Embed Size (px)
Citation preview

Contents
Summary
Review Article
Sports Medicine 10 (6): 355-364. 1990 0112-1642/90/0012-0355/$05.00/0 © Adis International Limited All rights reserved. SPORT2332
Weight lifting Training in Cardiac Patients Considerations
Robert S. McKelvie and Neil McCartney Departments of Medicine and Physical Education, McMaster University. Hamilton, Ontario, Canada
Summary .. ..... ........... ..................... ......................................... ..... ..... .. ... ............... .......... ..... ...... 355 I. The Physiological Response to Isometric (Static) Exercise .................. .. ......... .. ............... 356 2. The Physiological Response to Static-Dynamic Exercise ................................................. 357 3. Safety of Weightlifting in Patients with Coronary Artery Disease ........ .......................... 357
3.1 Acute Response to Weightlifting ..... ...................... ... ... ...................... .. ..... ...... .............. 358 3.2 Long Term Effects of Weightlifting Training .............................. .. .................. ..... ...... 360
4. Benefits of Weightlifting Training in Patients with Coronary Artery Disease ............... 360 4.1 Effects on Muscular Strength, Endurance, and Maximum Dynamic Power
Output ...................................................................................................... ....................... 360 4.2 Effects on the Circulatory Response During Lifting ............................ .. .................... 361 4.3 Effects on Risk Factors for Coronary Artery Disease ... ... .......................... ................ 361
5. Conclusions ................... ... .... ................................... .... ...................... ..... ... ....... ..... ... ... ......... 362 6. Recommendations ............. ........... .. ......... .. ...................... ...... ..... ..... ............. ... .................... 363
Cardiovascular disease is the leading cause of morbidity and mortality in most of the industrialised nations in the world. Many treatment strategies are used for patients with coronary artery disease. One of these strategies is the use of cardiac exercise rehabilitation.
The traditional approach to cardiac exercise rehabilitation has been the training of large muscle groups using aerobic activities such as cycling or walking. These types of activities have been demonstrated to improve maximal exercise performance and endurance. However, although aerobic performance is improved it does not address another very important component of exercise rehabilitation - namely muscular strength.
Weightlifting training has been demonstrated to improve muscular strength in healthy individuals. Until recently this form of exercise training of patients with cardiac disease has been avoided due to the haemodynamic response observed during isometric (static) exercise.
Weightlifting has recently been demonstrated not to be a pure isometric exercise and a different haemodynamic response has been found even in patients with cardiac disease. For this reason studies of weightlifting training have been performed in selected groups of patients with coronary artery disease. The results of these studies in this limited group of patients have demonstrated the activity is safe and beneficial in terms of improving the patient's functional capacity. Weightlifting training may also favourably affect the risk factors for coronary artery disease.
Based on studies reviewed in this paper, recommendations can be made for the weight-

356 Sports Medicine 10 (6) 1990
lifting training of patients with coronary artery disease. These include restriction to patients who are asymptomatic or only mildly symptomatic; initiation of training only after a period of aerobic training; the use of single limb activities; a maximum intensity no greater than 60% of I repetition maximum; patients train at their own rate; initially performed in a medically supervised programme; periodic reassessment of the exercise prescription; and patients should record their heart rate and response to exercise.
Cardiovascular disease is the leading cause of morbidity and mortality in most of the industrialised nations in the world with billions of health care dollars spent each year in the assessment and treatment of patients with coronary artery disease (CAD). As these patients are often young and active in the work force further money is spent on disability programmes due to time lost from their employment.
Cardiac exercise rehabilitation has become an accepted form of therapy for patients with CAD (O'Connor et al. 1989). The goals of a rehabilitation programme are to improve the physical fitness and psychological well-being of the patients. Recent studies that used meta-analysis to examine the trials of cardiac exercise rehabilitation studies have found that a further benefit may be a reduction in mortality (O'Connor et al. 1989; Oldridge et al. 1988).
The traditional approach to cardiac exercise rehabilitation has been to involve large muscle groups in aerobic activities such as walking and stationary cycling. Training effects for these activities have been well documented and are potentially beneficial for patients with CAD (Clausen et al. 1973; Clausen & Trap-Jensen 1980; Detry et al. 1971; Frick & Katila 1968; Hagberg et al. 1983). The results often include an increase in maximal oxygen uptake (V02max), an increase in exercise tolerance, a reduction in myocardial oxygen demand (MV02) at submaximal loads and an increase in the intensity of exercise needed to precipitate angina pectoris.
