Embed Size (px)
Citation preview

What’s New In Malaria
Treatment Guidelines
Dr Chua Hock Hin
Infectious Disease Unit
SGH

2013 2015

Malaria Infection
• Epidemiology
• Clinical manifestations
• Diagnosis
• Treatment
• Prevention

Malaria
• Infection caused by protozoan parasites of
the genus Plasmodium.
• Human malaria ( 5 species ) : P falciparum,
vivax, ovale ( 2 species ) and malariae.
• Simian malaria : P knowlesi
• Transmitted by female anopheles mosquitoe.

Epidemiology Of Malaria In Malaysia
• Majority of cases occur in Sarawak and Sabah
• Malaysia is now in the pre-elimination phase of malaria
control. ( NSPEM 2011-2020 )12,705
4,725
0.55
0.16

Epidemiology Of Malaria In Malaysia - 2012
• Human malaria – 61.6 % , Zoonotic – 38.4%
• Human malaria :
– P. vivax ( 50.2 % ) , P. falciparum ( 30.7% ) , P malariae ( 16.7 % )
– Indigenous cases ( 70.4% ), Imported ( 29.6% )
– Indigenous cases : Sabah -70.4%, Sarawak – 15.9%, Peninsular
Malaysia – 10.1%
• Zoonotic malaria : P knowlesi
– Sarawak ( 56.9 % ) , Peninsular M’sia ( 23.3% ), Sabah ( 19.8% )

The Changing Landscape
• In Malaysia :
• Most human malaria cases are “imported”
• Most locally acquired malaria are zoonotic
malaria – mainly P knowlesi.
• Worldwide :
• Emergence of artemisinin resistant malaria
in Greater Mekong subregion (GMS):
– Cambodia, Laos, Myanmar, Thailand &
Vietnam.

Malaria Cases in Sarawak 2012-2013
2012 2013
Locally Acquired P
falciparum14 0
Locally Acquired P vivax 310 97
Locally Acquired P knowlesi 1007 725
Total Locally Acquired 1331 822
Total Imported Malaria 246 183
TOTAL 1577 1005
Data courtesy of Dr Ooi Choo Huck, JKNS

It is a “Notifiable” Disease
• Malaria is a notifiable disease under the
Communicable Diseases Control Act 1988
which mandates notification within 7 days.
• To ensure early investigation & institution
of control measures, all practitioners are to
notify malaria cases within 24 hours to the
nearest health office.


P falciparum , vivax,
ovale – 48 hours
P knowlesi – 24 hours
P malariae – 72 hours

Clinical Features
• Incubation period : 10-14 days ( average )
• Symptoms occur within:
– 6 weeks in >90% for P falciparum infections
– 1 year for P vivax infections
– 9-12 days for P knowlesi infections

Clinical Features
• Early symptoms are non-specific.
• Most common presentation is high fever; “cold
stage” “hot stage” “sweating stage”
• In high transmission area, majority usually are
asymptomatic and infections are acquired
repeatedly throughout life.
• Immunity is often gradually lost when people
move out of the endemic areas for long
durations. ( many years )
Clinical Features Of Malaria
• Fever
• Headache, dizziness
• Arthralgias, myalgias,
back ache
• Abdominal pain
• Nausea, vomiting
• Diarrhoea
• Cough,
breathlessness
• Abnormal bleeding
• Jaundice
• Pallor
• Hepatosplenomegaly
• Petechiae, brusing
• Tachypnoea, hypoxia
• Acute abdomen

Biochemical Features
• Anaemia
• Thrombocytopenia
• Hypoglycemia
• Hyperbilirubinemia
• ↑ ALT/AST (usually mild)
• Renal failure
• Metabolic acidosis

Diagnosis Of Malaria
• Malaria must be excluded in :
– All febrile patients living in, or returning from,
an endemic country, regardless of whether
they have been taking anti-malarial drugs.
– All immigrants from malaria endemic
countries with fever.
• Consideration of the possibility of malaria
is an important step in diagnosis especially
in patient from outside endemic areas.
• Must always ask for travel history.

Diagnosis
• In all settings, clinical suspicion of malaria
should be confirmed with a parasitological
diagnosis.
• However, in settings where parasitological
diagnosis is not possible, the decision to
provide anti-malarial treatment must be
based on the prior probability of the illness
being malaria.
Diagnosis
• Malaria should be suspected in the
presence of
– Thrombocytopenia
– Relative lymphopenia
– Atypical lymphocytes
– Elevated LDH.

