Embed Size (px)
Citation preview

What Does All this Mean from the Patient Perspective?
For patients, palliative care is a key to:• relieve symptom distress • navigate a complex and confusing medical system• understand the plan of care• help coordinate and control care options• allow simultaneous palliation of suffering along with
continued disease modifying and rehabilitative treatments (no requirement to give up curative care)
• provide practical and emotional support for exhausted family caregivers

The Clinician Perspective
For clinicians, palliative care is a key tool to:
• Save time by helping to handle repeated, intensive patient-family communications, coordination of care across settings, comprehensive discharge planning
• Bedside management of pain and distress of highly symptomatic and complex cases, 24/7, thus supporting the treatment plan of the primary physician
• Promote patient and family satisfaction with the clinician’s quality of care

The Hospital Perspective
For hospitals, palliative care is a key tool to:
• effectively treat the growing number of people with complex advanced illness
• provide service excellence, patient-centered care
• increase patient and family satisfaction• improve staff satisfaction and retention • meet JCAHO quality standards• rationalize the use of hospital resources• increase capacity, reduce costs

Summary: Making the Case
• Universal human experience and universal health professional obligation.
• Palliative care improves quality of care for our sickest and most vulnerable patients and families.
• Palliative care is an integral part of geriatric medicine, contributes to goals of both functional recovery and best possible quality of life

How Do You Use this Information to Integrate Palliative and Geriatric
Medicine?The next 2 presentations will help you:• Tailor the case made here to your
practice setting• Create compelling business
marketing plans• Design and launch a program• Measure your success
Although the world is full of suffering, it is also full of the overcoming of it.
Helen KellerOptimism 1903

Appendix

More and more physicians are providing palliative care
• Number of hospital-based palliative care programs has doubled in recent years to more than 950
• One in five hospitals now offers palliative care• US News & World Report includes palliative care
in its criteria for “America’s Best Hospitals”• ABHPM certifying more and more physicians• Referral rates at established programs are
growing each year
Billings JA et al J Pall Med. 2001, AHA Survey 2002, Pan CX et al J Pall Med. 2001

But…
• Number of palliative care programs, specialists not sufficient to meet patient need
• In absence of comprehensive palliative care programs and PC specialists, physicians need basic PC clinical skills
Palliative Care Operational Resources
Go to www.capc.org 1. Palliative Care Leadership Centers: six premier
palliative care programs hosting site visits and providing ongoing mentoring
2. Web site: Comprehensive tools for starting and sustaining palliative care services: billing for palliative care services, clinical models, criteria for referral, clinical forms and procedures, technical assistance publications and presentations
3. CAPC seminars on building palliative care programs

CAPC Products
• Management and Training Seminars- next in Miami, March 2005
• www.capc.org• Palliative Care Leadership Centers• Publications:
A Guide to Establishing a Hospital-Based Palliative Care Program
Hospice-Hospital Partnerships The Case for Hospital Based Palliative Care

Palliative Care Leadership Centers
• Six exemplary programs for 2.5 d. site visits, hands-on learning, +1 yr. distance mentoring. Only available til Spring 2006 and filling up fast! Consistent curriculum, different hospital settings, and locations.
• “The site visit program made all the difference. Because of what our staff learned, our palliative care program has more patients, a larger budget, and much more legitimacy throughout the hospital. It really helped to have a leader in the field behind our efforts.”Erin Rhatigan, RN, HPNC/ Community Hospital of the Monterey Peninsula

Palliative Care Leadership Centers
• Fairview Health System- Minneapolis• Mt. Carmel Health System- Columbus,
OH• Medical College Wisconsin- Milwaukee• Palliative Care Center of the Bluegrass-
Lexington, KY• UCSF- San Francisco• Virginia Commonwealth University-
Richmond
CAPC Resources: Palliative Care Program Nuts and Bolts
•Leadership• Strengths and weaknesses of clinical
models• How to choose
• Resources: www.capc.org

Leadership• Physician• Nurse • Social Work, Care
Management• Chaplain• Pharmacist• Critical care• Hospitalist• Ethics• Oncology• Geriatrics• Nursing Department
• Rank and authority in institution
• Opinion leadership• Respect of others• Competence

