Embed Size (px)
Citation preview

What is catheter ablation – is it safe and who can it help?
Hugh Calkins MD Nicholas J. Fortuin Professor of Cardiology
Professor of Medicine Director of Electrophysiology
Johns Hopkins

Disclosures: None

1998

Initiation of AF from Pulmonary Vein Focus
Haissaguerre et al, NEJM 1998; 339:659-666
1998

Atrial Fibrillation – Focal Ablation Strategy
1998
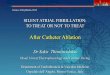
Segmental Lasso Guided Ablation
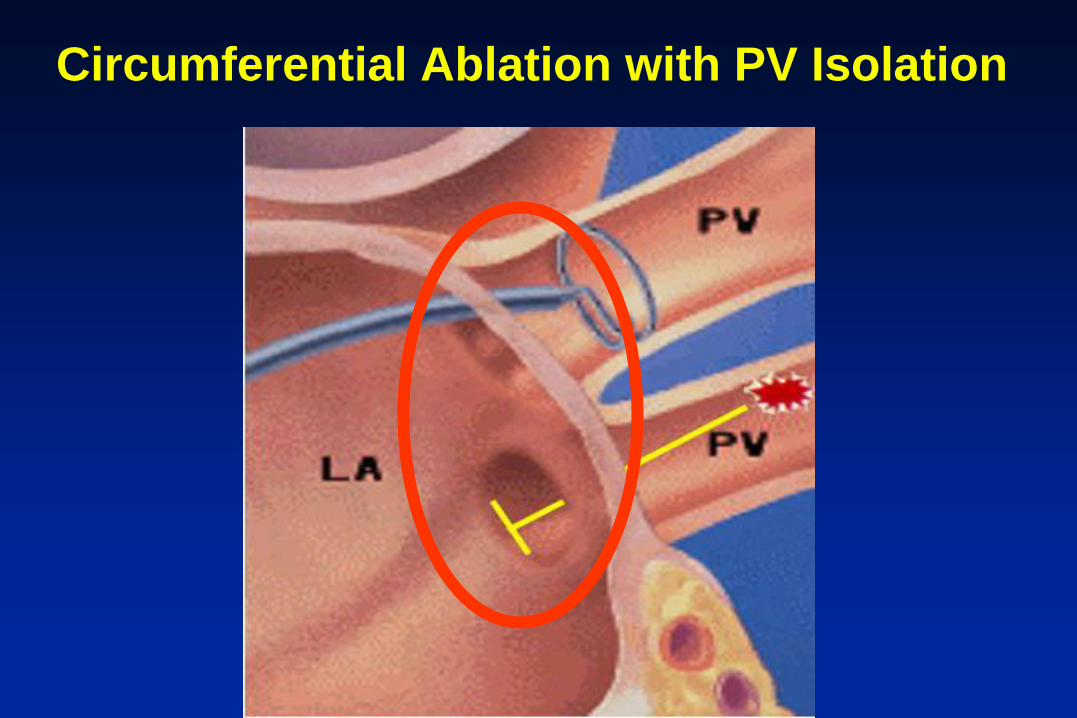
Circumferential Ablation with PV Isolation



Cryo Ablation


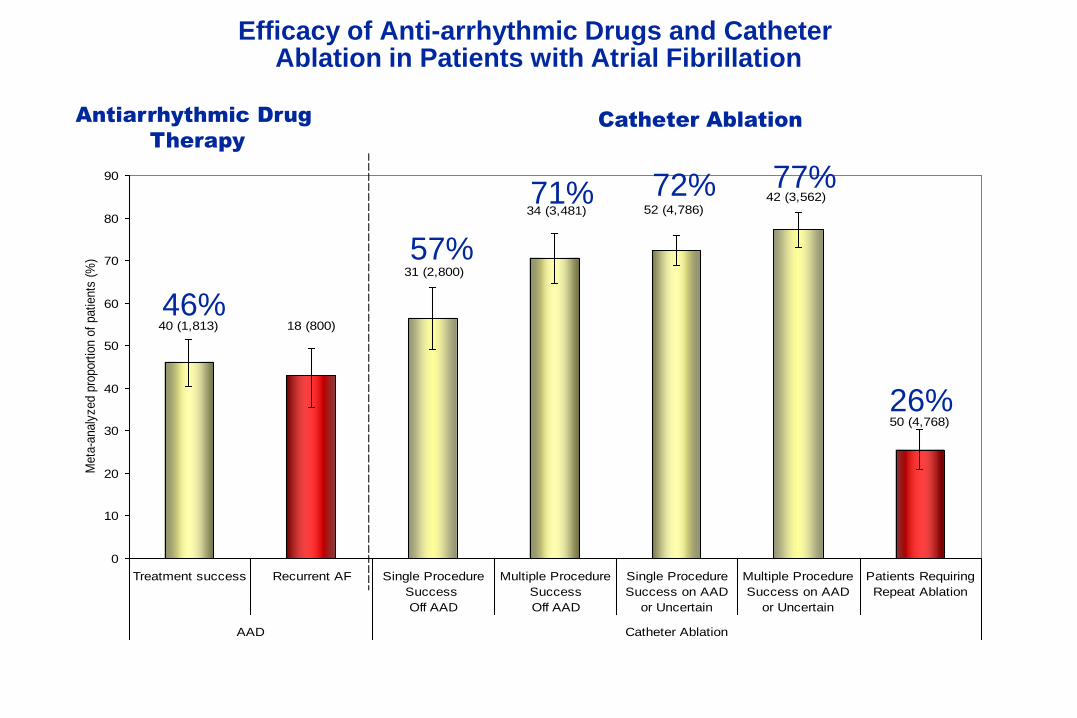
Efficacy of Anti-arrhythmic Drugs and Catheter Ablation in Patients with Atrial Fibrillation
34 (3,481)
40 (1,813) 18 (800)
52 (4,786)42 (3,562)
31 (2,800)
50 (4,768)
0
10
20
30
40
50
60
70
80
90
Treatment success Recurrent AF Single Procedure
Success
Off AAD
Multiple Procedure
Success
Off AAD
Single Procedure
Success on AAD
or Uncertain
Multiple Procedure
Success on AAD
or Uncertain
Patients Requiring
Repeat Ablation
AAD Catheter Ablation
Meta
-analy
zed p
roport
ion o
f patients
(%
)
Catheter Ablation Antiarrhythmic Drug
Therapy
57%
72% 71% 77%
26%
46%