Although aerobic training improves V02max, endurance and possibly reduces myocardial ischaemia, it does not address another very important component of rehabilitation - namely muscular strength. It can be argued that most activities of
daily living involve tasks which require considerable muscular strength such as lifting, carrying loads, and stair climbing but which do not overly tax the oxygen transport system. Recent studies have demonstrated that a decrease in muscular strength may be quite common among cardiac patients (McCartney et al. 1989a; Oldridge et al. 1989). Weightlifting training is an activity which can be used to improve the component of muscular strength (Gettman et al. 1978; Harris & Holly 1987), but despite this weightlifting training has not been generally used in cardiac exercise rehabilitation programmes.
The reluctance to use weightlifting training has probably been based on the acute circulatory response to static (e.g. isometric handgrip) work (Hanson & Nagle 1987). However, more recent studies have demonstrated a somewhat different circulatory response to weightlifting, and that this activity appears to be appropriate in patients with uncomplicated CAD (Haslam et al. 1988b; Kelemen et al. 1986).
This paper reviews the development of weightlifting training in CAD patients. Recommendations are provided to guide the prescription of weightlifting training for patients with CAD.
1. The Physiological Response to Isometric (Static) Exercise
The physiological response to static (isometric) exercise in normal subjects differs from the response to dynamic exercise (Asmussen 1981; Bezucha et al. 1982). Static exercise invokes an increase in cardiac output, heart rate and mean arterial blood pressure (Asmussen 1981; Bezucha et al. 1982; Hanson & Nagle 1987), with no change or a decrease in stroke volume and no change or

Weightlifting in Cardiac Patients
a slight increase in systemic vascular resistance (Asmussen 1981; Bezucha et al. 1982; Hanson & Nagle 1987; Helfant et al. 1971). An increase in stroke work without any significant change in left ventricular end diastolic pressure occurs, which suggests an increase in myocardial contractility (Grossman et al. 1973; Helfant et al. 1971). On the other hand, left ventricular end diastolic and end systolic volumes either increase or do not change during isometric exercise (Longhurst et al. 1981; Perez-Gonzales et al. 1981; Sagiv et al. 1985) suggesting a pressure load on the heart (Hanson & Nagle 1987; Mitchell & Wildenthal 1974). These physiological changes observed in healthy individuals during isometric exercise have been viewed as potentially detrimental to patients with CAD.
Isometric exercise in patients with CAD produces blood pressure and heart rate responses similar to those observed in healthy individuals, but the cardiac output is only slightly increased or unchanged and there is an associated increase in systemic vascular resistance (Hanson & Nagle 1987; Helfant et al. 1971). Furthermore, left ventricular volumes increase and stroke work decreases, reflecting an abnormal response of the left ventricle to this type of work (Grossman et al. 1973; Helfant et al. 1971). Based on these findings there was a concern that cardiac patients, especially those with more severe left ventricular dysfunction, would be at increased risk for developing pulmonary congestion, ventricular dysrhythmias and myocardial ischaemia during static exercise (Kivowitz et al. 1971; Mitchell & Wildenthal 1974; Paulsen et al. 1979; Vecht et al. 1978).
However, DeBusk et al. (1978) have demonstrated that the concerns about the circulatory response to static exercise in patients with CAD may not be warranted. In a study of patients 6 to 7 weeks after myocardial infarction which compared dynamic exercise (leg cycle ergometry 450 kpm, increasing by 150 kpm every 3 minutes to exhaustion) with static exercise (handgrip contraction or forearm flexion at 25% and 50% of maximum voluntary contraction) they found that ischaemic ST segment depression and significant ventricular ar-
357
rhythmias were more frequent in dynamic exercise (DeBusk et al. 1978).
2. The Physiological Response to Static-Dynamic Exercise
Most of the activities patients perform throughout the day are a combination of static and dynamic exercise. A study in healthy young male subjects has demonstrated that in combined staticdynamic exercise the circulatory response to static exercise is diminished as the component of dynamic activity increases (Kilborn & Persson 1981). This indicates the circulatory response to combined static-dynamic exercise is different than the response to static exercise alone. The response to static dynamic exercise has also been assessed in patients with CAD. These studies have not demonstrated an increased frequency of anginal symptoms, ST segment depression or ventricular dysrhythmias during static-dynamic exercise (Kerber et al. 1975; Sheldhal et al. 1983, 1985; Wilke et al. 1985,1989). The results of these studies would suggest the patient's circulatory response to static-dynamic exercise is acceptable and there is not an increase in the frequency of myocardial ischaemia or ventricular dysrhythmias. These findings have been substantiated by recent work which examined the safety of weightlifting in patients with CAD.
