Embed Size (px)
Citation preview

ECG
& E
P C
ase
S
62 The Official Journal of Korean Heart Rhythm Society
Introduction
Radiofrequency catheter ablation (RFCA) is
the first choice of treatment for symptomatic
AVNRT.1However,itsuseinpatientswithan-
atomicvariationscanbecomplicated.Here,we
presenttwocasesofcatheterablationforAVN-
RTinpatientswithanatomicvariations:anRA
septal diverticulum, and lung-disease-induced
heartdistortion,respectively.
Case1
A22-year-oldwomanpresentedwithpar-
oxysmal palpitation. Electrocardiography (ECG)
revealed narrowQRS tachycardiawith a pulse
rateof160beats/minduringpalpitation(Figure
1).Thepatient’sbloodpressurewas110/80mmHg
duringtachycardia.QRSrhythmwasregularand
pseudoR’wavewasobserved in theprecordial
leadfromV1toV3.Sinusrhythmwasrestored
following rapid administration of intravenous
adenosine(6mg).Thepatienthadnohistoryof
diseaseoroperations.Atransthoracicechocar-
diogram (TTE) showed normal left ventricular
ejectionfraction(60%)andnostructuralabnor-
malities.Forelectrophysiological(EP)investiga-
tion,a2-mmanda4-mmquadripolarcatheter
wereusedtorecordHisandrightventricular(RV)
activity, respectively. Unfortunately, placement
Received: May 23, 2014Revision Received: September 10, 2014accepted: September 14, 2014Correspondence: Sang Weon Park MD, PhD, Department of cardiology, Korea University Anam Hospital, 73, inchon-ro, Seongbuk-gu, Seoul 136-705, KoreaTel: +82-2-920-6394, Fax: +82-2-927-1478 E-mail: [email protected] Ko, MD, PhD, Division of cardiology
고려대학교 의과대학 내과학교실 노 승 영 / 박 상 원
Seung-Young Roh, MD / Sang Weon Park, MD, PhDDivision of Cardiology, Department of Internal Medicine, Korea University Medical Center, Seoul, Korea
Anatomical Obstacles to Catheter Ablation for Atrioventricular Nodal Reentrant Tachycardia
ABSTRACT
Atrioventricular nodal reentrant tachycardia (AVNRT) is one of the most common forms of arrhythmia. The first line of treatment is typically radiofrequency catheter ablation (RFCA), though the efficacy and safety of this procedure can be limited by anatomic variations. We present two cases of patients with anatomic variations undergoing RFCA for AVNRT. These variations were: first, a diverticulum in the right atrial (RA) septum, and second, heart distortion caused by a tuberculosis-destroyed lung. Despite efforts to normalize the procedure,
both variations complicated the execution of RFCA.
Key Words: ■ atrioventricular nodal reentrant tachycardia ■ catheter ablation ■ diverticulum ■ complication

63
ECG
& E
P C
ase
S
VOl.15 NO.3
Figure 1. ECG for Case 1. The patient presented with palpitations. The observed narrow QRS tachycardia was attributed to AVNRT fol-lowing EP investigation. Pseudo R' was observed in precordial lead from V1 to V3 (arrows).
Figure 2. Right atrial angiogram for Case 1. A pouch-like structure with contractility was observed in the lower septum of the RA (indi-cated by dot line in A and arrows). It was not definitely separated in RAO view. (A) LAO view. (B) RAO view.a, duodecapolar catheter for RA; b, quadripolar catheter for His; c, quadripolar catheter for RV; d, pigtail catheter for dye injection
A B

ECG
& E
P C
ase
S
64 The Official Journal of Korean Heart Rhythm Society
Figure 3. Coronary sinus angiogram by retrograde approach for Case 1. The pouch-like structure (indicated by arrows) in the right atrial septum was not enhanced.a, duodecapolar catheter for RA; b, quadripolar catheter for His; c, quadripolar catheter for RV; d, pigtail catheter for dye injection; e, Judkins catheter for left coronary angiogram *, coronary sinus ostium
Figure 4. ECG for Case 2. The patient presented with palpitation. The observed narrow QRS tachycardia was attributed to AVNRT fol-lowing EP investigation.
A B

