Embed Size (px)
Citation preview
Released November 6, 2017 ISSN 0799-3927
NOTIFICATIONS-
All clinical
sites
INVESTIGATION
REPORTS- Detailed Follow
up for all Class One Events
HOSPITAL ACTIVE
SURVEILLANCE-30
sites*. Actively pursued
SENTINEL
REPORT- 79 sites*.
Automatic reporting
*Incidence/Prevalence cannot be calculated
1
Week ending October 21, 2017 Epidemiology Week 42
WEEKLY EPIDEMIOLOGY BULLETIN NATIONAL EPIDEMIOLOGY UNIT, MINISTRY OF HEALTH, JAMAICA
Weekly Spotlight Close to 3 million people access hepatitis C cure
EPI WEEK 42
Hosted by the Government of Brazil, the World Hepatitis Summit 2017 is being co-organized by WHO and the World Hepatitis Alliance. The Summit aims to encourage more countries to take decisive action to tackle hepatitis, which still causes more than 1.3 million deaths every year and affects more than 325 million people.
Many countries are demonstrating strong political leadership, facilitating dramatic price reductions in hepatitis medicines, including through the use of generic medicines—which allow better access for more people within a short time.
In 2016, 1.76 million people were newly treated for hepatitis C , a significant increase on the 1.1 million people who were treated in 2015. The 2.8 million additional people starting lifelong treatment for hepatitis B in 2016 was a marked increase from the 1.7 million people starting it in 2015. But these milestones represent only initial steps – access to treatment must be increased globally if the 80% treatment target is to be reached by 2030.
However, funding remains a major constraint: most countries lack adequate financial resources to fund key hepatitis services.
Downloaded from:http://www.who.int/mediacentre/news/releases/2017/hepatitis-c-
cure/en/
SYNDROMES
PAGE 2
CLASS 1 DISEASES
PAGE 4
INFLUENZA
PAGE 5
DENGUE FEVER
PAGE 6
GASTROENTERITIS
PAGE 7
RESEARCH PAPER
PAGE 8
Released November 6, 2017 ISSN 0799-3927
NOTIFICATIONS-
All clinical
sites
INVESTIGATION
REPORTS- Detailed Follow
up for all Class One Events
HOSPITAL ACTIVE
SURVEILLANCE-30
sites*. Actively pursued
SENTINEL
REPORT- 79 sites*.
Automatic reporting
*Incidence/Prevalence cannot be calculated
2
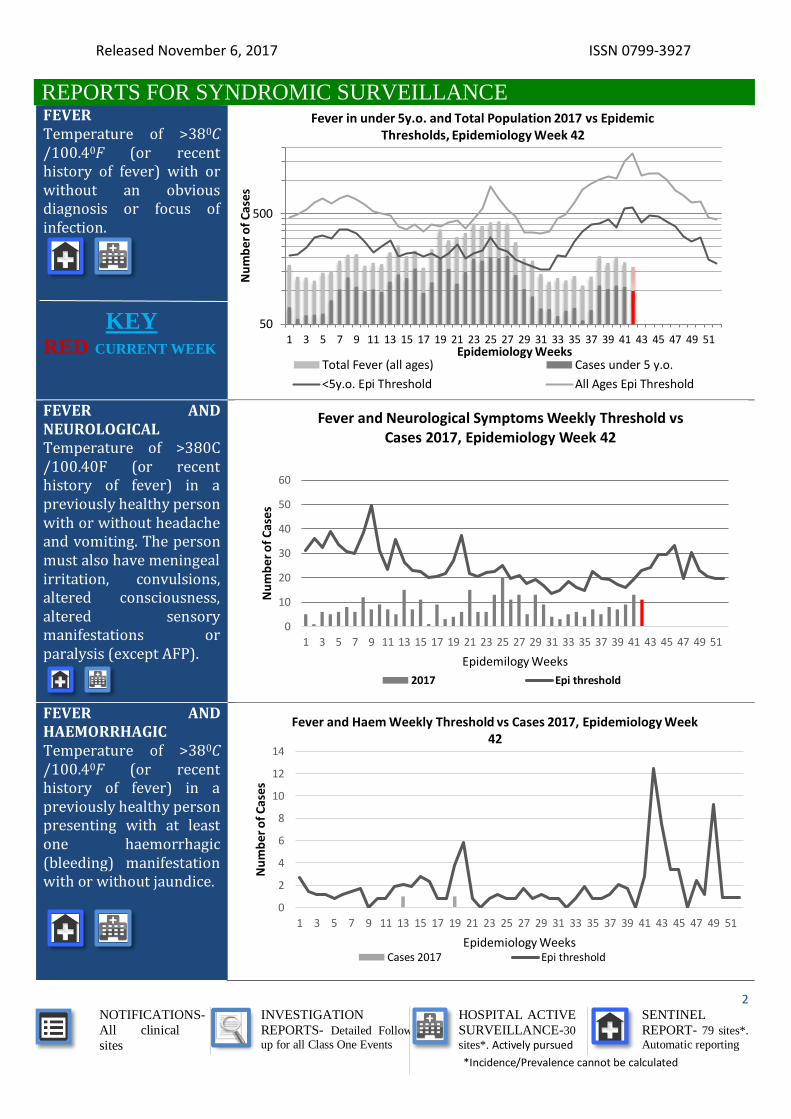
REPORTS FOR SYNDROMIC SURVEILLANCE FEVER Temperature of >380C /100.40F (or recent history of fever) with or without an obvious diagnosis or focus of infection.
