 days of the letter. 31-41st days of interest, auto recouped on 41st day.
Charged to the provider if an appeal is filed within 30 days (normal is 120) to stop the recoupment.
Paid to the provider if the money was recouped on the 41st day, appeal filed and overturned.
No interest is paid if the money is given back voluntarily, even if over turned on appeal.
Interest is each 30 days, not compounded. 11% Reference: CR7688 /July 12, updates
CR683/Sept 08
How does that interest work?
55RAC 2012

HDI and CGI have started sending their ‘New Issue Validation’ sample letters.
Statement of Work allows sampling of up to 10 claims (in addition the 45 day limit) to prove a vulnerability with a new issue. Results will be issued on the findings with data submitted to the New Issue Board/CMS.
HOT: Share what was requested so potential new items are know; preventive work.
EX) Readmission within 30 days for AMS.
Additional Documentation Request “Sample”
56RAC 2012

Document your waste. Recouped for charging 60 U when only 50 was documented. Used single use vial, but no wastage was documented. (pharmacy? Nursing? Eff 6-10)
Do not use default CPT codes. 99218/initial day OBS has a MUE of 1. However, some hospitals are using for OBS hrs in FL 44. If not required to use G code, leave blank.
Messages from Providers
57RAC 2012

MAC/NGS has an LCD (L25820) with document expectations for drugs and biologicals.
“The medical record must include the following information:◦ The name of the drug or biological administered◦ The routing of the administration◦ The dosage (e.g. mgs, mcgs, cc’s or ICUs)◦ The duration of the administration◦ When a portion of the drug or biological is discarded, the medical record
must clearly document the amt administered and the amount wasted or discarded.”
Policies on how this will be done – as other payers may not acknowledge the billing of wastage.
Reference on documentation of drugs
58RAC 2012

Nov 11, 2010's reply from Scott Wakefield, CMS Project Officer for CGI/ Region B:
"The 60 day timeframe for a RAC to respond to medical records sent by a provider is a contractual requirement for the RAC National Program, therefore, it is possible that non-compliance by the RAC may result in assessment of a lower score in their annual performance appraisal. This cumulative results of this appraisal impacts CMS's determination of whether to extend the incumbent RAC's contract for an additional year. I recommend you contact the RAC directly and inquire about follow up with the remaining records. I have copied certain CGI federal staff on this email and will request that they follow up with me."
No direct penalty, no auto closing/approved of case. UPDATE with new SOW: No payment to the RAC (9-11)
60 day response from RAC
59RAC 2012

19 inpts ADRs in 6 week period All 1 day or very short stay on inpt
surgeries
Messages from ProvidersCritical Access Hospital/HDI
Acute appy- day
CVA/TIA-1 day
Hypokalemia/Acute Renal failure – 2 days
Total shoulder – 1 day
HypotensivePt/readmit
GI bleed-2 days
Below knee amputation-1 day
Breast Reduction-1 day
Carbon monoxide-1
Pneumonia-2 days
Seizures/PNA-expired-1 day
Hemo cath placement-1
Total knee replacements – 2 days
Obstructivehepatisis-transferred
Non-union malleolus (surgery) -1 day
Panyctopenia – 1 day (?comfort care) 60RAC 2012

Medically unlikely edits have resulted in charge capture errors. Many MUEs are unknown to the providers. (Automated)
Examples:◦ 4 ST/92507 treated as per 15 instead of per
encounter. Only 1 is allowed◦ 4 EKG/93005 MUE is 3 in a given 24 hr outpt day.
Would have to appeal that the 4th one was medically necessary to the uniqueness of the pt’s needs.
Message from Providers
61RAC 2012

No auto crossovers/Medigap for pt portion. All pt portions are due to the pt or their supplement.
MAC can override the DRG that the RAC assigned. (Connolly/Cahaba) Which one is appealed?
Site prepares record so a “kindergartener’ can find the pertinent info prior to submission. (AK)
Upon receipt of the ADR, a letter is sent to the impacted physicians informing them of the request. Generates excellent conversation.. (NJ hospital)
More Messages from Providers
62RAC 2012

Underpayments are occurring too. EX) IA hospital billed transfer DRG – pt was to
have had HH or SNF care post inpt. Facility was paid a per diem vs DRG.RAC identified the underpayment as there were no claims from HH or SNF for the post care. Repaid full DRG for 7 accounts, $13,000.
Better practice idea: D/C planning verifies in the 3 day hold that the pt had above services. Revised discharge disposition.
Message from Providers
63RAC 2012