Outline
• Leadership of models
•Strengths and weaknesses of clinical models
• How to choose
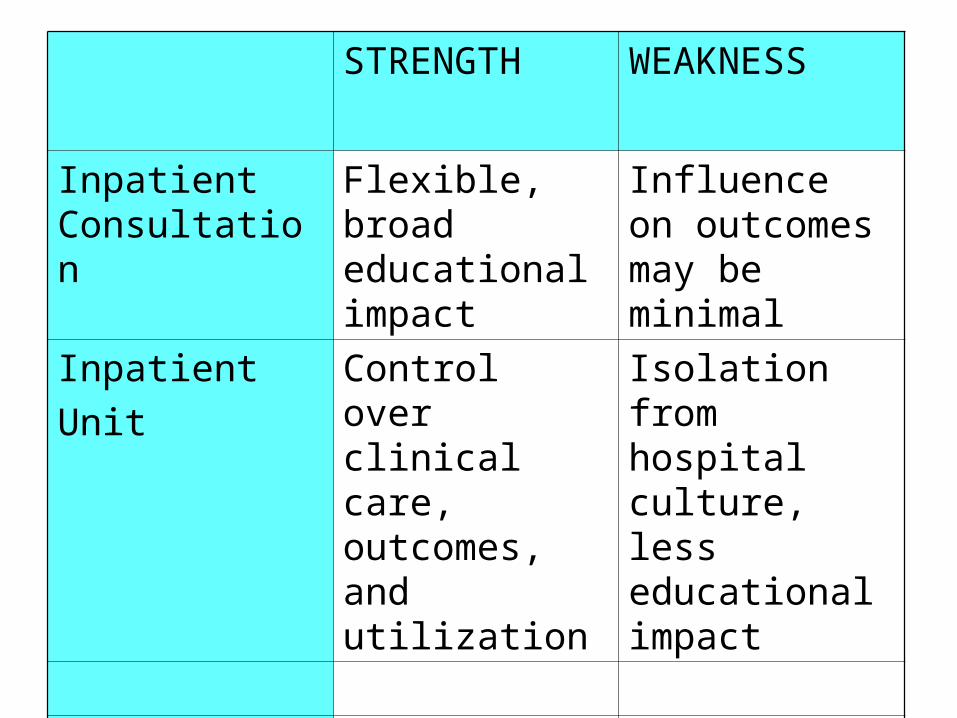
STRENGTH WEAKNESS
Inpatient Consultation
Flexible, broad educational impact
Influence on outcomes may be minimal
InpatientUnit
Control over clinical care, outcomes, and utilization
Isolation from hospital culture, less educational impact

Outline
• Leadership of models• Strengths and weaknesses
•How to choose

How to choose (where to start)
• What is needed?• What is possible? • Who wants to do this? • Who has the skills to do it? • Who can make the commitment to do this? • Who is most likely to be able to make the
case and gain support?• What is easy?• Where and with whom does support lie?

Bed Availability
Beds are not availableAll beds occupiedPatients ‘can’t get in’
Beds are availableClosed units
Consult Service easier Inpatient Unit Possible

Hospital Size
Small Hospital Large Hospital
Consult Service easier Inpatient Unit Possible
Physicians
Private Practice Staff Model-HMO, capitated care
Consultation Etiquette‘Open’ inpatient unit
Primary Care‘Closed’ inpatient unit

Local Culture
Private PracticeTraditional
Collaborative Patterns
Physician-led Nurse-Led
Hospice
Present Absent
Collaborate Home visits

Health Care Funding
Fee-for-Service Global Budget
Justify ServicesBased on Revenues,Cost avoidance
Justify ServicesBased on Utilization,Cost avoidance

How models chosen
• Administrator interest• Clinician interest• Loci of support• Community pressure• Serendipity (loss)• Opportunity

Summary: Assessing Needs and Choosing a Model
• Many variables influence program development
• Several leadership models• Several models• Strengths and weaknesses• Select the structure that is best for
you• No one right way

Where can you learn more palliative medicine content?

Domains of Palliative Care
• Communication, help with medical decision-making
• Expert symptom assessment and treatment
• Psychosocial and practical support, care coordination, and bereavement services

Communication
• Essential to practice of palliative medicine: decreases anxiety, improves well-being, satisfaction with providers and health care, and outcomes
• Good communication: honesty, willingness to talk about dying, sensitive delivery of bad news, listening, and encouraging questions.
• MD role: Articulating choices, likely benefits and burdens, and helping patient/family to make medically appropriate decisions in keeping with their goals.