KEY RED CURRENT WEEK
FEVER AND NEUROLOGICAL Temperature of >380C /100.40F (or recent history of fever) in a previously healthy person with or without headache and vomiting. The person must also have meningeal irritation, convulsions, altered consciousness, altered sensory manifestations or paralysis (except AFP).
FEVER AND HAEMORRHAGIC Temperature of >380C /100.40F (or recent history of fever) in a previously healthy person presenting with at least one haemorrhagic (bleeding) manifestation with or without jaundice.
50
500
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Nu
mb
er
of
Cas
es
Epidemiology Weeks
Fever in under 5y.o. and Total Population 2017 vs Epidemic Thresholds, Epidemiology Week 42
Total Fever (all ages) Cases under 5 y.o.
<5y.o. Epi Threshold All Ages Epi Threshold
0
10
20
30
40
50
60
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Nu
mb
er o
f C
ases
Epidemilogy Weeks
Fever and Neurological Symptoms Weekly Threshold vs Cases 2017, Epidemiology Week 42
2017 Epi threshold
0
2
4
6
8
10
12
14
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Nu
mb
er
of
Cas
es
Epidemiology Weeks
Fever and Haem Weekly Threshold vs Cases 2017, Epidemiology Week 42
Cases 2017 Epi threshold
Released November 6, 2017 ISSN 0799-3927
NOTIFICATIONS-
All clinical
sites
INVESTIGATION
REPORTS- Detailed Follow
up for all Class One Events
HOSPITAL ACTIVE
SURVEILLANCE-30
sites*. Actively pursued
SENTINEL
REPORT- 79 sites*.
Automatic reporting
*Incidence/Prevalence cannot be calculated
3
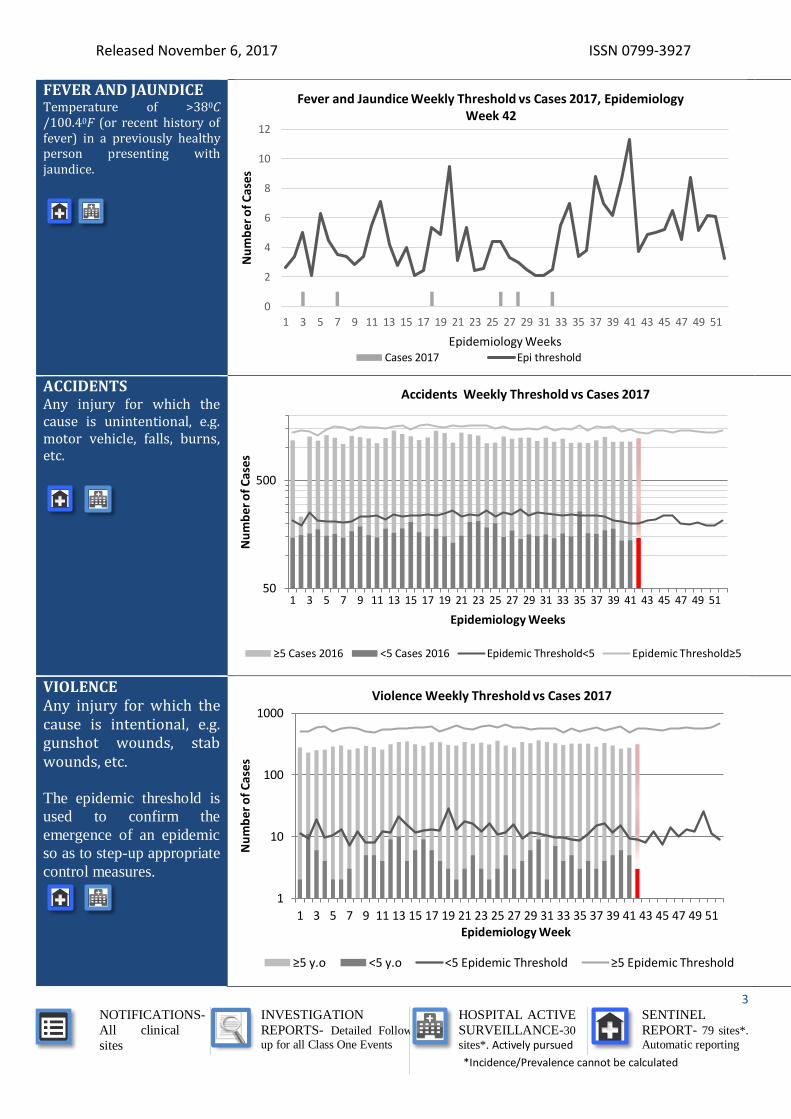
