Embed Size (px)
Citation preview

PATIENT NAME: DATE:
Check all that apply based on what you are CURRENTLY experiencing
CHILL AND FEVER
Averson to cold & feeling chilly WC/WH
Low grade fever (afternoon only) YIN-DEF
Constant low grade fever DAMP-HEAT
Fever in the middle of the night YIN-DEF
Chills & fever INTERMEDIATE
SWEATING
Head only STOMACH HEAT/DAMP HEAT
Arms & legs ST/SP DEF
Hands only LUNG QI DEF/NERVOUSNESS
Whole body LUNG QI DEF
Palms, soles & chest YIN DEF
Oil sweat on forehead YANG COLLAPSE
Sweating during day/night YANG DEF/YIN DEP (DAMP HEAT)
Oily sweat YANG DEF SEVERE
Sticky sweat YIN CALLAPSE
Yellow sweat DAMP HEAT
HEAD & BODY
HEADACHES
During the day QI/YANG DEF
Night time headaches BLOOD/YIN DEF
nape of neck headache TAI YANG (EX WC/KID DEF)
forehead headache YANG MING (ST HEAT/BLOOD DEF)
headache at temples/side SHAO YANG (EX WC/WH, LIV/GB FIRE)
Top of head JUE YIN (LIV BLOOD DEF)
Whole head EX WC
Heavy feeling DAMPNESS/PHLEGM
Inside the head, hurting brain KID DEF
Distending/throbbing headache LIV YANG RISING
Boring, like a nail BLOOD STASIS
Aggravated by fatique QI DEF
BODY PAIN
Pain all over w/tiredness QI/BLOOD DEF
After birth-dull pain BLOOD DEF
After birth-arms/shoulders LIV QI STAG
All muscle pain with hot sensation ST. HEAT
Pain with feeling heaviness DAMPNESS
FOOD & TASTE
TASTE
Bitter taste LIV/HEART FIRE
Constant bitter taste LIV FIRE
Sweet SP DEF/DAMP HEAT IN THE SP/ST
Sour FOOD RETENTION/LIV ST. DISHARMONY
Salty KID YIN DEF
Pungent LUNG HEAT
Lack of taste SP DEF
WELLNESS QUESTIONAIR
FOR DOCTORS USE ONLY
TPA WELLNESS * 43422 Business Park Dr., Temecula CA 92590 * (951) 693-5555 Page 1

STOOL
CONSTIPATION
Acute w/thirst, dry yellow tongue ST HEAT/SI HEAT
With small,bitty stools like goat's LIV QI STAG-HEAT ST
With abdominal pain INTERNAL COLD & YANG DEF
With dry stools, no thirst YIN DEF (KID/ST)
Stools not dry, butt difficult to pass LIV QI STAG
Constipation and diarrhea LIV QI STAG INVADING SP
DIARRHEA
With pain LIV/HEAT
Foul smell HEAT
Absence of smell COLD
Chronic SP/KD YANG DEF
Every day/evening morning KID YANG DEF
With abdominal pain INTERIOR COLD IN INTESTINES
With mucus in stools DAMP IN INTESTINES
With mucus and blood DAMP HEAT IN INTESTINES
Loose stools with undigested food SP QI DEF
With burning sensation in anus HEAT
Not loose/frequent diarrhea SP/ST QI DEF, SP QI SINKING
Black/dark stools BLOOD STASIS
Loose stools with borborygmus (stomach rumbling) SP DEF