BFMP
Blood may be sent in EDTA bottle but slide must
be made within 2 hours to minimize morphological
changes by anticoagulant in the tube.

When to do BFMP ?
• Do immediately.
• No need to wait for a peak of fever.
• If initial film is negative, repeat another 2
samples or more especially at peak of
fever.

BFMP
• Advantages :
– Detect malaria parasites at low densities.
( High Sensitivity )
– Can quantify the parasite load
– Able to distinguish different species and
stages of malaria parasite
• Disadvantages :
– Need training.
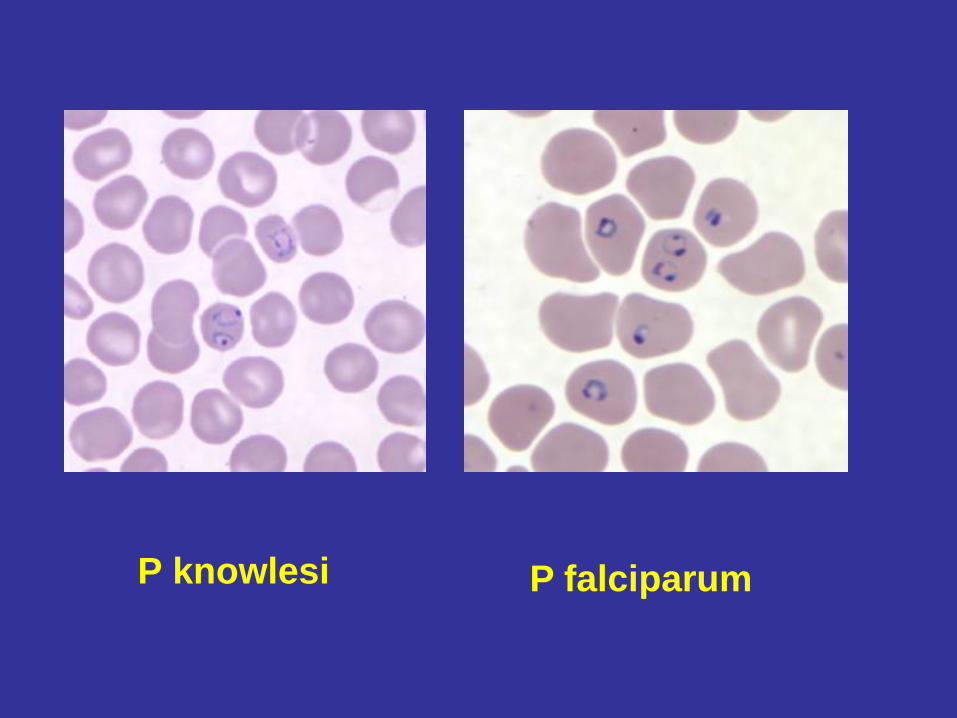
P knowlesi P falciparum

Rapid Diagnostic Tests - RDT
• Detection of circulating parasite antigens or
enzymes that are either genus or species specific.
• It cannot replace microscopy but can be
supplementary when malaria diagnosis is being
performed by relatively inexperienced staff (e.g.,
in low prevalence areas and outside normal
working hours).
• It has high sensitivity (>95%) and should be
highly stable in all situations.

RDT – HRP2
• Histidine-rich protein-2 is a water-soluble protein
produced by trophozoites and young ( but not
mature) gametocytes of P. falciparum. It detects
P. falciparum only.
• It should be used only for diagnosis of acute
malaria infections, and not for follow-up, as they
may remain positive for several weeks even after
successful treatment.

RDT – pLDH , aldolase based
• Plasmodium lactase dehydrogenase (pLDH) and
the pan-specific aldolase are produced by both
asexual and sexual stages (gametocytes) of
malaria parasites.
• The use of pLDH-based RDTs ( high sensitivity )
is recommended.
• No commercially available RDTs have been
sufficiently sensitive overall for P. knowlesi, thus a
negative pLDH or aldolase-based RDT does not
exclude the diagnosis of knowlesi malaria.
PCR
• Cases having microscopic appearance of
P malariae.
• Cases with clinical symptoms of malaria
but BFMP repeatedly negative.
• Mortality cases.