FEVER AND JAUNDICE Temperature of >380C /100.40F (or recent history of fever) in a previously healthy person presenting with jaundice.
ACCIDENTS Any injury for which the cause is unintentional, e.g. motor vehicle, falls, burns, etc.
VIOLENCE Any injury for which the cause is intentional, e.g. gunshot wounds, stab wounds, etc.
The epidemic threshold is
used to confirm the
emergence of an epidemic
so as to step-up appropriate
control measures.
0
2
4
6
8
10
12
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Nu
mb
er
of
Cas
es
Epidemiology Weeks
Fever and Jaundice Weekly Threshold vs Cases 2017, Epidemiology Week 42
Cases 2017 Epi threshold
50
500
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Nu
mb
er o
f C
ases
Epidemiology Weeks
Accidents Weekly Threshold vs Cases 2017
≥5 Cases 2016 <5 Cases 2016 Epidemic Threshold<5 Epidemic Threshold≥5
1
10
100
1000
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Nu
mb
er o
f C
ase
s
Epidemiology Week
Violence Weekly Threshold vs Cases 2017
≥5 y.o <5 y.o <5 Epidemic Threshold ≥5 Epidemic Threshold
Released November 6, 2017 ISSN 0799-3927
NOTIFICATIONS-
All clinical
sites
INVESTIGATION
REPORTS- Detailed Follow
up for all Class One Events
HOSPITAL ACTIVE
SURVEILLANCE-30
sites*. Actively pursued
SENTINEL
REPORT- 79 sites*.
Automatic reporting
*Incidence/Prevalence cannot be calculated
4
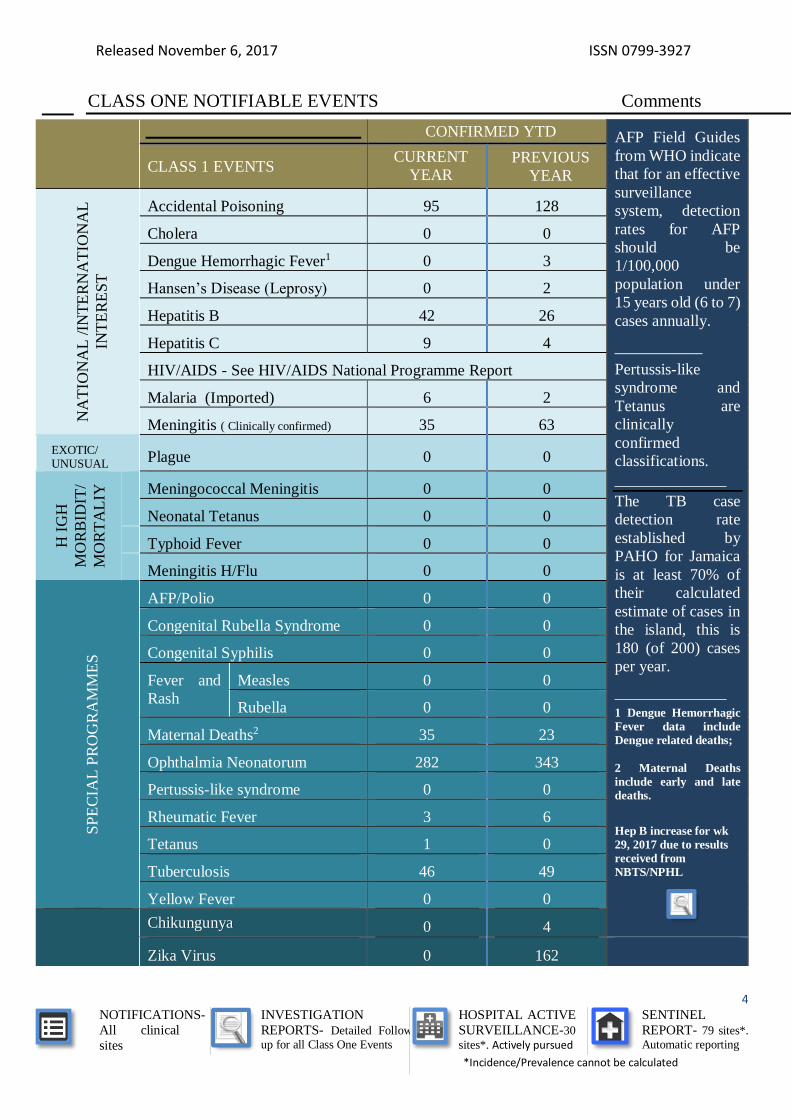
CLASS ONE NOTIFIABLE EVENTS Comments
CONFIRMED YTD AFP Field Guides
from WHO indicate
that for an effective
surveillance
system, detection
rates for AFP
should be
