Embed Size (px)
Citation preview

American Osteopathic College of Occupational and Preventive MedicineOMED 2012, San Diego, Tuesday, October 9, 2012
N-1
Physiological Altitude Threats:
Hypoxia, Trapped Gas, Decompression, etc
Lou Gilleran, MD, MPH, MSHSCAPT, MC (FS), USN
Outline
• Physiology of Decompressive Stress
• Respiratory Physiology
• Hypoxia and necessary protection
• Barotrauma
• Aviation DCS
• AGE
What is Pressure?
• From a microscopic pointof view, gas pressure iscaused by the collisionsof gas molecules on asurface. Each individualcollision provides a tinypush on the surface thatit contacts. The sum totalof all of these tiny forcesdetermines the airpressure. The physicalunits for pressure is forceper area.
Atmospheric Pressure
• Since the air (a gas) is afluid, the pressure forceacts in all directions, notjust downward. Thepressure force pushingdownward due to theweight of the air is thesame as the pressureforce acting sideways andeven upward.
14.7lbs.
One square inchcolumn of air fromSea level to space
Scale lbs Barometer Barometer
760mm Hg
29.92inches Hg
Measurement of Pressure Composition Of The Atmosphere
• Nitrogen 78% 597.0 mm Hg
• Oxygen 21% 159.0 mm Hg
• Other gasses & H2O 1% 4.0 mm Hg
760.0 mm Hg
@ Sea Level

American Osteopathic College of Occupational and Preventive MedicineOMED 2012, San Diego, Tuesday, October 9, 2012
N-2
Atmospheric“Shells”
TroposphereSea level -10 km (7 miles above sea level)
Thermosphere80 km to space
Mesosphere50 km - 80 km (56 miles above sea level)
Stratosphere10 km - 50 km (35 miles above sea level)
Human Operational Parameters
• Man is designed for terrestrial existence up to 10K’
– Troposphere defines this physiologic zone
– Troposphere is where weather, clouds, winds have greatestaffect
• Adiabatic (Lapse) Rate defines temperature reductionof 3.5°F/1,000 ft (6.4°C/km) of altitude increase
18,000 ftSea Level
Life at Altitude
Though theatmosphericpercentages ofgases stay the samewith increasedaltitude the “partialpressure” of gasesdecreases at higheraltitudes
O2 and Altitude
• Lack of O2 is a relatively ineffective stimulus andbegins to occur at about pO2 of 60 mm Hg.– Corresponds to about 10,000 ft. on room air and 39,000 ft.
on 100% O2.
• 1st sign is usually increased tidal volume (depth ofrespiration) “air hunger”
• Elevated pCO2 is the primary stimulus for increasedrespiratory rate
Physiological Responses at Altitude
1) At high altitudes there's less O2, therefore less dissolved O2 inthe blood.
2) The response is stimulation of peripheral chemoreceptorswhich send signals to respiratory drives.
3) Hyperventilation leads to Respiratory Alkalosis.
4) Respiratory alkalosis shift the Hb dissociation curve to the leftso that Hb can pick up O2 easier.
5) The kidney responds to alkalosis by generating H ions and thiswill correct the pH back to normal.
Pre-existing Cardiopulmonary Disease
• FAA allows Cabin Altitude up to 8k’ wherePAO2 is ~65 and O2 Sat 90% in healthy.
• Therapeutic O2 required if needed at baselinealtitude.
– Recommended if unable to climb 1 flight of stairsor walk 150’ w/o rest or dyspnia and
• CHF NYHA Class III-IV or baseline PaO2 <70mm Hg
• Angina CCS Class III-IV
• COPD PaO2 <70
• Medications in carry-on!