Why us? There does not appear to be any patterns to the requests. They are one of 3 hospitals in the area. Only one to be hit with audits.
Max # of records per 45 days: 48. Have had 143 in last 12 mon High DRG: 69/Transient Ischemia, 312/syncope & collapse,
101/seizures w/o MCC Complex:
◦ Sept, 2010 – 1st medically necessary audits. 48 had both DRG and MN. All 48 had 0-2 day LOS
◦ Appears Connolly is targeting the 2nd diagnosis that make up the CC or MCC◦ RAC Target DRGs: 981/982/983 Extensive & non-extensive OR procedures
unrelated to principle Dx. Also 330/sm & lg bowel procedures237/major cardiovascular w/MCC; 242/permanent cardiac pacemaker implant w/MCC.
4 highest MDCs: Respiratory, circulatory, digestive and Musculoskeletal & connective
Why us? A 300 not-for profit Texas story
64RAC 2012

Automated◦ MUEs – lab/80053 comprehensive metabolic profile & 83880 BNP◦ CPT 62311/lumbar injection. MUE only looks for the correct modifier
w/no considerations for distinct locations.
QUIRKY:◦ MAC assigns the overpayment amt for the demand letter. 1 demand letter
where the demand was more than submitted.◦ On at least 2 claims, the MAC approved a RAC denial and gave the RAC
permission to send out a demand letter. The RAC failed to do so. The MAC assumed we had not responded to a letter so they went ahead and recouped the payment.
Update 10-1144 complex requested each 45 days. 26% of all claims submitted results in denials. Each results letter is evaluated to determine to appeal or not. Overall, 15% denial rate. Considerable focus on education to prevent future denials.
More from Texas
65RAC 2012

If a provider performs a self audit, how should they notify the RAC?
A: If a provider does a self audit and identifies improper payment, the provider should report the improper payments to the appropriate MAC, FI or carrier. The exact information necessary for the self referral can be determined by contacting your Medicare claims processing contractor.
There are two types of self audits: 1) Commonly called a voluntary refund and is claim based. If the required claim information is included along with the amt of the improper payment, the claim will be adjusted. The RAC will be aware of the adjustment, but the refund does not preclude future review. 2) Involves extrapolation. If extrapolation is used, the claim processing contractor will review the case file to determine if it is acceptable. The MAC can accept or deny the extrapolation for the issue identified by the provider. If the claim MAC accepts the extrapolation, these claims will be excluded from the RAC review.
RAC 2012 66
RAC FAQ update #9503

Initial claim submission of Part B on a Part A claim is allowed. No Obs, no surgery, no anesthesia, no recovery. Ancillary only.
Rebilling of a denied inpt claim within the timely rebilling requirements is a Part B on a Part A claim. Bill type 12x. Ancillary only.
HOPE: AHA continues to champion trying to get CMS to allow bill type 131/regular outpt for a rebilled denied claim.
If the inpt is lost or no ability to bill for an inpt – then what
67RAC 2012

These revenue codes/department charges are billable on a Part B claim of a denied Part A service. 12x (Benefit Policy Manual, Chpt 6, section 10; Claims billing manual 100-04, Chpt 4, section 240)
27x/supplies; 30x/lab;32x/imaging; 331 & 335/chemo; 333/Radiation therapy; 34x/nuc med; 35x/CT; 379/anesthesia; 401/dx mammo; 402/ultrasound;403/screening mammo; 404/PET; 42x/PT; 43x/OT; 44x/ST; 46x/pulmonary; 48x/cardio, cath lab, cardiac stress test; 540-45/ambulance; 61x/MRI;634/Epo under 10,000 U; 635/Epo over 10,000 W;636/pharmacy;730-1/EKG & ECG tele;732/tele;739/EKG cardio lab;74x/EEG;77x/Vaccination adm;790/litho;920/other dx services; 921/vascular lab; 922/EMG;923/pap smear;929/invitro fertilization; 985/non-invasive physician. NO Surgery!
RAC 2012 68
Revenue Codes for Part B on a Part A claim