1/100,000
population under
15 years old (6 to 7)
cases annually.
___________
Pertussis-like
syndrome and
Tetanus are
clinically
confirmed
classifications.
______________
The TB case
detection rate
established by
PAHO for Jamaica
is at least 70% of
their calculated
estimate of cases in
the island, this is
180 (of 200) cases
per year.
______________
1 Dengue Hemorrhagic
Fever data include
Dengue related deaths;
2 Maternal Deaths
include early and late
deaths.
Hep B increase for wk
29, 2017 due to results
received from
NBTS/NPHL
CLASS 1 EVENTS CURRENT
YEAR PREVIOUS
YEAR
NA
TIO
NA
L /
INT
ER
NA
TIO
NA
L
INT
ER
ES
T
Accidental Poisoning 95 128
Cholera 0 0
Dengue Hemorrhagic Fever1 0 3
Hansen’s Disease (Leprosy) 0 2
Hepatitis B 42 26
Hepatitis C 9 4
HIV/AIDS - See HIV/AIDS National Programme Report
Malaria (Imported) 6 2
Meningitis ( Clinically confirmed) 35 63
EXOTIC/ UNUSUAL Plague 0 0
H I
GH
MO
RB
IDIT
/
MO
RT
AL
IY
Meningococcal Meningitis 0 0
Neonatal Tetanus 0 0
Typhoid Fever 0 0
Meningitis H/Flu 0 0
SP
EC
IAL
PR
OG
RA
MM
ES
AFP/Polio 0 0
Congenital Rubella Syndrome 0 0
Congenital Syphilis 0 0
Fever and
Rash
Measles 0 0
Rubella 0 0
Maternal Deaths2 35 23
Ophthalmia Neonatorum 282 343
Pertussis-like syndrome 0 0
Rheumatic Fever 3 6
Tetanus 1 0
Tuberculosis 46 49
Yellow Fever 0 0
Chikungunya 0 4
Zika Virus 0 162
Released November 6, 2017 ISSN 0799-3927
NOTIFICATIONS-
All clinical
sites
INVESTIGATION
REPORTS- Detailed Follow
up for all Class One Events
HOSPITAL ACTIVE
SURVEILLANCE-30
sites*. Actively pursued
SENTINEL
REPORT- 79 sites*.
