Embed Size (px)
Citation preview


Webinar AgendaWelcome & Introductions
Todd Molfenter, Dep. Director, NIATx, University of WI-Madison
Improving Collaboration Between PC & BHDavid Bingaman, Dep. Regional Administrator, HRSA Region V
Integration Models Laura Galbreath, Dep. Director, SAMHSA/HRSA Center for Integrated Health Solutions, National Council for Community Behavioral Healthcare
WI Case: Tri-County PartnershipsKristene Stacker, Exec. Dir., Fox Cities Community Health Center
Project Invitation – Next Steps

Improving Collaboration between Primary Care and
Behavioral Health Providers
December 13, 2011
David Bingaman, LCSWDHHS, HRSA
Office of Regional Operations

Improving Collaboration
• Cartesian Dichotomy• Separation/Fragmentation• Growing economic incentives
for a more effective approach

Improving Collaboration
• Primary care foundation• PCPs deliver half of BH care• PCPs prescribe 70% of
psychotropic drugs• PCPs have limited BH
training; widespread under diagnosis

Improving Collaboration
Impact of Mental Illness:26% suffer from a diagnosable
mental disorder in a given year; half meet criteria for 2 or more
Half of all cases begin by age 14 and ¾ have begun by age 24
Up to 70% of primary care visits stem from psychosocial issues

Improving Collaboration
• PCPs have limited time to treat psychosocial issues
• BH care inaccessible to PCPs• Many referrals do not result
in visits/services• Limited capacity of BH
system

Improving Collaboration
• MH consumers less likely to receive primary medical care
• SMI associated with increased morbidity and mortality

Improving Collaboration
Drivers of Change:• Berwick’s Triple Aim: Better care,
better health, and reduced cost through quality improvement
• Patient Centered Medical Home (2011)
• State and Federal budget cuts

Improving Collaboration
Drivers of Change, continuedAffordable Care Act:
Community Health CentersMedicaidMental Health & Substance Abuse ServicesAccountable Care Organizations

Improving CollaborationNASMHP Director’s Report: “Goodpublic policy will work to sustain,support and require integration ofservices between the two “safetynet” systems of CHCs and MHproviders with integration rangingfrom coordination of care to fullintegration of medical andbehavioral service.”

HRSA’s Resources for B.H. Integration into
Primary Care
http://bphc.hrsa.gov/technicalassist
ance/taresources/index.html

David Bingaman, LCSWDeputy Regional AdministratorHealth Resources & Services
Administration (HRSA)U. S. Department of Health & Human
Services233 N. Michigan Ave., Suite 200Chicago, IL [email protected]

Models for Primary and Behavioral Health Integration
Laura M Galbreath, MPP
Deputy Director, CIHS

“…in essence integrated health care is the systematic coordination of physical and behavioral health care. The idea is that physical and behavioral health problems often occur at the same time. Integrating services to treat both will yield the best results and be the most acceptable and effective approach for those being served.”
Connecting Body & Mind: A Resource Guide to Integrated Health Care in Texas and the U.S., Hogg Foundation for Mental Health

Primary Care Behavioral Health
Behavioral Health Referrals
Physical Health Status
CollaborativeCare

Individuals with Serious Mental Illness - The StatisticsPersons with serious mental illness (SMI) are dying at the
average age of 53 (comparable to Sub-Saharan Africa)While suicide and injury account for about 30-40% of
excess mortality, 60% of premature deaths in persons with schizophrenia are due to medical conditions such as cardiovascular, pulmonary and infectious diseases (NASMHPD, 2006)
OR state study found that those with co-occurring MH/SU disorders were at greatest risk (average age of death=45.1 years)



Top Ten Areas for Consideration in Developing and Supporting Patient Centered Health Care Homes
•State Level Leadership
•State Level Management
•Models/Strategies
•Culture
•Workforce
•Collaboration
•Confidentiality
•Finance
•Data
•Training