Definition Of Uncomplicated
• Symptomatic malaria without signs of
severity or evidence (clinical or
laboratory) of vital organ dysfunction.
Severe Malaria ( Clinical
Manifestation )
• Prostration
• Impaired consciousness
or unrousable coma
• Respiratory distress
( acidotic breathing )
• Convulsion (>2 in 24hr )
• Failure to feed
• Pulmonary oedema
( CXR )
• Abnormal spontaneous
bleeding
• Haemoglobinuria
• Jaundice + other organ
failure
• Shock / Circulatory
collapse
WHO Guidelines For Treatment
Of Severe Malaria 2010

Severe Malaria ( Laboratory )
• Severe anemia ( Hct < 24% or Hb < 8g/dL )
• Hypoglycaemia ( Blood sugar level < 3 mmol/L )
• Metabolic Acidosis ( HCO3 < 18 mmol/L )
• Renal impairment
• Hyperlactatemia
• Hyperparasetemia ( > 100,000 parasites/µl for
other plasmodium sp; for P knowlesi > 20,000
parasites/µl )


Treatment

Treatment
• Few factors :
–Malaria species
–Severity of illness
–G6PD status
–Special groups – pregnant mothers

Drugs Available• Chloroquine
• Quinine ( Oral & IV )
• Artemisinin derivative ( oral and IV )
• Primaquine


Treatment of Uncomplicated Plasmodium falciparum
Plasmodium falciparum infection should
be presumed to be chloroquine
resistance in most cases

Uncomplicated P falciparum
• Artemisinin-based combination
therapies (ACTs) are the recommended
treatments
– Riamet (artemether/lumefantrine) or
– AS/MQ (artesunate/mefloquine)
• Artemisinin and its derivatives should not
be used as monotherapy

Why Artemisinin?
• Short half life, auto-metabolism
• Rapid resolution of clinical symptoms
• Effective action against multi-drug
resistant P falciparum
• Few adverse effects
– Cough, body aches, nausea, vomiting,
anorexia, palpitation, dizziness, weakness,
skin rash and itchiness

Why Artemisinin?
• Rapid clearance of parasites
– reduce parasite density by a factor of 10,000 in each 48
hr asexual cycle ( 108 fold reduction within 3 days )
• Rapidly eliminated from blood in 1-3 hours, so
need combination with longer acting partner drug
– 3 day course of artemisinin derivative will clear ≥90% of
parasites, remaining 10% of parasites will be cleared
by partner drug
– Lumefantrine ( 4-5 days ) , mefloquine ( 2-3 weeks )
• Reduce gametocyte carriage

Artemether 20mg / Lumefantrine 120mg

First Line Treatment Of Uncomplicated P
falciparum
REGIME :
Artemisinin based combination therapy ( ACT )
Artemether ( 20mg ) and Lumefantrine ( 120mg )
( Wt > 35kg ) :
4 tablets stat followed by 4 tablets 8 hours later,
then 4 tablets twice daily for 2 days
TOTAL : 6 doses ( 24 tablets )

Practice points : Riamet
• For children
• 25 –34kg: 3 tabs ( Total 18 tablets )
• 15 –24kg: 2 tabs ( Total 12 tablets )
• 5 –14kg: 1 tab ( Total 6 tablets )
• If possible, must be given with fat to increase
absorption especially on 2nd and 3rd day of
treatment. ( To give after food or with milk )


Treatment Of Uncomplicated P falciparum
REGIME ( Alternatives ):
Other oral Artemisinin based combination therapy
( ACT )
Artesunate / mefloquine ( ASMQ )
T Quinine 10mg/kg TDS + doxycycline 100mg BD for
7 days


Artesunate-Mefloquine ( AS-MQ )
• Do not use in pregnancy ( 1st trimester )
• May cause seizure in children with
epilepsy
• Interact with quinine, chloroquine and
halofantrine and may cause arhythmia.
• Do not reuse within 60 days as increase
risk of neuropsychiatric side effects.

ASMQ Drug Interactions ↑Arrhymia
• Amiodarone
• Disopyramide
• TCA
• Phenothiazines
• Haloperidol
• Ketoconazole
• Moxifloxacin
• Metoclopramide

Artesunate-Mefloquine ( AS-MQ )
• Strength : Artesunate 100mg and
Mefloquine 220mg
• Dosage ( daily for 3 days ) :
– 5 – 8 kg: 1 tab ( 25mg AS / 55MQ )
– 9 –17kg: 2 tabs (25mg AS / 55MQ )
– 18 –29kg: 1 tab (100mg AS / 220MQ )
– ≥30kg: 2 tabs (100mg AS / 220MQ )

Treatment Of Uncomplicated P falciparum
REGIME :
Doxycyline and Tetracycline ~ AVOID in children
< 8 years old, pregnancy.
REGIME :
T Primaquine 0.25mg/kg single dose for anti-
gametocidal action at Day 1.
Avoid if patient is pregnant or breast feeding an infant < 6
months old or infant < 6 months old. Risk of severe
hemolysis with single dose in patient with G6PD deficient
is negligible.