Automatic reporting
*Incidence/Prevalence cannot be calculated
5
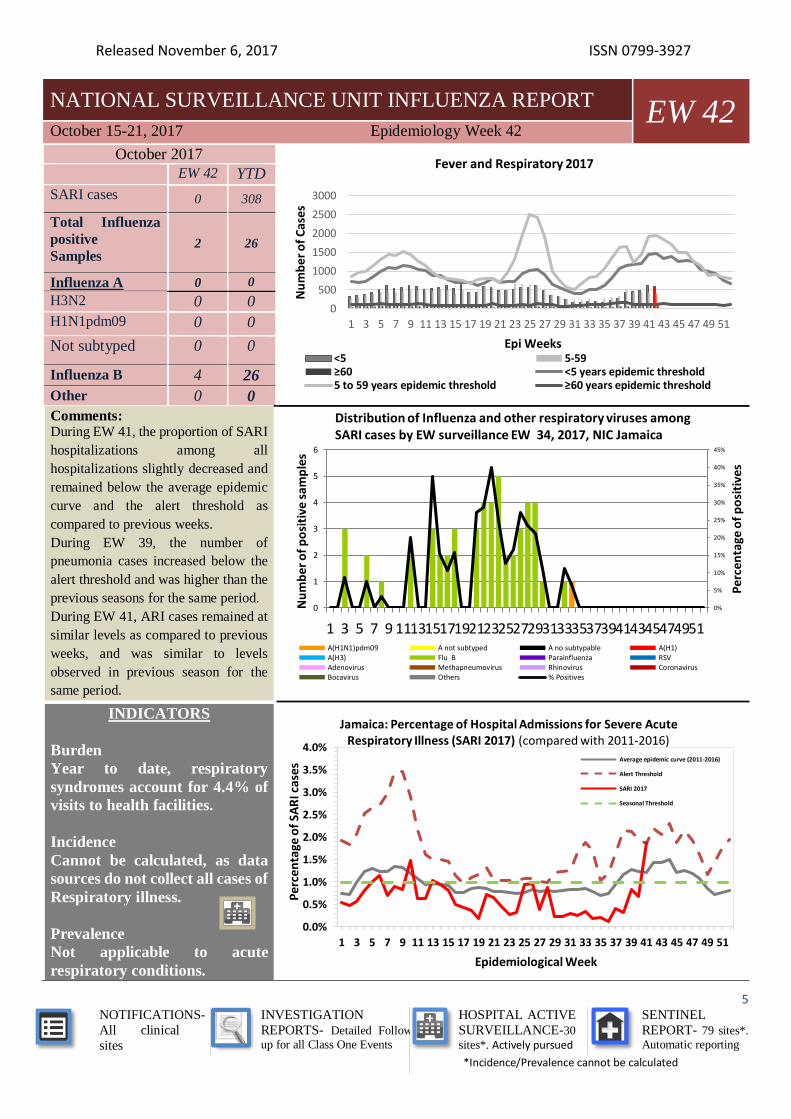
NATIONAL SURVEILLANCE UNIT INFLUENZA REPORT EW 42
October 15-21, 2017 Epidemiology Week 42
October 2017
EW 42 YTD
SARI cases 0 308
Total Influenza
positive Samples
2 26
Influenza A 0 0
H3N2 0 0
H1N1pdm09 0 0
Not subtyped 0 0
Influenza B 4 26
Other 0 0
Comments: During EW 41, the proportion of SARI
hospitalizations among all
hospitalizations slightly decreased and
remained below the average epidemic
curve and the alert threshold as
compared to previous weeks.
During EW 39, the number of
pneumonia cases increased below the
alert threshold and was higher than the
previous seasons for the same period.
During EW 41, ARI cases remained at
similar levels as compared to previous
weeks, and was similar to levels
observed in previous season for the
same period.
INDICATORS
Burden
Year to date, respiratory
syndromes account for 4.4% of
visits to health facilities.
Incidence
Cannot be calculated, as data
sources do not collect all cases of
Respiratory illness.
Prevalence
Not applicable to acute
respiratory conditions.