Borborygmus with abdominal distension LIV QI STAG
Flatulence LIV QI STAG
Flatulence with foul smell DAMP HEAT IN SP/ST HEAT
Flatulence without smell INT COLD D/T SP YANG DEF
URINE
Urinary incontinence KID DEF
Retention of urine DAMP HEAT IN UB
Difficulty urinating UB DAMP HEAT/KD DEF
Frequent and copious urination ID DEF
Frequent and scanty urination QI DEF
PAIN
Pain before urination QI STAG IN LOWER BURNER
Pain during urination HEAT IN UB
Pain after urination QI DEF
COLOR
Pale color COLD
Red/yellow/dark color HEAT
Cloudy/Murky/Thick DAMP IN UB
Abundant clear & pale BIAO
AMOUNT
Clear copious amount KD QI DEF/UB DYSFUNCTION
Large amount of urine KID YANG DEF
Scanty urine KID YIN DEF
Scanty yellow urgent painful urination DAMP HEAT IN UB
TPA WELLNESS * 43422 Business Park Dr., Temecula CA 92590 * (951) 693-5555 Page 2

SLEEP (Insomnia)
Hard time falling asleep HEART BLOOD DEF
Waking many times KID YIN DEF
Dream-distrubed sleep LIV/HEART FIRE
Restless sleep with dreams FOOD RETENSION
Waking up early morning, can't get back to sleep GB DEF
LETHARGY
Feeling sleepy after eating SP QI DEF
lethargy and dizziness PHLEGM
Extreme lethargy KID YANG DEF
EYES
Like needle pain & redness of eye(s) FIRE POISON IN HT
With swelling, redness of eye W-H INVASION/LIVER FIRE
blurry vision & floaters LIVER BLOOD DEF
Photophobia LIVER BLOOD DEF
Pressure in the eyes KID YIN DEF
Eye dryness LIV/KID YIN DEF
THIRST AND DRINKING
Absence of thirst SP/ST COLD
Thirst with no desire to drink DAMP HEAT
Thirst of warm liquids ST/KID YIN DEF
Thirst for cold liquids / warm liquids HEAT/COLD
TPA WELLNESS * 43422 Business Park Dr., Temecula CA 92590 * (951) 693-5555 Page 3
Treatment(s) you have received for this condition:
1) 2)
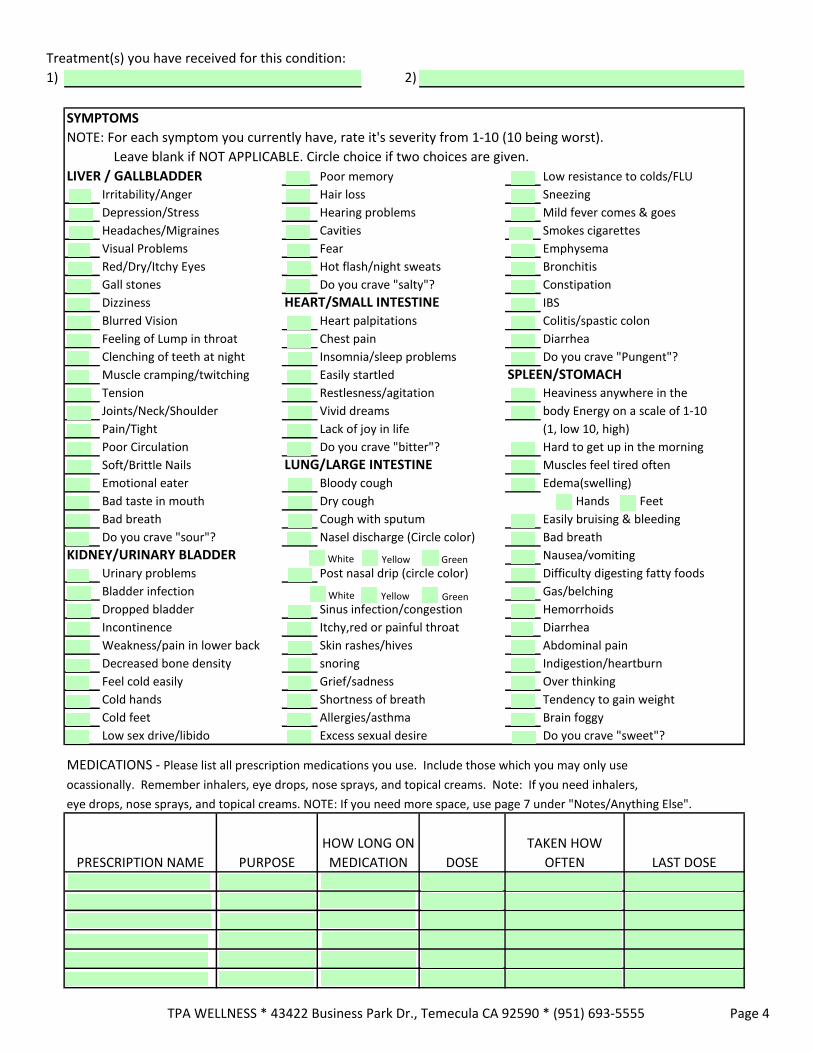
SYMPTOMS
NOTE: For each symptom you currently have, rate it's severity from 1-10 (10 being worst).
Leave blank if NOT APPLICABLE. Circle choice if two choices are given.
LIVER / GALLBLADDER Poor memory Low resistance to colds/FLU
Irritability/Anger Hair loss Sneezing
Depression/Stress Hearing problems Mild fever comes & goes
Headaches/Migraines Cavities Smokes cigarettes
Visual Problems Fear Emphysema
Red/Dry/Itchy Eyes Hot flash/night sweats Bronchitis
Gall stones Do you crave "salty"? Constipation
Dizziness HEART/SMALL INTESTINE IBS
Blurred Vision Heart palpitations Colitis/spastic colon
Feeling of Lump in throat Chest pain Diarrhea
Clenching of teeth at night Insomnia/sleep problems Do you crave "Pungent"?