American Osteopathic College of Occupational and Preventive MedicineOMED 2012, San Diego, Tuesday, October 9, 2012
N-3
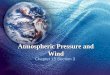
At 10,000 feet,alveolar pO2 is about60 mm Hg. This is onthe steep portion oftheoxygen/hemoglobindesaturation curve.Any additional climbin altitude withoutsupplemental oxygencan result in theinsidious onset ofhypoxia for theaircrewman.
Oxygen-Hemoglobin Dissociation Curve
Physiologic Atmospheric Grouping
Physiologic Deficient Zone10, 000 – 50, 000 ft
_____________________________ 10,000 ft
Physiological ZoneSea Level – 10,000 ft
Healthy individual fit without the aid ofspecial protective equipment
Aircraft Pressurization
Purpose and Types
• To ensure safety and comfort for the crew andpassengers
• Pressurization schedules
Commercial aircraft cabins are required to be pressurized such that the cabin pressure is not
to exceed an altitude of 8,000ft.
System Types
• Conventional
– used currently in all pressurized aircraft
– increase cabin pressure via on-board compressor
• Sealed Cabin
– used in space vehicles
– very high altitudes (80,000 ft)
Pressurization Systems• Isobaric systems maintain a constant cabin altitude
from a preselected altitude (generally from 2000-8000 ft) up to the service ceiling of the aircraft.
• Isobaric-differential systems maintain a constantaltitude until the pressure differential (usually 5psi) isreached and then the differential is maintained up tothe service ceiling of the aircraft.
• Sealed Cabin systems are used only in spacecraft andcarry their own supply of gases to createenvironment.
Aircraft Pressurization
Advantages
• Reduces possibility of:
– Hypoxia
– Decompression sickness
– Trapped gas problems
• Comfort / mobility / fatigue
• Cabin temperature control
• Communication

American Osteopathic College of Occupational and Preventive MedicineOMED 2012, San Diego, Tuesday, October 9, 2012
N-4
Aircraft Pressurization
Disadvantages
• Increased operating cost
• Added weight
• Reduced aircraft performance
• Risk of accidental pressure loss
Aircraft Pressurization
Jet EngineA/CUnit Cabin Outlet Valve
Ambient Air
Bleed AirOverboard
Vent
What Happens When Pressure Fails?• Decompression
– Explosive Decompression (less than 1 sec)
– Rapid Decompression (between 1-10 sec)
– Slow Decompression (greater than 10 sec)The NAVY averages 90 events per year or 2.5 occurrences /
100,000 flight hours
• Factors Affecting Severity– Volume of cabin
– Size of Opening
– Pressure Differential/ Ratio
– Flight Altitude
Physiological Effects of Decompression
• Rapid Decompression– Arterial Gas Embolism (AGE)
– Decompression Sickness(DCS)
– Hypoxia
– Trapped Gas Expansion (TGE)• G.I. Tract• Ears• Sinus• Lungs
• Slow– DCS
– Hypoxia (Insidious)
Arterial Gas Embolism
• Leakage of air from the lungs to thepulmonary circulation.
• Due to pressure – expansion oflungs.
• Pulmonary circulation goes right tothe brain.
• Coronary artery embolization canlead to myocardial infarction ordysrhythmia.
• Cerebral artery emboli can causestroke or seizures
Operational Problems
• Noise: Hissing to Explosion
• Fog: May be mistaken for smoke; decreasedvisual environment
• Flying debris, dust and dirt effect vision
• Temp changes:• Sea Level 70 F
• 25K 20 F
• 35K - 67 F
• 50K - 67 F

American Osteopathic College of Occupational and Preventive MedicineOMED 2012, San Diego, Tuesday, October 9, 2012
N-5
Altitude Threat Protection• Cabin Pressurization System
0 to 8,000ftAircraft ALT = Cabin ALT
35,000ftCabin at 14,500ft
24,500 to 50,000ftCabin ALT = Differential
8,000 to 24,500ftCabin ALT = 8,000ft
(Isobaric)
POSITIVE PRESSURE BREATHING (PPB)
Positive Pressure Breathing (PPB) is the deliveryof a gas to the respiratory tract at a pressure
greater than the ambient.
TYPES of PPB
Intermittent PPB
Pressure applied only during inspiration phase.
Used in SCUBA
Continuous PPB
Pressure applied throughout the breathing cycle
Primary type used in Military aviation
REQUIREMENT for PPB
Based on the level of hypoxia considered operationallyacceptable.
The Navy uses a minimal alveolar pO2 of 60 mm Hg
Reached at 39,000 ft, breathing 100% O2.
PPB is an emergency condition in operational aircraft.
Altitude Threat Protection
• Supplemental Oxygen System-Regulators
Increased PPB
Oxygen (O2)
RESPIRATORY EFFECTS of PPB
1. Distension of lungs and chest
2. Increased Pulmonary Ventilation (+50%)
3. Intrapleural Pressure
4. Breathing Effort
5. Venous Pooling/Distension
6. Reduction of Effective Blood Volume
7. Reduction in Cardiac Output (-30%)