0
500
1000
1500
2000
2500
3000
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Nu
mb
er o
f C
ases
Epi Weeks
Fever and Respiratory 2017
<5 5-59≥60 <5 years epidemic threshold5 to 59 years epidemic threshold ≥60 years epidemic threshold
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
0
1
2
3
4
5
6
1 3 5 7 9 111315171921232527293133353739414345474951
Per
cen
tage
of
po
siti
ves
Nu
mb
er o
f p
osi
tive
sam
ple
s
Distribution of Influenza and other respiratory viruses among SARI cases by EW surveillance EW 34, 2017, NIC Jamaica
A(H1N1)pdm09 A not subtyped A no subtypable A(H1)A(H3) Flu B Parainfluenza RSVAdenovirus Methapneumovirus Rhinovirus CoronavirusBocavirus Others % Positives
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
3.0%
3.5%
4.0%
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Per
cen
tage
of
SAR
I cas
es
Epidemiological Week
Jamaica: Percentage of Hospital Admissions for Severe Acute Respiratory Illness (SARI 2017) (compared with 2011-2016)
Average epidemic curve (2011-2016)
Alert Threshold
SARI 2017
Seasonal Threshold
Released November 6, 2017 ISSN 0799-3927
NOTIFICATIONS-
All clinical
sites
INVESTIGATION
REPORTS- Detailed Follow
up for all Class One Events
HOSPITAL ACTIVE
SURVEILLANCE-30
sites*. Actively pursued
SENTINEL
REPORT- 79 sites*.
Automatic reporting
*Incidence/Prevalence cannot be calculated
6
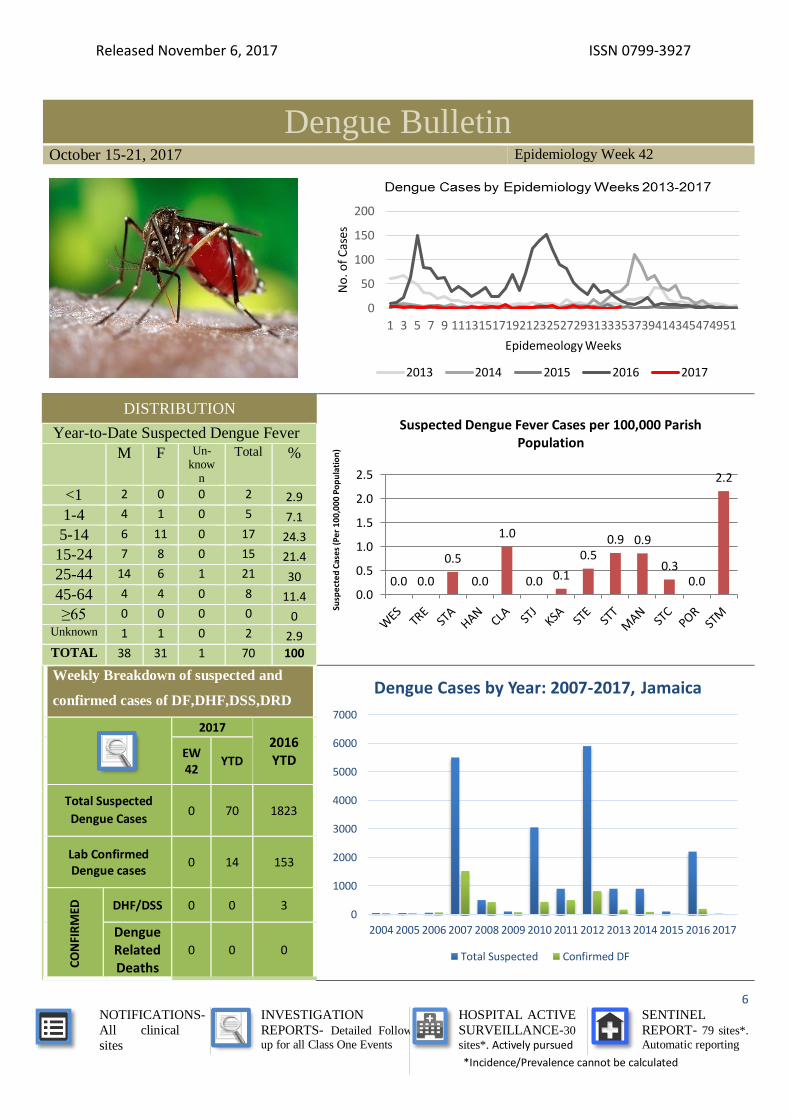
Dengue Bulletin October 15-21, 2017 Epidemiology Week 42
DISTRIBUTION
Year-to-Date Suspected Dengue Fever
M F Un-know
n
Total %
<1 2 0 0 2 2.9
1-4 4 1 0 5 7.1
5-14 6 11 0 17 24.3
15-24 7 8 0 15 21.4
25-44 14 6 1 21 30
45-64 4 4 0 8 11.4
≥65 0 0 0 0 0 Unknown 1 1 0 2 2.9 TOTAL 38 31 1 70 100
Weekly Breakdown of suspected and
confirmed cases of DF,DHF,DSS,DRD