Can I rebill or must I file an appeal? Call with CMS/HDI/WPS J5, a MAC 7-8-10 If RAC has identified a MUE due to a charge
capture error and there was an accurate CPT that should have been used, an appeal & corrected UB must be filed to get the money for the corrected CPT.
If the facility did data mining and found that the same issue had occurred on other claims, a corrected claim should be submitted.
Discuss with the MAC prior to either to ensure it is done correctly.
Message from CMS/HDI/WPS
69RAC 2012

If an inpt/outpt is denied and the facility determines a misunderstanding of a Medicare regulation occurred, to get the correct CPT code/corrected amt, the facility must appeal. Additionally, the RAC team should immediately discuss the need to continue to data mine similar issues.◦ Internal cost as manual rebill.◦ Only ancillary services can be rebilled◦ Pt had refund for inpt deductable; now will owe outpt coinsurance.◦ Perception to public◦ Real C A S H◦ Track and trend any recoupments with rebills separate from recoupments with
100% absorbed losses◦ Timeline for rebills must be followed
RAC 2012 70
To rebill or not to rebill –to appeal or not to appeal

• If the inpt is denied, the pt (and Medigap supplements) will be informed they don’t owe the inpt deductible. Refund to pt and/or supplement or auto recoupment.
• If the facility determines they would like to do a corrected claim submission once a decision is made not to appeal – the pt will receive notice they owe a new outpt deductible/coinsurance.
• If the outpt claim is denied payment, the pt will be informed they don’t owe the outpt portion.
• HINT: Develop scripts for the PFS staff to explain.• NOTE –all activity/recoupments can go back 3 years
beginning with 10-1-07 PD dates rolling forward.
RAC 2012 71
What will the pt impact be?

Dear pt As part of ABC hospital’s commitment to compliance, we
are continuously auditing to ensure accuracy and adherence to the Medicare regulations.
On (date), Medicare and ABC hospital had a dispute
regarding your (type of service). Medicare has determined to take back the payment and therefore, we will be refunding your payment of $ (or indicate if the supplemental insurance will be refunded.)
If you have any questions, please call our Medicare specialist, Susan Jones, at 1 -800-happy hospital. We apologize for any confusion this may have caused.
Thank you for allowing ABC hospital to serve your health care needs.
RAC 2012 72
Sample letter communication

June 26, 2009/CMS Website CMS reversed earlier decision to AUTO
recoupment SNF payment if the hospital is denied/recouped its 3 day qualifying stay.
If the hospital is recouped for any activity, Part B/physician will be evaluated, but not auto recouped.
Will look but not auto recoup in both.
RAC 2012 73
Payment recoupment impact

Medical Necessity “Setting” Has Started… Connolly, HDI, CGI ,
DCS + a little more
Value Added Section
74RAC 2012

New issue: Inpt Admissions without a Physician’s Inpt Admit Order.
Description: Admissions to the inpt setting require a physician’s order in order to qualify and be paid as an inpt stay.
Inpt hospital 10-01-07 open Reference info: CMS pub 100-02, Chpt 1,
section 10 and pub 100-4 Chpt 4, section 10 and 40.2.2
RAC 2012 75
The beginning of the Patient’s Story

Addition documentation letter received read:
“Good Cause for Issue: Chronic Obstructive Pulmonary Disease DRG 88 MS-DRG 190, 191 (Medical Necessity Review and MS-DRG Validation). During the course of the DRG validation, the RAC will also review the record for inpt admission order.
The documentation is being requested because COPD is one of CMS’s top volume DRGs. Therefore, DRG 88, currently MS-DRG 190 and 191 was selected to determine if the principle and secondary diagnoses were assigned inappropriately resulting in overpayments to the hospitals. An analysis of your billing data indicates that a potential aberrant billing practice may exist for these MS-DRGs.”
Ill hospital example/CGI
76RAC 2012

Dec 9, 2010 letter from Region A/DCS outlining rationale for why they were requesting medical records for numerous DRGs. They also gave a great outline of inpt vs obs.
“Inpt care rather than OBS is required only if the pt’s medical condition, safety or health would be significantly and directly threatened if care was provided in a less intensive setting. A patient must demonstrate signs and/or symptoms severe enough to warrant the need for medical care and must receive services of such intensity that they can be furnished safely and effectively only on an inpt basis.”
When auditing for ‘what does severity and intensity look like- look for the above issues to be addressed in the physicain admit note/order and the nursing bedside documentation.
Read the ADR’s – excellent teaching opportunity
77RAC 2012