3. Safety of Weightlifting in Patients with Coronary Artery Disease
Circuit weightlifting training may be defined as a series of resistance exercises (usually 10 or less) that are performed in a fixed sequence with little rest between exercise stations (15 to 60 seconds). Each exercise is performed at the same relative intensity (usually 40 to 60% of maximum voluntary contraction) and for 10 to 15 repetitions. Once a full circuit of exercises has been completed the subject performs an additional I to 2 circuits. The total workout time for this type of training usually ranges from 20 to 30 minutes.
Weightlifting is a form of static-dynamic exercise and recent studies have not demonstrated an

358
adverse response to this type of activity in patients with CAD (Kerber et al. 1975; Sheldhal et al. 1983, 1985; Wilke et al. 1985, 1989). Nevertheless, formal weightlifting to failure may be contraindicated; in a recent study by MacDougall et al. (1985) healthy male bodybuilders performing double-leg presses and single-arm curls at 95% of I repetition maximum (IRM) to failure generated a mean arterial blood pressure of 330/250mm Hg and 240/ 160mm Hg, respectively.
3.1 Acute Response to Weightlifting
The circulatory response and safety during weightlifting in patients with CAD has been examined by a number of investigators (Butler et al. 1987; Crozier-Ghilarducci et al. 1989; Featherston et al. 1987; Haslam et al. 1988b; Keleman et al. 1986; Stewart et al. 1988; Vander et al. 1986). Weightlifting does not appear to cause an increase in the frequency of anginal symptoms or signs of ischaemia on the electrocardiogram.
Vander et al. (1986) compared the electrocardiographic response and patient symptoms during weightlifting to those found during graded exercise testing. Despite the presence of ischaemic changes during exercise testing, there were no significant arrhythmias, ST segment changes or symptoms during the weightlifting. Similar results were found in a recent study by Haslam et al. (l988b).
Butler et al. (1987) used echocardiography to compare changes in wall motion between weightlifting and traditional aerobic exercise. The echocardiographic studies were begun within 1 minute after exercise and were completed within 5 minutes. With aerobic exercise a worsening of wall motion occurred in 5 of 61 left ventricular segments, while the motion in only 1 segment was found to deteriorate following weightlifting. These findings suggest the load on the cardiovascular system during weightlifting is no greater than occurs during aerobic exercise.
Blood pressure and heart rate responses have been examined in relation to weightlifting. The studies measured blood pressure, usually immediately following exercise noninvasively, using a
Sports Medicine /0 (6) 1990
Single arm curl 200 20% lRM 180 160 ___
Oi 140 J: E 120 .s 100 A
40% 1RM ----~ 80 ~--------------r-----~~~-----'" 60% lRM 80% lRM ~ 200 a.
180 ~ ~ 160 ..-r-III
140 120 .&
100~ 80 L-____________ ~ ______________ _
200
180 160
Oi 140 J:
Single leg press
20% lRM
E 120 .s 100 A
40% lRM ----------~ .... -----~ 80 I--------r------:=:--=:-:-----
'" 60% lRM 80% lRM ~ 200 ~
180 -~,---g 160 ....--ffi
140 120 A .& A ____
100 ~ .... _----- r-----80 L-_________ ~ ____________ ___
Double leg press 200 20% lRM 180
160 -~ 140 E 120 .s 100 A
~ 80 -------~ 600/0 1RM ~ 200
"'0: 180 ------ffi 160
140
40% lRM ---
120 .&
100A~~ 80~Trrn~~rrnn~~TMnn~TTTrnn~
R 2 4 6 8 10 12 14 E R 2 4 6 8 10 12 14 E
Repetitions
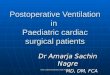
Fig. 1. Mean peak systolic, diastolic and average resting (f» and exercise (A) arterial pressure responses to single-arm curl, single-leg press and double-leg press exercise at the relative loads as functions of the number of repetitions (reprinted with permission from Haslam et al. I 988b).

Weightlifting in Cardiac Patients
sphygmomanometer, and demonstrated similar systolic pressure and rate pressure product (RPP) responses during weightlifting or aerobic exercise (Butler et al. 1987; Crozier-Ghilarducci et al. 1989; Keleman et al. 1986; Vander et al. 1986).
Featherston et al. (1987) found the diastolic blood pressure response to weightlifting (113 mm Hg) was greater than for aerobic exercise (79mm Hg); the systolic blood pressure response was similar for both types of exertion, but the heart rate response was lower during weightlifting with an accompanying lower RPP. It can be argued that lower RPP reflects a lower myocardial oxygen requirement during weightlifting. Furthermore, as coronary blood flow occurs mainly during diastole, the slower heart rate (longer diastolic period) and higher diastolic pressure (increased coronary perfusion pressure) would potentially improve myocardial perfusion as long as left ventricular end diastolic pressure did not increase in parallel. Studies to investigate this possibility are currently under way in our laboratory.