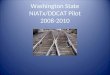
The Four Quadrant Clinical Integration Model (MH/SU)
Quadrant II
MH/SU PH Outstationed medical nurse
practitioner/physician at MH/SU site (with standard screening tools and guidelines) or community PCP
MH/SU clinician/case manager w/ responsibility for coordination w/ PCP
Specialty outpatient MH/SU treatment including medication-assisted therapy
Residential MH/SU treatment Crisis/ED based MH/SU interventions Detox/sobering Wellness programming Other community supports
Quadrant IV
MH/SU PH Outstationed medical nurse
practitioner/physician at MH/SU site (with standard screening tools and guidelines) or community PCP
Nurse care manager at MH/SU site MH/SU clinician/case manager External care manager Specialty medical/surgical Specialty outpatient MH/SU treatment
including medication-assisted therapy Residential MH/SU treatment Crisis/ED based MH/SU interventions Detox/sobering Medical/surgical inpatient Nursing home/home based care Wellness programming Other community supports
MH
/SU R
isk
/Co
mp
lexit
y
Quadrant I
MH/SUPH PCP (with standard screening tools
and MH/SU practice guidelines for psychotropic medications and medication-assisted therapy)
PCP-based BHC/care manager (competent in MH/SU)
Specialty prescribing consultation Wellness programming Crisis or ED based MH/SU
interventions Other community supports
Quadrant III
MH/SU PH PCP (with standard screening tools and
MH/SU practice guidelines for psychotropic medications and medication-assisted therapy)
PCP-based BHC/care manager (competent in MH/SU)
Specialty medical/surgical-based BHC/care manager
Specialty prescribing consultation Crisis or ED based MH/SU interventions Medical/surgical inpatient Nursing home/home based care Wellness programming Other community supports
Physical Health Risk/Complexity
Low High
Low
Hig
h
Persons with serious MH/SU conditions could be served in all settings. Plan for and deliver services based upon the needs of the individual, personal choice and the specifics of the community and collaboration.

Models of Bi-Directional IntegrationBehavioral Health –Disease Specific
• IMPACT• RWJ• MacArthur Foundation• Diamond Project• Hogg Foundation for Mental Health• Primary Behavioral Healthcare Integration
Grantees
Behavioral Health - Systemic Approaches• Cherokee Health System• Washtenaw Community Health
Organization• American Association of Pediatrics - Toolkit• Collaborative Health Care Association• Health Navigator Training
Physical Health• TEAMcare• Diabetes (American Diabetes Assoc)• Heart Disease• Integrated Behavioral Health Project –
California – FQHCs Integration • Maine Health Access Foundation –
FQHC/CMHC Partnerships• Virginia Healthcare Foundation – Pharmacy
Management• PCARE – Care Management
Consumer Involvement• HARP – Stanford• Health and Wellness Screening – New
Jersey (Peggy Swarbrick)• Peer Support (Larry Fricks)

Primary and BehavioralHealth Integration Works
PC→BH P-CARE - NIMH-funded Trial Medical case management for individuals
with serious mental illnesses Fewer medical ER visits, improved cardio
risk factors, and more likely to have a usual source of PCP care
PC→BH Diabetes Care Coordination - AHRQ Health Care Innovation
Nursing and mental health care coordination to educate and empower clients with SMI to manage their diabetes
The number of clients with ideal blood sugar levels increased from 32% to 43%. Mean health risk status improved significantly from baseline to program.
23
BH→PC RESPECT – MacArthur Initiative Cluster randomized controlled trial 60% response to treatment and 37% remission at
6 months, compared to 47% and 27% in usual care practices
BH→PC IMPACT Study Randomized clinical trial of collaborative care
intervention for elderly patients Showed significant improvements in symptoms
and functionality at 6 months, 12 months, and 2 years
BH→PC DIAMOND Initiative Adapted IMPACT program for general population
setting and studied outcomes 64% response to treatment and 44% remission at
6 months; 72% response and 52% remission at 12 months

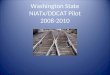
Relapse Prevention
Patient Registry Screening/ Monitoring
Consulting PsychiatristCare Manager
Primary Care Provider
Stepped CareApproach
Components of Collaborative Care Model

Collaborative care’s key ingredientsCare management – Patient education & empowerment, ongoing monitoring, care/provider coordination
Evidence-based treatments – Effective medication management, psychotherapy, disease management
Expert consultation for patients who are not improving
Systematic diagnosis and outcome tracking
Stepped care
Technology support – registriesJ. Unutzer, 2010, www.cimh.org/LinkClick.aspx?fileticket=84F6JQndwg8%3d&tabid=804 S. Gilbody et al, Arch Intern Med. 2006;166:2314-2321