2017
2016 YTD EW
42 YTD
Total Suspected
Dengue Cases 0 70 1823
Lab Confirmed Dengue cases
0 14 153
CO
NFI
RM
ED
DHF/DSS 0 0 3
Dengue Related Deaths
0 0 0
0
50
100
150
200
1 3 5 7 9 111315171921232527293133353739414345474951N
o. o
f C
ases
Epidemeology Weeks
2013 2014 2015 2016 2017
0.0 0.0
0.5
0.0
1.0
0.0 0.1
0.50.9 0.9
0.30.0
2.2
0.0
0.5
1.0
1.5
2.0
2.5
Susp
ect
ed
Cas
es
(Pe
r 1
00
,00
0 P
op
ula
tio
n)
Suspected Dengue Fever Cases per 100,000 Parish Population
0
1000
2000
3000
4000
5000
6000
7000
2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
Dengue Cases by Year: 2007-2017, Jamaica
Total Suspected Confirmed DF
Released November 6, 2017 ISSN 0799-3927
NOTIFICATIONS-
All clinical
sites
INVESTIGATION
REPORTS- Detailed Follow
up for all Class One Events
HOSPITAL ACTIVE
SURVEILLANCE-30
sites*. Actively pursued
SENTINEL
REPORT- 79 sites*.
Automatic reporting
*Incidence/Prevalence cannot be calculated
7
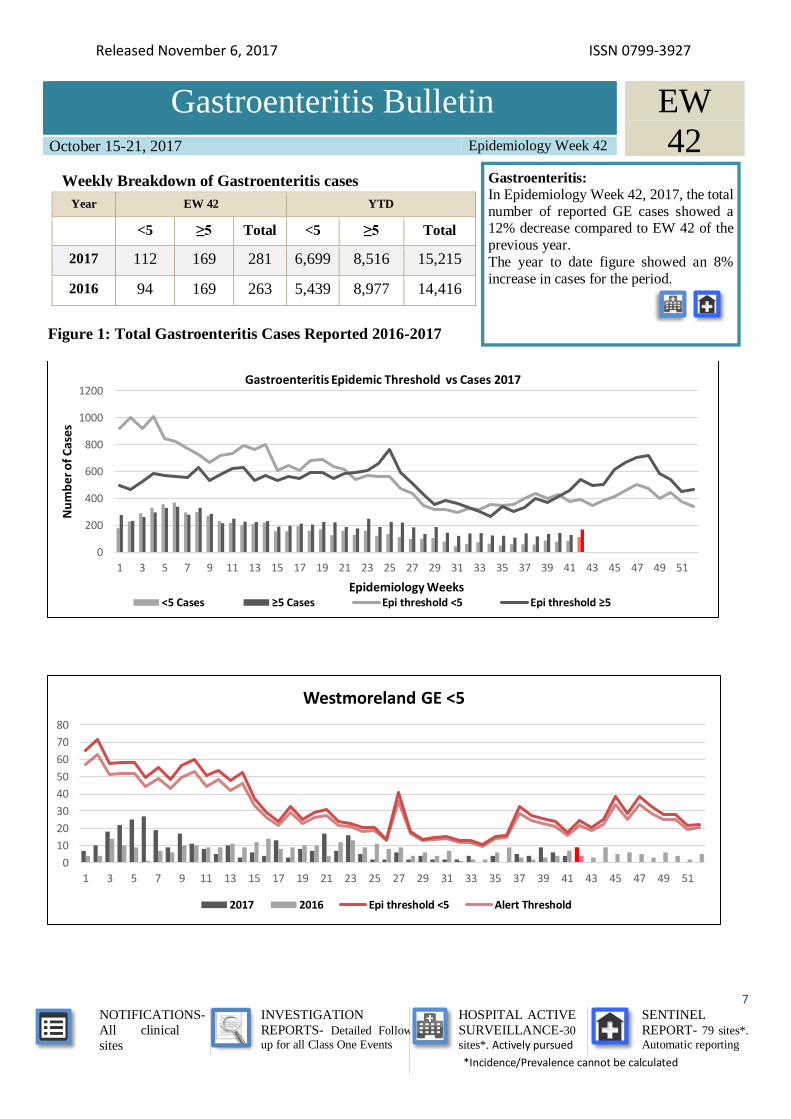
Gastroenteritis Bulletin October 15-21, 2017 Epidemiology Week 42
Year EW 42 YTD
<5 ≥5 Total <5 ≥5 Total
2017 112 169 281 6,699 8,516 15,215
2016 94 169 263 5,439 8,977 14,416
Figure 1: Total Gastroenteritis Cases Reported 2016-2017
0
200
400
600
800
1000
1200
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Nu
mb
er o
f C
ase
s
Epidemiology Weeks
Gastroenteritis Epidemic Threshold vs Cases 2017
<5 Cases ≥5 Cases Epi threshold <5 Epi threshold ≥5
0
10
20
30
40
50
60
70
80
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Westmoreland GE <5
2017 2016 Epi threshold <5 Alert Threshold
EW
42 Weekly Breakdown of Gastroenteritis cases Gastroenteritis:
In Epidemiology Week 42, 2017, the total
number of reported GE cases showed a 12% decrease compared to EW 42 of the
previous year.