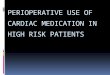
In a recent study (Haslam et al. 1988b), we measured the blood pressure directly using an intraarterial catheter in the brachial artery. During weightlifting, increases occurred in the systolic blood pressure, RPP and to a lesser extent the diastolic blood pressure (fig. I). These increases were greater than those found in studies where blood pressure was measured with a sphygmomanometer (Butler et al. 1987; Crozier-Ghilarducci et al. 1989; Kelemen et al. 1986; Vander et al. 1986). However, except for single-leg press at 80% I RM and doubleleg press at 60 and 80% of I RM, the RPP was the same during weightlifting as that observed during aerobic exercise at less than 85% of V02max (fig. 2). It was concluded that the responses were within a clinically acceptable range except perhaps for single-leg and double-leg press activities at high intensities, where some caution may be advised in prescribing these exercises for patients with CAD.
We recently performed a study (Wiecek et al. 1990) comparing blood pressure measurements made directly (intra-arterial catheter) and indirectly (sphygmomanometer) during weightlifting. The results demonstrated that compared to direct
359
250 1~0%._._._._._._._._._ • .lJ.
240
230 0 0 85% U 220 :l "0 e 210 a. e 200 0 :l
'" 190 '" Q) 0 a. 180 h.
cD OJ 60% a: 170 ------0------
160 0
150
140 ~
20 40 60 80
Relative load (% 1 RM)
Fig. 2. Mean maximum rate-pressure product (mean maximum peak heart rate X mean maximum peak systolic pressure/IOO) responses to single-arm curl (Ll), single- (0) and double-leg (0) press exercise as functions of relative work intensity [plotted as % of I repetition maximum (I RM)]. The mean rate-pressure product values recorded in progressive incremental cycle ergometer testing at 60%, 85% and 100% of the maximum achieved work are also indicated (reprinted with permission from Haslam et at. 1988b).
blood pressure measurements the indirect measurements consistently underestimated the systolic blood pressure response during weightlifting by 14 to 20%. These results also demonstrated that the blood pressure d(lcreases very quickly following termination of weightlifting, making it difficult to draw any conclusions about the pressure changes during exercise from postexercise assessment (fig. 3). Furthermore, we measured the intra-arterial pressure directly during a single-arm military press and found the systolic pressure response (170 ± 14.6mm Hg) was much greater than previously reported by Crozier-Ghilarducci et al. (1989) when using indirect measurement of blood pressure during this exercise.
In the research setting it would appear to be important to make direct measurements of arterial pressure when assessing the circulatory response to weightlifting, otherwise important changes in the

360
1 second-
Rest Exercise
t Immediately after
Sports Medicine 10 (6) 1990
25-30 sec after
Fig. 3. Tracing of a direct arterial blood pressure measurement using an intra-arterial catheter in the brachial artery while performing a I-arm military press at 60% of the I RM. The arrow represents the end of exercise, after which there is a rapid decline in the systolic and diastolic blood pressure (unpublished data).
blood pressure will go unobserved. This could potentially lead to the prescribing of certain weightlifting activities that may be unsafe for patients with CAD.
3.2 Long Term Effects of Weightlifting Training
Studies have examined whether adverse effects occur during a prescribed weightlifting training programme. The longest follow-up period has been by Stewart et al. (1988), in which 17 patients participated in circuit weightlifting for 3 years. Compared to the group of aerobically trained patients there was no difference in morbidity. The other studies that have examined circuit weightlifting training followed the patients during a lO-week training programme and did not find an increased incidence of cardiovascular problems (CrozierGhilarducci et at. 1989; Haslam et al. I 988a; Kelemen et at. 1986). In all of these studies patients were involved in aerobic exercise programmes for at least 3 months before institution of the weightlifting training. Furthermore, the total number of patients that have been formally studied is small and due to the study entrance criteria, they have all had stable CAD with well maintained left ventricular function.
Therefore it would appear that weightlifting training is safe in a well selected group of patients with stable CAD and reasonably good left ventricular function. There have been no studies performed to determine if weight lifting training is safe in patients with more severe symptoms or signs of
CAD. Therefore at the present time it would be advisable to limit weightlifting training to patients who have minimal symptoms of angina and reasonably well maintained left ventricular function; and who have successfully participated in a cardiac exercise rehabilitation programme for at least 3 months.
4. Benefits of Weightlifting Training in Patients with Coronary Artery Disease 4.1 Effects on Muscular Strength, Endurance, and Maximum Dynamic Power Output
Resistance training in healthy individuals has been demonstrated to improve strength, change body composition and produce a small increase in aerobic capacity (Gettman et at. 1978). These changes would be expected to occur in patients with CAD because the method of resistance training in patients with CAD is similar to that used in healthy individuals.