Copyright restrictions may apply.
Noheria, A. et al. Arch Intern Med 2008;168:581-586.
Catheter Ablation of Atrial Fibrillation Meta-Analysis of Four Randomized Clinical Trials

15
Irrigated Diagnostic/Ablation Catheter
• Steerable, multi-electrode, deflectable
• 3.5-mm tip and 3 ring electrodes
• 6 saline ports in the tip for irrigation and cooling (open irrigation)
• A location sensor and a temperature sensor incorporated into the tip

NAVISTAR® THERMOCOOL® Trial
Freedom From Chronic Failure (FDA Protocol 1° endpoint)
• N = 159 patients • 56 + 11 years • 67% male

0 100 200 300 400 500
Days
0%
20%
40%
60%
80%
100%
Tre
atm
en
t S
uccess
Primary Effectiveness Analysis Treatment Success
Blanked for Detectable AF
vs 7.3% (SE 2.9%)
CRYO 69.9% 114 / 163
DRUG 7.3% 6 / 82
30 days
KM estimate 68.6% (SE 3.9%)
OR = 29.5 (12.0 – 72.2) p < 0.001

Outcomes in 2012
Single Procedure Efficacy Multiple Procedure Efficacy Optimal Candidate: 60-80% 70-90% Moderate Candidate 45-65% 55 – 75% Poor candidate 35 – 50% 45 – 60%

0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Year
Co
mp
licat
ion
rat
e
Complication Rates of AF Ablation at Johns Hopkins 2001 - 2010
• No deaths.
• No atrial esophageal fistulas.
• No strokes in past 5 years.

Complications in 2012
Overall Complication Rate: 1% - 4%
Stroke /TIA – 0.5% - 1% Cardiac perforation / tamponade – 0.5% - 2% Vascular injury / bleeding – 0/5% - 1% Phrenic nerve injusy 0.2% - 1% Atrial esophageal fistula - < 1/1000 Gastroparesis – 0.2% - 0.5% Death - < 1/1000

What Can I Expect if I Have the Procedure ?
• Arrive early in the morning. • Meet with team of doctors to give informed consent. • This is your last chance to ask questions. • You may be asked to get a CT scan, an MRI scan, or a transesophageal echocardiogram before the procedure. • You will be sedated duration the procedure. • Some doctors prefer general anesthesia. • Many patients have a urinary catheter inserted – especially if using an irrigated ablation catheter. • Procedure duration 3 – 5 hours.

What Can I Expect if I Have the Procedure ?
• Discharged on a blood thinner for at least 2 months. • Recover in the hospital overnight. • Feel “beat up” for 1 – 3 days. • Chest pain is common after the procedure. • AF recurrences are common during the first three month healing phase. • On discharge given phone numbers to call if questions. • Follow-up appointment in 1 – 3 months.

Heart Rhythm, EuroPace, JICE March 1, 2012
Update on New AF Ablation Guidelines

Indications for Catheter Ablation Of Atrial Fibrillation

Patient Selection for Ablation
Courtesy of Hugh Calkins, MD.
More Optimal Patient Less Optimal Patient
Variable
Symptoms Highly symptomatic Minimally symptomatic
Class I and III drugs failed 1 0
AF type Paroxysmal Long-standing persistant
Age Younger (<70 years) Older (70 years)
LA size Smaller (<5.0 cm) Larger (5.0 cm)
Ejection fraction Normal Reduced
Congestive heart failure No Yes
Other cardiac disease No Yes
Pulmonary disease No Yes
Sleep apnea No Yes
Obesity No Yes
Prior stroke/TIA No Yes

Conclusion
• Catheter ablation of AF is an effective treatment strategy for atrial fibrillation.
• The efficacy of the procedure depends on many variables including the AF type, the patient population, the definition of success, and the intensity and duration of follow-up.
• Major complications occur in 1 to 4% of patients.
• Catheter ablation of AF is indicated in the treatment of patients with symptomatic AF refractory to at least one antiarrhythmic agent.

Thank You