The year to date figure showed an 8%
increase in cases for the period.

Released November 6, 2017 ISSN 0799-3927
NOTIFICATIONS-
All clinical
sites
INVESTIGATION
REPORTS- Detailed Follow
up for all Class One Events
HOSPITAL ACTIVE
SURVEILLANCE-30
sites*. Actively pursued
SENTINEL
REPORT- 79 sites*.
Automatic reporting
*Incidence/Prevalence cannot be calculated
8
RESEARCH PAPER
Strengthening Health Care Systems for HIV and AIDS in Jamaica: A Programme of Research and Capacity
Building 2007-2012
N Edwards1, E Kahwa2, D Kaseje3, J Mill4, J Webber5, S Roelofs6, M Walusimbi7, H Klopper8, J Harrowing8
1University of Ottawa, Canada
2The UWI School of Nursing, Mona, University of the West Indies, Jamaica
3Great Lakes University of Kisumu, Kenya,
4University of Alberta, Canada
5Canadian Nurses’ Association, Canada,
6Mulago Hospital, Uganda
7University of Western Cape, South Africa,
8University of Lethbridge, Canada
Objectives: To contribute to health systems strengthening for HIV and AIDS care in Jamaica by fostering dynamic
and sustained engagement of nurses in the process of change through capacity building in research and policy.
Methods: This work was done as part of an international program of research which was implemented in Jamaica
and three African countries (Kenya, Uganda and South Africa). Using mixed methods and participatory action
research, we tested the “leadership hub model” to invigorate nurses’ involvement in policy and research and
improve nursing care. Data collection included cross sectional surveys of nurses on clinical practice, quality
assurance and stigma; an institutional assessment of workplace policies and the impact of the HIV epidemic on the
nursing workforce. Capacity building included training in the policy development process, training in research skills
including opportunities for collaborating on research projects, research grants for junior investigators, and research
internships for nurses.
Results: Three research projects were completed in Jamaica. Sixteen (16) Jamaican nurses participated in the
international research internship to build capacity for research. Frontline nurses, nurse researchers, and decision
makers improved capacity in using and leading research to influence policy. Three (3) research proposals by junior
nurse researchers and three (3) HIV policy evaluation proposals by leadership hubs were funded and successfully
completed.
Conclusions: This program of research built research and policy capacity among nurses for leadership roles in
improving equity, quality and efficiency of health systems for HIV and AIDS care. Findings from the three
interrelated research projects will be presented.
The Ministry of Health
24-26 Grenada Crescent
Kingston 5, Jamaica
Tele: (876) 633-7924
Email: [email protected]






![[PPT]Inflammation/Fever - Arkansas State · Web view* Many non-infectious disorders can also produce fever NON-SPECIFIC Patterns of fever: Intermittent fever Remittent fever Sustained](https://img.pdfslide.us/doc/110x75/5ab7b6f17f8b9a28468bebe4/pptinflammationfever-arkansas-state-view-many-non-infectious-disorders-can.jpg)








![Dengue Fever/Severe Dengue Fever/Chikungunya Fever · Dengue fever and severe dengue (dengue hemorrhagic fever [DHF] and dengue shock syndrome [DSS]) are caused by any of four closely](https://img.pdfslide.us/doc/110x75/5e87bf3e7a86e85d3b149cd7/dengue-feversevere-dengue-feverchikungunya-dengue-fever-and-severe-dengue-dengue.jpg)