65
ECG
& E
P C
ase
S
VOl.15 NO.3
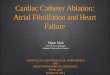
Figure 5. (A) Chest radiography for Case 2. The right lung was destroyed by prior tuberculosis infection. (B) Chest computed tomography for the same patient. The heart was rotated counter-clockwise and distorted by the destroyed lung.RV, right ventricle; LV, left ventricle; RA, right atrium
ofaduodecapolarcatheterintothecoronarysi-
nus(CS)failedasitcouldnotbeadvancedinto
theCSostium.Arightatrial(RA)angiogramwas
performed for structural analysis (Figure 2).A
pouch-likestructurewasobservedinthelower
septumoftheRA,neartheCSostium.Asthis
structureexhibitedcontractility,itwasdiagnosed
asadiverticulum,ratherthanaseptalaneurysm.
ACSangiogramrevealednoassociationbetween
thediverticulumandtheCS(Figure3).Attempts
toplacetheduodecapolarcatheterintheCSwere
impededbythediverticulum.AnEPstudywas
subsequently performed using a duodecapo-
lar catheter positioned at the RA. Tachycardia
wasinducedafteranatrio-His(AH)jump,and
atrioventricular and ventriculoatrial conduction
exhibiteddecrementalproperties.Clinicaltachy-
cardiawasattributedtoslow-fastAVNRTafter
differentialdiagnosticmaneuvers.Adeflectable
ablationcatheterwitha4-mmtipwaspositioned
at theanteriormarginof theCStoablate the
slowpathway.Theablationcatheterwasfound
tobeunstableyet itwaseasilymovedupand
downatthemarginoftheseptaldiverticulum.As
aresult,successfulRFCAwasonlyachievedafter
aconsiderabletimeinterval.
Case2
A71-year-oldmanwithatuberculosis-de-
stroyedlungpresentedwithpalpitationanddys-
pnea.Electrocardiography (ECG) revealednar-
row-QRStachycardiawithashortRP interval
andapulserateof170beats/minduringpalpita-
tion(Figure4).Thepatient’sbloodpressurewas
100/70mmHgatthetimeofrecording,andQRS
rhythmwasregular.Sinusrhythmwasrestored
followingrapidadministrationofintravenousad-
enosine(6mg).Thepatienthaddiabetesmel-
litus,hypertension,andahistoryofpulmonary
A B

ECG
& E
P C
ase
S
66 The Official Journal of Korean Heart Rhythm Society
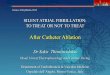
Figure 6. Electrogram (A) and catheter position (B) for Case 2. Before ablation, the lowest point for detection of His potential (in-dicated by arrows) was identified using the ablation catheter (d). (C) Electrogram and (D) catheter position at the time of ablation. Ablation was actually carried out at a lower point than that depicted in (B). His potential was not seen on the electrogram from the ablation catheter.a, duodecapolar catheter for right atrium and His; b, quadripolar catheter for His; c, quadripolar catheter for right ventricle
A
C
B
D