1st MN request, 90 records, DX listed below for the 6 MN new issues
Had DRG, MN and inpt accuracy listed on all
Ill Hospital Makes It Real/CGI
COPD Cardiac Arrhythmia
Excisional debridement
Heart failure and shock
Renal failure Extensive OR procedure unrelated to principal Dx
Disease/disorder of the respiratory system
Kidney & UTI
Espohagitis/gastronenteritis
Aneurysm repair Coronary bypass w/PTCA
Tracheostomy
Perc Cardiovasc procedures w/stent
GI Disorders Other circulatory system dx
Other vascular dx
Syncope and collapse
Red blood cell disorders
Atheroscleroris with MCC
Nervous system disorders
78RAC 2012

Rural Critical Access hospital. Ave Census 2 HDI “short stay change notification”. “After our
review, it is our determination that the claims listed should have been outpt OBS vs inpt.” 8-18-10
Direct admit from a clinic. HDI findings: “Pt chief complaint was hypoxia. The pt presented to ED
for acute bronchitis, severe COPD – admitted as an inpt. Past medical hx and the pre-existing conditions are stable. The medical records did not document pre-existing medical conditions or extenuating circumstances that make the acute inpt admission medically necessary. The med record document services that could be provided as an outpt service.”
All size hospitals are being impacted
79RAC 2012

“RAC will review documentation to validate the medical necessity of short stay, uncomplicated admissions of MS DRG (XXX). Medicare only pays for inpatient hospital services that are medically necessary for the setting billed and that are coded correctly. Medical documentation will be reviewed to determine that the services were medically necessary and were billed correctly.”“RACs will also review documentation for DRG Validation requiring that diagnostic and procedural information and the discharge status of the beneficiary, as coded and reported by the hospital on its claim, matches both the attending physician description and the information contained in the beneficiary’s medical record. Reviewers will validate for MS-DRG, principal diagnosis, secondary diagnoses and procedures affecting or potential affecting the DRG.” (Aug 2010)
Language with Connolly’s Notice
80RAC 2012

A) When validating all information prior to submission, be sure to specifically address any issues outlined in the letter. This applies to appeal or discussion periods or any communication. Simply stating that our patient was very sick -although accurate - the audit is auditing billed services (as reflected on the UB and 1500 forms) are accurately reflected in the medical record.
B) Do you have a clinical documentation improvement program? EXPAND It beyond typical physician documentation to clarify DRG issues to SEVERITY of illness/docs and INTENSITY of services /nursing. Grow the documentation to support the level of care billed..
C) Track and trend your own vulnerabilities thru the validation prior to submission process. The opportunities are endless for our records to be improved -including revising EMR documentation. Patterns of risk are excellent tools for ongoing education , process changes, form development and overall cohesive pt care. Charting by exception is the worst type of charting to show intensity of care. Tell the pt's story and outline the interventions, results, handoffs, etc that occurred.
Submission of Complex Hints
81RAC 2012

D) ALWAYS print off the EMR (even if you have an release of information vendor, especially if you have a hydrid record ) and closely audit the handoffs between the departments - closely looking for intensity of care, clarity in interventions (what we did about results, tele strips) and how the pt's condition continued to warrant an acute level of care.
E) Major focus on nursing's canned documentation with EMRs.. Number the pages; create a cover letter that CLEARLY shows the doc's order for inpt with WHY he wanted them in an acute care setting with a defined course of treatment plus highlights of test results, intensity of the condition, etc. The lack of this type of validation can easily result in a fragmented record with very difficult severity and intensity of care identified. (HOT SPOT: ER = paper; floor nursing = electronic. How many admits come thru the ER? Huge area of audit and focused documentation improvement.)
More submission hints
82RAC 2012

Which option should I use?
Discussion Period
Rebuttal Redetermination
The discussion period offers the opportunity to provide additional information to the RAC to indicate why recoupment should be initiated. It also offers the RAC opportunity to explain the rationale for the overpayment decision.
A rebuttal should be submitted only on rare occasions of extreme financial hardship. The rebuttal process allows the provider the opportunity to provide a statement and accompanying evidence indicating why the overpayment would cause extreme financial hardship.A rebuttal is not intended to review supporting medical documentation. A rebuttal should not duplicate the redetermination process.
A redetermination is the first level of appeal. A provider may request a redetermination when they are dissatisfied with the overpayment decision. A redetermination must be submitted within 30 days to prevent offset on the 41st day.
RAC 2012 83
Provider Options – RAC overpayment determination(Noridian Medicare Part A contractor, 3-10)

