Embed Size (px)
Citation preview
What can health informatics offer to improve the management of infection?
Prof Peter Davey
Community Health Sciences Division,College of Medicine, Nursing and Dentistry
www.dundee.ac.uk/[email protected]
1/15
Agenda• UK’s unique opportunities for research
with routine data• What is the added value of individual data
versus aggregate data?• Examples of record linkage studies from
primary and secondary care• What kind of information do we need to
make a difference to prevention and management of infection?
• What are SIRN’s plans for the future?2/15
3/15
UKCRC R&D Advisory Group to Connecting for Health Report2007
Within the UK, Scotland has pioneered systems of linkage since the mid 1970’s, when a far-sighted director of public health introduced the Community Health Index, the Scottish equivalent of the NHS number, and made it his mission to get this used in all NHS settings.
It is clear that Scotland has developed an enviable system and has much experience and expertise to share with other UK countries.
Experience in Denmark suggest that a population of perhaps 5 million may mark the upper limit of what is technically manageable. So it may be preferable to expand and link existing databases such as those in Manchester, Wirral and eastern Scotland, and create new ones, rather than attempting to build one repository for all of the UK’s medical information.”
4/15

Prof James Crooks Dr Ronnie Graham
October 1978• A uniform method
for indexing patient records in primary and secondary care will transform services and research, leading to a more integrated approach to health care.
October 1978
• “It might, then, be reasonable to suppose that a new system of information distribution would precede change in practice. It is however, abundantly clear to even the casual observer that our medical information handling has changed little with administrative restructuring.”
8/15www.dundee.ac.uk/hic
9/15
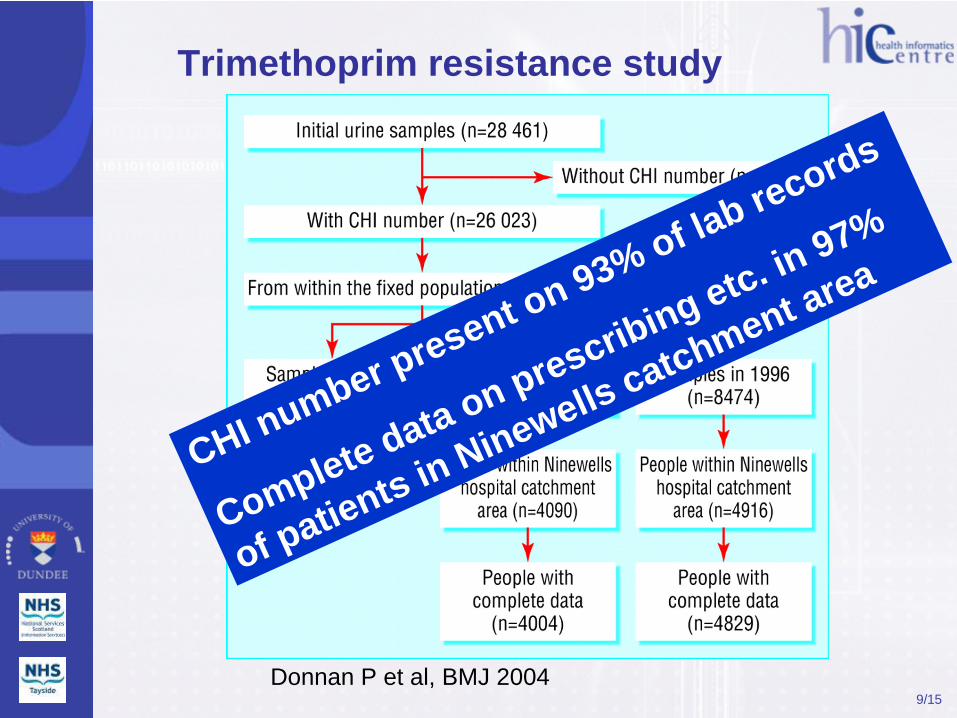
Trimethoprim resistance study
Donnan P et al, BMJ 2004
CHI number present on 93% of lab records
Complete data on prescribing etc. in 97%
of patients in Ninewells catchment area