Muscle cramping/twitching Easily startled SPLEEN/STOMACHTension Restlesness/agitation
Joints/Neck/Shoulder Vivid dreams
Pain/Tight Lack of joy in life
Poor Circulation Do you crave "bitter"?
Soft/Brittle Nails LUNG/LARGE INTESTINEEmotional eater Bloody cough
Bad taste in mouth Dry cough
Bad breath Cough with sputum
Do you crave "sour"? Nasel discharge (Circle color)
KIDNEY/URINARY BLADDERUrinary problems
Bladder infection
Dropped bladder
Incontinence
Weakness/pain in lower back
Decreased bone density
Feel cold easily
Cold hands
Cold feet
Low sex drive/libido
Post nasal drip (circle color)
Sinus infection/congestion
Itchy,red or painful throat
Skin rashes/hives
snoring
Grief/sadness
Shortness of breath
Allergies/asthma
Excess sexual desire
Heaviness anywhere in the
body Energy on a scale of 1-10
(1, low 10, high)
Hard to get up in the morning
Muscles feel tired often
Edema(swelling)
Hands Feet
Easily bruising & bleeding
Bad breath
Nausea/vomiting
Difficulty digesting fatty foods
Gas/belching
Hemorrhoids
Diarrhea
Abdominal pain
Indigestion/heartburn
Over thinking
Tendency to gain weight
Brain foggy
Do you crave "sweet"?
MEDICATIONS - Please list all prescription medications you use. Include those which you may only use
ocassionally. Remember inhalers, eye drops, nose sprays, and topical creams. Note: If you need inhalers,
eye drops, nose sprays, and topical creams. NOTE: If you need more space, use page 7 under "Notes/Anything Else".
PRESCRIPTION NAME PURPOSE
HOW LONG ON
MEDICATION DOSE
TAKEN HOW
OFTEN LAST DOSE
TPA WELLNESS * 43422 Business Park Dr., Temecula CA 92590 * (951) 693-5555 Page 4
White Yellow Green
White Yellow Green

On a scale of 1-10, rate your commitment to get rid of the problem(s) and feel better.
Have you had acupuncture treatments before?
If yes, who treated you and where?
Any concerns or fears about the needles?
What are your goals of your acupuncture visits?
1)
2)
3)
YOU FATHER MOTHER SPOUSE
AGE
AIDS/HIV
Alcohol Abuse
Anxiety
Anorexia/Bulimia
Arthritis
Asthritis
Asthma/Hay Fever/Allegy
Back Trouble
Bursitis
Cancer
Constipation
Depression
Diabetes
Digestive Trouble
Headaches
Heart Trouble
Liver Trouble
Migraine
Neck Pain
Thyroid Disorder
Suicidal Tendencies
Tobacco
Weight Problem
Other Emotional Problems
Other
If any of the above family members are deceased, please list their age at death and cause.
SURGERIES: (Including removal of wisdom teeth)
Date or Age Type of Surgery Location of Scar
PERSONAL MEDICAL & FAMILY HEALTH HISTORY
Please indicate which of the below health issues you or your family members are currently experiencing or experienced in the past. If experiencing currently, Place a C in the square, If experienced in the past, Place a P in the square. Leave blank those that
do not apply.
BROTHER(S) SISTER(S) CHILDREN
If yes, what?
TPA WELLNESS * 43422 Business Park Dr., Temecula CA 92590 * (951) 693-5555 Page 5

Hysterectomy - Ovaries removed? Yes No
Could you be pregnant now? Yes No
Number of: Pregnancies BirthsMiscarriages Abortions
Birth Control:None Spermicides IUDBirth Control Pills Barriers
Premenstrual syndrome (mark all that apply)Fluid retention Cravings Tender/weepyFluctuating emotions Fatigue IrritabilityTenderness in breasts Depression Loose stool
Yes NoNumber of days from one menstrual cycle to the next?
Moderate Light
Post-menopausal bleeding When did your last period start?Number of days bleeding lastsDescribe menstrual flow:
Color of menstrual flow: Dark Red
NoneHeavy
Bright Red Bloody Mucous
Cramping (Mark all that apply)Mild During period Do you feel ovulation?Moderate After period Bleeding between periods Severe Cramping in low back Infertility issuesBefore period In groin area Do you use pain medication?
What kind?
Clotting (mark all that apply) Size of clotts: Bright color Brown / Grainy DimeStringy Dark in color Nickel
LargerVaginal Discharge
White discharge Red & white dischargeYellow discharge yellow discharge with pussGreenish Watery/thick discharge
fishy smell/leathery smellDo you experience:
Vaginal dryness Use lubricants during intercourse?