Lessons from Practice Transformation to a Patient-Centered Medical Home
Six lessons from 36 family practice settings across the country that participated in a two-year practice transformation project1. “Becoming a patient-centered medical home (PCMH) requires transformation.
2. Technology needed for the PCMH is not plug-and- play.
3. Transformation to the PCMH requires personal transformation of physicians.
4. Change fatigue is a serious concern even within capable and highly motivated practices.
5. Transformation to a PCMH is a developmental process.
6. Transformation is a local process.”
Resonates with the experience in implementing integrated care—this is also a process of transforming personal and organizational practice in the context of local relationships—ideally, the medical home and integration
changes can be woven together

Services Available from CIHS
• Web-based Resources (http://www.integration.samhsa.gov)
• eSolutions Newsletter• National Webinars• Regional and State Based Learning Communities• Health Home Consultation to States

Tri-County Partnerships
Calumet, Outagamie and Winnebago Counties working
together with Fox Cities Community Health Center.

Who am I?
Kristene Stacker, R.N. Executive Director Fox Cities Community Health Ctr. (FCCHC)

Fox Cities Community Health Center: FCCHC
Started in 1997 as free community clinic.
2005 became a FQHC (Federally Qualified Community Health Center).
Board of Directors comprised of 51% consumer/users of the Health Center.
2009 served 6,989 individual consumers with 22,000 encounters.

Service Area Outagamie County:
176,695K; 9.8% growth since 2000. 11.9% over 65; 24.7% under 18. 91% white;.1% black; 1.7% American Indian; 3%
Asian 3.6% Hispanic. 8.7% below poverty. (increase from 6.9 in 09) Health and Human Services agency. Regionalized Family Care County. County HHS Budget of 59.3 million. Median household income $55,100

Service Area Winnebago County:
166,994 (2010 data) 12.8% 65 or older; 21.1% under 18 92.59% white, 1.8 %Black, 3.5% Hispanic, .6%
Native American, 2.3 Asian. 11.9 % Below Poverty increase from 6.9 in 2009) Human Services Agency. Regionalized Family Care County. 58 Million County HS Budget. Median Household income $47,486

Service Area Calumet County:
48,971K 20.5% growth since 2000. 3rd fastest growing county is State. 94.3 % White,
.5 %Black, 3.5% Hispanic,2.1@ Asian, .4% Native American.
26.9 under 18; 10.8 over 65. 5.5 % Below Poverty. Median Household income $65,600 Health and Human Services. Regionalized Family Care. 14.9 million County HS Budget (2011).

Outagamie/FCCHC MH Pilot
2009 began discussions. 4 main objectives
Address increasing length of wait for outpatient MH services.
Increase MH services available. Increase access for Medical Assistance
patients. Begin integration of MH into primary
care.

A Phased Approach to Expansion
Phase I began 4/09 with FCCHC IM physician providing care at crisis diversion facility.
Phase II increase FCCHC’s MH counselor to 70% productivity expectation and add 2 contracted MH therapists from County to FCCHC.

Phased Approach
Phase III 8/09 added contract psychiatrist 6 hours per week.
Additional 4 hours per month psychiatric care to Brewster Village (County Nursing Home).
Most recently, increased to 14 hours per week of psychiatry time.

Phased Approach-2011 Added 2 FTE Licensed Professional
Counselors to clinic employment in 2011.
Calumet County added LPC for weekly contract hours for group treatment related to sex offender grant.
Added contract BH providers through county contracts and other community providers.

Project Outcomes FCCHC saw improvement in both
provider productivity and management of MH program.
FCCHC had 900 MH visits in first 6 months w/ average no show rate of 15% (reduced from 30-40%).
Increase in access to MH services within the region. FCCHC access to MH services 5 days/wk.

Next Steps Todd Molfenter, Dep. Director, NIATx, University of WI-Madison
InvitationFive-month collaborative (Feb-July 2012), no fee to
participate.Improve collaboration between FQHCs and behavioral
health agencies offering substance abuse services. Application:
http://www.niatx.net/WordDoc/WICollaboration/application_WI.docxApplication deadline: Friday, January 6, 2012
Project KickoffWorkshop: Madison, February 16, 8:30am-3:30pm
Questions? Call Carol Sherbeck, (608) 265-5997
or email [email protected]