Kelemen et at. (1986) weight-trained patients who had trained aerobically for 3 months in a cardiac exercise rehabilitation programme. The control group continued their aerobic training and the treatment group had weightlifting training substituted for a volleyball programme for a lO-week period. Patients who performed weightlifting training had an average increase in strength of 24% and an increase in maximum treadmill time from 619 to 694 seconds, whereas there were no changes in the control group.
Haslam et al. (1988a) examined the effects of weightlifting training on strength and aerobic per-

Weightlifting in Cardiac Patients
formance in patients with cardiac disease. All the patients in this study had been aerobically trained for 3 months prior to the initiation of weightlifting training. The control group continued aerobic training and the treatment group performed both aerobic and weightlifting training, for 10 weeks with both groups performing the same amount of total exercise. After training, strength was significantly increased only in the treatment group and, in addition, the number of times the initial I RM could be performed increased to 14 in the weight-trained patients, but only to 4 in the control group. Following training a significant 15% improvement in maximal power output in cycle ergometer performance occurred in the treatment group while no change was observed in the control group. Symptom-limited endurance while cycling at 80% of the initial maximum power output increased in the treatment group following training, with the time to reach a Borg rating of perceived exertion scale of 7 (very severe) increasing from 541 seconds before training to 1128 seconds after training. Endurance for the control group increased from 604 seconds before training to 672 seconds after training.
Crozier-Ghilarducci et al. (1989) also examined the effects of a IO-week weightlifting training programme on patients with CAD and found a significant increase in strength. However, since aerobic capacity was not assessed and they did not include a control group in the study, it is difficult to assess the overall impact of the weightlifting training.
4.2 Effects on the Circulatory Response During Lifting
Weightlifting training may also produce a reduction in blood pressure at rest and during exercise. Stone et al. (1982) found a reduction in resting systolic blood pressure following 8 weeks of weightlifting training in 9 college-aged males, while Hurley et al. (1988) observed a significant reduction in resting supine diastolic blood pressure after 16 weeks of weightlifting training, but no changes
361
were observed in resting supine systolic blood pressure or in standing blood pressure.
We have recently examined the effects of weightlifting training on the circulatory response to weightlifting in a healthy group of males aged 60 to 70 years (McCartney et al. 1989b). In this study the subjects were assessed before and after 12 weeks of progressive weightlifting training. Following training the systolic pressure, diastolic pressure, heart rate and RPP responses were significantly lower during the lifting of identical submaximal loads. This response has not been examined in patients with CAD and studies need to be designed to assess the circulatory response in patients following training. However, if the response is similar to that observed in healthy males the potential exists for patients, following training, to perform strength-related activities of daily living with a lower blood pressure and RPP. This would mean patients may often perform ADL much below their anginal threshold and therefore have fewer episodes of angina throughout the day and a better quality of life. Furthermore, the reduced circulatory response during ADL may mean patients are performing these activities with greater safety. At the present time these are reasonable hypotheses but remain to be proven through further research studies.
4.3 Effects on Risk Factors for Coronary Artery Disease
The effect of weightlifting training on altering some of the risk factors for CAD has also been examined in a limited number of studies. Stone et al. (1982) found 12 weeks of weightlifting training was associated with reductions in total cholesterol to high density lipoprotein cholesterol (HDL-C) ratio and low density lipoprotein cholesterol (LDLC) concentrations. Significant decreases in body fat were also observed therefore it was unclear whether the reductions were related to the training or decrease in the body fat.
Hurley et al. (1988) have also examined the effects of weight lifting training on lipid levels. In this study there was an increase in HDL-C, and de-

362
creases in LDL-C and total cholesterol/HDL-C. These changes were observed despite no change in the percentage of body fat and this suggests weightlifting training acts independently to alter blood lipid levels. Several other studies i~ healthy subjects have examined the effects of weightlifting training on lipid levels and most have found an increase in HDL-C and a decrease in LDL-C (Fripp & Hodgson 1987; Goldberg et al. 1984; Johnson et al. 1982; Kokkinos et al. 1988, 1989; Ulrich et al. 1987; Weltman et al. 1987). However, because of limitations in the design of these studies, further work is needed to determine whether weightlifting training alters blood lipid levels.
Although weightlifting training does not appear to alter glucose tolerance it does alter the insulin response to glucose (Hurley et al. 1988; Miller et al. 1984). Lower insulin levels are observed for any given blood glucose level (Hurley et al. 1988) and this may be protective against atherosclerosis (Stout 1985).