Association between prevalence of trimethoprim resistant bacteria in urine & practice level variables
• Analysis of practice level data obscured important associations between antibiotic prescribing and resistance.– Wide practice variation in resistance (26-50% of
bacteria isolated) and prescribing (67-357 prescriptions per 100 practice patients).
– At practice level, no association of prescribing with resistance (P = 0.101)
– At the patient level resistance was significantly associated with exposure to trimethoprim (P < 0.001) or to other antibiotics (P = 0.002).
• The results show the added value of individual patient data for research on the outcomes of prescribing.
10/15
Ecological fallacy – variation in drug use at the
population level correlates poorly with individual
patient outcome
11/15
In response to: Donnan et al Br Med J 328:1297, 2004.
Leading the way in Europe:
http://www.eu-burden.info/burden/pages/home.php
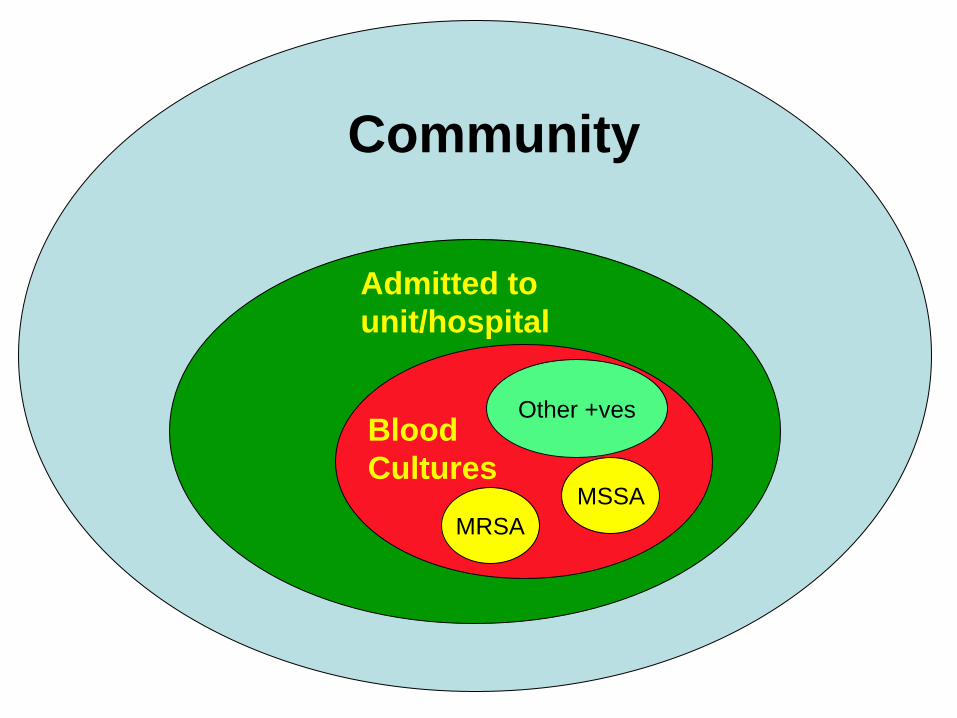
MRSAMSSA
Blood Cultures
Admitted to unit/hospital
Community
Other +ves

Analysis:HAI As A Time Dependent Variable
0 1
2 3 4 5
No HAI
HAI
Discharge DischargeDeath Deathchange LOS is an R package to:• describe any multistate model• compute and visualize transition probabilities• compute and visualize change in LOSHAI, hospital-acquired infection; LOS, length of stay Wangler M et al. R News 6;2, May 2006
Design BURDEN WP5 & WP 7
• Two matched cohort studies:–Hospital acquired, drug resistant
bacteraemia & controls–Hospital acquired drug sensitive
bacteraemia & controls• Matched by ward & calendar
date (within 7 days)

WP 5 & WP 7• Four comparisons:1.Full cohort vs two randomly
selected comparators2.Electronic vs case note
comorbidity3.90 day mortality vs in hospital
mortality and 30 day4.Additional burden of readmission
http://www.idrn.org/antimicrobial_prescribing.php