Treatment Of Uncomplicated P falciparum :
Treatment Failure
REGIME :
Alternative oral Artemisinin based combination
therapy ( ACT )
1st time : Riamet, then use ASMQ
T Quinine 10mg/kg TDS + doxycycline 100mg BD for
7 days


Basically its about
• Safety – risk of teratogenicity in pregnancy
especially in 1st trimester
• Adequate dose vs overdose
• Drug interactions – patient co-infected with
HIV and TB



Treatment Of Uncomplicated P vivax / ovale
• Plasmodium vivax and ovale infection are
chloroquine sensitive except those who
acquired from overseas such as Papua
New Guinea, Oceania countries.

Treatment Of Uncomplicated P vivax / ovale
REGIME ( Chloroquine Sensitive ):
T.Chloroquine 10mg base/kg (max 600mg ) followed by 5mg/kg
( max 300mg ) 6hrs later and 5mg/kg/day for 2 days or 10mg/kg
Day 1 and 2 followed by 5mg/kg Day 3(Total 25mg/kg )
T Primaquine 0.5 mg/kg/day ( usual 30mg base ) for 14 days is
given to eradicate hypnozoite in G6PD normal patient.
T Primaquine 0.75 mg/kg weekly for 8 weeks in mild variant
G6PD deficiency patient.
Treatment Of Uncomplicated P vivax / ovale
REGIME ( Suspected chloroquine resistant /
treatment failure ):
T. Arthemether – Lumefantrine ( Riamet )
AND
T Primaquine 30mg once daily for 14 days

Toxicity of primaquine
• Abdominal discomfort, nausea, vomiting
– Usually resolved if taken with food
– Can given in divided doses
• Haemolytic Anaemia
– Occurs in people with G6PD deficiency
– Begins 24 –72 hours after commencing primaquine
– Severity depends on degree of enzyme deficiency
– Haemolysis less severe or absent using primaquine
45mg or 60mg weekly for 8 weeks

Preventing relapses in pregnant and
breastfeeding women
• Chloroquine 300mg prophylaxis weekly
until delivery or breastfeeding completed
• If failed chloroquine, mefloquine can be
used
• Primaquine ( full course ) to be given post-
delivery

First Line Treatment Of Uncomplicated P
knowlesi
REGIME :
Artemisinin based combination therapy ( ACT )
Artemether ( 20mg ) and Lumefantrine ( 120mg )
( Wt > 35kg ) :
4 tablets stat followed by 4 tablets 8 hours later,
then 4 tablets twice daily for 2 days
TOTAL : 6 doses ( 24 tablets )

Treatment Of Uncomplicated P knowlesi
REGIME ( Alternatives ):
Artesunate / mefloquine ( ASMQ ) for 3 days
T.Chloroquine 10mg base/kg (max 600mg ) followed
by 5mg/kg ( max 300mg ) 6hrs later and 5mg/kg/day
for 2 days

Management of Severe And
Complicated Malaria• It is caused by presence of high density of
asexual forms of plasmodium in patient’s body.
• P falciparum and knowlesi infection, occasionally
P vivax infection.
• It has high mortality ( approaching 100% ) if
untreated particularly cerebral malaria.
• With prompt, effective antimalarial treatment and
supportive care, the rate falls to 10–20% overall.


Therapeutic Objectives
• The main objective is to prevent death.
• Secondary objectives are prevention of disabilities
and prevention of recrudescent infection.
• Management of severe malaria :
– Clinical assessment
– Specific anti-malarial treatment
– Additional treatment
– Supportive care

General Management
• Take a complete history and physical
examination• Prostration
• Impaired consciousness
or unarousable coma
• Respiratory distress
( acidotic breathing )
• Multiple convulsion ( >2
within 24 hours )
• Failure to feed
• Pulmonary oedema
( CXR )
• Abnormal spontaneous
bleeding
• Haemoglobinuria
• Jaundice + other organ
failure
• Shock / Circulatory
collapse

General Management
• Blood investigations :
– Blood C&S
– FBC, BUSE, Creatinine, LFT, Blood sugar,
PT/PTT
– CXR
– ABG
– Serum lactate ( if available )
• CSF investigations ( LP )

Malaria Treatment
• All patients should be admitted.
• Only in exceptional case where admission is not
possible, patient is to be managed as outpatient
with close monitoring.
• Admission is mandatory for :
– Severe/ complicated malaria
– Patient unable to tolerate orally
– Patient with G6PD deficiency
– Pregnant mothers
– Severe malnutrition
– Children

When to refer to hospital with
specialist ?• All severe / complicated malaria cases
• Pregnant mothers.
• Patient with significant co-morbidities eg
hepatic or renal dysfunction.