How to Communicate• Establish realistic, attainable goals of care
• Help patients and families understand scope of illness and likely progression
• Identify relevant values and goals• Define “acceptable” and “unacceptable”
quality of life• Define choices to be made and their
benefits and burdens• Help with decision-making• Develop care plans that maximize
chances that goals will be achieved

Establishing Goals of Medical Care
Communicating Bad News
Withholding/Withdrawing Treatment
Get started and create the right setting: Plan what to say, create a conducive setting, allow adequate time, and determine who else should be present
Establish what the patient knows: Clarify the situation and context in which the discussion about goals is occurring
Establish what the patient knows: What is known, access ability to comprehend, reschedule if unprepared
Establish and review the goals of care
Explore both what patients are expecting and hoping to accomplish: Help identify realistic and non realistic goals
Establish how much the patient wants to know? Recognize and support different preferences. People handle information differently
Establish the context of the current discussion: What has changed to precipitate the discussion?
Suggest realistic goals: Explore how goals can be achieved and work through unreasonable/ nonrealistic expectations
Share the Information: Say it then stop (avoid jargon, pause frequently, check for understanding, use silence), don’t minimize the information
Discuss specific treatment(s) in context of goals of care: Will continuation or initiation of the treatment meet the goals of care?
Communication Protocol

Discuss alternatives to the proposed treatment and what will happen if the patient decides not to have the treatment
Respond empathetically to feelings: Be prepared for strong emotions and allow time for response, listen, encourage description of feelings. Allow silence
Make a plan and follow through: What treatments will be undertaken to meet goals. What treatments will not be utilized. Establish a concrete plan for follow-upReview and revise periodically as needed
Planning/Follow up: Plan for next steps, discuss potential sources of support, give contact information, assess patient safety and supports, repeat news at future visits
Document, disseminate (i.e., to family, other healthcare team members), and implement plan for withdrawal of treatment
Protocol, continued

Symptom Assessment and Treatment
3 items necessary for good pain and symptom management:
1. Routine and repeated assessment
2. Skill in prescribing3. Treatment of side effects

Symptom Assessment and Treatment
• Pain management• Pain meds administered on standing or
regular basis• PRN or rescue doses available for
breakthrough pain or pain not controlled by regimen
• All patients on opioids should be started on a bowel regimen
• WHO analgesic ladder should be used as a guide for most pain syndromes

WHO Analgesic Ladder• Mild Pain (1-3/10 on a 10 point scale): Begin
acetaminophen or a non-steroidal antiinflammatory agent (consider opioids instead in older adults)
Moderate Pain (4-7/10): Begin an opioid combination product (acetaminophen + codeine, acetaminophen + oxycodone, acetaminophen + hydrocodone) and dose based upon opioid half life (3-4 hours) not acetaminophen half life (6-8 hours).
Severe Pain (8-10/10): Begin a strong standing opioid (hydromorphone, morphine sulfate, oxycodone) and titrate until pain relief is obtained or intolerable side effects develop. Long acting opioids (sustained release morphine/oxycodone, transdermal fentanyl) should be started after pain is well controlled and steady state is achieved.

Symptom Assessment and Treatment: Pain
• Rescue doses employing immediate release opioids, dose should be 10% of the 24 hour total opioid dose and given every hour (oral) and every 15 - 30 minutes (parenteral) as needed. Methadone should only be used by clinicians experienced in its use.
• Adjuvant agents (corticosteroids, anticonvulsants, tricyclic antidepressants, bisphosphonates) should be employed for specific pain syndromes when applicable (e.g., neuropathic pain).

50% of pain management = side effect management
• Constipation• Nausea• Confusion, sedation

Constipation
• Does not resolve!• Morbidity: obstruction, nausea,
delirium, perforation, death• Prevention; monitoring; check for and
treat impaction• Rx: softeners, polyethylene glycol
powder Miralax, senna, bisacodyl tabs or suppositories, sorbitol, mg citrate, enemas

Nausea
• CTZ- area postrema of medulla; vestibular; delayed gastric emptying
• Tolerance develops: Usually resolves after 3 – 5 days
• If persistent nausea – evaluate for other causes
• Metoclopramide, haloperidol, diphenhydramine (DA, 5HT, histamine)

Sedation• Side effect versus need to catch up on sleep after
pain resolves• Tolerance develops rapidly (hours)• Sedation always predates respiratory depression• If RR < 8 and patient unarousable, use 10:1
dilution of naloxone, tirate to arousal, and monitor closely
• Naloxone half life = minutes• Persistent sedation usually multifactorial• Rx- identify and treat underlying contributors,
opiate dose adjustment, opiate rotation, antipsychotics, psychostimulants,

If you don’t ask you won’t know. Routine assessment is prerequisite to good
symptom management.
• Pain• Weakness• Fatigue• Anorexia/cachexia• Constipation• Dyspnea• Nausea• Constipation
• Anxiety• Depression• Delirium• Sleep• Energy• Hopes and fears• Biggest concern• Tools at
www.promotingexcellence.org

Practical Support and Care Coordination:Mobilizing Community Resources
• 95% of the illness and the care occurs at home
• Families provide >70% of long term care• Most patient/family needs cannot be met in
physician offices and hospitals• Physicians can help by coordinating array of
community services for patients and families – Home safety and needs evaluation, PACE, visiting RN/home care services, case management, hospice, financial planning resources, Medicaid eligibility, family support groups.