67
ECG
& E
P C
ase
S
VOl.15 NO.3
tuberculosis.ATTEshowedpreservedleftven-
tricularejectionfraction(55%)andnostructural
abnormality.Chestradiographyandchestcom-
puted tomography showed a severely distorted
lung(Figure5),andcounter-clockwiserotation
oftheheart.InRAangiography,theRAexhibited
erectmorphology.AnEPinvestigationwassub-
sequentlyperformedusinga2-mmanda4-mm
quadripolarcatheter torecordHisandRVac-
tivity,respectively.Aduodecapolarcatheterwas
positionedattheCSandtheRA.Clinicaltachy-
cardiawasattributedtoslow-fastAVNRTonthe
basisofEPinvestigation.Duetothehighriskof
atrioventricular(AV)block,owingtothepatient’s
advancedageanddistortedheartstructure,the
ablation focus was carefully considered. First,
thelowestlevelfordetectionofHispotentialwas
identified(Figure6A,B).Next,aposteriorap-
proachwas taken, via themiddle or posterior
septalregionneartheCSostium(Figure6D).His
potentialwasnotobservedontheelectrogramof
theablationcatheter(Figure6C).Energydeliv-
eryresultedinsuccessfulinductionofjunctional
rhythm,thoughablationwasimmediatelyabort-
edonobservingventriculoatrial(VA)conduction
blocksomesecondslater.AhighdegreeofAV
blockwithconcurrenthypotensionoccurred.The
AVblockwas initially sustainedbuteventually
recoveredaftereighthours;thePRintervalnor-
malizedaftertwoweeks.
Discussion
AVNRTisoneofthemostcommontachyar-
rhythmias,andcanbetreatedbycatheterabla-
tion.Thiscanbehazardouswhentheslowpath-
wayisincloseproximitytothenormalconduction
system.Thus,aclearunderstandingofcardiac
anatomyisessentialbeforeAVNRTablation.
We have reported two complicated AVNRT
casesrelatedtorightheartanatomicabnormali-
ties.Inthefirstcase,anRAseptaldiverticulum
compromisedthepositioningandstabilityofthe
catheter.Binderetal.analyzed103casesofcon-
genitalmalformationsoftheRAandtheCS.2Of
the103casesstudied,13wereassociatedwithan
RAsinglediverticulumandthesewerepredomi-
nantlyasymptomatic.Thepresentationofsymp-
toms suchas supraventricular tachycardiawas
frequentlyinducedbyarrhythmia.
Wepresentthefirstreportedcaseofasingle
diverticulumintheRAseptum.Previousstudies
havereportedcasesofRAdiverticulapredomi-
nantlylocalizedtotheRAfreewallortheCS.2-7
TheRAseptaldiverticulumdescribedinthiscase
wasseparatedfromtheCS,asdemonstratedby
theangiogram.Becausethediverticulumexhib-
ited contractility consistentwith theheartbeat,
weruledoutthealternativediagnosisofseptal
aneurysm, in which contractility would not be
observed.8
Acquiredanatomicdistortionscanalsointer-
ferewithRFCAforAVNRT.Inthesecondcase,
safetywasensuredbyusingnumerousmethods:
(1)RAangiogram,(2)confirmationofthelowest
pointfordetectionofHispotential,(3)aposte-
riorapproachneartheCSostium,and(4)vigilant
observation ofVA conduction.A contemporary
transienthighdegreeAVblockwasnevertheless
seentooccur.
Foreffectiveandsafecatheterablationinpa-
tientswith anatomic obstacles, an overview of
thepreciseanatomyiscritical.Angiogramsand
carefulmappingcanfacilitatetheidentificationof
anatomicvariants,andcanconfirmprecisecath-
eterpositioning.

ECG
& E
P C
ase
S
68 The Official Journal of Korean Heart Rhythm Society
Conclusion
WehavereportedtwodifficultAVNRTcasesre-
latedtorightheartanatomicvariation:thefirst,
anRAseptalaneurysm,andthesecond,heart
distortion due to tuberculosis-destroyed lung.
Anatomic obstacles can compromise successful
catheterablationforAVNRT.
Reference
1. Katritsis DG, Camm AJ. Atrioventricular nodal reentrant tachycardia. Circulation. 2010;122:831-840.
2. Binder TM, Rosenhek R, Frank H, Gwechenberger M, Maurer G, Baum-gartner H. Congenital malformations of the right atrium and the coro-nary sinus: an analysis based on 103 cases reported in the literature and two additional cases. Chest. 2000;117:1740-1748.
3. Morrow AG, Behrendt DM. Congenital aneurysm (diverticulum) of the right atrium. Clinical manifestations and results of operative treatment. Circulation. 1968;38:124-128.
4. Di Segni E, Siegal A, Katzenstein M. Congenital diverticulum of the heart arising from the coronary sinus. Br Heart J. 1986;56:380-384.
5. Pastor BH, Forte AL. Idiopathic enlargement of the right atrium. Am J Cardiol. 1961;8:513-518.
6. Morishita Y, Kawashima S, Shimokawa S, Taira A, Kawagoe H, Na-kamura K. Multiple diverticula of the right atrium. Am Heart J. 1990;120:1225-1227.
7. Sheldon WC, Johnson CD, Favaloro RG. Idiopathic enlargement of the right atrium. Report of four cases. Am J Cardiol. 1969;23:278-284.
8. Mugge A, Daniel WG, Angermann C, Spes C, Khandheria BK, Kronzon I, Freedberg RS, Keren A, Denning K, Engberding R, Sutherland GR, Vered Z, Erbel R, Visser CA, Lindert O, Hausmann D, Wenzlaff P. Atrial septal aneurysm in adult patients. A multicenter study using transthoracic and transesophageal echocardiography. Circulation. 1995;91:2785-2792.