General Management
• Admit patient to ICU or HDU
• Patient should be referred to physician or
intensivist
• IV artesunate ( 2.4mg/kg ) stat and at least
for 3 doses ( 24 hours ) before switching to
oral antimalarial if patient improves and
can tolerate orally.
• Close monitoring.
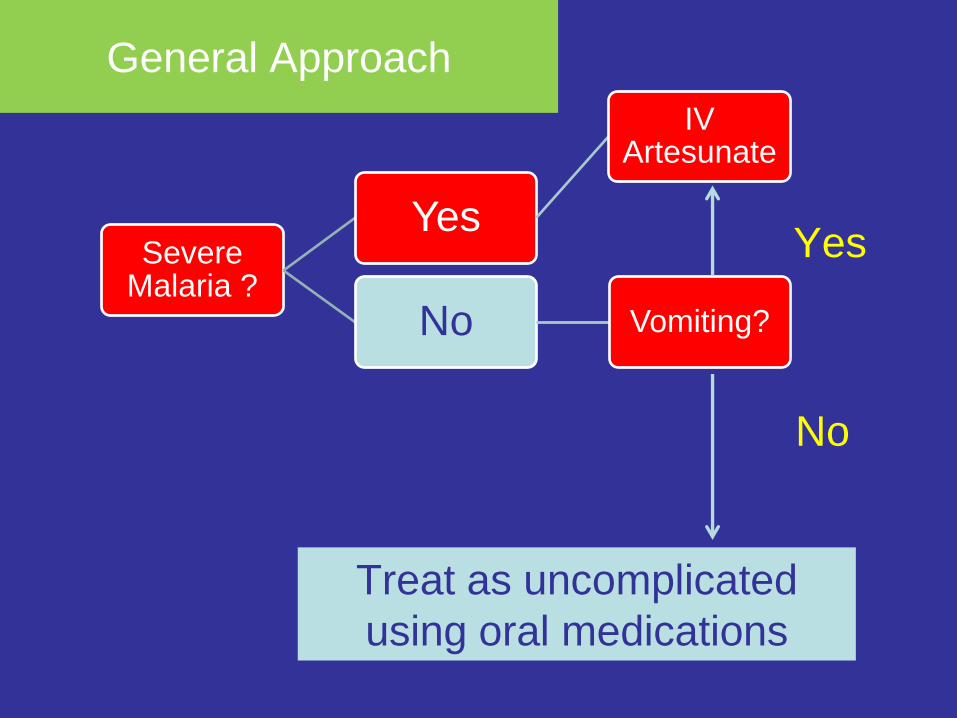
Severe Malaria ?
Yes
IV Artesunate
No Vomiting?
Yes
No
Treat as uncomplicated
using oral medications
General Approach

Treatment Of Severe/ Complicated P
falciparum/ knowlesi
Artesunate ( IV )
Loading dose 2.4mg/kg ( IV/IM ) given stat, 12 hours, 24
hours then once a day.
Change to riamet / AS-MQ when able to tolerate oral
medications or at least after 3 doses of IV artesunate


Treatment Of Severe/ Complicated P
falciparum
QUININE IV
Loading dose usually 20mg/kg but should be used with
“CARE” followed by 10mg/kg 3 times ( 8 hours later )
daily for 7 days. Earlier adjustment of dose by reducing 30
to 50% should be done after loading dose in liver
impairment and renal failure.
Change to oral quinine once stabilize and tolerate orally
Be careful in patient with prolong QTc on ECG, electrolyte
imbalance particularly hypokalemia and hypoglycaemia.
PLUS
T Doxycycline 100mg 12 hourly for 7 days

The danger of “Quinine”
• It should not be given as bolus IV – lethal
hypotension.
• Each dose of parenteral quinine must be
administered as a slow, rate-controlled
infusion (usually diluted in 5% dextrose
and infused over 4 h). The infusion rate
should not exceed 5 mg salt/kg bw per
hour.
• Overdose – blindness and deafness ( rare)

What about if no IV access prior
to hospitalization ? • Children < 6 years old :
• IM artesunate : rectal artesunate : IM
artemether : IM quinine.
• Older children or adults :
• IM artesunate : IM artemether : IM quinine.