Discussion period
Rebuttal Redetermination
Who do I Contract
RAC Contractor/MAC Contractor/MAC
Timeframe Day 1-40 Day 1-15 Day 1-120; must be submitted within 120 days of demand letter. To prevent offset on day 41; file within 30 days but interest will accrue (Transmittal 141)
Timeframe begins Automated review-upon demand letter:Complex-upon results letter
Date of demand letter
Upon receipt of demand letter
Timeframe ends Day 40 (offset begins on day 41)
Day 15 Day 120RAC 2012 84
More on Provider Options

Audit Results and Better Practice Ideas
To Reduce Risk
85RAC 2012

“HDI has signed a 5 year license with Milliman Care Guidelines. HCI will use the care guidelines content and software to review Medicare claims.
HDI will use the annually updated evidence based care guidelines products.
The Care Guidelines promote healthcare quality by providing clinical guidelines based on the best available clinical evidence.”
CMS does not mandate or endorse any specific guidelines or criteria for utilization review.”
Feb 25, 2009 “Evidence-based care guidelines will be used to combat waste in Medicare program.”
RAC 2012 86
RAC HealthDataInsights licenses Milliman Care guidelines

An inpatient is a person who has been admitted to a hospital for bed occupancy for purposes of receiving inpatient hospital services. Generally, a patient is considered an inpatient if formally admitted as inpatient with the expectation that he or she will remain at least overnight and occupy a bed even though it later develops that the patient can be discharged or transferred to another hospital and not actually use a hospital bed overnight.” “However, the decision to admit a patient is a complex medical judgment which can be made only after the physician has considered a number of factors, including the patient's medical history and current medical needs, the types of facilities available to inpatients and to outpatients, the hospital's by-laws and admissions policies, and the relative appropriateness of treatment in each setting. Factors to be considered when making the decision to admit include such things as:– The severity of the signs and symptoms exhibited by the patient;
– The medical predictability of something adverse happening to the patient…”
RAC 2012 87
Medicare’s Inpt definitionMedicare benefit policy manual chpt 1 10

Trailblazer/MAC Jurisdiction 4, 8-30-10 “Inappropriate Hospital Admission vs Outpt Observation”
Medicare requirements that the inpt admission begins when the admission order is written. Additionally, all physician orders must have a date and a legible signature.
Physician’s decision to treat the pt as an outpt or inpt are reflected in the physician’s orders. The pt’s condition, history and current dx test results, along with the physician’s medical judgment, availability of treatment modalities and hospital admission policies should be considered when making a decision to provide inpt level of care. If a physician determines additional information is making a medical decision for inpt admission, the physician may elect to place in OBS outpt status.
88
Physician and Hospital Shared Risk – Pt Status
RAC 2012

Scenario 1 An inpt claim is submitted for medical review
◦ The claim is without a written and signed physician order for admission◦ The documentation is without an admit note describing the reason for
admission to an inpt level of care/LOC◦ The services rendered could have been rendered in an outpt setting◦ The screening tool indicates the intensity of services and the severity of
illness of the pt’s condition as documented did not support the medical necessity for inpt LOC
◦ Medical review decision: Denied because documentation does not support the medical necessity for an acute level of care
◦ IF THE PATIENT’S CONDITION REQUIRES INPT ADMISSION, the physician needs to document an inpt admission order with a progress note describing the medical decision for the inpt admission and the intended treatment plan to address the patient’s condition.
◦ Internet Only Medicare Manual (IOM) Pub 100-04, Medicare Claims Processing Manual; chapter 1, section 50.3; chapter 3, section 40.2.2.k
89
More from Trailblazers
RAC 2012

Variance rate: 40% Common findings:
◦ UR/physician dialogue may indicate inpt, but the documentation in the admission order (or subsequent physician documentation) is not sufficient to address the severity of the pt’s condition for today’s condition that warrants an inpt acute level of care.
◦ “Meets or doesn’t meet Interqual” does not make an inpt. Medicare’s definition is not well known.
◦ Weakness in EMRs that do not address the ‘uniqueness’ of the pt’s care and intensity of the service that is being performed. (Nursing documentation- no narrative to support electronic-no ability to expand on the uniqueness of the pt’s story.)
RAC 2012 90
1 day stays