American Osteopathic College of Occupational and Preventive MedicineOMED 2012, San Diego, Tuesday, October 9, 2012
N-6
Applications of PPB
The physiological ceiling is raised from 39,000 ft to45,000 ft.
In a sudden decompression (up to 50,000 ft) PPB canbe used to maintain consciousness in order to effect
an emergency descent.Applications in increased G-tolerance
Disadvantages of PPB
6,000 ft increase is fairly smallPotential physiological problems
Reverses the normal breathing pattern - training required tocompensate
FatiguingCommunications become very difficult
Can induce hyperventilation
Hypoxia
Definition
• State of oxygen deficiency in cells andtissues sufficient to cause impairmentof function.
• Hypoxemia refers specifically to adeficiency of O2 in the blood and willlikely result in hypoxia
Histotoxic(Poisoning)
Stagnant(Pooling)
Hypemic(Blood)O2
O2
O2O2
Hypoxic(Altitude)
Types Of Hypoxia
Hypoxic Hypoxia
Causes:
• Ascent to altitude
• Malfunctioning equipment
• Loss of cabin pressurization
• Improper O2 equipment usage
Diminished O2 available to lungs
Carbon Monoxide
Hemorrhage
Anemia
Sulfa Drugs
Hypemic Hypoxia
Causes:
Reduced O2 carrying capacity of blood

American Osteopathic College of Occupational and Preventive MedicineOMED 2012, San Diego, Tuesday, October 9, 2012
N-7
Carbon Monoxide
Wear and deterioration of airframe seals and opening of seamsincreases susceptibility. This will allow exhaust fumes and toxicgases to infiltrate crew compartment.
Flight personnel effects
– Carboxyhemoglobin (COHb) levels of 15-25% produceheadache and nausea. With prolonged exposure, muscularweakness, dizziness, and confusion occur.
– 25%, electrocardiographic changes, stupor, and eventualunconsciousness will occur.
Stagnant HypoxiaPooling or reduced flow of blood,as seen in heart failure and coldenvironments
Can be caused by inactivity,restriction of movements
Or G-Forces (G-LOC)
Effect of G ForcesEffect of G Forces
Normal Grey/black Out GLOC
Gs
Histotoxic HypoxiaInability of cells to take up or utilize oxygen fromthe bloodstream, despite physiologically normaldelivery of oxygen to such cells and tissues.
• Alcohol
• Medication (Narcotics, etc)
• Cyanide
• CO also Hypemic Hypoxia cause
Factors Influencing Onset Rate
• Cabin altitude
• Rate of ascent
• Duration of exposure
• Individual tolerance
• Physical fitness and activity
• Self imposed and environmental stress
Signs and SymptomsObjective Symptoms
•Increased respiration rate and depth•Cyanosis (may not be evident in anemia)•Pallor•Mental confusion•Poor judgment•Muscle twitching•Cold clammy skin

American Osteopathic College of Occupational and Preventive MedicineOMED 2012, San Diego, Tuesday, October 9, 2012
N-8
Signs and SymptomsSubjective Symptoms
•Air Hunger
•Apprehension
• Fatigue
•Nausea
•Headache
•Dizziness
•Hot and cold flashes
• Euphoria
• Belligerence
• Blurred vision
• Numbness
• Tingling
Stages of Hypoxia
• Indifferent Stage
• Compensatory Stage
• Disturbance Stage
• Critical Stage
Indifferent Stage
• Altitudes:
– Air: 0 - 10,000 feet
– 100% O2: 34,000 - 39,000 feet
• Symptoms: decrease in night vision @ 4000 feet
• acuity
• color perception
Compensatory Stage
• Altitudes:
Air: 10,000 - 15,000 feet
100% O2: 39,000 - 42,000 feet
• Symptoms: impaired efficiency, drowsiness,poor judgment and decreased coordination
Disturbance Stage
• Altitudes:
Air: 15,000 - 20,000 feet
100% O2: 42,000 - 44,800 feet
Critical Stage
• Altitudes
Air: 20,000 feet and above100% O2: 44,800 feet and above
• Signs: loss of consciousness,convulsions and death

American Osteopathic College of Occupational and Preventive MedicineOMED 2012, San Diego, Tuesday, October 9, 2012
N-9
Time of Useful Consciousness (TUC)
Effective Performance Time (EPT)
The period of time from the loss of oxygen supply or
exposure to an oxygen poor environment to the time
when deliberate function is lost
FL 430 & above 9-12 seconds
FL 400 15 - 20 seconds
FL 350 30 - 60 seconds
FL 300 1 - 2 minutes
FL 280 2 1/2 - 3 minutes
FL 250 3 - 5 minutes
FL 220 8 - 10 minutes
FL 180 20 - 30 minutes
Expected Performance Times
put back on oxygen
Time off Oxygen
1 minute
2 minutes
3 minutes
4 minutes
5 minutes
6 minutes
Warning
Effect of Rapid Decompression on TUC/EPT
Time of useful consciousness (TUC) from
hypoxia can be reduced by as much as
30 to 50 percent following a rapid
decompression
Treatment of Hypoxia
• Maximum oxygen under pressure• Connections check – check security• Breathe at a rate and depth slightly less
than normal until symptoms disappear.• Descent below 10,000 feet and land as
soon as conditions permit.