The studies examining the effects on risk factors have all been performed on healthy individuals. Further studies need to be performed in patients with CAD to determine if there is a beneficial effect on risk factors for CAD in this group.
5. Conclusions
Weightlifting is not a pure static exercise, but more a static-dynamic type of exercise. The circulatory response to moderate weightlifting in patients with CAD is not like that found with pure static exercise but is more similar to the 'volume overload' response found with dynamic (aerobic) activities.
Studies of weightlifting training in patients with CAD have demonstrated that significant increases in muscular strength occur in these patients. Furthermore, a significant increase in maximal functional capacity is observed, indicating that weightlifting training has a significant beneficial effect on the aerobic capacity of the patient with CAD. Many ADL consist of a significant resistance component and the improvement in strength and aerobic ca-
Sports Medicine 10 (6) 1990
pacity following weightlifting training should allow patients to perform these activities with greater ease.
Data from healthy elderly subjects indicate the blood pressure and RPP responses are reduced while lifting any given submaximal load following weightlifting training. This would mean that following weightlifting training in patients with CAD
they would be performing ADL at a lower blood pressure and RPP, thus they would be performing these activities well below their anginal threshold. Further studies need to be performed to substantiate these hypotheses of an improved circulatory response, and improved quality of life during ADL.
Studies from healthy subjects have suggested that weightlifting training may beneficially alter certain risk factors for CAD. There are only a limited amount of data presently available to support this theory in healthy individuals. There have been no studies in cardiac patients to determine whether risk factors are altered with weightlifting training. Therefore much further work needs to be performed to assess the role of weightlifting training in altering risk factors in patients with CAD.
It is important to emphasise that studies examining the effect of weightlifting training have all been performed on patients who were asymptomatic or mildly symptomatic and who had been aerobically trained for at least 3 months prior to beginning weightlifting training. Furthermore, no studies have examined if the circulatory response to ADL is altered by weightlifting training or if anginal symptoms or fatigue are reduced during ADL following weightlifting training. We suggest that further studies need to be performed before weightlifting training can be advocated for patients with more severe symptoms of angina. The circulatory response during strength-related ADL, and the ease with which these activities are performed following weightlifting training needs to be assessed to determine if a beneficial response occurs. Finally, the effect on left ventricular function during weightlifting and the response to weightlifting training must be assessed in patients with CAD of varying severity.

Weightlifting in Cardiac Patients
6. Recommendations
The studies reviewed in this paper allows the formulation of recommendations for weightIifting training of patients with CAD:
I. Restrict weightlifting training to patients who are asymptomatic or are only mildly symptomatic (less than or equal to New York Heart Association Functional Class I).
2. WeightIifting training should only be initiated after a period (3 months) of aerobic exercise training.
3. Single limb activities should be performed as double limb activities may produce too great an increase in blood pressure and RPP responses.
4. Exercises should be limited to 60% of 1 RM as intensities greater than this for some exercises produce unacceptable increases in blood pressure and RPP. Furthermore, training at this intensity will produce the previously discussed beneficial changes.
5. Patients should proceed through a weightlifting training circuit at their own pace, and should not be instructed to take a fixed amount of rest after each set.
6. WeightIifting training should be performed in a medically supervised programme. Once proper techniques and the patient's response to the training have been monitored (6 months) the weightlifting training could be performed in an unsupervised setting.
7. The weightlifting training exercise prescription should be initially reassessed every 4 weeks, then after 6 months reassessment could be performed every 6 months.
8. Patients should record their response (heart rate and symptoms) to the exercise following each set just as they would during aerobic training activities.
Acknowledgements
The secretarial assistance of Christine StefTann in the preparation of this manuscript was greatly appreciated. Dr McKelvie is a Career Scientist ofthe Ontario Ministry of Health.