Problematic diagnoses and other risk areas:◦ Rule out – anything! If a physician is not clear as to the
reason for admit/undetermined dx or course of treatment, place in OBS, aggressively work up the pt and rule in= inpt; rule out= discharge safely. (Exceptions do exist)
◦ Using a non-treating physician to confirm inpt status does not replace or supplement the attending/treating physician’s documentation.
◦ Conversations to support “admitting to inpt” is rarely actually documented in the record.
◦ H&Ps and D/C summaries are not consistently present.◦ Normal OUTPT Surgeries being ordered as inpt
surgeries…not on the inpt only list. UR needs to work closely with surgery scheduling.
RAC 2012 91
More inpt status challenges

Definite misunderstanding of what OBS is. Viewed as a time frame rather than a pt’s
condition. (Miracle 23 hr cures = discharge or Monday am quarterbacking to ‘fix weekend.”)
Billable hrs vs hrs in a bed Audit three types of OBS:
◦ ER to OBS – saw provider onsite◦ Post procedure to recovery to OBS◦ Direct from a provider or SNF to a bedHighmark/MAC , new inpt/OBS
www.highmarkmedicareservices.com/bulletins/parta/newsrooms/news09302010
RAC 2012 92
Observation is not a mini-inpt

• Variance rate two fold:– To be an inpt 40%– To remain an inpt 60%
• Audit focus:– Medically appropriate to be an inpt– Medically appropriate to remain an inpt for all 3
days.– Severity of illness/1st day; intensity of service/all 3
midnights.– Common weakness: Social admits= TOUGH
RAC 2012 93
3 Day SNF qualifying stay

• When submitting a request for an appeal, you have different options.
• Submit in writing or via fax. When utilizing the fax, there is no need to follow up with a hard copy of the documentation.
• Submit your request only one time, utilizing only one method.
• Duplicate submissions or following up with hardcopy may delay your appeal.
• If you are bringing attention to a specific item you are faxing, please circle or indicate by asterisk, as highlights do not appear when the fax Is received.
Aug 20, 2010
WPS Medicare Redetermination Requests – 1st level of appeal
94RAC 2012

Begin charge capture/charge reconciliation audits. Department head ownership!
Begin ongoing reimbursement education with audits of billed services against documentation.
Focus on identified weaknesses from benchmark audits, RAC automated results and complex reviews – with corrective action plans.
Last thoughts…
95RAC 2012

Joint audits. Physicians and providers audit the inpt, OBS and 3 day SNF qualifying stay to learn together.
Education on Pt Status. Focus on the ER to address the majority of the after hours ‘problem’ admits.
Identify physician champions. Patterns can be identified with education to help prevent repeat problems.
Create pre-printed order forms/documentation forms. Allows for a standard format for all caregivers.
96
Working together to reduce risk and improve the pt’s story
RAC 2012

CMS Project Officers Contacts
• Region A (DCS)– www.dcsrac.com
– 1-866-201-0580
– CMS RAC Contact: [email protected]
• Region B (CGI)– http://racb.cgi.com
– 1-877-316-7222
– CMS RAC Contact: [email protected]
• Region C (Connolly)– www.connollyhealthcare.com/RAC
– 1-866-360-2507
– CMS RAC Contact: Olive Taylor, CMS.hhs.gov
• Region D (HDI)– http://racinfo.healthdatainsights.com
– 1-866-590-5598 Part A
– 1-866-376-2319 Part B
– CMS RAC Contact: Brian. [email protected]
• CMS assigns a project officer to each RAC. Use if abuse of the SOW or other issues are occurring.
97RAC 2012

• New issues will be posted, RAC specific• There is a CMS/project officer assigned to each RAC• New issues are being added/some are being taken off.
• Region A-DCS [email protected] 866 201 0580• Region B-CGI [email protected] 877 316 7222• Region C-Connolly
www.connollyhealthcare.com/RAC; RAC [email protected] 8663602507
• Region D-HDI [email protected] 866590 5598
RAC 2012 98
Contact Info for RACs (9-10)

Day Egusquiza, PresidentAR Systems, IncBox 2521Twin Falls, Id 83303208 423 [email protected]
Thanks for joining us!Free info line available.Plus our training website: www.healthcare-
seminar.comRAC 2012 99
AR Systems’ Contact Info