Association Between Antibiotic Prescribing and Complications of RTI
Presentation Complication Risk without antibiotics, per 10,000 treated
Number Needed to Treat
Sore throat Scarlet feverQuinsy
314
10,9144,520
Otitis media Mastoiditis 3 Not effectiveURTI Pneumonia 14 15,817LRTI Pneumonia 196 73
Age 0-45-15
16-64>65
14612114747
What kind of information do we need to make a difference?• What might work?
– Modelling interventions (prevention, diagnosis or management)
– Unintended as well as intended consequences– Patient, professional and policy maker
perspectives• How can we maximise the impact of
interventions on practice?• How should we evaluate interventions?• What is the impact of context?
19/15
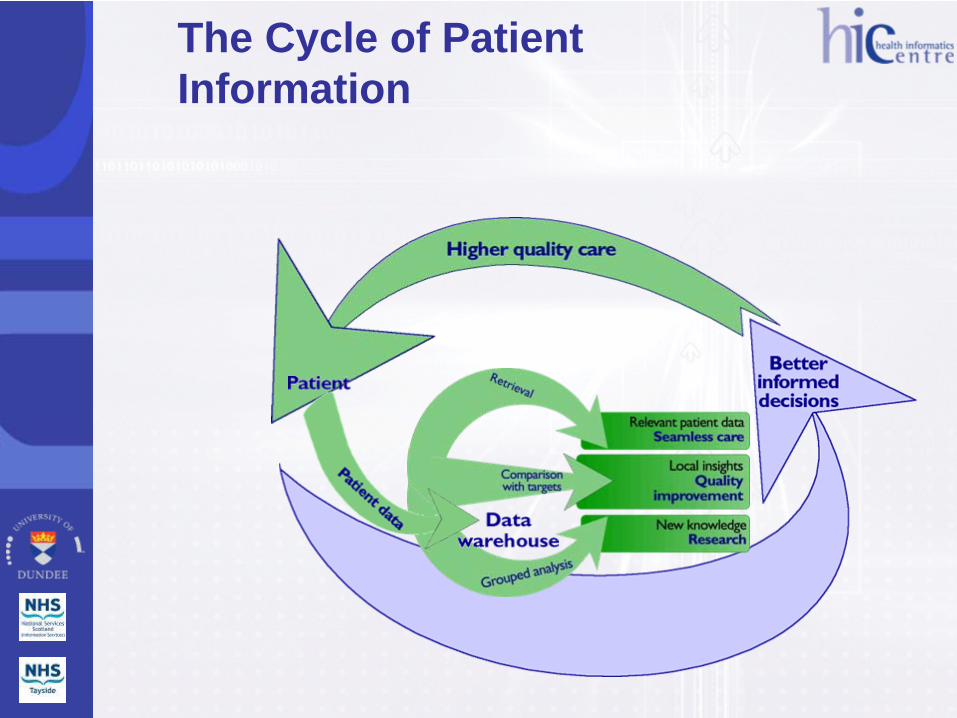
The Cycle of Patient Information
• Ann: using information to help patients make decisions
• Brenda: Improving the patient’s journey of care
• David: Involving people in research
• Joan: Do people become resistant to antibiotics?
• Morag: using information to promote oral health
• Dr Menzies: confidentiality and privacy
Core Principles of HIC
• PrivacyNo individual patient or practitioner can be traced from data sent to / held by HIC without permission
• TransparencyClear standard operating procedures applied across diseases and geographical areas
• InvolvementProduce value to contributors of data

Collaborative Research Scotland
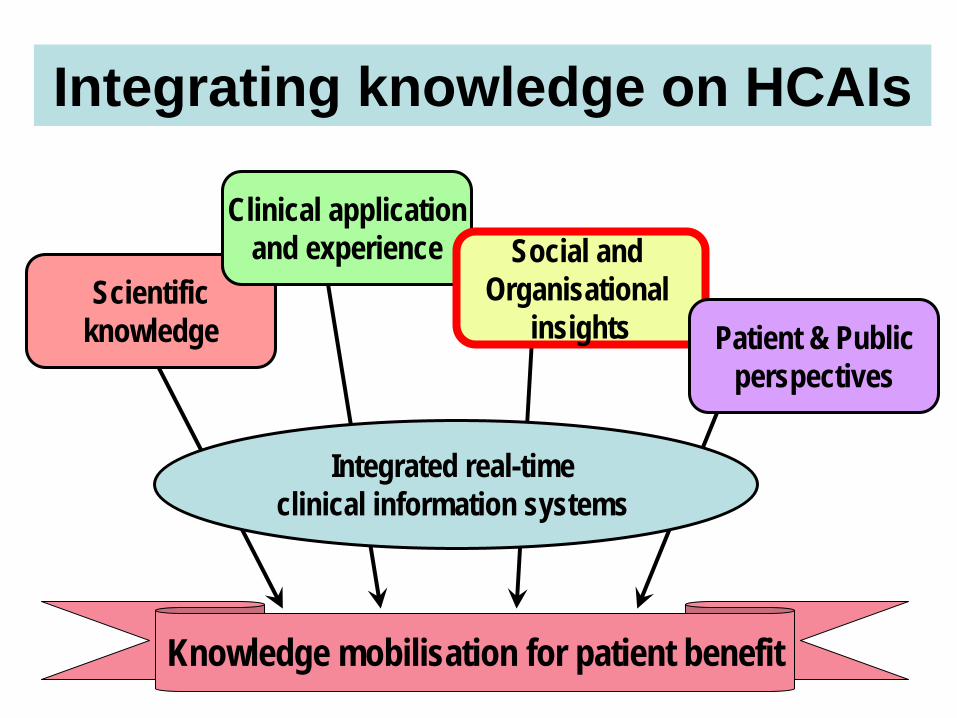
Integrating knowledge on HCAIs
Scientific knowledge
Clinical application and experience Social and
Organisational insights Patient & Public
perspectives
Integrated real-time clinical information systems
Knowledge mobilisation for patient benefit





