American Osteopathic College of Occupational and Preventive MedicineOMED 2012, San Diego, Tuesday, October 9, 2012
N-10
Oxygen Paradox
• Temporary worsening ofhypoxia symptoms afteradministration of 100%O2
• Caused by physiologicalreaction to a suddenflood of oxygen richblood
• Very rare occurrence
• Remain on 100% O2
Hyperventilation• Definition: An abnormal increase in the rate
and or depth of breathing.
• Causes:• Emotional Stress
• Improper Pressure Breathing
• Altitude hypoxia
• Primary Physiological Results
– Hypocapnia (loss of carbon dioxide [CO2])
– Alkalosis (shift in pH balance)
HYPERVENTILATION - EFFECTS
• Respiratory System
– CO2 + H2O H2CO3 H+ + HCO3-
– Direction of flow is determined by pCO2
– Hyperventilation causes a decrease in pCO2
(hypocapnia), therefore a decrease in H+
– The result is alkalosis
HYPERVENTILATION - EFFECTS
• Central Nervous System– Brain protects itself against chemical imbalance of
blood by restricting blood flow.
– The combined effects of the vasoconstriction anddilation and the Bohr effect cause a stagnanthypoxia to the brain.
– This stagnant hypoxia can result in LOC
– The alkalosis leads to neuromuscular irritabilitywhich can lead to spasms and tetany
HYPERVENTILATION - EFFECTS
• Cardiovascular System
– The hypocapnia/alkalosis causes
• peripheral vasodilation
• cerebral vasoconstriction
– The result is a restriction in blood flow to thebrain
– The Bohr Effect
• Shift of the oxyhemoglobin curve to the left
• restricts oxygen off-loading in the brain
• Dizziness• Numbness• Tightening of muscles• Coolness• Muscle tremors• Tingling• Faintness• Vision impairment• Tetany• Slight nausea
Hyperventilation Symptoms
Onset of symptoms slow and gradual; muscleactivity spastic especially in upper extremities; skinis pale or clammy.

American Osteopathic College of Occupational and Preventive MedicineOMED 2012, San Diego, Tuesday, October 9, 2012
N-11
Treatment of Hyperventilation
• Maximum oxygen under pressure• Connections check – check security• Breathe at a rate and depth slightly less
than normal until symptoms disappear.• Descent below 10,000 feet and land as
soon as conditions permit.
Hyperventilation vs. Hypoxia
Wayne –April,1958 Aviation Med: 307-15
Hypoxia
Dizziness –18.0 %
Visual Disturb –17.6%
Lightheaded – 9.9%
Tingling – 6.0%
Hot or Cold Flash –3%
BOTTOM LINE: Impossible to determine clinically w/o blood gas.
GENERAL RULE: If below 10K’ = Hyperventilation
If above 10K’ = Hypoxia
Hyperventilation
– Dizziness – 27%
– Visual Disturb – 4.2%
– Lightheaded – 26%
– Tingling 15.7%
– Hot or Cold Flash –3%
Trapped Gas Expansion (TGE)Barotrauma
• Causes
• Symptoms
• Prevention
• Treatment
Boyle’s Law
• At constant temperature for a fixed mass, theabsolute pressure and the volume of a gas areinversely proportional
Middle Ear
Cause of block — Blocked or constrictedeustachian tube or upper respiratory infection(URI); usually occurs on descent
Treatment (Ascent)Yawning, Chew & Swallow
Treatment (Descent)Valsalva
Avoid valsalva on ascent andStay ahead of pressure
changes
Post Flight Ear Block
TREATMENT = Frequent Valsalva