Other Resources
1. Communication and decision-making2. Pain and symptom management3. Care coordination, commmunity
resources for patients and families

Communication
1. Buckman R. How to Break Bad News: A Guide for Health Care Professionals. Baltimore: Johns Hopkins University Press, 1992 - The definitive guide for communicating bad news.
2. Meier DE, Back AL, Morrison RS. The inner life of physicians and care of the seriously ill. JAMA 2001; 286:3007-14. - Practical approaches to self care for physicians caring for seriously ill patients
3. EPEC - A continuing medical education program providing detailed protocols for major communication topics (www.epec.net)
4. The Center for Palliative Care of Harvard University Medical School - Continuing medical education programs in communication skills for practicing clinicians (http://www.hms.harvard.edu/cdi/pallcare/)

Symptom Assessment and Treatment1. Doyle D, Hanks G, MacDonald N. Oxford Textbook of
Palliative Medicine: Second Edition. Oxford: Oxford University Press, 1998. Comprehensive textbook of palliative care.
2. Morrison RS, Meier DE. Geriatric Palliative Care. New York: Oxford University Press, 2003. Comprehensive textbook of palliative care focused specifically on older adults.
3. Education for Physicians in End of Life Care www.epec.net - A continuing medical education program providing practical advice for managing pain and other symptoms
4. Fast Facts and Concepts on End of Life Care- Concise evidence based summaries on treatment of common symptoms www.mcw.edu/pallmed/html/about1.html
5. palliativedrugs.com growthhouse.org stoppain.org

Psycho‑Social Support and Care Coordination
1. Elderweb- A comprehensive listing of services for older adults including resources for personal care needs, care coordination, and home care www.elderweb.com
2. EPEC - Contains modules on psycho-social support and grief and bereavement www.epec.net
3. National Agency for Home Care and Hospice www.nahch.org and National Hospice and Palliative Care Organization www.nhpco.org - Trade organizations whose web sites provide comprehensive lists of member home care agencies and hospices searchable by city and zip code.
4. Growthhouse - Grief and Bereavement Resources www.growthhouse.org5. Bereavement and Hospice Support Netline –An online directory of
bereavement and hospice bereavement programs in the U.S www.ubalt.edu/www/bereavement
6. Centers for Medicare and Medicaid Services (CMS) - Information about Medicare coverage and Medicaid eligibility. Information about PACE programs (including their location) and Medicare Choice Programs (which may include case management) can also be obtained at www.cms.gov.

Education is Not OptionalTraining opportunities• ELNEC www.aacn.nche.edu/elnec• EPEC www.epec.net• DELeTCC www.deletcc.coh.org• EPERC www.eperc.mcw.edu• AAHPM www.aahpm.org• Harvard www.hms.harvard.edu/cdi/pallcare/• Fellowship training
www.aahpm.org• ANP palliative care training programs,
ANCC certification
www.hpna.org www.nursingworld.org• MD Certification: ABHPM
www.abhpm.org

“I don’t know enough about palliative care.”
• Get training (EPEC, ELNEC, DELeTCC, AAHPM-HPNA, Harvard advanced courses)
• Subscribe to the J of Palliative Medicine. Get the Oxford Textbook of Palliative Medicine
• Do a site visiting program (Palliative Care Leadership Centers, Cleveland Clinic, Beth Israel Med Ctr in NYC, San Diego Hospice, others)
• Take a year off and do a fellowship or an APN degree program

“Our hospital doesn’t have expertise in palliative care.”
• www.epec.net -MD• www.aacn.nche.ed
u/elnec -RN
• www.deletcc.coh.org• www.EPERC.mcw.edu• APN www.hpna.org• Fellowships
www.aahpm.org• Site visiting programs
• Read• Harvard course• Go to the AAHPM
annual meeting• Use the web
• www.palliativedrugs.com
• www.growthhouse.org• www.stoppain.org
• Learn by doing