Pulmonary Oedema
• High mortality ( over 80% in falciparum malaria);
the prognosis is better in vivax malaria.
• It may develop several days after starting
treatment, at a time when the patient’s general condition is improving and the ↓ parasitemia.
• Management :
• a. Close input output monitoring ( Give adequate
fluids to maintain the circulation and correct
dehydration ).

Pulmonary Oedema
• b. Children : Half normal saline (0.45%) with 5%
dextrose with maintenance fluids (3-4ml/kg/hour),
Adults : normal saline at 1-2ml/kg/hour, until the
patient is able to take and retain oral fluids.
• c. Rapid fluid boluses are contraindicated in
severe malaria resuscitation.
• Dehydration should be managed cautiously and
ideally guided by urine output. ( aim > 1ml/kg/ hr),
unless the patient has anuric renal failure or
pulmonary oedema.

General Management
• If GCS is reduced, consider lumbar puncture ( if
not contra-indicated ) to rule our meningitis.
• If secondary infection is suspected, a septic
workout is to be done and institute broad
spectrum antibiotic such as ceftriazone 2g OD.
• Monitor – clinical and parasitological response.
• High fever – paracetamol and tepid sponging.

Role of adjunct therapy ?
• This is in reference to any additional
therapy that modifies physiologic
processes caused by malaria.

Exchange blood transfusion
• No RCT or consensus on indications, benefit
and risk.
• Requires expertise and intense monitoring.
• Rationale
– Reduce parasite burden ( can be achieved with
artemisinin )
– Rapidly reduced both Ag load and parasite toxins,
host metabolic and toxic mediators
– Alleviate microcirculatory obstruction replace with
more deformable cells


Severe Malaria In Pregnancy
• Women in the second and third trimesters of
pregnancy are more likely to have severe
malaria.
• In low-transmission settings, this is often
complicated by pulmonary oedema and
hypoglycaemia.
• Maternal mortality is approximately 50%, which
is higher than in non-pregnant adults.
• Fetal death and premature labour are common.

Severe Malaria In Pregnancy
• Parenteral artesunate is the treatment of choice
in all trimesters.
• Obstetric advice should be sought at an early
stage, a paediatrician alerted.
• Blood glucose should be checked frequently -
hypoglycaemia should be expected, and it is
often recurrent if the patient is receiving quinine.
• Severe malaria may also present immediately
post delivery.
• Post partum bacterial infection is a common
complications.

Congenital Malaria
• Uncommon ( Incidence : 0.3- 33% )
• Transmission during pregnancy or labour.
• Symptoms occur between 10- 30 days of age
( 14 hour to several months )
• May mimic neonatal sepsis.
• Treatment :
– P vivax ( chloroquine – total 25mg base/ kg )
– P falciparum ( quinine 10mg/kg TDS for 1 week )
• No need primaquine as no tissue / exo-
erythrocytic phase.

Discharge
• In high transmission settings, it is important
to keep the patients warded until they are
cleared of gametocytes which play a crucial
role in the spread of malaria and thus of
public health concern.
• Otherwise, the patients can be discharged
once they are clinically well with two
negative BFMP slides within 48 hours.

Follow-up After Discharge
• Current recommendation :
• Follow-up 28 days for all anti-malarial
medication to assess cure rate and drug
efficacy on weekly basis.

Malaria Prevention
• Mosquitoe avoidance measures
– Insect repellant ( DEET 20-50% )
– Wear long sleeves and pants
– Insecticide treated mosquitoe net
• Chemoprophylaxis
– Countries patient is travelling to
– Trips – length, specific areas
– Drug availability and drug-drug interaction
– Drug allergies.
Chemoprophylaxis
• Patient with severe splenic dysfunction or
pregnant women should avoid traveling to
endemic areas.
• 2 types :
– Suppressive : Chloroquine, mefloquine, doxycycline,
proguanil ( effective against erythrocytic stage ) ,
need to take up to 4 weeks after returning from risk
area.
– Causal : Atovaquone/ proguanil ( Malarone ) and
primaquine. ; take till 7 days after returning from risk
area.