American Osteopathic College of Occupational and Preventive MedicineOMED 2012, San Diego, Tuesday, October 9, 2012
N-12
Maxillary
Treatment is to stop ascent or descent then follow protocolPrevention is better option!
Frontal
Ethmoids
Sphenoids
The Sinuses
If your sinuses become blocked by a cold, pressure can’t be equalized withaltitude change and pain will result
Warning:
• Onset rate of SinusSqueeze (Block) mayoccur faster than MiddleEar problems.
• Leaves little time foraircrew decision making
• Sinus pain may beincapacitating if painsevere enough.
Teeth Barodentalgia
• Tooth pain normally occurs on ascent
• Causes: Caries or failing and/or illfittingdental repair/appliance; loose filling;abscess; swollen maxillary sinus(impacted wisdom tooth).
• Treatment
–Descend
–Dental treatment
Gastrointestinal Tract
• Occurs on ascent when trapped gasexpands
• Treatment :
– Start as soon as symptoms appear
– Relieve gas by belching or passingflatus
– Position change / Massage affectedarea
– If problems continue, descend
Vasovagal Syncope:
• Brief loss of consciousness caused by a sudden drop in yourheart rate and blood pressure, which reduces blood flow to yourbrain.
• Vagus nerve is overstimulated by parsympathetic nerves fromabdominal organs and causes the body's blood vessels to dilateand the heart to slow down. This anti-adrenaline effectdecreases the ability of the heart to pump blood upward to thebrain against gravity.
Prevention

American Osteopathic College of Occupational and Preventive MedicineOMED 2012, San Diego, Tuesday, October 9, 2012
N-13
Recommendations
• Watch Diet: Avoid foods that can cause excessgas formation such as cauliflower, broccoli,onions, cabbage and pumpkin.
• Avoid carbonated beverages or drinkingrapidly before flight.
• Avoid chewing gum on ascent.Cola Cola
Intro to Decompression SicknessGases In Solution – Henry’s Law
At a constant temperature, the amount of a given gasdissolved in a given type and volume of liquid is directly
proportional to the partial pressure of that gas in equilibriumwith that liquid.
55.1 in Hg
1.2 mm Hg CO2
34 degrees C
29.92 in Hg
(1 atm = 101.3 kPa = 14.7 psi = 760 mm Hg = 29.92 in Hg)
0.3 mm Hg CO2
34 degrees C
Decompression Sickness
• Decreased pressureforms releases nitrogen.
• Under normalcircumstances, the bodyis able to “off-gas” theexcess nitrogen.
• Rapid ascent or highaltitudes can result inbubbles.
• Bubbles block bloodflow.
• Venous Gas Embolism(VGE) occurs commonlyand is cleared by lung -rarely results in DCS
DCS is uncommon below 18,000 feet
Decompression Sickness (DCS)
• Joint Pain - Bends
• CNS disorders - Staggers
• Lung Involvement - Chokes
• Skin symptoms – Creeps
Decompression Sickness Factors
• Rate of ascent
• Altitude
• Time
• Body Composition
• Age
• Activity
• Dehydration
• Previous injury
Symptoms
• Local Joint Pain 89%
• Leg 30%
• Arm 70%
• Dizziness (The Staggers) 5.3%
• Paralysis 2.3%
• Shortness of Breath 1.6%
• Extreme Fatigue and Pain 1.3%
• Collapse with unconsciousness 0.5%

American Osteopathic College of Occupational and Preventive MedicineOMED 2012, San Diego, Tuesday, October 9, 2012
N-14
DCS Incidence While Breathing 100%Oxygen
Delayed Decompression Sickness
80% of delayed DCS cases occur within 1 hour ofexposure.
Occasionally occur within 24 hours of exposure.
24 HOURRestriction BetweenSCUBA and Flying
Haldane Equation
• Dissolved gas followed byevolved gas.
• Body could tolerate up to a2:1 ratio.
Sea level - 760 mm Hg
18,000 ft - 380 mm Hg
• 760:380 = 2:1
30 FSW – 1520 mm Hg
Sea level – 760 mm Hg
• 1520:760 = 2:1
30 FSW to 8,000 ft ?1520:545 = 2.8 : 1
Protection/Prevention
• Cabin pressurization (primary method)
• Denitrogenation (Preoxygenate 30 min+)
• Exercise during preoxygenationenhances denitrogenation process.
Training
Hypoxia Symptoms are individualized and fairly consistent over time makinghypoxia training a worthy endeavor for aircrew enabling early
recognition and corrective action.

American Osteopathic College of Occupational and Preventive MedicineOMED 2012, San Diego, Tuesday, October 9, 2012
N-15
Last scary thing
•Ebullism: Formation of gas bubbles in bodily fluids due toreduced pressure.
•A system of liquid & gas at equilibrium will result invaporization of liquid to gas. Water pressure is 47mmHg andthe PB at 60k’ is 47mmHg. Voila bubbles and their negativeramifications
•This is known as Armstrong’s line.
•Pressure suits as worn in high altitude surveillance aircraftand extravehicular space travel are required to prevent thispotentially lethal ocurrence