Mark all that apply:Pelvic inflammatory disease Ovarian CystsSTD's Hot FlashesEndometriosis Breast CystsMastitis Yeast infection/Vaginitis/Other discharge
Impotence Weak erectionDischarge from penis Prostate problemsTesticular pain or lump infertilityPremature ejaculation Low sex driveSTD's Do you wake with morning erection?
WOMEN ONLY
Menstruation and Menstrual Cycle
MEN ONLY
TPA WELLNESS * 43422 Business Park Dr., Temecula CA 92590 * (951) 693-5555 Page 6
Fresh Red Purple/Blackish color
If yes, products used:
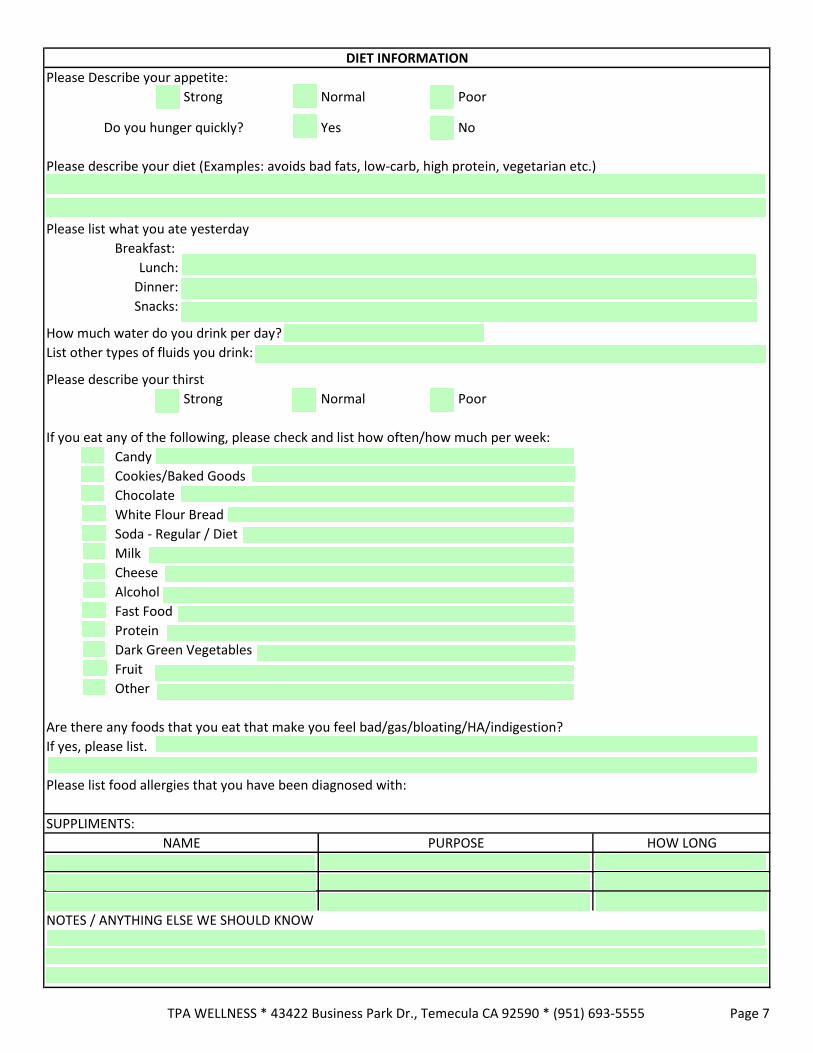
Please Describe your appetite:
Strong Normal Poor
Do you hunger quickly? Yes No
Please describe your diet (Examples: avoids bad fats, low-carb, high protein, vegetarian etc.)
Please list what you ate yesterday
Breakfast:
Lunch:
Dinner:
Snacks:
How much water do you drink per day?
List other types of fluids you drink:
Please describe your thirst
Strong Normal Poor
If you eat any of the following, please check and list how often/how much per week:
Candy
Cookies/Baked Goods
Chocolate
White Flour Bread
Soda - Regular / Diet
Milk
Cheese
Alcohol
Fast Food
Protein
Dark Green Vegetables
Fruit
Other
Are there any foods that you eat that make you feel bad/gas/bloating/HA/indigestion?
If yes, please list.
Please list food allergies that you have been diagnosed with:
SUPPLIMENTS:
NOTES / ANYTHING ELSE WE SHOULD KNOW
NAME PURPOSE HOW LONG
DIET INFORMATION
TPA WELLNESS * 43422 Business Park Dr., Temecula CA 92590 * (951) 693-5555 Page 7