363
References
Asmussen E. Similarities and dissimilarities between static and dynamic exercise. Circulation Research 48 (Suppl. I): 1-3-1-10. 1981
Bezucha GR, Lenser MC, Hanson PG, Nagle FJ. Comparison of hemodynamic responses to static and dynamic exercise. Journal of Applied Physiology 53: 1589-1593, 1982
Butler RM, Beierwaltes WH, Rogers FJ. The cardiovascular response to circuit weight training in patients with cardiac disease. Journal of Cardiopulmonary Rehabilitation 7: 402-409, 1987
Clausen JP, Trap-Jensen J. Effects of training on the distribution of cardiac output in patients with coronary artery disease. Circulation 42: 611, 1970
Clausen JP, Klausen K. Rasmussen B. Trap-Jensen J. Central and peripheral circulatory changes after training of the arms or legs. American Journal of Physiology 225: 675-682. 1973
Clausen JP. Trap-Jensen J. Effects of training on the distribution of cardiac output in patients with coronary artery disease; Circulation 42: 611. 1970
Crozier-Ghilarducci LE. Holly RG. Amsterdam EA. Effects of high resistance training in coronary artery disease. American Journal of Cardiology 64: 866-870. 1989 culation 58: 368-375. 1978
Detry JRM, Rousseau M, Vandenbroucke G, Kusumi F, Brasseur LA, et al. Increased arteriovenous oxygen difference after physical training in coronary heart disease. Circulation 44: \09-118, 1971
Featherston JF, Holly RG, Amsterdam EA. Physiological responses to weight lifting in cardiac patients. Medicine and Science in Sports and Exercise 19: S93, 1987
Frick MH, Katila M. Hemodynamic consequences of physical training after myocardial infarction. Circulation 37: 192-202, 1968
Fripp RR. Hodgson JL. Effect of resistive training on plasma lipid and lipoprotein levels in male adolescents. Journal of Pediatrics Ill: 926-931, 1987
Gettman LR. Ayres JJ, Pollock ML, Jackson A. The effect of circuit weight training on strength cardiorespiratory function and body composition of adult men. Medicine and Science in Sports and Exercise \0: 171-176, 1978
Goldberg LE, Elliot DL, Schulz RW. Kloster FE. Changes in lipid and lipoprotein levels after weight-training. Journal of the American Medical Association 252: 504-506, 1984
Grossman W, Mclaurin LP, Saltz SB, Paraskos JA, Dalen JE, et al. Changes in the inotropic state of the left ventricle during isometric exercise. British Heart Journal 35: 697-704. 1973
Hagberg JM, Ehsani AA, Holloszy JO. Effect of 12 months of intense exercise training on stroke volume in patients with coronary artery disease. Circulation 67: 1194-1199, 1983
Hanson P, Nagle F. Isometric exercise: cardiovascular responses in normal and cardiac populations. Cardiology Clinics 5: 157-170, 1987
Harris KA. Holly RG. Physiological response to circuit weight training in borderline hypertensive subjects. Medicine and Science in Sports and Exercise 19: 246-252, 1987
Haslam D, McCartney N, McKelvie RS, Sale DG, Jones NL. Weight training in cardiac patients. Medicine and Science in Sports and Exercise 20: S90, 1988a
Haslam RS, McCartney N, McKelvie RS, MacDougall JD. Direct measurements of arterial blood pressure during formal weightlifting in cardiac patients. Journal of Cardiopulmonary Rehabilitation 8: 213-225, 1988b
Helfant RH, De Villa MA, Meister S. Effect of sustained isometric handgrip exercise on left ventricular performance. Circulation 44: 982-993, 1971
Hurley BF, Hagberg JM, Goldberg AP, Seals DR, Ehsani AA, et

364
al. Resistance training can reduce coronary risk factors without altering V02ma. or percent body fat. Medicine and Science in Sports and Exercise 20: 150-154, 1988
Johnson CC, Stone MH, Lopez SA, Hergberg JA, Kilgore TL, et al. Diet and exercise in middle-aged men. Journal of the American Dietetic Association 81: 695-701, 1982
Kelemen MH, Stewart KJ, Gillilan RE, Ewart GK, Valenti SA, et al. Circuit weight training in cardiac patients. Journal of the American College of Cardiology 7: 38-42, 1986
Kerber RE, Miller RA, Najjar SM. Myocardial ischemic effects of isometric dynamic and combined exercise in coronary artery disease. Chest 67: 388-394, 1975
Kilborn A, Persson J. Cardiovascular response to combined dynamic and static exercise. Circulation Research 48: 1-93-1-97, 1981
Kivowitz C, Parmley W, Donoso R, Marcus H, Ganz W. et al. Effects of isometric exercise on cardiac performance: the grip test. Circulation 44: 994-1002, 1971
Kokkinos PF. Hurley BF, Smutok MA, Farner C, Reece C. et al. Lipoprotein-lipid profiles and post-heparin lipase activities are unaltered from strength training. Medicine and Science in Sports and Exercise 21: S 116, 1989
Kokkinos PF. Hurley BF, Vaccaro P, Patterson JC, Gardner LB, et al. Effects of low- and high-repetition resistive training on lipoprotein-lipid profiles. Medicine and Science in Sports and Exercise 20: 50-54, 1988
Longhurst JC, Kelly AR, Gonyeu WJ, Mitchell JH. Chronic training with static and dynamic exercise: cardiovascular adaptation. and response to ex<~rcise. Circulation Research 48 (Suppl. I): 1171-1178,1981
MacDougall JD, Tuxen D, Sale DG, Moroz JR, Sutton JR. Arterial blood pressure response to heavy resistance exercise. Journal of Applied Physiology 58: 785-790, 1985
McCartney N, Martin J, McKelvie RS, MacDougall JD, Sale DG. Weight training induced attenuation of the pressor response to weightlifting in older males. Medicine and Science in Sports and Exercise 21: S2, 1989b
McCartney N, Oldridge NB, Hicks A, Jones NL. Maximal isokinetic cycle ergometry in patients with coronary artery disease. Medicine and Science in Sports and Exercise 21: 313-318. 1989a
Miller WJ, Sherman WM, Ivy JL. Effect of strength training on glucose tolerance and post-glucose insulin response. Medicine and Science in Sports Exercise 16: 539-543, 1984
Mitchell JH, Wildenthal K. Static (isometric) exercise and the heart: physiological and clinical considerations. Annual Review of Medicine 24: 269-381,1974
O'Connor GT, Buring JE, YusufS, Goldhaber SZ, Olmstead EM, et al. An overview of randomized trials of rehabilitation with exercise after myocardial infarction. Circulation 80: 234-244, 1989
Oldridge NB, Guyatt GH, Fischer MS, Rimm AA. Cardiac rehabilitation after myocardial infarction: combined experience of randomized clinical trials. Journal of the American Medical Association 260: 945-950, 1988
Oldridge NB, McCartney N, Hicks A, Jones NL. Improvement in maximal isokinetic cycle ergometry with cardiac rehabili-
Sports Medicine 10 (6) 1990
tation. Medicine and Science in Sports and Exercise 21: 308-312, 1989
Paulsen WJ, Boughner DR, Friesen A, Persaud JA. Ventricular response to isometric and isotonic exercise. Echocardiographic assessment. British Heart Journal 42: 521-527, 1979
Perez-Gonzales JF, Schiller NB, Parmley WW. Direct and noninvasive evaluation of the cardiovascular response to isometric exercise. Circulation Research 48 (Suppl. I): 1138-1148, 1981
Sagiv M, Hanson P, Besozzi M, Nagle F. Left ventricular responses to upright isometric handgrip and deadlift in men with coronary artery disease. American Journal of Cardiology 55: 1298-1302, 1985
Sheldhal LM, Wilke NA, Tristani FE, Kalbfleisch JH. Response of patients after myocardial infarction to carrying a graded series of weight loads. American Journal of Cardiology 52: 698-703, 1983
Sheldhal LM, Wilke NA, Tristani FE, Kalbfleisch JH. Responses to repetitive static-dynamic exercise in patients with coronary artery disease. Journal of Cardiac Rehabilitation 5: 139-145, 1985
Stewart KJ, Mason M, Kelemen MH. Three-year participation in circuit weight training improves muscular strength and selfefficacy in cardiac patients. Journal of Cardiopulmonary Rehabilitation 8: 292-296, 1988
Stone MH, Blessing D, Byrd R, Tew J, Boatwright D. Physiological effects of a short term resistive training program on middle-aged untrained men. National Strength and Conditioning Association Journal (October-November): 16-20, 1982
Stout RW. Overview of the association between insulin and atherosclerosis. Metabolism 34 (Suppl.): 7-12, 1985
Ulrich IH, Reid CM, Yeater RA. Increased HDL-cholesterollevels with a weight-training program. Southern Medical Journal 80: 328-331, 1987
Vander LB, Franklin BA, Wrisley D, Rubenfire M. Acute cardiovascular response to circuit weight training in patients with cardiac disease. Annals of Sports Medicine 2: 165-169,1986
Vecht RJ, Graham GWS, Sever PS. Plasma noradrenaline concentrations during isometric exercise. British Heart Journal 40: 1216-1220, 1978
Weltman A, Janney C, Rians CB, Strand K, Katch Fl. The effects of hydraulic resistance strength training on serum lipid levels in prepubertal boys. American Journal of Diseases in Children 141: 777-780, 1987
Wiecek EM, McCartney N, McKelvie RS. A comparison of direct and indirect measures of arterial pressure during weightlifting in patients with coronary artery disease. American Journal of Cardiology, in press, 1990
Wilke NA, Sheldhal LM, Levandoski SG, Hoffman MD, Tristani FE. Weight carrying versus handgrip exercise testing in men with coronary artery disease. American Journal of Cardiology 64: 736-740. 1989
Wilke NA, Sheldhal LM, Tristani FE, Hughes CV. The safety of static-dynamic effort soon after myocardial infarction. American Heart Journal I 10: 542-545. 1985
Correspondence and reprints: Dr Robert S. McKelvie, Room 518, McMaster Clinic, Hamilton General Hospital, Hamilton, Ontario L8L 2X2, Canada.